 Rosanna Squitti
Rosanna Squitti Carlo Salustri2
Carlo Salustri2 Mariacristina Siotto
Mariacristina Siotto- 1Molecular Markers Laboratory, IRCCS Istituto Centro San Giovanni di Dio—Fatebenefratelli, Brescia, Italy
- 2Institute of Cognitive Sciences and Technologies (CNR), Rome, Italy
- 3Department of Laboratory Medicine, Research and Development Division, San Giovanni Calibita—Fatebenefratelli Hospital, Rome, Italy
- 4Don Carlo Gnocchi ONLUS Foundation, Milan, Italy
A commentary on
Drew’s paper (1) contains a helpful overview of the numerous works published on the interaction between copper and beta-amyloid (Aβ) in Alzheimer’s disease (AD). However, his linking of the usefulness of therapeutic copper chelation in AD primarily to copper–Aβ coordination chemistry appears to us to be limited. First, Aβ’s “causative” role is challenged by various types of evidence; second, one must consider that AD is a complex disease, contributing to the development of many risk factors.
While still trusting pathogenesis theories, such as the “amyloid cascade” (2), or the “metal hypothesis” (3), and more recent ones proposing a loss of Aβ’s capability to properly handle copper (4–6), one should not overlook the literature on the relationship between AD stages and copper concentrations in serum, plasma, cerebrospinal fluid, and the brain. Many studies have investigated whether a significant difference in copper levels exists between AD patients and healthy individuals, and whether those levels correlate with the patient clinical picture.
Drew notes the controversies surrounding the conclusions of these studies. Nevertheless, a number of meta-analyses published in the last 5 years undoubtedly show that the copper levels are lower in AD brains than in healthy ones [see, e.g., the comparison of 115 AD patients with 123 healthy controls by Ref. (7)], while the copper levels are higher in AD patients’ serum [see, e.g., Wang et al.’s comparison of 1,768 AD patients with 2,514 healthy controls (8)]. Subsequent studies have shown the similar results. Three studies confirmed lower levels of copper in the brain (9–11). Considering general circulation studies, two studies reported no overall differences in outcomes, while five studies show higher levels of copper in AD patients vs. controls (Table 1). Moreover, a recent meta-analysis (12) comparing 879 AD patients with 1712 controls has shown that the plasma copper component that circulates not bound to ceruloplasmin (non-Cp copper) is increased in AD, as confirmed by studies published after this publication (13, 14).
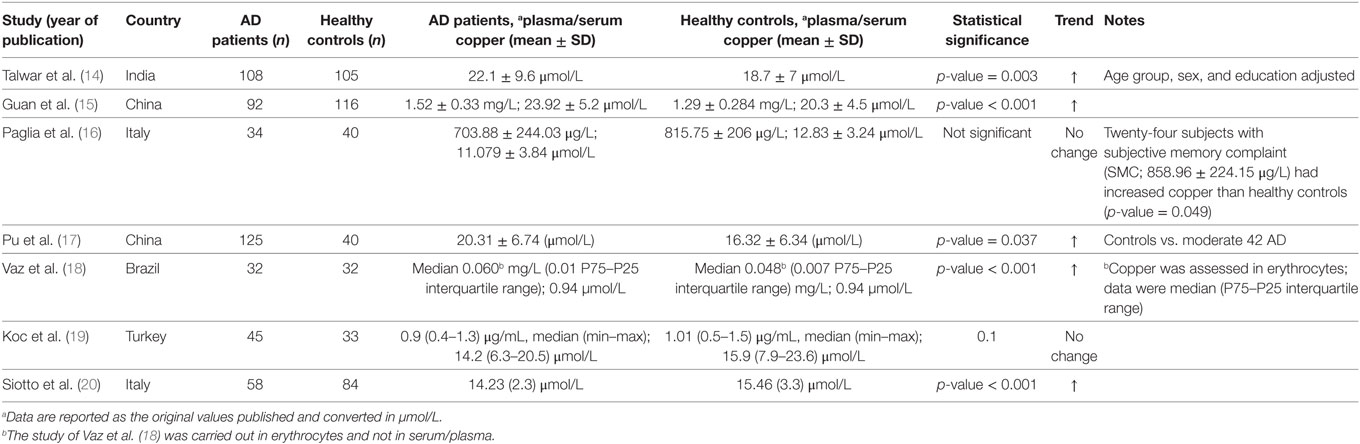
Table 1. Studies on copper in Alzheimer’s disease (AD) patients and healthy controls [published after the meta-analysis published in 2015 (8)].
Thus, AD appears as characterized by an aberrant copper homeostasis: higher non-Cp copper levels in the blood stream and lower levels in the brain, exactly like in Wilson disease (WD) (21), although at a much milder level. In fact, James and coworkers (22) demonstrated that in the brain areas strongly damaged by AD, lower levels of total copper coexist with higher levels of copper not bound to proteins (non-Cp copper in the brain), as it occurs in WD. Furthermore, lower values of serum ceruloplasmin specific activity coexist with higher levels of non-Cp copper (20). In summary, a mild degree of failure of copper control appears to occur in AD.
Recently, some genetic studies [reported in Ref. (23)] have contributed to our understanding by demonstrating that the presence of ATP7B (WD) gene’s variants increases (from 1.63 to 5.16 odds ratio) the risk of developing AD. The gene’s variant K832R has been the object of a recent in-vivo study demonstrating that this AD-related ATP7B variant is a loss-of-function allele in Drosophila (24). Further genetic studies are in progress to verify whether AD patients with higher non-Cp copper levels are also carriers of multiple rare ATP7B gene mutations. However, should that be the case, copper toxicosis could be possibly prevented/treated with chelating or anti-copper agents, as in WD.
Moreover, Brewer has drawn attention on possible beneficial effects of more tolerable zinc-based therapies. He (25) describes post-hoc results presented by Dr. Diana Pollack at various meetings, showing zinc therapy as capable of stopping cognitive decline: by restricting Pollack’s post-hoc analysis to those among her patients who were aged 70 years or older (14 zinc treated and 15 placebo treated), Brewer showed that the latter scored significantly better in the Alzheimer’s Disease Assessment Scale cognitive subscale, Clinical Dementia Rating Scale Sum of Boxes, and Mini–Mental State Examination than placebo patients.
In 2002, our laboratory attempted a study on the effects of d-penicillamine (d-pen) in AD (26). Penicillamine is known to promote “de-coppering” in WD by forming copper–penicillamine complexes, which are then excreted with the urine. In our study, 77.8% of the AD patients under d-pen treatment showed a 24-h urinary excretion higher than 200 μg/day, which is 5× the value (40 μg/day) which is widely accepted as representative of a “normal” copper excretion (27). A 5 μg/day × 40 μg/day excretion is considered the “d-pen challenge test” cutoff, supportive of WD diagnosis in asymptomatic patients (28). The d-pen test, however, is not disease-specific. Individuals suffering from hepatic cirrhosis, for example, also show excretion values higher than the mentioned cutoff. In AD patients under d-pen treatment (26), this is suggestive of failure a copper control.
Unfortunately, when excretion reaches levels that make the copper balance negative, some patients treated with WD under d-pen treatment show a serious “iatrogenic” deterioration (often referred to as “paradoxical effect”), with an increase of the neurological symptoms. This effect is believed to be caused by a frantic mobilization and redistribution of copper which results in high copper level in the brain and in the blood (29, 30). Manifestation of similar neurological symptoms in our study on AD forced an early interruption (26). This is suggestive, however, of copper homeostasis abnormalities, as some authors commented (31). Nevertheless, up to that point, d-pen had shown a positive effect in reducing oxidative stress.
In conclusion, we agree with Drew that the metal–Aβ1–xinteractions can be downstream of an underlying pathology of AD. However, we deem this not to be a valid reason for abandoning therapeutic chelation of copper ions in AD that has not been yet thoroughly tested. In our opinion, anti-copper therapies appear to have excellent chances to affect positively the condition for a percentage of AD patients, in agreement with the notion of the existence of different AD “sub-types” (32–35).
Author Contributions
RS, CS, MR, and MS contributed to the concepts expressed in the commentary. All authors contributed to the conceptualization of the manuscript, its realization, and writing. In particular, MS evaluated the chemical coordination part of the Drew’s manuscript and the clinical chemistry part of our commentary. RS reviewed the meta-analysis section, and MR and CS reviewed the genetic part. CS revised English editing.
Conflict of Interest Statement
RS reports personal fees in the past 3 years and other interests from Canox4drug SPA (Italy), and IGEA Research Corporation (Miami, FL, USA) outside the submitted work. Other authors have no conflict of interest to declare.
Funding
RS was supported by Italian Ministry of Health, Ricerca Corrente.
References
1. Drew SC. The case for abandoning therapeutic chelation of copper ions in Alzheimer’s disease. Front Neurosci (2017) 11:317. doi:10.3389/fnins.2017.00317
2. Hardy JA, Higgins GA. Alzheimer’s disease: the amyloid cascade hypothesis. Science (1992) 256(5054):184–5. doi:10.1126/science.1566067
3. Bush AI, Tanzi RE. Therapeutics for Alzheimer’s disease based on the metal hypothesis. Neurotherapeutics (2008) 5(3):421–32. doi:10.1016/j.nurt.2008.05.001
4. Lee HG, Castellani RJ, Zhu X, Perry G, Smith MA. Amyloid-β in Alzheimer’s disease: the horse or the cart? Pathogenic or protective? Int J Exp Pathol (2005) 86(3):133–8. doi:10.1111/j.0959-9673.2005.00429.x
5. Cavaleri F. Paradigm shift redefining molecular, metabolic and structural events in Alzheimer’s disease involves a proposed contribution by transition metals. Defined lengthy preclinical stage provides new hope to circumvent advancement of disease- and age-related neurodegeneration. Med Hypotheses (2015) 84(5):460–9. doi:10.1016/j.mehy.2015.01.044
6. Kepp KP. Alzheimer’s disease: how metal ions define β-amyloid function. Coord Chem Rev (2017). doi:10.1016/j.ccr.2017.05.007
7. Schrag M, Mueller C, Oyoyo U, Smith MA, Kirsch WM. Iron, zinc and copper in the Alzheimer’s disease brain: a quantitative meta-analysis. Some insight on the influence of citation bias on scientific opinion. Prog Neurobiol (2011) 94(3):296–306. doi:10.1016/j.pneurobio.2011.05.001
8. Wang ZX, Tan L, Wang HF, Ma J, Liu J, Tan MS, et al. Serum iron, zinc, and copper levels in patients with Alzheimer’s disease: a replication study and meta-analyses. J Alzheimers Dis (2015) 47(3):565–81. doi:10.3233/JAD-143108
9. House E, Esiri M, Forster G, Ince PG, Exley C. Aluminium, iron and copper in human brain tissues donated to the medical research council’s cognitive function and ageing study. Metallomics (2012) 4(1):56–65. doi:10.1039/c1mt00139f
10. Graham SF, Nasaruddin MB, Carey M, Holscher C, McGuinness B, Kehoe PG, et al. Age-associated changes of brain copper, iron, and zinc in Alzheimer’s disease and dementia with Lewy bodies. J Alzheimers Dis (2014) 42(4):1407–13. doi:10.3233/JAD-140684
11. Szabo ST, Harry GJ, Hayden KM, Szabo DT, Birnbaum L. Comparison of metal levels between postmortem brain and ventricular fluid in Alzheimer’s disease and nondemented elderly controls. Toxicol Sci (2016) 150(2):292–300. doi:10.1093/toxsci/kfv325
12. Squitti R, Simonelli I, Ventriglia M, Siotto M, Pasqualetti P, Rembach A, et al. Meta-analysis of serum non-ceruloplasmin copper in Alzheimer’s disease. J Alzheimers Dis (2014) 38(4):809–22. doi:10.3233/JAD-131247
13. Squitti R, Siotto M, Cassetta E, El Idrissi IG, Colabufo NA. Measurements of serum non-ceruloplasmin copper by a direct fluorescent method specific to Cu(II). Clin Chem Lab Med (2017) 55(9):1360–7. doi:10.1515/cclm-2016-0843
14. Talwar P, Grover S, Sinha J, Chandna P, Agarwal R, Kushwaha S, et al. Multifactorial analysis of a biomarker pool for Alzheimer disease risk in a North Indian population. Dement Geriatr Cogn Disord (2017) 44(1–2):25–34. doi:10.1159/000477206
15. Guan C, Dang R, Cui Y, Liu L, Chen X, Wang X, et al. Characterization of plasma metal profiles in Alzheimer’s disease using multivariate statistical analysis. PLoS One (2017) 12(7):e0178271. doi:10.1371/journal.pone.0178271
16. Paglia G, Miedico O, Cristofano A, Vitale M, Angiolillo A, Chiaravalle AE, et al. Distinctive pattern of serum elements during the progression of Alzheimer’s disease. Sci Rep (2016) 6:22769. doi:10.1038/srep22769
17. Pu Z, Xu W, Lin Y, He J, Huang M. Oxidative stress markers and metal ions are correlated with cognitive function in Alzheimer’s disease. Am J Alzheimers Dis Other Demen (2017) 32(6):353–9. doi:10.1177/1533317517709549
18. Vaz FNC, Fermino BL, Haskel MVL, Wouk J, de Freitas GBL, Fabbri R, et al. The relationship between copper, iron, and selenium levels and Alzheimer disease. Biol Trace Elem Res (2017). doi:10.1007/s12011-017-1042-y
19. Koc ER, Ilhan A, Zubeyde A, Acar B, Gurler M, Altuntas A, et al. A comparison of hair and serum trace elements in patients with Alzheimer disease and healthy participants. Turk J Med Sci (2015) 45(5):1034–9. doi:10.3906/sag-1407-67
20. Siotto M, Simonelli I, Pasqualetti P, Mariani S, Caprara D, Bucossi S, et al. Association between serum ceruloplasmin specific activity and risk of Alzheimer’s disease. J Alzheimers Dis (2016) 50(4):1181–9. doi:10.3233/JAD-150611
21. Fujiwara N, Iso H, Kitanaka N, Kitanaka J, Eguchi H, Ookawara T, et al. Effects of copper metabolism on neurological functions in Wistar and Wilson’s disease model rats. Biochem Biophys Res Commun (2006) 349(3):1079–86. doi:10.1016/j.bbrc.2006.08.139
22. James SA, Volitakis I, Adlard PA, Duce JA, Masters CL, Cherny RA, et al. Elevated labile Cu is associated with oxidative pathology in Alzheimer disease. Free Radic Biol Med (2012) 52(2):298–302. doi:10.1016/j.freeradbiomed.2011.10.446
23. Squitti R, Siotto M, Arciello M, Rossi L. Non-ceruloplasmin bound copper and ATP7B gene variants in Alzheimer’s disease. Metallomics (2016) 8(9):863–73. doi:10.1039/c6mt00101g
24. Mercer SW, Wang J, Burke R. In vivo modeling of the pathogenic effect of copper transporter mutations that cause Menkes and Wilson diseases, motor neuropathy, and susceptibility to Alzheimer’s disease. J Biol Chem (2017) 292(10):4113–22. doi:10.1074/jbc.M116.756163
25. Brewer GJ. Copper excess, zinc deficiency, and cognition loss in Alzheimer’s disease. Biofactors (2012) 38(2):107–13. doi:10.1002/biof.1005
26. Squitti R, Rossini PM, Cassetta E, Moffa F, Pasqualetti P, Cortesi M, et al. D-penicillamine reduces serum oxidative stress in Alzheimer’s disease patients. Eur J Clin Invest (2002) 32(1):51–9. doi:10.1046/j.1365-2362.2002.00933.x
27. Roberts EA, Schilsky ML; American Association for Study of Liver Diseases (AASLD). Diagnosis and treatment of Wilson disease: an update. Hepatology (2008) 47(6):2089–111. doi:10.1002/hep.22261
28. Nicastro E, Ranucci G, Vajro P, Vegnente A, Iorio R. Re-evaluation of the diagnostic criteria for Wilson disease in children with mild liver disease. Hepatology (2010) 52(6):1948–56. doi:10.1002/hep.23910
30. Bandmann O, Weiss KH, Kaler SG. Wilson’s disease and other neurological copper disorders. Lancet Neurol (2015) 14(1):103–13. doi:10.1016/S1474-4422(14)70190-5
31. Hoogenraad TU. Paradigm shift in treatment of Alzheimer’s disease: zinc therapy now a conscientious choice for care of individual patients. Int J Alzheimers Dis (2011) 2011:492686. doi:10.4061/2011/492686
32. Amtage F, Birnbaum D, Reinhard T, Niesen WD, Weiller C, Mader I, et al. Estrogen intake and copper depositions: implications for Alzheimer’s disease? Case Rep Neurol (2014) 6(2):181–7. doi:10.1159/000363688
33. Tecchio F, Vecchio F, Ventriglia M, Porcaro C, Miraglia F, Siotto M, et al. Non-ceruloplasmin copper distinguishes a distinct subtype of Alzheimer’s disease: a study of EEG-derived brain activity. Curr Alzheimer Res (2016) 13(12):1374–84. doi:10.2174/1567205013666160603001131
34. Squitti R, Simonelli I, Cassetta E, Lupoi D, Rongioletti M, Ventriglia M, et al. Patients with increased non-ceruloplasmin copper appear a distinct sub-group of Alzheimer’s disease: a neuroimaging study. Curr Alzheimer Res (2017). doi:10.2174/1567205014666170623125156
Keywords: copper, Alzheimer’s disease, beta-amyloid peptide, chelation therapy, metals
Citation: Squitti R, Salustri C, Rongioletti M and Siotto M (2017) Commentary: The Case for Abandoning Therapeutic Chelation of Copper Ions in Alzheimer’s Disease. Front. Neurol. 8:503. doi: 10.3389/fneur.2017.00503
Received: 27 June 2017; Accepted: 08 September 2017;
Published: 25 September 2017
Edited by:
Stefano L. Sensi, Università degli Studi “G. d’Annunzio” Chieti—Pescara, ItalyReviewed by:
Gianfranco Spalletta, Fondazione Santa Lucia (IRCCS), ItalyPaul Anthony Adlard, Florey Institute of Neuroscience and Mental Health, Australia
Copyright: © 2017 Squitti, Salustri, Rongioletti and Siotto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosanna Squitti, cm9zYW5uYS5zcXVpdHRpQGFmYXIuaXQ=