 Ana Luisa Corona-Nakamura1
Ana Luisa Corona-Nakamura1 Martha Judith Arias-Merino2Eleazar Iván Ávila-Esparza1María de Lourdes Tolentino-Corona1César Cuauhtémoc Cañedo-Castañeda3Héctor Enrique Flores-Salinas1Juan Fernando Corona-Macías4Martha Elena Vázquez-Arias4*
Martha Judith Arias-Merino2Eleazar Iván Ávila-Esparza1María de Lourdes Tolentino-Corona1César Cuauhtémoc Cañedo-Castañeda3Héctor Enrique Flores-Salinas1Juan Fernando Corona-Macías4Martha Elena Vázquez-Arias4*- 1Department of Internal Medicine, Mexican Institute of Social Security, Western National Medical Center, High Specialty Medical Unit, Guadalajara, Mexico
- 2Research Committee, Western Clinical Research Institute, Zapopan, Mexico
- 3Department of Neurosurgery, Mexican Institute of Social Security, Western National Medical Center, High Specialty Medical Unit, Guadalajara, Mexico
- 4University Center for Health Sciences, University of Guadalajara, Guadalajara, Mexico
Introduction: Nosocomial infectious ventriculitis caused by multidrug-resistant (MDR) Gram-negative bacilli associated with external ventricular drainage (EVD) placement poses a significant mortality burden and hospital costs.
Objectives: This study aims to analyze the characteristics, ventriculitis evolution, treatment, and outcomes of patients with ventriculitis due to MDR Gram-negative bacilli associated with EVD placement.
Methods: A retrospective cohort study focusing on patients with nosocomial infection caused by MDR Gram-negative bacilli while on EVD was conducted from 2019 to 2022. Medical, laboratory, and microbiological records were collected. The antibiotic resistance of the Gram-negative bacilli isolated in the cerebrospinal fluid (CSF) of patients was analyzed. The risk factors were identified using univariate risk models and were analyzed using survival curves (Cox regression). An adjusted Cox proportional hazards model was also constructed.
Results: Among 530 patients with suspected EVD-associated ventriculitis, 64 patients with isolation of Gram-negative bacilli in CSF were included. The estimated mortality was 78.12%. Hemorrhages (intracranial, subarachnoid, and intraventricular) were observed in 69.8% of patients. Acinetobacter baumannii, Klebsiella pneumoniae, and Pseudomonas aeruginosa were the most frequently isolated bacilli. In the univariate analysis, significant risk factors for mortality included arterial hypertension, a Glasgow Coma Scale (GCS) score of ≤ 8, invasive mechanical ventilation (IMV) upon hospital admission and during hospitalization, septic shock, and ineffective treatment. The adjusted Cox proportional hazards model revealed that septic shock (HR = 3.3, 95% CI = 1.5–7.2; p = 0.003) and ineffective treatment (HR = 3.2, 1.6–6.5, 0.001) were significant predictors. A high resistance to carbapenems was found for A. baumannii (91.3%) and P. aeruginosa (80.0%). Low resistance to colistin was found for A. baumannii (4.8%) and P. aeruginosa (12.5%).
Conclusion: Ineffective treatment was an independent hazard factor for death in patients with ventriculitis caused by MDR Gram-negative bacilli associated with EVD.
Introduction
Antimicrobial resistance is one of the significant threats to global public health. The World Health Organization estimated that antimicrobial resistance was directly attributable to 1.27 million deaths worldwide in 2019 (1). Among healthcare-associated postoperative infections, patients with neuroinfections experience prolonged hospital stays, along with high hospital costs, and are at a high risk of death (2–4). Among these neuroinfections, ventriculitis associated with external ventricular drain (EVD) placement has a reported prevalence between 0% and 22% (2, 5).
EVDs serve as a common temporary treatment in patients who have high intracranial pressure secondary to acute hydrocephalus caused by blockage of the cerebrospinal fluid (CSF) circulation. Generally, such blockage are caused by tumor obstruction, followed by chronic infectious meningitis, hemorrhage (intraventricular, subarachnoid, and intracranial), cranial trauma, CSF leak, and decompressive craniectomy (2, 6, 7).
Placement of a foreign body into a normally sterile (e.g., ventricular) cavity facilitates the entry of skin flora and pathogenic microorganisms present in the hospital environment. Patients who have undergone ventriculostomy are highly vulnerable because of their underlying condition and can acquire a nosocomial infection (frequently caused by multidrug-resistant (MDR) microorganisms). In addition, many antibiotics may not penetrate the ventricles (8).
Tunkel et al. (2) reported four mechanisms that occur most frequently in CSF shunts that enable a patient to acquire infections: (a) colonization of the shunt at the time of surgery, (b) retrograde infection from the distal end of the shunt, (c) through the skin while inserting a needle to collect CSF for culture or injecting a drug into the ventricular reservoir and (d) hematogenous seeding due to bacteremia. Sweid et al. (9) reported EVD replacement, CSF leak, and prolonged stay in the hospital to be risk factors associated with a higher risk of ventriculostomy infection.
New headaches, fever, nausea, vomiting, lethargy, and changes in mental status may be indicative of infectious ventriculitis. However, patients who have suffered a hemorrhage or who have a subarachnoid tumor may also present these clinical features (2).
Often, the diagnosis of ventriculitis is difficult to establish because it has an insidious onset and patients have unusual symptoms (10). The most important test to establish the diagnosis of ventriculitis is CSF culture. According to the Infectious Diseases Society of America (IDSA), several features are indicative of an infection associated with an EVD: single or multiple positive CSF cultures, pleocytosis and/or hypoglycorrhachia, and clinical symptoms suggesting ventriculitis or meningitis (2).
The most frequent bacterial pathogens isolated in the CSF of patients with ventriculitis associated with EVD use are skin commensals, such as coagulase-negative Staphylococcus species (including Staphylococcus aureus) and Gram-negative bacilli, such as Acinetobacter baumannii, Pseudomonas aeruginosa, Klebsiella pneumoniae, and Escherichia coli (3, 5). Solo-Peleteiro et al. (11) reported 75 bacterial isolates from CSF samples from patients with EVD-associated ventriculitis and found that nearly 65% of them corresponded to Gram-positive cocci and 28% to Gram-negative bacilli (most frequently E. coli, A. baumannii, and K. pneumoniae).
Studies of the problems associated with nosocomial infections (particularly infections caused by MDR Gram-negative bacilli) can clarify the risk factors of nosocomial infections, formulation of pathogen-surveillance protocols, and risk of death. The aim of this study was to enrich national/international information on these topics to provide useful data to improve daily clinical practice in hospitals.
Materials and methods
A retrospective cohort study was designed covering the period 2019–2022. We included hospitalized patients who had undergone a neurosurgical procedure, who required an EVD, and who presented with nosocomial ventriculitis caused by MDR Gram-negative bacilli.
The present study was designed in two sections. In the first section, we analyzed data from patients selected according to the following case definition: Patients with CSF culture positive for Gram-negative bacilli (with isolation of a single type of bacteria) collected in the operation theater during replacement of an EVD in the first event of nosocomial infection.
“Nosocomial ventriculitis” was defined to originate after a neurosurgical procedure (placement/replacement of an EVD) in the hospital. Clinical suspicion of infection was based on IDSA criteria: (1) having a positive CSF culture (for Gram-negative bacilli isolates); (2) having at least two of the following symptoms: new or worsening altered mental status (the presence of a new headache, nausea, lethargy, and/or altered state of consciousness); and fever (>38.0°C) in the absence of another focus of infection. The cytochemical analysis of CSF was done to identify hypoglycorrhachia, hyperproteinorrachia, and pleocytosis. Magnetic resonance imaging and computed tomography of the cranium were used only to make a differential diagnosis (these data were not included in the present study) (2, 12).
The inclusion criteria were patients aged ≥17 years having nosocomial ventriculitis after neurosurgery caused by EVD replacement by Neurosurgery and Infectious Diseases Services. Positivity of CSF culture found after EVD replacement was considered (IDSA criteria). The exclusion criteria were as follows: patients with post-neurosurgical ventriculitis due to placement/replacement of an internal ventricular drain (ventriculoperitoneal shunt valve) and those with incomplete medical records (2). Data for the study were collected from medical, laboratory, and microbiological records.
Several variables were studied, including the primary disease that necessitated ventriculostomy as well as conditions upon hospital admission (hereafter termed “admission”) and during hospitalization: neurological status (based on the Glasgow Coma Scale (GCS) score; invasive mechanical ventilation (IMV); septic shock; number of ventriculostomies; EVD duration (days); hospitalization duration; evolution of ventriculitis; treatment; outcomes; and laboratory and microbiological findings). Patients were divided into two groups: “survivors” and “non-survivors.”
The mortality prognostic factors of patients with ventriculitis selected based on isolated Gram-negative bacilli were also analyzed. Upon admission, these prognostic factors included a low GCS score (3–8), a history of arterial hypertension, and IMV. During hospitalization, these prognostic factors included the number of ventriculostomies before infection, presentation of septic shock, resistance to carbapenems, and receiving ineffective treatment (non-efficacious treatment). The latter understood was in relation to the presence of MDR Gram-negative bacilli (with resistance to ≥3 families of antibiotics), particularly resistance to carbapenems, and patients who received a suboptimal dose of polymyxin E (colistin; <14 days) (13, 14).
In the second section, a complementary analysis of the Gram-negative bacilli isolated from the CSF samples was done. Positive cultures taken through the EVD outside theater were excluded. We also excluded CSF samples considered to be contaminated or that had been colonized by pathogens. Positive CSF cultures from patients without symptoms of infection or pleocytosis and/or hypoglycorrhachia were considered to be contaminated. Colonization was considered if multiple CSF cultures or positive Gram stains were found with a normal CSF cell count without clinical symptoms suggesting ventriculitis or if normal concentrations of glucose and protein in CSF were observed (2).
Parameters set by the Clinical and Laboratory Standards Institute (CLSI) and the European Committee on Antimicrobial Susceptibility Testing (EUCAST, 2020) were used to interpret antibiotic susceptibility. The epidemiological cutoff values (minimum inhibitory concentration of wild-type organisms) were ≥2 mg/L for the most important members of Enterobacteriaceae and Acinetobacter species and ≥4 mg/L for P. aeruginosa (15).
Statistical analyses
In the first section, a description of the demographic variables, primary disease, and clinical status of patients upon admission and during hospitalization, ventriculitis evolution, treatment, and outcomes was made. The microbiological and cytochemical findings of CSF were also documented. The frequency distribution of data was analyzed by the Kolmogorov–Smirnov test. Median values and interquartile ranges (IQRs) were used if the data did not have a normal distribution. The receiver operating characteristics (ROC) curves were created to establish points between survivors and non-survivors in terms of quantitative variables. Using a univariate model, a risk analysis was carried out between survivors and non-survivors. Significant mortality risk factors were analyzed using survival curves (Cox regression) considering admission as the initial time and patient death as the final event. The effects of the set of variables suggesting a death poor prognosis on the hazard ratio (HR) were analyzed through the construction of an adjusted Cox proportional hazards model (p < 0.05). An additional univariate analysis was undertaken to analyze the factors suggesting a poor prognosis for patients with ventriculitis based on isolated Gram-negative bacilli.
In the second section, resistance to different antibiotics by bacterial isolates in CSF was described. The resistance found according to isolated Gram-negative bacilli, as well as risk estimation by univariate analysis, was also described.
Univariate analyses were done using the Mann–Whitney U-test. Qualitative variables were examined using the χ2 test or Fisher's exact test. The results were considered significant if the p < 0.05. SPSS 25 (IBM, Armonk, NY, USA) was employed for statistical analyses.
Results
Of 530 patients with suspected ventriculitis associated with an EVD between 2019 and 2022, 791 isolates from CSF samples were obtained. A total of 415 patients (78.3%) with negative cultures were excluded. Of the remaining patients, 115 (21.7%) had 376 positive cultures. A total of 112 isolates were eliminated from patients with positive cultures for Gram-positive cocci or bacilli and fungi and 102 (91.1%) from patients with positive cultures for Gram-positive cocci. Of the 264 samples in which Gram-negative bacilli were found, A. baumannii was found in 102 (38.6%). According to the case definition, 64 patients were included in our analysis (Figure 1).
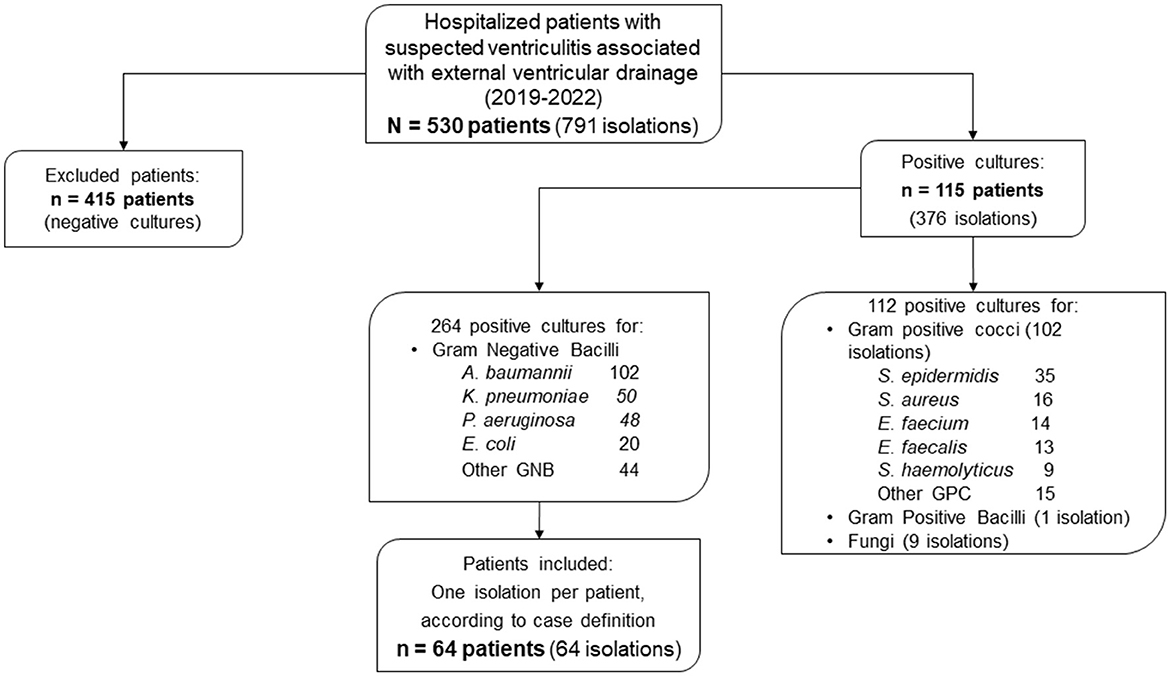
Figure 1. Participant flowchart.
All EVDs were replaced in theater. In all cases, the type of catheter replaced was not impregnated with antibiotics or silver nanoparticles.
The median age of patients was 51 (range, 17–82) years, and 33 were men (51.6%). The group of non-survivors was 50/64 patients (78.12%).
Hemorrhagic brain events (intracranial, subarachnoid, or intraventricular hemorrhage; 69.8%), decompressive craniectomy (31.7%) aneurysm (22.2%), CSF fistula (20.6%), ischemic stroke (16.1%), obstructive brain tumor (14.3%), traumatic brain injury (12.9%), arteriovenous malformation (12.7%), brain herniation (3.2%), and tubercular meningitis (1.6%) were the primary diseases suffered by the patients.
Upon admission, 52 patients (81.3%) had hydrocephalus. Arterial hypertension was found in 29 out of 63 (46.0%) of cases. Forty-six patients (73%) were found to have neurological deficits. Twenty-four patients (39.3%) had a GCS score of 3–8. Twenty-six patients (44.8%) required IMV upon admission. During hospitalization, 47 patients required IMV (78.3%) and 31 patients (49.2%) presented with septic shock. The duration of hospitalization was 3–169 (median, 30; IQR, 14–50) days. A median of 10 (IQR, 7–16) days for each ventriculostomy per patient was estimated (Table 1). All CSF samples had pleocytosis, with a median of 695 (IQR, 131–2173) cells/μL and 66.7% had ≥200 cells/μL. In addition, 57.1% of samples had hypoglycorrhachia (<0.30 g/L), and hyperproteinorrachia (≥1 g/L) was noted in 87.3% of samples.
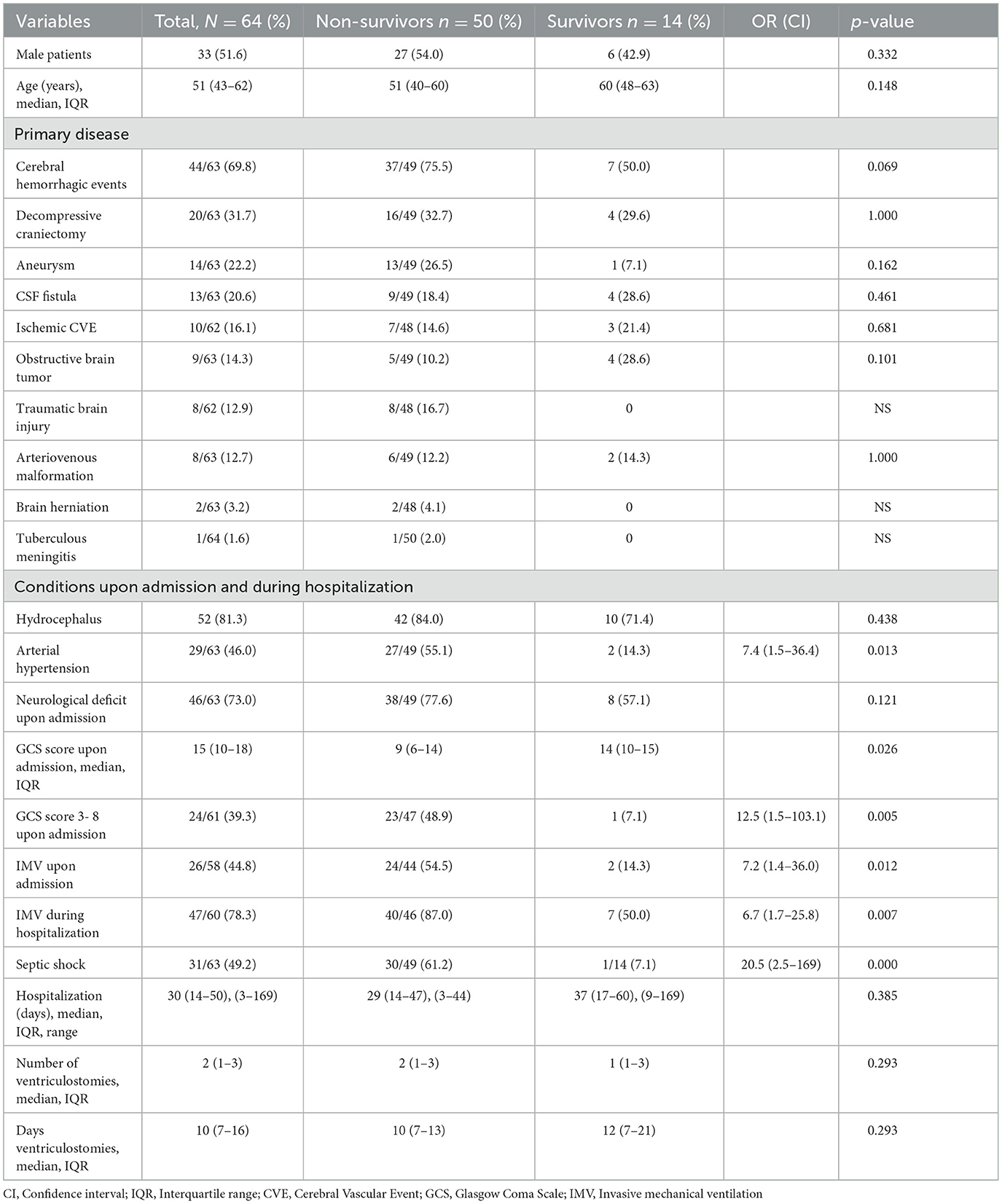
Table 1. Demographic characteristics, comorbidities, and complications of patients with ventriculitis due to MDR Gram-negative bacilli.
In CSF cultures, 26 (40.6%) were positive for A. baumannii, 11 (17.2%) for K. pneumoniae, 10 (15.6%) for P. aeruginosa, 8 (12.5%) for E. coli, and the remaining 9 (14.1%) for other Gram-negative bacilli (Enterobacter cloacae, Stenotrophomonas maltophilia, Proteus mirabilis, and Pseudomonas stutzeri).
We discovered that 32 out of 58 samples (55.2%) showed resistance to carbapenems, 31 out of 57 (54.4%) to meropenem, 56 out of 61 (91.8%) to third-generation cephalosporins, and 45 out of 60 (75.0%) to cefepime. Resistance to quinolones was noted in 46 out of 58 (79.3%) of samples, 37 out of 58 (63.8%) to aminoglycosides, 24 out of 55 (43.6%) to tigecycline, and 5 out of 47 (10.6%) to colistin (Table 2).
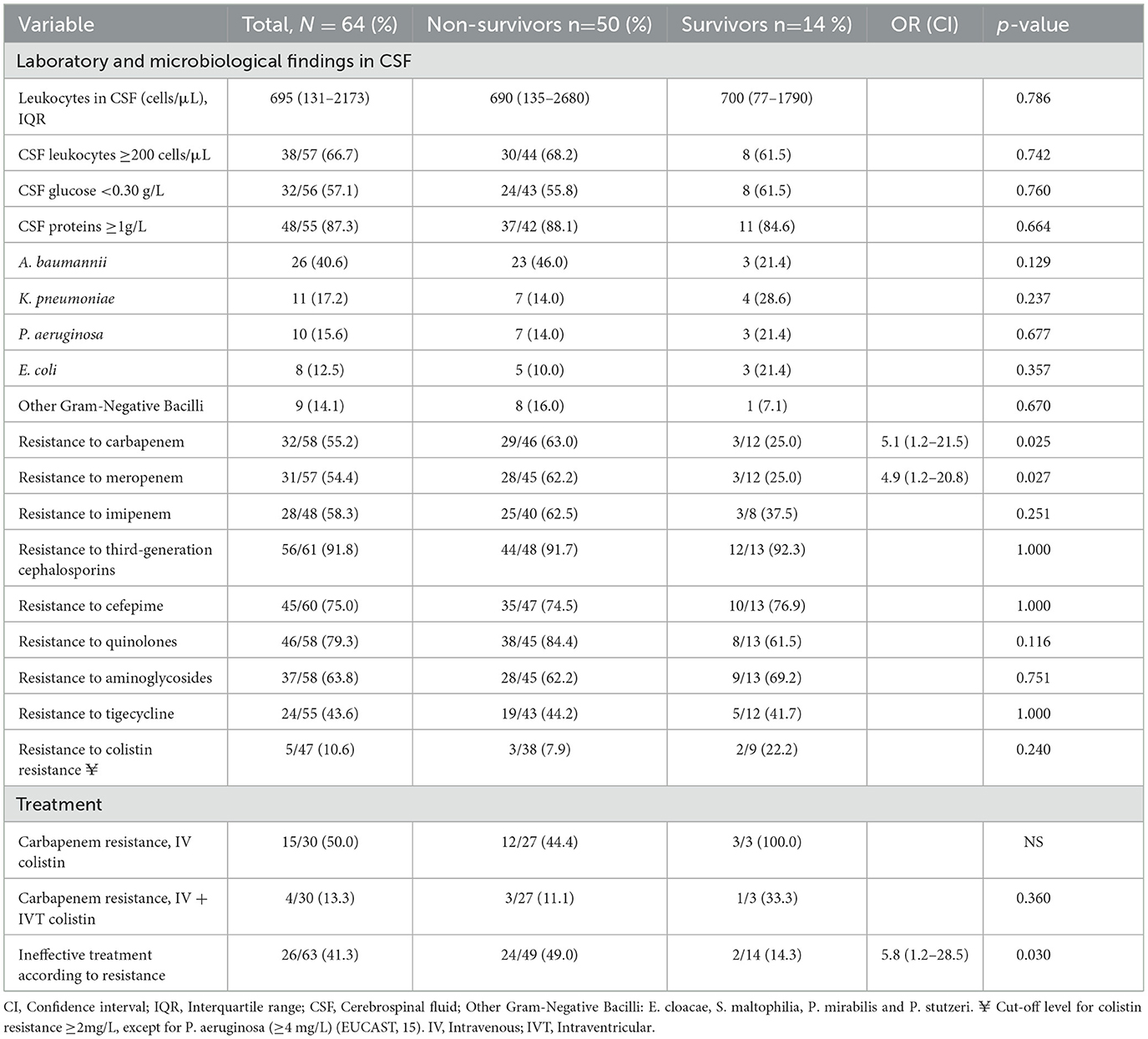
Table 2. Cytochemical and microbiological findings in CSF and treatment of patients with ventriculitis due to MDR Gram-negative bacilli.
In the univariate analysis, several risk factors were associated with death: having arterial hypertension [odds ratio (OR) = 7.4, 95% confidence interval (CI) = 1.5–36.4, p = 0.013]; a GCS score of 3–8 (12.5, 1.5–103, 0.005); IMV upon admission (7.2, 1.4–36.0, 0.012); IMV during hospitalization (6.7, 1.7–25.8, 0.007); septic shock (20.5, 2.5–169, 0.000) (Table 1).
In relation to the univariate analysis of the resistance of Gram-negative bacilli to antibiotics, resistance to carbapenems (5.1, 1.2–21.5, 0.025) and meropenem (4.9, 1.2–20.8, 0.027) was significant. Receiving ineffective treatment (non-effective treatment) in relation to antibiotic resistance was also a risk factor associated with death (5.8, 1.2–28.5, 0.030) (Table 2).
To construct the adjusted Cox model, several prognostic variables that were significant in the univariate analysis were taken into consideration: arterial hypertension, low GCS score upon admission, IMV upon admission and during hospitalization, septic shock, and ineffective treatment. Table 3 shows the results of the adjusted Cox proportional hazards model. Septic shock (HR = 3.3, CI 1.5–7.2, p = 0.003) and ineffective treatment (HR = 3.2, CI 1.6–6.5, p = 0.001) were significant. The patient survival graphs of these two hazard conditions for mortality are shown in Figure 2.
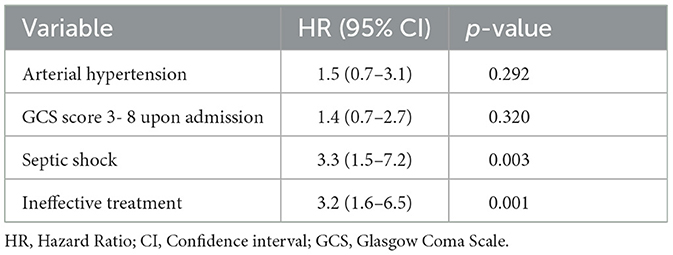
Table 3. Adjusted Cox proportional hazards model.
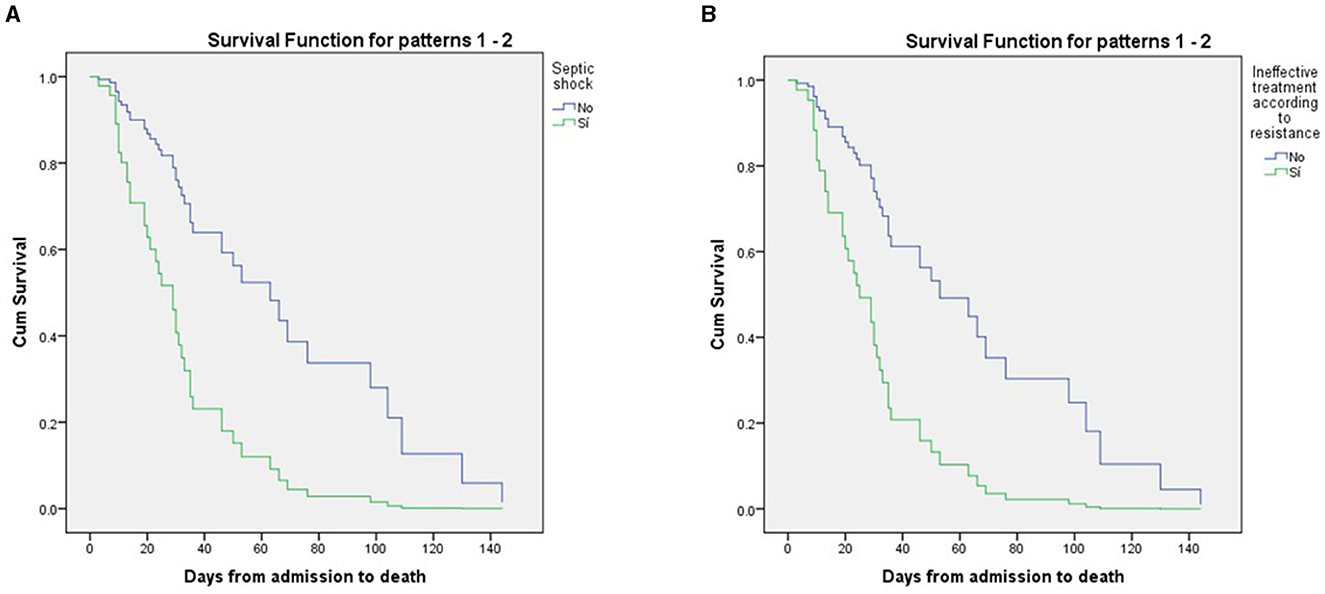
Figure 2. Patients survival analysis using cox regression (A) Septic shock and (B) ineffective treatment.
Table 4 shows the factors leading to a poor prognosis according to Gram-negative bacilli most frequently observed in isolates from the CSF cultures of patients, and the main bacteria were A. baumannii, P. aeruginosa, K. pneumoniae, and E. coli. Carbapenem resistance was reported in 21 out of 23 (91.3%) of A. baumannii isolates and 23 out of 26 (88.5%) of A. baumannii isolates were from non-survivors. For patients with A. baumannii isolates, the requirement for IMV upon admission (OR = 4.9, CI = 1.6–15.3, p = 0.006), as well as the resistance to carbapenems for A. baumannii (OR = 22.9, CI = 4.6–115.4, p = 0.000) were estimated to be risk factors.
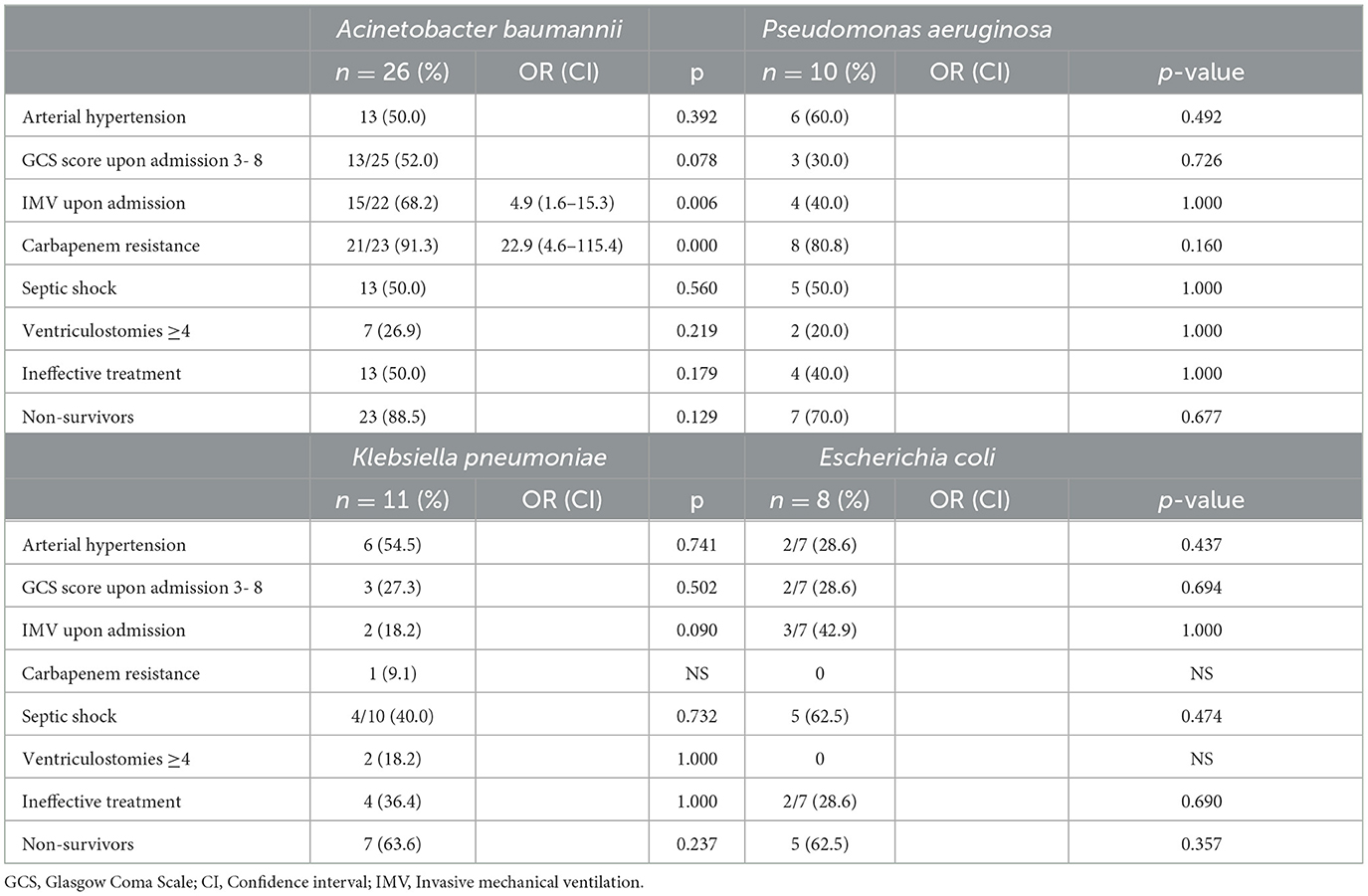
Table 4. Poor prognostic factors in patients with ventriculitis due to external ventricular drain (2019–2022).
Gram-negative bacilli isolated
The following resistances of the selected isolates to different antibiotics were found: 91.8% for cephalosporins, ceftriaxone (84.6%), ceftazidime (80.0%), cefepime (75.0%); 79.3% for ciprofloxacin; 74.0% for ampicillin/sulbactam; 73.3% for aztreonam; 53.3% for gentamicin; and 55.2% for carbapenems (imipenem 58.3%, meropenem 54.4%). The highest sensitivities were obtained for colistin (resistance of 10.6%) followed by amikacin (resistance of 40%) (Table 5).

Table 5. Resistance to antibiotics of all isolated bacilli in patients with ventriculitis (2019–2022).
Table 6 shows the antimicrobial resistance described for each isolated Gram-negative bacillus. For A. baumannii, resistance was found to piperacillin/tazobactam, third-generation cephalosporins and amikacin (100%), ciprofloxacin (96.0%), cefepime (92.3%), carbapenems (91.3%) (meropenem 90.9% and imipenem 90.5%), gentamicin (73.1%), tigecycline (52.0%), and colistin (4.8%). For P. aeruginosa, resistance was found to third-generation cephalosporins (100%), carbapenems (80.0%), piperacillin/tazobactam (71.4%), amikacin (66.7%), cefepime (55.6%), and colistin (12.5%). For K. pneumoniae, resistance was found to third-generation cephalosporins (72.7%), ciprofloxacin (70.0%), aminoglycosides (54.5%), extended-spectrum β-lactamase (50.0%), and colistin (25.0%). For E. coli, resistance was found to third-generation cephalosporins (87.5%), ciprofloxacin (62.5%), aminoglycosides (50.0%), gentamicin (50.0%), and extended-spectrum β-lactamases (100%).
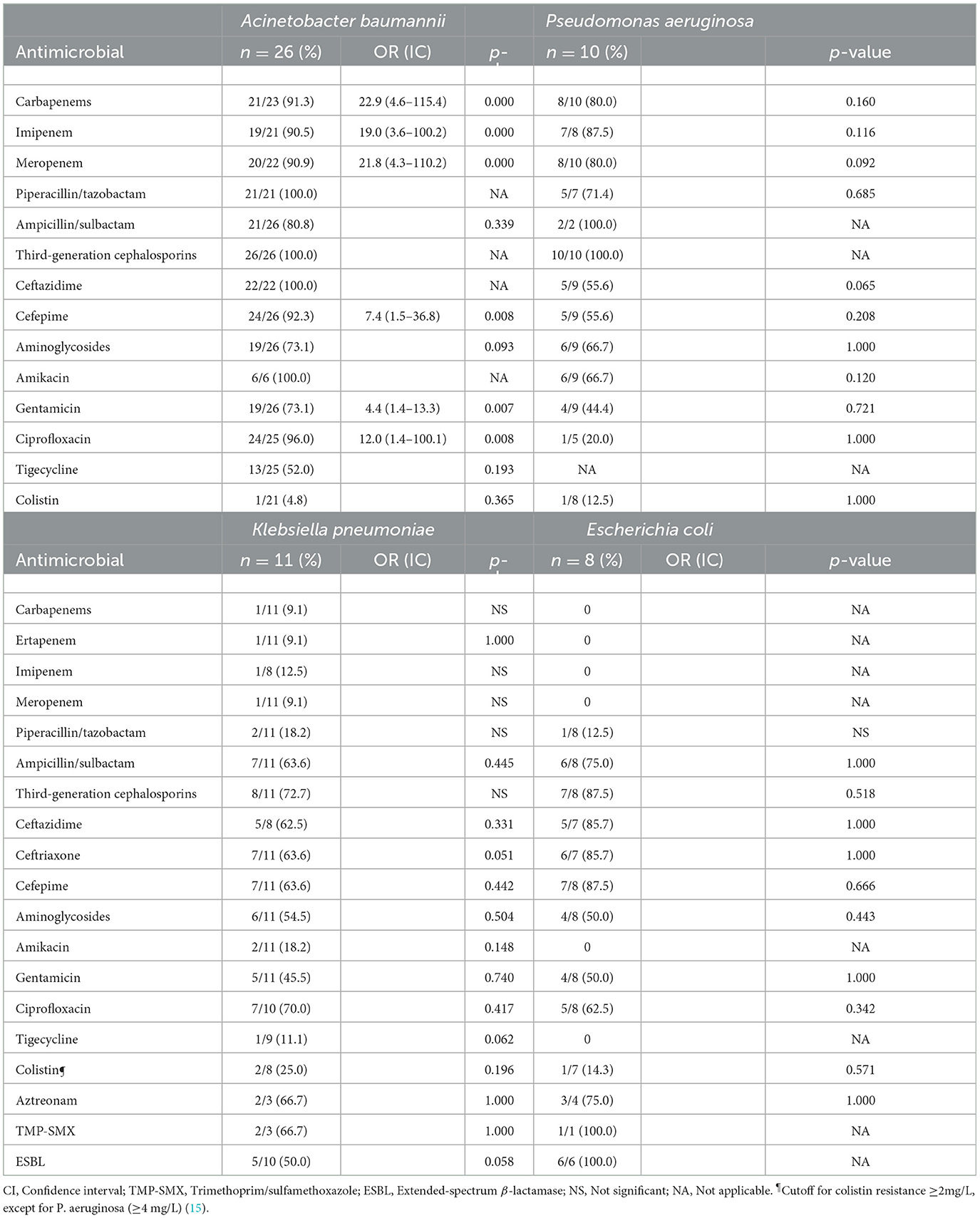
Table 6. Antimicrobial resistance in patients with ventriculitis (2019–2022).
In the univariate analysis, the risk factors for resistance were observed only in A. baumannii isolates. To carbapenems with OR 22.9 (4.6–115.4), p = 0.000 (including imipenem and meropenem); cefepime with OR 7.4 (1.5–36.8), p = 0.008; gentamicin with OR 4.4 (1.4–13.3), p = 0.007, and ciprofloxacin with OR 12.0 (1.4–100.1), p = 0.008.
Discussion
According to the case definition, 64 patients who met the eligibility criteria were selected. Ventriculitis is considered to be an unusual complication, which is potentially fatal. The prognosis is worse if ventriculitis is associated with an infection by MDR Gram-negative bacilli (particularly A. baumannii) (10, 16).
The most serious problem in nosocomial infections associated with neurosurgery is ventriculitis, which has a poor prognosis and causes death or the development of a vegetative state in up to 70% of patients. Ventriculitis becomes even more complex in patients who acquire A. baumannii infection, with nosocomial meningitis due to this bacillus causing death in up to 72.7% of cases (8, 16, 17). In our study, there was a high mortality, estimated at 78.12% (50 of 64 patients died). Of the 26 patients with A. baumannii in CSF, 23 (88.5%) died.
We registered 530 patients with suspected ventriculitis associated with an EVD. Of these, 115 (21.7%) patients developed microbiological ventriculitis associated with an EVD, which was slightly lower than that reported by Dorresteijn et al. (18) (23.0%) in a meta-analysis. In addition, the main indication for EVD replacement was identical: hemorrhage (cerebral, intracranial, subarachnoid, intraventricular) estimated at 69.8% in our study and 69.0% in the study of Dorresteijn et al. (18).
The prevalence of EVD-associated infections has been reported to range from 0.0 to 23.2%. In a retrospective cohort study in Austria between 2008 and 2019, out of 396 patients, 32 patients (8.1%) with EVD-associated infections were reported. CSF samples mainly contained Gram-positive cocci, and only three patients (9.3%) had Gram-negative bacilli in their samples (19).
There are epidemiological differences in the prevalence of causative agents between countries. A higher prevalence of Gram-negative bacilli has been reported in some developing countries. However, a growing trend in the prevalence of these bacilli is observed globally, mainly P. aeruginosa, A. baumannii, and K. pneumoniae resistant to carbapenems (12, 16).
Most of our patients had hydrocephalus. An EVD is frequently used for the management of acute hydrocephalus. Hydrocephalus can arise as a secondary complication of hemorrhage (intraventricular or subarachnoid) or as a complication following an inflammatory reaction (infectious or non-infectious) (20, 21).
A significant number of patients presented with neurological deficits upon admission and required IMV. Ventriculitis is difficult to diagnose clinically because it is masked by the disease that led to EVD placement (22).
If cytochemical parameters in CSF are inconclusive, the diagnosis of ventriculitis is difficult. One must determine if the test results are due to inflammation after neurosurgery, device placement, or infection. In our study, a positive CSF culture for Gram-negative bacilli was an inclusion criterion. Hence, the diagnosis was confirmed in all patients according to IDSA 2017 criteria. Most patients had pleocytosis (≥200 cells/μL), hypoglycorrhachia, and hyperproteinorrachia. After EVD insertion, pleocytosis (mean count ≥175 cells/μL) in CSF is a decisive indicator of infection (2).
The importance of A. baumannii as an MDR pathogen found at a high frequency in patients with ventriculitis associated with EVD use has been highlighted in several studies (6, 23, 24). Herein, the prevalence of A. baumannii in CSF was estimated to be 40.6%. It was the highest in relation to other Gram-negative bacilli isolated from CSF (followed by K. pneumoniae at 17.2%). Ye et al. (23) reported, in a retrospective study of patients with ventriculitis/meningitis, a prevalence of 39.1% of A. baumannii in CSF samples.
In our univariate analysis, arterial hypertension, a low GCS score (≤8), IMV upon admission and during hospitalization, the presentation of septic shock, resistance to carbapenems, and receiving ineffective treatment were risk factors for death. Sharma et al. (25) undertook a study on the post-neurosurgical infection (meningitis/ventriculitis) by Acinetobacter species. In their univariate analysis, arterial hypertension, a low GCS score, and septic shock were risk factors for death. They also reported, using a multivariate Cox proportional hazards model, age ≥40 years, pleocytosis (≥200 cells/μL), and having several comorbidities to be risk factors for death. Panic et al. (26) used logistic regression analysis for patients with A. baumannii infection. They found IMV and GCS scores ≤ 8 to be associated with a poor outcome (26). In our adjusted analysis of the Cox proportional hazards model, the presentation of septic shock and ineffective treatment resulted in significant HRs.
A favorable prognosis for patients with nosocomial ventriculitis depends on the speed with which treatment is initiated. Hospital environments with MDR Gram-negative bacilli have been associated with an increased risk of death from meningitis/ventriculitis, isolation of A. baumannii, and administration of inappropriate empiric treatments (12, 27).
A significant number of our non-survivor patients had A. baumannii in CSF samples. The next most prevalent pathogens found in CSF were P. aeruginosa, K. pneumoniae, and E. coli. The risks of a poor prognosis were associated with A. baumannii isolates in CSF samples that required IMV upon admission and if A. baumannii was also resistant to carbapenems.
Gram-negative bacilli isolated
For the strains of Gram-negative bacilli isolated in CSF samples, clear resistance to cephalosporins, ciprofloxacin, ampicillin/sulbactam, and aztreonam was observed. Our data on antibiotic resistance were similar to those reported by Ye et al. (23). However, their data indicated higher antibiotic resistance rates compared to our results for ceftazidime (80.0% vs. 85.9%), ceftriaxone (84.6% vs. 93.9%), cefepime (75.0% vs. 82.6%), ciprofloxacin (79.3% vs. 80.2%), ampicillin/sulbactam (74.0% vs. 79.7%), aztreonam (73.3% vs. 76.5%), gentamicin (53.3% vs. 71.8%), and amikacin (40.0% vs. 53.2%). In relation to carbapenems, the resistance rate estimated by Ye et al. (23) was much higher than that in the bacterial strains isolated in our study (e.g., imipenem, 58.3% vs. 97.8%; meropenem, 54.4% vs. 81.9%). Resistance to colistin was low in both studies (10.6% vs. 11.6%).
The A. baumannii isolates in CSF samples exhibited high resistance (73.1%−100%) to piperacillin/tazobactam, amikacin, third- and fourth-generation cephalosporins, carbapenems (meropenem and imipenem), and gentamicin. Similar results were found for P. aeruginosa isolates in CSF samples. Low resistance to colistin was found in both bacilli. Isolates of K. pneumoniae and E. coli did not show significant resistance to carbapenems.
For A. baumannii isolates, an increased risk of resistance to carbapenems, cefepime, gentamicin, and ciprofloxacin was found. Panic et al. (26) reported A. baumannii to be the most prevalent bacillus in CSF samples from patients in a hospital specializing in infectious diseases, and they found resistance to carbapenems in all samples.
According to the IDSA 2017 guidelines, in patients with nosocomial ventriculitis/meningitis due to Gram-negative bacilli, empirical management is with meropenem. Colistin should be only administered if there is resistance to carbapenems (2). Several authors have reported the high resistance of Gram-negative bacilli to carbapenems (especially A. baumannii, >40%), so the recommended empirical treatment should be concomitant use of colistin intravenous (IV) and intraventricular (IVT) (4, 14, 24).
Given the minimal resistance to colistin found by our bacterial isolates, this indication would be appropriate for our patients. However, in cases of an inadequate response to systemic antimicrobial therapy using colistin (IVT and IV), colistin combined with another drug should be attempted. Tigecycline (IVT) combined with colistin (IVT) could be a good option against carbapenem-resistant A. baumannii and K. pneumoniae. However, in the case of our A. baumannii isolates in CSF samples, tigecycline resulted in high resistance (52.0%) (28–30).
Treatment with colistin (IVT) has been recommended to ensure penetration of this antibiotic into ventricles, but it should be carried out simultaneously with IV administration. The dose and time of administration must be specified (i.e., strict monitoring of treatment must be maintained) (2, 4, 24).
A co-formulation of ceftazidime/avibactam (IV) could be a good treatment option for neurosurgical interventions against P. aeruginosa and Enterobacteriaceae (K. pneumoniae and E. coli) that produce KPC-type carbapenemases (31).
Ineffective treatment was an independent factor that affected mortality directly. The therapeutic challenge is very great for infections of the central nervous system. One must deepen knowledge of the pharmacokinetics and pharmacodynamics of antibiotics and establish better recommendations for their use. Randomized clinical trials and prospective cohort studies are needed to accurately determine the potential benefit of treatments targeting MDR pathogens (32, 33).
Limitations
The retrospective design of our study implied limitations. There was high variability regarding the prevalence of EVD-associated infectious ventriculitis and mortality. These variations (in addition to the clinical particularities of patients) were due to the different definitions of infectious ventriculitis, patient selection criteria, and the methodology used in different studies. Our study cohort was collected during the coronavirus disease-2019 pandemic, as well as conjunctural changes in the México Health System that directly influenced patient care in our hospital.
Conclusions
In the placement/replacement of an EVD, in addition to the disease severity of the patients who require it, multiple factors must be considered: maintaining strict standards of healthcare inside and outside theaters; adequate availability of and accessibility to antibiotics; and synchronization with the microbiological laboratory. Thus, providing patients with a timely diagnosis and efficacious treatment that ensures more favorable outcomes, reduced stay in hospital, low healthcare costs, and low risk of death is crucial. Despite the similarities identified in previous studies with our patients and our microbiological data, each hospital center must face the problems of its own environment as well as the clinical particularities of its target population. Our hospital usually receives patients with diseases in advanced stages of illness and from all over Western Mexico, hence the complexity of our hospital care.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Institutional Review Board of the Western National Medical Center of the Mexican Institute of Social Security with Registration numbers: R-2021–1301–221 and R-2023–1301–036. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AC-N: Writing – review & editing, Writing – original draft. MA-M: Writing – review & editing, Writing – original draft. EÁ-E: Writing – review & editing. MT-C: Writing – review & editing. CC-C: Writing – review & editing. HF-S: Writing – review & editing. JC-M: Writing – review & editing. MV-A: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Antimicrobial Resistance - World Health Organization. (WHO). Available online at: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance (accessed January 29, 2024).
2. Tunkel AR, Hasbun R, Bhimraj A, Byers K, Kaplan SL, Scheld WM. Diseases society of America's clinical practice guidelines for healthcare-associated ventriculitis and meningitis. Clin Infect Dis. (2017) 64:e34–65. doi: 10.1093/cid/ciw861
3. Hussein K, Bitterman R, Shofty B, Paul M, Neuberger A. Management of post-neurosurgical meningitis: narrative review. Clin Microbiol Infect. (2017) 23:621–8. doi: 10.1016/j.cmi.2017.05.013
4. Mohammed N, Savardekar AR, Patra DP, Narayan V, Nanda A. The 21st-century challenge to neurocritical care: the rise of the superbug Acinetobacter baumannii. A meta-analysis of the role of intrathecal or intraventricular antimicrobial therapy in reduction of mortality. Neurosurg Focus. (2017) 43:FOCUS17443. doi: 10.3171/2017.8.FOCUS17443
5. Dorresteijn KRIS, Brouwer MC, Jellema K, van de Beek D. Bacterial external ventricular catheter-associated infection. Expert Rev Anti Infect Ther. (2020) 18:219–29. doi: 10.1080/14787210.2020.1717949
6. Hasbun R. Healthcare-associated ventriculitis: current and emerging diagnostic and treatment strategies. Expert Rev Anti Infect Ther. (2021) 19:993–9. doi: 10.1080/14787210.2021.1866544
7. Walek KW, Leary OP, Sastry R, Asaad WF, Walsh JM, Mermel L, et al. Decreasing external ventricular drain infection rates in the neurocritical care unit: 12-year longitudinal experience at a single institution. World Neurosurg. (2021) 150:e89–e101. doi: 10.1016/j.wneu.2021.02.087
8. Soto-Hernández JL, Ramírez-Crescencio MA, Reyes-Ramírez G, Sánchez-Ramos A, Hernández-Velásquez M, Angeles Morales V, et al. Infecciones nosocomiales en un hospital de pacientes neurológicos, análisis de 10 años [Nosocomial infections at a neurologic hospital, analysis of 10 years]. Gac Med Mex. (2002) 138:397–404.
9. Sweid A, Weinberg JH, Abbas R, El Naamani K, Tjoumakaris S, Wamsley C, et al. Predictors of ventriculostomy infection in a large single-center cohort. J Neurosurg. (2020) 134:1218–1225. doi: 10.3171/2020.2.JNS192051
10. Georgakopoulou VE, Spandidos DA, Papalexis P, Gkoufa A, Aravantinou-Fatorou A, Angelopoulou E, et al. Outcomes in meningitis-ventriculitis treated with intravenous or intrathecal plus intravenous colistin: A meta-analysis. Exp Ther Med. (2023) 25:293. doi: 10.3892/etm.2023.11992
11. Solo-Peleteiro A, Diéguez P, Pérez-Rodríguez MT, Galárraga RA, Pérez-Landeiro A, Álvarez-Fernández M. Cerebrospinal fluid drainage-related ventriculitis due to multidrug-resistant microorganisms. Enferm Infecc Microbiol Clin. (2022) 40:322–5. doi: 10.1016/j.eimce.2020.12.005
12. Karvouniaris M, Brotis A, Tsiakos K, Palli E, Koulenti D. Current Perspectives on the diagnosis and management of healthcare-associated ventriculitis and meningitis. Infect Drug Resist. (2022) 15:697–721. doi: 10.2147/IDR.S326456
13. Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. (2012) 18:268–81. doi: 10.1111/j.1469-0691.2011.03570.x
14. Pandey S, Li L, Deng XY, Cui DM, Gao L. Outcome following the treatment of ventriculitis caused by multi/extensive drug resistance gram negative bacilli; Acinetobacter baumannii and Klebsiella pneumonia. Front Neurol. (2019) 9:1174. doi: 10.3389/fneur.2018.01174
15. Satlin MJ, Lewis JS, Weinstein MP, Patel J, Humphries RM, Kahlmeter G, et al. Clinical and laboratory standards institute and European committee on antimicrobial susceptibility testing position statements on polymyxin B and colistin clinical breakpoints. Clin Infect Dis. (2020) 71:e523–9. doi: 10.1093/cid/ciaa121
16. Tuon FF, Penteado-Filho SR, Amarante D, Andrade MA, Borba LA. Mortality rate in patients with nosocomial Acinetobacter meningitis from a Brazilian hospital. Braz J Infect Dis. (2010) 14:437–40. doi: 10.1590/S1413-86702010000500003
17. Fursova NK, Fursov MV, Astashkin EI, Fursova AD, Novikova TS, Kislichkina AA, et al. Multidrug-resistant and extensively drug-resistant Acinetobacter baumannii causing nosocomial meningitis in the neurological intensive care unit. Microorganisms. (2023) 11:2020. doi: 10.3390/microorganisms11082020
18. Dorresteijn KRIS, Jellema K, van de Beek D, Brouwer MC. Factors and measures predicting external CSF drain-associated ventriculitis: a review and meta-analysis. Neurology. (2019) 93:964–72. doi: 10.1212/WNL.0000000000008552
19. Khalaveh F, Fazel N, Mischkulnig M, Vossen MG, Reinprecht A, Dorfer C. Risk factors promoting external ventricular drain infections in adult neurosurgical patients at the intensive care unit-a retrospective study. Front Neurol. (2021) 12:734156. doi: 10.3389/fneur.2021.734156
20. Rojas-Lora M, Corral L, Zabaleta-Carvajal I, López-Ojeda P, Fuentes-Mila V, Romera-Peregrina I, et al. External ventriculostomy-associated infection reduction after updating a care bundle. Ann Clin Microbiol Antimicrob. (2023) 22:59. doi: 10.1186/s12941-023-00612-z
21. Hussein K, Rabino G, Feder O, Eghbaryeh H, Zayyad H, Sviri G, et al. Risk factors for meningitis in neurosurgical patients with cerebrospinal fluid drains: prospective observational cohort study. Acta Neurochir. (2019) 161:517–24. doi: 10.1007/s00701-019-03801-y
22. Ulloque-Caamaño L, Mo-Carrascal J, Maraby J, Narvaez-Rojas A, Quintana-Pajaro L, Ramos-Villegas Y, et al. Ventriculitis associated with extraventricular drainage: etiology, diagnosis and treatment focused on neurocritic care units. Ventriculitis asociada a drenaje extraventricular: etiología, diagnóstico y tratamiento enfocado a unidades de cuidados neurocríticos. Cir Cir. (2019) 87:230–40. doi: 10.24875/CIRU.18000052
23. Ye Y, Kong Y, Ma J, Shi G. Carbapenem-resistant gram-negative bacteria-related healthcare-associated ventriculitis and meningitis: antimicrobial resistance of the pathogens, treatment, and outcome. Microbiol Spectr. (2022) 10:e0025322. doi: 10.1128/spectrum.00253-22
24. Fotakopoulos G, Makris D, Chatzi M, Tsimitrea E, Zakynthinos E, Fountas K. Outcomes in meningitis/ventriculitis treated with intravenous or intraventricular plus intravenous colistin. Acta Neurochir. (2016) 158:603–10. doi: 10.1007/s00701-016-2702-y
25. Sharma R, Goda R, Borkar SA, Katiyar V, Agarwal S, Kumar A, et al. Outcome following postneurosurgical Acinetobacter meningitis: an institutional experience of 72 cases. Neurosurg Focus. (2019) 47: FOCUS19278. doi: 10.3171/2019.5.FOCUS19278
26. Panic H, Gjurasin B, Santini M, Kutlesa M, Papic N. Etiology and outcomes of healthcare-associated meningitis and ventriculitis-a single center cohort study. Infect Dis Rep. (2022) 14:420–27. doi: 10.3390/idr14030045
27. Senturk GC, Ozay R, Kul G, Altay FA, Kuzi S, Gurbuz Y, et al. Evaluation of post-operative meningitis: comparison of meningitis caused by Acinetobacter spp. and Other Possible Causes Turk Neurosurg. (2019) 29:804–10.
28. Paul M, Carrara E, Retamar P, Tängdén T, Bitterman R, Bonomo RA, et al. European society of clinical microbiology and infectious diseases (ESCMID) guidelines for the treatment of infections caused by multidrug-resistant Gram-negative bacilli (endorsed by European society of intensive care medicine). Clin Microbiol Infect. (2022) 28:521–47. doi: 10.1016/j.cmi.2021.11.025
29. Tsolaki V, Karvouniaris M, Manoulakas E, Kotlia P, Karadontas V, Fotakopoulos G, et al. Intraventricular CNS treatment with colistin-tigecycline combination: a case series. J Crit Care. (2018) 47:338–41. doi: 10.1016/j.jcrc.2018.07.025
30. Theofanopoulos A, Fermeli D, Vekios D, Bizos A, Marangos M, Constantoyannis C, et al. Successful treatment of pan-drug resistant Acinetobacter baumannii nosocomial meningitis/ventriculitis by combined intravenous and intrathecal colistin-tigecycline administration: a case series. Infez Med. (2023) 31:103–7. doi: 10.53854/liim-3101-14
31. Yasmin M, Nutman A, Wang L, Marshall S, Chen K, Wang J, et al. Utilizing ceftazidime/avibactam therapeutic drug monitoring in the treatment of neurosurgical meningitis caused by difficult-to-treat resistant Pseudomonas aeruginosa and KPC-Producing Enterobacterales. Open Forum Infect Dis. (2023) 10:ofad507. doi: 10.1093/ofid/ofad507
32. Cabrera-Maqueda JM, Fuentes Rumí L, Valero López G, Baidez Guerrero AE, García Molina E, Díaz Pérez J, et al. Difusión de los antibióticos en el sistema nervioso central [Antibiotic diffusion to central nervous system]. Rev Esp Quimioter. (2018) 31:1–12.
33. Lodise TP, Bassetti M, Ferrer R, Naas T, Niki Y, Paterson DL, et al. All-cause mortality rates in adults with carbapenem-resistant Gram-negative bacterial infections: a comprehensive review of pathogen-focused, prospective, randomized, interventional clinical studies. Expert Rev Anti Infect Ther. (2022) 20:707–19. doi: 10.1080/14787210.2022.2020099
Keywords: external ventricular drain, EVD-associated ventriculitis, gram-negative bacilli, multidrug-resistant, mortality hazard ratios
Citation: Corona-Nakamura AL, Arias-Merino MJ, Ávila-Esparza EI, Tolentino-Corona MdL, Cañedo-Castañeda CC, Flores-Salinas HE, Corona-Macías JF and Vázquez-Arias ME (2024) Ventriculitis due to multidrug-resistant gram-negative bacilli associated with external ventricular drain: evolution, treatment, and outcomes. Front. Neurol. 15:1384206. doi: 10.3389/fneur.2024.1384206
Received: 08 February 2024; Accepted: 04 April 2024;
Published: 26 April 2024.
Edited by:
U. K. Misra, Sanjay Gandhi Post Graduate Institute of Medical Sciences (SGPGI), IndiaReviewed by:
Marami Das, Gauhati Medical College and Hospital, IndiaNeera Chaudhry, Vardhman Mahavir Medical College and Safdarjung Hospital, India
Copyright © 2024 Corona-Nakamura, Arias-Merino, Ávila-Esparza, Tolentino-Corona, Cañedo-Castañeda, Flores-Salinas, Corona-Macías and Vázquez-Arias. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Martha Elena Vázquez-Arias, martha.vazquez3564@academicos.udg.mx