 Samina Naeem Khalid1*
Samina Naeem Khalid1* Farid Midhet2
Farid Midhet2 Qudsia Uzma3
Qudsia Uzma3 Ellen Mpangananji Thom4
Ellen Mpangananji Thom4 Shehla Baqai2
Shehla Baqai2 Muhammad Talha Khan2
Muhammad Talha Khan2 Areeba Memon5
Areeba Memon5
- 1MNCH Department, Health Services Academy, Islamabad, Pakistan
- 2Bahria University Medical & Dental College, Bahria Medical University Campus, Karachi, Pakistan
- 3MNCAH (Maternal Neonatal, Child and Adolescent Health), World Health Organization, NIH, Islamabad, Pakistan
- 4Reproductive Health, World Health Organization, NIH, Islamabad, Pakistan
- 5Resident Internal Medicine, SUNY Upstate Medical University, Syracuse, NY, United States
Background: Induced abortions (IA) remain a serious public health issue in Pakistan despite social constraints and legal prohibitions. The number is alarmingly high, and the study done by the Population Council (2012) indirectly estimated 2.2 million abortions per year and an abortion rate of 50 per 1,000 women.
Methodology: This study reports the results of a secondary data analysis of the Pakistan Maternal Mortality Survey 2019 to compare the women who reported having an IA in the last three years with those having a live birth in the same period. A nested case-control comparison of women reporting IA as cases and those having a live birth as controls. Logistic regression was used to estimate odds ratios (OR) for major risk factors of maternal mortality after adjusting for women's age, parity, education, and wealth quintile.
Results: Results show that recent use of family planning, having a prior history of pregnancy loss, and higher gravidity are all linked to IA (P < 0.05). On the other hand, neither the average household education nor the women's education affects the rates. The other associated factors include parity, past use of family planning, socioeconomic status, place of residence, and the educational level of women. These correlations are based only on uncorrected odds ratios and do not account for confounding variables.
Conclusion: Women having past miscarriages, having several children, or improperly using family planning methods are more likely to have induced abortions. These findings can help medical professionals develop evidence-based policies and regulations.
Background
Globally, an estimated 73 million induced abortions occur each year, roughly 29% of all pregnancies. Among the unintended pregnancies, 61% end up in an abortion, and most of these abortions are clandestine and unsafe (1). It is a major preventable cause of maternal mortality and morbidity. The complications of unsafe abortions lead to both physical and mental health issues, which place women in cumbersome social and financial affliction, and burden communities and the health care system. The lack of provision of safe, timely, affordable, and respectful post-abortion care services is a critical public health problem (2). Between 2010 and 2014, Ganatra and colleagues estimated that 25 million unsafe abortions were performed worldwide, while a staggering 88% occurred in developing countries. Asia, in particular South and Central Asia, contributed to more than half of these unsafe abortions. This sheds light on the impact of unsafe abortion in places with already limited access to services of safe abortion (3).
Despite a significant decline in fertility since the 1990s, a relatively high total fertility rate (TFR) grapples Pakistan with a current estimate of 3.6 births per woman. The unmet need for family planning remains high at about 17.3%, and the majority of pregnancies are unintended (4). The most likely reason for this is the low use of modern contraceptives: just 48.6% of couples utilize a modern method of family planning. In Pakistan, the only data on the incidence of induced abortions comes from indirect studies. Using the Abortion Incidence Complications Method (AICM), the Population Council estimated that the number of induced abortions was 2.25 million in 2012, with an abortion rate of 50 per 1,000 reproductive-age women (15–49 years) (5). In a second round of this study in 2023, the abortion rate was estimated at 66 per 1,000 women of reproductive age (6). Post-abortion complications were reported to have increased in this period, from 15% in 2012 to 21% in 2023.
The AICM mainly uses data on women undergoing post-abortion care (PAC) reported in health facilities to indirectly estimate the total incidence of induced abortions. To account for abortions that do not require medical care, the AICM uses a multiplier, which is the inverse of the fraction of abortions that result in the utilization of facility-based care. Though the AICM attempts to distinguish between induced and spontaneous abortions, it assumes an implausibly low (indeed, factually incorrect) incidence of miscarriages. This methodological flaw therefore concludes an artificially or erroneously high number of induced abortions. Moreover, the AICM assumes that miscarriages rarely require medical care, even though they occur in 10%–20% of pregnancies and many need treatment. In Mexico, AICM estimates were up to 10 times higher than actual figures due to misclassified miscarriages (7). Critics argue that reliance on aggregated health facility data further distorts results, especially in regions with limited diagnostic capabilities.
Pakistan's maternal mortality ratio (MMR) declined from 276 deaths per 100,000 live births in 2007 (Pakistan Demographic and Health Survey) to 186 in 2019 (Pakistan Maternal Mortality Survey). During this period, the proportion of maternal deaths due to abortion-related complications doubled, from 5% in 2007 to 10% in 2019. However, it may be noted that the assignment of cause of maternal death in the two surveys was through a process of verbal autopsy (VA) interviews and a review of VA information by a panel of experts and that the classification of causes may not always explicitly distinguish induced abortion from spontaneous abortion (miscarriage) or ectopic pregnancy (8).
Abortion has remained a controversial subject in Pakistan, which practices a near-total ban on this procedure. More recently, the government of Pakistan has begun to shoulder more responsibilities to address safe abortion service provision within the current laws, together with NGO support (9). There remains, however, the practice of unsafe abortion, particularly in women of low socio-economic status, which leads to medical complications and death (10). Women in Pakistan are bound in an intricate knot of laws regarding abortion, where women have to bear mental, psychological, social, and legal consequences whenever they seek abortion services (11).
Abortion stigma still exists significantly in Pakistani society, which affects women who have had an abortion. This stigma often leads to secrecy, suffering, and isolation among the affected (12). Although the majority of Pakistanis appear to condone having an abortion as long as there is danger posed to physical health, this is far less accepted when the intended reason for abortion is mental health (13). Recently, there has been progress in the political scenario where both the NGOs and the government have worked together to focus on unsafe abortion as a public health issue (9). Additionally, measuring abortion prevalence in Pakistan presents considerable challenges due to the interlinking of legal restrictions and societal stigma. A survey in Karachi found that 16% of women over the age of 18 years had an abortion, much more than the rate of abortion obtained by asking respondents directly. This result indicates that indirect exposure may be successful in increasing the reporting of abortion (14).
Even though unsafe abortion is prevalent, as shown by the Pakistan Maternal Mortality Survey conducted in 2019 and other studies, there is still a lack of understanding of the underlying causes of induced abortion. This in-depth analysis, therefore, focuses on providing answers to the questions raised above in terms of the demographic, reproductive, and socio-cultural factors that influence abortion decision-making.
Methodology
Pakistan Maternal Mortality Survey 2019 (PMMS 2019) was a national survey exclusively on maternal mortality and morbidity, which was conducted by the National Institute of Population Studies (4), Government of Pakistan, with technical assistance from the Demographic and Health Surveys (DHS), USAID. The sample included 136,226 households in the four provinces, AJK, and GB. Births and deaths of the last three years were recorded to identify maternal deaths and estimate the maternal mortality ratio. In a 10% sub-sample of households, 14,703 ever-married women aged 15–49 years were interviewed to identify complications of health services utilization in pregnancy, delivery, and postpartum in the last three years (8).
All women reporting a pregnancy in the last three years were asked about induced abortion; however, there was possible under-reporting (abortion rate was 12/1,000 women aged 15–49), and direct estimation of the abortion rates by biological, demographic, and socioeconomic factors would have been misleading. To overcome this difficulty, an unmatched nested case-control study was designed, whereby the women who reported an induced abortion in the last 3 years were regarded as cases (n1 = 170; sampling fraction = 1.00). The controls were randomly selected from women who reported having a live birth during the last three years (n2 = 1,729; sampling fraction = 0.20). Binary logistic regression (SPSS version 19.0) was used to estimate adjusted odds ratios (AOR) for the association between reported induced abortion and the risk factors of interest. The sampling scheme of the PMMS 2019 was such that the clusters were numerous (n = 1,096) and of very small size. Because the intra-cluster correlations were close to zero, the need for generalized estimating equations (GEE) was not critical. A comparison was made of the women reporting an induced abortion with those having a live birth in the same period to find the differences in biological and socio-demographic risk factors. The adjusted odds ratios, along with the 95% confidence intervals and p-value, were calculated.
Results
The causal links of age, parity, and pregnancy history on the odds of induced abortion were adjusted for household socioeconomic status (14) Urban/Rural residences were analyzed. Table 1 presents the adjusted odds ratios (AOR) and 95% confidence intervals (CI) to assess the significance of the associations. The history of prior pregnancy loss indicates that women with a history of at least one pregnancy loss have 1.55 times higher odds of induced abortion compared to those with no previous pregnancy loss (p < 0.05). Table 1 further shows that the odds of induced abortion do not significantly differ between nulligravida (no previous pregnancies) and women with 1–5 pregnancies. However, women with six or more pregnancies have 2.65 times higher odds of induced abortion compared to nulligravida (p < 0.05).
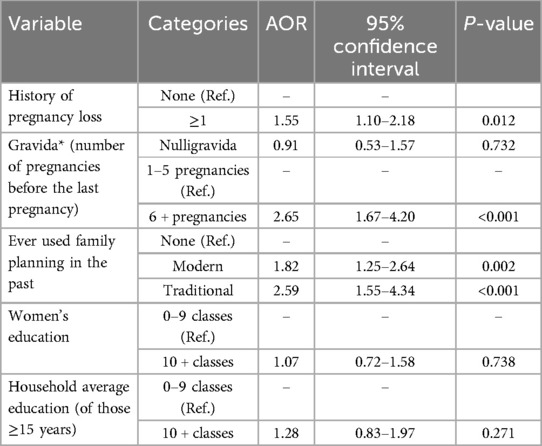
Table 1. Association of history of pregnancy loss, gravidity, ever use of family planning, women's education, and household average education on induced abortions: adjusted odds ratios (AOR) and 95% confidence limits (adjusted for age, parity, household's SES, and urban/rural residence).
Women who have ever used modern or traditional family planning methods have significantly higher odds of induced abortion compared to those who have not used any family planning methods. The odds ratios are 1.82 and 2.59, respectively. There is no significant association between a woman's education level (10 or more classes) and the odds of induced abortion. Also, there is no significant association between the household's average education level (10 or more classes) and the odds of induced abortion.
Table 2 presents the unadjusted OR and 95% CI for the association of age, parity, and pregnancy history with the odds of induced abortion. In terms of age group, compared to women aged 25–34 years (reference category), those under 25 years had slightly lower odds of induced abortion (OR = 0.69). Still, this difference was not statistically significant (p = 0.072). Similarly, women aged 35 years and above had slightly higher odds of induced abortion (OR = 1.31), but again, this difference was not statistically significant (p = 0.531).
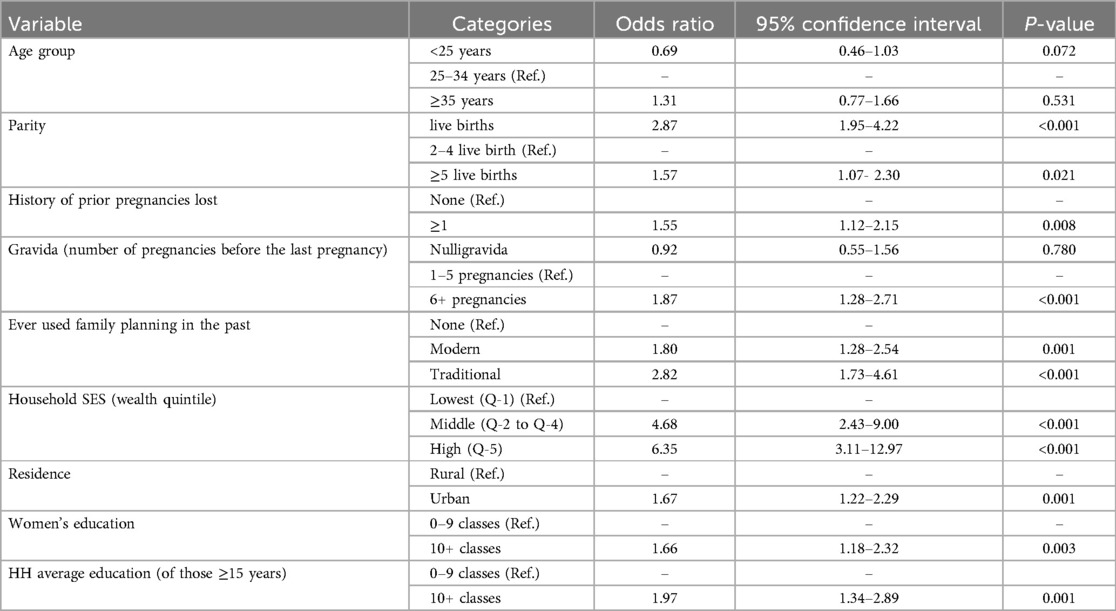
Table 2. Association of age, parity, and pregnancy history on the odds of induced abortion: unadjusted odds ratios and 95% confidence limits.
Regarding parity, women with 2–4 live births (reference category) had significantly higher odds of induced abortion compared to those with 1 live birth (OR = 2.87, p < 0.001). On the other hand, women with five or more live births also had slightly higher odds of induced abortion (OR = 1.57, p-value of 0.021). Considering the history of pregnancy loss, women with at least one pregnancy loss had significantly higher odds of induced abortion compared to those with no history of pregnancy loss (OR = 1.55, p = 0.008).
Table 2 also shows that the nulligravida women (those who have never been pregnant before) had slightly lower odds of induced abortion compared to women with 1–5 pregnancies (OR = 0.92), not statistically significant (p = 0.780). However, women with 6 or more pregnancies had significantly higher odds of induced abortion (OR = 1.87, p < 0.001).
When considering the use of family planning methods in the past, or having ever used modern methods of family planning, there were significantly higher odds of induced abortion compared to those who had not used any family planning methods (OR = 1.80, p = 0.001). Similarly, women who had used traditional family planning methods had even higher odds of induced abortion (OR = 2.82, p < 0.001).
Table 2 also shows that compared to the women in the lowest SES category (Q-1), middle (Q-2 to Q-4), and high (Q-5) SES categories had significantly higher odds of induced abortion (OR = 4.68 and 6.35, respectively, both p < 0.001). Similarly, women residing in urban areas had significantly higher odds of induced abortion (OR = 1.67, p = 0.001). Additionally, women with higher levels of education had significantly higher odds of induced abortion (ORs = 1.66, p < 0.001). Similarly, in households with higher average education, the odds of induced abortion were also significantly higher (OR = 1.97, p < 0.001).
According to Table 3, the use of long-acting Reversible Contraception (LARC) before the last pregnancy was associated with significantly higher odds of induced abortion (OR = 2.75, p = 0.002). Similarly, the use of traditional family planning methods was also associated with significantly higher odds of induced abortion (OR = 2.62, p < 0.001). On the other hand, the use of short-term family planning methods was associated with moderately higher odds of induced abortion (OR = 1.68, p = 0.011). The use of modern family planning methods also showed a significant association with increased odds of induced abortion (OR = 1.82, p = 0.002).

Table 3. Family planning method ever used (before the last pregnancy) and the odds of induced abortion.
The odds of Induced Abortion with sons and daughters alive show that if there are no previous children (reference group), women with 1–2 sons alive had significantly higher odds of induced abortions (OR = 1.90, p = 0.013). However, women with three or more sons alive did not show a significant difference (OR = 0.88, 95% CI: 0.57–1.37, p = 0.584). Similarly, women with 1–2 daughters alive had significantly higher odds of induced abortions compared to women with no previous children (OR = 2.03, p = 0.007). On the other hand, women with three or more daughters alive did not show a significant difference in the odds of induced abortions (OR = 1.02, p = 0.924).
In the present analysis, however, no significant differences in self-reported illness before or during pregnancy were found between women having an abortion and those having a live birth, except for gestational diabetes, which was significantly higher among women who had a live birth. Similarly, there were no significant differences in receiving antenatal care from a skilled provider between the two groups. The PMMS 2019 was a household survey, and data on fetal anomalies were not available. Also, there were no significant differences in the health-seeking behavior of pregnant women having a live birth or having an induced abortion. Unfortunately, PMMS 2019 did not elicit information about the reasons for the decision to seek an induced abortion.
Discussion
The analysis of the PMMS 2019 offers an account of various factors that influence maternal mortality in the country (8). This article aims to provide a comprehensive overview of induced abortions based on the findings of this survey. The goal is to contribute to the existing body of knowledge and guide efforts to improve women's reproductive health outcomes in Pakistan. According to the data from the Guttmacher Institute, Pakistan performed almost 2.2 million unsafe abortions in 2012 (5). This emphasizes how urgently more research is required to explore the causes and policy changes to address the issue.
The subject of unsafe abortion is quite complicated and is impacted not only by medical, health, and related variables but also by social and legal challenges. This study highlights the intricate connections between variables influencing induced abortion by looking at the causal links of age, parity, pregnancy history, family planning use, and socioeconomic factors.
The issue of lack of prenatal care and delayed recognition of an unwanted pregnancy are potential contributors to the decision to seek an induced abortion. The data of the present study showed the limitation that women do not seek medical care early in the first trimester of pregnancy, leading to a lack of identification of the complications or abnormalities. This delay can sometimes lead to more complex decisions about abortion later in pregnancy, where options may be more limited. In the present analysis, however, no significant differences were found in health-seeking behavior between the pregnant women who had a live birth and those who had an induced abortion. Utilization of antenatal care does not seem to have an association with the induced abortions reported in the PMMS 2019.
This study showed that age may not significantly impact the likelihood of induced abortions within the studied population. However, age has frequently been mentioned in previous research as a possible contributing factor because of its link to higher parity or unwanted pregnancies (15–17). The absence of notable results in this particular study, however, suggests that other factors might have a greater influence on abortion decisions than age.
There is a significant link between parity and induced abortion. If a woman has two to four live births instead of one, her chance of having an induced abortion is much lower. This could be because women who have had more children tend to be more stable and have more knowledge of reproductive health choices. On the other hand, an increased, albeit not statistically significant, odds of induced abortion are shown in women who have had five or more live births. Socioeconomic pressures related to increased family numbers or health issues could cause this trend. Women who have had more live births are more likely to choose an induced abortion, suggesting that some interventions are required for women who may find it difficult to use family planning (FP). Multiple other studies done in various countries have shown rates of increased induced abortion with increasing parity (18–20).
The findings also suggest that the odds of induced abortion are greatly increased by the history of a miscarriage. Women who have lost a pregnancy at least once are 1.55 times more likely to have an induced abortion than women who have never lost a pregnancy before. This result emphasizes how crucial it is to take prior pregnancy experiences into account when assessing the odds of abortion, as they might be affected by psychological or medical issues that influence their choices for future pregnancies (21–23).
The analysis of the present study shows higher odds of induced abortion with ever use of family planning (FP) methods. This apparent paradox may reflect the influence of reproductive intention, where women using contraception are more motivated to avoid pregnancy and are thus more likely to terminate an unintended pregnancy if it occurs. Moreover, the phenomenon of risk compensation may play a role, wherein the perceived protection provided by FP may incentivize increased sexual activity, thus raising the chances of failure-related unintended pregnancies. In addition, the predominance of short-term or traditional contraceptive methods with higher failure rates may contribute to this trend. These findings underscore the importance of improving access to, and education about, effective contraceptive use and reproductive autonomy (24, 25).
Other factors observed in this study linked with induced abortion include: education levels, urban areas, and socioeconomic status (18). There were higher odds of induced abortion among women who have high socioeconomic status, live in cities, and have more education. Higher socioeconomic status (SES) individuals often face greater opportunity costs, such as disruptions to their career progression, higher education, or modern lifestyle, which can have an impact on their reproductive choices. As a result, they may be more likely to seek an abortion when facing an unintended pregnancy. This pattern might result from complex relationships involving cultural factors, reproductive health awareness, and healthcare availability. Greater access to family planning services may also result from higher SES and education levels, but there may also be more pressure or expectations impacting abortion decisions. The findings of the present study are contrary to the study done in Ethiopia, which shows that illiteracy leads to a lack of uptake of family planning services, leading to unwanted pregnancies (26). Other studies also show that family planning services help to reduce induced abortion rates (27, 28). A study done in Bali also showed these factors influencing rates of induced abortion (28).
According to a study done by the Guttmacher Institute, if all unmet requirements of FP are addressed, the cost of abortion care could be drastically decreased because contraception reduces unplanned pregnancies. For every dollar more spent on increasing access to contraception, Pakistan would save $ 4.52 on the cost of maternity, neonatal, and abortion care for all women of reproductive age (29).
Pakistan's Penal Code of the 1860 legal framework only authorizes abortions when necessary to save a woman's life or for medical purposes. This poses consequences of the refusal of doctors to do abortions on demand and leads to the use of unskilled force, such as Dais (Traditional Birth Attendants) and Quacks, by women seeking induced abortions, risking their lives. Couples also face anxiety about being judged by society, nervousness about judging themselves, and silence among women who have undergone abortion procedures (11). It also inhibits access to post-abortion care (PAC) services, which is important in the reduction of maternal mortality caused by unwanted pregnancies (30). Neighboring countries like India have very high unsafe abortion rates even after having legalized abortion through the 1971 Medical Termination of Pregnancy Act (MTPA). A study published in 2019 showed an incidence of 67% unsafe abortions when abortion had been legalized for around 50 years (31). Moreover, evidence suggests that while abortion was responsible for only 8% of maternal deaths before 1972 in India, that proportion increased to 15%–30% after 1972 (32). This raises doubts about whether restrictive abortion laws cause more unsafe abortions, from the closest country for which we have such evidence. There is a need to broaden the availability of contraceptives, provide better training for providers, and include men in family planning programs (33).
The present study draws attention to the complex relationship between demographic, reproductive, and socioeconomic factors and induced abortion in Pakistan. Reproductive health education should be prioritized, and access to high-quality family planning services should be enhanced through targeted measures. Programs specifically designed to account for distinct sociocultural backgrounds can close gaps in contraceptive use efficacy.
It is crucial to remember that, due to legal limitations and the delicate nature of the subject, there is a dearth of information, and it is difficult to gather reliable data on the frequency and causal links of induced abortions, as many women choose to undergo the procedure in secret and under dangerous circumstances. This research can help close the information gaps and provide guidance for policies and interventions aimed at enhancing women's reproductive health outcomes. An extensive strategy is needed to devise and comprehend contextual elements to create culturally aware and efficacious interventions. In Pakistan, the Federal Ministry of National Health Services Regulations and Coordination, in collaboration with Ipas, has developed and endorsed national and provincial guidelines for the provision of post-abortion care (PAC) services. These guidelines aim to improve healthcare outcomes by ensuring that PAC procedures are carried out in a safe and medically sound manner (34, 35).
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Ethics statement
The studies involving humans were approved by Health Services Academy IRB Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SNK: Conceptualization, Data curation, Formal analysis, Methodology, Resources, Writing – original draft, Writing – review & editing. FM: Conceptualization, Data curation, Formal analysis, Methodology, Resources, Writing – original draft, Writing – review & editing. SB: Writing – review & editing. QU: Resources, Writing – review & editing. ET: Resources, Writing – review & editing. MTK: Writing – review & editing. AM: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bearak J, Popinchalk A, Ganatra B, Moller A-B, Tunçalp Ö, Beavin C, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990–2019. Lancet Glob Health. (2020) 8(9):e1152–61. doi: 10.1016/S2214-109X(20)30315-6
2. World Health Organization. Abortion: Key Facts. Geneva: World Health Organization (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/abortion (Accessed June 14, 2025).
3. Ganatra B, Gerdts C, Rossier C, Johnson BR, Tunçalp Ö, Assifi A, et al. Global, regional, and subregional classification of abortions by safety, 2010–14: estimates from a Bayesian hierarchical model. Lancet. (2017) 390(10110):2372–81. doi: 10.1016/S0140-6736(17)31794-4
4. National Institute of Population Studies (NIPS), ICF. Pakistan Demographic and Health Survey 2017–18. Islamabad: National Institute of Population Studies and ICF (2018). Available online at: https://dhsprogram.com/pubs/pdf/FR354/FR354.pdf (Accessed June 23, 2025).
5. Sathar Z, Singh S, Fikree FF. Induced abortions and unintended pregnancies in Pakistan. Stud Fam Plann. (2014) 45(4):471–91. doi: 10.1111/j.1728-4465.2014.00012.x
6. Junaidi I. 6.6 Pc women of reproductive age had abortion in 2023. Dawn News. Karachi: ICF (2024). Available online at: https://www.dawn.com (Accessed June 23, 2025).
7. Koch E, Aracena P, Gatica S, Bravo M, Huerta-Zepeda A, Calhoun BC. Fundamental discrepancies in abortion estimates and abortion-related mortality: a reevaluation of recent studies in Mexico with special reference to the international classification of diseases. Int J Womens Health. (2012) 4:613–23. doi: 10.2147/IJWH.S38063
8. National Institute of Population Studies (NIPS). Pakistan Maternal Mortality Survey 2019. Islamabad: National Institute of Population Studies (2019). Available online at: https://www.nips.org.pk (Accessed June 23, 2025).
9. Sharma AC, Hussain S, Mahmood T. Notes from the field: political norm change for abortion in Pakistan. Reprod Health Matters. (2019) 27(2):126–32. doi: 10.1080/09688080.2019.1616810
10. Husain U, Fatima S, Hussain S. Septic abortions: an outcome of criminal abortion. J Pak Med Assoc. (2022) 16(05):691. doi: 10.47391/JPMA.691
11. Lashari U. Abortion laws in Pakistan and around the world: a case study of Roe vs Wade. SSRN working paper. Rochester, NY: Social Science Research Network (2023). Available online at: https://ssrn.com/abstract=4488037 (Accessed June 14, 2025).
12. Hanschmidt F, Linde K, Hilbert A, Riedel Heller SG, Kersting A. Abortion stigma: a systematic review. Perspect Sex Reprod Health. (2016) 48(4):169–77. doi: 10.1363/48e8516
13. Aftab M, Khan A, Malik S. Partiality of the general population towards abortion and the awareness regarding it: a cross sectional study Pak J Med Health Sci. (2021) 15(9):2193–7. doi: 10.53350/pjmhs211592193
14. Huber-Krum S, Saeed A, Sami N. An application of the list experiment to estimate abortion prevalence in karachi, Pakistan. Stud Fam Plann. (2020) 46(Suppl 1):13–24. doi: 10.1111/sifp.12116
15. Sesay FR, Kamara SI, Kamara SM. Determinants of induced abortion among women of reproductive age: evidence from the 2013 and 2019 Sierra Leone demographic and health survey. BMC Womens Health. (2023) 23(1):44. doi: 10.1186/s12905-023-02195-5
16. Habib MA, Raynes Greenow C, Nausheen S, Soofi SB, Sajid M, Ahmed I, et al. Prevalence and determinants of unintended pregnancies amongst women attending antenatal clinics in Pakistan. BMC Pregnancy Childbirth. (2017) 17:156. doi: 10.1186/s12884-017-1339-z
17. Ajayi AI, Mudefi E, Yusuf MSV, Adeniyi OV. Prevalence and correlates of induced abortion: results of a facility-based cross-sectional survey of parturient women living with HIV in South Africa. BMC Publ Health. (2022) 19(1):220. doi: 10.1186/s12889-022-14650-3
18. Rahmadhani W, Mustofa DI, Setiawan KI, Lestari ME, Dewi AP, Noviryana E. Age factors that affect pregnant mothers ability to have an abortion. J Sex Reprod Health Sci. (2023) 2(1):84-92. doi: 10.26753/jsrhs.v2i1.710
19. Liu J, Wu S, Xu J, Temmerman M, Zhang W-H. A global systematic review and meta-analysis of prevalence of repeat induced abortion and correlated risk factors. Eur J Contracept Reprod Health Care. (2023) 63(5):321–33. doi: 10.1080/13625187.2023.2212278
20. Deliana D, Rahayu S. The correlation of parity and maternal age with the incidence of abortion. ALINEA: Health Sci Med Int J. (2024) 1(3):23–8. doi: 10.70743/alinea.v1i3.4
21. Giannandrea SA, Cerulli C, Anson E, Chaudron LH. Increased risk for postpartum psychiatric disorders among women with past pregnancy loss. J Womens Health. (2013) 22(9):760–8. doi: 10.1089/jwh.2012.4011
22. Cuenca D. Pregnancy loss: consequences for mental health. Front Glob Womens Health. (2023) 3:1032212. doi: 10.3389/fgwh.2022.1032212
23. Turesheva A, Ukybassova T, Aimagambetova G, Terzic M. Recurrent pregnancy loss etiology, risk factors, diagnosis, and management: fresh look into a full box. J Clin Med. (2023) 12(12):4074. doi: 10.3390/jcm12124074
24. Zhang W-H, Wu S, Temmerman M. Family planning needs and induced abortion in China: two cross-sectional studies. Eur J Public Health. (2016) 26(Suppl 1):ckw166. doi: 10.1093/eurpub/ckw166.003
25. Mohapatra V, Mohanty SK, Mishra PS. Family planning practices among women seeking induced abortion: an institution-based cross-sectional study from eastern India. J Family Med Prim Care. (2022) 11(10):6339–44. doi: 10.4103/jfmpc.jfmpc_448_22
26. Ayele M, Girma D, Hailu A. Magnitude and associated factors of unmet need for family planning among reproductive-aged women in Ethiopia: an umbrella review. PLoS One. (2024) 19(8):e0308085. doi: 10.1371/journal.pone.0308085
27. Ganatra B, Faundes A, Benagiano G. Role of birth spacing, family planning services, safe abortion services and post-abortion care in reducing maternal mortality. Best Pract Res Clin Obstet Gynaecol. (2016) 36:145–55. doi: 10.1016/j.bpobgyn.2016.07.003
28. Belachew TB, Asmamaw DB, Emiru TD. Emergency contraceptive knowledge and associated factors among abortion experienced reproductive age women in Ethiopia: a multilevel analysis using EDHS 2016 data. BMC Womens Health. (2023) 23(1):775. doi: 10.1186/s12905-023-02738-w
29. Supanji IMW, Putra IGNE. Relationship between maternal age, education, and parity in the incidence of spontaneous abortion in Bali. J Appl Sci Travel Health. (2022) 10(4):3091–5. Available at: https://journal.unhas.ac.id/index.php/jasth/article/view/24878. (Accessed June 14, 2025).
30. Iqbal H. Investing in the Sexual and Reproductive Health of Adolescents in Pakistan. New York: Guttmacher Institute (2021). Available onilne at: https://knowledgecommons.popcouncil.org/focus_sexual-health-repro-choice/133/ (Accessed June 23, 2025).
31. Baig M, Mubeen K. Determinants of inadequate provision and utilization of post abortion care services in Pakistan. J Asian Midwives. (2018) 5(1), 31-45. Available online at: https://ecommons.aku.edu/cgi/viewcontent.cgi?article=1059&context=jam
32. Yokoe R, Rowe R, Choudhury SS, Rani A, Zahir F, Nair M. Unsafe abortion and abortion-related death among 1.8 million women in India. BMJ Glob Health. (2019) 4(3):e001491. doi: 10.1136/bmjgh-2019-001491
33. World Health Organization. Complications of Abortion: Technical and Managerial Guidelines for Prevention and Treatment. Geneva: World Health Organization (1995). Available online at: https://iris.who.int/bitstream/handle/10665/40349/9241544694.pdf?sequence=1 (Accessed June 23, 2025).
34. Arshad A, Aziz H, Shabbir G, Shakya S, Munir Z. Improving safe post-abortion care practices: a study on interventions implemented by Ipas Pakistan. Front Public Health. (2023) 11:1004381. doi: 10.3389/fpubh.2023.1004381
35. Mulhern O, Niazi R, Parveen T, Singh S. Postabortion Care in Pakistan: 2023 Assessment of the Health System’s Capacity to Provide Care. New York: Guttmacher Institute (2024). Available online at: https://www.guttmacher.org/report/postabortion-care-in-pakistan-2023-assessment-of-capacity (Accessed June 23, 2025).
Keywords: abortions, maternal health, PMMS 2019, risk factors, pregnancy loss
Citation: Khalid SN, Midhet F, Uzma Q, Thom EM, Baqai S, Khan MT and Memon A (2025) Factors associated with induced abortions in Pakistan: a comprehensive analysis of Pakistan maternal mortality survey 2019. Front. Reprod. Health 7:1536582. doi: 10.3389/frph.2025.1536582
Received: 29 November 2024; Accepted: 9 June 2025;
Published: 10 July 2025.
Edited by:
Sule Yildiz, Koç University School of Medicine, TürkiyeReviewed by:
Azna Zuberi, Northwestern University, United StatesCalum Miller, University of Oxford, United Kingdom
Copyright: © 2025 Khalid, Midhet, Uzma, Thom, Baqai, Khan and Memon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Samina Naeem Khalid, ZHJzYW1pbmFAaHNhLmVkdS5waw==