 Rachana Gangwani
Rachana Gangwani Amelia Cain
Amelia Cain Amy Collins1
Amy Collins1 Jessica M. Cassidy
Jessica M. Cassidy- 1Department of Allied Health Sciences, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
- 2Human Movement Sciences Curriculum, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
The International Classification of Functioning, Disability and Health framework recognizes that an individual's functioning post-stroke reflects an interaction between their health condition and contextual factors encompassing personal and environmental factors. Personal factors significantly impact rehabilitation outcomes as they determine how an individual evaluates their situation and copes with their condition in daily life. A key personal factor is self-efficacy—an individual's belief in their capacity to achieve certain outcomes. Self-efficacy influences an individual's motivational state to execute behaviors necessary for achieving desired rehabilitation outcomes. Stroke rehabilitation practice and research now acknowledge self-efficacy and motivation as critical elements in post-stroke recovery, and increasing evidence highlights their contributions to motor (re)learning. Given the informative value of neuroimaging-based biomarkers in stroke, elucidating the neurological underpinnings of self-efficacy and motivation may optimize post-stroke recovery. In this review, we examine the role of self-efficacy and motivation in stroke rehabilitation and recovery, identify potential neural substrates underlying these factors from current neuroimaging literature, and discuss how leveraging these factors and their associated neural substrates has the potential to advance the field of stroke rehabilitation.
Introduction
Stroke is a heterogeneous condition resulting in profound and wide-ranging effects on physical, psychological, and social aspects of an individual's life (1, 2). Neurorehabilitation is an important component in an individual's recovery post-stroke (3). The World Health Organization (WHO) International Classification of Functioning, Disability and Health (ICF) model is a universally recognized framework for health and disability (4) that delineates various levels of disability in stroke, including impairments, activity limitations, and participation restrictions (5). Rehabilitation therapists and clinicians utilize this framework to guide evaluation, treatment strategies, and goal-setting post-stroke (6).
Early stroke rehabilitation practice primarily focuses on recovery of impairments in the body structure and function domain of the ICF to optimize physical functioning. Such an approach is frequently based on motor learning principles of providing intensive, progressive, and task-specific interventions to improve physical function and capacity (i.e., what a person can do in a standardized, controlled environment post-stroke) (7, 8). However, improvement in physical capacity does not translate to improvement in physical performance (i.e., what a person actually does in his or her daily environment) (9). This suggests that improvement in the body structure and function domain may not necessarily translate to improvement in social participation or reintegration into pre-stroke life roles. Expanding the focus of post-stroke rehabilitation beyond the domain of body structure and function may therefore promote more meaningful outcomes that translate to real-world participation.
A relevant feature in the ICF model is the inclusion of contextual factors, including environmental and personal factors (10). The latter refers to factors that are not a part of an individual's health condition or health state. Personal factors include gender, age, co-morbidities, socioeconomic status, education, and behavioral characteristics such as self-efficacy and motivation (11). These personal factors relate to performance and participation outside of the clinical environment (12). Self-efficacy relates to “beliefs in one's capabilities to organize and execute courses of action required to produce given attainments” (13). Individuals with high self-efficacy post-stroke typically have greater confidence to participate in activities of daily living (ADLs), higher ability to overcome barriers in their recovery, and typically possess greater psychosocial functioning and well-being compared to those with low self-efficacy (14, 15). As recent work indicates baseline ADL function as an important prognostic factor of functional independence during early post-stroke recovery (16), self-efficacy also contributes to post-stroke recovery and rehabilitation outcomes. Closely related to self-efficacy is motivation, which refers to an individual's will to perform a certain behavior toward achieving their goal and is one of the processes through which self-efficacy affects human functioning and impacts post-stroke rehabilitation outcomes (17). An individual's level of self-efficacy influences their motivation as exemplified in the following ways: determination of goals that individuals set for themselves, determination of effort expended by an individual in achieving their goal(s), determination of how long an individual perseveres when faced with challenges, and determination of an individual's resilience to failure (18). Given the importance of self-efficacy and motivation in goal-setting, perseverance, and resilience, these personal factors are key contributors to recovery and rehabilitation processes, including those related to stroke.
Motor learning theories such as the Dynamic Systems Theory and OPTIMAL (Optimizing Performance through Intrinsic Motivation and Attention for Learning) Theory have incorporated personal factors to explain motor (re)learning post-stroke (19, 20), whereby the optimization of learning and recovery depend on an individual's level of self-efficacy and motivation. Interventions aimed at enhancing these personal factors have demonstrated a reduction in functional decline 3–12 months post-stroke (21), significant improvement in rehabilitation outcomes including the Reintegration to Normal Living Index and Activities-specific Balance Confidence (ABC) Scale (22), and significant functional recovery at 6 months post-stroke (23). Further, such interventions in individuals with chronic conditions, including stroke, demonstrated lasting improvement in coping strategies including symptom management, increased physical activity, less fatigue, and fewer hospital visits due to secondary complications (24).
The assessment of self-efficacy and motivation primarily entails self-report scales and questionnaires, which introduce limitations related to response bias and subjectivity with scoring (25, 26). Brain-based measures acquired through neuroimaging may provide greater objectivity. Past research examining neuroimaging-based biomarkers of stroke recovery have shown the utility of these measurements in describing post-stroke injury and behavioral status as well as predictive value in post-stroke recovery and treatment response (27–29). Expanding biomarker development to elucidate neural substrates subserving self-efficacy and motivation may hold important clinical implications. Identifying neural correlates of self-efficacy and motivation, for instance, may provide information beyond what conventional measures alone convey. This information may result in a more objective assessment of self-efficacy and motivation to better tailor motor (re)learning and treatment strategies. In this review, we identify potential neural substrates underlying motivation, self-efficacy, and constructs of self-efficacy such as self-agency from current neuroimaging literature, and discuss how leveraging these factors and their associated neural substrates has the potential to advance the field of stroke rehabilitation.
There are a number of systematic reviews on self-efficacy and motivation in stroke focusing on the role of these factors in stroke rehabilitation outcomes (30–32) and their implementation in treatment and intervention strategies (30, 33). Findings from these systematic reviews have demonstrated significant associations between self-efficacy and post-stroke outcomes such as quality of life, activities of daily living (ADLs), mobility, and depression (30, 31) and have encouraged the incorporation of these factors in rehabilitation programming (33) and medical curriculum (31). This review examines the roles of self-efficacy and motivation in stroke rehabilitation and recovery while distinguishing itself from other reviews by bridging topics of self-efficacy and motivation with neuroimaging and biomarker development.
An Overview of Self-Efficacy and Motivation
Albert Bandura's Social Cognitive Theory describes learning as a dynamic process arising from the interaction between person, environment, and behavior to explain goal-directed behavior and its maintenance across time (34, 35). Self-efficacy is an important feature of Social Cognitive Theory that refers to the control of human action through an individual's beliefs in their capabilities to produce desired outcomes by their actions (34).
Since self-efficacy impacts stroke rehabilitation (e.g., sustaining progress and coping with setbacks), understanding how self-efficacy beliefs originate is important. Self-efficacy beliefs arise from the following instances: (1) Performance mastery. Successful performance experiences raise mastery and efficacy expectations. Once established, enhanced self-efficacy tends to generalize to other situations in which performance was lacking (36). In individuals with stroke, the enhancement of self-efficacy occurs through the accomplishment of therapy goals through independent effort. (2) Vicarious experience. Observing others perform activities generates expectations in observers that they may achieve similar outcomes with persistent effort (37). (3) Verbal persuasion. Individuals believe in their ability to successfully cope with adverse experiences based on the encouragement from others, including health care professionals and family members (38). (4) Emotional arousal. An individual's emotional state influences their level of self-efficacy (38). For example, stressful situations may perpetuate emotions that negatively affects an individual's self-efficacy or their perceived ability to accomplish rehabilitation goals.
While performance mastery, vicarious experiences, verbal persuasion, and emotional arousal shape one's degree of self-efficacy, self-efficacy impacts human functioning through several psychological processes (39). (1) Cognitive processes. Individuals' self-efficacy influences the anticipatory scenarios that they mentally construct and rehearse. In rehabilitation settings, for example, individuals with high self-efficacy, visualize successful scenarios entailing positive rehabilitation outcomes, whereas those with low self-efficacy, visualize failure scenarios. In adverse situations, those with low self-efficacy tend to lower their aspirations, which negatively impacts their performance. In contrast, those with high self-efficacy, typically establish and pursue ambitious goals for themselves (40). (2) Motivational processes. Self-efficacy is key in the self-regulation of motivation (41). Individuals motivate themselves and guide their actions based on their beliefs of what they can do and set goals for themselves and plan the course of action accordingly. Thus, high self-efficacy results in greater motivation to set ambitious yet attainable rehabilitation goals along with effective planning to execute behaviors necessary to achieve those goals. (3) Affective processes. Self-efficacy is also key in anxiety arousal. Individuals with high self-efficacy typically manage anxiety and stressful conditions in a productive manner during rehabilitation; whereas, those with low self-efficacy cannot (42). (4) Selection processes. Self-efficacy influences the types of activities that individuals decide to pursue (42). Those with diminished self-efficacy actively avoid activities during rehabilitation that they believe exceed their capabilities (42). In contrast, those with heightened self-efficacy readily undertake challenging activities and select situations that they judge themselves capable of handling. A construct of self-efficacy relevant to stroke rehabilitation discussed below is self-agency, which refers to the belief that one's action is the consequence of one's intention (43). Bandura's Social Cognitive Theory describes agency as an individual's ability to control and regulate their thinking, motivation, and behavior with existing self-beliefs (i.e., self-efficacy) (43). Motivation, self-efficacy, and constructs of self-efficacy such as self-agency therefore play a central role in post-stroke recovery and rehabilitation outcomes.
Self-Efficacy and Motivation in Stroke Rehabilitation
Until recent years, stroke rehabilitation often emphasized impairment mitigation; however, evidence suggests that impairment mitigation does not necessarily translate to improved participation in daily activities or enhanced quality of life (9). Thus, it is necessary to consider and evaluate all aspects of the ICF model to develop a more thorough understanding of stroke recovery. Further, as rehabilitation outcomes depend on patients' attitudes, self-beliefs, and motivation, post-stroke outcomes are therefore contingent on an individual's ability to actively participate in the rehabilitation process. Yet, barriers to post-stroke recovery, including depression (44) and anxiety (45), may compromise an individual's level of self-efficacy and motivation thereby impacting physical capacity and participation (46) and resulting in lower engagement during rehabilitation (47). For instance, recent work by Stewart et al. (48) that examined self-efficacy for reach speed and accuracy in individuals with chronic stroke displaying mild motor impairment found self-efficacy to be a significant predictor of affected arm reaching performance (48). Complimenting these findings is work showing a significant positive association between individuals' level of motivation at the start of inpatient post-stroke rehabilitation and level of independence with ADLs at the end of rehabilitation as measured by the Functional Independent Measurement scale (49). In addition to engagement in the rehabilitation process, low self-efficacy and motivation may also negatively influence treatment adherence (50, 51). Work by Caetano et al. (52) revealed that self-efficacy for walking, along with walking ability, explained 80% of the variance in exercise adherence in individuals post-stroke (52). As these collective findings imply, self-efficacy and motivation influence rehabilitation outcomes, and this likely occurs through several routes. First, as a primary focus of stroke rehabilitation is to facilitate an individual's volitional movement, a patient's motivation and self-efficacy beliefs influence their motor behavior (20). High self-efficacy and motivation enhance future expectations and generate autonomy, which may translate to individuals setting ambitious rehabilitation goals and a stronger commitment to achieve those goals (20). Second, self-efficacy and motivation influence the perceived demand related to task performance, which may further impact an individual's task preparation during rehabilitation (53). Individuals with high self-efficacy and motivation thus focus more on achievable elements of the task and less on potential shortcomings. Third, enhanced expectations arising from high self-efficacy positively impact cognitive processes such as working memory and attention (54), which are imperative for effective (re)learning following stroke. Lastly, enhanced expectations are related to increased dopaminergic mediation, which modulates motivation to guide future behavior (55). Thus, self-efficacy and motivation can enhance post-stroke rehabilitation outcomes and participation by influencing various motivational, cognitive and physiological aspects to ensure that goals are effectively coupled with desired actions in real-life.
Self-efficacy and motivation are also incorporated in self-management and home-based rehabilitation programs to promote long-term behavioral change and its maintenance over time following inpatient hospitalization (56). Post-stroke self-management programs led by therapists incorporating self-efficacy and motivation factors focus on goal-setting and empowering individuals with information, support and resources to facilitate post-acute care transition and symptom management (15, 57, 58). Such self-management strategies have resulted in improved confidence in recovery, better long-term health outcomes, and a reduction in post-stroke complications (33, 59, 60) as evidenced by increased physical activity, improved self-reported mobility and fine motor-skill performance, and elevated balance confidence (61, 62). The recent Taking Charge after Stroke (TaCAS) study examined a novel self-management program in community dwelling individuals within 16 weeks post-stroke (63). As a departure from the SMART (Specific, Measurable, Achievable, Realistic/relevant, and Timed) approach, the Take Charge intervention instead incorporated elements of Self-Determination Theory (64) by fostering autonomy, confidence, and purpose. Participants explored and discussed important aspects of their lives, including people, along with priorities that they hoped to address over the next 12 months. Compared to control participants that received written stroke education, individuals completing the Take Charge intervention demonstrated significantly higher quality of life scores (Short Form 36 Physical Component Summary, SF-36) and significantly lower odds of dependency (modified Rankin scale 3–5) at 12 months post-stroke. A notable finding of the TaCAS study was a significant dose effect with higher quality of life scores observed with an additional Take Charge session (63).
Other interventions incorporating self-efficacy and motivation factors delivered by rehabilitation therapists include individualized coaching (65) and cognitive strategy training (66). Individualized coaching is a patient-centered process that aims to facilitate and empower the individual to achieve self-determined goals related to their health and wellness (67). In individuals with stroke, personalized coaching involving goal-setting, monitoring of goals, and motivation counseling resulted in improved physical activity behavior and participation as measured by the number of weekly exercise sessions, intensity and duration of exercise, and step count at 1 year post-stroke (68). Similarly, cognitive strategy training incorporates an integrated approach from behavioral and cognitive psychology fields. Here, a therapist guides the patient in goal-setting and facilitates skill acquisition through a guided recovery process where the patient (learner) identifies a problem and uses feedback and guidance from the therapist to generate potential solutions (69). Such training enhanced patients' self-monitoring capabilities and problem-solving skills that led to successful rehabilitation outcomes (70–72). Rehabilitation approaches and strategies integrating concepts of self-efficacy and motivation therefore have the potential to optimize post-stroke recovery outcomes through enhanced patient autonomy and participation during the recovery process.
Assessment of Self-Efficacy and Motivation
Measurement of self-efficacy typically occurs through self-reports and questionnaires whereby individuals rate their degree of confidence in performing a specific task (73). One measure of self-efficacy, referred to as self-efficacy magnitude, is determined by summing the total positive or yes responses from an individual wherein a greater number of positive responses implies greater self-efficacy (73). Another measure, self-efficacy strength, is determined by summing the confidence ratings across all performance levels with higher scores representing greater confidence levels (74). For example, the General Self-Efficacy Scale (GSES) (75) is a 10-item psychometric scale that rates an individual's level of self-efficacy based on their self-beliefs of meeting task demands in a broad array of contexts. Responses utilize a 4-point Likert Scale with scores ranging between 10 and 40 (higher scores suggest higher self-efficacy). Similarly, several subjective patient-based measures of motivation exist (25, 76). However, these scales demonstrate limited reliability and validity with notable methodological limitations (77). The overall subjective nature of self-efficacy and motivation questionnaires therefore likely limits their widespread use in rehabilitation. Establishing greater objectivity in the assessment of self-efficacy and motivation would benefit both research and clinical settings by providing a more holistic understanding of the individual.
Neuroimaging and Biomarker Development
The application of structural and functional neuroimaging in stroke rehabilitation propelled the development of biomarkers or measurements reflecting underlying cellular and molecular events associated with clinical status and/or evolution (27). Stroke recovery biomarkers have the potential to enhance the accuracy of post-stroke recovery and treatment response prediction (27). For instance, structural neuroimaging measures derived from magnetic resonance imaging (MRI), diffusion tensor imaging (DTI), and transcranial magnetic stimulation that convey corticospinal tract integrity have informed motor recovery and treatment outcomes in stroke (78–80). Similarly, functional neuroimaging measures reflecting cortical oscillatory activity and functional connectivity as measured by electroencephalography, magnetoencephalography, and functional MRI, respectively, have also demonstrated similar associations with post-stroke recovery of motor (81), somatosensory (82), language (83), and cognitive function (84). Collectively, these measurements of brain structure and physiological function have provided a more comprehensive understanding of stroke recovery. Additionally, evidence also suggests greater prediction accuracy with the use of neuroimaging biomarkers in conjunction with clinical outcome measures vs. clinical outcome measures alone (85). While the emphasis of these neuroimaging measures has encompassed mostly improvement and recovery of impairment and function, the utility of these measures may also apply to the assessment of personal factors such as self-efficacy and motivation. The identification of pertinent neural correlates (i.e., relevant neural structures and connections) of self-efficacy and motivation may enhance the accuracy of existing post-stroke recovery prediction models.
Neural Correlates of Self-Efficacy
There is a limited but growing body of literature utilizing neuroimaging to identify potential neurological correlates of self-efficacy and its constructs such as self-agency (Table 1). Most studies in existence predominantly involve young adults with no significant neurological history. One of the largest studies to date conducted by Nakagawa et al. (91) involved 1,204 young adults (91). Using a combination of MRI and DTI measures, the investigators determined that higher general self-efficacy scores related to lower mean diffusivity (higher neuronal density) from the lenticular nucleus (putamen and globus pallidus). These findings compliment previous work demonstrating contributions from the putamen to motor control and skill acquisition (93, 94). Previous research findings have also shown that putamen volume positively correlates with perceptual-motor performance and that functional connections between the sensorimotor cortex and the posterior putamen strengthen in parallel with learning (95). Collectively, these findings substantiate the contributions of the putamen in both motor learning and self-efficacy processes. The findings by Nakagawa et al. (91) also align with work illustrating contributions from the globus pallidus in the development and control of learning in humans (96). The corticostriatal loop connects cortical motor planning regions with subcortical structures, including the thalamus, putamen, and globus pallidus to efficiently execute and control motor behavior (97). Together, these findings underscore the importance and relevance of the lenticular nucleus as a neural substrate of both self-efficacy and motor learning and control.
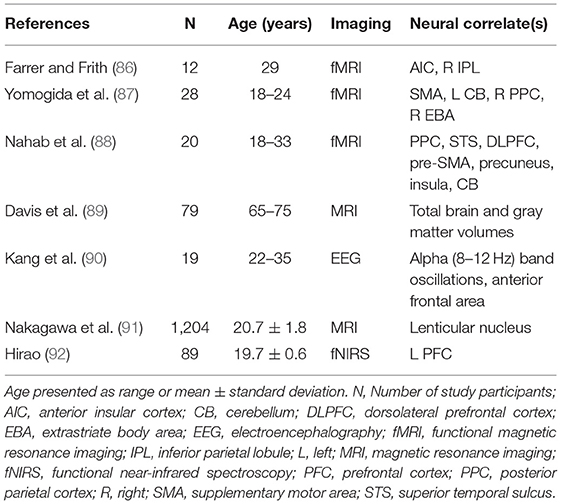
Table 1. Neural correlates of self-efficacy identified in healthy individuals.
In addition to subcortical structures, Hirao (92) also identified the prefrontal cortex as a crucial region of self-efficacy. Using functional near-infrared spectroscopy (fNIRS), they compared changes in prefrontal activation during a verbal fluency task across 89 healthy young adults previously categorized into low, moderate, and high self-efficacy groups. Investigators found significantly less left prefrontal activation in the low self-efficacy group as compared to the moderate self-efficacy group, which infers potential involvement of prefrontal cortical activity in self-efficacy. These findings supplement past work showing contributions from prefrontal cortex in self-regulation or behaviors that result in the fulfillment of one's intended goals (98, 99). Combined, these findings suggest the importance of prefrontal cortex in both self-efficacy and self-regulation in goal-directed behavior. Future investigation is necessary to determine how these findings translate to the rehabilitation environment where outcomes depend on the consistency of goal-directed behavior. In a study in 79 community-dwelling older women, Davis et al. (89) specifically assessed self-efficacy related to falls using the ABC Scale and found that falls self-efficacy positively correlated with both total brain and gray matter volumes. These findings resonate with previous findings that found that increased risk of falls in those with advancing age occurs in part due to decreases in brain volume and reduced cognition (100). Given the occurrence of falls post-stroke and the impact of stroke on brain volume (101), determining the predictive value of total brain volume on falls self-efficacy may be an effective future research direction.
While the aforementioned studies focus on neural correlates of self-efficacy, several studies of young adults with no neurological conditions (86–88, 90) have also examined neural correlates of self-agency. As previously defined, self-agency is a construct of self-efficacy that refers to an individual's ability to influence their own functioning by regulating their thinking, motivation, and behavior with existing self-beliefs to achieve desired outcomes (43). Work employing functional MRI (fMRI), identified several cortical regions and neural structures associated with self-agency (86–88): anterior insula and the right inferior parietal lobule, posterior parietal cortex (PPC), superior temporal sulcus (STS), dorsolateral prefrontal cortex (DLPFC), pre-supplementary motor area (pre-SMA), precuneus, insula, cerebellum, supplementary motor area (SMA), right posterior parietal cortex (PPC), and right extra striate body area (EBA). Relatedly, a meta-analysis encompassing 15 fMRI studies across 228 study participants identified activation of the insula as a neural correlate of self-agency (102).
As expected, several regions associated with self-efficacy also relate to self-agency, and these regions, in turn, contribute to motor system function (ventral premotor cortex, SMA, pre-SMA, and cerebellum) and to cognition and information processing (DLPFC, PPC, and insula) (103). The anterior insula, for instance, shares connections with sub-regions of the prefrontal cortex, such as the dorsolateral and ventromedial prefrontal cortices, that control attention and working memory (104). These cognitive processes are imperative for motor relearning post-stroke and impact subsequent rehabilitation outcomes (105). Similarly, recent neurophysiological and neuroimaging evidence acknowledges the involvement of PPC and premotor regions in internal monitoring of self- and externally-generated movements (106), which are essential components in relearning and regaining movement post-stroke. Additional studies are needed to provide a definitive understanding of how neural structures concomitantly involved in self-agency and motor and cognitive processing influence post-stroke rehabilitation outcomes.
Apart from the anatomical structures associated with self-agency, EEG work involving a virtual reality motor paradigm in a healthy cohort highlighted neural oscillatory activity in the alpha (8–12 Hz) band (90). Decreases in relative alpha power, specifically overlying central, bilateral parietal, and right temporal areas, related to greater self-agency. Additionally, significant decrease in alpha coherence (connectivity) involving regions overlying anterior frontal cortex negatively correlated with self-agency. Past work demonstrating the involvement of neural oscillations in the alpha frequency band in stroke recovery (107, 108) encourage additional work to validate these findings in a stroke cohort.
Neural Correlates of Motivation
Akin to the self-efficacy literature, most studies examining neural correlates of motivation involve fMRI in healthy adults (Table 2). Given the close relationship between self-efficacy and motivation, many of the anatomical regions previously reported above have also been identified in studies of motivation. In 161 young adults (19–24 years of age), Lee and Reeve (110) found that greater anterior insular cortex activation related to greater motivation (110), which aligns with other work highlighting greater interactions between anterior insular cortex and striatum associated with greater motivation (109, 114). Together, these findings substantiate past research showing contributions from the ventral and dorsal anterior insula to an individual's motivational state with the latter region specifically contributing to the updating of motivational states according to associated goal-directed actions (116). Other regions identified by fMRI include prefrontal, sensorimotor, middle cingulate, and visual cortices (111, 112, 115) along with nucleus accumbens and precuneous (112), with greater recruitment of these regions associated with greater motivation. Interestingly, in an effort to establish a causal link between motivation and frontopolar (FPC) cortex, Soutschek et al. (117) stimulated FPC with transcranial direct current stimulation (tDCS) in 141 healthy adults (117). Facilitation of this region with anodal tDCS increased participant motivation to put forth additional effort necessary to obtain a reward. This is consistent with prior work highlighting the FPC in goal-directed behavior (118). Determining how these findings extrapolate to neurorehabilitation is a necessary next step.
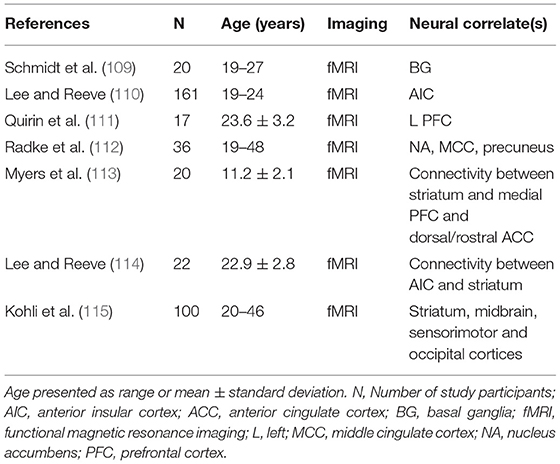
Table 2. Neural correlates of motivation identified in healthy individuals.
Emerging work in pediatric neuroimaging has also identified potential key regions associated with motivation particularly related to grit and growth mindset (113). The former refers to the long-term perseverance toward a goal and the latter refers to the belief that effort improves talent. The investigators found that grit positively correlated with ventral striatal networks including structural connectivity to medial prefrontal and rostral anterior cingulate cortices, implicated in perseverance and reward. Participants' growth mindset positively correlated with dorsal striatal structural connectivity (113). These findings pose significant implications in neurorehabilitation. Grit and growth mindset are essential to conditions with long-term recovery trajectories involving motor (re)learning, and identifying structural connections that subserve these constructs may spur the development of targeted therapeutic approaches.
Discussion
This review serves as a point of integration for self-efficacy and motivation literature, stroke rehabilitation, and neuroimaging. There exists an extensive array of evidence in the literature highlighting the influence of self-efficacy and motivation on post-stroke rehabilitation outcomes, including individuals' engagement and adherence to rehabilitation. Limitations in current self-efficacy and motivation assessment methods, combined with recent application of neuroimaging-based biomarkers in stroke, prompted a review of the neuroimaging literature to identify potential neural substrates underlying motivation and self-efficacy. This particular objective distinguishes this review from others. Research findings utilizing fMRI, fNIRS, and EEG revealed several pertinent anatomical structures and regions–several of which were associated with learning. Identifying ways to enhance an individual's self-efficacy and motivation has the potential to advance post-stroke rehabilitation and promote lasting behavioral change (119). Ascertaining neural substrates subserving these personal factors may benefit this effort.
An increasing number of clinical research studies in stroke rehabilitation recognize the value of patient-centered measures, reporting interactions between self-efficacy, participation, capacity (120, 121). The consideration of personal factors such as self-efficacy and motivation may adjudicate the disconnect between functional improvement in rehabilitation settings and enhanced participation in the natural environment. Additionally, factors of self-efficacy and motivation also determine how an individual copes with difficult situations during rehabilitation. Greater self-efficacy and motivation positively affect an individual's ability to manage and overcome stressful conditions (18, 42). As stroke rehabilitation focuses on an individual's voluntary movement, an individual's self-beliefs and attitudes are fundamental in determining rehabilitation outcomes. Moreover, these biopsychological factors also influence long term behavior change (122) and return to work post-stroke (123). Lastly, there is growing evidence of time and dose-dependent effects of rehabilitation on functional improvement post-stroke (124–126). As discussed earlier, self-efficacy and motivation influence an individual's engagement in and adherence to rehabilitation, and these factors may therefore also impact the treatment dosage that an individual receives. Therapists and other medical professionals involved in the rehabilitation process should therefore implement strategies in their clinical practice to foster self-efficacy and motivation among their patients (127). Components of the Take Charge intervention (63) and elements from ASAP (Accelerated Skills Acquisition Program) entailing the celebration of patient effort and collaboration between therapist and patient provide additional direction (128). Such strategies are particularly imperative in the inpatient rehabilitation setting where boredom is a common sentiment reported in individuals post-stroke (129). A systematic review examining inpatient post-stroke rehabilitation experiences from 560 participants across 10 countries attributed feelings of boredom, frustration, and powerlessness, in part, to the physical environment (i.e., rehabilitation setting) (130). Individuals frequently desired more activities, stimulation, and practice opportunities both during and after their therapy sessions. Purposeful structuring of the rehabilitation environment based on the individual may also cultivate motivation and self-efficacy during this critical period of recovery in addition to the patient-therapist relationship.
In order to leverage self-efficacy and motivation to advance stroke rehabilitation, there must first be accurate tools to assess these factors. Current assessment tools involve self-reported questionnaires wherein individuals must either response in yes or no or rate themselves on a Likert Scale. Considering the subjective nature of scoring and lack of standardization of scoring ranges in these assessments, these tools may have limited reliability and validity. Furthermore, such measures might have reduced accuracy in assessing self-efficacy and motivation due to possible response bias (131). This bias may be due to participant hesitancy or the need to give socially desirable answers. To mitigate these issues, utilizing neuroimaging-based measurements in conjunction with self-reported scores may provide more accurate characterization of self-efficacy and motivation post-stroke. Evidence supporting the use of neurologic biomarkers in combination with behavioral measure (85) along with recommendations from the Stroke Recovery and Rehabilitation Roundtable (SRRR) to incorporate biomarker data into future stroke recovery research (27) encourage the expansion of biomarker development to self-efficacy and motivation assessment.
In addition to potentially enhancing the objectivity of self-efficacy and motivation assessment, neural correlates of self-efficacy and motivation may also foster a more person-centered approach in motor learning and rehabilitation. Our review of the neuroimaging literature resulted in the identification of several potentially important structures and regions that require further investigation in individuals with stroke as the literature predominantly involved young adults without significant neurological history. Future work should confirm if similar brain-behavior associations reside in individuals with stroke. Further, similar to how biomarkers may differentiate treatment “responders” from “non-responders,” neural correlates of self-efficacy and motivation may also define those with varying levels of self-efficacy and motivation. Such information may inform an individual's treatment and recovery trajectory and also guide therapists in their delivery of feedback and structuring of tasks during therapy sessions. Neural structures and connections associated with self-efficacy and motivation may also guide clinical researchers in their development of stroke recovery prediction models and interventions. Given the relevance of self-efficacy and motivation in motor learning/control and stroke rehabilitation, inclusion of these personal factors in stroke recovery prediction models may enhance predictive performance and provide additional therapeutic targets.
The majority of studies reviewed utilized MRI and fMRI technologies. While these neuroimaging techniques have been widely utilized in stroke, their lack of accessibility and portability limit their application in a stroke rehabilitation setting. Technologies such as fNIRS and EEG may prove valuable in the examination of self-efficacy and motivation in a rehabilitation setting, particularly at the bedside, while also enabling researchers to examine various neural networks and connectivity-based measurements. Given the complexity of self-efficacy and motivation, it is likely that neural correlates underlying these factors extend beyond an anatomical structure.
To promote consistency across clinical trial methodology and outcomes research in stroke, the SRRR proposed a universal battery of assessments for researchers (132). Though the current battery does not contain participation measurements or baseline measures of self-efficacy or motivation, several function- and activity-specific measurements with documented psychometric properties exist: ABC Scale (133), Falls Efficacy Scale (134), Walk-12 (135), Short Self-Efficacy for Exercise Scale (136), and the Confidence in Arm and Hand Movement Questionnaire (137). For the purposes of obtaining a baseline measurement of general self-efficacy and/or motivation specific to stroke rehabilitation, we recommend the Stroke Self-Efficacy Questionnaire (SSEQ) (138) and the Stroke Rehabilitation Motivation Scale (SRMS) (25). Briefly, the 13-item SSEQ assesses self-efficacy beliefs related to everyday tasks and self-management (e.g., bed mobility, ambulation, dressing, coping with frustrations of stroke, and exercise adherence) (138). The questionnaire possesses high internal consistency (Cronbach's alpha = 0.90) and criterion validity with the Falls Efficacy Scale (Spearman's r = 0.803, p < 0.001) (138). The 28-item SRMS, adapted from the Sports Motivation Scale (139), assesses internal and external motivation (25). Though the scale demonstrated good inter-rater reliability and internal consistency, it is important to note the small sample size (n = 18) involved in the initial testing (25). Despite previous acknowledgment regarding the limitations of current self-efficacy and motivation assessments, obtaining baseline measures of self-efficacy and/or motivation is important since these factors influence constructive behaviors, attitudes, and beliefs in post-stroke recovery. Baseline knowledge of one's self-efficacy and/or motivation may inform recovery potential and treatment and learning responses while also serving as a potential covariate in a clinical trial. Thus, assessment of self-efficacy and motivation using self-reported measures in conjunction with objective neuroimaging-based measures have implications in both stroke rehabilitation practice and research.
Conclusion
Self-efficacy and motivation are important factors in stroke recovery and rehabilitation. The therapist-patient relationship and rehabilitation setting play significant roles in nurturing self-efficacy and motivation in patients. The use of neuroimaging to identify potential neural substrates of self-efficacy and motivation will enrich our understanding of stroke recovery and rehabilitation. There is a limited but growing body of literature concerning neural substrates of self-efficacy and motivation, and this work collectively inspires additional work in clinical populations, including stroke, to generate novel research questions, experimental paradigms, and treatment targets to optimize post-stroke recovery and rehabilitation outcomes.
Author Contributions
JMC conceptualized the paper. RG, ACa, and ACo conducted literature reviews. RG wrote the paper. ACa, ACo, and JMC edited the paper. All authors have read and approved the submitted version.
Funding
This work was funded by the National Institutes of Health: R00HD091375 (JMC).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Divani AA, Majidi S, Barrett AM, Noorbaloochi S, Luft AR. Consequences of stroke in community-dwelling elderly: the health and retirement study, 1998 to 2008. Stroke. (2011) 42:1821–5. doi: 10.1161/STROKEAHA.110.607630
2. Katzan IL, Thompson NR, Uchino K, Lapin B. The most affected health domains after ischemic stroke. Neurology. (2018) 90:e1364–71. doi: 10.1212/WNL.0000000000005327
3. Dimyan MA, Cohen LG. Neuroplasticity in the context of motor rehabilitation after stroke. Nat Rev Neurol. (2011) 7:76–85. doi: 10.1038/nrneurol.2010.200
4. Lexell J, Brogårdh C. The use of ICF in the neurorehabilitation process. NeuroRehabilitation. (2015) 36:5–9. doi: 10.3233/NRE-141184
5. Schepers VP, Ketelaar M, van de Port IG, Visser-Meily JM, Lindeman E. Comparing contents of functional outcome measures in stroke rehabilitation using the international classification of functioning, disability and health. Disabil Rehabil. (2007) 29:221–30. doi: 10.1080/09638280600756257
6. Leonardi M, Fheodoroff K. Goal setting with ICF (international classification of functioning, disability and health) and multidisciplinary team approach in stroke rehabilitation. In: Platz T, editor. Clinical Pathways in Stroke Rehabilitation. Cham: Springer (2021). p. 35–56.
7. Winstein C, Lewthwaite R, Blanton SR, Wolf LB, Wishart L. Infusing motor learning research into neurorehabilitation practice: a historical perspective with case exemplar from the accelerated skill acquisition program. J Neurol Phys Ther. (2014) 38:190–200. doi: 10.1097/NPT.0000000000000046
8. Levin MF, Demers M. Motor learning in neurological rehabilitation. Disabil Rehabil. (2021) 43:3445–43. doi: 10.1080/09638288.2020.1752317
9. Waddell KJ, Strube MJ, Bailey RR, Klaesner JW, Birkenmeier RL, Dromerick AW, et al. Does task-specific training improve upper limb performance in daily life poststroke? Neurorehabil Neural Repair. (2017) 31:290–300. doi: 10.1177/1545968316680493
10. Peterson DB. International classification of functioning, disability and health: an introduction for rehabilitation psychologists. Rehabil Psychol. (2005) 50:105. doi: 10.1037/0090-5550.50.2.105
11. Müller R, Geyh S. Lessons learned from different approaches towards classifying personal factors. Disabil Rehabil. (2015) 37:430–8. doi: 10.3109/09638288.2014.923527
12. Hoyle M, Gustafsson L, Meredith P, Ownsworth T. Participation after stroke: do we understand all the components and relationships as categorised in the ICF? Brain Impair. (2012) 13:4–15. doi: 10.1017/BrImp.2012.9
14. Schwarzer R, Fuchs R. Self-efficacy and health behaviours. Predicting Health Behav Res Pract Soc Cogn Models. (1996) 163:196.
15. Marks R, Allegrante JP. A review and synthesis of research evidence for self-efficacy-enhancing interventions for reducing chronic disability: implications for health education practice (part II). Health Promot Pract. (2005) 6:148–56. doi: 10.1177/1524839904266792
16. Chen WC, Hsiao MY, Wang TG. Prognostic factors of functional outcome in post-acute stroke in the rehabilitation unit. J Formos Med Assoc. (2021). doi: 10.1016/j.jfma.2021.07.009. [Epub ahead of print].
17. Schunk DH. Self-efficacy, motivation, and performance. J Appl Psychol. (1995) 7:112–37. doi: 10.1080/10413209508406961
18. Bandura A. Self-regulation of motivation and action through goal systems. In: Cognitive Perspectives on Emotion and Motivation. Berlin: Springer (1988). p. 37–61.
19. Holt KG, Wagenaar RO, Saltzman E. A dynamic systems/constraints approach to rehabilitation. Rev Bras Fisioter. (2010) 14:446–63. doi: 10.1590/S1413-35552010000600002
20. Wulf G, Lewthwaite R. Optimizing performance through intrinsic motivation and attention for learning: the OPTIMAL theory of motor learning. Psychon Bull Rev. (2016) 23:1382–414. doi: 10.3758/s13423-015-0999-9
21. Kendall E, Catalano T, Kuipers P, Posner N, Buys N, Charker J. Recovery following stroke: the role of self-management education. Soc Sci Med. (2007) 64:735–46. doi: 10.1016/j.socscimed.2006.09.012
22. Huijbregts MP, Myers AM, Streiner D, Teasell R. Implementation, process, and preliminary outcome evaluation of two community programs for persons with stroke and their care partners. Top Stroke Rehabil. (2008) 15:503–20. doi: 10.1310/tsr1505-503
23. Fryer CE, Luker JA, McDonnell MN, Hillier SL. Self management programmes for quality of life in people with stroke. Cochrane Database Syst Rev. (2016) 2016:Cd010442. doi: 10.1002/14651858.CD010442.pub2
24. Lorig KR, Ritter P, Stewart AL, Sobel DS, Brown BW Jr, Bandura A, et al. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med Care. (2001) 39:1217–23. doi: 10.1097/00005650-200111000-00008
25. White G, Cordato D, O'Rourke F, Mendis R, Ghia D, Chan D. Validation of the stroke rehabilitation motivation scale: a pilot study. Asian J Gerontol Geriatr. (2012) 7:80–7.
26. Maujean A, Davis P, Kendall E, Casey L, Loxton N. The daily living self-efficacy scale: a new measure for assessing self-efficacy in stroke survivors. Disabil Rehabil. (2014) 36:504–11. doi: 10.3109/09638288.2013.804592
27. Boyd LA, Hayward KS, Ward NS, Stinear CM, Rosso C, Fisher RJ, et al. Biomarkers of stroke recovery: consensus-based core recommendations from the stroke recovery and rehabilitation roundtable. Neurorehabil Neural Repair. (2017) 31:864–76. doi: 10.1177/1545968317732680
28. Findlater SE, Hawe RL, Mazerolle EL, Al Sultan AS, Cassidy JM, Scott SH, et al. Comparing CST lesion metrics as biomarkers for recovery of motor and proprioceptive impairments after stroke. Neurorehabil Neural Repair. (2019) 33:848–61. doi: 10.1177/1545968319868714
29. Moulton E, Magno S, Valabregue R, Amor-Sahli M, Pires C, Lehéricy S, et al. Acute diffusivity biomarkers for prediction of motor and language outcome in mild-to-severe stroke patients. Stroke. (2019) 50:2050–6. doi: 10.1161/STROKEAHA.119.024946
30. Jones F, Riazi A. Self-efficacy and self-management after stroke: a systematic review. Disabil Rehabil. (2011) 33:797–810. doi: 10.3109/09638288.2010.511415
31. Korpershoek C, van der Bijl J, Hafsteinsdóttir TB. Self-efficacy and its influence on recovery of patients with stroke: a systematic review. J Adv Nurs. (2011) 67:1876–94. doi: 10.1111/j.1365-2648.2011.05659.x
32. Cheong MJ, Kang Y, Kang HW. Psychosocial factors related to stroke patients' rehabilitation motivation: a scoping review and meta-analysis focused on South Korea. Healthcare (Basel). (2021) 9:211. doi: 10.3390/healthcare9091211
33. Parke HL, Epiphaniou E, Pearce G, Taylor SJ, Sheikh A, Griffiths CJ, et al. Self-management support interventions for stroke survivors: a systematic meta-review. PLoS ONE. (2015) 10:e0131448. doi: 10.1371/journal.pone.0131448
34. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
35. Joseph RP, Daniel CL, Thind H, Benitez TJ, Pekmezi D. Applying psychological theories to promote long-term maintenance of health behaviors. Am J Lifestyle Med. (2016) 10:356–68. doi: 10.1177/1559827614554594
36. Bandura A, Jeffery RW, Gajdos E. Generalizing change through participant modeling with self-directed mastery. Behav Res Ther. (1975) 13:141–52. doi: 10.1016/0005-7967(75)90008-X
37. Bandura A, Barab PG. Processes governing disinhibitory effects through symbolic modeling. J Abnorm Psychol. (1973) 82:1–9. doi: 10.1037/h0034968
38. Strauser DR. Applications of self-efficacy theory in rehabilitation counseling. J Rehabil. (1995) 61:7–12.
39. Bandura A. Perceived self-efficacy in cognitive development and functioning. Educ Psychol. (1993) 28:117–48. doi: 10.1207/s15326985ep2802_3
40. Bandura A. Regulation of cognitive processes through perceived self-efficacy. Dev Psychol. (1989) 25:729. doi: 10.1037/0012-1649.25.5.729
41. Bandura A, Schunk DH. Cultivating competence, self-efficacy, and intrinsic interest through proximal self-motivation. J Pers Soc Psychol. (1981) 41:586. doi: 10.1037/0022-3514.41.3.586
42. Bandura A, Freeman WH, LightseyR. Self-Efficacy: The Exercise of Control. Berlin: Springer (1999).
43. Bandura A. Self-efficacy mechanism in human agency. Am Psychol. (1982) 37:122. doi: 10.1037/0003-066X.37.2.122
44. Gupta A, Deepika S, Taly AB, Srivastava A, Surender V, Thyloth M. Quality of life and psychological problems in patients undergoing neurological rehabilitation. Ann Indian Acad Neurol. (2008) 11:225–30. doi: 10.4103/0972-2327.44557
45. Ahn DH, Lee YJ, Jeong JH, Kim YR, Park JB. The effect of post-stroke depression on rehabilitation outcome and the impact of caregiver type as a factor of post-stroke depression. Ann Rehabil Med. (2015) 39:74–80. doi: 10.5535/arm.2015.39.1.74
46. French MA, Miller A, Pohlig RT, Reisman DS. Depressive symptoms moderate the relationship among physical capacity, balance self-efficacy, and participation in people after stroke. Physical Therapy. (2021) 101:pzab224. doi: 10.1093/ptj/pzab224
47. Forgea MC, Lyons AG, Lorenz RA. Barriers and facilitators to engagement in rehabilitation among stroke survivors: an integrative review. Rehabil Nurs. (2021) 46:340–7. doi: 10.1097/RNJ.0000000000000340
48. Stewart JC, Lewthwaite R, Rocktashel J, Winstein CJ. Self-efficacy and reach performance in individuals with mild motor impairment due to stroke. Neurorehabil Neural Repair. (2019) 33:319–28. doi: 10.1177/1545968319836231
49. Rapoliene J, Endzelyte E, Jasevičiene I, Savickas R. Stroke patients motivation influence on the effectiveness of occupational therapy. Rehabil Res Pract. (2018) 2018:9367942. doi: 10.1155/2018/9367942
50. Jack K, McLean SM, Moffett JK, Gardiner E. Barriers to treatment adherence in physiotherapy outpatient clinics: a systematic review. Man Ther. (2010) 15:220–8. doi: 10.1016/j.math.2009.12.004
51. Jurkiewicz MT, Marzolini S, Oh P. Adherence to a home-based exercise program for individuals after stroke. Top Stroke Rehabil. (2011) 18:277–84. doi: 10.1310/tsr1803-277
52. Caetano LCG, Pacheco BD, Samora GAR, Teixeira-Salmela LF, Scianni AA. Self-efficacy to engage in physical exercise and walking ability best predicted exercise adherence after stroke. Stroke Res Treat. (2020) 2020:2957623. doi: 10.1155/2020/2957623
53. Smith SL, West RL. The application of self-efficacy principles to audiologic rehabilitation: a tutorial. Am J Audiol. (2006) 15:46–56. doi: 10.1044/1059-0889(2006/006)
54. Nuutila K, Tapola A, Tuominen H, Kupiainen S, Pásztor A, Niemivirta M. Reciprocal predictions between interest, self-efficacy, and performance during a task. Front Educ. (2020) 5:36. doi: 10.3389/feduc.2020.00036
55. Mohebi A, Pettibone JR, Hamid AA, Wong JT, Vinson LT, Patriarchi T, et al. Dissociable dopamine dynamics for learning and motivation. Nature. (2019) 570:65–70. doi: 10.1038/s41586-019-1235-y
56. Sit JW, Chair SY, Choi KC, Chan CW, Lee DT, Chan AW, et al. Do empowered stroke patients perform better at self-management and functional recovery after a stroke? A randomized controlled trial. Clin Interv Aging. (2016) 11:1441–50. doi: 10.2147/CIA.S109560
57. Barlow J, Sturt J, Hearnshaw H. Self-management interventions for people with chronic conditions in primary care: examples from arthritis, asthma and diabetes. Health Educ J. (2002) 61:365–78. doi: 10.1177/001789690206100408
58. Dobkin BH. Behavioral self-management strategies for practice and exercise should be included in neurologic rehabilitation trials and care. Curr Opin Neurol. (2016) 29:693–9. doi: 10.1097/WCO.0000000000000380
59. Lennon S, McKenna S, Jones F. Self-management programmes for people post stroke: a systematic review. Clin Rehabil. (2013) 27:867–78. doi: 10.1177/0269215513481045
60. Sakakibara BM, Kim AJ, Eng JJ. A systematic review and meta-analysis on self-management for improving risk factor control in stroke patients. Int J Behav Med. (2017) 24:42–53. doi: 10.1007/s12529-016-9582-7
61. Allen KR, Hazelett S, Jarjoura D, Wickstrom GC, Hua K, Weinhardt J, et al. Effectiveness of a postdischarge care management model for stroke and transient ischemic attack: a randomized trial. J Stroke Cerebrovasc Dis. (2002) 11:88–98. doi: 10.1053/jscd.2002.127106
62. Preston E, Dean CM, Ada L, Stanton R, Brauer S, Kuys S, et al. Promoting physical activity after stroke via self-management: a feasibility study. Top Stroke Rehabil. (2017) 24:353–60. doi: 10.1080/10749357.2017.1304876
63. Fu V, Weatherall M, McPherson K, Taylor W, McRae A, Thomson T, et al. Taking charge after stroke: a randomized controlled trial of a person-centered, self-directed rehabilitation intervention. Int J Stroke. (2020) 15:954–64. doi: 10.1177/1747493020915144
64. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. (2000) 55:68. doi: 10.1037/0003-066X.55.1.68
65. Rethorn ZD, Pettitt CD. What is the effect of health coaching delivered by physical therapists? A systematic review of randomized controlled trials. Phys Ther. (2019) 99:1354–70. doi: 10.1093/ptj/pzz098
66. McEwen SE, Donald M, Jutzi K, Allen KA, Avery L, Dawson DR, et al. Implementing a function-based cognitive strategy intervention within inter-professional stroke rehabilitation teams: changes in provider knowledge, self-efficacy and practice. PLoS ONE. (2019) 14:e0212988. doi: 10.1371/journal.pone.0212988
67. Frates EP, Moore MA, Lopez CN, McMahon GT. Coaching for behavior change in physiatry. Am J Phys Med Rehabil. (2011) 90:1074–82. doi: 10.1097/PHM.0b013e31822dea9a
68. Morris JH, Macgillivray S, McFarlane S. Interventions to promote long-term participation in physical activity after stroke: a systematic review of the literature. Arch Phys Med Rehabil. (2014) 95:956–67. doi: 10.1016/j.apmr.2013.12.016
69. McEwen SE, Huijbregts MP, Ryan JD, Polatajko HJ. Cognitive strategy use to enhance motor skill acquisition post-stroke: a critical review. Brain Inj. (2009) 23:263–77. doi: 10.1080/02699050902788493
70. Liu KP, Chan CC, Lee TM, Li LS, Hui-Chan CW. Self-regulatory learning and generalization for people with brain injury. Brain Inj. (2002) 16:817–24. doi: 10.1080/02699050210127295
71. McEwen SE, Polatajko HJ, Huijbregts MP, Ryan JD. Exploring a cognitive-based treatment approach to improve motor-based skill performance in chronic stroke: results of three single case experiments. Brain Inj. (2009) 23:1041–53. doi: 10.3109/02699050903421107
72. Skidmore ER, Dawson DR, Butters MA, Grattan ES, Juengst SB, Whyte EM, et al. Strategy training shows promise for addressing disability in the first 6 months after stroke. Neurorehabil Neural Repair. (2015) 29:668–76. doi: 10.1177/1545968314562113
73. Lee C, Bobko P. Self-efficacy beliefs: comparison of five measures. J Appl Psychol. (1994) 79:364. doi: 10.1037/0021-9010.79.3.364
74. van der Bijl JJ, Shortridge-Baggett LM. The theory and measurement of the self-efficacy construct. Sch Inq Nurs Pract. (2001) 15:189–207.
75. Lennings C. An evaluation of a generalized self-efficacy scale. Pers Individ Differ. (1994) 16:745–50. doi: 10.1016/0191-8869(94)90215-1
76. Durand VM, Crimmins DB. The Motivation Assessment Scale. In: Hersen M, Bellack A, editor. Dictionary of Behavioral Assessment Techniques. Pergamon (1988). pp. 309–310.
77. Shankar S, Miller WC, Roberson ND, Hubley AM. Assessing patient motivation for treatment: a systematic review of available tools, their measurement properties, and conceptual definition. J Nurs Meas. (2019) 27:177–209. doi: 10.1891/1061-3749.27.2.177
78. Talelli P, Greenwood R, Rothwell J. Arm function after stroke: neurophysiological correlates and recovery mechanisms assessed by transcranial magnetic stimulation. Clinical Neurophysiol. (2006) 117:1641–59. doi: 10.1016/j.clinph.2006.01.016
79. Cassidy JM, Tran G, Quinlan EB, Cramer SC. Neuroimaging identifies patients most likely to respond to a restorative stroke therapy. Stroke. (2018) 49:433–8. doi: 10.1161/STROKEAHA.117.018844
80. Lin DJ, Cloutier AM, Erler KS, Cassidy JM, Snider SB, Ranford J, et al. Corticospinal tract injury estimated from acute stroke imaging predicts upper extremity motor recovery after stroke. Stroke. (2019) 50:3569–77. doi: 10.1161/STROKEAHA.119.025898
81. Cassidy JM, Wodeyar A, Wu J, Kaur K, Masuda AK, Srinivasan R, et al. Low-frequency oscillations are a biomarker of injury and recovery after stroke. Stroke. (2020) 51:1442–50. doi: 10.1161/STROKEAHA.120.028932
82. Liang X, Koh C-L, Yeh C-H, Goodin P, Lamp G, Connelly A, et al. Predicting post-stroke somatosensory function from resting-state functional connectivity: a feasibility study. Brain Sci. (2021) 11:1388. doi: 10.3390/brainsci11111388
83. Hartwigsen G, Volz LJ. Probing rapid network reorganization of motor and language functions via neuromodulation and neuroimaging. Neuroimage. (2021) 224:117449. doi: 10.1016/j.neuroimage.2020.117449
84. Schellhorn T, Aamodt EB, Lydersen S, Aam S, Wyller TB, Saltvedt I, et al. Clinically accessible neuroimaging predictors of post-stroke neurocognitive disorder: a prospective observational study. BMC Neurol. (2021) 21:89. doi: 10.1186/s12883-021-02117-8
85. Kim B, Winstein C. Can neurological biomarkers of brain impairment be used to predict poststroke motor recovery? A systematic review. Neurorehabil Neural Repair. (2017) 31:3–24. doi: 10.1177/1545968316662708
86. Farrer C, Frith CD. Experiencing oneself vs. another person as being the cause of an action: the neural correlates of the experience of agency. Neuroimage. (2002) 15:596–603. doi: 10.1006/nimg.2001.1009
87. Yomogida Y, Sugiura M, Sassa Y, Wakusawa K, Sekiguchi A, Fukushima A, et al. The neural basis of agency: an fMRI study. Neuroimage. (2010) 50:198–207. doi: 10.1016/j.neuroimage.2009.12.054
88. Nahab FB, Kundu P, Gallea C, Kakareka J, Pursley R, Pohida T, et al. The neural processes underlying self-agency. Cereb Cortex. (2011) 21:48–55. doi: 10.1093/cercor/bhq059
89. Davis JC, Nagamatsu LS, Hsu CL, Beattie BL, Liu-Ambrose T. Self-efficacy is independently associated with brain volume in older women. Age Ageing. (2012) 41:495–501. doi: 10.1093/ageing/afs029
90. Kang SY, Im CH, Shim M, Nahab FB, Park J, Kim DW, et al. Brain networks responsible for sense of agency: an EEG study. PLoS ONE. (2015) 10:e0135261. doi: 10.1371/journal.pone.0135261
91. Nakagawa S, Takeuchi H, Taki Y, Nouchi R, Kotozaki Y, Shinada T, et al. Lenticular nucleus correlates of general self-efficacy in young adults. Brain Struct Funct. (2017) 222:3309–18. doi: 10.1007/s00429-017-1406-2
92. Hirao K. Comparison of hemodynamic responses in the prefrontal cortex according to differences in self-efficacy. Biol Res Nurs. (2017) 19:450–5. doi: 10.1177/1099800417706141
93. Balleine BW, O'Doherty JP. Human and rodent homologies in action control: corticostriatal determinants of goal-directed and habitual action. Neuropsychopharmacology. (2010) 35:48–69. doi: 10.1038/npp.2009.131
94. Durieux PF, Schiffmann SN, de Kerchove d'Exaerde A. Targeting neuronal populations of the striatum. Front Neuroanat. (2011) 5:40. doi: 10.3389/fnana.2011.00040
95. Raz N, Williamson A, Gunning-Dixon F, Head D, Acker JD. Neuroanatomical and cognitive correlates of adult age differences in acquisition of a perceptual-motor skill. Microsc Res Tech. (2000) 51:85–93. doi: 10.1002/1097-0029(20001001)51:1andlt
96. Hong S, Hikosaka O. The globus pallidus sends reward-related signals to the lateral habenula. Neuron. (2008) 60:720–9. doi: 10.1016/j.neuron.2008.09.035
97. Horga G, Maia TV, Marsh R, Hao X, Xu D, Duan Y, et al. Changes in corticostriatal connectivity during reinforcement learning in humans. Hum Brain Mapp. (2015) 36:793–803. doi: 10.1002/hbm.22665
98. Kelley WM, Wagner DD, Heatherton TF. In search of a human self-regulation system. Annu Rev Neurosci. (2015) 38:389–411. doi: 10.1146/annurev-neuro-071013-014243
99. Kelley NJ, Gallucci A, Riva P, Romero Lauro LJ, Schmeichel BJ. Stimulating self-regulation: a review of non-invasive brain stimulation studies of goal-directed behavior. Front Behav Neurosci. (2018) 12:337. doi: 10.3389/fnbeh.2018.00337
100. Liu Y, Chan JS, Yan JH. Neuropsychological mechanisms of falls in older adults. Front Aging Neurosci. (2014) 6:64. doi: 10.3389/fnagi.2014.00064
101. Werden E, Cumming T, Li Q, Bird L, Veldsman M, Pardoe HR, et al. Structural MRI markers of brain aging early after ischemic stroke. Neurology. (2017) 89:116–24. doi: 10.1212/WNL.0000000000004086
102. Sperduti M, Delaveau P, Fossati P, Nadel J. Different brain structures related to self- and external-agency attribution: a brief review and meta-analysis. Brain Struct Funct. (2011) 216:151–7. doi: 10.1007/s00429-010-0298-1
103. Zito GA, Wiest R, Aybek S. Neural correlates of sense of agency in motor control: a neuroimaging meta-analysis. PLoS ONE. (2020) 15:e0234321. doi: 10.1371/journal.pone.0234321
104. Namkung H, Kim SH, Sawa A. The insula: an underestimated brain area in clinical neuroscience, psychiatry, and neurology. Trends Neurosci. (2017) 40:200–7. doi: 10.1016/j.tins.2017.02.002
105. VanGilder JL, Hooyman A, Peterson DS, Schaefer SY. Post-stroke cognitive impairments and responsiveness to motor rehabilitation: a review. Curr Phys Med Rehabil Rep. (2020) 8:461–8. doi: 10.1007/s40141-020-00283-3
106. Ogawa K, Inui T. Lateralization of the posterior parietal cortex for internal monitoring of self- versus externally generated movements. J Cogn Neurosci. (2007) 19:1827–35. doi: 10.1162/jocn.2007.19.11.1827
107. Westlake KP, Hinkley LB, Bucci M, Guggisberg AG, Findlay AM, Henry RG, et al. Resting state alpha-band functional connectivity and recovery after stroke. Exp Neurol. (2012) 237:160–9. doi: 10.1016/j.expneurol.2012.06.020
108. Cassidy JM, Wodeyar A, Srinivasan R, Cramer SC. Coherent neural oscillations inform early stroke motor recovery. Hum Brain Mapp. (2021) 42:5636–647. doi: 10.1002/hbm.25643
109. Schmidt L, Lebreton M, Cléry-Melin ML, Daunizeau J, Pessiglione M. Neural mechanisms underlying motivation of mental versus physical effort. PLoS Biol. (2012) 10:e1001266. doi: 10.1371/journal.pbio.1001266
110. Lee W, Reeve J. Self-determined, but not non-self-determined, motivation predicts activations in the anterior insular cortex: an fMRI study of personal agency. Soc Cogn Affect Neurosci. (2013) 8:538–45. doi: 10.1093/scan/nss029
111. Quirin M, Meyer F, Heise N, Kuhl J, Küstermann E, Strüber D, et al. Neural correlates of social motivation: an fMRI study on power versus affiliation. Int J Psychophysiol. (2013) 88:289–95. doi: 10.1016/j.ijpsycho.2012.07.003
112. Radke S, Seidel EM, Eickhoff SB, Gur RC, Schneider F, Habel U, et al. When opportunity meets motivation: neural engagement during social approach is linked to high approach motivation. Neuroimage. (2016) 127:267–76. doi: 10.1016/j.neuroimage.2015.12.014
113. Myers CA, Wang C, Black JM, Bugescu N, Hoeft F. The matter of motivation: striatal resting-state connectivity is dissociable between grit and growth mindset. Soc Cogn Affect Neurosci. (2016) 11:1521–7. doi: 10.1093/scan/nsw065
114. Lee W, Reeve J. Identifying the neural substrates of intrinsic motivation during task performance. Cogn Affect Behav Neurosci. (2017) 17:939–53. doi: 10.3758/s13415-017-0524-x
115. Kohli A, Blitzer DN, Lefco RW, Barter JW, Haynes MR, Colalillo SA, et al. Using expectancy theory to quantitatively dissociate the neural representation of motivation from its influential factors in the human brain: an fMRI study. Neuroimage. (2018) 178:552–61. doi: 10.1016/j.neuroimage.2018.05.021
116. Wager TD, Barrett LF. From affect to control: Functional specialization of the insula in motivation and regulation. biorxiv [Preprint]. (2017) 102368. doi: 10.1101/102368
117. Soutschek A, Kang P, Ruff CC, Hare TA, Tobler PN. Brain stimulation over the frontopolar cortex enhances motivation to exert effort for reward. Biol Psychiatry. (2018) 84:38–45. doi: 10.1016/j.biopsych.2017.11.007
118. Hosoda C, Tsujimoto S, Tatekawa M, Honda M, Osu R, Hanakawa T. Plastic frontal pole cortex structure related to individual persistence for goal achievement. Commun Biol. (2020) 3:194. doi: 10.1038/s42003-020-0930-4
119. Sheeran P, Maki A, Montanaro E, Avishai-Yitshak A, Bryan A, Klein WM, et al. The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: a meta-analysis. Health Psychol. (2016) 35:1178. doi: 10.1037/hea0000387
120. Danks KA, Pohlig RT, Roos M, Wright TR, Reisman DS. The relationship between walking capacity, biopsychosocial factors, self-efficacy and walking activity in individuals post stroke. J Neurol Phys Therapy. (2016) 40:232. doi: 10.1097/NPT.0000000000000143
121. French MA, Moore MF, Pohlig R, Reisman D. Self-efficacy mediates the relationship between balance/walking performance, activity, and participation after stroke. Top Stroke Rehabil. (2016) 23:77–83. doi: 10.1080/10749357.2015.1110306
122. Brouwer-Goossensen D, van Genugten L, Lingsma HF, Dippel DWJ, Koudstaal PJ, den Hertog HM. Self-efficacy for health-related behaviour change in patients with TIA or minor ischemic stroke. Psychol Health. (2018) 33:1490–501. doi: 10.1080/08870446.2018.1508686
123. Kobylańska M, Kowalska J, Neustein J, Mazurek J, Wójcik B, Bełza M, et al. The role of biopsychosocial factors in the rehabilitation process of individuals with a stroke. Work. (2018) 61:523–35. doi: 10.3233/WOR-162823
124. Huang HC, Chung KC, Lai DC, Sung SF. The impact of timing and dose of rehabilitation delivery on functional recovery of stroke patients. J Chin Med Assoc. (2009) 72:257–64. doi: 10.1016/S1726-4901(09)70066-8
125. Klassen TD, Dukelow SP, Bayley MT, Benavente O, Hill MD, Krassioukov A, et al. Higher doses improve walking recovery during stroke inpatient rehabilitation. Stroke. (2020) 51:2639–48. doi: 10.1161/STROKEAHA.120.029245
126. Dromerick AW, Geed S, Barth J, Brady K, Giannetti ML, Mitchell A, et al. Critical Period After Stroke Study (CPASS): A phase II clinical trial testing an optimal time for motor recovery after stroke in humans. Proc Natl Acad Sci U S A. (2021) 118:e2026676118. doi: 10.1073/pnas.2026676118
127. Oyake K, Suzuki M, Otaka Y, Tanaka S. Motivational strategies for stroke rehabilitation: a descriptive cross-sectional study. Front Neurol. (2020) 11:553. doi: 10.3389/fneur.2020.00553
128. Lewthwaite R, Winstein CJ, Lane CJ, Blanton S, Wagenheim BR, Nelsen MA, et al. Accelerating stroke recovery: body structures and functions, activities, participation, and quality of life outcomes from a large rehabilitation trial. Neurorehabil Neural Repair. (2018) 32:150–65. doi: 10.1177/1545968318760726
129. Kenah K, Bernhardt J, Cumming T, Spratt N, Janssen H. The prevalence of boredom in stroke survivors during inpatient rehabilitation. Int J Stroke. (2018) 13:23–23.
130. Luker J, Lynch E, Bernhardsson S, Bennett L, Bernhardt J. Stroke survivors' experiences of physical rehabilitation: a systematic review of qualitative studies. Arch Phys Med Rehabil. (2015) 96:1698–708.e1610. doi: 10.1016/j.apmr.2015.03.017
131. Bandura A. Guide for constructing self-efficacy scales. In: Pajares F, Urdan F, editors. Adolescence and Education: Self-Efficacy and Adolescence, Vol. 5. Greenwich, CT: Information Age (2006). pp. 307–337.
132. Kwakkel G, Lannin NA, Borschmann K, English C, Ali M, Churilov L, et al. Standardized measurement of sensorimotor recovery in stroke trials: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable. Int J Stroke. (2017) 12:451–61. doi: 10.1177/1747493017711813
133. Powell LE, Myers AM. The activities-specific balance confidence (ABC) scale. J Gerontol A Biol Sci Med Sci. (1995) 50:M28–34. doi: 10.1093/gerona/50A.1.M28
134. Tinetti ME, Richman D, Powell L. Falls efficacy as a measure of fear of falling. J Gerontol. (1990) 45:P239–43. doi: 10.1093/geronj/45.6.P239
135. Holland A, O'Connor R, Thompson A, Playford E, Hobart J. Talking the talk on walking the walk. J Neurol. (2006) 253:1594–602. doi: 10.1007/s00415-006-0272-2
136. Shaughnessy M, Resnick BM, Macko RF. Reliability and validity testing of the short self-efficacy and outcome expectation for exercise scales in stroke survivors. J Stroke Cerebrov Dis. (2004) 13:214–9. doi: 10.1016/j.jstrokecerebrovasdis.2004.07.002
137. Chen S, Lewthwaite R, Schweighofer N, Winstein CJ. Discriminant validity of a new measure of self-efficacy for reaching movements after stroke-induced hemiparesis. J Hand Ther. (2013) 26:116–23. doi: 10.1016/j.jht.2012.09.002
138. Jones F, Partridge C, Reid F. The Stroke Self-Efficacy Questionnaire: measuring individual confidence in functional performance after stroke. J Clin Nurs. (2008) 17:244–52. doi: 10.1111/j.1365-2702.2008.02333.x
Keywords: stroke, self-efficacy, motivation, neurorehabilitation, neuroimaging, biomarker
Citation: Gangwani R, Cain A, Collins A and Cassidy JM (2022) Leveraging Factors of Self-Efficacy and Motivation to Optimize Stroke Recovery. Front. Neurol. 13:823202. doi: 10.3389/fneur.2022.823202
Received: 26 November 2021; Accepted: 13 January 2022;
Published: 24 February 2022.
Edited by:
Julie Bernhardt, University of Melbourne, AustraliaReviewed by:
Gauthier Jean-Marc Everard, Catholic University of Louvain, BelgiumShuangxi Chen, University of South China, China
Copyright © 2022 Gangwani, Cain, Collins and Cassidy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica M. Cassidy, jcassidy@med.unc.edu