 Bruno Kopp1,2*
Bruno Kopp1,2* Nina Rösser2,3Sandra Tabeling2,4Hans Jörg Stürenburg4
Nina Rösser2,3Sandra Tabeling2,4Hans Jörg Stürenburg4 Bianca de Haan5
Bianca de Haan5 Hans-Otto Karnath5,6
Hans-Otto Karnath5,6 Karl Wessel2,3
Karl Wessel2,3- 1Department of Neurology, Hannover Medical School, Hannover, Germany
- 2Cognitive Neurology, Technische Universität Braunschweig, Braunschweig, Germany
- 3Department of Neurology, Braunschweig Hospital, Braunschweig, Germany
- 4Department of Neurology, Klinik Niedersachsen, Bad Nenndorf, Germany
- 5Division of Neuropsychology, Center of Neurology, Hertie-Institute for Clinical Brain Research, University of Tübingen, Tübingen, Germany
- 6Department of Psychology, University of South Carolina, Columbia, SC, USA
One of Luria's favorite neuropsychological tasks for challenging frontal lobe functions was Link's cube test (LCT). The LCT is a cube construction task in which the subject must assemble 27 small cubes into one large cube in such a manner that only the painted surfaces of the small cubes are visible. We computed two new LCT composite scores, the constructive plan composite score, reflecting the capability to envisage a cubical-shaped volume, and the behavioral (dis-) organization composite score, reflecting the goal-directedness of cube construction. Voxel-based lesion-behavior mapping (VLBM) was used to test the relationship between performance on the LCT and brain injury in a sample of stroke patients with right hemisphere damage (N = 32), concentrated in the frontal lobe. We observed a relationship between the measure of behavioral (dis-) organization on the LCT and right frontal lesions. Further work in a larger sample, including left frontal lobe damage and with more power to detect effects of right posterior brain injury, is necessary to determine whether this observation is specific for right frontal lesions.
Introduction
Luria (1966) proposed that the frontal lobes are essential for organizing goal-directed behavioral sequences, and accordingly, that frontal lobe damage disrupts the self-regulated structure of behavior. For frontal lobe patients, individual fragments of sensation and perception, of thought and action may be preserved; yet, the process of organizing these fragments into a useful structure is severely impaired. According to Luria (1966), the plan of action, if existent, loses its regulatory influence on behavior, and the goal-directed structure of behavior is replaced by disorganized behavior. Thus, rather than examining relevant properties and conditions, these patients often behave in an impulsive manner, i.e., without an analysis of what needs to be done, or of what objects and operations are available to do it.
One of Luria's favorite neuropsychological tasks for challenging frontal lobe functions was Link's cube test (LCT; Link, 1919, 1923)1. The LCT asks patients to construct a single large cube by assembling 27 small cubes in such a manner that only the painted surfaces of the small cubes are visible (see Figure 1). The large cube was first of all presented to the subject in the original LCT. Only after its demolition, the subject started to construct a replication, rendering the LCT basically a technique for the assessment of visuo-constructive abilities (Link, 1919). In Luria's variant of the LCT, the initial presentation of the large cube was omitted2, rendering the LCT a spatial problem solving task—the problem being defined by the mismatch between the initial state of the scattered small cubes (see Figure 1, left panel) and the spatially arranged final goal state of these cubes (see Figure 1, right panel).
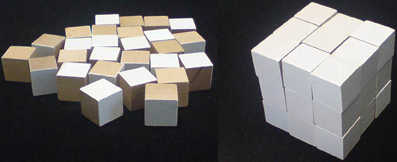
Figure 1. The stimulus materials of the LCT (Metzler, 2000). Left panel: 27 small wooden cubes (3 by 3 by 3 cm each) are scattered on the table in front of the subject. Eight of them have three white surfaces and three wooden surfaces. Twelve cubes have two white and four wooden surfaces, six cubes have one white and five wooden surfaces. One cube is all wooden. Right panel: The subject is instructed to construct a single large cube—by using all small cubes—whose outer surface is entirely white. Reproduced from Kopp et al. (2008) with permission of the copyright owner.
Metzler (2000) published an assessment instrument which he called Standardisierte Link'sche Probe (Standardized Link's Test). Metzler's variant of Luria's LCT introduced 10 behavior ratings to be made by the examiner for various aspects of the examinee's performance3. Metzler (2000) also described the results that he obtained from a normative sample (N = 220; age in years: M = 33.5, SD = 14.3; age range 14–60) of healthy individuals and from two patient samples: 69 patients with frontal damage of mixed etiology (age in years: M = 38.8, SD = 15.0) as well as 38 neurological (without known frontal lobe damage) and psychiatric patients (age in years: M = 32.0, SD = 12.8). Analyses of the completed ratings for the total sample (N = 327) indicated that these measures were highly inter-correlated, with the average correlation amounting to 0.59. A factor analysis identified only one factor that explained over 63 percent of the variance for all 10 measures. Estimates of internal consistency of the 10 scores yielded good coefficients for the total sample (α = 0.93). Consequently, Metzler (2000) focused on the LCT global composite measure which he obtained by summing up the 10 rating scores. Estimates of inter-rater reliability of LCT scores (correlation coefficients) were reasonably high (LCT global composite r = 0.98, 0.64 ≤ r ≤ 1.00 for LCT scores).
Criterion validity of the LCT global composite score could also be established. Metzler (2000) found the LCT global composite score to be the neuropsychological measure most sensitive to the presence of frontal lobe damage in the patient group with documented lesions (N = 69; the mean z-score of these patients amounted to Mz = −2.65; SDz = 1.56), although the test battery included many tests that are traditionally considered to be tests of frontal functioning (i.e., verbal letter fluency Henry and Crawford, 2004, Stroop test Perret, 1974; Stuss et al., 2001; Demakis, 2004, and Wisconsin Card Sorting Test Milner, 1963; Heaton et al., 1993; Demakis, 2003). Furthermore, the LCT global composite score was sensitive to the presence of lateralized frontal lobe damage: Patients with lesions restricted to the right-sided frontal lobe achieved lower global composite LCT scores (M = 5.6, SD = 4.6; in relation to M = 21.9, SD = 4.8 that were obtained from the N = 220 healthy individuals) compared to patients with lesions restricted to the left-sided frontal lobe (M = 12.3, SD = 8.0). Yet, despite these promising results, more research is needed on the sensitivity of the LCT toward (right-lateralized) frontal lobe damage (Kopp et al., 2008).
The study by Metzler (2000) was the first, and to our knowledge, only study suggesting an association between frontal lobe damage and poor performance on the LCT. This study, however, assessed patients with lesions from many different etiologies. Specifically, the majority (67%) of his patients suffered from traumatic brain injury. Traumatic brain injury typically results in diffuse and multifocal brain damage that is difficult to visualize and demarcate (Smith et al., 2003) with the full neurological damage extending considerably beyond the borders of the visible lesion. As a consequence, the cognitive deficits displayed by the majority of the patients in the study by Metzler (2000) may not be solely due to the visible lesion in the right frontal lobe.
In the present study, we investigated the sensitivity of performance on the LCT (Metzler, 2000) to frontal lobe damage in stroke patients based on a voxel-based lesion-behavior mapping approach (VLBM; Rorden and Karnath, 2004; Rorden et al., 2007, 2009). The VLBM method can be used when the regions of brain injury are sufficiently clearly defined. In this case, the lesions are manually identified for each patient before individual brains are realigned into a common stereotaxic space [i.e., the Montreal Neurological Institute (MNI) space]. Finally, statistical techniques can be applied which test, on the basis of individual brain voxels, whether lesioned voxels are reliably associated with impaired behavior (see Materials and Methods for details).
Metzler's study (2000) suggested sensitivity of performance on the LCT to lesions in the frontal lobes, with right frontal damage associated with particularly severe impairment. Here, we are looking to replicate that right frontal association in a sample of stroke patients where lesions are clearly demarcated. Thus, we aimed to replicate and more rigorously assess the hypothesized association between right frontal lobe damage and performance on the LCT.
Materials and Methods
Subjects
Thirty-two (19 male, 13 female) acute first-ever, right-hemisphere-damaged stroke patients with damage centering on or involving the frontal lobe in most patients participated in the study (see Table 1 for details). We solely included right-hemisphere-damaged stroke patients in order to examine whether performance on the LCT is sensitive to focal right frontal lesions. In addition, task performance of left-hemisphere-damaged stroke patients might be distorted due to paresis and/or apraxia of the dominant hand. Further, left-hemisphere strokes might have hampered the capability to understand task instructions, due to the potential presence of sensory aphasia4. Patients with diffuse or bilateral brain lesions due to traumatic brain injury, brain tumors, subcortical arteriosclerotic encephalopathy, or any other dementing disease were excluded. Patients without prior psychiatric disease or those without alcohol or drug abuse were recruited. Further, patients with gross neurological defects (pronounced pain as reported by the patient, left homonymous hemianopia as revealed by clinical examination, hemispatial visual neglect) were also excluded to make sure that these symptoms did not interfere with task performance4. Spatial neglect was diagnosed when a patient showed the characteristic clinical behavior such as orienting toward the ipsilesional side when addressed from the front or the left and/or ignoring contralesionally located people or objects. All patients gave their informed written consent to participate in the study, in accordance with the ethical standards of the Declaration of Helsinki. Table 1 shows demographic and neuropsychological participant characteristics. Appropriate ethical approval was obtained from the Ethics Committee at the Technische Universität Braunschweig.
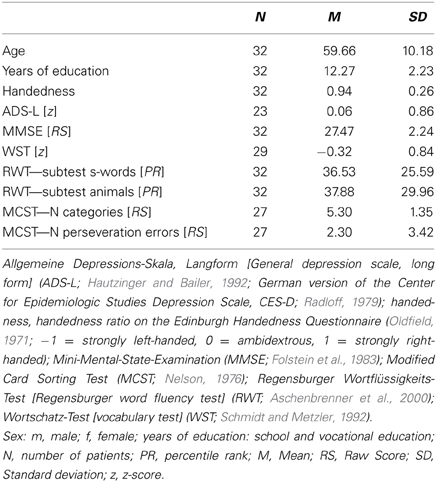
Table 1. Demographic and neuropsychological patient characteristics.
Test Description, Administration and Scoring
The stimulus materials and the specifications for administering the LCT are presented in Figure 1. The LCT behavior ratings consist of the following 10 scores (cf. Metzler, 2000, for more details):
(1) Exploration. The item provides a rating of behavioral evidence for “preliminary investigative activity,” problem identification, and means-end analysis, most notably inspection and sorting of the small cubes. If patients sorted all cubes, the score was three; if they sorted a subset of cubes, the score was two; if they merely inspected individual cubes, the score was one; if they did not explore the cubes at all, the score was zero.
(2) Spatial sub-goaling. The item provides a rating about how the edge length of the large cube was planned. If patients counted the small cubes and correctly calculated the edge length of the large cube, the score was three; if they counted, but calculated incorrectly, the score was two; if they counted, but did not calculate, the score was one; if they did not count nor calculate, the score was zero.
(3) Action organization. The item provides a rating of the capability to organize goal-directed sequences of actions. If patients showed planned, consequential and goal-directed use of the small cubes, the score was three; if they did so, but also showed spontaneous and needless behaviors, the score was two; if they showed grossly disorganized behavior, the score was one; if they showed behavioral chaos, the score was zero.
(4) Mental spatial structure. The item provides a rating of whether patients built the idea of a three-dimensional cube resting on a quadratic basic shape, and whether their actions followed this anticipated final goal state in a stringent manner. If patients showed behavioral evidence for a three-dimensional imagination, for a quadratic shape, and for a stringent use of the small cubes, the score was three; if they showed behavioral evidence for a three-dimensional imagination, yet placed the small cubes in a highly insecure manner, the score was two; if they failed to show behavioral evidence for both, a three-dimensional imagination and for a quadratic basic shape, the score was one; if they constructed non-quadratic shapes (such as rectangles, rings, or walls) in a single layer, the score was zero.
(5) Attention control. The item provides a rating of the capability to maintain attention to the color of the outer surface of the large cube. If patients committed only a few surface color errors, and if they corrected these errors during construction, the score was three; if they committed several surface color errors, and if they failed to correct one or two of these errors during construction, the score was two; if they failed to control for surface color errors, and if they failed to correct several of these errors during construction, the score was one; if they committed many surface color errors, and if they failed to correct many of these errors, the score was zero.
(6) Error correction. The item provides a rating of the organization of error correction, ranging from the goal-directed search for errors by re-constructing specific parts of the cube to the repeated demolishing of the entire cube. If no error correction was required, the score was three; if the search for errors proceeded in a well-regulated manner, the score was two; if the search for errors proceeded in a less orderly manner with some needless cube deconstructions, the score was one; if the search for errors proceeded in a disordered manner with many needless cube deconstructions, the score was zero.
(7) Edge length. The item provides a rating about how the edge length of the large cube was achieved. If patients reached at the correct edge length of the large cube immediately, the score was three; if they began initially with an incorrect edge length, but corrected the edge length by themselves, the score was two; if they began initially with an incorrect edge length, and if they corrected the edge length only when an obvious lack of small cubes enforced them to do this, the score was one; if they repeatedly constructed their large cube with an incorrect edge length, and if they did not achieve to correct the edge length by themselves, the score was zero.
(8) Final state. The item provides a rating about the appropriateness of the final state. If the final state was without any error, the score was three; if the final state featured one or two errors, the score was two; if the final state manifested three or five errors, the score was one; if the final state showed many errors, or if the large cube was incomplete, or if the task was aborted, the score was zero.
(9) Number of cues. The item provides a rating of the number of cues that were given to the patient. If no cues were provided, the score was three; if the instruction was repeated or explained once, the score was two; if the instruction was repeated or explained twice, or if cues on incorrect construction were given, the score was one; if multiple cues were provided, the score was zero.
(10) Time requirement. The item categorizes the amount of time required on the task. If patients needed less than 4 min, the score was three; if they needed 4–6 min, the score was two; if they needed 6–10 min, the score was one; if they needed more than 10 min, the score was zero.
Instructions were worded as follows: “Your task is to construct one large cube by assembling the many small cubes that lie in front of you. If we look at it, the large cube must appear white throughout. That's why some, but not all, of the surface areas of the small cubes are white. Please bear in mind that the later invisible surface area of the large cube must also be white. None of the small cubes may be left over. And also keep in mind: Cubes are defined as having three sides of equal length. I measure the time it takes you to construct the large cube, but the time it takes is of only negligible importance to me. I am mainly interested in seeing how you solve your task. Do you have questions before we start?”
It is appropriate to provide cues to the patient under the following conditions: (1) The patient constructs walls or rectangles, but not a cube, even after several attempts. (2) The patient uses repeatedly wrong edge lengths. (3) The patient refuses further participation. (4) The patient accomplished the cube, but with errors that are not recognized by the patient. Cues may consist of parts of the instructions, including the explanation of how cubes are defined, or hints on errors.
The LCT global composite score was computed (range: 0–30) by summing up the 10 individual LCT rating values (Metzler, 2000). Apart from the LCT global composite score, two new LCT composite scores were computed: First, the LCT constructive plan composite score (range: 0–9) comprised the sum composed of (2) spatial sub-goaling, (4) mental spatial structure, and (7) edge length. These three ratings target the capability to mentally form an appropriate constructive plan and to enable this plan to provide a regulatory influence on construction behavior. In Metzler's study (2000), the average inter-correlation between these three rating values amounted to 0.71, a finding that can be considered as evidence for the relatively distinct homogeneity of these three ratings. Second, the LCT behavioral (dis-) organization composite score (range: 0–9) comprised the sum composed of (3) action organization, (5) attention control, and (6) error correction. These three ratings target the goal-directedness of single units of behavior with regard to the demand to solve the LCT problem efficiently. In Metzler's study (2000), the average inter-correlation between these three rating values amounted to 0.69, a finding that can be considered as evidence for the relatively distinct homogeneity of these three ratings. Note that these averaged intra-score correlations (i.e., 0.71 and 0.69, respectively), should be contrasted with the average inter-correlation between all remaining items after exclusion of these six intra-score correlations, which amounted to 0.57.
There is also a psychometric rationale for combining individual scores to linearly combined composite scores, such as the LCT constructive plan composite score and the LCT behavioral (dis-) organization composite score. Specifically, the reliability of linearly combined composite measures exceeds the reliabilities of the individual measures upon which they are based (Nunnally and Bernstein, 1994), thereby enhancing the chance to detect brain-behavior relationships.
Lesion Analysis
Magnetic resonance imaging (MRI) was performed in 28 stroke patients and computed tomography (spiral CT) scanning was performed in four patients. The initial scanning was optionally repeated during the following days until the infarcted area became clearly demarcated. The mean time interval between lesion onset and the MRI scan that was used for the present analysis amounted to 4.3 days (SD = 3.1); the mean time interval between time of lesion and CT scanning lasted 0.25 days (SD = 0.5). MRI scans were obtained on a 1.5 T echo planar imaging (EPI) capable system (Philips Intera, Philips Medical Systems, Best, The Netherlands). The MRI protocol used diffusion-weighted imaging (DWI, N = 12) and T2-weighted fluid-attenuated inversion-recovery imaging (FLAIR, N = 16). DWI was performed with a single-shot EPI spin echo sequence [25 axial slices; repetition times (TR), either 3690, 4000, 4452, 5060, 5300, or 6360 ms; echo times (TE), either 90, 95, or 120 ms; field of view (FOV), 230 × 230 mm2; matrix 64 × 64 pixels; slice thickness, 5 mm; gap, 5.5 mm]. The FLAIR sequences were acquired with 25 axial slices (thickness, 5 mm) with an interslice gap of 5.5 mm, a FOV of 220 × 220 mm2, TR of either 4000, 5397, 5500, or 6000 ms, and TE of either 89, 91, 100, or 120 ms. CTs were obtained on a spiral scanning system (Somatom Sensation 16, Siemens Healthcare, Erlangen, Germany) with a slice thickness of 3 mm infratentorial and 6 mm supratentorial and an in-plane resolution of 0.5 × 0.5 mm.
Lesion location was evaluated using MRIcroN software (Rorden et al., 2007, www.mricro.com). For patients with MRI scans, the boundaries of lesions were delineated directly on the individual MRI scans. Both the MRI scan and the lesion shape were then mapped into stereotaxic space using the normalization algorithm provided by SPM5 (www.fil.ion.ucl.ac.uk/spm/software/spm5/). Cost–function masking was employed (Brett et al., 2001) for determination of the transformation parameters.
In patients with spiral CT scans, lesions were drawn directly by an experienced neurologist (Hans-Otto Karnath; blinded for test performance) on the slices of a normalized T1-weighted template MRI scan from the MNI with a 1 × 1 mm in-plane resolution, distributed with the MRIcroN toolset. Lesions were mapped onto the slices that correspond to MNI Z-coordinates [−16, −8, 0, 8, 16, 24, 32, and 40 mm] by using the identical or the closest matching axial slices of each individual patient.
To evaluate the relationship between lesion location and performance on the three LCT composite scores [global composite score, constructive plan composite score, and behavioral (dis-) organization composite score], three voxel-based lesion-behavior analyses were performed using the MRIcroN toolset (Rorden et al., 2007; www.mricro.com). These statistical analyses were based on the Brunner–Munzel (BM) test (Brunner and Munzel, 2000) where, for each voxel, the behavioral scores of patients with a lesion in that voxel and patients with a lesion elsewhere are statistically compared using non-parametrical statistics. Only voxels that were damaged in at least three patients were included in the analysis (N = 150497 voxels). We controlled for multiple comparisons using permutation-based thresholding (Kimberg et al., 2007) using 4000 iterations. Significant results presented survived a 5% permutation based false positive probability threshold. We additionally used the MRIcroN toolset to calculate power maps originally described for situations where behavioral data is binomial by Rudrauf et al. (2008), and extended to situations where behavioral data is continuous as mentioned by Gläscher et al. (2009), for each of the three voxel-based lesion-behavior analyses. These power maps highlight the areas of the brain where we had enough power to potentially detect a significant effect using the same threshold as our main analyses (p < 0.05 using permutation-based thresholding to correct for multiple comparisons).
Results
Neuropsychological Test Results on the LCT
Table 2 summarizes the performance of the patients on the LCT. The average LCT global composite score amounted to M = 10.97 (SD = 8.65), against M = 22.8 (SD = 4.3) in healthy males and M = 20.8 (SD = 5.2) in healthy females of Metzler's (2000) study. Our patients thus, achieved higher LCT global composite scores than Metzler's (2000) right frontal lesion patients (M = 5.6, SD = 4.6), but slightly lower LCT global composite scores than Metzler's (2000) left frontal lesion patients (M = 12.3, SD = 8.0). Task difficulty differed between the 10 LCT ratings, with LCT mental spatial structure being the easiest item (M = 1.72, SD = 0.96), and LCT time requirement being the most difficult item (M = 0.66, SD = 0.83). The average LCT constructive plan composite score amounted to M = 4.28 (SD = 3.12), against M = 6.24 (SD not provided) in the total sample (N = 327; i.e., healthy controls and patients) of Metzler (2000). The average LCT behavioral (dis-) organization composite score amounted to M = 3.00 (SD = 2.74), against M = 5.34 (SD not provided) in the total sample (N = 327; i.e., healthy controls and patients) of Metzler (2000).
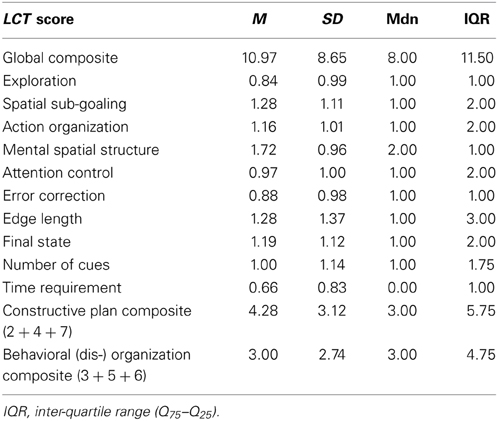
Table 2. Neuropsychological results on the LCT.
Lesion Analyses: LCT Scores
Table 3 summarizes the results obtained with the BM-test over the three LCT composite scores [LCT global composite score, LCT constructive plan composite score, and LCT behavioral (dis-) organization composite score] to identify whether or not there were voxels that, when injured, were associated with the presence of behavioral disturbances on the LCT. Statistical significance was found solely for the behavioral (dis-) organization composite score (i.e., the sum over the items 3, 5, and 6).
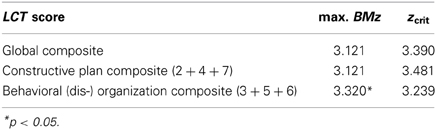
Table 3. Brunner–Munzel test statistics (maximum Brunner–Munzel z-score, critical Brunner–Munzel z-score) over the three LCT composite scores.
Lesion Analyses: Lesion Overlap and Power Maps
Figure 2A shows an overlay lesion plot of all 32 patients in eight axial slices of a standard brain (i.e., in MNI space). Inspection of Figure 2A reveals that the maximum lesion overlap occurred in the right prefrontal cortex (PFC) where up to 10 patients showed lesions in single voxels. Figure 2B shows the results of the retrospective power analyses for each of the three LCT composite scores. These power maps demonstrate that in all areas where the lesions of at least three patients overlapped, we had sufficient power to potentially detect a significant difference between the behavioral scores of patients with a lesion and the behavioral scores of patients without a lesion.
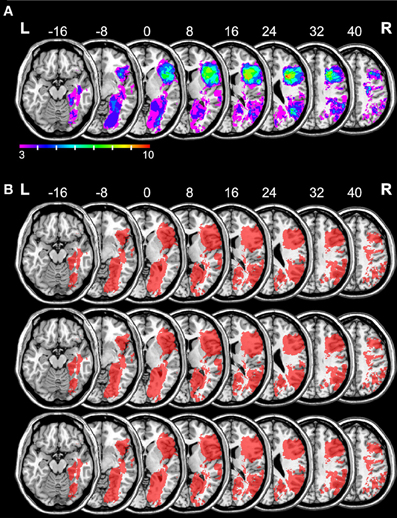
Figure 2. Overlay lesion plot of all 32 patients and the results of the retrospective power analyses for each of the three LCT composite scores. The number of overlapping lesions (A) is illustrated by color, from violet (N = 3) to red (N = 10). Maximum overlap occurred in the right frontal lobe. The results of the power analyses (B) are shown in red [top row: LCT global composite, middle row: LCT constructive plan composite, bottom row: LCT behavioral (dis) organization composite]. These power maps demonstrate that in all areas where the lesions of at least three patients overlapped, we had sufficient power to potentially detect a significant difference between the behavioral scores of patients with a lesion and the behavioral scores of patients without a lesion. Numbers indicate MNI z-coordinates.
Lesion Analyses: LCT Behavioral (dis-) Organization Composite Score
Figure 3C depicts the location of those voxels for which the voxel-based lesion-behavior analysis revealed a significant association between voxel damage and the LCT behavioral (dis-) organization composite score (cf. Table 3). Inspection of this map reveals a particular area within the right frontal lobe that is statistically related with low LCT behavioral (dis-) organization composite scores. Specifically, a significant BMz value of 3.32 was found in a voxel at MNI coordinates X = 37, Y = 19, Z = 32, a white matter coordinate underneath cortical area BA9 (depicted in red, see also the magnified cut-out). The presence of a lesion in this voxel was associated with lower LCT behavioral (dis-) organization composite scores.
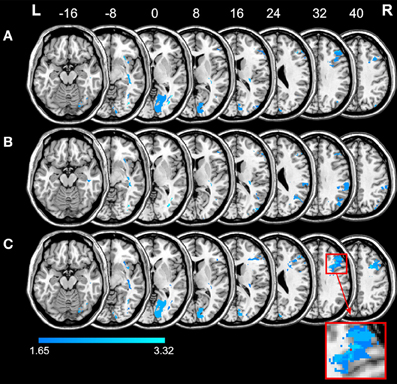
Figure 3. Anatomical results obtained from the voxel-based lesion-behavior mapping on the LCT global composite score (A), the LCT constructive plan composite score (B), and the LCT (dis-) organization composite score (C). The anatomical results without control for multiple comparisons (zcrit = 1.65) are depicted in blue. The significant result obtained for the LCT behavioral (dis-) organization composite score is shown in red (see magnified cut-out for a better view). Numbers indicate MNI z-coordinates.
Figure 3 additionally shows the results of the statistical analysis without correction for multiple comparisons for the LCT global composite score, for the LCT constructive plan composite score, and for the LCT (dis-) organization composite score (blue). These maps allow the reader to assess whether the single significant voxel really represents a statistical value that differs meaningfully from statistical values obtained from other areas of the brain. As can be seen from Figure 3A, the LCT global composite score was associated with lesions in two regions of the brain, notably an occipital and a lateral prefrontal region, but none of the voxels within these regions survived correction for multiple comparisons. Further, as revealed by Figure 3B, superior parietal lesions and fronto-parietal white matter lesions led to decrements in the LCT constructive plan composite score, but again, none of the voxels within these regions survived correction for multiple comparisons. Finally, Figure 3C reveals an occipital and a lateral prefrontal region related to (dis-) organized composite performance on the LCT, but only a single voxel within the lateral prefrontal region (see above) reached the conventional level of significance after correction for multiple comparisons.
Discussion
We observed a relationship between performance on the LCT and frontal lobe injury in a sample of stroke patients with right hemisphere damage. Specifically, as revealed by VLBM, right frontal lesions affected the measure of behavioral (dis-) organization on the LCT. The association between frontal lobe damage and behavioral (dis-) organization on the LCT surpassed significance in a single voxel within the right frontal lobe (BA9). The current study adds to the literature in multiple ways: First, it represents a shift from a purely clinical approach toward a more scientific one when it is compared to Luria's (1966) approach. Second, whereas Metzler's (2000) sample included patients with traumatic brain injury in its majority, our sample consisted solely of stroke patients with clearly demarcable lesions. Traumatic brain injury results in diffuse and multifocal brain damage, such that cognitive deficits displayed by the vast majority of the patients in the study by Metzler (2000) may not be solely due to their visible frontal lesions. Notwithstanding these shortcomings, Metzler (2000) reported a sensitivity of the LCT global composite score to frontal lesions, with right frontal damage associated with particularly severe impairment. Here, we established for the first time an association between the newly developed LCT (dis-) organization composite score and focal lesions in the right frontal lobe.
The relationship between right frontal damage and behavioral (dis-) organization on the LCT is of importance against the background that there are few measures available for assessing functional disability in right frontal patients (Lezak, 1995; Vallesi, 2012). For example, while verbal fluency can be considered a test of left frontal function (Henry and Crawford, 2004; Baldo et al., 2006), nonverbal analogs of verbal fluency, such as design fluency, do not seem to provide comparably sensitive and specific indices of right frontal function (Baldo et al., 2001). However, the data presented here need to be interpreted with caution mainly for three reasons: First, the majority of the patients in the current sample had right frontal lesions, and an extended sample should include both patients with right and left frontal lobe damage in order to examine whether or not our observation is specific for right frontal lesions. Second, the extended sample should also include many more patients with right posterior damage in order to examine whether or not our observation is specific for frontal lesions. With regard to this issue it is interesting that the LCT constructive plan score was associated with lesions in superior parietal areas of the right cerebral hemisphere. However, this finding needs replication in a sample of stroke patients with right posterior damage since none of the voxels within these parietal regions survived correction for multiple comparisons. Third, exclusion of patients with visual field defects or with hemispatial neglect generally reduces the generalizability of our claims.
According to our clinical experience, the LCT is an ingenious method to assess core aspects of executive behavior (Kopp et al., 2008; Kopp, 2012), and according to the results that we obtained in the current study, the LCT behavioral (dis-) organization composite score is a promising tool for the assessment of neuropsychological sequelae of right frontal damage. Further, the LCT is a non-routine task that requires solving a rather unfamiliar problem (Karnath et al., 1991). Numerous earlier neuropsychological studies addressed problem solving abilities (e.g., Goel and Grafman, 1995; Morris et al., 1997; Carlin et al., 2000; Colvin et al., 2001; Goel et al., 2001; see Grafman, 2007; Goel, 2009, for reviews). Most widely used are Tower Tests (Tower of Hanoi: Glosser and Goodglass, 1990; Tower of London: Shallice, 1982; Tower of Toronto: Saint-Cyr et al., 1988). Goel and Grafman (1995) have argued that while the well-structured Tower Tests are interesting cognitive tasks, they must be considered sub-optimal tasks because problem solving deficits typically emerge in ill-structured real-world situations5. As a consequence of this, a number of researchers have moved beyond well-structured neuropsychological tests and tried to approximate real-world situations (Eslinger and Damasio, 1985; Shallice and Burgess, 1991; Dimitrov et al., 1996; Goel et al., 1997; Channon and Crawford, 1999; Goel and Grafman, 2000). With regard to the ill-structured/well-structured distinction, the LCT should be considered as an intermediate task that is less well-structured than Tower Tests, but that is also less ill-structured than typical real world tasks. It should also be noted that the LCT is a dual task (Baddeley et al., 1997) since efficient performance on it requires patients to divide attention between achieving the cubical-shaped volume and the requested color surface.
To conclude, our findings suggest that aspects of performance, namely the degree of behavioral (dis-) organization, on the LCT are sensitive to right frontal lobe damage. However, all our patients suffered from damage to the right frontal lobe and we can thus, not compare the performance of patients with damage to the right frontal lobe to the performance of patients with damage elsewhere. We can, as a consequence, not draw firm conclusions concerning the specificity of the relationship between damage to the right frontal lobe and behavioral (dis-) organization on the LCT. Specifically, future work should examine performance on the LCT in patients with left frontal lesions and in patients with posterior lesions. Future collection of data should also identify the extent to which behavioral (dis-) organization on the LCT maps on real-world behaviors. Finally, we would like to stress that the scoring system is the major weakness of the LCT assessment since some of the behavioral measures seem overly subjective. Improving the assessment of performance on the LCT might be found in the application of virtual reality techniques to minimize the influence of non-objective factors that potentially affect LCT scores. Further improvements of the quantitative scoring system for assessing dysexecutive behavior on the LCT will eventually enhance the objectivity, reliability and validity of this assessment technique.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was supported by the ZNS—Hannelore Kohl Stiftung, Bonn, Germany [grant number 2004007 to Karl Wessel and Bruno Kopp], by the Erwin-Röver-Stiftung, Hannover, Germany [grant number 20082014 to Karl Wessel], by the Deutsche Forschungsgemeinschaft [DFG; grant numbers KA 1258/15-1 to Hans-Otto Karnath and HA 58393/3-1 to Bianca de Haan and Hans-Otto Karnath] through an “Open Access Publikationsfonds” to the Hannover Medical School.
Footnotes
1. ^Henry Charles Link (1889–1952) was a psychologist and the author of a book which was entitled Employment Psychology—The Application of Scientific Methods to the Selection, Training, and Rating of Employees (Link, 1919). He described the cube test in Chapter XI (entitled Apprentice tool makers and machinists, pp. 123–129) of this book: “The cube test consists of a three-inch cube, painted in green on the outside. The cube is cut into 27 one-inch cubes. The large cube is placed before the subject and he is told that it will be demolished into 27 small cubes and that he must restore them so that the large cube looks exactly as it did before, viz., green on all sides with no wood color exposed.” (p. 124). (cf. www.archive.org/texts/flipbook/flippy.php?id=employmentpsycho031643mbp, downloaded 4-12-2011. This quote follows the second edition of the book which was published in 1924). In a journal article which was published some years later, Link described the cube test in the following words: “The first (… of three tests …) consisted of a three-inch cube, painted black on the outside and then cut up into 27 one-inch cubes. The 27 small cubes were scattered on a table and the apprentice was asked to put them together into one three-inch cube which, like the original, was entirely black with no natural wood surface exposed.” (Link, 1923, p. 37). Interestingly, Link (1919, 1923) did not provide any information on how to score subjects' performance on his cube test.
2. ^Luria's variant of the LCT seems to be based on Link's (1923) journal article since this description of the task did not mention the initial presentation of the large cube to the subject.
3. ^Metzler's variant of the LCT was substantially based on his professional experience in Luria's laboratory (Metzler, pers. commun., May 13, 2003). The second edition of the Standardisierte Link'sche Probe is available since 2012 from Hogrefe Publishing, Göttingen, Germany.
4. ^A possible statistical solution to the problem would be to use the severity of hemiparesis, apraxia, aphasia, pain, hemianopia, neglect and other neuropsychological disturbances as covariates. However, covariance analysis presupposes the separation of patients into meaningful groups of individuals, as in neuropsychological group studies, and it further requires a number of restrictive conditions to be met such as, for example, that the slopes of the regression lines (which relate covariates and dependent variables), fitted to the groups, to be parallel.
5. ^The ill-structured/well-structured distinction classifies problems based on the amount of information that is available to the problem solver (Reitman, 1964). Tower Tests are typical examples of well-structured problems. In such tasks, the start state is completely specified, as is the goal state and the set of legal state transformations. Planning a meal for guests is a paradigmatic example of an ill-structured task. Here, the start state, the goal state, and the transformation function are incompletely specified (Goel, 1995).
References
Aschenbrenner, S., Tucher, O., and Lange, K. W. (2000). Regensburger Wortflüssigkeits-Test [Regensburger word fluency test] (RWT). Göttingen: Hogrefe.
Baddeley, A., Della Sala, S., Papagno, C., and Spinnler, H. (1997). Dual-task performance in dysexecutive and nondysexecutive patients with a frontal lesion. Neuropsychology 11, 187–194. doi: 10.1037/0894-4105.11.2.187
Baldo, J. V., Schwartz, S., Wilkins, D., and Dronkers, N. F. (2006). Role of frontal versus temporal cortex in verbal fluency as revealed by voxel-based lesion symptom mapping. J. Int. Neuropsychol. Soc. 12, 896–900. doi: 10.1017/S1355617706061078
Baldo, J. V., Shimamura, A. P., Delis, D. C., Kramer, J., and Kaplan, E. (2001). Verbal and design fluency in patients with frontal lobe lesions. J. Int. Neuropsychol. Soc. 7, 586–596. doi: 10.1017/S1355617701755063
Brett, M., Leff, A. P., Rorden, C., and Ashburner, J. (2001). Spatial normalisation of brain images with focal lesions using cost function masking. Neuroimage 14, 486–500. doi: 10.1006/nimg.2001.0845
Brunner, E., and Munzel, U. (2000). The nonparametric Behrens-Fisher problem: asymptotic theory and a small-sample approximation. Biometrical J. 42, 17–25. doi: 10.1002/(SICI)1521-4036(200001)42:1<17::AID-BIMJ17>3.0.CO;2-U
Carlin, D., Bonerba, J., Phipps, M., Alexander, G., Shapiro, M., and Grafman, J. (2000). Planning impairments in frontal lobe dementia and frontal lobe lesion patients. Neuropsychologia 38, 655–665. doi: 10.1016/S0028-3932(99)00102-5
Channon, S., and Crawford, S. (1999). Problem-solving in real-life-type situations: the effects of anterior and posterior lesions on performance. Neuropsychologia 37, 757–770. doi: 10.1016/S0028-3932(98)00138-9
Colvin, M. K., Dunbar, K., and Grafman, J. (2001). The effects of frontal lobe lesions on goal achievement in the water jug task. J. Cogn. Neurosci. 13, 1129–1147. doi: 10.1162/089892901753294419
Demakis, G. J. (2003). Meta-analytic review of the sensitivity of the Wisconsin Card Sorting Test to frontal and lateralized frontal brain damage. Neuropsychology 17, 255–264. doi: 10.1037/0894-4105.17.2.255
Demakis, G. J. (2004). Frontal lobe damage and tests of executive processing: a meta-analysis of the category test, stroop test, and trail-making test. J. Clin. Exp. Neuropsychol. 26, 441–450. doi: 10.1080/13803390490510149
Dimitrov, M., Grafman, J., and Holnagel, C. (1996). The effects of frontal lobe damage on everyday problem solving. Cortex 32, 357–366. doi: 10.1016/S0010-9452(96)80057-8
Eslinger, P. J., and Damasio, A. R. (1985). Severe disturbance of higher cognition after bilateral frontal lobe ablation: patient EVR. Neurology 35, 1731–1741. doi: 10.1212/WNL.35.12.1731
Folstein, M. F., Robins, L. N., and Helzer, J. E. (1983). The mini-mental state examination. Arch. Gen. Psychiatry 40, 812. doi: 10.1001/archpsyc.1983.01790060110016
Gläscher, J., Tranel, D., Paul, L. K., Rudrauf, D., Rorden, C., Hornaday, A., et al. (2009). Lesion mapping of cognitive abilities linked to intelligence. Neuron 61, 681–691. doi: 10.1016/j.neuron.2009.01.026
Glosser, G., and Goodglass, H. (1990). Disorders in executive control functions among aphasics and other brain-damaged patients. J. Clin. Exp. Neuropsychol. 12, 485–501. doi: 10.1080/01688639008400995
Goel, V. (2009). “Cognitive neuroscience of thinking,” in Handbook of Neuroscience for the Behavioral Sciences, eds G. G. Berntson and J. T. Cacioppo (New York, NY: Wiley), 417–429.
Goel, V., and Grafman, J. (1995). Are the frontal lobes implicated in “planning” functions? Interpreting data from the Tower of Hanoi. Neuropsychologia 33, 623–642. doi: 10.1016/0028-3932(95)90866-P
Goel, V., and Grafman, J. (2000). Role of the right prefrontal cortex in ill-structured planning. Cogn. Neuropsychol. 17, 415–436. doi: 10.1080/026432900410775
Goel, V., Grafman, J., Tajik, J., Gana, S., and Danato, D. (1997). A study of the performance of patients with frontal lobe lesions in a financial planning task. Brain 120, 1805–1822. doi: 10.1093/brain/120.10.1805
Goel, V., Pullara, D., and Grafman, J. (2001). A computational model of frontal lobe dysfunction: working memory and the Tower of Hanoi. Cogn. Sci. 25, 287–313. doi: 10.1207/s15516709cog2502_4
Grafman, J. (2007). “Planning and the brain,” in The Human Frontal Lobes: Functions and Disorders, ed B. L. Miller and J. L. Cummings (New York, NY: Guilford), 249–261.
Hautzinger, M., and Bailer, M. (1992). Allgemeine Depressions-Skala [General depression Scale] (ADS). Göttingen: Beltz Test GmbH.
Heaton, R. K., Chelune, G. J., Talley, J. L., Kay, G. G., and Curtiss, G. (1993). Wisconsin Card Sorting Test Manual. Lutz, FL: Psychological Assessment Resources.
Henry, J. D., and Crawford, J. R. (2004). A meta-analytic review of verbal fluency performance following focal cortical lesions. Neuropsychology 18, 284–295. doi: 10.1037/0894-4105.18.2.284
Karnath, H.-O., Wallesch, C.-W., and Zimmermann, P. (1991). Mental planning and anticipatory processes with acute and chronic frontal lobe lesions: a comparison of maze performance in routine and non-routine situations. Neuropsychologia 29, 271–290. doi: 10.1016/0028-3932(91)90042-7
Kimberg, D. Y., Coslett, H. B., and Schwartz, M. F. (2007). Power in voxel-based lesion-symptom mapping. J. Cogn. Neurosci. 19, 1067–1080. doi: 10.1162/jocn.2007.19.7.1067
Kopp, B. (2012). A simple hypothesis of executive function. Front. Hum. Neurosci. 6:159. doi: 10.3389/fnhum.2012.00159
Kopp, B., Tabeling, S., Moschner, C., and Wessel, K. (2008). Kognitive Hirnleistungen des präfrontalen Kortex – Neurowissenschaft und Klinik. [Cognitive functions of the prefrontal cortex: neuroscience and clinic.] Nervenarzt 79, 143–152. doi: 10.1007/s00115-007-2319-8
Link, H. C. (1919). Employment Psychology – The Application of Scientific Methods to the Selection, Training, and Rating of Employees. New York, NY: MacMillan.
Link, H. C. (1923). Psychological tests in industry. Ann. Am. Acad. Polit. Soc. Sci. 110, 32–44. doi: 10.1177/000271622311000105
Metzler, P. (2000). Standardisierte Link‘sche Probe zur Beurteilung exekutiver Funktionen. [Standardized Link's Test for the assessment of executive functions]. Frankfurt: Swets Test Services.
Milner, B. (1963). Effects of different brain lesions on card sorting. The role of the frontal lobes. Arch. Neurol. 9, 90–100. doi: 10.1001/archneur.1963.00460070100010
Morris, R. G., Miotto, E. C., Feigenbaum, J. D., Bullock, P., and Polkey, C. E. (1997). The effect of goal-subgoal conflict on planning ability after frontal- and temporal-lobe lesions in humans. Neuropsychologia 35, 1147–1157. doi: 10.1016/S0028-3932(97)00009-2
Nelson, H. E. (1976). A Modified Card Sorting Test sensitive to frontal lobe defects. Cortex 12, 313–324. doi: 10.1016/S0010-9452(76)80035-4
Oldfield, R. C. (1971). The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9, 97–113. doi: 10.1016/0028-3932(71)90067-4
Perret, E. (1974). The left frontal lobe of man and the suppression of habitual responses in verbal categorical behaviour. Neuropsychologia 12, 323–330. doi: 10.1016/0028-3932(74)90047-5
Radloff, L. S. (1979). The CES-D Scale: a self-report depression scale for research in the general population. Appl. Psych. Meas. 1, 385–401. doi: 10.1177/014662167700100306
Reitman, W. R. (1964). “Heuristic decision procedures, open constraints, and the structure of ill-defined problems,” in Human Judgments and Optimality, ed M. W. Shelly and G. L. Bryan (New York, NY: Wiley), 282–315.
Rorden, C., Fridriksson, J., and Karnath, H.-O. (2009). An evaluation of traditional and novel tools for lesion behavior mapping. Neuroimage 44, 1355–1362. doi: 10.1016/j.neuroimage.2008.09.031
Rorden, C., and Karnath, H.-O. (2004). Using human brain lesions to infer function: a relic from a past era in the fMRI age? Nat. Rev. Neurosci. 5, 813–819. doi: 10.1038/nrn1521
Rorden, C., Karnath, H.-O., and Bonilha, L. (2007). Improving lesion-symptom mapping. J. Cogn. Neurosci. 19, 1081–1088. doi: 10.1162/jocn.2007.19.7.1081
Rudrauf, D., Mehta, S., Bruss, J., Tranel, D., Damasio, H., and Grabowski, T. J. (2008). Thresholding lesion overlap difference maps: application to category-related naming and recognition deficits. Neuroimage 41, 970–984. doi: 10.1016/j.neuroimage.2007.12.033
Saint-Cyr, J. A., Taylor, A. E., and Lang, A. E. (1988). Procedural learning and neostriatal dysfunction in man. Brain 111, 941–959. doi: 10.1093/brain/111.4.941
Schmidt, K.-H., and Metzler, P. (1992). Wortschatztest [vocabulary test] (WST). Weinheim: Beltz Test GmbH.
Shallice, T. (1982). Specific impairments of planning. Philos. Trans. R. Soc. Lond. B Biol. Sci. 298, 199–209. doi: 10.1098/rstb.1982.0082
Shallice, T., and Burgess, P. (1991). Deficits in strategy application following frontal lobe damage in man. Brain 114, 727–741. doi: 10.1093/brain/114.2.727
Shallice, T., and Burgess, P. (1996). The domain of supervisory processes and temporal organization of behaviour. Philos. Trans. R. Soc. Lond. B Biol. Sci. 351, 1405–1411. doi: 10.1098/rstb.1996.0124
Smith, D. H., Meaney, D. F., and Shull, W. H. (2003). Diffuse axonal injury in head trauma. J. Head Trauma Rehabil. 18, 307–316. doi: 10.1097/00001199-200307000-00003
Stuss, D. T., Floden, D., Alexander, M. P., Levine, B., and Katz, D. (2001). Stroop performance in focal lesion patients: dissociation of processes and frontal lobe lesion location. Neuropsychologia 39, 771–786. doi: 10.1016/S0028-3932(01)00013-6
Keywords: executive function, problem solving, spatial behavior, Link's cube test, right hemisphere damage, frontal lobe
Citation: Kopp B, Rösser N, Tabeling S, Stürenburg HJ, de Haan B, Karnath H-O and Wessel K (2014) Disorganized behavior on Link's cube test is sensitive to right hemispheric frontal lobe damage in stroke patients. Front. Hum. Neurosci. 8:79. doi: 10.3389/fnhum.2014.00079
Received: 18 June 2013; Accepted: 31 January 2014;
Published online: 17 February 2014.
Edited by:
Lesley K. Fellows, Montreal Neurological Hospital and Institute, CanadaReviewed by:
Lesley K. Fellows, Montreal Neurological Hospital and Institute, CanadaMelissa Duff, University of Iowa, USA
Copyright © 2014 Kopp, Rösser, Tabeling, Stürenburg, de Haan, Karnath and Wessel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bruno Kopp, Department of Neurology, Hannover Medical School, Carl-Neuberg-Str. 1, 30625 Hannover, Germany e-mail:a29wcC5icnVub0BtaC1oYW5ub3Zlci5kZQ==