 René Castien
René Castien Willem De Hertogh
Willem De Hertogh- 1Department of General Practice and Elderly Care Medicine, EMGO Institute for Health and Care Research, VU University Medical Center, Amsterdam, Netherlands
- 2Amsterdam Movement Sciences, Faculty of Behavioral and Movement Sciences, Vrije Universiteit, Amsterdam, Netherlands
- 3Department of Rehabilitation Sciences and Physiotherapy, Faculty of Medicine and Health Sciences, University of Antwerp, Antwerpen, Belgium
The most prevalent primary headaches tension-type headache and migraine are frequently associated with neck pain. A wide variety of treatment options is available for people with headache and neck pain. Some of these interventions are recommended in guidelines on headache: self-management strategies, pharmacological and non-pharmacological interventions. Physical treatment is a frequently applied treatment for headache. Although this treatment for headache is predominantly targeted on the cervical spine, the neurophysiological background of this intervention remains unclear. Recent knowledge from neuroscience will enhance clinical reasoning in physical treatment of headache. Therefore, we summarize the neuro- anatomical and—physiological findings on headache and neck pain from experimental research in both animals and humans. Several neurophysiological models (referred pain, central sensitization) are proposed to understand the co-occurrence of headache and neck pain. This information can be of added value in understanding the use of physical treatment as a treatment option for patients with headache and neck pain.
Introduction
Headache causes substantial pain and disability in people's daily life and delivers a high burden and cost to society that is estimated only in Europe at 173 billion Euro per year (1). The most prevalent primary headaches worldwide are tension-type headache (TTH) and migraine. These types of headache are frequently associated with neck pain (2, 3). A recent open population study reported a 1-year prevalence of neck pain of 68.4% and more in people with primary headache compared to people without primary headache (85.7 vs. 56.7%; OR 3.0, 95% CI 2.0–4.4). After adjusting for age, gender, education and poor self-rated health, the prevalence of neck pain (56.7%) was still significantly higher in people with only migraine (76.2%), migraine ánd TTH (89.3%), and only TTH (88.4%) in comparison with people without headaches (4). People with headache and neck pain frequently visit health care providers such as medical doctors (general practitioners, neurologists) and physical therapists in their quest for diagnosis and treatment (5). A broad pallet of treatment options is available, including reassurance, self-management strategies, pharmacological, and non-pharmacological treatments. Evidence for the effectiveness of physical therapy for headache is limited (6, 7). Despite this lack of solid scientific back-up, physical therapy is worldwide a frequently used alternative or complementary treatment and included in several clinical guidelines as an alternative treatment option (The European Federation of Neurological Societies (EFNS) guideline, Italian guideline for primary headaches) (5, 8, 9). In daily practice, a combination of treatment options is often used, and the combination of pharmacological (acute and prophylactic drugs) and non-pharmacological (education, physical therapies, exercises, biofeedback) interventions is indeed considered to be an efficient approach in headache disorders (10). Additional research concerning non-pharmacological prophylactic treatment strategies of headache is however urgently needed (11). For disciplines that target the cervical spine in order to decrease headache, it is pivotal for clinical reasoning to understand the neuro-physiological background of headache and neck pain (12). Recently, new insights have emerged on the relation between extracranial input from the (upper) cervical spine and headache from experimental research in both animals and humans (13). This recent information can be of great value to understand and to (re)design physical approaches for different types of headache in combination with neck pain. In this review we first describe the neuro-anatomical and neuro-physiological findings from experimental studies on the trigemino-cervical complex (TCC). We then discuss neurophysiological models to explain the co-occurrence of headache and neck pain such as referred pain and generalized hyperexcitability. We further present the relation of cervical spine dysfunction and headache and research on modulation of nociception at the TCC. Finally, we describe physical treatment as an option to treat headache and neck pain.
Trigemino-cervical Complex, the Anatomical Basis
Experimental research has contributed to further neuro-physiological insights in the relation of headache and neck pain. Knowledge of the neuro-anatomical structures and neural activity within the TCC seems paramount. The frequent co-occurrence of headache and neck pain is attributed to common nociceptive innervation of the head and neck in the dorsal horn C1-2, located in the trigemino-cervical complex. Animal (14, 15) and human (15) anatomical studies have shown that the TCC extends from the medulla (pars oralis and pars interpolaris) to the first and second cervical segments (pars caudalis) (Figure 1). In the TCC, the pars caudalis receive first order nociceptive Aδ- and C afferent neurons of the ophthalmic nerve together with first order Aδ- and C nociceptive afferent neurons from predominantly the dorsal root C2. These afferent neurons are directly or indirectly connected via wide dynamic range neurons to second-order neurons (16). The ophthalmic nerve delivers nociceptive input via small diameter Aδ- and C afferent nerve fibers to nociceptive second-order neurons in the superficial and deep layers of the medullary dorsal horn C1 and 2 in the TCC (17, 18). The upper cervical root C2 represents Aδ- and C nociceptive afferent information of vessels and dura mater of the posterior fossa, and myofascial structures of the upper cervical segments. This nociceptive input from the upper cervical nerve root C2 is well-documented and has a structural overlap with nociceptive nerve endings from the ophthalmic nerve root at the first and second cervical dorsal horn in the TCC (19–27). An extracranial origin of meningeal nociception is suggested by Schueler et al. by demonstrating in vitro that collaterals of trigeminal afferents form functional connections between intra- and extracranial tissues in rats and humans. So, information from pericranial muscles can reach the dura mater by ortho- and antidromic conduction through axon collaterals and possibly influence meningeal functions and the generation of headache in humans (28, 29). This finding on collateral afferent connections matches with the anatomical (30) and functional relation (31) of the dura and suboccipital muscles in the upper cervical region in humans. Therefore, the neuro-anatomical connection of ophthalmic and cervical nociceptive afferents on second order neurons at the pars caudalis of the TCC, is pivotal to understand the occurrence of headache and neck pain.
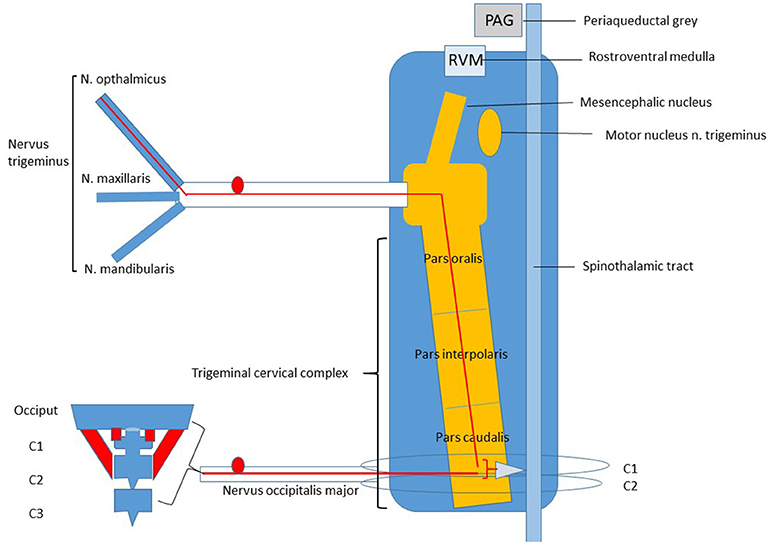
Figure 1. Trigeminal Cervical Complex (TCC).
Referred Pain
The convergence of cervical ánd trigeminal nociceptive small diameter Aδ- and C fibers on the C1 and C2 dorsal horn provides a neuro-anatomical basis for the clinical phenomenon of referred pain. The co-occurrence of headache and neck pain can be explained by referred pain: pain originating from the neck is perceived as originating from the head and vice versa.
Evidence From Animal Studies
Animal-experimental neuro-physiological studies recording input of nociceptive afferent fibers at the C1-2 dorsal horn in animals contributed to the understanding of referred pain in both directions, i.e., from the neck to the head (20) and from the head to the neck (21). Vernon et al. described the increased activity in C1/C2 dorsal horns in rats after injection of inflammatory mustard oil in deep paraspinal tissues at the level of the left C1-C2 joint. Activation of trigeminal afferents of the supratentorial dura mater by mustard oil (MO) showed an enlargement of cervical cutaneous mechanoreceptive fields together with a significant (p < 0.001) increase in the excitability to electrical stimulation of the greater occipital nerve in C-fiber responses (21). Unilateral electric stimulation of the greater occipital nerve in cats increased metabolic activity in the dorsal horn C1 and C2. Stimulation of trigeminally-innervated structures showed a similar distribution to the trigeminal nucleus caudalis (32). Based on these findings, the well-recognized clinical phenomenon of head pain that is perceived frontal and occipital and in the upper neck may be the result of overlap of nociceptive information at the level of second order neurons.
Headache during a migraine attack seems to be primarily based on activation of the trigeminovascular pathways by increased visceral nociceptive Aδ- and C fibers input of the dura and intracranial vessels on the TCC. This input is frequently restricted to the territory of the ophthalmic nerve, but may extend as pain to the occipital region of the head which is innervated by the greater occipital nerve C2 (33). These results indicate that headache as well as neck pain can be perceived as referred pain.
Evidence From Human Studies
Clinical evidence of referred pain based on convergence of cervical- and ophthalmic nociceptive Aδ- and C afferent input originating from different structures has been observed in human studies. Clinical observations have shown that intracranial nociceptive input of arteries, but also extracranial nociceptive input originating from the vertebral artery is able to provoke painful sensations in the area of the forehead (34, 35). Provocation of headache by applying experimental nociceptive stimuli to upper cervical structures has been reported in several studies. Injection of saline in the neck and suboccipital region (36), sterile water (37) and low-frequency nerve stimulation (38) over the upper cervical dorsal roots have shown to provoke headache. In a narrative review on the diagnosis and treatment of cervicogenic headache, Bogduk has described several experimental studies on humans reporting referred pain patterns on the head caused by stimulation of nociceptive afferent input from myofascial structures of the upper cervical spine (39). In 23 out of 32 patients with cervicogenic headache the pain in the head was relieved completely after a diagnostic anesthetic block at the lateral atlanto-axial joints (C1-2) (40). Mechanical nociceptive afferent stimuli -by giving a firm pressure to myofascial structures of upper cervical segments (C0-3)- also provoke the patient's typical headache in patients with cervicogenic headache (41), TTH, and migraine (42, 43). Extensive research is available on trigger points in cervical and suboccipital muscles eliciting headache (44). In summary, convergence of cervical and trigeminal nociceptive afferents on second order neurons at the TCC can cause headache as referred pain via stimulation of cervical nociceptive input of the upper cervical segments by administration of fluid-irritants or mechanical pressure.
Generalized Hyperexcitability
Hyperexcitability of second order neurons in the TCC as a result of a continuous increased peripheral somatic and vascular nociceptive activity (45–48), a decrease of supraspinal inhibition (49) or a combination of both mechanisms can cause headache (50, 51). Activation of the trigeminovascular pathways increased by vascular nociceptive Aδ- and C fibers input of the dura and intracranial vessels on the TCC seems to be typical for migraine (47). Still, at present there is an ongoing debate what is causing the hyperexcitability of second order neurons in the TCC during migraine. Levy et al noticed that sensory innervation of the cranial meninges and immune and vascular cells may have a major role, but evidence for neurogenic inflammation during migraine and its contribution to meningeal nociception is limited (52). Prolonged or ongoing peripheral nociceptive input via trigger points in pericranial or cervical myofascial structures may contribute to hyperexcitability of second-order neurons at the C1 and C2 dorsal horn of the TCC in TTH, but evidence for this hypothesis is limited (53). Hyperexcitability of nociceptive second order neurons in the dorsal horn of C1-2 can also be caused by a decrease of endogeneous driven supraspinal descending inhibition of the periaqueductal gray (PAG), nucleus raphe magnus, or rostroventral medulla. This can lead to clinical signs such as hypersensitivity, allodynia and reduced pain thresholds in the cranio-cervical region and even in extra- cephalic regions. In patients with chronic TTH, but not with episodic TTH, most studies report lower pressure, thermal and electrical pain thresholds in the cephalic region (54). In patients with migraine pain threshold to pressure, cold and heat stimuli in the cephalic region are found to be lower during the ictal phase than during the interictal phase of migraine or healthy controls (55). For pain pressure thresholds in the cranio-cervical region a significant decrease is described in research on patients with migraine and CTTH compared to healthy controls (56). The interaction between supraspinal descending inhibitory systems and peripheral nociceptive input in the TCC seems to be a prerequisite for the characteristics as well as in the development of episodic to chronic headache syndromes (57). Thus, trigger points or tender, painful myofascial structures at the upper cervical segments in headache patients can either emerge or be a source of hyperexcitability of second-order neurons C1-C2.
Cervical Musculoskeletal Dysfunctions in Headache
Cervical musculoskeletal dysfunctions of joints and muscles have been observed in patients with migraine, TTH and cervicogenic headache (58–62). In the context of the neurophysiological interconnection between the dorsal root of C2 (greater occipital nerve) and the TCC, it may be not surprising that in participants with headache most cervical musculoskeletal dysfunctions are present in the upper cervical spine. Palpation of trigger points in suboccipital muscles and trapezius (63–66), restricted motion of the cervical segments C0-3 (43, 67), and stress on joints in the upper cervical spine (41, 42) are related to different types of headache. Although there seems to be a relation between (upper) cervical musculoskeletal dysfunctions and headache, these are documented in studies with a case–control design. Thus, no causal relation can be determined, nor solid conclusions can be drawn on this relation.
Modulation of Nociception at the TCC: Evidence From Animal Studies
Evidence is emerging that addressing the cervical spine can modulate pain at the TCC. Nöbel et al. reported that injection of a nociceptive stimulant (α,β-meATP) into the temporal muscle in rats induces ongoing activity of spinal trigeminal neurons with meningeal receptive fields. In the same study local anesthesia of single neck muscles, but not of the musculus temporalis, shows a significant decrease of the provoked central trigeminal activity (68). This supports the modulation of pain in the TCC by reduction of peripheral cervical muscular nociceptive afferent input. Supraspinal diffuse noxious inhibitory control (DNIC) on convergent neurons in the trigeminal nucleus caudalis in rats can be initiated by activation of Aδ- and C fibers. Villaneuva et al. and Bouhassira et al. demonstrated that induced activity of convergent neurons in the trigeminal nucleus caudalis was decreased up to 80% by activation of Aδ- and C fibers (69, 70). Afferent Aδ- and C input originating from the neck is not restricted to the TCC. Local administration of nerve growth factor into semispinal neck muscles in anesthetized mice shows not only stronger Fos immunoreactivity in the superficial layers I and II of the of cervical spinal dorsal horns C1, C2, and C3, but also in supraspinal structures such as the PAG and the medullary lateral reticular nucleus (71–76). Nearly 50% of all ventro-lateral PAG-projecting spinal neurons were found in the upper cervical segments and these segments are thereby potentially an important source to activate the ventrolateral PAG (71, 77). Activation of the ventrolateral PAG by deep somatic (deep neck muscles) and visceral pain not only leads to a resting state, but also to inhibition of trigeminal afferents (76, 78). The participation of this phenomenon in inhibition of trigeminal afferents is proposed (79, 80).
Modulation of Nociception at the TCC: Evidence From Human Studies
In a clinical study, Busch et al established modulation of nociception at the TCC by detecting a decrease of R2 response areas (AUC) and significantly increased R2 latencies of the nociceptive blink reflex only at the side of an anesthetic unilateral nerve blockade of the greater occipital nerve with prilocaine in healthy persons. These findings not only confirmed previous results related to anatomical and functional convergence of trigeminal and cervical afferent pathways, but also suggested that modulation hereof could be beneficial in treatment of primary headache disorders (81). In patients with headache, blocking afferent nociceptive input by anesthesia of the GON (82, 83) or in the facet joint C1-2 (40, 84) has proven to be effective in reducing headache. Piovesan et al. described the decrease of headache in a patient with migraine after light massage of the greater occipital nerve (85). Another clinical study by Watson and Drummond (42) reported the provocation as well as the resolution of headache in migraine patients with sustained manual pressure in the suboccipital region. The referred pain during the provocation test was decreased in parallel with a change in the trigeminal nociceptive blink reflex. This finding supposes the previously proposed model that stimulation of myofascial Aδ- and C fibers by manual pressure can activate the supraspinal DNIC system that acts specifically on spinal wide-dynamic-range (WDR) neurons and is able to modulate nociception at the TCC (69, 86).
Physical Treatment of Headache and Neck Pain
The neuro-anatomical and—physiological relation between brainstem nuclei, the (upper) neck and trigeminal nerve has to be incorporated in development of physical treatment for headache targeted at the cervical spine, especially the upper cervical region. According to the ‘gate-control' hypothesis, the relative high amount of proprioceptive afferent muscular input of upper cervical segments (87) to the central nervous system may alter nociceptive Aδ- and C fibers afferent input. Stimulation of proprioceptive input by active exercises for neck muscles may decrease the excitability of second order neurons at the TCC (11) and activation of the supraspinal DNIC system by stimulation of myofascial Aδ- and C fibers by manual pressure techniques at the upper cervical spine can be of added value (42). The importance of an active treatment of neck muscles is supported by the findings of a systematic review of Varatharajan et al. stating that an active physical treatment including exercises shows promising results on reduction of headache associated with neck pain (7).
Discussion
In the last decades experimental research in both animals and humans on neuro-anatomy and neuro-physiology has contributed to understand the co-occurrence of headache and neck pain. Based on this information we further present a neuro-physiological background for physical treatment of headache and neck pain. Studies have gain new insights on the neuro-anatomical and neuro-physiological relation between headache and neck pain, but also raise questions if and how this relation can be influenced by physical treatment. Headache (migraine, tension-type headache, cervicogenic headache), neck pain, and cervical musculoskeletal dysfunctions seem to be related in case-control studies, although the strength, significance and explanation of this relation varies per type of headache.
Clinicians have to consider, by sound clinical reasoning, whether cervical musculoskeletal dysfunctions are related to the patient's headache and which neurophysiological mechanisms could be involved. Therefore, we support the recommendation to classify headache according to the ICHD III criteria and to determine cervical musculoskeletal dysfunctions in patients with migraine, tension-type headache and cervicogenic headache (88). Additionally, tests on pain sensitivity can be included to understand the underlying pathophysiological mechanism. In their clinical judgement, clinicians have to consider all collected patient data: headache symptoms and neck pain, related cervical musculoskeletal dysfunction, tests on pain sensitivity in the cervico-cephalic and extra-cervico-cephalic regions (pressure pain thresholds) and reproduction of headache by pressure or stretch on musculoskeletal structures (43). To understand underlying neurophysiological mechanisms (local nociceptive provocation, referred pain, generalized hyperexcitability) remains challenging, but is necessary to identify patients who may benefit of treatment of the neck (89). The presented neurophysiological knowledge in this paper can be helpful to guide clinicians in this clinical reasoning process.
It is a great challenge for clinicians and researchers to develop effective treatment strategies for headache targeted on modulation of cervical afferent input in order to decrease the excitability of first- to second order neurons at the level of the TCC. Experimental studies of the neurophysiological effect of physical treatment and randomized clinical trial on this topic are scarce and urgently warranted. Meanwhile, there is no standard recipe for physical treatment on the neck for different types of headache. But clinicians may be encouraged by recent evidence and new insights on headache and neck pain and may use this knowledge in clinical reasoning to provide a tailored and evidence based neuro-physiological approach for patients with headache and neck pain.
Author Contributions
RC and WD: concept development and writing of the manuscript; Both authors approved the final version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Linde M, Gustavsson A, Stovner LJ, Steiner TJ, Barré J, Katsarava Z, et al. The cost of headache disorders in Europe: the eurolight project. Eur J Neurol. (2012) 19:703–11. doi: 10.1111/j.1468-1331.2011.03612.x
2. Landgraf MN, von Kries R, Heinen F, Langhagen T, Straube A, Albers L. Self-reported neck and shoulder pain in adolescents is associated with episodic and chronic migraine. Cephalalgia. (2016) 36:807–11. doi: 10.1177/0333102415610875
3. Plesh O, Adams SH, Gansky SA. Self-reported comorbid pains in severe headaches or migraines in a US national sample. Headache. (2012) 52:946–56. doi: 10.1111/j.1526-4610.2012.02155.x
4. Ashina S, Bendtsen L, Lyngberg AC, Lipton RB, Hajiyeva N, Jensen R. Prevalence of neck pain in migraine and tension-type headache: A population study. Cephalalgia. (2015) 35:211–9. doi: 10.1177/0333102414535110
5. Moore CS, Sibbritt DW, Adams J. A critical review of manual therapy use for headache disorders: prevalence, profiles, motivations, communication and self-reported effectiveness. BMC Neurol. (2017) 17:61. doi: 10.1186/s12883-017-0835-0
6. Luedtke K, Allers A, Schulte LH, May A. Efficacy of interventions used by physiotherapists for patients with headache and migraine–systematic review and meta-analysis. Cephalalgia. (2016) 36:474–92. doi: 10.1177/0333102415597889
7. Varatharajan S, Ferguson B, Chrobak K, Shergill Y, Côté P, Wong JJ, et al. Are non-invasive interventions effective for the management of headaches associated with neck pain? An update of the bone and joint decade task force on neck pain and its associated disorders by the ontario protocol for traffic injury management (OPTIMa). Eur Spine J. (2016) 25:1971–99. doi: 10.1007/s00586-016-4376-9
8. Bendtsen L, Evers S, Linde M, Mitsikostas DD, Sandrini G, Schoenen J. EFNS guideline on the treatment of tension-type headache - Report of an EFNS task force. Eur J Neurol. (2010) 17:1318–25. doi: 10.1111/j.1468-1331.2010.03070.x
9. Sarchielli P, Granella F, Prudenzano MP, Pini LA, Guidetti V, Bono G, et al. Italian guidelines for primary headaches: 2012 revised version. J Headache Pain. (2012) 13:31–70. doi: 10.1007/s10194-012-0437-6
10. Gaul C, Liesering-Latta E, Scha fer B, Fritsche G, Holle D, Schäfer B, et al. Integrated multidisciplinary care of headache disorders: a narrative review. Cephalalgia. (2016) 36:1181–91. doi: 10.1177/033310241561741
11. Coppola G, Di Lorenzo C, Serrao M, Parisi V, Schoenen J, Pierelli F. Pathophysiological targets for non-pharmacological treatment of migraine. Cephalalgia. (2016) 36:1103–11. doi: 10.1177/0333102415620908
12. Fernández-de-Las-Peñas C, Cuadrado ML. Physical therapy for headaches. Cephalalgia. (2016) 36:1134–42. doi: 10.1177/0333102415596445
13. Burstein R, Blake P, Schain A, Perry C. Extracranial origin of headache. Curr Opin Neurol. (2017) 30:263–71. doi: 10.1097/WCO.0000000000000437
14. Kerr FWL. Structural relation of the trigeminal spinal tract to upper cervical roots and the solitary nucleus in the cat. Exp Neurol. (1961) 4:134–48. doi: 10.1016/0014-4886(61)90036-X
15. Olszewski J. On the anatomical and functional organization of the spinal trigeminal nucleus. J Comp Neurol. (1950) 92:401–13 doi: 10.1002/cne.900920305
16. Phelan KD, Falls WM. The spinotrigeminal pathway and its spatial relationship to the origin of trigeminospinal projections in the rat. Neuroscience. (1991) 40:477–96. doi: 10.1016/0306-4522(91)90135-B
17. Schepelmann K, Ebersberger A, Pawlak M, Oppmann M, Messlinger K. Response properties of trigeminal brain stem neurons with input from dura mater encephali in the rat. Neuroscience. (1999) 90:543–54. doi: 10.1016/S0306-4522(98)00423-0
18. Levy D, Strassman AM. Mechanical response properties of A and C primary afferent neurons innervating the rat intracranial dura. J Neurophysiol. (2002) 88:3021–31. doi: 10.1152/jn.00029.2002
19. Abrahams VC, Anstee G, Richmond FJ, Rose PK. Neck muscle and trigeminal input to the upper cervical cord and lower medulla of the cat. Can J Physiol Pharmacol. (1979) 57:642–51. doi: 10.1139/y79-098
20. Vernon H, Sun K, Zhang Y, Yu XM, Sessle BJ. Central Sensitization Induced in trigeminal and upper cervical dorsal horn neurons by noxious stimulation of deep cervical paraspinal tissues in rats with minimal surgical trauma. J Manipulative Physiol Ther. (2009) 32:506–14.doi: 10.1016/j.jmpt.2009.08.012
21. Bartsch T, Goadsby PJ. Increased responses in trigeminocervical nociceptive neurons to cervical input after stimulation of the dura mater. Brain. (2003) 126:1801–13. doi: 10.1093/brain/awg190
22. Bartsch T, Goadsby PJ. Stimulation of the greater occipital nerve induces increased central excitability of dural afferent input. Brain. (2002) 125:1496–509. doi: 10.1093/brain/awf166
23. Kerr FWL. Central relationships of trigeminal and cervical primary afferents in the spinal cord and medulla. Brain Res. (1972) 43:561–72. doi: 10.1016/0006-8993(72)90408-8
24. Chudler EH, Foote WE, Poletti CE. Responses of cat C1 spinal cord dorsal and ventral horn neurons to noxious and non-noxious stimulation of the head and face. Brain Res. (1991) 555:181–92. doi: 10.1016/0006-8993(91)90341-R
25. Hu JW, Sun KQ, Vernon H, Sessle BJ. Craniofacial inputs to upper cervical dorsal horn: Implications for somatosensory information processing. Brain Res. (2005) 1044:93–106. doi: 10.1016/j.brainres.2005.03.004
26. Morch CD, Hu JW, Arendt-Nielsen L, Sessle BJ. Convergence of cutaneous, musculoskeletal, dural and visceral afferents onto nociceptive neurons in the first cervical dorsal horn. Eur J Neurosci. (2007) 26:142–54. doi: 10.1111/j.1460-9568.2007.05608.x
27. Le Doaré K, Akerman S, Holland PR, Lasalandra MP, Bergerot A, Classey JD, et al. Occipital afferent activation of second order neurons in the trigeminocervical complex in rat. Neurosci Lett. (2006) 403:73–77. doi: 10.1016/j.neulet.2006.04.049
28. Schueler M, Messlinger K, Dux M, Neuhuber WL, De Col R. Extracranial projections of meningeal afferents and their impact on meningeal nociception and headache. Pain. (2013) 154:1622–31. doi: 10.1016/j.pain.2013.04.040
29. Schueler M, Neuhuber WL, De Col R, Messlinger K. Innervation of rat and human dura mater and pericranial tissues in the parieto-temporal region by meningeal afferents. Headache. (2014) 54:996–1009. doi: 10.1111/head.12371
30. Palomeque-Del-Cerro L, Arráez-Aybar LA, Rodríguez-Blanco C, Guzmán-García R, Menendez-Aparicio M O-P-VÁ. A systematic review of the soft-tissue connections between neck muscles and dura mater: the myodural bridge. Spine. (2016) 42:49–54. doi: 10.1097/BRS.0000000000001655
31. Venne G, Rasquinha BJ, Kunz M, Ellis RE. Rectus capitis posterior minor. Spine. (2017) 42:E466–73. doi: 10.1097/BRS.0000000000001867
32. Goadsby PJ, Knight YE, Hoskin KL. Stimulation of the greater occipital nerve increases metabolic activity in the trigeminal nucleus caudalis and cervical dorsal horn of the cat. Pain. (1997) 73:23–8. doi: 10.1016/S0304-3959(97)00074-2
33. Bartsch T, Goadsby PJ. Anatomy and physiology of pain referral patterns in primary and cervicogenic headache disorders. Headache Curr. (2005) 2:27–52. doi: 10.1111/j.1743-5013.2005.20203.x
34. Maruyama H, Nagoya H, Kato Y, Deguchi I, Fukuoka T, Ohe Y, et al. Spontaneous cervicocephalic arterial dissection with headache and neck pain as the only symptom. J Headache Pain. (2012) 13:247–53. doi: 10.1007/s10194-012-0420-2
35. Gottesman R, Sharma P, Robinson K, Arnan M, Tsui M, Ladha K N-TD. Clinical Characteristics of symptomatic vertebral artery dissection. Neurologist. (2013) 18:245–54. doi: 10.1097/NRL.0b013e31826754e1
36. Schmidt-Hansen PT, Svensson P, Jensen TS, Graven-Nielsen T, Bach FW. Patterns of experimentally induced pain in pericranial muscles. Cephalalgia. (2006) 26:568–77. doi: 10.1111/j.1468-2982.2006.01078.x
37. Piovesan EJ, Kowacs PA, Tatsui CE, Lange MC, Ribas LC, Werneck LC. Referred pain after painful stimulation of the greater occipital nerve in humans: Evidence of convergence of cervical afferences on trigeminal nuclei. Cephalalgia. (2001) 21:107–9. doi: 10.1046/j.1468-2982.2001.00166.x
38. Johnston MM, Jordan SE, Charles AC. Pain referral patterns of the C1 to C3 nerves: Implications for headache disorders. Ann Neurol. (2013) 74:145–8. doi: 10.1002/ana.23869
39. Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol. (2009) 8:959–68. doi: 10.1016/S1474-4422(09)70209-1
40. Aprill C, Axinn MJ, Bogduk N. Occipital headaches stemming from the lateral atlanto-axial (C1-2) joint. Cephalalgia. (2002) 22:15–22. doi: 10.1046/j.1468-2982.2002.00293.x
41. Hall T, Briffa K, Hopper D, Robinson K. Reliability of manual examination and frequency of symptomatic cervical motion segment dysfunction in cervicogenic headache. Man Ther. (2010) 15:542–6. doi: 10.1016/j.math.2010.06.002
42. Watson DH, Drummond PD. Head pain referral during examination of the neck in migraine and tension-type headache. Headache. (2012) 52:1226–35. doi: 10.1111/j.1526-4610.2012.02169.x
43. Luedtke K, Starke W, May A. Musculoskeletal dysfunction in migraine patients. Cephalalgia. (2018) 38:865–75. doi: 10.1177/0333102417716934
44. Arendt-Nielsen L. Headache: muscle tension, trigger points and referred pain. Int J Clin Pract Suppl. (2015) 69:8–12. doi: 10.1111/ijcp.12651
45. Roch M, Messlinger K, Kulchitsky V, Tichonovich O, Azev O, Koulchitsky S. Ongoing activity in trigeminal wide-dynamic range neurons is driven from the periphery. Neuroscience. (2007) 150:681–91. doi: 10.1016/j.neuroscience.2007.09.032
46. Goadsby PJ. Migraine pathophysiology. Headache. (2005) 45:14–24. doi: 10.1111/j.1526-4610.2005.4501003.x
47. Goadsby PJ, Holland PR, Martins-oliveira M, Hoffmann J, Schankin C, Akerman S. Pathophysiology of migraine – a disorder of sensory processing. Physiol Rev. (2017) 97:553–622 doi: 10.1152/physrev.00034.2015
48. Olesen J, Burstein R, Ashina M, Tfelt-hansen P, Care C, Israel B. Origin of pain in migraine : evidence for peripheral sensitisation. Lancet Neurol. (2009) 8:679–690. doi: 10.1016/S1474-4422(09)70090-0
49. Ossipov MH, Dussor GO, Porreca F. Review series central modulation of pain. J Clin Invest. (2010) 120:3779–87. doi: 10.1172/JCI43766
50. Burstein R. Deconstructing migraine headache into peripheral and central sensitization. Pain. (2001) 89:107–10. doi: 10.1016/S0304-3959(00)00478-4
51. Goadsby PJ, Bartsch T. On the functional neuroanatomy of neck pain. Cephalalgia. (2008) 28 (Suppl. 1):1–7. doi: 10.1111/j.1468-2982.2008.01606.x
52. Levy D, Labastida-ramirez A, Maassenvandenbrink A. Current understanding of meningeal and cerebral vascular function underlying migraine headache. Cephalalgia. (2018) 1:333102418771350. doi: 10.1177/0333102418771350
53. Bendtsen L, Fernández-De-La-Peñas C. The role of muscles in tension-type headache. Curr Pain Headache Rep. (2011) 15:451–8. doi: 10.1007/s11916-011-0216-0
54. Bezov D, Ashina S, Jensen R, Bendtsen L. Pain perception studies in tension-type headache. Headache. (2011) 51:262–71. doi: 10.1111/j.1526-4610.2010.01768.x
55. Russo A, Coppola G, Pierelli F, Parisi V, Silvestro M, Tessitore A, et al. Pain Perception and Migraine. Front Neurol. (2018) 9:576. doi: 10.3389/fneur.2018.00576
56. Castien RF, van der Wouden JC, De Hertogh W. Pressure pain thresholds over the cranio-cervical region in headache: a systematic review and meta-analysis. J Headache Pain. (2018) 19:9. doi: 10.1186/s10194-018-0833-7
57. Bartsch T. Migraine and the neck new insights from basic data. Curr Pain Headache Rep. (2005) 9:191–6. doi: 10.1007/s11916-005-0061-0
58. Abboud J, Marchand A-A, Sorra K, Descarreaux M. Musculoskeletal physical outcome measures in individuals with tension-type headache : a scoping review. Cephalalgia. (2013) 33:1319–36. doi: 10.1177/0333102413492913
59. Robertson BA, Morris ME. The role of cervical dysfunction in migraine: A systematic review. Cephalalgia. (2008) 28:474–83. doi: 10.1111/j.1468-2982.2008.01545.x
60. Zito G, Jull G, Story I. Clinical tests of musculoskeletal dysfunction in the diagnosis of cervicogenic headache. Man Ther. (2006) 11:118–29. doi: 10.1016/j.math.2005.04.007
61. Amiri M, Jull G, Bullock-Saxton J, Darnell R, Lander C. Cervical musculoskeletal impairment in frequent intermittent headache. Part 2: Subjects with concurrent headache types. Cephalalgia. (2007) 27:891–8. doi: 10.1111/j.1468-2982.2007.01346.x
62. Szikszay TM, Hoenick S, von Korn K, Meise R, Schwarz A, Starke W, et al. Which examination tests detect differences in cervical musculoskeletal impairments in people with migraine? a systematic review and meta-analysis. Phys Ther. (2019). doi: 10.1093/ptj/pzz007. [Epub ahead of print].
63. Couppé C, Torelli P, Fuglsang-Frederiksen A, Andersen KV, Jensen R. Myofascial trigger points are very prevalent in patients with chronic tension-type headache: a double-blinded controlled study. Clin J Pain. (2007) 23:23–7. doi: 10.1097/01.ajp.0000210946.34676.7d
64. Fernández-de-las-Peñas C, Ge HY, Alonso-Blanco C, González-Iglesias J, Arendt-Nielsen L. Referred pain areas of active myofascial trigger points in head, neck, and shoulder muscles, in chronic tension type headache. J Bodyw Mov Ther. (2010) 14:391–6. doi: 10.1016/j.jbmt.2009.06.00
65. Fernández-de-las-Peñas C, Ge HY, Arendt-Nielsen L, Cuadrado ML, Pareja JA. Referred pain from trapezius muscle trigger points shares similar characteristics with chronic tension type headache. Eur J Pain. (2007) 11:475–82. doi: 10.1016/j.ejpain.2006.07.005
66. Fernández-de-las-Peñas C, Alonso-Blanco C, Cuadrado ML, Gerwin RD, Pareja JA. Trigger points in the suboccipital muscles and forward head posture in tension-type headache. Headache. (2006) 46:454–60. doi: 10.1111/j.1526-4610.2006.00288.x
67. Ogince M, Hall T, Robinson K, Blackmore AM. The diagnostic validity of the cervical flexion-rotation test in C1/2-related cervicogenic headache. Man Ther. (2007) 12:256–62. doi: 10.1016/j.math.2006.06.016
68. Nöbel M, Feistel S, Ellrich J, Messlinger K. ATP-sensitive muscle afferents activate spinal trigeminal neurons with meningeal afferent input in rat – pathophysiological implications for tension-type headache. J Headache Pain. (2016) 17:75. doi: 10.1186/s10194-016-0668-z
69. Villanueva L, Cadden SW, Le Bars D. Diffuse noxious inhibitory controls (DNIC): evidence for post-synaptic inhibition of trigeminal nucleus caudalis convergent neurones. Brain Res. (1984) 321:165–8. doi: 10.1016/0006-8993(84)90695-4
70. Bouhassira D, Le Bars D, Villanueva L. Heterotopic activation of A delta and C fibres triggers inhibition of trigeminal and spinal convergent neurones in the rat. J Physiol. (1987) 389:301–17. doi: 10.1113/jphysiol.1987.sp016658
71. Clement CI, Keay KA, Podzebenko K, Gordon BD, Bandler R. Spinal sources of noxious visceral and noxious deep somatic afferent drive onto the ventrolateral periaqueductal gray of the rat. J Comp Neurol. (2000) 425:323–44. doi: 10.1002/1096-9861(20000925)425:33.0.CO;2-Z
72. Mouton LJ, Klop EM, Holstege G. C1-C3 spinal cord projections to periaqueductal gray and thalamus: A quantitative retrograde tracing study in cat. Brain Res. (2005) 1043:87–94. doi: 10.1016/j.brainres.2005.02.042
73. Malick A, Burstein R. Cells of origin of the trigeminohypothalamic tract in the rat. J Comp Neurol. (1998) 400:125–44.
74. Panfil C, Makowska A, Ellrich J. Brainstem and cervical spinal cord Fos immunoreactivity evoked by nerve growth factor injection into neck muscles in mice. Cephalalgia. (2006) 26:128–35. doi: 10.1111/j.1468-2982.2005.01005.x
75. Keay KA, Bandler R. Anatomical evidence for segregated input from the upper cervical spinal cord to functionally distinct regions of the periaqueductal gray region of the cat. Neurosci Lett. (1992) 139:143–8. doi: 10.1016/0304-3940(92)90538-I
76. Keay KA, Clement CI, Owler B, Depaulis A, Bandler R. Convergence of deep somatic and visceral nociceptive information onto a discrete ventrolateral midbrain periaqueductal grey region. Neuroscience. (1994) 61:727–32. doi: 10.1016/0306-4522(94)90395-6
77. Klop EM, Mouton LJ, Holstege G. Segmental and laminar organization of the spinal neurons projecting to the periaqueductal gray (PAG) in the cat suggests the existence of at least five separate clusters of spino-PAG Neurons. J Comp Neurol. (2000) 428:389–410. doi: 10.1002/1096-9861(20001218)428:3<389::AID-CNE2>3.0.CO;2-B
78. Keay KA, Li QF, Bandler R. Muscle pain activates a direct projection from ventrolateral periaqueductal gray to rostral ventrolateral medulla in rats. Neurosci Lett. (2000) 290:157–60. doi: 10.1016/S0304-3940(00)01329-X
79. Knight YE, Goadsby PJ. The periaqueductal grey matter modulates trigeminovascular input: A role in migraine? Neuroscience. (2001) 106:793–800. doi: 10.1016/S0306-4522(01)00303-7
80. Goadsby PJ, Bartsch T, Dodick DW. Occipital nerve stimulation for headache: mechanisms and efficacy. Headache. (2008) 48:313–8. doi: 10.1111/j.1526-4610.2007.01022.x
81. Busch V, Jakob W, Juergens T, Schulte-Mattler W, Kaube H, May A. Functional connectivity between trigeminal and occipital nerves revealed by occipital nerve blockade and nociceptive blink reflexes. Cephalalgia. (2006) 26:50–5. doi: 10.1111/j.1468-2982.2005.00992.x
82. Ashkenazi A, Young WB. The effects of greater occipital nerve block and trigger point injection on brush allodynia and pain in migraine. Headache. (2005) 45:350–4. doi: 10.1111/j.1526-4610.2005.05073.x
83. Afridi SK, Shields KG, Bhola R, Goadsby PJ. Greater occipital nerve injection in primary headache syndromes - prolonged effects from a single injection. Pain. (2006) 122:126–9. doi: 10.1016/j.pain.2006.01.016
84. Cooper G, Bailey B, Bogduk N. Cervical zygapophysial joint pain maps. Pain Med. (2007) 8:344–53. doi: 10.1111/j.1526-4637.2006.00201.x
85. Piovesan EJ, Di Stani F, Kowacs PA, Mulinari RA, Radunz VH, Utiumi M, et al. Massaging over the greater occipital nerve reduces the intensity of migraine attacks: Evidence for inhibitory trigemino-cervical convergence mechanisms. Arq Neuropsiquiatr. (2007) 65:599–604. doi: 10.1590/S0004-282X2007000400010
86. Sessle BJ. Acute and chronic craniofacial pain: brainstem mechanisms of nociceptive transmission and neuroplasticity, and their clinical correlates. Crit Rev Oral Biol Med. (2000) 11:57–91. doi: 10.1177/10454411000110010401
87. Liu J-X, Thornell L-E, Pedrosa-Domellöf F. Muscle spindles in the deep muscles of the human neck: a morphological and immunocytochemical study. J Histochem Cytochem. (2003) 51:175–86. doi: 10.1177/002215540305100206
88. Jull G, Hall T. Cervical musculoskeletal dysfunction in headache: How should it be defined? Musculoskelet Sci Pract. (2018) 38:148–50. doi: 10.1016/j.msksp.2018.09.012
Keywords: physical treatment, headache, neck pain, pain, neurology, clinical reasoning, neurophysiology
Citation: Castien R and De Hertogh W (2019) A Neuroscience Perspective of Physical Treatment of Headache and Neck Pain. Front. Neurol. 10:276. doi: 10.3389/fneur.2019.00276
Received: 13 December 2018; Accepted: 04 March 2019;
Published: 26 March 2019.
Edited by:
Massimiliano Valeriani, Bambino Gesù Children Hospital (IRCCS), ItalyReviewed by:
César Fernández-de-las-Peñas, Universidad Rey Juan Carlos, SpainYohannes W. Woldeamanuel, Stanford University, United States
Copyright © 2019 Castien and De Hertogh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: René Castien, r.castien@vumc.nl