 Håkon Ihle-Hansen
Håkon Ihle-Hansen Hege Ihle-Hansen
Hege Ihle-Hansen Else Charlotte Sandset
Else Charlotte Sandset Guri Hagberg1,2
Guri Hagberg1,2- 1Department of Medicine, Bærum Hospital- Vestre Viken Hospital Trust, Drammen, Norway
- 2Oslo Stroke Unit, Department of Neurology, Oslo University Hospital, Ullevål, Norway
Carotid artery atherosclerosis, the result of a multitude of vascular risk factors, is a promising marker for use in risk stratification. Recent evidence suggests that carotid artery atherosclerosis affects cognitive function and is an independent risk factor for the development of cognitive impairment. Both atherosclerosis and cognitive impairment develop over a prolonged period (years), and due to the aging population, markers to identify persons at risk are needed. Carotid artery atherosclerosis can easily be visualized using non-invasive ultrasound, potentially enabling early and intensified risk factor management to preserve cognitive function or delay further decline. However, the burden of atherosclerosis and temporal exposure required to pose a risk of cognitive impairment is unclear. This mini-review aims to explore the available evidence on the association between carotid atherosclerosis and cognition, and furthermore identify the remaining gaps in knowledge.
Introduction
The prevention of cognitive impairment is one of the most significant challenges of our time with up to 10 million new cases each year (1). The consequences of underlying vascular risk factors such as hypertension increase the risk of both atherosclerosis and cognitive impairment. Monitoring and treating vascular risk factors mid-life is a promising strategy to prevent dementia later in life (2). Furthermore, the burden of atherosclerosis correlates to the underlying burden of vascular risk factors (3) and can be viewed as a surrogate marker of total vascular risk.
Vascular risk factors including atherosclerosis seem to contribute not only to vascular cognitive impairment, but also in the pathophysiology of Alzheimers disease (4). It has been proposed that there may be a convergence of mechanisms in vascular and neurodegenerative processes that cause impairments of cognition. These mechanisms are not yet fully elucidated, but most likely mediated through small vessel disease, endothelial dysfunction, silent ischemia, and reduced cerebral blood flow, which precedes neurodegeneration and amyloid accumulation (5).
Atherosclerosis represents a systemic multifactorial and inflammatory disease affecting the vascular bed (6). It develops gradually over years, first as a thickening of the vessel wall‘s innermost layer - the intima (7), this can either abate or progress into an atherosclerotic plaque and a vascular stenosis (8). Several studies have shown an independent association between atherosclerosis and increased risk of cognitive impairment (9, 10). Predilection sites for atherosclerosis are large and medium-sized arteries as well as areas where laminar blood flow is disturbed.
The carotid artery is ideally placed for ultrasound examination and assessment of atherosclerosis. Different types of angiography examinations are available but either demand more resources or are associated with radiation exposure, leaving ultrasound best suited for screening purposes. Atherosclerosis in the carotid arteries correlates with the presence of atherosclerosis in other vessels (11). Definitions of subclinical atherosclerotic disease in various studies include increased intima-media thickness (IMT), atherosclerotic plaques, and asymptomatic stenosis. Assessment of subclinical carotid artery atherosclerosis holds promise as a marker to identify persons at risk and those who may benefit from intensified risk factor management to prevent further progression of atherosclerosis and cognitive decline.
Symptomatic atherosclerosis in pre- and intra- cerebral vessels increases the risk of brain damage with an associated increased risk of cognitive impairment (12). However, the link between subclinical atherosclerosis (meaning nearly or completely asymptomatic) and cognitive function in stroke-free subjects is not as clear, the available evidence is mainly from large population-based cohort studies.
In this mini-review, focusing on subclinical atherosclerosis located in the carotid arteries, we aim to explore the currently available evidence on the association between carotid atherosclerosis and cognition. Furthermore, evaluate any potential progressive relationships, and identify the remaining gaps in knowledge.
Subclinical Carotid Atherosclerosis and Cognition
Several large population studies have assessed the association between atherosclerosis and cognitive function, 20,000 with cross sectional design and 50,000 with a longitudinal design with long term follow-up (up 20 years) between initial assessment of atherosclerosis and outcome, i.e., worsening in cognitive performance or dementia (13). The studies included in our mini-review are described in detail in Table 1.
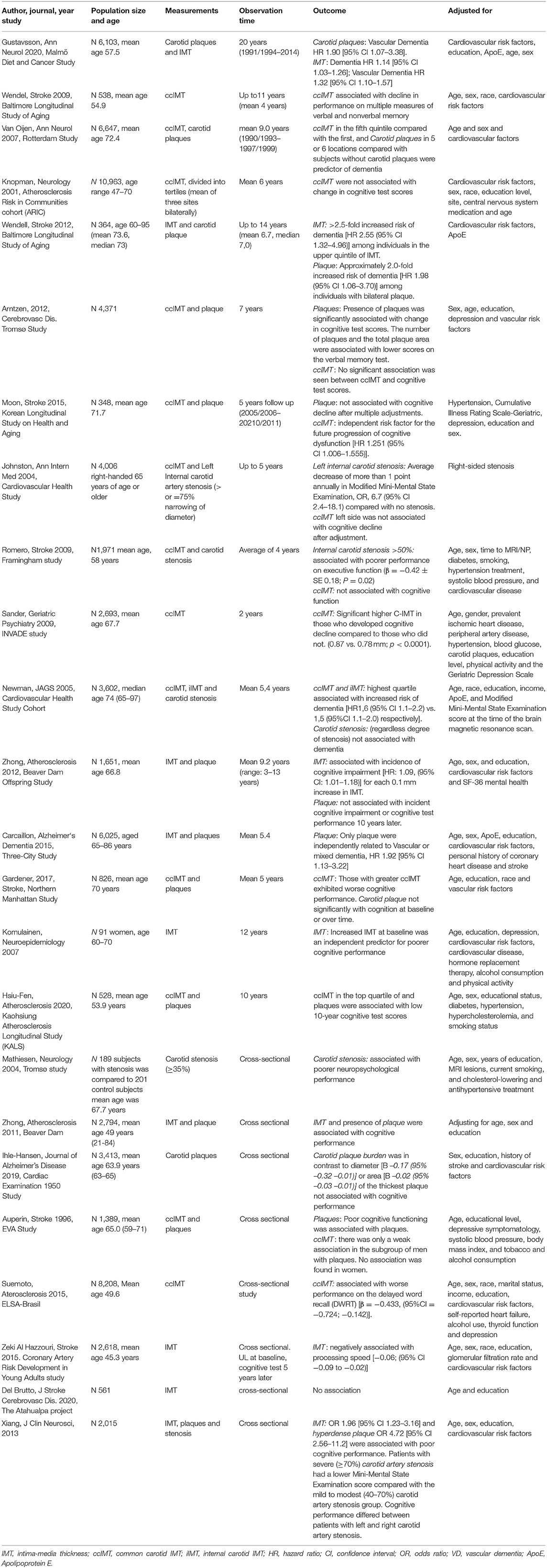
Table 1. Excerpts from relevant populations-based studies.
Association between subclinical atherosclerosis and cognitive performance in subjects free of known cognitive impairment was explored in 8 studies with a cross sectional design (14–21). Seven cross-sectional studies have found an association between markers of atherosclerosis and cognitive function (14–16, 18–21).
Four studies found an association between greater IMT and reduced performance in some specific cognitive domains (14, 16, 18, 22). The majority of studies included subjects with more advanced atherosclerosis, i.e., plaque, plaque burden, and stenosis (14–16, 20, 21), supporting the notion of an inverse association between increasing atherosclerotic burden and cognitive function.
Nine studies including a total of 23,000 patients showed associations between higher IMT and deterioration of cognitive performance over time (9, 13, 23–30). On the other hand, the level of IMT was not associated with decreased cognitive performance in five studies including in total 27,000 patients (10, 31–34).
The location of the IMT measurement may be of importance. In the Framingham study, greater IMT in the internal carotid artery was associated with impaired cognitive function. However, no such association was found when assessing the common carotid intima-media thickness (ccIMT) and cognitive impairment (32).
Further, eight studies reported associations between carotid plaque/stenosis and decreasing cognitive performance and cognitive impairment in long-time follow-up (10, 13, 27, 30–33, 35), and four studies showed that plaque/stenosis was superior to IMT at predicting cognitive decline (10, 31–33).
Discussion
There is a significant association between different subclinical atherosclerosis measures and cognition in large population studies, both in studies with cross-sectional design and in longitudinal studies showing progressive changes over time.
The current evidence suggests a stronger association between cognitive impairment and more pronounced subclinical atherosclerosis. In the Cardiovascular Health Study and the Framingham study, asymptomatic ≥50% carotid artery stenosis (conventionally defined as significant atherosclerosis) predicted poorer cognitive performance (10, 32). Both studies failed to find an association between ccIMT and cognition.
Some studies reported no association between continuous measures of IMT and cognitive function, while as a dichotomized variables were significant (35). While increased IMT may represent non-atherosclerotic age-associated changes in the vessel wall, vessel wall tension, or an adaptive response to changes in flow, it is believed that IMT in the upper reference range is less likely to reflect these non-atherosclerotic processes.
Whether the location of atherosclerosis is relevant is still unclear. In the Framingham study, they found that IMT in the internal carotid artery (ICA), in contrast to ccIMT, was more associated with cognitive impairment (32). Atherosclerosis develops earlier in vessel bifurcations and origins such as the carotid bulb and proximal ICA which could explain associations between IMT and cognitive impairment in ICA, but not common carotid artery. However, atherosclerosis (including increased IMT) in other locations than the carotid arteries have also been associated with reduced cognition, supporting the hypothesis that atherosclerosis is a systemic disease of the vascular bed (36).
The exact pathophysiological mechanisms of atherosclerosis-induced cognitive impairment have not yet been identified. Population-based studies do not have the ideal design to illicit an answer and mechanisms may include cerebral changes resulting from silent embolization, inflammation or hypoperfusion (2, 37, 38). Increased arterial stiffness leads to increased pulse-wave velocity,pulsatile pressure and flow in the small vessels (2, 39), and a potential failure in the blood-brain barrier. Since the pathological mechanisms remain unknown, the possibility of reverse causality or that atherosclerosis and cognitive impairment develop in parallel cannot with certainty be excluded. A major limitation of the available evidence is the absence of a universal understanding of how to define and assess subclinical atherosclerosis. Measurement of increased IMT, which is thought to represent the first structural change in the atherosclerotic process, is affected by the exact timing of measurement (varies throughout a cardiac cycle), the location of measurement, and the software algorithm used. Carotid plaques which are more strongly associated with traditional cardiovascular risk factors (3) and proven to be a better predictor of a future cardiovascular event, are highly age-dependent, with a lower prevalence in younger populations (3). Plaque detection rate is also affected by the resolution of the ultrasound devices. As most of the studies were conducted in the ‘90s with older ultrasound devices, an underestimation of plaque occurrence is likely. Furthermore, the definition of plaque is not consistent between the different studies.
As with the assessment of atherosclerosis, evaluation and definition of cognitive impairment lack standardization. The use of different cognitive test batteries, and the definition of cognitive impairment across studies makes it difficult to draw clear conclusions. There are conflicting findings regarding which cognitive domains that are most vulnerable to atherosclerotic carotid disease. In general, vascular cognitive impairment is typically characterized by reduced speed of information processing, complex attention, and frontal-executive functioning (40). However, it seems likely that vascular disease contributes to the cascade of neurodegeneration (2), also affecting other cognitive domains.
Future Perspectives
Despite associations between atherosclerosis and cognitive function seen in many populations, the amount of atherosclerosis required to pose a risk of cognitive impairment is unclear and is likely both age and person dependent.
Ultrasound of the carotid arteries is a cheap and non-invasive and technique to quantify atherosclerotic burden. Future studies should use standardized imaging protocols, standard definitions of atherosclerosis, and predefined outcome measures. Whether subclinical atherosclerosis poses different risk at different ages and whether different locations, and or intensifying risk factor management can contribute to halting further cognitive impairment needs further exploration.
Conclusion
Subclinical carotid artery atherosclerosis provides additional information about vascular risk factors burden in realtion to cognitive performance. More research is needed to address whether the assessment of carotid artery atherosclerosis could be used to identify people at increased risk of cognitive impairment and justify intensified risk factor management.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Towards a Dementia Plan: A WHO Guide. (2018). http://apps.who.int/iris/bitstream/handle/10665/272642/9789241514132-eng.pdf?ua=1 (accessed August 30, 2018).
2. Gorelick PB, Scuteri A, Black SE, DeCarli C, Greenberg SM, Iadecola C, et al. Vascular contributions to cognitive impairment and dementia a statement for healthcare professionals from the American heart association/American stroke association. Stroke. (2011) 42:2672–713. doi: 10.1161/STR.0b013e3182299496
3. Ihle-Hansen H, Vigen T, Ihle-Hansen H, Ronning OM, Berge T, Thommessen B, et al. Prevalence of carotid plaque in a 63- to 65-year-old norwegian cohort from the general population: the ACE (Akershus Cardiac Examination) 1950 study. J Am Heart Assoc. (2018) 7:e008562. doi: 10.1161/JAHA.118.008562
4. Viswanathan A, Rocca WA, Tzourio C. Vascular risk factors and dementia: how to move forward? Neurology. (2009) 72:368–74. doi: 10.1212/01.wnl.0000341271.90478.8e
5. Yew B, Nation DA. Cerebrovascular resistance: effects on cognitive decline, cortical atrophy, and progression to dementia. Brain J Neurol. (2017) 140:1987–2001. doi: 10.1093/brain/awx112
6. Stoll G, Bendszus M. Inflammation and atherosclerosis: novel insights into plaque formation and destabilization. Stroke. (2006) 37:1923–32. doi: 10.1161/01.STR.0000226901.34927.10
7. Abrams J. Clinical practice. Chronic stable angina. New Eng J Med. (2005) 352:2524–33. doi: 10.1056/NEJMcp042317
8. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. New Eng J Med. (2005) 352:1685–95. doi: 10.1056/NEJMra043430
9. Newman AB, Fitzpatrick AL, Lopez O, Jackson S, Lyketsos C, Jagust W, et al. Dementia and Alzheimer's disease incidence in relationship to cardiovascular disease in the cardiovascular health study cohort. J Am Geriatr Soc. (2005) 53:1101–7. doi: 10.1111/j.1532-5415.2005.53360.x
10. Johnston SC, O'Meara ES, Manolio TA, Lefkowitz D, O'Leary DH, Goldstein S, et al. Cognitive impairment and decline are associated with carotid artery disease in patients without clinically evident cerebrovascular disease. Ann Intern Med. (2004) 140:237–47. doi: 10.7326/0003-4819-140-4-200402170-00005
11. Craven T, Ryu J, Espeland M, Kahl F, McKinney W, Toole J, et al. Evaluation of the associations between carotid artery atherosclerosis and coronary artery stenosis. A case-control study. Circulation. (1990) 82:1230–42. doi: 10.1161/01.CIR.82.4.1230
12. Bakker FC, Klijn CJ, Jennekens-Schinkel A, Kappelle LJ. Cognitive disorders in patients with occlusive disease of the carotid artery: a systematic review of the literature. J Neurol. (2000) 247:669–76. doi: 10.1007/s004150070108
13. Gustavsson AM, van Westen D, Stomrud E, Engström G, Nägga K, Hansson O. Midlife atherosclerosis and development of Alzheimer or vascular dementia. Ann Neurol. (2020) 87:52–62. doi: 10.1002/ana.25645
14. Zhong W, Cruickshanks KJ, Huang GH, Klein BE, Klein R, Nieto FJ, et al. Carotid atherosclerosis and cognitive function in midlife: the beaver dam offspring study. Atherosclerosis. (2011) 219:330–3. doi: 10.1016/j.atherosclerosis.2011.07.013
15. Mathiesen EB, Waterloo K, Joakimsen O, Bakke SJ, Jacobsen EA, Bønaa KH. Reduced neuropsychological test performance in asymptomatic carotid stenosis: the tromsø study. Neurology. (2004) 62:695–701. doi: 10.1212/01.WNL.0000113759.80877.1F
16. Xiang J, Zhang T, Yang QW, Liu J, Chen Y, Cui M, et al. Carotid artery atherosclerosis is correlated with cognitive impairment in an elderly urban Chinese non-stroke population. J Clin Neurosci. (2013) 20:1571–5. doi: 10.1016/j.jocn.2013.02.026
17. Del Brutto OH, Mera RM, Recalde BY, Del Brutto VJ. Carotid intima-media thickness, cognitive performance and cognitive decline in stroke-free middle-aged and older adults. The atahualpa project. J Stroke And Cerebrovasc Dis. (2020) 29:104576. doi: 10.1016/j.jstrokecerebrovasdis.2019.104576
18. Zeki Al Hazzouri A, Vittinghoff E, Sidney S, Reis JP, Jacobs DR >Jr, et al. Intima-media thickness and cognitive function in stroke-free middle-aged adults: findings from the coronary artery risk development in young adults study. Stroke. (2015) 46:2190–6. doi: 10.1161/STROKEAHA.115.008994
19. Suemoto CK Santos IS Bittencourt MS Pereira AC Goulart AC Rundek T . Subclinical carotid artery atherosclerosis and performance on cognitive tests in middle-aged adults: Baseline results from the ELSA-Brasil. Atherosclerosis. (2015) 243:510–5. doi: 10.1016/j.atherosclerosis.2015.10.008
20. Auperin A, Berr C, Bonithon-Kopp C, Touboul PJ, Ruelland I, Ducimetiere P, et al. Ultrasonographic assessment of carotid wall characteristics and cognitive functions in a community sample of 59- to 71-year-olds. The EVA Study Group. Stroke. (1996) 27:1290–5. doi: 10.1161/01.STR.27.8.1290
21. Ihle-Hansen H, Vigen T, Berge T, Hagberg G, Engedal K, Ronning OM, et al. Carotid atherosclerosis and cognitive function in a general population aged 63-65 years: data from the akershus cardiac examination (ACE) 1950 study. J Alzheimers Dis. (2019) 70:1041–9. doi: 10.3233/JAD-190327
22. Suemoto CK, Nitrini R, Grinberg LT, Ferretti RE, Farfel JM, Leite RE, et al. Atherosclerosis and dementia: a cross-sectional study with pathological analysis of the carotid arteries. Stroke. (2011) 42:3614–5. doi: 10.1161/STROKEAHA.111.628156
23. Wendell CR, Zonderman AB, Metter EJ, Najjar SS, Waldstein SR. Carotid intimal medial thickness predicts cognitive decline among adults without clinical vascular disease. Stroke. (2009) 40:3180–5. doi: 10.1161/STROKEAHA.109.557280
24. Gardener H, Caunca MR, Dong C, Cheung YK, Elkind MSV, Sacco RL, et al. Ultrasound markers of carotid atherosclerosis and cognition: the northern manhattan study. Stroke. (2017) 48:1855–61. doi: 10.1161/STROKEAHA.117.016921
25. Zhong W, Cruickshanks KJ, Schubert CR, Acher CW, Carlsson CM, Klein BE, et al. Carotid atherosclerosis and 10-year changes in cognitive function. Atherosclerosis. (2012) 224:506–10. doi: 10.1016/j.atherosclerosis.2012.07.024
26. Moon JH, Lim S, Han JW, Kim KM, Choi SH, Park KS, et al. Carotid intima-media thickness is associated with the progression of cognitive impairment in older adults. Stroke. (2015) 46:1024–30. doi: 10.1161/STROKEAHA.114.008170
27. van Oijen M, de Jong FJ, Witteman JC, Hofman A, Koudstaal PJ, Breteler MM. Atherosclerosis and risk for dementia. Ann Neurol. (2007) 61:403–10. doi: 10.1002/ana.21073
28. Sander K, Bickel H, Förstl H, Etgen T, Briesenick C, Poppert H, et al. Carotid- intima media thickness is independently associated with cognitive decline. The INVADE study. Int J Geriatr Psychiatry. (2010) 25:389–94. doi: 10.1002/gps.2351
29. Komulainen P, Kivipelto M, Lakka TA, Hassinen M, Helkala EL, Patja K, et al. Carotid intima-media thickness and cognitive function in elderly women: a population-based study. Neuroepidemiology. (2007) 28:207–13. doi: 10.1159/000108112
30. Lin HF, Huang LC, Chen CK, Juo SH, Chen CS. Carotid atherosclerosis among middle-aged individuals predicts cognition: a 10-year follow-up study. Atherosclerosis. (2020) 314:27–32. doi: 10.1016/j.atherosclerosis.2020.10.015
31. Carcaillon L, Plichart M, Zureik M, Rouaud O, Majed B, Ritchie K, et al. Carotid plaque as a predictor of dementia in older adults: the three-city study. Alzheimers Dement. (2015) 11:239–48. doi: 10.1016/j.jalz.2014.07.160
32. Romero JR, Beiser A, Seshadri S, Benjamin EJ, Polak JF, Vasan RS, et al. Carotid artery atherosclerosis, MRI indices of brain ischemia, aging, and cognitive impairment: the Framingham study. Stroke. (2009) 40:1590–6. doi: 10.1161/STROKEAHA.108.535245
33. Arntzen KA, Schirmer H, Johnsen SH, Wilsgaard T, Mathiesen EB. Carotid atherosclerosis predicts lower cognitive test results: a 7-year follow-up study of 4,371 stroke-free subjects - the Tromso study. Cerebrovasc Dis. (2012) 33:159–65. doi: 10.1159/000334182
34. Knopman D, Boland LL, Mosley T, Howard G, Liao D, Szklo M, et al. Cardiovascular risk factors and cognitive decline in middle-aged adults. Neurology. (2001) 56:42–8. doi: 10.1212/WNL.56.1.42
35. Wendell CR, Waldstein SR, Ferrucci L, O'Brien RJ, Strait JB, Zonderman AB. Carotid atherosclerosis and prospective risk of dementia. Stroke. (2012) 43:3319–24. doi: 10.1161/STROKEAHA.112.672527
36. Rossetti HC, Weiner M, Hynan LS, Cullum CM, Khera A, Lacritz LH. Subclinical atherosclerosis and subsequent cognitive function. Atherosclerosis. (2015) 241:36–41. doi: 10.1016/j.atherosclerosis.2015.04.813
37. Poggesi A, Pasi M, Pescini F, Pantoni L, Inzitari D. Circulating biologic markers of endothelial dysfunction in cerebral small vessel disease: a review. J Cerebr Blood Flow Metab. (2016) 36:72–94. doi: 10.1038/jcbfm.2015.116
38. de la Torre JC. Is Alzheimer's disease a neurodegenerative or a vascular disorder? Data, dogma, and dialectics. Lancet Neurol. (2004) 3:184–90. doi: 10.1016/S1474-4422(04)00683-0
39. O'Rourke MF, Safar ME. Relationship between aortic stiffening and microvascular disease in brain and kidney: cause and logic of therapy. Hypertension. (2005) 46:200–4. doi: 10.1161/01.HYP.0000168052.00426.65
40. World Health Organization. International Classification of Diseases for Mortality and Morbidity Statistics (11th Revision) (2018). Available online at: https://icd.who.int/browse11/l-m/en (accessed April 24, 2021).
Keywords: IMT, cognitive function, dementia, plaque, carotid artery atherosclerosis
Citation: Ihle-Hansen H, Ihle-Hansen H, Sandset EC and Hagberg G (2021) Subclinical Carotid Artery Atherosclerosis and Cognitive Function: A Mini-Review. Front. Neurol. 12:705043. doi: 10.3389/fneur.2021.705043
Received: 04 May 2021; Accepted: 30 June 2021;
Published: 28 July 2021.
Edited by:
Mirjam R. Heldner, University Hospital Bern, SwitzerlandReviewed by:
Marina Sorrentino Hernandes, Emory University, United StatesTheodoros Karapanayiotides, Aristotle University of Thessaloniki, Greece
Copyright © 2021 Ihle-Hansen, Ihle-Hansen, Sandset and Hagberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Håkon Ihle-Hansen, haaihl@vestreviken.no