 Ludivine Chamard Witkowski1,2,3*
Ludivine Chamard Witkowski1,2,3* Mathieu Mallet1
Mathieu Mallet1 Mathieu Bélanger1,2,3
Mathieu Bélanger1,2,3 Alier Marrero1,3
Alier Marrero1,3 Grant Handrigan4
Grant Handrigan4- 1Vitality Health Network, Dr. Georges-L.-Dumont University Hospital Centre, Moncton, NB, Canada
- 2Faculté de Médecine et des Sciences de la Santé, Université de Sherbrooke, Sherbrooke, QC, Canada
- 3Centre de Formation Médicale du Nouveau-Brunswick, Moncton, NB, Canada
- 4École de Kinésiologie et de Loisir, Université de Moncton, Moncton, NB, Canada
Multiple Sclerosis (MS) is a neurodegenerative disease associated with cognition and balance impairments, which can lead to accidental falls. Postural control requires cognitive resources. This interaction is quantifiable by using the dual-task paradigm. The cognitive-postural interference (CPI) is commonly evaluated through an assessment of the dual-task cost (DTC). The aim of this review was to summarize literature related to process, results and effects of CPI in MS patients. The Prisma statement was used to guide this systematic review. Eligible articles had to include participants with MS for whom CPI was assessed using the DTC. A total of 14 articles meeting inclusion criteria were retained. All studies used the double stance with eyes open for the postural task component. Three types of cognitive tasks were used: Stroop Color–Word Test (SCWT), Word List Generation and Backward Counting. However, cognitive task scores in single or dual task were unavailable in 11 studies, which prevented calculating the DTC for that task. Prioritization instructions were provided in seven studies. Mutual interference was shown in three studies, postural interference in nine and postural facilitation in two. This review highlights the presence of CPI among MS patients. Postural interference usually occurred during dual task while cognitive performance during dual task was rarely reported. Postural task performance does not appear to vary based on EDSS level. We advise authors of future studies to use the SCWT in combination with postural task measure (sway area and postural sway) for DT assessment, with explicit prioritization instructions. Further, the cognitive and postural tasks should be performed in ST and DT and all results should be presented.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and neurodegenerative disease of the central nervous system affecting visual, cerebellar, sensory, and motor functions. MS is associated with executive dysfunction and postural impairments and affects quality of life in 85% of patients (1). Imbalance and risk of falling are reported in early MS patients with absence of clinical disability (2). Moreover, 65% of MS patients have some form of cognitive impairment (3).
Postural control is defined as the body's ability to maintain adequate gravity alignment when maintaining an upright posture with voluntary and involuntary movements (4). It is a complex task that requires integration of visual, vestibular, and somatosensory information by the central nervous system (5). Postural control involves specific cortical areas, and attentional and executive dysfunctions are associated with motor disorders (6). There is a physiological relationship between attention, cognition and balance; these functions are, respectively, treated by the frontal lobes, the thalami and the cerebellum, which are linked by a neuronal network (7).
Postural and cognitive disorders were traditionally measured independently in MS patients; however, the simultaneous assessment of postural and cognitive performances demonstrated an interaction suggesting shared attentional resources (8, 9).
The cognitive-postural interference (CPI) is measured by performing a dual task (DT) examination, which involves conducting a postural task along with a cognitive task and comparing performance with that of single-task conditions. The dual-task cost (DTC) is used to quantify the CPI, which represents the percent difference between DT and ST performance (10). Specifically, in cases where higher values indicate better performance, DTC (%) can be calculated as:
and for variables where higher values indicate worse performance as:
Further, taking consideration of the DTC of both tasks is important when assessing DTC since nine scenarios can occur: (1) No DT interference; (2) Motor Facilitation; (3) Cognitive Facilitation; (4) Mutual Facilitation; (5) Motor-related cognitive interference; (6) Cognitive-related motor interference; (7) Motor-priority trade-off; (8) Cognitive-priority trade-off; and (9) Mutual interference (11).
There is interest in studying the CPI as it provides insight into real-life affectations of postural control challenges for MS patients who experience cognitive and balance disorders. However, the studies that have reported CPI in MS have used methods and inclusion criteria that differ and may present diverging results.
Two systematic reviews on the CPI were published in recent years (9, 12). However, these reviews included studies published before 09/01/2014 (9) or between 01/01/2005 and 31/10/2015 (12). As CPI in persons with MS is a potentially useful clinical outcome, it is important to have the most recent information to aid further research into CPI as a clinical outcome measurement (9, 12).
The objective of this systematic review was to compare and contrast clinical studies that have assessed CPI in MS patients, including radiologically isolated syndrome (RIS) patients and clinically isolated syndrome (CIS) and to summarize evidence emerging from these studies.
Methods
This review is based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations, and the search strategy—including keywords and choice of databases (13)—was developed in collaboration with an experienced librarian. Searches were conducted in PubMed, ScienceDirect and SPORTdiscus for potentially relevant studies without date restrictions (last updated in October 2018). The keywords applied for this search were {“Multiple Sclerosis”} AND {“Dual Task” OR “Dual Task Cost” OR Cognitive-Motor Interference”} AND {“Balance” OR “Posture”}. Previous reviews were excluded but examined to identify publications that may have been missed by our search strategy. Reference lists of eligible studies were also reviewed to ensure that all potentially eligible studies were retrieved. Eligible studies were peer-reviewed and original studies, published in either English or French, whose MS participants were performing postural (i.e., double stance, eyes open) and cognitive tasks at the same time. All types of quantitative study designs were eligible for this review.
The exclusion criteria were: (1) studies concerning walking; (2) studies concerning effectiveness of rehabilitation process; and (3) studies concerning effectiveness of medications, unless the pre-treatment data were available.
Once duplicates were removed, titles and abstracts were assessed independently by two reviewers (LCW and MM). The full texts of articles considered potentially eligible were then assessed. Any disagreement between the two reviewers led to a discussion and group-based decision about study inclusion. Results extraction was also conducted by two independent reviewers (LCW and MM). Quality assessment was performed with two tools, the National Service Framework Typology of Evidence—Quality Assessment (NSFTE—QA) (14) and the Quality Assessment of Diagnostic Accuracy Studies 2 tool (QUADAS-2) (15). For the QUADAS-2 tool, we applied it in the same manner that was described by Learmonth et al. (12), for the assessment of the judgement of bias for patient selection, index test and flow of the participants. We modified our judgment of bias for the reference standard element to whether or not there were baseline measures of the ST for each of the cognitive and motor tasks for each study. Study type, methodological information, inclusion criteria, number of MS and control participants, Expanded Disability Status Scale (EDSS) score, type of cognitive and postural tasks, and performance scores in single (cognitive and postural) and in dual task were collected. The DTC for the MS participants was calculated for each study. When a large amount of posture and cognitive data were available in an article, the sway area and the Stroop color and word test (SCWT) (16) were used in the DTC calculation, as they were the most frequently used tests, which facilitated data comparison. It is important to note that the DTC values were calculated using the group average performance of the single and dual task (cognitive and postural). The DTC was then represented on a graph to classify CPI patterns. A balance variable was presented on the X-axis, where a positive result was indicative of improved balance (reduced sway area) during the DT and a negative result would show impaired balance (increased sway area) compared to the ST. Similarly, a negative to positive continuum was used to represent the cognitive variable on the Y-axis (10).
Results
A total of 42 distinct references were found. Of these, 23 were excluded after reading the titles and abstracts, and seven more were excluded once they were read in full. Two additional articles were then added to the list following verification of authors' libraries, for a total of 14 articles included in this literature review (Figure 1).
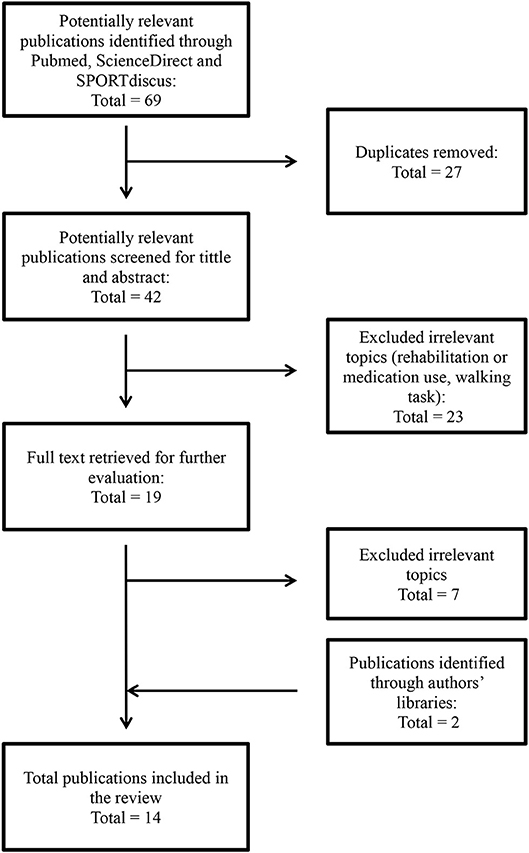
Figure 1. Flowchart of the systematic literature search. The figure was inspired by Moher et al. (13).
The 14 manuscripts were published between 2010 and 2018 (Table 1). Most of these studies (nine) were cross-sectional and seven had a control group of healthy subjects. One publication had a patient group consisting of subjects with CIS (22) and one with RIS (20), the other publications had subjects with clinically defined diagnostics of MS. The type of MS was not always specified; three articles had patients with relapsing-remitting MS (21, 23, 24) and one with relapsing-remitting and secondary progressive MS patients (26). The inclusion criteria of the MS group were heterogeneous. Most studies had broad inclusion criteria in terms of disability (7, 23–27). Some studies involved patients with an already advanced level of disability, in terms of high EDSS score (4.0–6.5 for the moderate disability group) (17), or risk of falling evaluated with the number of falls during the previous year (21, 28, 29) or moderate to severe spasticity (19), whereas others included patients with low disability represented by low EDSS score (3.0 or less) (18); radiologically (20) or CIS (22). One study (17) compared two distinct groups of MS patients by their degree of disability (Mild vs. Moderate). Some studies excluded patients over 40 years old (28), 45 years old (21, 22) and 55 years old (7, 26, 27). One study (29) involved older patients (50–75 years old). Most studies included patients who had been stable for 1–3 months, could stand upright, and were free of major visual or cognitive impairment (7, 18, 21, 26, 27). Some studies excluded patients with severe depression (7, 18, 26, 27).
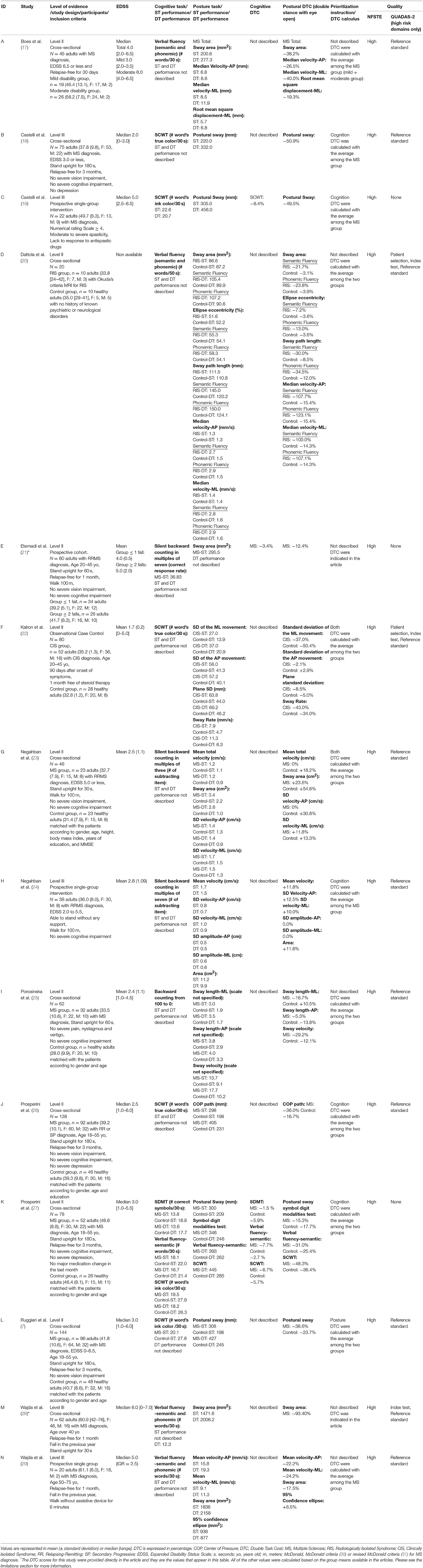
Table 1. Summary of the characteristics of the studies included in the review.
The median EDSS score of MS patients included ranged from 2.0 to 6.0, while the average EDSS score ranged from 1.7 to 2.8. The cognitive tasks chosen were tasks that we could qualify as executive function tests. In six studies it was the SCWT, which measures mental flexibility and inhibition capacity (32). Categorical or phonemic word fluencies (e.g., Word List Generation) was used in five studies. These tests measure lexical access as well as mental flexibility (33). Silent Backward Counting with different multiples was used in four studies. This test is more often used to measure the working memory (34). Subjects of one study (27) performed three different cognitive tasks: the SCWT, Word List Generation and the Symbol Digit Test.
For the postural task, participants were evaluated on a force platform where the center of pressure was generated by trials in a double stance with eyes open. Many centers of pressure metrics (e.g., postural sway, sway velocity, and sway area) were generated, but several articles did not have the same center of pressure metrics. Regarding the number of trials, eight studies did only one trial for each postural condition (7, 18–21, 25–27), four studies did two trials (17, 24, 28, 29) and two studies did three trials (22, 23). Concerning the duration of the trials, most of the studies collected the data for a period of 30 s, two studies for 50 s (20, 25) and one for 60 s (21).
When it was not directly available in the article, we calculated the cognitive and postural DTC from the available data. The graphical representation of the DTC results from all of the eligible studies is presented in Figure 2. Only three articles had the baseline scores of the cognitive task (during the ST). In these studies, the cognitive/postural DTC showed mutual interference (19, 21, 27). Since the other studies did not present information on baseline score of the cognitive task, their results could not be positioned along the X-axis. Two studies (23, 24) showed a postural facilitation during the DT and the 12 showed a postural interference.
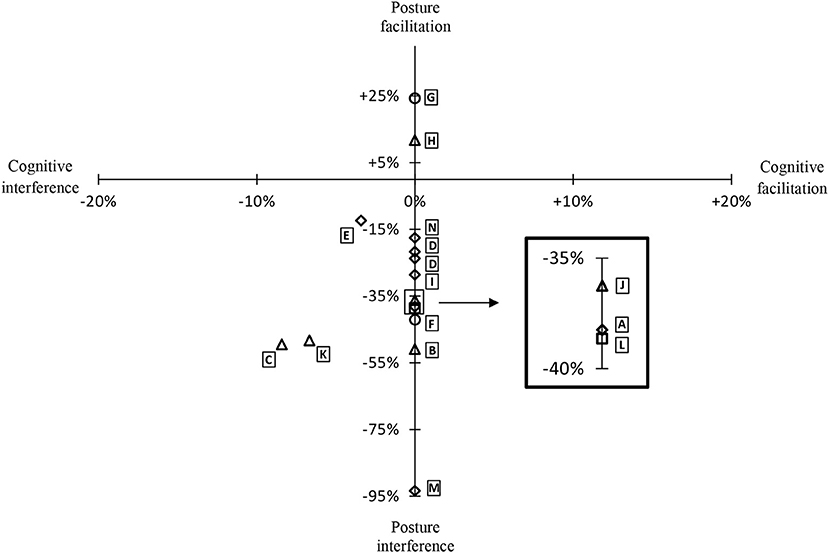
Figure 2. Graphical representation of the DTC (MS subjects) for the included studies of the review. Prioritization instructions: ♢, No instructions, □, Posture, ▵, Cognition, ◦, Both tasks. The DTC from de study of Datolla et al. (20) (D) are represented by two points for the semantic and phonetic fluency tasks.
Prioritization instructions were explicitly stated in eight publications, for either the postural task or the cognitive, or both. Five studies (18, 19, 24, 26, 27) had instructed the participants to prioritize the cognitive task and one study asked them to prioritize the postural task (7). Two studies (22, 23) had instructions to prioritize equally both of the tasks during the DT.
Concerning the group differences for the DTC, there were five studies that reported postural interference during the DT condition for both the control groups and the MS groups, with the MS groups showing the largest interference (7, 20, 22, 25, 26). One study reported postural facilitation during the DT condition for both the control group and the MS group, with the control group increasing their performance the most (23). One study used three cognitive tests, and also included the ST cognitive performance scores enabling calculation of the cognitive DTC, and their results differ between the tests: for the SDMT cognitive task DTC for both control and MS groups there was cognitive interference, with the MS group demonstrating less interference, for the verbal fluency and SCWT cognitive tasks DTC for both control and MS groups' demonstrated cognitive interference with the MS group demonstrating greater interference. For this study, the same tendency was found for the postural DTC (27).
Discussion
In this study, we systematically reviewed methods and results of 14 studies assessing CPI in MS patients. Despite considerable variation in research protocols, most studies documented that DT is associated with a motor related-cognitive interference or motor interference. This signifies that the postural task is affected when the MS patient simultaneously performs a cognitive task. This creates increased falling risks for MS patients in many common situations during activities of daily living, such as standing and talking on the telephone or withdrawing money from an automated banking machine (9).
It would seem that during the DT, the neurological processes associated with postural control and attention share the same neural network in MS patients, which can lead to a deterioration of the postural performance during the DT or vice versa (21), even in a population with no neurological deficit like patients with isolated radiological syndrome (20).
Several theories have been posited to explain the CPI. First, the attentional capacity theory suggests that an individual has a limit to his or her ability to pay attention. During the DT, the capacity is exceeded and one or both tasks' performance will decline (8, 9). Second, the bottleneck theory proposes that due to limited resources, only one task can be performed at a time (35). Third, the self-awareness theory suggests that a person will prioritize one task over the other in a rather conscious way depending on factors such as the environmental demands and task complexity. For example, during the DT, MS patients would alter prioritization of tasks depending on the complexity of the cognitive task and the difficulty of the motor task (36).
This last theory could explain the results of the two studies where there was a postural improvement during the DT (23, 24). It is difficult to know exactly what occurred for the patients of these two studies, as the authors did not present results of cognitive single and double tasks, so we do not know if the cognitive task was improved or worsened by the dual tasking. These publications used a cognitive task considered easier than the ones used in other studies in term of difficulty, however one other study used silent backward counting and found contradictory results (21), that is decreased performance during DT for the MS patients. Furthermore, a recent systematic review and meta-analysis concluded that there are postural control deficits in people with MS when compared to healthy controls (37).
Although the postural task used was similar across studies, the cognitive tasks varied. For example, the SCWT evaluates the executive functions that are most often affected in MS, such as processing speed, long-term memory and attention (3, 38, 39). The SCWT uses a list of names which represent colors printed in the ink of another color (40), and the task consists in reading color names, naming the color of colored dots and naming the intentionally differently displayed color of colors' names. Unlike computation or language tasks, the SCWT is not considerably influenced by level of education. However, mental arithmetic and verbal fluency tasks, as used in other studies, do not require specific materiel and can be used without visual restrictions, which facilitates their use in MS patients with visual impairment. However, it is possible that tasks such as silent backward counting may be too simple for some participants and therefore, the task difficulty varies between participants. It is even possible that such tests allow patients to shift their focus externally and to permit the CNS to perform automatically the postural task more efficiently. A recent study in older adults suggested that an external focus and cognitive task could improve postural control and that could be by the automaticity of sway (41).
Only one study compared various cognitive tasks within their sample population. Prosperini et al. (27) investigated the SDMT, verbal fluency (i.e., semantic) and the SCWT in a sample of 52 adults with MS. They found that there was no main effect on DTC between the three cognitive tasks between the adults with MS and those without MS, with each approximately equally creating a cognitive interference. For the postural task performance, it was found that the SCWT had the largest impact on performance for the adults with MS, when compared with controls; however, their analysis reveals that all of the cognitive tasks created a balance interference in both the adults with MS and those without MS. These results suggest that in order to differentiate those with MS from those without MS for postural performance, the SCWT cognitive task is most effective.
Some studies were interested in MS patients with little or no disability, and those that did investigate found that there was a CPI in the early stage of the disease, such as RIS and CIS patients (20, 22). In this way, the DT paradigm may have the advantage of revealing subtle deficits because of its sensitivity and could even facilitate an early diagnosis of MS. This test challenges the diagnosis of isolated radiological syndrome that is based on the theory that brain lesions are not related to any symptoms (20). That CPI is present in such patients is based on two hypotheses raised by a functional MRI study that indicated lesions could have disconnected two distinct circuits (7), including the anterior and superior corona radiata which connects cerebellum, striatum and pre-frontal areas, and the anterior thalamic peduncles, which connects frontal lobes and anterior/midline nuclear groups of thalami. Accordingly, it indicates that the frontal lobe, which is responsible for executive functions, is related to the cerebellum, which is responsible for balance, but also with the thalamus that contains the sensory pathways used for the pallesthesia. These lesions disconnected the pathways and can cause postural and cognitive impairments during the DT.
The EDSS score seemed to be an important factor to have homogeneous groups, as it was a frequent inclusion criterion. However, one with severely disabled patients did not show more severe interference (29). In addition, another study (17) tested two different groups of MS patients (mild vs. moderate disability) and showed no significant difference in the two groups. Based on these results, we recommend that there should be more research efforts focused on determining appropriate criteria for establishing homogeneity of groups and investigating the differences between EDSS levels and cognitive and motor task performance in persons with MS.
Only three studies (19, 21, 27) presented the results of the cognitive task in single and dual task conditions, thus permitting calculation of the cognitive DTC. These studies showed cognitive and motor interference. Two of these studies (19, 27) prioritized cognition. However, even in these contexts, the two tasks, regardless if they were cognitive or postural, demonstrated performance decrements during dual task performance. Furthermore, it seems that there is less of a difference between the cognitive tests in ST vs. DT than for the postural tests (see Table 1). In other words, the cognitive tasks' performances were negatively influenced, but the postural tasks were even more affected. Therefore, these results demonstrate the importance of standardizing and presenting instructions on task prioritization and also of collecting the task performances in both dual and single task situations.
Concerning group differences, seven studies included a control group thus permitting the comparison between controls and MS participants. For all seven studies the control groups always performed better than the MS participants, thus indicating that the performance of a DT negatively affects the MS groups more than the control groups. However, there was one exception for one specific cognitive task (i.e., SDMT) in the study by Prosperini et al. (27) that showed the opposite effect based on the DTC calculation, with the MS group outperforming the control group for both cognitive and postural tasks. It is important to note that Prosperini et al. (27) did not find the same results as we did likely because of the difference in the manner that the DTC were calculated. For our calculations, we measured the DTC with the group averages because this was the only information available in the published article, and this affects the outcome and interpretation of the DTC results. The limitations section below describes this is more detail.
This systematic review is not without limitations, the primary limitation is in the manner that our DTC scores were obtained. The DTC scores presented in Table 1 were either presented directly in the text of the articles (21, 28) or were calculated based on the information available in each of the articles (7, 17–20, 22–27, 29). When the DTC scores were not available in the articles, the DTCs were calculated by using the group ST and DT means, and it is unclear how much of a difference exists in the DTCs calculated by using the group means compared to using the individual DTC scores to obtain the mean DTC score. For an example of how the two methods can vary, Wajda et al. (28) provided the ST and DT postural scores and provided the DTC mean calculated based on the individual values. When we calculate the DTC using the group means of the ST and DT postural scores, we do not obtain the same value as the DTC score that was calculated with the individual scores. However, this occurred only for this instance and the other articles all used the same method of using the group means to calculate the DTC score. In addition, our objective was to focus solely on postural and cognitive tasks in persons with MS. There are other tasks in activities of daily living that are also of interest to explore the cognitive-motor interferences in persons with MS.
In conclusion, this review highlights the presence of a CPI, whereby impairments in MS patients are associated with postural interference in situations of DT. The level of postural interference was not related to the degree of incapacity as determined by EDSS score. These results suggest that situations when MS patients have to deal with postural and cognitive tasks simultaneously expose them to increased balance impairment, an important precursor of risk of falls. From an assessment perspective, recommendations emanating from this review include that the SCWT appears as the most appropriate cognitive task to use in combination with postural task measure (sway area and postural sway) in the context of DT assessment. Also, DT assessment requires delivery of explicit prioritization instructions to avoid conscious prioritization of one task over another. Further, the cognitive and postural tasks must be performed in ST and DT, and all the results must be presented to provide a clear understanding of CPI affectations.
Data Availability
All datasets generated for this study are included in the manuscript/supplementary files.
Author Contributions
MM authored the original draft of this systematic review. LC and GH contributed to the modification of the manuscript for submission. MB and AM provided critical feedback and helped shape the final version of the manuscript. MM and GH contributed equally to the conception of the idea upon which is based this manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Larocca NG. Impact of walking impairment in multiple sclerosis : perspectives of patients and care partners. Patient. (2011) 4:189–201. doi: 10.2165/11591150-000000000-00000
2. Martin CL, Phillips BA, Kilpatrick TJ, Butzkueven H, Tubridy N, McDonald E, et al. Gait and balance impairment in early multiple sclerosis in the absence of clinical disability. Mult Scler J. (2006) 12:620–8. doi: 10.1177/1352458506070658
3. Chiaravalloti ND, DeLuca J. Cognitive impairment in multiple sclerosis. Lancet Neurol. (2008) 7:1139–51. doi: 10.1016/S1474-4422(08)70259-X
4. Pollock AS, Durward BR, Rowe PJ, Paul JP. What is balance? Clin Rehabil. (2000) 14:402–6. doi: 10.1191/0269215500cr342oa
5. Marsden CD, Merton PA, Morton HB. Human postural responses. Brain. (1981) 104:513–34. doi: 10.1093/brain/104.3.513
6. Yogev-Seligmann G, Hausdorff JM, Giladi N. The role of executive function and attention in gait. Mov Disord. (2008) 23:329–42. doi: 10.1002/mds.21720
7. Ruggieri S, Fanelli F, Castelli L, Petsas N, De Giglio L, Prosperini L. Lesion symptom map of cognitive–postural interference in multiple sclerosis. Mult Scler J. (2018) 24:653–62. doi: 10.1177/1352458517701313
8. Woollacott M, Shumway-Cook A. Attention and the control of posture and gait tte review of an emerging area of research. Gait Posture. (2002) 16:1–14. doi: 10.1016/S0966-6362(01)00156-4
9. Wajda DA, Sosnoff JJ. Cognitive-motor interference in multiple sclerosis: a systematic review of evidence, correlates, and consequences. Bio Med Res Int. (2015) 2015:720856. doi: 10.1155/2015/720856
10. Plummer P, Eskes G. Measuring treatment effects on dual-task performance: a framework for research and clinical practice. Front Human Neurosci. (2015) 9:225. doi: 10.3389/fnhum.2015.00225
11. Plummer P, Eskes G, Wallace S, Giuffrida C, Fraas M, Campbell G, et al. Cognitive-motor interference during functional mobility after stroke: state of the science and implications for future research. Arch Phys Med Rehabil. (2013) 94:2565–74 e6. doi: 10.1016/j.apmr.2013.08.002
12. Learmonth YC, Ensari I, Motl RW. Cognitive motor interference in multiple sclerosis: insights from a systematic quantitative review. Arch Phys Med Rehabil. (2017) 98:1229–40. doi: 10.1016/j.apmr.2016.07.018
13. Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLOS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
14. Turner-Stokes L, Harding R, Sergeant J, Lupton C, McPherson K. Generating the evidence base for the National Service Framework for long term conditions : a new research typology. Clin Med. (2006) 6:91–7. doi: 10.7861/clinmedicine.6-1-91
15. Whiting PF. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Internal Med. (2011) 155:529. doi: 10.7326/0003-4819-155-8-201110180-00009
16. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. (1935) 18:643–62. doi: 10.1037/h0054651
17. Boes MK, Sosnoff JJ., Socie MJ, Sandroff BM, Pula JH, Motl RW. Postural control in multiple sclerosis: effects of disability status and dual task. J Neurol Sci. (2012) 315:44–8. doi: 10.1016/j.jns.2011.12.006
18. Castelli L, De Luca F, Marchetti MR, Sellitto G, Fanelli F, Prosperini L. The dual task-cost of standing balance affects quality of life in mildly disabled MS people. Neurol Sci. (2016) 37:673–9. doi: 10.1007/s10072-015-2456-y
19. Castelli L, Prosperini L, Pozzilli C. Balance worsening associated with nabiximols in multiple sclerosis. Mult Scler J. (2019) 25:113–7. doi: 10.1177/1352458518765649
20. Dattola V, Logiudice AL, Bonanno L, Famà F, Milardi D, Chillemi G, et al. Does the radiologically isolated syndrome exist? A dual-task cost pilot study. Neurol Sci. (2017) 38:2007–13. doi: 10.1007/s10072-017-3094-3
21. Etemadi Y. Dual task cost of cognition is related to fall risk in patients with multiple sclerosis: a prospective study. Clin Rehabil. (2017) 31:278–84. doi: 10.1177/0269215516637201
22. Kalron A, Dvir Z, Achiron A. Effect of a cognitive task on postural control in patients with a clinically isolated syndrome suggestive of multiple sclerosis. Eur J Phys Rehabil Med. (2011) 47:579–86.
23. Negahban H, Mofateh R, Arastoo AA, Mazaheri M, Yazdi MJS, Salavati M, et al. The effects of cognitive loading on balance control in patients with multiple sclerosis. Gait Posture. (2011) 34:479–84. doi: 10.1016/j.gaitpost.2011.06.023
24. Negahban H, Monjezi S, Mehravar M, Mostafaee N, Shoeibi A. Responsiveness of postural performance measures following balance rehabilitation in multiple sclerosis patients. J Bodywork Mov Ther. (2018) 22:502–10. doi: 10.1016/j.jbmt.2017.06.008
25. Porosinska A, Pierzchała K, Mentel M, Karpe J. Evaluation of postural balance control in patients with multiple sclerosis – effect of different sensory conditions and arithmetic task execution. A pilot study. Neurol Neurochir Pol. (2010) 44:35–42. doi: 10.1016/S0028-3843(14)60405-9
26. Prosperini L, Castelli L, Sellitto G, De Luca F, De Giglio L, Gurreri F, et al. Investigating the phenomenon of “cognitive-motor interference” in multiple sclerosis by means of dual-task posturography. Gait Posture. (2015) 41:780–5. doi: 10.1016/j.gaitpost.2015.02.002
27. Prosperini L, Castelli L, De Luca F, Fabiano F, Ferrante I, De Giglio L. Task-dependent deterioration of balance underpinning cognitive-postural interference in MS. Neurology. (2016) 87:1085–92. doi: 10.1212/WNL.0000000000003090
28. Wajda DA, Motl RW, Sosnoff JJ. Correlates of dual task cost of standing balance in individuals with multiple sclerosis. Gait Posture. (2014) 40:352–6. doi: 10.1016/j.gaitpost.2014.04.209
29. Wajda DA, Motl RW, Sosnoff JJ. Three-month test-retest reliability of center of pressure motion during standing balance in individuals with multiple sclerosis. Int J MS Care. (2016) 18:59–62. doi: 10.7224/1537-2073.2015-014
30. McDonald WI, Compston A, Edan G, Goodkin D, Hartung H-P, Lublin FD, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the international panel on the diagnosis of multiple sclerosis. Ann Neurol. (2001) 50:121–7. doi: 10.1002/ana.1032
31. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi M, et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann Neurol. (2011) 69:292–302. doi: 10.1002/ana.22366
32. Barbarotto R, Laiacona M, Frosio R, Vecchio M, Farinato A, Capitani E. A normative study on visual reaction times and two Stroop colour-word tests. Ital J Neurol Sci. (1998) 19:161–70. doi: 10.1007/BF00831566
33. Strauss E, Sherman EMS, Spreen O. (2006). A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary. New York, NY: Oxford University Press.
34. Raghubar KP, Barnes MA, Hecht SA. Working memory and mathematics: a review of developmental, individual difference, and cognitive approaches. Learn Individual Differ. (2010) 20:110–22. doi: 10.1016/j.lindif.2009.10.005
35. Pashler H. Graded capacity-sharing in dual-task interference? J Exp Psychol Human Percept Perform. (1994) 20:330–42. doi: 10.1037//0096-1523.20.2.330
36. Patel P, Lamar M, Bhatt T. Effect of type of cognitive task and walking speed on cognitive-motor interference during dual-task walking. Neuroscience. (2014) 260:140–8. doi: 10.1016/j.neuroscience.2013.12.016
37. Comber L, Sosnoff JJ, Galvin R, Coote S. Postural control deficits in people with Multiple Sclerosis: a systematic review and meta-analysis. Gait Posture. (2018) 61:445–52. doi: 10.1016/j.gaitpost.2018.02.018
38. Ruggieri RM, Palermo R, Vitello G, Gennuso M, Settipani N, Piccoli F. Cognitive impairment in patients suffering from relapsing-remitting multiple sclerosis with EDSS < or = 3.5. Acta Neurol Scand. (2003) 108:323–6. doi: 10.1034/j.1600-0404.2003.00157.x
39. Patti F, Amato MP, Trojano M, Bastianello S, Tola MR, Goretti B, et al. Cognitive impairment and its relation with disease measures in mildly disabled patients with relapsing-remitting multiple sclerosis: baseline results from the Cognitive Impairment in Multiple Sclerosis (COGIMUS) study. Mult Scler. (2009) 15:779–88. doi: 10.1177/1352458509105544
40. Vanderhasselt M-A, De Raedt R, Baeken C. Dorsolateral prefrontal cortex and Stroop performance: tackling the lateralization. Psychon Bull Rev. (2009) 16:609–12. doi: 10.3758/PBR.16.3.609
Keywords: dual-task, multiple sclerosis, cognition, postural control, balance, cognitive-postural interference
Citation: Chamard Witkowski L, Mallet M, Bélanger M, Marrero A and Handrigan G (2019) Cognitive-Postural Interference in Multiple Sclerosis. Front. Neurol. 10:913. doi: 10.3389/fneur.2019.00913
Received: 04 June 2019; Accepted: 06 August 2019;
Published: 23 August 2019.
Edited by:
Brian M. Sandroff, University of Alabama at Birmingham, United StatesReviewed by:
Renee Veldkamp, University of Hasselt, BelgiumRicardo Constantino Ginestal, Hospital Clínico San Carlos, Spain
Copyright © 2019 Chamard Witkowski, Mallet, Bélanger, Marrero and Handrigan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ludivine Chamard Witkowski, ludivine_chamard@hotmail.com