 Wu Zhang
Wu Zhang Chunmiao Mai
Chunmiao Mai Hongmin Chen
Hongmin Chen Huijun Zhang
Huijun Zhang- 1The First Affiliated Hospital of Jinan University, Jinan University, Guangzhou, China
- 2School of Stomatology of Jinan University, Jinan University, Guangzhou, China
- 3School of Management, Guangdong University of Technology, Guangzhou, China
- 4Center for Studies of Psychological Application, Guangdong Provincial Key Laboratory of Mental Health and Cognitive Science, School of Psychology, South China Normal University, Guangzhou, China
- 5Mental Quality Education Center, Beijing Technology and Business University, Beijing, China
Introduction: Researchers have made efforts to distinguish the behavioral differences and underlying mechanisms that explain the various possible outcomes of dieting (success, failure and relapse). Although extensive research has demonstrated that eating behavior and individual impulsiveness are closely related to subjective appetite and decision making, very few studies have investigated how subjective and appetite impulsiveness is affected by reactive dieting.
Methods: In the present study, we utilized the power of food scale (PFS) and the intertemporal choice task and to examine subjective appetite and impulsivity of decision making in orthodontic patients. As a result of their orthodontic devices and the subsequent pain and discomfort caused by eating, these patients become reactive dieters. In order to explore the dynamic influence of orthodontic treatment on appetite and impulsiveness, we collected data for both patients and control participants across three testing sections. We also computed a regression model for further exploration in explaining how potential factors contributed to different choices.
Results: We found that the orthodontic group scored significantly lower in PFS than the control group, which indicated a suppression in appetite. Besides, reward and waiting time were significant factors in computational perspective. Moreover, although patients showed a bias in choosing smaller, immediate reward options, they exhibited a decrease in the delay discounting rate as treatment progressed. These findings confirm that subjective appetite and impulsiveness were inhibited due to reactive dieting.
Introduction
People proactively control their diet for a variety of reasons, such as weight control, keeping fit, reducing blood glucose and lipids, religious fasting. During the dieting process, one has to overcome food temptation or even ignore nutritional needs to achieve a healthy balance between subjective desires and objective goals. For dieting to be successful, previous eating habits need to be changed by inhibiting dietary needs. Consequently, the inhibition capacity of each individual plays a key role in whether they will succeed in dieting or not.
Eating habits are also closely related to individual impulsiveness. Generally, impulsive individuals find it difficult to manage their diet and develop good eating habits. This phenomenon has been observed in a variety of diverse groups (Nederkoorn et al., 2006a,b; van den Berg et al., 2011; Weafer and Fillmore, 2012). More specifically it has been found that impulsiveness is closely related to inhibition capacity. Extensive research had demonstrated that bingeing individuals show lower inhibition capacity in comparison to healthy controls towards food stimuli in response inhibition tasks (Volkow and Wise, 2005; Grosshans et al., 2011; Lyu et al., 2016). Personal body mass index (BMI) has been seen to be positively associated with reaction time in a stop-signal task among impulsive individuals (Mühlberg et al., 2016), demonstrating that people with high trait impulsivity and poor control in weight have the difficulty in inhibiting responses. Individuals with relatively low inhibition capacity have been shown to consume much more high-calorie foods than those with a higher inhibition capacity (Houben, 2011; Houben and Jansen, 2011). In a recent study, dieters passively viewed food cues while activity in the inferior frontal gyrus, a brain region associated with inhibitory control, was measured (Lopez et al., 2016). Results showed reduced activation in this region in dieters with high desire to food compared to the dieters with low desire. This suggests that more cognitive resources were required to inhibit food stimuli-related impulsivity in order to balance the cognitive conflict between food temptation and dietary needs (Keller and Hartmann, 2016). These results suggest that top-down regulation of appetite plays a key role in determining whether dieters were able to diet successfully. This is consistent with the notion that regulation ability determines whether people can control eating behavior effectively (Papies et al., 2008; Werthmann et al., 2011).
Therefore, the training to improve regulation ability has been used as an approach to inhibit appetite for specific foods in individuals (Houben and Jansen, 2011; Houben, 2011; Veling et al., 2011a; Forman et al., 2016; Adams et al., 2017). This training was particularly effective for long-term dieters (Veling et al., 2011b). Results showed that foods related to nogo-signals were rated lowly while foods related to go-signals were rated more highly.
The above studies demonstrate that appetite control and the ability to behaviorally inhibit food-related stimuli are closely related. In addition to this line of research, the relationship between appetite and inhibition within the context of decision making has also been examined (Bartholdy et al., 2016). For instance, a study has found that the ability of overweight women to choose to delay gratification is positively correlated to their ability to inhibit food. Indeed, this correlation was more significant when they were shown food-related stimuli compared to when they were shown non-food stimuli, indicating that impulsiveness on decision making tasks can be influenced by inhibition capacity of food-related stimuli (Yeomans and Brace, 2015). Overall, these results offer some suggestion that eating and appetite do not only involve behavioral inhibition of food stimuli, but are also likely to engage more complex processes of impulsivity inhibition relating to goal-based decision making.
However, the aforementioned studies only focused on the participants with obesity or eating disorder, and thereafter have difficulty in distinguishing the effect of dietary habits from the effect of inherent factors, e.g., metabolic capability. In addition, the motivation of proactive dieter who changes his or her eating habits intentionally is associated with inhibiting behavior. Given the scarcity of relevant studies, we aimed to explore more fully the question of whether dietary habits or appetite influence impulsiveness in normal individuals.
Orthodontic treatment has a great impact on both the eating habits and appetite of patients especially in the early stage of the procedure. During this stage, arch wire attachments are used to apply direct force to irregular teeth. This inflicts pain and discomfort on patients, which in turn causes dietary restriction. This leads to an alteration in the eating habits of orthodontic patients such that they become more restricted. Thus, the application of orthodontic devices triggers a conflict between the desire to eat food and the oral pain and discomfort that they experience as a consequence of trying to satisfy this desire. In this way it is similar to individuals who proactively overcome food temptation in order to lose weight. That is, orthodontic patients have to overcome eating difficulties and various forms of discomfort caused by orthodontic treatment in the short term in order to achieve future improvement in oral aesthetics and functionality. But they have no specific motivation on diet. Given the notion that orthodontic devices cause patients to modulate their diet in a reactive manner, we can argue that changes in eating habits may affect their ability to balance short-term difficulties with long-term improvements. Through studies of orthodontic patients, it will be possible to develop a deeper understanding about how individual eating habits and appetite influence impulsivity in decision making.
Such a conflict between immediate discomfort and future interests lends itself to intertemporal choice (Frederick et al., 2002). This refers to choices in which individuals must make a tradeoff between costs and benefits occurring at different times (Liang and Liu, 2011). The classic example of such a tradeoff involves smaller sooner (SS) rewards and larger longer (LL) rewards. From the perspective of a rational economist, people should choose larger delayed rewards to maximize their interest. However, people are generally biased towards more immediate rewards. This is especially true for individuals who are highly impulsive (Thaler, 1981; O’Donoghue and Rabin, 1999). Mazur (1984) proposed that people tend to discount the subjective value of money as a function of delays in time. He explained this choice pattern mathematically using a hyperbolic function: SV = R/(1 + kT), where SV represents the subjective value of the delayed reward R associated with waiting time T, and k was the delay discounting rate. The first goal of this study was to explore whether appetitive changes brought about by orthodontic devices impact impulsivity in decision making during treatment. Impulsivity in this case refers to an increased preference for immediate rewards. More specifically this can be described as an increase in the delay discounting rate.
The classic intertemporal choice paradigm modulates two dimensions, available reward and waiting time. Traditionally a bias for immediate rewards has been explained as the result of subjective devaluation as a function of delayed time, as described by the hyperbolic discounting model (Mazur, 1984; Laibson, 1997). But other studies have put forward different perspectives. Hariri et al. (2006) found that high discounters exhibited greater ventral striatal activation in comparison to low discounters when they were faced with immediate rewards, demonstrating that high discounters overestimate immediate rewards rather than underestimate future rewards. Another ERP study has drawn similar conclusions that high discounters overvalue immediate rewards (Cherniawsky and Holroyd, 2013). However, some researchers consider that the bias to immediate rewards in high discounters is generated by amplified subjective temporal perception (Zauberman et al., 2009). Thus, the second goal of this study was to examine the delay discounting rate of orthodontic patients in more detail by determining the influence of appetitive changes on both the reward sensitivity and time sensitivity during intertemporal choice.
In this study, we utilized the power of food scale (PFS; Cappelleri et al., 2009) to evaluate subjective appetite and an intertemporal choice task to explore individual impulsiveness on decision making. We measured the performance of a group of orthodontic patients on these two tasks and compared it with a group of normal controls. In orthodontics, the treatment process is divided into various temporal periods (Brown and Moerenhout, 1991): early treatment (2 weeks after applying devices), middle adaptation (4 weeks later), and subsequent adaptation period (4 months later). In order to explore the dynamic effects of eating habits and appetite on impulsivity in decision making, we tracked behavior changes across three distinct sections: the first, before treatment; the second, early treatment; and the third, adaptation to treatment. Previous studies have observed that inhibition training in behavioral responding to food stimuli can lead to a subsequent devaluation in the attractiveness of those food items. Given this finding, we hypothesized that a reduction in appetite caused by orthodontic-related difficulties in eating would lead to a reduction in impulsive responding of patients. More specifically, patients would choose less SS options in the intertemporal task and show a related reduction in their delay discounting rate after the application of an orthodontic device. Meanwhile, the orthodontic devices led to restraint on patients’ daily diet instead of their monetary rewards. Therefore, we predicted that the time sensitivity of patients, rather than reward sensitivity, would change significantly as a result of orthodontic treatment. This prediction is driven by the assumption that, during treatment, patients would have had to overcome conflicts between long time-consuming treatment and urgent desires of improving appearance. A consequently weakened sensitivity to time as well an underestimation of subjective time perception would bring about a decrease in choices for SS options.
Materials and Methods
Participants
The orthodontic patients were recruited from the dental department of a public hospital and were devoted to the treatment of orthodontics. They had never received orthodontic treatment before our recruitment. Thirty-three of them finished all measures in three test sections. Participants who performed absolute choice preference in the task were excluded. After exclusion, the orthodontics group consisted of 30 patients who would undergo orthodontic treatment (11 males, 19 females; mean age = 23.40, SD = 5.78; education = 14.00, SD = 1.92). The control group consisted of 31 adults (7 males, 24 females; mean age = 22.42, SD = 2.29; education = 15.13, SD = 1.80). They were recruited from local community and campus. Groups were matched on sex (χ2 = 1.45, p = 0.23) and age (t(59) = 0.88, p = 0.38). But the orthodontics group had shorter education years than the control group (t(59) = −2.37, p = 0.02). All participants were right-handed, had normal or corrected-to-normal vision, were not color-blind, had no psychiatric illness and had not experienced dieting or suffered from eating disorders.
All orthodontic patients wore Self-brackets (Demon Q) and Demon CuNiTi Round 0.014 from KaVo-Sybron Dental Co., Ltd (Shanghai).
This study was carried out in accordance with the recommendations of Ethics Guideline, the Human Research Ethics Committee for Non-Clinical Faculties in South China Normal University. The protocol was approved by the Human Research Ethics Committee for Non-Clinical Faculties in South China Normal University. All subjects gave written informed consent in accordance with the Declaration of Helsinki. They could gain 50 RMB as reward after finishing all the three tests.
Measurement Scale
The PFS was developed to assess the psychological impact of food and as a measure of subjective appetite for palatable food (Cappelleri et al., 2009). It has since been revised into an Asian version (Yoshikawa et al., 2012). The scale consists of 15 items, involving three levels of food proximity: food available indicates the degree of the desire to eat when palatable food is available in the environment but not physically present, food present indicates the degree of the desire when palatable food is present at hand, food tasted indicates the degree of the desire when we taste palatable food but not consume it (Cappelleri et al., 2009). Each item is rated from one to five points. Higher total scores indicate a greater influence of palatable food in the three contexts with different food proximity, referred to participant’s decreased ability to resist food temptation and increasing odds of being obese.
Task
The intertemporal choice task required participants to select one of two monetary reward choices. One choice represented an immediate but smaller reward, the other one represented a larger but delayed reward. Participants were instructed that aim of the task was to assess how people make decisions about different monetary rewards. Each trial consisted of one option with a relatively smaller monetary reward (5, 10, 20, 30, 40, 50, 60, 70, 80, 90 yuan) obtainable right now (SS option), and one option with a relatively larger monetary reward (100 yuan) obtainable after a longer delay (LL option). Participants were asked to choose by pressing a key corresponding to the laterality of their preferred option I left or right). Reward sensitivity was calculated as the difference between every combination of LL and SS presented during the task (Δ Reward: 10, 20, 30, 40, 50, 60, 70, 80, 90, 95 yuan). Waiting time was calculated as the difference between the waiting time associated with LL and SS options (Δ Time: 1 day, 1 week, 1 month, 6 months, 1 year and 2 years). Each trial ran as follows: a fixation point (“+”) appeared in the screen center for 1,000 ms. Then reward options were presented for 5,000 ms or disappeared once an option had been selected. Following this, feedback on the participant’s choices was presented for 1,000 ms (see Figure 1). Pairs of stimuli were displayed randomly and counterbalanced across the left and right side of the screen. Each amount (from ¥5 to ¥ 95) and delay duration were repeated twice (one time per left and right side). The computerized task consisted of 120 trials.
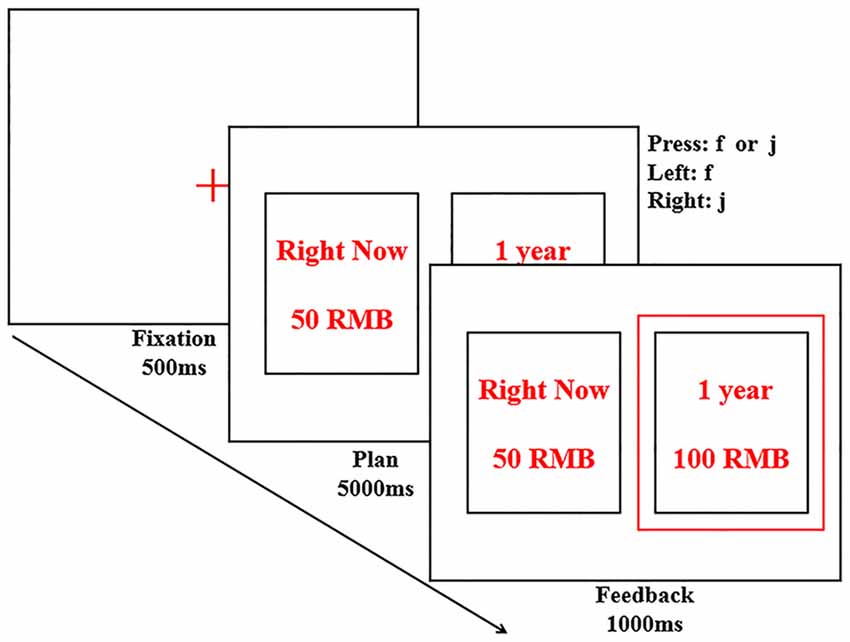
Figure 1. Illustration of the procedure in the intertemporal choice task. Subjects were asked to choose one of the options by pressing “f” or “j” key and shown feedback in red frame. In this trial, the participant chose an option with Δ Time of 1 year and Δ Reward of 50 yuan. In the actual experiment, options were presented in Chinese.
Procedure
All participants were required to participant in the behavioral tasks and fill all measurement scales involved in three separate sections. Experimental tasks and conditions were maintained the same for each section. The orthodontics group participated in the first section before they adopted the orthodontic treatment. This represented a baseline measure. The second section was conducted 2 weeks after the orthodontic devices have been put in place. This section aimed to probe how the orthodontic treatment had affected patient performance. The third and last section was conducted 6 weeks after the treatment. This represented the adaption phase for orthodontic patients at which point, according to customary orthodontic wisdom, patients will have gotten used to the treatment. Control participants completed all three sections in accordance with the time intervals of the patient group.
All data were collected in the behavioral lab affiliated with South China Normal University. Once participants arrived at the lab, they were given instructions about what was required from them during the experiment. All stimuli were presented on a 14-inch computer screen which was positioned 23 inches away from participant. Each experimental section consisted of two parts: the PFS scale and the intertemporal choice task. Sufficient practice was provided prior to the main tasks to ensure that participants were familiar with what was required of them. The whole procedure lasted 20 min and included breaks.
Statistical Analysis
The data of subjects who performed absolute choice preference (always chose most of the SS or LL in three tasks) were eliminated from further analysis. Three patients who always chose SS options in all the three tests and two controls who always selected LL options were excluded. Reaction trials too fast (RT <500 ms) or too slow (RT >4,000 ms) were further eliminated. Over the three sections, 1%, 1% and 4% of trials in the orthodontics group respectively were removed as a consequence. The control group had 2%, 0.4% and 1% of trials removed.
This study aimed to explore the dynamic impact of orthodontic treatment on decision-making. We measured reward sensitivity (Δ Reward), time sensitivity (Δ Time), the percentage of SS choice, reaction time and delay discounting rate (k value) to quantify decision-making behavior. We conducted a 2 (group: orthodontics and controls) × 10 (Δ Reward: 10, 20, 30, 40, 50, 60, 70, 80, 90, 95 yuan) × 6 (Δ Time: 1 day, 1 week, 1 month, 6 months, 1 year and 2 years) × 3 (test time: first, second and third test) mixed design.
Data analyses were performed using SPSS 17.0 including χ2 test, independent T-test, repeated measures ANOVA, post hoc comparisons and logistics regression. Behavioral performances of the two groups were compared across the three research sections.
Results
Measurement Scale
Scores for PFS of all participants were calculated (see Figure 2). We computed a mixed ANOVA with group as a between-subjects factor, test time as a within-subject factor and PFS scores as dependent variable. We found that the main effects for both group (F(1,59) = 13.07, p = 0.001, = 0.18, power = 0.95) and time (F(2,118) = 11.75, p < 0.001, = 0.17, power = 0.99) were significant. Multiple comparisons (LSD, Least Significant Difference; same as follows) showed differences between PFS scores taken from the first and second sections and between the first and third sections (p = 0.001 and p < 0.001 respectively). The interaction effect was also statistically significant (F(2,118) = 7.13, p = 0.001, = 0.11, power = 0.93). A simple effects test showed that there were significant differences in PFS scores for the two groups across all three sections (all ps < 0.02). PFS scores for the orthodontics group were generally lower than those of the control group. More importantly, they showed a decrease over testing sections, which suggests that appetite declined with time.
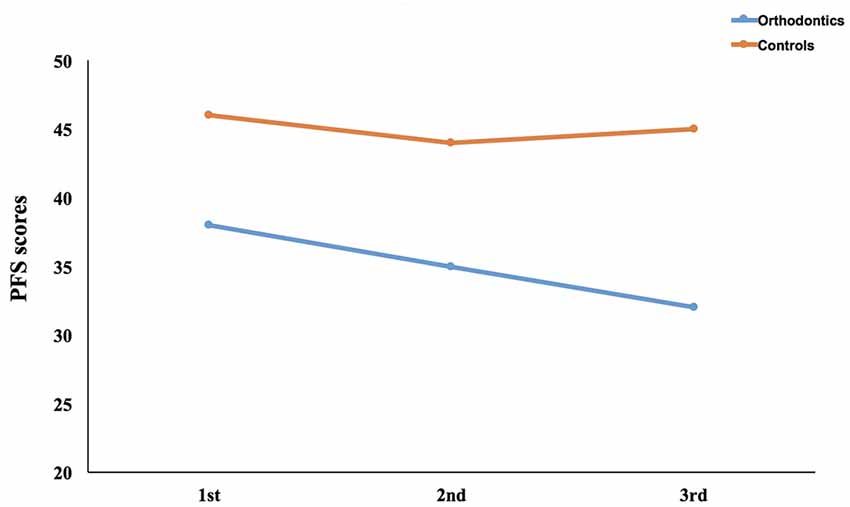
Figure 2. Results of power of food scale (PFS) across three sections. We calculated the PFS scores in all the three sections between the orthodontics group and the control group.
Reaction Time
We calculated a mixed ANOVA with reaction time as a dependent variable, group as a between-subjects factor (see Table 1). Choice (SS, LL) and test time were used as within-subject factors. The main effect of group was marginally significant (F(1,59) = 3.42, p = 0.07, = 0.06, power = 0.44), while that of choice was not significant (F(1,59) = 0.87, p = 0.36, = 0.02, power = 0.15). As the test time yielded a main effect (F(2,118) = 42.29, p < 0.001, = 0.42, power = 1.00), post hoc tests were conducted and showed that the reaction time decreased significantly with testing sections (all ps < 0.001). Although the interaction effect between group and choice yielded a clearly significant difference (F(1,59) = 6.94, p = 0.01, = 0.11, power = 0.74), none of the interaction effects reached the point of statistical significance (all ps > 0.6). A simple effects test indicated that participants from the orthodontics group were faster than those in the control group across all the three sections when selecting SS options (all ps < 0.05), however this was not evident when considering the LL option.
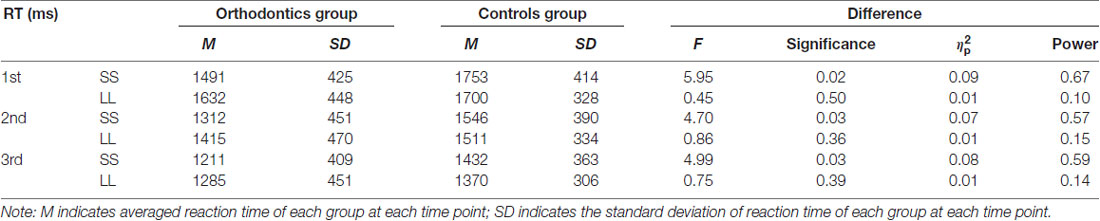
Table 1. Performance of reaction time.
Choice Preference
To evaluate preference in choice between the two groups, we calculated a mixed ANOVA with percentage of SS options as a dependent variable (see Table 2). Only the main effect of group was evident (F(1,59) = 20.70, p < 0.001, = 0.26, power = 0.99), revealing that participants from the orthodontics group showed a much stronger bias to SS option than those from the control group. Results from reaction time performance and choice preference confirm that orthodontics patients preferred to choose smaller and sooner rewards with greater impulsivity than control participants.
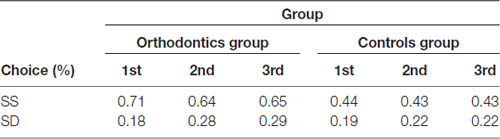
Table 2. Performance of choice preference.
Reward Sensitivity
Reward amount and waiting time were dominant factors affecting decision making. People would balance these two indices when considering SS and LL options. We quantified how monetary reward sensitivity and time sensitivity influenced decision behavior.
The index of Δ Reward was grouped into three values: small Δ (10≤Δ≤30), medium Δ (40≤Δ≤60), large Δ (70≤Δ≤95). To examine the impact of reward sensitivity on choice performance between the two groups across different sections (see Figure 3), we conducted a mixed variance analysis using group as a between-subjects factor, Δ Reward and test time as within-subject factors and percentage of SS options chosen as the dependent variable. We found that the main effect of group was highly significant (F(1,59) = 20.76, p < 0.001, = 0.26, power = 0.99), suggesting that participants from the orthodontics group performed with higher levels of impulsivity toward immediate rewards. The factor Δ Reward was also found to be significant (F(2,118) = 134.88, p < 0.001, = 0.70, power = 1.00). Multiple comparisons revealed that participants chose a significantly higher percentage of SS options for small Δ compared to both medium Δ (p < 0.001) and large Δ (p < 0.001). They also chose a higher percentage of SS options for medium Δ compared to large Δ (p < 0.001). However, neither the main effect of test time, nor the interaction of two factors and three factors were significant. The two groups performed similarly with respect to their patterns of SS options as a function of Δ Reward.
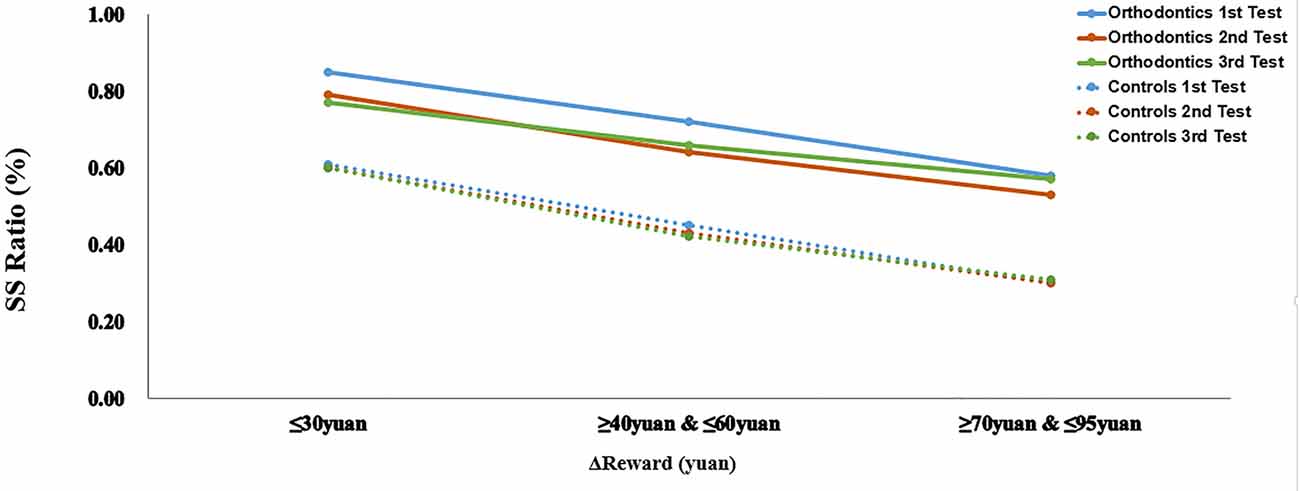
Figure 3. Performance as a function of Δ Reward. The percentage of smaller sooner (SS) choices are presented separately according to the increasing differences in reward magnitude between two groups across three testing sections.
Time Sensitivity
In the following calculation, units of time were represented uniformly as days. The index of Δ Time was divided into six levels: 1 day, 7, 30, 183, 365 and 730 days. The performance of SS selection was calculated between the two groups across the three sections (see Figure 4). A mixed analysis of variance was fit to the data using percentage of SS options as the dependent variable, group was a between-subjects factor and Δ Time as a within-subject factor. We found that main effects for both groups (F(1,59) = 20.94, p < 0.001, = 0.26, power = 0.99) and waiting time (F(5,295) = 165.19, p < 0.001, = 0.74, power = 1.00] to be significantly different. Multiple comparisons showed that the two groups differed in every pairwise comparisons (p < 0.001). The interaction effect between groups and waiting time was clearly significant (F(5,295) = 4.22, p = 0.001, = 0.07, power = 0.96) while all other interaction effects were not significant. A simple effects results showed that two groups differed in all Δ Time conditions (all ps < 0.01) in the first section. The similar patterns were observed in both the second and third test (all ps < 0.05) except in the condition of waiting for 1 day, in which participants did not exhibit different time sensitivity. These results confirm that participants from the orthodontics group showed a greater bias for more impatient choices. A covariate analysis that took education into account did not make a difference to this pattern of results.
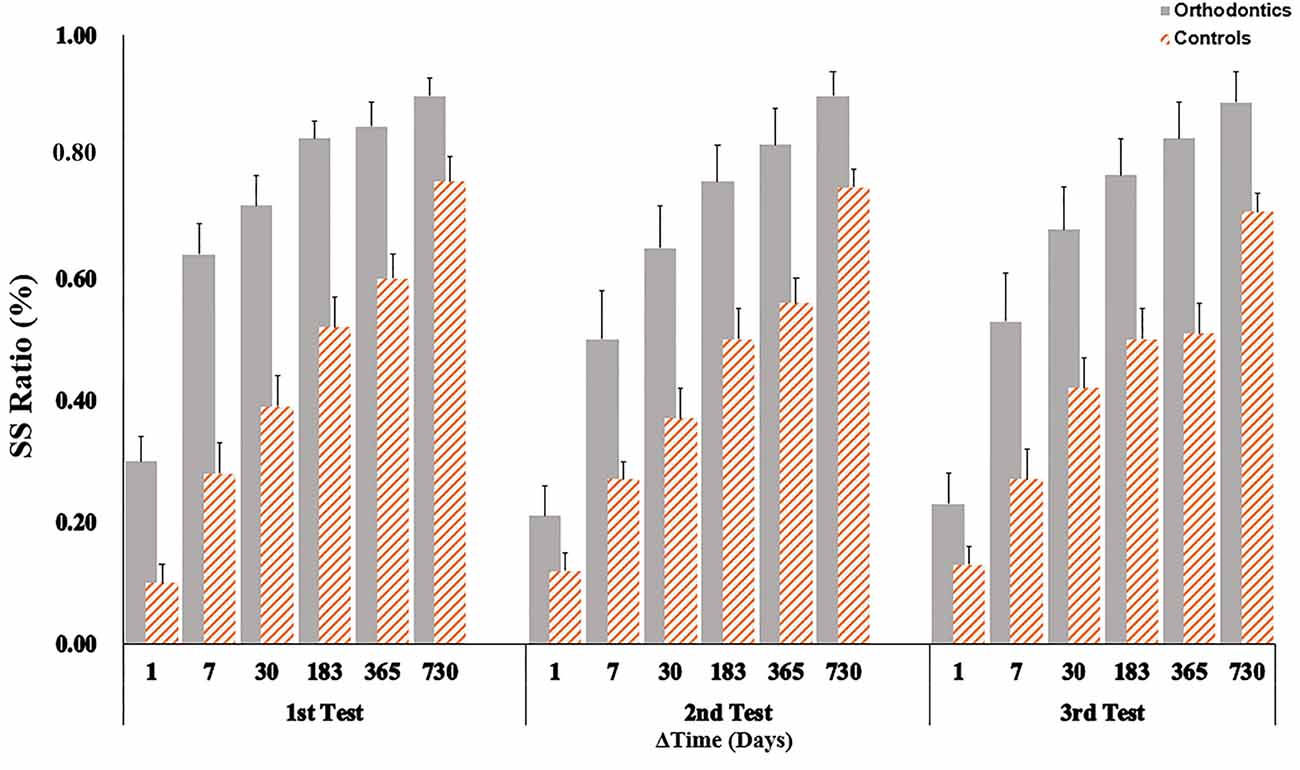
Figure 4. Performance as function of Δ Time. The percentage of SS choices were shown for six different time intervals. Orthodontic patients were biased to choose SS options in each waiting time condition for each section. Error bars showed one standard error.
Binary Logistic Regression in Choice
We computed multivariate unconditional logistics regression to assess how reward and waiting time contributed to the subjects’ choices in trial-by-trial levels. The possible independent variables were considered as Δ Reward and Δ Time. They were z-scored normalized before regression. The dependent variable was the choice (SS = 1, LL = 0). We measured regression coefficients β, odds ratio, 95% confidence interval as well as significance (in the level of p < 0.05), using forward stepwise regression based on maximum likelihood estimation. The overall results were reported in the following table (see Table 3).

Table 3. Overall model of Δ Reward and Δ Time in choice.
Results showed that two factors were significant in explaining the choice (respectively, βΔReward = −2.35, ORΔReward = 0.10, pΔReward < 0.001; βΔTime = 2.65, ORΔTime = 14.18, pΔTime < 0.001). The constant was also significant in the model (β = 0.27, OR = 1.30, p < 0.001). These results confirmed the meaningful relation between reward, waiting time and choice.
To further estimate the contribution of Δ Reward and Δ Time between two group in each test, we calculated the Regression coefficients β values respectively (see Table 4). The independent variables were group, β type and test time while the dependent variable was coefficient β value. We measured a three-factor mixed analysis of variance. However, no significant effect was found in either main effect or interaction effect.
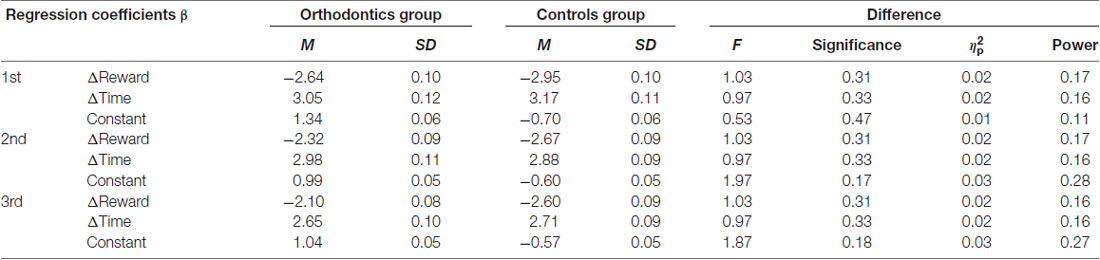
Table 4. Contribution of Δ Reward and Δ Time between two group.
Delay Discounting Function
To examine how subjects discounted rewards according to waiting time before and after orthodontic treatment, we calculated the discount factor for each testing section. Delayed discounts predicted the degree of how people devalued rewards over time. The discount rate is conventionally described through the hyperbolic function (Grossbard and Mazur, 1986; Mazur, 1987). In this study, the hyperbolic function was:
In order to derive the discount rate of each participant (k parameter) when SS option was selected, Grecucci et al. (2014) had transformed equation 1 into formula as follows:
In this formula, RLL represented the reward linked to LL option (RLL = 100), RSS represented the reward linked to SS option, WLL was the waiting time related to LL option and WSS was the waiting time related to SS option (WSS = 0). In this study, the formula could be simplified into: k = ΔReward/(RSS*Δ Time).
To compare the discounting rates between two groups over time, we used group and test time as independent variables with k value as the dependent variable and entered them into a mixed variance analysis (see Table 5). Results showed that the main effect of group was significant (F(1,59) = 13.52, p = 0.001, = 0.19, power = 0.95) although test time was not significant (F(2,118) = 0.87, p = 0.42, = 0.01, power = 0.20). A significant interaction effect was evident (F(2,118) = 3.20, p = 0.04, = 0.05, power = 0.60), with a simple effects test indicating differences in pairwise comparisons (all ps < 0.05). The tendency to discount reward with time of orthodontics patients was greater than that of control participants across all three sections. Post hoc comparison of k value in the orthodontics group showed that there was an obvious difference between the first and second section (p = 0.04), while a significant difference was not observed between the second and third test (p = 0.84). This result demonstrated a remarkable decrease in the discounting rate of orthodontics in the second section.

Table 5. Discounting rate (k value) of both groups.
Some research (Appelhans et al., 2012; Grecucci et al., 2014) had estimated “indifference points,” a balanced index between instant reward and delayed reward in the intertemporal task. It was supposed the point in which people selected 50% equally in SS option (or LL option). In this point, people valued equally in the two options. According to the equation transformation (Grecucci et al., 2014), the computation formula could be as follows:
These points were measured by converting the subjective values. In this study, the formula could be simplified into: WLL = (RLL − RSS)/(k*RSS). To devalue 100 RMB to 50 RMB in the 3rd section, the patients needed 4 days while the controls needed 13 days.
Hyperbolic function graphs were plotted in GraphPad Prism 5 in accordance with the degree of discount in two groups respectively across the three sections (as shown in Figure 5). These show that steepness of the discount curve was greater for the orthodontics group compared to the control group. We also calculated the area under the hyperbolic curve (AUC) for each participant in each section (see Table 6). We performed a mixed ANOVA on groups and test sections as independent variables and AUC as the dependent variable. The main effect of groups was markedly significant (F(1,59) = 25.57, p < 0.001, = 0.30, power = 0.99) while that of test time was only marginally significant (F(2,118) = 2.88, p = 0.06, = 0.05, power = 0.55). The interaction effect was also significant (F(2,118) = 4.46, p = 0.01, = 0.07, power = 0.76). A further simple effects test revealed that AUC of orthodontics patients was clearly larger than controls across all three sections (all ps < 0.002). Consistent with patterns derived from k values, post hoc comparisons showed that the AUC increased significantly in the second test compared to the first test (p = 0.003) but it was similar to the third test (p = 0.65).
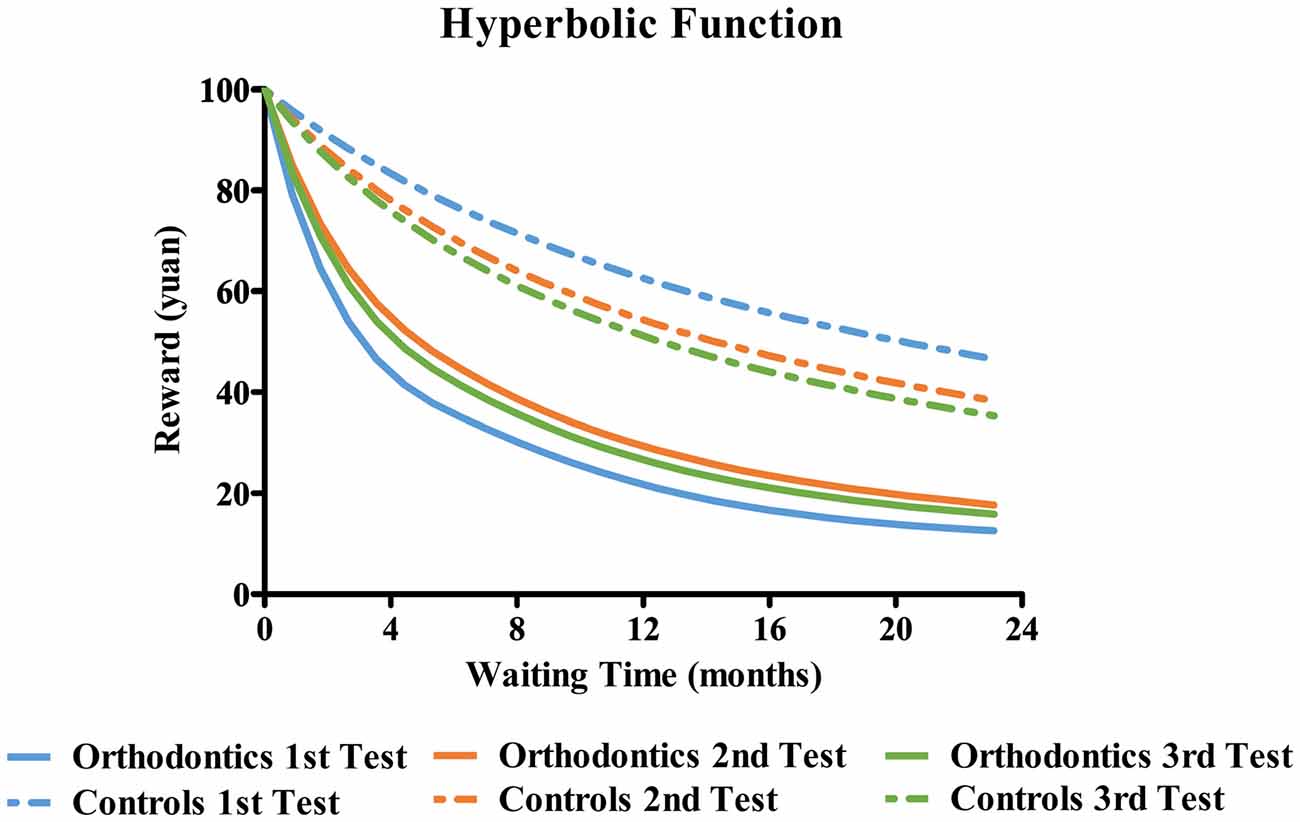
Figure 5. Waiting time and Hyperbolic Function. Fitted hyperbolic functions were plotted for a fixed reward of 100 yuan for both groups according to their k values across three sections. For the purposes of graphical presentation, the unit of waiting time was converted from “days” to “months”. As is illustrated, the orthodontic patients showed steeper discount function compared to control participants across all the three sections.

Table 6. Area behind the curve of two groups (Area).
Task Difficulty
To verify whether the task difficulty made a difference in the reaction time, we measure general linear regression to explore the effects of group and Δutility on reaction time. The choice utility was calculated according to the hyperbolic function: SV = R/(1 + kT). The utility of SS choice was the SS reward while the utility of LL choice was the subjective value after devaluation of LL reward. The Δutility was the result of the difference between LL utility and SS utility.
The results showed that the regression model was significant (F = 217.28, p < 0.01). The factor of group was remarkable in the regression model (t = 85.53, p < 0.01) while the factor of Δutility was excluded to the model (t = 1.38, p = 0.17). 10% of the variation of the reaction time can be explained by changes in the group (corrected R2 = 0.01). These results revealed that reaction time was the result of the difference between two groups rather than the task difficulty.
Individual Appetite and Delay Discounting
In order to explore the relationship between food sensitivity and impulsiveness of decision making in the intertemporal choice task, we computed Pearson correlation analyses between PFS scores (and three PFS subscale scores), as well as SS ratio, RTs of SS choice, and k value for the three sections. Results indicated that individual appetite and task performance were not significantly correlated (all ps > 0.1).
Discussion
This study examined whether appetitive changes caused by difficulties in eating affected impulsivity in decision making. We did this by comparing performance in an intertemporal choice task before and after orthodontic treatment with a group who did not undergone this treatment. The results confirmed our hypothesis that the appetite of orthodontic patients would be suppressed after installation of orthodontic devices, and that there would be a subsequent decrease in impulsiveness as measured by the intertemporal choice task.
There has been a great deal of research on the relationship between individual impulsivity and dietary inhibition, as well as behavioral inhibition. Impulsivity and dietary inhibition may engage a common neural mechanism. For example, the intensity of activity in the brain region of known as the dorso-lateral prefrontal cortex (DLPFC) is generally regarded as an indicator of behavior inhibition capacity. It is closely related to biases in preference for SS options as well as the delay discounting rate in the intertemporal choice task (He et al., 2016; Wesley and Bickel, 2014), and is thought to predict the success rate of individuals in their endeavor to diet or inhibit eating (Weygandt et al., 2015). A serial study has found that the activation intensity of DLPFC during intertemporal choice was positively correlated with dietary inhibition (Dong et al., 2016). Spontaneous neuronal activity of DLPFC in the resting state has also been found to be negatively correlated with dietary inhibition (Dong et al., 2015). These results suggest that these two processes share common neural mechanism. As such, difficulties in eating or dietary inhibition are likely to affect individual impulsivity. Recent studies have illustrated that inhibition training of specific foods contributes to the suppression of food sensitivity and evaluation (Chen Z. et al., 2016; Chen et al., 2017). The researchers manipulated go-nogo training on participants by using food pictures as stimuli, as well as requiring them to evaluate the attractiveness of food pictures related to go-signal and nogo-signal before and after the training. This study supported the arguments that the evaluation to food was affected by individual’s inhibition tendency and that the effect of inhibition training might further affect subjective appetite. Our study was consistent with this notion. Thus, we interpret a persistent reduction in impulsiveness as indexed by the intertemporal choice task is a consequence of eating difficulties experienced by patients as a result of their orthodontics devices through the common neural circuit of behavioral inhibition and impulsivity (Chen S. et al., 2016). Our findings build on this evidence by suggesting that the impact of eating inhibition on behavior not only affect food-related behavior, but also can also be extended to general decision making tasks. In respect to decision making, some previous studies had computed regression analysis in intertemporal choice paradigm to explore the possible factors to the final choice (Appelhans et al., 2012; Grecucci et al., 2014). In our study, the results of regression model have demonstrated the significant contribution of reward factor and waiting time factor to the choice performance.
We found that patients’ subjective appetite for food changed dynamically as the course of the orthodontic treatment progressed. However, previous research in which proactive dieters were more strongly influenced by food after dieting over time suggests the opposite conclusion (Forman et al., 2007). We can put forward two possibilities for this discrepancy. One possibility is that self-report measures are unlikely to accurately reflect the subjective state of participants because of measurement bias and social commitment bias (Sayette et al., 2000). Usually obese individuals tend to underreport subjective appetite or hunger state because of social pressures or feelings of shame (Stunkard, 1959). Indeed, eating tasks have been found to be more effective than self-report measures for subjective appetite (Nijs et al., 2010). The second possibility might be that the orthodontics patients, as reactive dieters, inhibited appetite in order to eat less and to avoid pain and discomfort. This type of appetite inhibition can be described as a more reactive when compared to the more proactive response exhibited by individuals who choose to diet. Besides, this result didn’t support the assumption of the correlation between appetite and impulsiveness. Further studies would benefit from making use of more accurate and objective measures to explain subjective appetite.
In the present study, we observed a significant reduction in subjective appetite in reactive dieters. These were patients faced with pain and discomfort in eating due to the application of orthodontic devices. In addition, we found an associated decrease in impulsive monetary choices over time. According to the hyperbolic function, the smaller this delay discounting rate, the slower the individual discounted subjective value and the less impulsive they were in their decision making (Myerson et al., 2013). This finding demonstrated that the inhibition of eating behaviors regulated impulsivity inhibition in decision making, suggesting the presence of a common physiological mechanism.
It was revealed that the patients had shown a highly impulsive level at the beginning as compared to the controls. One possible explanation was due to their personality of impulsiveness. Wittmann and Paulus (2008) argued that individual differences in temporal perception were likely to affect the delay discounting rate in intertemporal choices to some extent. They observed that an overestimation of time led to an SS bias while underestimation of time led to more LL options. Orthodontic treatment is a medical procedure that carries patients with pain and eating difficulty. Most adult patients make a decision to undertake orthodontic treatment because they are unhappy with their facial appearance and the associated negative impact it has on their daily life. The strong conflict between eager to become good-looking and having to wait patiently are likely to drive them overestimate the time and result in a high impulsivity level.
Limitation
A general limitation of the current study is the significantly higher impulsiveness level in patients as compared to controls in each test section, which make doubts in the generalization of findings about the inhibition effect of reactive dieting in impulsiveness. It is hard to explain this always highly impulsive level in patients at the behavioral perspective. Two groups were categorized based upon whether adopting orthodontic treatment rather than scale measurement. We didn’t control the initial level of impulsivity between two groups. However, it is notable that two groups were balanced in demographics and the grouping criteria was the orthodontic treatment. All the dynamic changes in patients were in result of the treatment effect, more specifically were due to reactive dieting. To control for potential confounding effects in impulsivity, it would be better to utilize the Barratt Impulsiveness Scale (Hollander et al., 1998) as the pre-inclusion standard. A longer tracking examination is helpful to reveal whether the impulsiveness level in patients will continuously decrease along with the treatment.
In respect of reward sensitivity and time sensitivity, they were not significantly affected by orthodontic treatment. The lack of such effects suggests that changes in task performance from patients across sections were related to the interaction of variation between reward magnitude and delay, rather than one specific factor.
An additional limitation is subjective appetite and impulsivity did not differ after a long-term adaptation of orthodontic treatment. Patients exhibited similar levels of food sensitivity and decision-making performance from one stage of treatment to the next. This implies that changes in behavioral and psychological aspects were not affected by the adaptation in 6 weeks after the orthodontic treatment. Whether there is a significant adaptive effect in subsequent treatment periods remains to be seen and would require further, longitudinal study. It would be beneficial to consider whether or not patients remained in a state of reactive dieting and experienced associated difficulties in eating when they are in the late stage of treatment.
Conclusion
This novel study explored the subjective appetite and impulsiveness of decision making in reactive dieters. We found that both of these factors were affected by the restricted diet brought about by the application of orthodontic devices. Reactive dieting suppressed subjective appetite as well as individual impulsivity. This study adds to our understanding of how reactive dieting influences aspects of physiology and behavior.
Author Contributions
WZ and HZ designed the study. CM and WZ collected research data. All four authors finished the manuscript.
Funding
This work was supported by the National Natural Science Foundation of China (No. 31600931) and Guangdong Medical Research Foundation (No. A2017260).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
Adams, R. C., Lawrence, N. S., Verbruggen, F., and Chambers, C. D. (2017). Training response inhibition to reduce food consumption: mechanisms, stimulus specificity and appropriate training protocols. Appetite 109, 11–23. doi: 10.1016/j.appet.2016.11.014
Appelhans, B. M., Woolf, K., Pagoto, S. L., Schneider, K. L., Whited, M. C., and Liebman, R. (2012). Inhibiting food reward: delay discounting, food reward sensitivity, and palatable food intake in overweight and obese women. Obesity 19, 2175–2182. doi: 10.1038/oby.2011.57
Bartholdy, S., Dalton, B., O’Daly, O. G., Campbell, I. C., and Schmidt, U. (2016). A systematic review of the relationship between eating, weight and inhibitory control using the stop signal task. Neurosci. Biobehav. Rev. 64, 35–62. doi: 10.1016/j.neubiorev.2016.02.010
Brown, D. F., and Moerenhout, R. G. (1991). The pain experience and psychological adjustment to orthodontic treatment of preadolescents, adolescents, and adults. Am. J. Orthod. Dentofacial Orthop. 100, 349–356. doi: 10.1016/0889-5406(91)70073-6
Cappelleri, J. C., Bushmakin, A. G., Gerber, R. A., Leidy, N. K., Sexton, C. C., Karlsson, J., et al. (2009). Evaluating the power of food scale in obese subjects and a general sample of individuals: development and measurement properties. Int. J. Obes. 33, 913–922. doi: 10.1038/ijo.2009.107
Chen, S., Dong, D., Jackson, T., Su, Y., and Chen, H. (2016). Altered frontal inter-hemispheric resting state functional connectivity is associated with bulimic symptoms among restrained eaters. Neuropsychologia 81, 22–30. doi: 10.1016/j.neuropsychologia.2015.06.036
Chen, Z., Veling, H., Dijksterhuis, A., and Holland, R. W. (2016). How does not responding to appetitive stimuli cause devaluation: evaluative conditioning or response inhibition? Mol. Cell. Endocrinol. 145, 1687–1701. doi: 10.1037/xge0000236
Chen, Z., Veling, H., Dijksterhuis, A., and Holland, R. W. (2017). Do impulsive individuals benefit more from food go/no-go training? Testing the role of inhibition capacity in the no-go devaluation effect. Appetite 124, 99–110. doi: 10.1016/j.appet.2017.04.024
Cherniawsky, A. S., and Holroyd, C. B. (2013). High temporal discounters overvalue immediate rewards rather than undervalue future rewards: an event-related brain potential study. Cogn. Affect. Behav. Neurosci. 13, 36–45. doi: 10.3758/s13415-012-0122-x
Dong, D., Jackson, T., Wang, Y., and Chen, H. (2015). Spontaneous regional brain activity links restrained eating to later weight gain among young women. Biol. Psychol. 109, 176–183. doi: 10.1016/j.biopsycho.2015.05.003
Dong, D., Wang, Y., Jackson, T., Chen, S., Wang, Y., Zhou, F., et al. (2016). Impulse control and restrained eating among young women: evidence for compensatory cortical activation during a chocolate-specific delayed discounting task. Appetite 105, 477–486. doi: 10.1016/j.appet.2016.05.017
Forman, E. M., Hoffman, K. L., McGrath, K. B., Herbert, J. D., Brandsma, L. L., and Lowea, M. R. (2007). The power of food scale predicts chocolate cravings and consumption and response to a cravings intervention. Appetite 49:291. doi: 10.1016/j.appet.2007.03.071
Forman, E. M., Shaw, J. A., Goldstein, S. P., Butryn, M. L., Martin, L. M., Meiran, N., et al. (2016). Mindful decision making and inhibitory control training as complementary means to decrease snack consumption. Appetite 103, 176–183. doi: 10.1016/j.appet.2016.04.014
Frederick, S., Loewenstein, G., and O’Donoghue, T. (2002). Time discounting and time preference: a critical review. J. Econ. Lit. 40, 351–401. doi: 10.1257/jel.40.2.351
Grecucci, A., Giorgetta, C., Rattin, A., Guerreschi, C., Sanfey, A. G., and Bonini, N. (2014). Time devours things: how impulsivity and time affect temporal decisions in pathological gamblers. PLoS One 9:e109197. doi: 10.1371/journal.pone.0109197
Grossbard, C. L., and Mazur, J. E. (1986). A comparison of delays and ratio requirements in self-control choice. J. Exp. Anal. Behav. 45, 305–315. doi: 10.1901/jeab.1986.45-305
Grosshans, M., Loeber, S., and Kiefer, F. (2011). Implications from addiction research towards the understanding and treatment of obesity. Addict. Biol. 16, 189–198. doi: 10.1111/j.1369-1600.2010.00300.x
Hariri, A. R., Brown, S. M., Williamson, D. E., Flory, J. D., de Wit, H., and Manuck, S. B. (2006). Preference for immediate over delayed rewards is associated with magnitude of ventral striatal activity. J. Neurosci. 26, 13213–13217. doi: 10.1523/JNEUROSCI.3446-06.2006
He, Q., Chen, M., Chen, C., Xue, G., Feng, T., and Bechara, A. (2016). Anodal stimulation of the left DLPFC increases IGT scores and decreases delay discounting rate in healthy males. Front. Psychol. 7:1421. doi: 10.3389/fpsyg.2016.01421
Hollander, E., DeCaria, C. M., Mari, E., Wong, C. M., Mosovich, S., Grossman, R., et al. (1998). Short-time single-blind fluvoxamine treatment of pathological gambling. Am. J. Psychiatry 155, 1781–1783. doi: 10.1176/ajp.155.12.1781
Houben, K. (2011). Overcoming the urge to splurge: influencing eating behavior by manipulating inhibitory control. J. Behav. Ther. Exp. Psychiatry 42, 384–388. doi: 10.1016/j.jbtep.2011.02.008
Houben, K., and Jansen, A. (2011). Training inhibitory control. A recipe for resisting sweet temptations. Appetite 56, 345–349. doi: 10.1016/j.appet.2010.12.017
Keller, C., and Hartmann, C. (2016). Not merely a question of self-control: the longitudinal effects of overeating behaviors, diet quality and physical activity on dieters’ perceived diet success. Appetite 107, 213–221. doi: 10.1016/j.appet.2016.08.007
Laibson, D. (1997). Golden eggs and hyperbolic discounting. Q. J. Econ. 112, 443–478. doi: 10.1162/003355397555253
Liang, Z. Y., and Liu, H. (2011). Exploring the nature of intertemporal choice. Adv. Psychol. Sci. 19, 959–966. doi: 10.3724/SP.J.1042.2011.00959
Lopez, R. B., Milyavskaya, M., Hofmann, W., and Heatherton, T. F. (2016). Motivational and neural correlates of self-control of eating: a combined neuroimaging and experience sampling study in dieting female college students. Appetite 103, 192–199. doi: 10.1016/j.appet.2016.03.027
Lyu, Z., Zheng, P., and Jackson, T. (2016). Attention disengagement difficulties among average weight women who binge eat. Eur. Eating Disord. Rev. 24, 286–293. doi: 10.1002/erv.2438
Mazur, J. E. (1984). Tests of an equivalence rule for fixed and variable reinforcer delays. J. Exp. Psychol. Anim. Behav. Process. 10, 426–436. doi: 10.1037/0097-7403.10.4.426
Mazur, J. E. (1987). “An adjusting procedure for studying delayed reinforcement,” in Quantitative Analyses of Behavior: The Effect of Delay and of Intervening Events on Reinforcement Value (Vol. 5), eds M. L. Commons, J. E. Mazur, J. A. Nevin and H. Rachlin (Hillsdale, NJ: Erlbaum), 55–73.
Mühlberg, C., Mathar, D., Villringer, A., Horstmann, A., and Neumann, J. (2016). Stopping at the sight of food’how gender and obesity impact on response inhibition. Appetite 107, 663–676. doi: 10.1016/j.appet.2016.08.121
Myerson, J., Green, L., and Warusawitharana, M. (2013). Area under the curve as a measure of discounting. J. Exp. Anal. Behav. 76, 235–243. doi: 10.1901/jeab.2001.76-235
Nederkoorn, C., Braet, C., Van Eijs, Y., Tanghe, A., and Jansen, A. (2006a). Why obese children cannot resist food: the role of impulsivity. Eat. Behav. 7, 315–322. doi: 10.1016/j.eatbeh.2005.11.005
Nederkoorn, C., Smulders, F. T. Y., Havermans, R. C., Roefs, A., and Jansen, A. (2006b). Impulsivity in obese women. Appetite 47, 253–256. doi: 10.1016/j.appet.2006.05.008
Nijs, I. M. T., Muris, P., Euser, A. S., and Franken, I. H. (2010). Differences in attention to food and food intake between overweight/obese and normal-weight females under conditions of hunger and satiety. Appetite 54, 243–254. doi: 10.1016/j.appet.2009.11.004
O’Donoghue, T., and Rabin, M. (1999). Doing it now or later. Am. Econ. Rev. 89, 103–124. doi: 10.1257/aer.89.1.103
Papies, E. K., Stroebe, W., and Aarts, H. (2008). The allure of forbidden food: on the role of attention in self-regulation. J. Exp. Soc. Psychol. 44, 1283–1292. doi: 10.1016/j.jesp.2008.04.008
Sayette, M. A., Shiffman, S., Tiffany, S. T., Niaura, R. S., Martin, C. S., and Shadel, W. G. (2000). The measurement of drug craving. Addiction 95, S189–S210. doi: 10.1046/j.1360-0443.95.8s2.8.x
Stunkard, A. (1959). Obesity and the denial of hunger. Psychosom. Med. 21, 281–290. doi: 10.1097/00006842-195907000-00004
Thaler, R. (1981). Some empirical evidence on dynamic inconsistency. Econ. Lett. 8, 201–207. doi: 10.1016/0165-1765(81)90067-7
van den Berg, L., Pieterse, K., Malik, J. A., Luman, M., Willems van Dijk, K., Oosterlaan, J., et al. (2011). Association between impulsivity, reward responsiveness and body mass index in children. Int. J. Obes. 35, 1301–1307. doi: 10.1038/ijo.2011.116
Veling, H., Aarts, H., and Papies, E. K. (2011a). Using stop signals to inhibit chronic dieters’ responses toward palatable foods. Behav. Res. Ther. 49, 771–780. doi: 10.1016/j.brat.2011.08.005
Veling, H., Aarts, H., and Stroebe, W. (2011b). Fear signals inhibit impulsive behavior toward rewarding food objects. Appetite 56, 643–648. doi: 10.1016/j.appet.2011.02.018
Volkow, N., and Wise, R. (2005). How can drug addiction help us understand obesity? Nat. Neurosci. 8, 555–560. doi: 10.1038/nn1452
Weafer, J., and Fillmore, M. (2012). Alcohol-related stimuli reduce inhibitory control of behavior in drinkers. Psychopharmacology 222, 489–498. doi: 10.1007/s00213-012-2667-3
Werthmann, J., Roefs, A., Nederkoorn, C., Mogg, K., Bradley, B. P., and Jansen, A. (2011). Can(not) take my eyes off it: attention bias for food in overweight participants. Health Psychol. 30, 561–569. doi: 10.1037/a0024291
Wesley, M. J., and Bickel, W. K. (2014). Remember the future II: meta-analyses and functional overlap of working memory and delay discounting. Biol. Psychiatry 75, 435–448. doi: 10.1016/j.biopsych.2013.08.008
Weygandt, M., Mai, K., Dommes, E., Ritter, K., Leupelt, V., Spranger, J., et al. (2015). Impulse control in the dorsolateral prefrontal cortex counteracts post-diet weight regain in obesity. Neuroimage 109, 318–327. doi: 10.1016/j.neuroimage.2014.12.073
Wittmann, M., and Paulus, M. P. (2008). Decision making, impulsivity and time perception. Trends Cogn. Sci. 12, 7–12. doi: 10.1016/j.tics.2007.10.004
Yeomans, M. R., and Brace, A. (2015). Cued to act on impulse: more impulsive choice and risky decision making by women susceptible to overeating after exposure to food stimuli. PLoS One 10:e0137626. doi: 10.1371/journal.pone.0137626
Yoshikawa, T., Orita, K., Watanabe, Y., and Tanaka, M. (2012). Validation of the Japanese version of the power of food scale in a young adult population. Psychol. Rep. 111, 253–265. doi: 10.2466/08.02.06.15.pr0.111.4.253-265
Keywords: orthodontic patients, reactive dieters, impulsiveness, intertemporal choice, subjective appetite
Citation: Zhang W, Mai C, Chen H and Zhang H (2018) Impulsiveness in Reactive Dieters: Evidence From Delay Discounting in Orthodontic Patients. Front. Hum. Neurosci. 12:347. doi: 10.3389/fnhum.2018.00347
Received: 28 February 2018; Accepted: 13 August 2018;
Published: 31 August 2018.
Edited by:
Delin Sun, Duke University, United StatesReviewed by:
Ning Ma, RIKEN Brain Science Institute (BSI), JapanYing Wang, University of Science and Technology of China, China
Copyright © 2018 Zhang, Mai, Chen and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hongmin Chen, Y2hlbmhtQGJ0YnUuZWR1LmNu
Huijun Zhang, emhhbmdodWlqdW5AZ21haWwuY29t
† These authors have contributed equally to this work