 Elisa García
Elisa García Samantha Sánchez-Noriega
Samantha Sánchez-Noriega Guadalupe González-PachecoAlejandro Naat González-Vázquez
Guadalupe González-PachecoAlejandro Naat González-Vázquez Antonio Ibarra
Antonio Ibarra Roxana Rodríguez-Barrera*
Roxana Rodríguez-Barrera*- Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Campus Norte, Huixquilucan de Degollado, CP, Mexico
Background: Currently, combined therapies could help to reduce long-term sequelae of spinal cord injury (SCI); stem cell therapy at the site of injury in combination with other therapies has shown very promising results that can be transferred to the clinical field. Nanoparticles (NPs) are versatile technologies with applications to medical research for treatments of SCI since they could deliver therapeutic molecules to the target tissue and may help to reduce the side effects of non-targeted therapies. This article's purpose is to analyze and concisely describe the diverse cellular therapies in combination with NPs and their regenerative effect after SCI.
Methods: We reviewed the literature related to combinatory therapy for motor impairment following SCI that has been published by Web of Science, Scopus, EBSCO host, and PubMed databases. The research covers the databases from 2001 to December 2022.
Result: Animal models of SCI have shown that the combination of NPs plus stem cells has a positive impact on neuroprotection and neuroregeneration. Further research is required to better understand the effects and benefits of SCI on a clinical level; therefore, it is necessary to find and select the most effective molecules that are capable of exacerbating the neurorestorative effects of the different stem cells and then try them out on patients after SCI. On the other hand, we consider that synthetic polymers such as poly [lactic-co-glycolic acid] (PLGA) could be a candidate for the design of the first therapeutic strategy that combines NPs with stem cells in patients with SCI. The reasons for the selection are that PLGA has shown important advantages over other NPs, such as being biodegradable, having low toxicity levels, and high biocompatibility; In addition, researchers could control the release time and the biodegradation kinetics, and most importantly, it could be used as NMs on other clinical pathologies (12 studies on www.clinicaltrials.gov) and has been approved by the Federal Food, Drug, and Cosmetic Act (FDA).
Conclusion: The use of cellular therapy and NPs may be a worthwhile alternative for SCI therapy; however, it is expected that the data obtained from interventions after SCI reflect an important variability of molecules combined with NPs. Therefore, it is necessary to properly define the limits of this research to be able to continue to work on the same line. Consequently, the selection of a specific therapeutic molecule and type of NPs plus stem cells are crucial to evaluate its application in clinical trials.
1. Introduction
Spinal cord injury (SCI) has detrimental effects on the spinal cord (SC), which results in the loss of motor, autonomic, and sensory functions with devastating consequences on the wellbeing and productivity of patients and their families. The pathophysiology of SCI is divided into primary and secondary injuries. Over time, the lesion progresses to a chronic phase, which prevents regeneration due to the development of the astroglial fibrous scar that surrounds the cystic cavities. The care of patients with SCI is a challenging task that requires the multidisciplinary collaboration of many scientists and specialists. Different therapies have been developed to reduce the damage related to the injury; however, a single treatment is not enough. Nowadays, combined therapies could help to reduce long-term sequelae; stem cell therapy at the site of injury is a well-studied option. Transplantation of mesenchymal stem cells (MSCs), neural stem cells (NSCs), and olfactory ensheathing cells (OECs) has been investigated as a potential therapy for SCI. It has been seen that MSCs can reduce the activation of the inflammatory response and promote functional recovery. NSCs are a source of astrocytes with beneficial functions, including the preservation of tissue integrity and neurotrophic support for neurons; finally, OECs are promising candidates for the promotion of neural repair as potential therapies for SCI. However, the neuroprotector and neuroregenerative effects are limited or depend on many variables; if these cells are combined with other therapies, very promising results can be obtained and transferred to the clinic. On the other hand, the use of nanoparticles (NPs) is a novel strategy used on diverse pathologies, due to their unique properties, are multifaceted nanotechnologies can offer efficient treatments because they have the ability to apply therapeutic molecules to the target tissue and therefore reduce the side effects by its high diffuse and compatibility. This article aimed to analyze and briefly describe the different types of cell therapies targeting MSCs, NSCs, and OECs individually and the advantages in combination with NPs as innovative treatments for their regenerative effects after SCI.
2. Incidence of spinal cord injury
Spinal cord injury is among the most worrying disabilities related to the nervous system. It is considered a global public health problem that affects patients physically, psychologically, and even socially. Furthermore, SCI refers to the damage to the SC as a result of some type of degenerative disease or due to severe trauma; vehicular accidents are usually the most frequent cause of SCI (1). According to the World Health Organization (WHO), it is estimated that each year there are between 40 and 80 new cases per million inhabitants worldwide of which 90% are of traumatic origin. Nevertheless, the number of cases of non-traumatic origin is constantly increasing as well (2, 3). This incidence is estimated at 10.5 new cases per 100,000 inhabitants per year. Singh et al. reported in 2014 that SCI has a higher prevalence in the United States of America with 906 cases per million inhabitants than in the Rhône-Alpes region, France and Helsinki, Finland, both with <280 cases per million population (4).
2.1. Pathophysiology of spinal cord injury
At present, a large number of economic resources are invested in different institutions around the world to carry out hundreds of investigations to study the pathophysiology and degenerative evolution of SCI and to learn more about the pathological mechanisms in order to develop new and more effective alternative therapies. This is a consequence of the worrying and increasing morbidity and mortality that this destructive neurological and pathological state entails (2).
In general terms, the pathophysiology of SCI is divided into an acute phase and a chronic phase. During its progression, a cascade of destructive events occurs from inflammatory processes, oxidative stress, cell apoptosis, and ischemia, which give place to the loss of locomotor and sensory functions (3). SCI triggers a series of biochemical and cellular events that eventually lead to the death of neurons, oligodendrocytes, astrocytes, and cell precursors. The main determinants of the severity of SCI are the extent of initial destruction (2, 3, 5).
Acute SCI commonly occurs from severe trauma to the spine where vertebral fractures or dislocations also occur. The primary injury appears immediately after the initial injury and is divided into two stages: Initially, it involves neural tissue damage, axonal connection interruption, glial membrane detachment, and hemorrhage. While clinical evidence suggests this causes a complete loss of functions, it has been observed that certain axonal connections remain during the primary SCI phase, demonstrating the existence of a state when there is only a partial lesion (2, 3, 6).
The secondary injury is triggered by the primary injury, causing other chemical and mechanical damages to the rachidial tissue. This produces neuronal excitotoxicity due to the high accumulation of calcium inside the cells increases the concentrations of reactive oxygen species and the release of glutamate. These events cause oxidative damage in proteins, phospholipids, and nucleic acids which can cause neurological dysfunction. Neuronal and glial damage include augmented cell permeability, edema, ion dysregulation, vascular damage, lipid peroxidation, apoptotic signaling, excitotoxicity, inflammation, demyelination, Wallerian degeneration, fibroglial scarring, and cyst formation (2, 3). Neuroinflammatory mechanisms could be induced by the events of secondary injury or on the other side the inflammatory response exacerbates it. For this reason, it is known that neuroinflammation after SCI can induce both beneficial and detrimental effects on locomotor function recovery; hence, it is necessary to characterize all the implications caused by inflammation to approach therapy research correctly (7).
The inflammatory response starts from the disruption of the blood–brain barrier (BBB), and the rupture of blood vessels causes hemorrhage into the spinal tissues, thus increasing the permeability of immune cells from the circulatory system to the lesion microenvironment, followed by monocyte, neutrophil, lymphocyte, and macrophage infiltration to the spine. The inflammatory cytokine output such as interleukin (IL)-1α, IL-1β, IL-6, and tumor necrosis factor (TNF-α), 6 to 12 h after injury, as a result of immune cells and anti-inflammatory cytokines presence, a neurological inflammatory process is given (3, 6, 8). During the acute phase (48 h after the lesion), vast inflammatory cells migrate into the exposed tissue and secrete cytokines (5). At this early phase, neutrophils reach their peak 24 h post-lesion. Afterward, the chronological arrival of inflammatory cells is characterized, in the subacute phase, by microglia peaking on day 7 and T cells peaking on day 9 after the lesion. Furthermore, at the late phase, a secondary injury cascade, starting 14 days after the injury, the peak of cellular inflammation takes place on day 60 post-lesion (characterized by the high prevalence of microglia) and it is still detectable for all three cell types over 180 days (9). Inflammation progresses through the action of pro-inflammatory cytokines, which include TNFα, gamma-interferon (IFNγ), CXC motif chemokine ligand 1 (CXCL1), IL-1, IL-12, IL-18, and the granulocyte–macrophage colony-stimulating factor (GMCSF), and it is solved with anti-inflammatory cytokines such as IL-4, IL-10, and IL-13 (10).
The presence of T helper cells (Th) in CNS is regulated by three specific points: subarachnoid vessels, choroid plexus and parenchyma, and post-capillary venules. CD4+ T cells might also become tissue-resident after inflammatory episodes (11). These cells modulate how innate and adaptive immune cells function and are recruited through the secretion of anti-inflammatory cytokines and growth factors. One crucial feature of T cells is the immunological synapse, which is the connection that allows an adaptive immune response to mediate injury repair and then differentiates to variable phenotypes of T cells according to the cytokines that are released, except for Th1 and Th2 subsets (12). The acute lesion is usually distinguished by the presence of Th1 subsets that control the discharge of pro-inflammatory cytokines, such as IL-2, IL-12, and IFNγ, therefore resulting in demyelination and parenchyma destruction, although their possible beneficial effects are still under debate. Prior to that, at the subacute phase, Th2, Treg, and Th17 prevalence can be identified due to the release of IL-4, IL-10, IL-17, and IL-23 cytokines, protecting the spine from autoimmune effects. If the microenvironment characteristics are optimal and the susceptibility of the individual is appropriate, recovery could be enhanced during this phase by reducing neuroinflammation (11). However, several articles show that different Th phenotypes can mediate immune-mediated damage, Exacerbated inflammatory response or even generate autoimmune CNS inflammation (9, 13). In addition, inflammatory conditions allow the predominance of T-cell phenotypes, such as Th1 and Th17 (14). Even though they mainly secrete a profile of pro-inflammatory cytokines, they also contribute to lesion repair by different pathways: Reactive astrocytes help to the restoration of BBB by inducing endothelial tight junction repair, cleaning cellular debris, and reducing excitotoxicity (15). Reactive astrocytes form a dense glial scar at the edge of the lesion surrounding a central lesion composed of proteoglycans and activated phagocytic microglia/macrophages. These cells have a constant cross-talk interaction with phagocytic cells by the release of different profiles of cytokines and chemokines (16). The formation of this scar limits the spread of necrotic, apoptotic, and infiltrating inflammatory cells, inhibiting neuroinflammation (7). Furthermore, negatively, the formation of glial scar interrupts axonal regeneration (15). To counteract all these harmful effects, strategies have been designed for therapeutic biomaterials to control neuroinflammation.
Now, different drugs regulate or inhibit different mechanisms involved in the inflammatory response; however, the direct effect is not possible and that limited the recovery after SCI and has a secondary consequence that depends on the type of drug administered. A viable strategy for solving it is nanomedicine, which has increased its importance and presence in different investigations in recent years. This has a fundamental role in the design of new therapeutic strategies in pharmacology, such as the controlled kinetic release and bioavailability of active ingredients, managing to increase the effectiveness of already established treatments, and reducing adverse effects. In the technological branch, nanomaterials such as NPs and nanofibers are being developed to serve as a replacement for the neural tissue affected or lost in SCI, as well as nanopharmaceuticals that manages to integrate the tissue to its normal state (17–19).
3. Nanomaterials for neuroprotection and neuroregenerative processes
In the past few years, active explorative studies had analyzed the relevance of nanomaterials (NMs) as a treatment for neurodegeneration and the processes they imply. NMs and the different applications they have been given make possible drug delivery on SC or between a combination strategy with cellular therapy by promoting its differentiation or action intending to promote neuroregeneration. The mentioned approaches seek to become possible solutions to trespass the BBB (20).
Nanomaterials are materials with nanoscale dimensions, whose proportions vary from 1 to 100 nm. These materials, in contrast to other bulk molecules, have singularities that distinguish them. In recent decades, NMs gained insight as environmental-safe, lightweight, pH labile, and easily disintegrated materials (20, 21). NMs are known to have a promising role in the intervention of neuronal injury (21).
Nanomaterials could be the answer to solving therapeutic issues because of their particularities such as their size. They offer the possibility of employing them as nano-carriers specifically targeted to the site of injury for enhancing the bioavailability of drugs and broadening their time in circulation (22). In addition, NM-formed NPs are able to restore axonal regeneration with regard to promoting signal pathways on neural cells or stem cells applied, which could reinstitute conduction in SCI through progressive axonal re-growth (23). Scaffolds constructed upon NMs aid in microenvironment recreation, according to its fundamental nature (24).
Not long ago, diverse research works were dedicated to identifying NMs as a treatment for SCI. By their nano-size ranges, the neuroprotective drugs compacted by NMs increase their availability specifically on the SC site of injury. Nanomaterial-mediated drug delivery has exposed relevant therapeutic advances, showing results like reduced neuronal damage which allows motor recovery. In addition, this drug delivery system has been engineered and utilized as dendrimers, nanocapsules, silica NPs (SNPs), carbon nanotubes, and graphene sheets to prevent further neurodegeneration after SCI (25). The study of nanostructured drugs has been sectioned in two: (1) drug encapsulation within the nanostructure during the time of synthesis and its coupling with conjugation reactions and (2) promotion under general development, growth, or differentiation of stem cells in the treatment of neurological diseases (26).
4. Nanoparticles on spinal cord injury
Multiple variants of NPs have been under trial for the treatment of SCI. The components of NPs vary from metals or ceramics (gold, silver, iron oxide, cadmium, and zinc) (27–29), polymers [poly(lactic-co-glycolic acid (PLGA), and polycaprolactone] (30, 31), liposomes (32, 33), exosomes (34, 35), carbon-based NPs (CNPs), SNPs (36) and numerous other types (37–39). The various existing types of NPs have intrinsic advantages and disadvantages; therefore, a meticulous investigation should be pursued before selecting a particular type of NPs regarding the specific requirements of the study. The relevance of this rigorous selection is a consequence of the potential problems associated with BBB permeability and the complex organization of the CNS when applying NPs in the SC. The different properties of NP charge and surface are important parameters to take into consideration for SC applications (40). Positively charged variants have been tested within experimental models of SCI, being more efficiently internalized into cells in comparison with neutral and negatively charged NPs (41). In addition, positively charged NPs have a greater absorption into the liver when they are circulated in the bloodstream (42). Concerning the uptake of negatively charged NPs, it has been shown to be more agile when penetrating tissues than positively charged particles, while the positively charged particles are taken up more rapidly by proliferating cells (43). The specificity of NPs' surface charge depends on the purpose of their application, and the characteristics of the surface charge are capable of creating unique interactions with cells, leading to more desirable outcomes following recovery in SCI.
Nowadays, nanotechnology as a therapeutic approach for SCI has gained inordinate progress using different types of NPs for drug delivery, on Table 1 resumed the principal advantages.
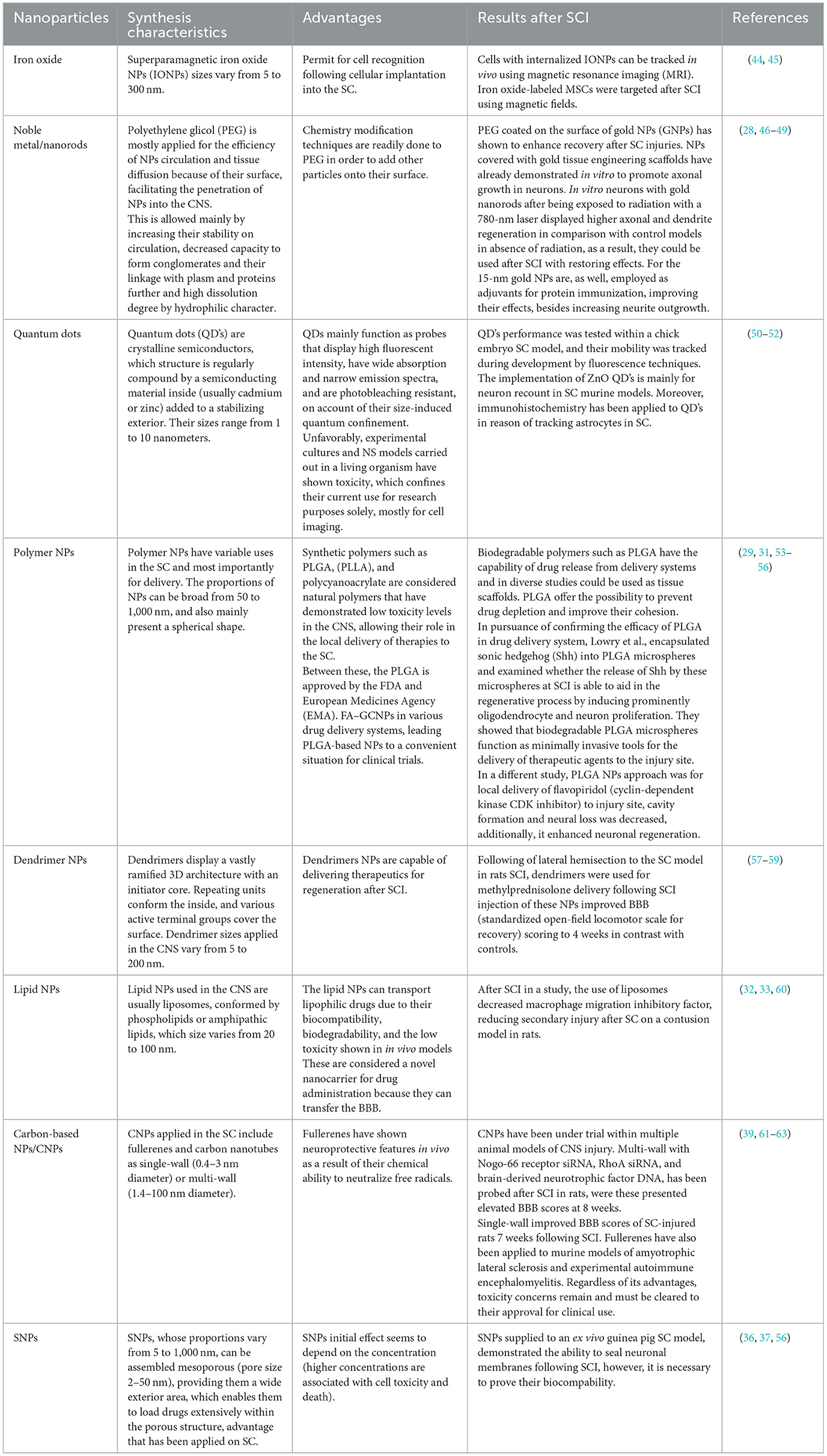
Table 1. Different types of nanoparticles used on spinal cord injury.
5. Use of cellular therapy and nanoparticles after SCI
Spinal cord injury implies that SC microenvironment changes in the early weeks post-injury, such as scar formation; therefore, combined therapies are needed. Animal model studies have shown that stem cell grafts are a potentially effective approach for SC regeneration by substituting necrotic nerve cells with differentiated MSCs, NSCs, and OECs; novel supporting cell transplants for remyelination, re-growth, and connection of the injured axons; and provide a protective environment for cells when transplanted into the injury site to prevent further harm by releasing protective substances such as growth factors, decreasing toxins such as free radicals, and preventing the spreading of the injury by reducing inflammation posterior to injury (64).
6. Recent advances in the combination of cellular therapy with stem cells and nanoparticles after a spinal cord injury
6.1. Mesenchymal stem cells and nanoparticles
Mesenchymal stem cells are an attractive approach for cellular therapy due to their self-renewal ability and differentiation to multiple variable mesenchymal lineages. As multipotent cells, MSCs are able to differentiate into other mesodermal tissues such as bone, cartilage, and cardiac muscle. Immunomodulatory properties and paracrine mechanisms of MSC benefits have been described in multiple studies (65, 66). MSCs have favorable effects by stem cell therapy after SCI, as a result of the advantages listed: (1) simple isolation and cryopreservation, (2) preserve regenerative ability and self-renew ability even at −80°C, (3) elevated proliferation rate and potential of multilineage differentiation, and 4) decreased the immunoreactivity and graft-vs.-host reaction of transplanted allogeneic MSCs (66, 67).
The principal sources of MSCs are bone marrow, umbilical cord blood, adipose tissue, and peripheral blood, even though they can be obtained from a variable range of tissues. MSCs are a viable option for lessening the negative pathophysiological effects of SCI (65). In regard to recovery after SCI, therapeutic methods mainly focus on achieving axon re-growth, inhibition of apoptosis, and substitution of damaged cells with oligodendrocytes in favor of axon remyelination (68). When MSCs are administered to the injury site following SCI, they produce and release different growth factors, including brain-derived neurotrophic factor (BDNF), glial derivate neurotrophic factor (GDNF), vascular endothelial growth factor (VEGF), insulin-like growth factor (IGF), fibroblast growth factor (FGF-2), and transforming growth factor (TGFβ), the molecules that promote axonal regeneration. In addition, MSCs downregulate apoptosis by reducing levels of apoptotic molecules and increasing the survival molecules in SCI animal models. Another important effect of these cells on cytokines is an increase in serum IL-10 and a decrease in tumor TNFα, which plays a relevant role in T-cell transitions from pro-inflammatory Th1 to anti-inflammatory Th2 phenotype, as well as macrophage phenotype transition from M1 (immune surveillance) to M2 (downregulating immune response). Through these mechanisms, MSCs enhance the survival and development of neurons and axonal regeneration (69, 70).
Stem cell transplantation is receiving increased attention as a therapeutic approach for the treatment of neurological diseases (71, 72). At the time of writing this article, there were 52,055 clinical trials involving neurological diseases and 743 involving stem cell-based therapy for neurological diseases. After SCI, only 60 studies included stem cell-based therapy and only six studies used NPs and stem cells on other pathologies (www.clinicaltrials.gov, accessed on 8 December 2022). Although a limited research area exists for stem cells' potentiated effect with NPs, MSCs have an immunomodulatory effect; however, none of these cells have produced more than a partial recovery of function, being an active area of research.
The therapeutic strategies that combination with NPs could potentially exacerbate the neurorestorative effect of MSCs, based on these foundations in 2015, Tukmachev et al. exposed that superparamagnetic IONPs can promote the taking in of MSCs at the injury site in a rat model of SCI (45). In the same context, Vishwakarma et al. developed a novel gadolinium-SPIO (Gd-SPIO) that acts like magnetic NPs with an elevated level of biocompatibility and potentially acquires a better contrast in MRI. As a result, it was proposed that the transplantation of neuronal cells labeled with Gd-SPIONPs could be an excellent approach for achieving high-contrast imaging and non-intrusive cell trapping at specific sites while remaining unaffected by inhibitory molecules. In a different study, magnetically labeled MSCs were introduced into the subarachnoid space in both the magnet and non-magnet groups. MSCs agglomerations were detected superficial to the SCI in the magnet group; on the contrary, few MSCs were observed in the non-magnet group. The hindlimb motor function of the magnet group displayed a significant improvement in comparison with the non-magnet groups (73). Furthermore, this combined therapeutic approach for regeneration after SCI is capable of potentiating the use of tissue engineering strategies to effectively bridge the injury (74). As regards, anti-inflammatory, anti-oxidative, and anti-excitotoxicity effects of ferulic acid (FA) and glycol chitosan (GC), both can be contemplated as natural neuroprotective compounds (75, 76). FA is capable of absorbing a hydrogen atom to form a phenoxy radical by the phenolic hydroxyl group; as a result, it protects cells from oxidative stress (76). Apart from that, the primary amines of GC might have a relevant role in neuroprotection. Wu et al. produced hydrophobic self-assembled FA-GCNPs by chemical conjugation, which displayed neuroprotective effects of FA–GCNPs following SCI. Systemic administration of these NPs promoted neuron cells and axons survival at the injury site and reduced the number of macrophages and activated astrocytes. Hence, these neuroprotective effects led to significant recovery after SCI (77).
The regenerative efficacy of IONPs-treated human MSCs was evaluated using exosome-mimetic nanovesicles (NV-IOPs) in a SCI model, with the results showing an increased amount of therapeutic growth factors associated with IONPs, which were slowly ionized to iron ions for the activation of JNK and c-Jun signaling cascades in human NSCs. In vivo systemic administration of these with magnetic guidance upregulated their number at the injury site. In addition, NV-IONP agglomeration promoted angiogenesis, generated anti-inflammatory and anti-apoptotic effects in SCI, and therefore had beneficial effects on SC function (78).
The principal focus of experimental models of SCI is stem cell transplantation into injured SC for motor recovery; however, bladder dysfunction investigation is almost none. However, Lee et al. investigated the effect of B10 human MSCs grafts into the bladder wall of SCI rats to prove their capability of collagen deposit inhibition and cystometric parameter improvement. Consequently, the SCI rats decreased their weights and collagen deposition, and furthermore, these cells differentiated into smooth muscle cells. The transplanted B10 cells helped to prevent bladder fibrosis and bladder dysfunction in the rat SCI model. Therefore, MSCs-based cell transplantation is a potential therapeutic approach for bladder dysfunction in patients with SCI (79).
Human NSCs are derived from induced pluripotent stem cells (iPSC-NSC), human MSCs, and a pH-responsive polyacetal–curcumin nanoconjugate (PA-C), which promote the sustained secretion of curcumin delivered into the intrathecal space in SCI contusion model in rats with stem cell transplantation. As a consequence, the locomotor function was improved (BBB scale), scars had reduced in size, and β-III tubulin-positive axons, motoneurons, and myelinated tracts were preserved. PA-C therapy promoted microglia into an anti-inflammatory phenotype (80). These studies advocate that MSC combination with other therapies is possible in favor of boosting their therapeutic potential. For example, another cell therapy is NSCs.
6.2. Neural stem cells and nanoparticles
These cells are multipotent cells with a high capacity for self-renewal and multidirectional differentiation potential to separate themselves into mature neurons and glial cell phenotypes. This provides a promising strategy, which could restore neuron loss after injury or in disease states. However, treatments with NSCs present challenges in terms of their regulation and evaluation of outcomes, including survival, distribution, differentiation, and integration. Long-term therapies generally focus on secondary damage alterations such as neuroinflammation and maladaptive plasticity, aiming at preserving the tissue and multiplying the production of exogenous NSCs to increase regeneration (26, 81). The combination of nanotechnology with stem cells is continuously developing and has shown that it can favor clinical and therapeutic diagnosis in various CNS diseases. NPs are innovative components for regenerative medicine due to their physicochemical characteristics (26, 82); they can be made of organic, inorganic, or composite-based materials and can be combined with different polymers to improve their hydrophilicity, biocompatibility, bioavailability, targeting capacity, and approach efficacy that can reduce dose-related and drug release at the site of injury (29).
GNPs provide a very effective method for introducing substances into cells and are characterized as being non-toxic, non-immunogenic, and biocompatible, which makes them ideal resources to be applied in biomedicine (83). The GNPs are distributed as negatively charged or positively charged. After SCI, GNPs positively increase neuronal growth when incorporated into embryonic cells or NSCs when applied on rats with SCI, promoting neuroregeneration and motor recovery function, thus suggesting that transplantation may be an effective therapy for injury repair (84).
Chitosan NPs (ChNPs) and valproic acid (VANPs) have shown efficacy as protective agents in SCI treatment. A study in 2021 found that ChNPs treatment with VANPs benefited tissue regeneration and locomotor function after SCI, significantly improved NSC proliferation and secretion levels of neurotrophic factors, promoted the outgrowth of neurite since it stimulated overexpression of microtubule-associated protein, and decreased IL-1β, IL-6, and TNF-α expression (85).
Chitosan NPs have chemical characteristics that are determined by two variables: molecular weight and the degree of acetylation (DA). Previous research has shown that DA plays a key role in the incorporation of artificial membranes, the sealing of mammalian membranes, and, finally, the restoration of neurophysiological function ex vivo (56).
Poly[lactic-co-glycolic acid] is a biodegradable polymer approved by the US FDA and the EMA. It has drawn attention due to its excellent biocompatibility and biodegradability, as well as its predictable biodegradation kinetics. Due to these characteristics, it has been used as a nanocarrier, has low toxicity and immunogenicity, and allows prolonged drug release. PLGA-encapsulated methylprednisolone has been used in SCI, and it has demonstrated a decrease in secondary injuries related to inflammation as well as a significant regenerative outcome 7 days post-injury (30). Another study has used electrospun nanofibers of PLGA and PEG, which enhanced the adhesion and proliferation of NSC derived from induced pluripotent stem cells (iPS). iPS derived from NSCs proved greater differentiation potential on the exterior of PLGA/PEG biomaterials. Furthermore, scaffold strategies combined with iPSC-NPC therapy have been demonstrated to improve functional SC rehabilitation after transection (86).
Neuroregeneration through NSCs in combination with NPs could provide promising therapies to repair and/or regenerate the damage caused by neurodegenerative diseases; likewise, these therapies may emerge as alternatives in the diagnosis of some CNS disorders.
In SCI, the use of NPs can increase the survival rate, decrease the diffusion of stem cells after transplantation, elevate the rate of differentiation into functional neurons, and direct the growth of stem cells. NPs and stem cells can be complementary therapeutic options.
6.3. Olfactory ensheathing cells and nanoparticles
Olfactory ensheathing cells are a resident of glial cells which are found in the peripheral nervous system (PNS) and CNS and are mostly observed in the central olfactory bulb (OB) and the nasal olfactory mucosa (87). They come with the surface of olfactory nerve fibroblasts, in order to hold the bundles of olfactory nerve fibers from the nasal mucosa for permitting synapsis in the OB (88). A study has shown that OB transplants can be differentiated for generating connections between the periphery and brain (87).
Brain-derived neurotrophic factor, GDNF, and NGF are expressed for OECs, and these are important for the propagation and guidance of axons, displaying similar features with astrocytes and Schwann cells (89, 90). The neurotrophic factors are able to protect neurons as a result of their capacity to inhibit the formation of scars and promote axonal re-establishment (91). They also are crucial for neural regeneration in reason of their capacity to proliferate and migrate from PNS and CNS. Recent studies have shown that extracellular vehicles (EVs) with OECs regulate cell–cell communication, viability, and toxicity (92).
Additional studies are needed to know more about the effect of the combining OECs and NPS ChABC-loaded PLGA at the injured site 1 week following the contusion, demonstrating myelin in the group with NPs ChABC-loaded PLGA and a significant therapeutic effect on functional recovery (93). Other outcomes demonstrate a function for human OEC-derived EVs in NSC proliferation and oxidative stress-induced neuronal toxicity model (94).
Fan et al. showed that isolated exosomes by the PEG-based method are a critical role in immunomodulation and could be engulfed by microglia and polarized anti-inflammatory response after SCI. The disadvantage is that the categorized EVs may perhaps trespass on other cell membranes, causing the results to be misinterpreted. Further studies are needed with regard to giving greater evidence about the effectiveness of this combinatory therapy with OECs and NPs (34).
7. Limitations and future prospects
Animal models of SCI have demonstrated that the combination of NPs plus stem cells has a positive impact on neuroprotection and neuroregeneration. Additional studies are needed for a better understanding of the effects and profits of SCI on a clinical level; therefore, it is necessary to find and select the most effective molecules that are capable of exacerbating the neurorestorative effects of the different stem cells and then try them out on patients after SCI. On the other hand, we consider that PLGA NPs could be the first therapeutic strategy that combines NPs with stem cells that could be used on patients with SCI because these NPs have shown important advantages compared to other NPs that have been previously approved by the FDA. These specific NPs are biodegradable and have shown low toxicity levels and high biocompatibility. In addition, researchers could control the release time and the biodegradation kinetics, and most importantly, it could be used as NMs on other clinical pathologies (12 studies on www.clinicaltrials.gov).
8. Conclusion
The use of cellular therapy and NPs can be an attractive strategy for SCI therapy; nevertheless, the data obtained from interventions after SCI will reflect an important variability of molecules used on NPs. Therefore, it is necessary to properly define the limits of this research to be able to continue to work on the same line. Consequently, the selection of a specific therapeutic molecule and the type of NPs plus stem cells is crucial to evaluate the application in clinical trials.
Author contributions
EG: conceptualization, formal analysis, investigation, methodology, project administration, writing the original draft, and reviewing and editing. SS-N: data curation, investigation, methodology, and reviewing language and editing. GG-P: data curation, investigation, methodology, writing the original draft, and reviewing language and editing. AG-V: data curation, investigation, methodology, and writing the original draft. AI: supporting and project management supervision. RR-B: conceptualization, formal analysis, investigation, methodology, project administration, writing the original draft, reviewing and editing, and project administration management (main). All authors contributed to the article and approved the submitted version.
Funding
EG and RR-B have been financed by Universidad Anáhuac México Campus Norte.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Spinal Cord Injury (2022). Available online at: https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury
2. Anjum A, Yazid MD, Fauzi Daud M, Idris J, Ng AMH, Selvi Naicker A, et al. Spinal cord injury: pathophysiology, multimolecular interactions, and underlying recovery mechanisms. Int J Mol Sci. (2020) 21:7533. doi: 10.3390/ijms21207533
3. Ahuja CS, Wilson JR, Nori S, Kotter MRN, Druschel C, Curt A, et al. Traumatic spinal cord injury. Nat Rev Dis Prim. (2017) 3:17018. doi: 10.1038/nrdp.2017.18
4. Singh A, Tetreault L, Kalsi-Ryan S, Nouri A, Fehlings MG. Global prevalence and incidence of traumatic spinal cord injury. Clin Epidemiol. (2014) 6:309–31. doi: 10.2147/CLEP.S68889
5. Badhiwala JH, Ahuja CS, Fehlings MG. Time is spine: a review of translational advances in spinal cord injury. J Neurosurg Spine. (2019) 30:1–18. doi: 10.3171/2018.9.SPINE18682
6. Eckert MJ, Martin MJ. Trauma: spinal cord injury. Surg Clin North Am. (2017) 97:1031–45. doi: 10.1016/j.suc.2017.06.008
7. Liu X, Zhang Y, Wang Y, Qian T. Inflammatory response to spinal cord injury and its treatment. World Neurosurg. (2021) 155:19–31. doi: 10.1016/j.wneu.2021.07.148
8. Monje M. Spinal cord injury - healing from within. N Engl J Med. (2021) 384:182–4. doi: 10.1056/NEJMcibr2030836
9. Beck KD, Nguyen HX, Galvan MD, Salazar DL, Woodruff TM, Anderson AJ. Quantitative analysis of cellular inflammation after traumatic spinal cord injury: evidence for a multiphasic inflammatory response in the acute to chronic environmen. Brain. (2010) 133(Pt 2):433–47. doi: 10.1093/brain/awp322
10. Bloom O, Herman PE, Spungen AM. Systemic inflammation in traumatic spinal cord injury. Exp Neurol. (2020) 325:113143. doi: 10.1016/j.expneurol.2019.113143
11. Korn T, Kallies A. T cell responses in the central nervous system. Nat Rev Immunol. (2017) 17:179–94. doi: 10.1038/nri.2016.144
12. Baruch K, Schwartz M. CNS-specific T cells shape brain function via the choroid plexus. Brain Behav Immun. (2013) 34:11–6. doi: 10.1016/j.bbi.2013.04.002
13. Conti A, Cardali S, Genovese T, Di Paola R, La Rosa G. Role of inflammation in the secondary injury following experimental spinal cord trauma. J Neurosurg Sci. (2003) 47:89–94.
14. Pang QM, Chen SY, Xu QJ, Zhang M, Liang DF, Fu SP, et al., Effects of astrocytes and microglia on neuroinflammation after spinal cord injury and related immunomodulatory strategies. Int Immunopharmacol. (2022) 108:108754. doi: 10.1016/j.intimp.2022.108754
15. Wang R, Zhou R, Chen Z, Gao S, Zhou F. The glial cells respond to spinal cord injury. Front Neurol. (2022) 13:844497. doi: 10.3389/fneur.2022.844497
16. Hellenbrand DJ, Quinn C, Piper ZJ, Morehouse CN, Fixel JA, Hanna AS. Inflammation after spinal cord injury: a review of the critical timeline of signaling cues and cellular infiltration. J Neuroinflamm. (2021) 18:284. doi: 10.1186/s12974-021-02337-2
17. Najahi-Missaoui W, Arnold RD, Cummings BS. Safe nanoparticles: are we there yet? Int J Mol Sci. (2020) 22:385. doi: 10.3390/ijms22010385
18. Chakraborty A, Ciciriello AJ, Dumont CM, Pearson RM. Nanoparticle-based delivery to treat spinal cord injury-a mini-review. AAPS PharmSciTech. (2021) 22:101. doi: 10.1208/s12249-021-01975-2
19. Zimmermann R, Alves YV, Sperling LE, Pranke P. Nanotechnology for the treatment of spinal cord injury. Tissue Eng Part B Rev. (2021) 27:353–365. doi: 10.1089/ten.teb.2020.0188
20. Gopal V, Mahadevan K. Nanotechnology in spinal cord injury: a new hope for overcoming barriers to treatment. J Spinal Surg. (2015) 2:78–84. doi: 10.5005/jp-journals-10039-1061
21. Saracino GA, Cigogninin D, Silva D, Caprini A, Gelain F. Nanomaterials design and tests for neural tissue engineering. Chem Soc Rev. (2013) 42:225–62. doi: 10.1039/C2CS35065C
22. Pourhassan-Moghaddam M, Zarghami N, Mohsenifar A, Rahmati M, Gholizadeh D, Akbarzadeh A, et al., Watercress-based gold nanoparticles: biosynthesis, mechanism of formation and study of their biocompatibility in vitro. Micro Nano Lett. (2014) 9:345–50. doi: 10.1049/mnl.2014.0063
23. Fawcett JW. Overcoming inhibition in the damaged spinal cord. J. Neurotrauma. (2006) 23:371–83. doi: 10.1089/neu.2006.23.371
24. Zhang L, Webster TJ. Nanotechnology and nanomaterials: promises for improved tissue regeneration. Nano Today. (2009) 4:66–80. doi: 10.1016/j.nantod.2008.10.014
25. Viswanathan VK, Rajaram Manoharan SR, Subramanian S, Moon A. Nanotechnology in spine surgery: a current update and critical review of the literature. World Neurosurg. (2019) 123:142–55. doi: 10.1016/j.wneu.2018.11.035
26. Zhang G, Khan AA, Wu H, Chen L, Gu Y, Gu N. The application of nanomaterials in stem cell therapy for some neurological diseases. Curr Drug Targets. (2018) 19:279–98. doi: 10.2174/1389450118666170328115801
27. Lee KJ, Browning ML, Nallathamby PD, Osgood CJ, Xu XH. Silver nanoparticles induce developmental stage-specific embryonic phenotypes in zebrafish. Nanoscale. (2013) 5:11625–36. doi: 10.1039/c3nr03210h
28. Papastefanaki F, Jakovcevski J, Poulia N, Djogo N, Schulz F, Martinovic T, et al. Intraspinal delivery of polyethylene glycol-coated gold nanoparticles promotes functional recovery after spinal cord injury. Mol Ther. (2015) 23:993–1002. doi: 10.1038/mt.2015.50
29. Nejati-Koshki K, Mortazavi Y, Pilehvar-Soltanahmadi Y, Sheoran S, Zarghami N. An update on application of nanotechnology and stem cells in spinal cord injury regeneration. Biomed Pharmacother. (2017) 90:85–92. doi: 10.1016/j.biopha.2017.03.035
30. Chvatal SA, Kim Y-T, Bratt-Leal AM, Lee H, Bellamkonda RV. Spatial distribution and acute anti-inflammatory effects of Methylprednisolone after sustained local delivery to the contused spinal cord. Biomaterials. (2008) 29:1967–75. doi: 10.1016/j.biomaterials.2008.01.002
31. Papa S, Ferrari R, De Paola M, Rossi F, Mariani A, Caron I, et al. Polymeric nanoparticle system to target activated microglia/macrophages in spinal cord injury. J Controll Release. (2014) 174:15–26. doi: 10.1016/j.jconrel.2013.11.001
32. Liu Y, Wang C-Y, Kong XH, Wang HJ, Chang J, Zhang DP, et al. Novel multifunctional polyethylene glycol-transactivating-transduction protein-modified liposomes cross the blood-spinal cord barrier after spinal cord injury. J Drug Target. (2010) 18:420–9. doi: 10.3109/10611860903434001
33. Wang H, Zhnag S, Liao Z, Wang C, Liu Y, Feng S, et al. PEGlated magnetic polymeric liposome anchored with TAT for delivery of drugs across the blood-spinal cord barrier. Biomaterials. (2010) 31:6589–96. doi: 10.1016/j.biomaterials.2010.04.057
34. Fan H, Chen Z, Tang HB, Shan LQ, Chen ZY, Wang XH, et al. Exosomes derived from olfactory ensheathing cells provided neuroprotection for spinal cord injury by switching the phenotype of macrophages/microglia. Bioeng Transl Med. (2021) 7:e10287. doi: 10.1002/btm2.10287
35. Huang JH, Yin XM, Xu Y, Xu CC, Lin X, Ye FB, et al., Systemic administration of exosomes released from mesenchymal stromal cells attenuates apoptosis, inflammation, and promotes angiogenesis after spinal cord injury in rats. J Neurotrauma. (2017) 34:3388–96. doi: 10.1089/neu.2017.5063
36. KneŽević NŽ, Durand J-V. Large pore mesoporous silica nanomaterials for application in delivery of biomolecules. Nanoscale. (2015) 7:2199–209. doi: 10.1039/C4NR06114D
37. Cho Y, Shi R, Ivanisevic A, Borgens RB. Functional silica nanoparticle-mediated neuronal membrane sealing following traumatic spinal cord injury. J Neurosci Res. (2010) 88:1433–44. doi: 10.1002/jnr.22309
38. Dengler EC, Liu J, Kerwin A, Torres S, Olcott CM, Bowman BN, et al. Mesoporous silica-supported lipid bilayers (protocells) for DNA cargo delivery to the spinal cord. J Controll Release. (2013) 168:209–24. doi: 10.1016/j.jconrel.2013.03.009
39. Tang ZK, Zhang L, Wang N, Zhang XX, Wen GH, Li GD, et al. Superconductivity in 4 angstrom single-walled carbon nanotubes. Science. (2001) 292:2462–5. doi: 10.1126/science.1060470
40. Jo DH, Kim JH, Lee TG, Kim JH. Size, surface charge, and shape determine therapeutic effects of nanoparticles on brain and retinal diseases. Nanomed Nanotechnol Biol Med. (2015) 11:1603–11. doi: 10.1016/j.nano.2015.04.015
41. Yue ZG, Wei W, Lv PP, Yue H, Wang LY, Su ZG, et al. Surface charge affects cellular uptake and intracellular trafficking of chitosan-based nanoparticles. Biomacromolecules. (2011) 12:2440–6. doi: 10.1021/bm101482r
42. Xiao K, Li Y, Luo J, Lee JS, Xiao W, Gonik AM, et al. The effect of surface charge on in vivo biodistribution of PEG-oligocholic acid based micellar nanoparticles. Biomaterials. (2011) 32:3435–46. doi: 10.1016/j.biomaterials.2011.01.021
43. Anderson KD, Guest JD, Dietrich WD, Bartlett Bunge M, Curiel R, Dididze M, et al. Safety of autologous human schwann cell transplantation in subacute thoracic spinal cord injury. J Neurotrauma. (2017) 34:2950–63. doi: 10.1089/neu.2016.4895
44. Vaněček V, Zablotskii V, Forostyak S, RuŽička J, Herynek V, Babič M, et al. Highly efficient magnetic targeting of mesenchymal stem cells in spinal cord injury. Int J Nanomed. (2012) 7:3719–30. doi: 10.2147/IJN.S32824
45. Tukmachev D, Lunov O, Zablotskii V, Dejneka A, Babic M, Syková E, et al. An effective strategy of magnetic stem cell delivery for spinal cord injury therapy. Nanoscale. (2015) 7:3954–8. doi: 10.1039/C4NR05791K
46. Doria G, Conde J, Veigas B, Giestas L, Almeida C, Assunção M, et al. Noble metal nanoparticles for biosensing applications. Sensors. (2012) 12:1657–87. doi: 10.3390/s120201657
47. Baranes K, Shevach M, Shefi O, Dvir T. Gold nanoparticle-decorated scaffolds promote neuronal differentiation and maturation. Nano Lett. (2016) 16:2916–20. doi: 10.1021/acs.nanolett.5b04033
48. Paviolo C Haycock JW, Yong J, Yu A, Stoddart PR, McArthur SL. Laser exposure of gold nanorods can increase neuronal cell outgrowth. Biotechnology and bioengineering, (2013) 110:2277–91. doi: 10.1002/bit.24889
49. Jokerst JV, Lobovkina T, Zare RN, Gambhir SS. Nanoparticle PEGylation for imaging and therapy. Nanomedicine. (2011) 6:715–28. doi: 10.2217/nnm.11.19
50. Agarwal R, Domowicz MS, Schwartz NB, Henry J, Medintz I, Delehanty JB, et al. Delivery and tracking of quantum dot peptide bioconjugates in an intact developing avian brain. ACS Chem Neurosci. (2015) 6:494–504. doi: 10.1021/acschemneuro.5b00022
51. Pathak S, Tolentino R, Nguyen K, D'Amico L, Barron E, Cheng L, et al. Quantum dot labeling and imaging of glial fibrillary acidic protein intermediate filaments and gliosis in the rat neural retina and dissociated astrocytes. J Nanosci Nanotechnol. (2009) 9:5047–54. doi: 10.1166/jnn.2009.GR08
52. Matsuyama K, Ihsan N, Irie K, Mishima K, Okuyama T, Muto H. Bioimaging application of highly luminescent silica-coated ZnO-nanoparticle quantum dots with biotin. J Colloid Interface Sci. (2013) 399:19–25. doi: 10.1016/j.jcis.2013.02.047
53. Kreuter J. Drug delivery to the central nervous system by polymeric nanoparticles: what do we know? Adv Drug Deliv Rev. (2014) 71:2–14. doi: 10.1016/j.addr.2013.08.008
54. Rollerova E, Jurcovicova J, Mlynarcikova A, Szabova E, Kovriznych J, Zeljenkova D. Polymeric nanoparticles - targeted drug delivery systems for treatment of CNS disorders and their possible endocrine disrupting activities. Endocr Regul. (2011) 45:49–60.
55. Elliott Donaghue I, Shoichet MS. Controlled release of bioactive PDGF-AA from a hydrogel/nanoparticle composite. Acta Biomater. (2015) 25:35–42. doi: 10.1016/j.actbio.2015.08.002
56. Chen B, Bohnert D, Borgens RB, Cho Y. Pushing the science forward: chitosan nanoparticles and functional repair of CNS tissue after spinal cord injury. J Biol Eng. (2013) 7:1–9. doi: 10.1186/1754-1611-7-15
57. Xu L, Zhang H, Wu Y. Dendrimer advances for the central nervous system delivery of therapeutics. ACS Chem Neurosci. (2014) 5:2–13. doi: 10.1021/cn400182z
58. He H, Li Y, Jia XR, Du J, Ying X, Lu WL, et al. PEGylated Poly(amidoamine) dendrimer-based dual-targeting carrier for treating brain tumors. Biomaterials. (2011) 32:478–87. doi: 10.1016/j.biomaterials.2010.09.002
59. Cerqueira SR, Oliveira JM, Silva NA, Leite-Almeida H, Ribeiro-Samy S, Almeida A, et al. Microglia response and in vivo therapeutic potential of methylprednisolone-loaded dendrimer nanoparticles in spinal cord injury. Small. (2013) 9:738–49. doi: 10.1002/smll.201201888
60. Lasa-Saracibar B, Estella-Hermoso de Mendoza A, Guada M, Dios-Vieitez C, Blanco-Prieto MJ. Lipid nanoparticles for cancer therapy: state of the art and future prospects. Expert Opin Drug Deliv. (2012) 9:1245–61. doi: 10.1517/17425247.2012.717928
61. Ding S, Bao Y, Lin Y, Pan Y, Fan Y, Wan J, et al. Neuroprotective effect of functionalized multi-walled carbon nanotubes on spinal cord injury in rats. Int J Clin Exp Pathol. (2015) 8:15769–77.
62. Ding RG, Lu GQ, Yan ZF, Wilson MA. Recent advances in the preparation and utilization of carbon nanotubes for hydrogen storage. J Nanosc Nanotechnol. (2001) 1:7–29. doi: 10.1166/jnn.2001.012
63. Roman JA, Niedzielko TL, Haddon RC, Parpura V, Floyd CL. Single-walled carbon nanotubes chemically functionalized with polyethylene glycol promote tissue repair in a rat model of spinal cord injury. J Neurotrauma. (2011) 28. doi: 10.1089/neu.2010.1409
64. Dasari VR, Veeravalli KK, Dinh DH. Mesenchymal stem cells in the treatment of spinal cord injuries: a review. World J Stem Cells. (2014) 6:120–33. doi: 10.4252/wjsc.v6.i2.120
65. Seo JH, Cho S-R. Neurorestoration induced by mesenchymal stem cells: potential therapeutic mechanisms for clinical trials. Yonsei Med J. (2012) 53:1059–67. doi: 10.3349/ymj.2012.53.6.1059
66. Harris DT. stem cell banking for regenerative and personalized medicine. Biomedicines. (2014) 2:50–79. doi: 10.3390/biomedicines2010050
67. Hejcl A, Jendelova P, Sames M, Sykova E. The use of mesenchymal stem cells in the experimental and clinical therapy of spinal cord injury. Ceska Slov Neurol Neurochirur. (2014) 77:560–7.
68. Jaramillo-Merchán J, Jones J, Ivorra JL, Pastor D, Viso-León MC, Armengól JA, et al., Mesenchymal stromal-cell transplants induce oligodendrocyte progenitor migration and remyelination in a chronic demyelination model. Cell Death Dis. (2013) 4:e779. doi: 10.1038/cddis.2013.304
69. Castillo-Melendez M, Yawno T, Jenkin G, Miller SL. Stem cell therapy to protect and repair the developing brain: a review of mechanisms of action of cord blood and amnion epithelial derived cells. Front Neurosci. (2013) 7:194. doi: 10.3389/fnins.2013.00194
70. Chiossone L, Conte R, Spaggiari GM, Serra M, Romei C, Bellora F, et al. Mesenchymal stromal cells induce peculiar alternatively activated macrophages capable of dampening both innate and adaptive immune responses Stem Cells. (2016) 34:1909–21. doi: 10.1002/stem.2369
71. Uchida S, Hayakawa K, Ogata T, Tanaka S, Kataoka K, Itaka K. Treatment of spinal cord injury by an advanced cell transplantation technology using brain-derived neurotrophic factor-transfected mesenchymal stem cell spheroids. Biomaterials. (2016) 109:1–11. doi: 10.1016/j.biomaterials.2016.09.007
72. Lindvall O, Kokaia Z. Stem cells for the treatment of neurological disorders. Nature. (2006) 441:1094–6. doi: 10.1038/nature04960
73. Sasaki H, Tanaka N, Nakanishi K, Nishida K, Hamasaki T, Yamada K, et al. Therapeutic effects with magnetic targeting of bone marrow stromal cells in a rat spinal cord injury model. Spine. (2011) 36:933–8. doi: 10.1097/BRS.0b013e3181eb9fb0
74. Vishwakarma SK, Bardia A, Paspala SA, Khan AA. Magnetic nanoparticle tagged stem cell transplantation in spinal cord injury: a promising approach for targeted homing of cells at the lesion site. Neurol India. (2015) 63:460–1. doi: 10.4103/0028-3886.158294
75. Pangestuti R, Kim S-K. Neuroprotective properties of chitosan and its derivatives. Mar Drugs. (2010) 8:2117–28. doi: 10.3390/md8072117
76. Srinivasan M, Sudheer AR, Menon VP. Ferulic Acid: therapeutic potential through its antioxidant property. J Clin Biochem Nutr. (2007) 40:92–100. doi: 10.3164/jcbn.40.92
77. Wu W, Lee S-Y, Wu X, Tyler JY, Wang H, Ouyang Z, et al. Neuroprotective ferulic acid (FA)-glycol chitosan (GC) nanoparticles for functional restoration of traumatically injured spinal cord. Biomaterials. (2014) 35:2355–64. doi: 10.1016/j.biomaterials.2013.11.074
78. Kim HY, Kumar H, Jo MJ, Kim J, Yoon JK, Lee JR, et al. Therapeutic efficacy-potentiated and diseased organ-targeting nanovesicles derived from mesenchymal stem cells for spinal cord injury treatment. Nano Lett. (2018) 18:4965–75. doi: 10.1021/acs.nanolett.8b01816
79. Lee HJ, An J, Doo SW, Kim JH, Choi SS, Lee SR, et al., Improvement in spinal cord injury-induced bladder fibrosis using mesenchymal stem cell transplantation into the bladder wall. Cell Transplant. (2015) 24:1253–63. doi: 10.3727/096368914X682125
80. Bonilla P, Hernandez J, Giraldo E, González-Pérez MA, Alastrue-Agudo A, Elkhenany H, et al. Human-induced neural and mesenchymal stem cell therapy combined with a curcumin nanoconjugate as a spinal cord injury treatment. Int J Mol Sci. (2021) 22:5966. doi: 10.3390/ijms22115966
81. Zarepour A, Bal Öztürk A, Koyuncu Irmak D, Yaşayan G, Gökmen A, Karaöz E, et al., Combination therapy using nanomaterials and stem cells to treat spinal cord injuries. Eur J Pharm Biopharm. (2022) 177:224–40. doi: 10.1016/j.ejpb.2022.07.004
82. Zhang B, Yan W, Zhu Y, Yang W, Le W, Chen B, et al. Nanomaterials in neural-stem-cell-mediated regenerative medicine: imaging and treatment of neurological diseases. Adv Mater. (2018) 30:1705694. doi: 10.1002/adma.201705694
83. Boisselier E, Astruc D. Gold nanoparticles in nanomedicine: preparations, imaging, diagnostics, therapies and toxicity. Chem Soc Rev. (2009) 38:1759–82. doi: 10.1039/b806051g
84. Han GH, Ko WK, Kim SJ, Lee D, Jeong D, Han I, et al., Neuron-inducing therapy using embryonic neural progenitor cells embedding positively charged gold nanoparticles in rats with complete spinal cord injury. Clin Transl Med. (2022) 12:e981. doi: 10.1002/ctm2.981
85. Wang D, Wang K, Liu Z, Wang Z, Wu H. Valproic acid labeled chitosan nanoparticles promote the proliferation and differentiation of neural stem cells after spinal cord injury. Neurotox Res. (2021) 39:456–6. doi: 10.1007/s12640-020-00304-y
86. Pang M, Shu T, Chen R, Liu C, He L, Yang Y, et al. Neural precursor cells generated from Induced pluripotent stem cells with gelatin sponge-electrospun PLGA/PEG nanofibers for spinal cord injury repair. Int J Clin Exp Med. (2016) 9:1–10.
87. Li L, Adnan H, Xu B, Wang J, Wang C, Li F, Tang K. Effects of transplantation of olfactory ensheathing cells in chronic spinal cord injury: a systematic review and meta-analysis. Eur Spine J. (2015) 24:919–30. doi: 10.1007/s00586-014-3416-6
88. Tabakow P, Raisman G, Fortuna W, Czyz M, Huber J, Li D, et al. Functional regeneration of supraspinal connections in a patient with transected spinal cord following transplantation of bulbar olfactory ensheathing cells with peripheral nerve bridging. Cell Transplant. (2014) 23:1631–55. doi: 10.3727/096368914X685131
89. Gomez RM, Sanchez MY, Portela-Lomba M, Ghotme K, Barreto GE, Sierra J, et al. Cell therapy for spinal cord injury with olfactory ensheathing glia cells (OECs). Glia. (2018) 66:1267–301. doi: 10.1002/glia.23282
90. Roxana R-B, Karla S-Z, Julián G-S, Lisset Karina N-T, Estefanía de la Cruz C, Elisa G-V. Transplantation or transference of cultured cells as a treatment for spinal cord injury. In:Antonio I, Elisa G-V, Gabriel G-S, , editors. Spinal Cord Injury Therapy. Rijeka: IntechOpen (2019). Ch. 7.
91. Tang YY, Guo WX, Lu ZF, Cheng MH, Shen YX, Zhang YZ. Ginsenoside Rg1 promotes the migration of olfactory ensheathing cells via the PI3K/Akt pathway to repair rat spinal cord injury. Biol Pharm Bull. (2017) 40:1630–7. doi: 10.1248/bpb.b16-00896
92. Ao Q, Wang AJ, Chen GQ, Wang SJ, Zuo HC, Zhang XF. Combined transplantation of neural stem cells and olfactory ensheathing cells for the repair of spinal cord injuries. Med Hypoth. (2007) 69:1234–7. doi: 10.1016/j.mehy.2007.04.011
93. Azizi M, Farahmandghavi F, Joghataei MT, Zandi M, Imani M, Bakhtiari M, et al. ChABC-loaded PLGA nanoparticles: a comprehensive study on biocompatibility, functional recovery, and axonal regeneration in animal model of spinal cord injury. Int J Pharm. (2020) 577:119037. doi: 10.1016/j.ijpharm.2020.119037
Keywords: nanomaterials, nanoparticles, cellular therapy, spinal cord injury, combinatory therapy
Citation: García E, Sánchez-Noriega S, González-Pacheco G, González-Vázquez AN, Ibarra A and Rodríguez-Barrera R (2023) Recent advances in the combination of cellular therapy with stem cells and nanoparticles after a spinal cord injury. Front. Neurol. 14:1127878. doi: 10.3389/fneur.2023.1127878
Received: 20 December 2022; Accepted: 06 March 2023;
Published: 26 April 2023.
Edited by:
Filippo Rossi, Polytechnic University of Milan, ItalyReviewed by:
Wenyan Li, Army Medical University, ChinaChengyan Chu, Dalian Municipal Central Hospital, China
Copyright © 2023 García, Sánchez-Noriega, González-Pacheco, González-Vázquez, Ibarra and Rodríguez-Barrera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roxana Rodríguez-Barrera, roxana.rodriguezb@anahuac.mx