 Marta Reina-Couto1,2,3,4
Marta Reina-Couto1,2,3,4 Carolina Silva-Pereira1,2
Carolina Silva-Pereira1,2 Patrícia Pereira-Terra1,2
Patrícia Pereira-Terra1,2 Janete Quelhas-Santos1
Janete Quelhas-Santos1 João Bessa1
João Bessa1 Paula Serrão1,2
Paula Serrão1,2 Joana Afonso1,2Sandra Martins5
Joana Afonso1,2Sandra Martins5 Cláudia Camila Dias6,7
Cláudia Camila Dias6,7 Manuela Morato8,9
Manuela Morato8,9 João T Guimarães5,10Roberto Roncon-Albuquerque3,11José-Artur Paiva3,12
João T Guimarães5,10Roberto Roncon-Albuquerque3,11José-Artur Paiva3,12 António Albino-Teixeira1,2†
António Albino-Teixeira1,2† Teresa Sousa1,2†*
Teresa Sousa1,2†*- 1Departamento de Biomedicina—Unidade de Farmacologia e Terapêutica, Faculdade de Medicina da Universidade do Porto (FMUP), Porto, Portugal
- 2Centro de Investigação Farmacológica e Inovação Medicamentosa, Universidade do Porto (MedInUP), Porto, Portugal
- 3Serviço de Medicina Intensiva, Centro Hospitalar Universitário São João (CHUSJ), Porto, Portugal
- 4Serviço de Farmacologia Clínica, CHUSJ, Porto, Portugal
- 5Serviço de Patologia Clínica, CHUSJ and EPIUnit, Instituto de Saúde Pública, Universidade do Porto, Porto, Portugal
- 6Departamento de Medicina da Comunidade, Informação e Decisão em Saúde, FMUP, Porto, Portugal
- 7CINTESIS—Centro de Investigação em Tecnologias e Serviços de Saúde, Porto, Portugal
- 8Laboratório de Farmacologia, Departamento de Ciências do Medicamento, Faculdade de Farmácia da Universidade do Porto, Porto, Portugal
- 9LAQV/REQUIMTE, Faculdade de Farmácia, Universidade do Porto, Porto, Portugal
- 10Departamento de Biomedicina—Unidade de Bioquímica, FMUP, Porto, Portugal
- 11Departamento de Cirurgia e Fisiologia, FMUP, Porto, Portugal
- 12Departamento de Medicina, FMUP, Porto, Portugal
Aims: Inflammation-driven endothelitis seems to be a hallmark of acute heart failure (AHF) and cardiogenic shock (CS). Endocan, a soluble proteoglycan secreted by the activated endothelium, contributes to inflammation and endothelial dysfunction, but has been scarcely explored in human AHF. We aimed to evaluate serum (S-Endocan) and urinary endocan (U-Endocan) profiles in AHF and CS patients and to correlate them with biomarkers/parameters of inflammation, endothelial activation, cardiovascular dysfunction and prognosis.
Methods: Blood and spot urine were collected from patients with AHF (n = 23) or CS (n = 25) at days 1–2 (admission), 3-4 and 5-8 and from controls (blood donors, n = 22) at a single time point. S-Endocan, U-Endocan, serum IL-1β, IL-6, tumour necrosis factor-α (S-TNF-α), intercellular adhesion molecule-1 (S-ICAM-1), vascular cell adhesion molecule-1 (S-VCAM-1) and E-selectin were determined by ELISA or multiplex immunoassays. Serum C-reactive protein (S-CRP), plasma B-type natriuretic peptide (P-BNP) and high-sensitivity troponin I (P-hs-trop I), lactate, urea, creatinine and urinary proteins, as well as prognostic scores (APACHE II, SAPS II) and echocardiographic left ventricular ejection fraction (LVEF) were also evaluated.
Results: Admission S-Endocan was higher in both patient groups, with CS presenting greater values than AHF (AHF and CS vs. Controls, p < 0.001; CS vs. AHF, p < 0.01). Admission U-Endocan was only higher in CS patients (p < 0.01 vs. Controls). At admission, S-VCAM-1, S-IL-6 and S-TNF-α were also higher in both patient groups but there were no differences in S-E-selectin and S-IL-1β among the groups, nor in P-BNP, S-CRP or renal function between AHF and CS. Neither endocan nor other endothelial and inflammatory markers were reduced during hospitalization (p > 0.05). S-Endocan positively correlated with S-VCAM-1, S-IL-6, S-CRP, APACHE II and SAPS II scores and was positively associated with P-BNP in multivariate analyses. Admission S-Endocan raised in line with LVEF impairment (p = 0.008 for linear trend).
Conclusion: Admission endocan significantly increases across AHF spectrum. The lack of reduction in endothelial and inflammatory markers throughout hospitalization suggests a perpetuation of endothelial dysfunction and inflammation. S-Endocan appears to be a biomarker of endothelitis and a putative therapeutic target in AHF and CS, given its association with LVEF impairment and P-BNP and its positive correlation with prognostic scores.
Introduction
Acute heart failure (AHF) is broadly defined as a rapid onset of new or worsening signs and symptoms of heart failure (HF) (McDonagh et al., 2021). These are due to an increase in left ventricular (LV) filling pressure with consequent pulmonary congestion but not necessarily associated with low cardiac output - both HF with reduced or preserved ejection fraction seem to have similar hospital admissions and readmissions (Metra and Teerlink, 2017). In fact, the economic burden of HF is becoming one of the most problematic public health issues with increasing prevalence and costs. Due to the ageing of the population and progressive treatment of HF with significant reduction of mortality (Benjamin et al., 2019; Groenewegen et al., 2020), it represents nowadays the most common diagnosis in patients over 65 years-old with unscheduled admission to hospital in high-income nations (Braunwald, 2015). It also reflects our poor pathophysiologic knowledge because no AHF clinical trials have shown to improve in-hospital symptoms and postdischarge clinical outcomes compared with placebo (Tomasoni et al., 2019), except maybe recently for sacubitril/valsartan where early titration before discharge was demonstrated to be associated with favourable reduction of natriuretic biomarkers, an accepted surrogate for prognostication (Velazquez et al., 2019; Wachter et al., 2019).
From what is known so far, pathophysiology in AHF is presently viewed as consisting theoretically of two phases - initiation and amplification phase (Sabbah, 2017) - in a spiral of multiple concurrent mechanisms contributing for worsening HF and end-organ damage (Harjola et al., 2017). A progressive chronic energetic exhaustion of the failing myocardium or a crescendo of vascular stiffness dependent on neurohormonal activation (Mentz and O'Connor, 2016) with inflammation (Reina-Couto et al., 2021) and endothelial disruption, fluid accumulation and cardiac vicious workload (Colombo et al., 2008) results in the clinical cardinal sign of congestion in most patients with AHF, but a smaller proportion presents with peripheral hypoperfusion or cardiogenic shock (CS) (Chioncel et al., 2017b). This most severe form of AHF remains with an unchanged mortality as high as 50% and also with few evidence-based effective therapeutics (Thiele et al., 2019). Interestingly, we still cannot conclude whether congestion is cause or consequence of endothelial dysfunction (Colombo et al., 2014; Colombo et al., 2015) which remains to be explored in AHF. Nevertheless, even though endothelial dysfunction prognostic significance is well recognized in chronic HF (Alem, 2019; Zuchi et al., 2020), the classical methods for its evaluation are technically challenging and have limited its clinical implementation (Shantsila et al., 2012). Also, the assessment of systemic endothelial biomarkers is not yet consolidated for clinical practice, namely for AHF.
Endocan, previously designated as endothelial cell-specific molecule-1 (ESM-1), is a soluble dermatan sulfate proteoglycan synthetized specifically by endothelial cells, probably mirroring inflammation-driven “endothelitis” (Lassalle et al., 1996). There has been an increasing interest in exploring endocan’s utility as a biomarker in a wide spectrum of pathological states, particularly in sepsis, acute respiratory distress syndrome and several cardiovascular diseases (De Freitas Caires et al., 2018; Bessa et al., 2020). Increased values independently related with prognosis and cardiovascular events have been recently reported for endocan in coronary and chronic HF patients (Kosir et al., 2019; Ziaee et al., 2019) and its therapeutic potential has just started to be explored for cancer (Zhang et al., 2021). As it can be easily detected in the human bloodstream and was proved to be stable, intact and reliable in critical patients (Gaudet et al., 2017), we aimed to explore serum and urinary endocan profiles in AHF and CS patients, where endothelial activation and congestion seem to be plausible and specific hallmarks. Furthermore, we analysed their correlation with prognostic parameters as well as with mechanistic biomarkers of inflammation, endothelial activation or cardiovascular dysfunction.
Materials and methods
Study design and population
The present study is part of a larger research project (RIFF-HEART—Resolution of inflammation: a missing key to improve acute heart failure treatment and prognosis?) involving patients admitted to the Service of Intensive Care Medicine of a tertiary hospital (Centro Hospitalar Universitário São João, CHUSJ).
We performed a single-centre cohort study and consecutively recruited patients with a single diagnosis of AHF (n = 23) or CS (n = 25) admitted to the Service of Intensive Care Medicine of CHUSJ, from January 2017 to December 2019. Controls (n = 22) were recruited among healthy blood donor volunteers from the Service of Immunohemotherapy of CHUSJ, from September 2017 to October 2017. All eligible patients (or their legal representative) provided written informed consent to participate in the study. Blood donor volunteers provided verbal informed consent. The study protocol conforms to the Guidelines for Good Clinical Practice and the ethical guidelines of the 1975 Declaration of Helsinki. The study was approved by the institution’s ethics committee (CES 75-16).
Clinical data and sample collection
Physical examination of the patients was performed during their Intensive Care Unit (ICU) stay and a record of demographic and clinical data was completed by the medical team of the project and anonymously coded to the project database, along with laboratory data, guaranteeing confidentiality. Illness severity was assessed by the Acute Physiology and Chronic Health Evaluation II (APACHE II) and Simplified Acute Physiology Score II (SAPS II) scoring systems at ICU admission, as well as by the values of the natriuretic peptide in use in our centre (plasma B-type natriuretic peptide, P-BNP) and the echocardiographic LV ejection fraction (LVEF). ICU length of stay, total hospital length of stay, in-hospital mortality and mortality at 1 year were also evaluated.
Blood and spot urine samples were collected in patients (AHF and CS groups) at 3 different time points during ICU stay, whenever possible: up to 48 h (days 1–2, admission), on days 3–4 and on days 5–8 after ICU admission. All samples from CS patients on mechanical circulatory support were obtained at days 1–2, days 3–4 and days 5–8 after veno-arterial extracorporeal membrane oxygenation (VA-ECMO) initiation which coincided with ICU admission. Samples (blood and spot urine) from controls were collected at a single time point. All samples were processed within 1–2 h of collection and stored at −80°C until assayed.
Routine clinical biochemical and cardiac markers
P-BNP and plasma high-sensitivity troponin I (P-hs-trop I) were measured by chemiluminescent microparticle immunoassays using an Abbot® Architect i2000 automated analyser (Abbott® Diagnostics, Lake Forest, IL, USA). A Beckman Coulter® AU5400 automated clinical chemistry analyser (Beckman Coulter®, Portugal) was used for the quantification of serum C-reactive protein (S-CRP) by an immunoturbidimetric assay, serum urea (S-Urea) concentration by a kinetic urease/glutamate dehydrogenase method, plasma and urine creatinine by the colorimetric Jaffe method and urinary protein by the pyrogallol red method. Lactate was evaluated by blood gas analysis.
Quantification of serum and urinary endocan
Serum and urinary endocan (S-Endocan and U-Endocan, respectively) were quantified by enzyme-linked immunosorbent assays (ELISA) using commercial kits (S-Endocan: “Just Do It ELISA Kit H1”, JDIEK H1, Lunginnov, Lille, France; U-Endocan: Human ESM1/Endocan ELISA Kit, LS-F24487, LSBio, Inc., Seattle, USA). U-Endocan values were corrected for urinary creatinine concentrations.
Quantification of other biomarkers of endothelial activation and inflammation
Other serum endothelium activation markers (serum intercellular adhesion molecule 1, S-ICAM-1; serum vascular cell adhesion molecule 1, S-VCAM-1; serum E-Selectin, S-E-Selectin) and proinflammatory cytokines (serum interleukin 6, S-IL-6; serum interleukin one beta, S-IL-1β; serum tumour necrosis factor alpha, S-TNF-α) were evaluated by multiplex immunoassays using a Luminex 200™ xMAP™ analyzer (Luminex Corporation, Austin, TX, USA), according to the protocols of Human Premixed Multi-Analyte Magnetic Assay (R&D Systems, Inc., Minneapolis, USA) and Human High Sensitivity T Cell Magnetic Bead Panel (Milliplex® Map kit, Millipore Corporation, Billerica, MA, USA), respectively. Raw data analysis (mean fluorescence intensity) was performed using a standard five parameter logistic (5-PL) curve fit created by the Luminex xPONENT ® Software (version 3.1).
Data and statistical analysis
Results are expressed as mean ± standard error of the mean (SEM) or as median (25th percentile; 75th percentile) for data with normal or non-normal distribution, respectively, or as percentage, and are graphically represented as Box and Whiskers plots (Figures 1–5 and Figure 8) or as scatter plots (Figures 6, 7) or as Kaplan-Meier plot (survival analysis; Supplementary Figure S1). Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (Levey et al., 2009). Statistical analysis was conducted using the GraphPad Prism 9 software (La Jolla, USA) and the IBM SPSS Statistics 27 software (IBM Corporation, New York, USA). Results were analysed by unpaired Student’s t-test or Mann–Whitney U-test, for comparisons between two groups, or by one-way ANOVA followed by a Tukey’s multiple comparison test or a Kruskal–Wallis test followed by a Dunn’s post hoc test, for comparison between three groups, where appropriate. The value of p for linear trend was estimated by one-way ANOVA followed by a post hoc test for trend, after applying a base 10 log transformation to the variables with non-normal distribution. Categorical variables were analysed by the Fisher’s exact test or by the Chi-Square test. Biomarkers evolution throughout the hospitalization was analysed by Wilcoxon matched pairs signed rank test. Spearman’s correlation analysis was used to estimate correlations between sets of nonparametric data in AHF and CS patients at admission. All p values of <0.050 were considered significant.
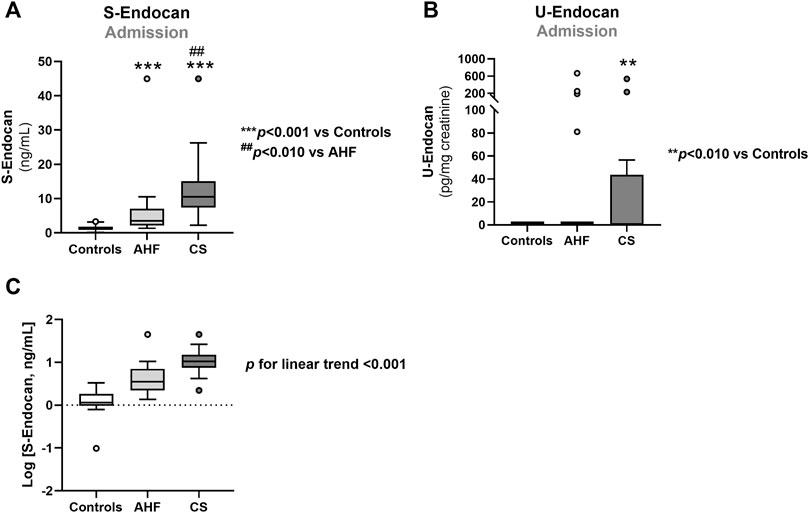
FIGURE 1. Serum endocan (A,C) and urinary endocan (B) concentrations at admission in controls, CS and AHF patients. Results are presented in Box-and-Whiskers plot. AHF, acute heart failure; CS, cardiogenic shock; S-Endocan, serum endocan; U-Endocan, urinary endocan.
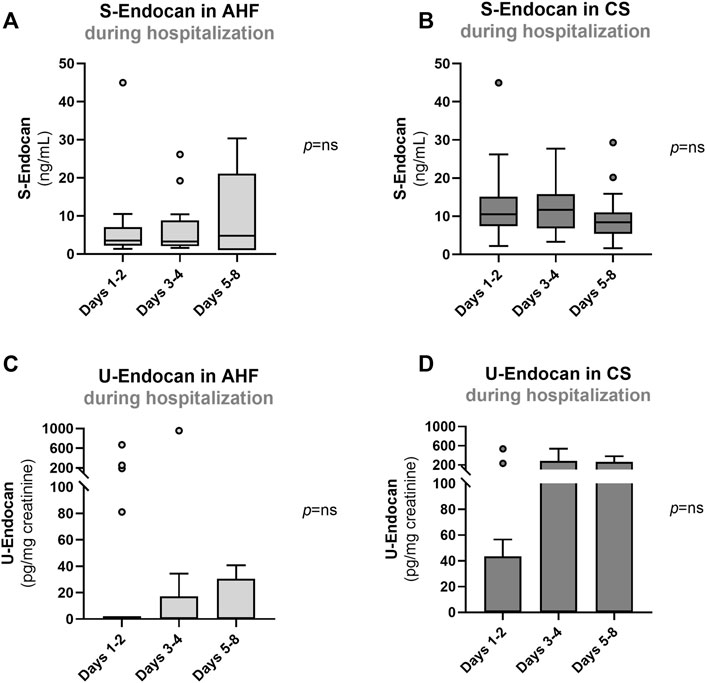
FIGURE 2. Serum (A, B) and urinary endocan (C, D) at days 1–2, days 3–4 and 5–8 in patients with AHF or with CS. Results are presented in Box-and-Whiskers plot. AHF, acute heart failure; CS, cardiogenic shock; S-Endocan, serum endocan; U-Endocan, urinary endocan.
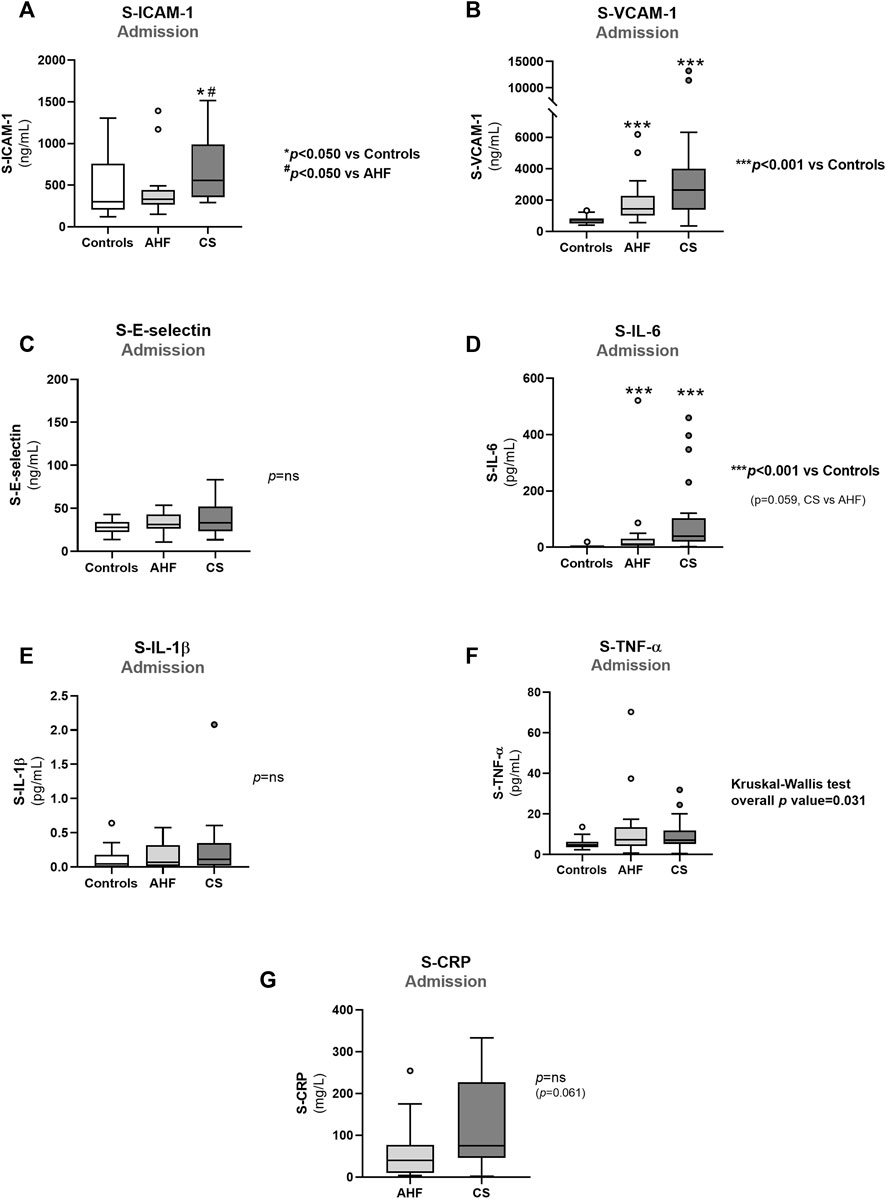
FIGURE 3. Admission values of biomarkers of endothelial dysfunction and inflammation in controls, AHF and CS: (A) S-ICAM-1; (B) S-VCAM-1); (C) S-E-Selectin; (D) S-IL-6; (E) S-IL-1β; (F) S-TNF-α; (G) S-CRP. Results are presented in Box-and-Whiskers plot. AHF, acute heart failure; CS, cardiogenic shock; S-CRP, serum C-reactive protein; S-E-Selectin, serum E-Selectin; S-ICAM-1, serum intercellular adhesion molecule 1; S-IL-1β, serum interleukin 1β; S-IL-6, serum interleukin 6; S-TNF-α, serum tumour necrosis factor alpha; S-VCAM-1, serum vascular cell adhesion molecule 1.
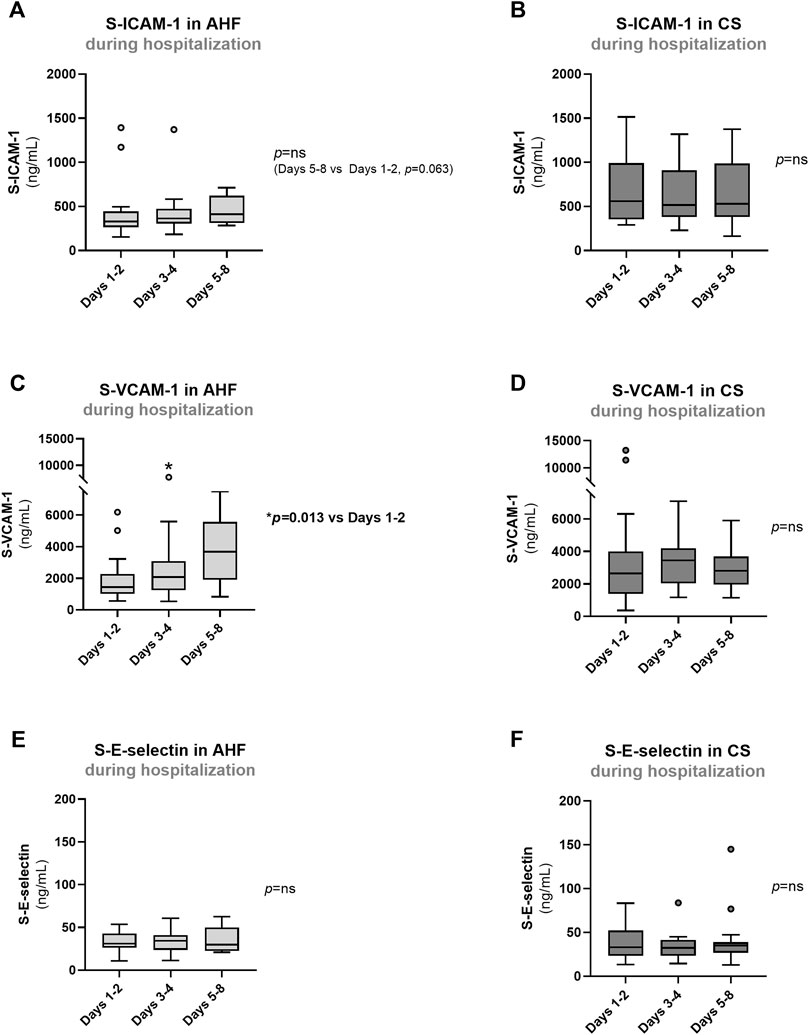
FIGURE 4. Evolution of biomarkers of endothelial dysfunction in AHF and CS patients during hospitalization: (A,B) S-ICAM-1; (C,D) S-VCAM-1); (E,F) S-E-Selectin. Results are presented in Box-and-Whiskers plot. AHF, acute heart failure; CS, cardiogenic shock; S-E-Selectin, serum E-Selectin; S-ICAM-1, serum intercellular adhesion molecule 1; S-VCAM-1, serum vascular cell adhesion molecule 1.
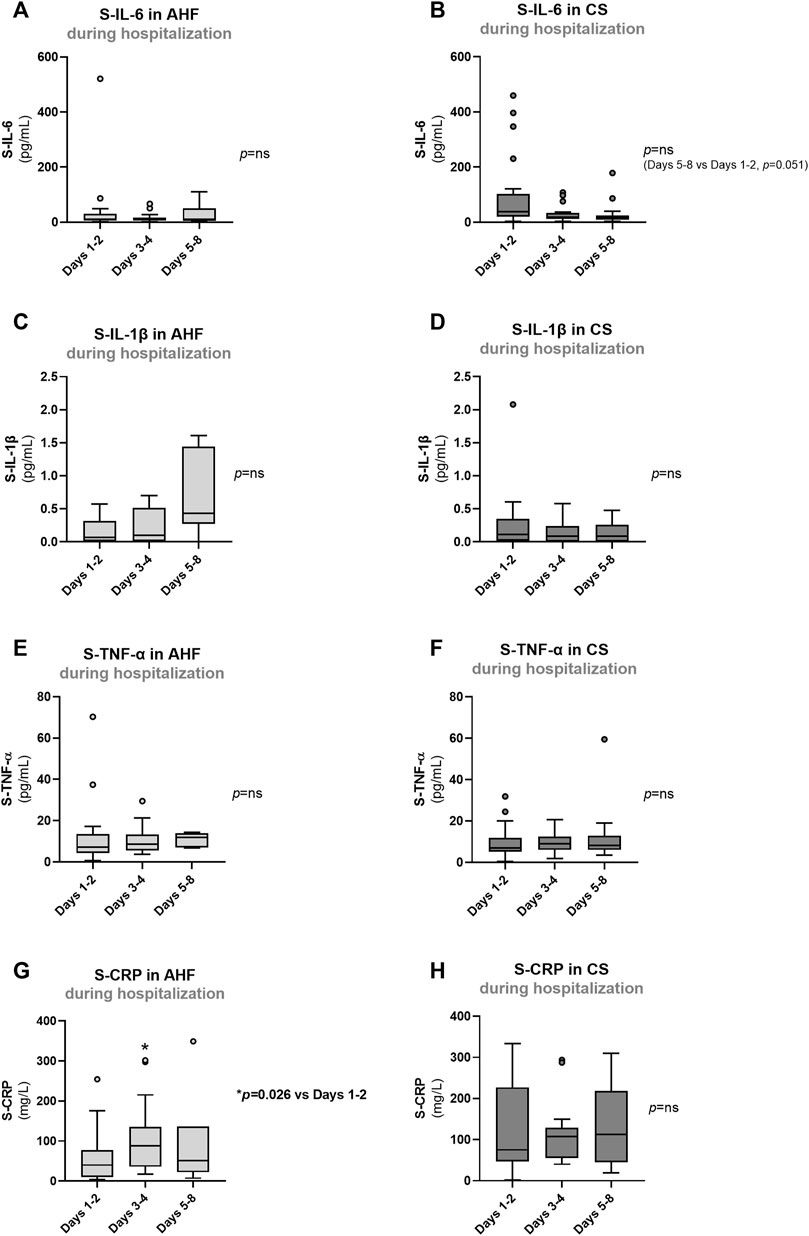
FIGURE 5. Evolution of biomarkers of inflammation in AHF and CS patients during hospitalization: (A,B) S-IL-6; (C,D) S-IL-1β; (E,F) S-TNF-α; (G,H) S-CRP. Results are presented in Box-and-Whiskers plot. AHF, acute heart failure; CS, cardiogenic shock; S-CRP, serum C-reactive protein; S-IL-1β, serum interleukin 1β; S-IL-6, serum interleukin 6; S-TNF-α, serum tumour necrosis factor alpha.
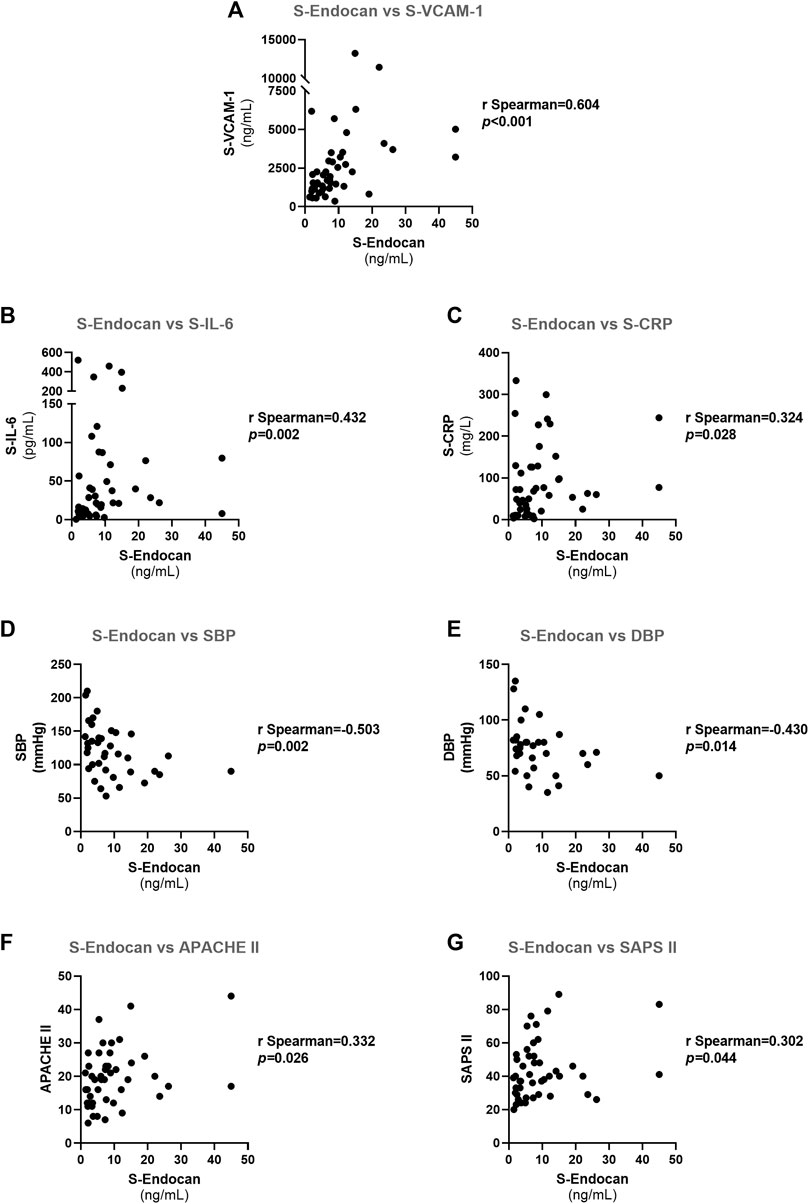
FIGURE 6. Spearman correlations for serum endocan in all patients at admission: (A) S-Endocan vs. S-VCAM-1; (B) S-Endocan vs. S-IL-6; (C) S-Endocan vs. S-CRP; (D) S-Endocan vs. S-SBP; (E) S-Endocan vs. DBP; (F) S-Endocan vs. APACHE II; (G) S-Endocan vs. SAPS II. APACHE II, acute physiology and chronic health evaluation II; DBP, diastolic blood pressure; SAPS II, simplified acute physiology score (SAPS) II; SBP, systolic blood pressure; S-Endocan, serum endocan; S-CRP, serum C-reactive protein; S-IL-6, serum interleukin 6; S-VCAM-1, serum vascular cell adhesion molecule 1.
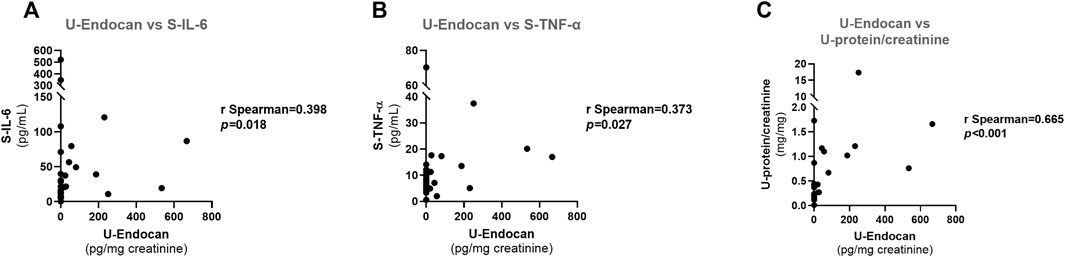
FIGURE 7. Spearman correlations for urinary endocan in all patients at admission: (A) U-Endocan vs. S-IL-6; (B) U-Endocan vs. S-TNF-α; (C) U-Endocan vs. U-protein/creatinine. S-IL-6, serum interleukin 6; S-TNF-α, serum tumour necrosis factor alpha; U-Endocan, urinary endocan; U-protein/creatinine, urinary protein/creatinine.
Repeated measures multivariate analyses were conducted to determine the relationship between S-Endocan (as dependent variable) and endothelial activation markers (S-VCAM-1), inflammation (S-IL-6), cardiac markers (P-BNP and P-hs-trop I), systolic and diastolic blood pressure (SBP and DBP, respectively) and prognostic scores, adjusted for some confounders, namely age and gender.
The ability of S-Endocan, U-Endocan, S-VCAM-1, P-BNP and APACHE II and SAPS II scores to discriminate in-hospital mortality was evaluated by plotting receiver operating characteristic (ROC) curves and computing the area under the curve (AUC).
To prevent possible bias in clinical evaluation, all the patients were examined by the same medical team included in the project. To assure comparability of biomarkers assessment, samples from controls, AHF and CS groups were evenly distributed in each assay plate. There were missing values in some biomarkers due to insufficient volume to perform sample processing, dilution tests and assays. In addition, some routine clinical biomarkers could only be assessed at a single time point during hospitalization due to hospital’s internal policies, and we had not permission to measure routine clinical biomarkers in controls (blood donor volunteers), except for creatinine, or to have access to their hospital laboratory reports. The final number per group for the biomarkers/parameters evaluated at admission was as following: APACHE II score, n = 23 vs. 23 (AHF vs. CS); P-BNP, n = 20 vs. 17 (AHF vs. CS); P-hs-trop I, n = 23 vs. 23 (AHF vs. CS); eGFR, n = 22 vs. 23 vs. 23 (Controls vs. AHF vs. CS); SAPS II score, n = 23 vs. 23 (AHF vs. CS); S-Urea, n = 23 vs. 23 (AHF vs. CS); U-protein/creatinine ratio, n = 22 vs. 15 (AHF vs. CS); S-ICAM-1, n = 22 vs. 23 vs. 24 (Controls vs. AHF vs. CS); S-VCAM-1, n = 22 vs. 23 vs. 24 (Controls vs. AHF vs. CS); S-E-Selectin, n = 22 vs. 23 vs. 24 (Controls vs. AHF vs. CS); S-TNF-α, n = 22 vs. 23 vs. 24 (Controls vs. AHF vs. CS); S-IL-1β, n = 22 vs. 23 vs. 24 (Controls vs. AHF vs. CS); S-IL-6, n = 22 vs. 23 vs. 24 (Controls vs. AHF vs. CS); S-CRP, n = 23 vs. 23 (AHF vs. CS). To avoid biasing the results, no imputation for missing values was used.
Preliminary values of S-Endocan (putative marker for endothelitis) obtained in controls and in patients with AHF or CS were used to estimate sample size by G Power 3.1 software. We found that a sample size of 6 participants/patients in each group would be sufficient to obtain a statistical study power of 80% at a 5% level of significance. The final sample size was defined according to the RIFF-HEART project’s primary objectives that consisted in characterizing not only endothelitis, but also resolution of inflammation markers at admission and during hospitalization.
Reporting of the study conforms to STROBE statement along with references to STROBE and the broader EQUATOR guidelines (Simera et al., 2010).
Results
Population demographic, clinical and biochemical characterization
General demographic characteristics, clinical and biochemical parameters are shown in Table 1.
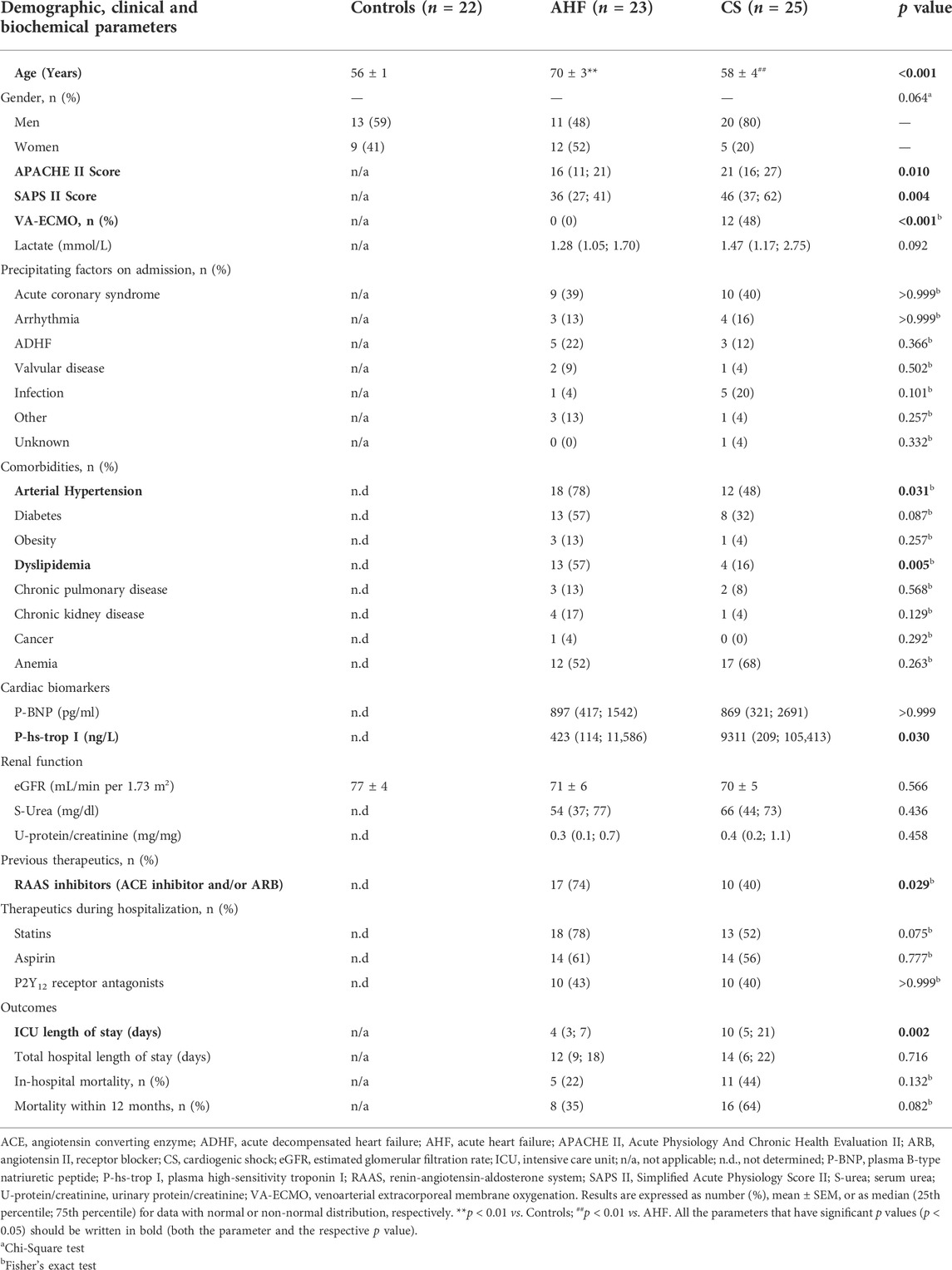
TABLE 1. Demographic, clinical and biochemical characteristics at admission and outcomes of study population.
In this study, 22 healthy controls and 48 patients, 23 with AHF and 25 with CS, were assessed. Male patients were more prevalent in the CS group (n = 20), compared to AHF (n = 11) and controls (n = 13), with this difference among groups being borderline significant (p = 0.064). Patients in the AHF group were significantly older than controls and CS patients (Controls: 56 ± 1 year; AHF: 70 ± 3 years; CS: 58 ± 4 years, p < 0.001). As expected, APACHE II and SAPS II scores were significantly higher in the CS group, in which 48% of the patients were supported with VA-ECMO.
Precipitating factors on admission were identical for AHF and CS groups, with acute coronary syndrome being the predominant trigger in both groups, followed by acutely decompensated HF in AHF and infection in CS patients, respectively. Arterial hypertension, diabetes, dyslipidemia and anemia were the most prevalent comorbidities in both groups, but the AHF group presented a significantly higher number of patients with arterial hypertension and dyslipidemia. The AHF group also included a significantly higher number of patients that were being treated with renin-angiotensin-aldosterone system (RAAS) inhibitors prior to admission when compared to the CS group. Regarding therapeutics throughout hospitalization, AHF and CS groups showed no significant differences in the number of patients on statin, aspirin or P2Y12 receptor antagonist therapies.
Patients with CS had significantly higher concentration of P-hs-trop I at admission, but no differences were found in P-BNP nor in lactate values when compared to AHF patients. We did not find significant differences in eGFR between all groups or in serum urea and proteinuria at admission between AHF and CS groups. CS patients had a longer length of stay in the ICU than patients with AHF, but there were no differences between these groups regarding the total length of hospital stay. There was a high in-hospital mortality and 1-year mortality in both groups (Table 1). Although no significant differences were observed in mortality parameters between AHF and CS patients, the CS group had a tendentially higher 1-year mortality (CS = 64% vs. AHF = 35%, p = 0.082) (Table 1). A Kaplan-Meier survival plot is shown in Supplementary Material, Supplementary Figure S1. The median survival time for the ICU patients evaluated was 13 months.
S-Endocan and U-Endocan at admission and during hospitalization
At admission, S-Endocan was significantly higher in AHF (p < 0.001 vs. controls) and even higher in CS (p < 0.001 vs. controls; p < 0.010 vs. AHF; p < 0.001 for linear trend) (Figures 1A,C), whereas U-Endocan was only significantly higher in CS patients (Figure 1B). During hospitalization, we found no significant reduction in S-Endocan (Figures 2A,B) or U-endocan values (Figures 2C,D) in both patient groups.
CS patients that were on RAAS inhibitors prior to admission had significantly lower concentrations of S-Endocan [8.1 (5.1; 12.2) vs. 12.4 (8.5; 22.9) ng/ml, p = 0.026, Supplementary Table S1] at admission, but no changes were detected in other time points or in U-Endocan or in AHF patients. Treatment with statin, aspirin or P2Y12 receptor antagonists throughout hospitalization did not affect S-Endocan or U-Endocan in AHF or CS patients (Supplementary Table S1).
Other biomarkers of endothelial activation and inflammation
Concerning other endothelial activation biomarkers, we found significantly higher admission values of S-ICAM-1 in CS patients compared to AHF patients and controls (p < 0.050). However, admission S-ICAM-1 concentration in AHF patients did not differ from control values (p > 0.050) (Figure 3A). Admission S-VCAM-1 was increased by 2-fold in AHF and almost by 4-fold in CS patients compared to controls (p < 0.001 for AHF and CS vs. controls), but no differences were found in admission S-E-Selectin values among the groups (Figures 3B,C, respectively). Both S-ICAM-1 and S-VCAM-1 concentrations linearly increased across the AHF spectrum (p for linear trend = 0.010 for S-ICAM and p for linear trend<0.001 for S-VCAM-1).
Patients with AHF or CS exhibited higher admission values of inflammatory markers such as S-IL-6 (p < 0.001) and S-TNF-α (overall p value = 0.031) compared to controls (Figures 3D,F). There were no significant differences in admission values of S-IL-1β among the groups (Figure 3E) or in admission S-CRP concentrations between AHF and CS groups (Figure 3G). During hospitalization, there was no significant reduction in any of the endothelial and inflammatory markers evaluated (Figures 4, 5). In fact, at days 3–4, we observed a significant increase of S-VCAM-1 and S-CRP in AHF patients (Figures 4C, 5G, respectively).
Treatment with RAAS inhibitors prior to admission was associated with tendentially lower concentrations of S-VCAM-1 [1717 (1108; 2332) vs. 3524 (2141; 5252) ng/ml, p = 0.058, Supplementary Table S1] in CS patients at admission, but no significant changes were detected in other time points or in other endothelial cell adhesion molecules or in AHF patients (Supplementary Table S1). Statin treatment throughout hospitalization did not affect endothelial cell adhesion molecules in CS patients, but in AHF patients was associated with significantly higher values of E-Selectin at admission and at days 3–4 (Supplementary Table S1). Regarding antiplatelet therapy throughout hospitalization, both aspirin and P2Y12 receptor antagonists were associated with opposite effects on endothelial cell adhesion molecules, being associated with a significant reduction of S-VCAM-1 at admission in CS patients and with an increase of S-ICAM-1 at admission and days 3–4 in AHF patients (Supplementary Table S1).
Comparisons in CS patients with or without VA-ECMO
At admission, there were no significant differences in demographic or in routine biochemical parameters between the VA-ECMO group (n = 12) and the conventional medical therapy (CMT) group (n = 13), except for the age, the VA-ECMO patients being younger (48 ± 4 years vs. 68 ± 4 years, p = 0.004, VA-ECMO vs. CMT). During hospitalization, no significant differences were observed between CMT and VA-ECMO groups in S-Endocan, U-Endocan or any of the other endothelial and inflammatory markers evaluated (data not shown), although S-CRP was tendentially higher in the VA-ECMO group at days 5–8 (VA-ECMO: 158.5 (85.6; 223.5 mg/L vs. CMT: 55.7 (24.3; 148.4) mg/L, p = 0.068).
Correlation analysis
Within all patients at admission, S-Endocan was inversely correlated with SBP (r = −0.503, p = 0.002) and DBP (r = −0.430, p = 0.014) (Figures 6D,E, respectively) and positively correlated with S-VCAM-1 (r = 0.604, p < 0.001), S-IL-6 (r = 0.432, p = 0.002) and S-CRP (r = 0.324, p = 0.028) (Figures 6A–C respectively), as well as with usually recognized prognosis surrogates of ICU patients, such as APACHE II (r = 0.332, p = 0.026) and SAPS II (r = 0.302, p = 0.044) scores (Figures 6F,G, respectively).
U-Endocan was positively correlated with S-IL-6 (r = 0.398, p = 0.018), S-TNF-α (r = 0.373, p = 0.027) and U-protein/creatinine (r = 0.665, p < 0.001) (Figures 7A–C, respectively).
Repeated measures multivariate analyses
The repeated measures multivariate analyses, considering all values during hospitalization and adjusted for age and gender, confirmed the positive relationship of S-Endocan with S-VCAM-1 previously detected in correlation analysis and evidenced a positive association with P-BNP, with higher values of these biomarkers being associated with higher S-Endocan values (Table 2). S-Endocan also had a borderline significant positive association with APACHE II score (Adjusted β = 0.377; 95% CI: −0.030–0.784, p = 0.069). The inverse relationships of S-Endocan with SBP or DBP were also confirmed in these multivariate analyses, with lower SBP and DBP values being associated with higher S-Endocan values (Table 2).
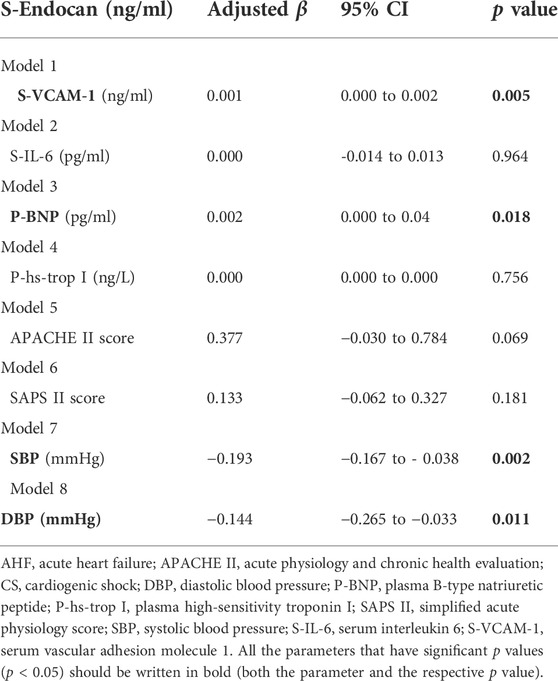
TABLE 2. Repeated measures multivariate models for S-Endocan in AHF and CS patients. (Adjusted β), 95% confidence intervals (95% CI) and p value estimated by repeated measures multivariate models with S-Endocan as the dependent variable and adjusted for age and gender.
S-Endocan stratification by LVEF and mortality
When patients were stratified according to 2021 guidelines classification based on echocardiographic LVEF (McDonagh et al., 2021), admission S-Endocan values significantly increased in line with the degree of LVEF impairment (p for linear trend = 0.008) (Figure 8A). This was not observed for S-VCAM-1 values at admission (p for linear trend = 0.202) (Figure 8B).
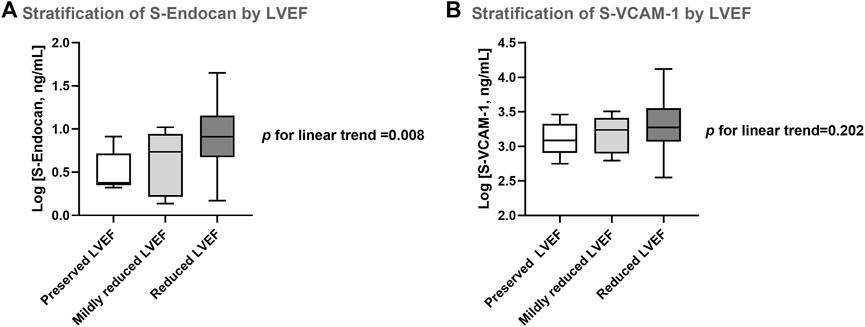
FIGURE 8. Serum endocan (A) and VCAM-1 (B) stratified by left ventricular ejection fraction (LVEF). Preserved LVEF: LVEF ≥50%; mildly reduced LVEF: LVEF 41–49%; reduced LVEF: LVEF ≤40%. Results are presented in Box-and-Whiskers plot. S-Endocan, serum endocan; S-VCAM-1, serum vascular cell adhesion molecule 1.
Regarding the stratification of endocan values according to the mortality within 12 months, although non-survivors presented higher median values of S-Endocan at admission when compared to survivors (S-Endocan - Non-survivors: 7.9 (5.2; 13.5) ng/ml vs. Survivors: 6.2 (2.4; 9.8) ng/ml), these differences did not reach statistical significance (p = 0.158). Moreover, among CS patients, non-survivors presented higher median values of U-Endocan compared to survivors (U-Endocan—CS Non-survivors:10.3 (0.0; 100.2) pg/mg creatinine vs. CS Survivors: 0.0 (0.0; 25.6) pg/mg creatinine), although this was not statistically significant (p = 0.497).
Performance of S-Endocan, U-Endocan, S-VCAM-1, P-BNP and prognostic scores as predictors of in-hospital mortality
APACHE II and SAPS II had similar and the highest AUC values for the prediction of in-hospital mortality, both being significant [AUCAPACHE II: 0.790 (95% CI: 0.643–0.938), p = 0.002; AUCSAPS II: 0.807 (95% CI: 0.664–0.951), p = 0.001)] (Supplementary Table S2). When comparing confidence intervals, S-Endocan seemed to perform, at least, as well as P-BNP and S-VCAM-1 and also did not appear to be significantly different from APACHE II and SAPS II scores (Supplementary Table S2).
Discussion
Our study highlights that inflammation-driven endothelitis might be a major pathophysiological mechanism across AHF spectrum, as evidenced by elevated concentrations of S-Endocan, S-VCAM-1, S-IL-6 and S-TNF-α both in AHF and CS group of patients. Of these parameters, S-Endocan seems the most promising biomarker since it not only raises with the hemodynamic severity of clinical presentation at admission but, most surprisingly, also increases with LVEF dysfunction. The positive correlation of S-Endocan with routine ICU prognostic scores and, particularly, its positive association with P-BNP in multivariate analyses suggest its relevance for inclusion in larger multimarker panels for AHF prognostication and eventually for future therapeutic targeting.
After many negative or neutral AHF trials, newer therapeutic targets are demanded once they are validated in pilot mechanistic studies where surrogate markers prove a solid and comprehensive inference for clinical benefit (Gheorghiade et al., 2005b). Endothelial dysfunction is prevalent and seems to be a predictor of adverse events in HF patients, also implicated in HF development and progression (Alem, 2019; Zuchi et al., 2020). Of note, therapies that have shown consistently to improve HF survival (e.g. angiotensin-converting enzyme inhibitors, spironolactone, beta blockers, etc) were demonstrated to simultaneously improve endothelial function (Marti et al., 2012). Therefore, a new interest in endothelial activation is re-emerging not only for risk stratification but also as a potential therapeutic target (De Keulenaer et al., 2017; Premer et al., 2019). The most validated theory considers that nitric oxide (NO) regulation of vascular tone contributes to the hemodynamic status in acute HF. Its imbalance with vasoconstrictors and reactive oxygen species determines increased vascular stiffness in pulmonary and systemic circulation and consequently ventricular workload and neurohormonal activation (Marti et al., 2012). Numerous clinical trials explored this therapeutically, either directly through drugs that modulate NO release, such as nebivolol (SENIORS trial) (Flather et al., 2005), or indirectly through drugs acting on cGMP-signalling axis, such as sildenafil (RELAX trial) (Redfield et al., 2013), riociguat (LEPHT study) (Bonderman et al., 2013) or vericiguat (SOCRATES trial) (Gheorghiade et al., 2015) and, ultimately, via the neprilysin inhibitor sacubitril that inhibits natriuretic peptide degradation causing amplification of the intracellular level of cGMP via natriuretic peptide receptor-A (McMurray et al., 2014). However, endothelial dysfunction extends beyond NO-mediated effects in the endothelium and its role in HF pathophysiology is more complex than previously anticipated. Endothelial dysfunction is now viewed as a common and important feature of all circulatory beds in HF, regardless of LVEF spectrum (Triposkiadis et al., 2019).
Although several non-invasive techniques have been developed for endothelial function testing, including flow-mediated vasodilation and finger plethysmography, these techniques are hardly implemented in the clinical daily practice. Due to these difficulties, some studies have quantified circulating endothelial biomarkers in HF patients, and, therefore, the measurement of many circulating endothelial biomarker candidates is becoming promising (Walczak et al., 2015). Circulating endothelial cells in the peripheral blood as well as E-selectin, von Willebrand factor and soluble thrombomodulin were shown to be significantly higher in patients with HF although they did not present significant differences between AHF and chronic HF and did not correlate with P-BNP (Chong et al., 2006a), ejection fraction or New York Heart Association (NYHA) class (Chong et al., 2006b). Also, VCAM-1 and ICAM-1 were shown to be associated with the development of new post-acute myocardial infarction HF symptoms (Lino et al., 2019) and increased subset-specific monocyte expression of their receptors were observed in AHF patients, with potential prognostic value of VCAM-1R (Wrigley et al., 2013) and sVCAM-1 after ST-elevation myocardial infarction (Hayek et al., 2021). But of all these, serum endocan has been one of the most qualified for the cardiovascular arena (Bessa et al., 2020).
In fact, in our work, most endothelial biomarkers, but not P-BNP, seem to differentiate AHF phenotype of presentation, since admission concentrations of S-ICAM-1, S-VCAM-1 and S-Endocan were significantly higher in CS patients. Among them, S-Endocan and S-VCAM-1 were also significantly increased in AHF patients, besides being linearly associated with the hemodynamic presentation of AHF. However, only S-Endocan increased in line with the degree of LVEF impairment evaluated by echocardiography. Thus, it may potentially be the first biomarker correlated with the severity of presentation of AHF phenotype and LVEF impairment, ultimately being anticipated as a better surrogate for prognostication in this entity if we consider hypoperfusion phenotype as the worst indicator for in-hospital mortality (Chioncel et al., 2019). This is corroborated by its positive association with P-BNP in repeated measures multivariate analysis adjusted for age and gender, as well as by its positive correlations with APACHE II and SAPS II. P-BNP (Metra et al., 2007) and LVEF (Solomon et al., 2007; O'Connor et al., 2008) are well established surrogates for prognosis in AHF and CS patients, although with some particularities and limitations (Chioncel et al., 2017a; Pang et al., 2019; Salah et al., 2019), whereas APACHE II and SAPS II are mostly validated for ICU patients in general. Accordingly, in our study, CS patients have longer ICU length of stay and tended to have a higher 1-year mortality, but there were no significant differences in in-hospital mortality between the AHF or CS groups. This might have resulted from a selection bias of AHF patients, which were only recruited from ICU, implicating selection of most severe patients, for example with need of non-invasive ventilation support. Moreover, the significantly older age of AHF patients and the higher prevalence of myocarditis (non-coronary etiologies) in CS group might also have contributed to these outcomes (Harjola et al., 2015). Noteworthy, we found that non-survivors had higher admission values of S-Endocan compared to survivors, although this did not reach statistical significance probably due to the aforementioned reasons and also to the exploratory nature of this small study, not designed to detect differences between survivors and non-survivors. We further assessed the performance of S-Endocan, U-Endocan, S-VCAM-1, P-BNP, APACHE II and SAPS II at admission to discriminate in-hospital mortality using ROC analysis. As already established, APACHE II and SAPS II are the best models for predicting mortality and this was confirmed again by their higher and significant AUC values. This was expected since they are a composite of clinical and analytical variables. However, when comparing confidence intervals, their performance did not appear to be significantly different from that of S-Endocan. This biomarker also seemed to perform, at least, as well as P-BNP and S-VCAM-1 in relation to in-hospital mortality, with the clinical advantage of being linearly associated with both hemodynamic presentation and ventricular dysfunction, which no analytical parameter demonstrated until now. These results are in line with previous studies, where for example, in ventilator-associated pneumonia, higher endocan concentrations were seen in non-survivors at day 1 and 7 (El Halim and Sayed, 2015) and also in patients with acute respiratory distress syndrome (ARDS) (Tang et al., 2014). In severe sepsis, a cut-off point was determined at days 1, 4, and 7, where higher endocan values were associated with poor prognosis (Hsiao et al., 2018) and with the need for mechanical ventilation (Mangat et al., 2017), thus representing a better biomarker than procalcitonin (Pauly et al., 2016; Zhao and Dong, 2017). Also remarkably, U-Endocan was even more evidently higher in CS non-survivors but again not statistically significant. Furthermore, its performance to discriminate in-hospital mortality did not appear to be significantly different from the other endothelial biomarkers tested.
Human endocan is synthetized by the vascular endothelium, namely by the pulmonary and kidney endothelial cells (Lassalle et al., 1996) but, unlike the other proteoglycans of the endothelial glycocalyx, it circulates freely in the bloodstream (Gaudet et al., 2017). The catabolism of endocan is not well known, resulting probably from proteolytic degradation and hepatic metabolism (De Freitas Caires et al., 2013; Nault et al., 2013). Urinary endocan is probably derived from kidney endothelial cells and in our work it was markedly higher in CS, suggesting locally increased renal endothelial dysfunction in these patients. Although it was positively correlated with proteinuria, which might indicate a relationship with glomerular lesion, we did not observe significant differences in renal function parameters between AHF and CS patients. Interestingly, urinary endocan was also positively correlated with inflammatory biomarkers such as IL-6 and TNF-α, reinforcing endocan association with inflammatory status. In contrast to our work, in populations with community acquired pneumonia, circulating endocan did not correlate with IL-6 or VCAM-1 at admission (Smart et al., 2018). This probably suggests that, in AHF, endocan is more timely linked to the inflammatory response and could potentially better reflect the complex multitude of pathophysiological pathways of AHF patients or even add incremental value to a multi-marker multi-point strategy of risk stratification (Lassus et al., 2013; Demissei et al., 2016).
We did not observe a reduction of endocan values or of other endothelial and inflammatory biomarkers during the first week of hospitalization in both patient groups. In other studies, namely on post-operative cardiac surgery patients, endocan was shown to peak very quickly at 6 h and slowly decline but it did not return to baseline at day 5 (Madhivathanan et al., 2016). Furthermore, higher endocan concentrations were observed in patients with the longest duration of norepinephrine support (Bougle et al., 2018) and could predict nosocomial pneumonia earlier and better than CRP (Perrotti et al., 2018). Endocan was also shown to increase during sepsis, worsening into multiple organ dysfunction syndrome (MODS), as well as to decrease when sepsis improves (Ioakeimidou et al., 2017). Severe sepsis with endocan concentrations remaining above 6.28 ng/ml at days 1, 4, and 7 was already demonstrated to be associated with poor prognosis (Hsiao et al., 2018). Of note, in our study, CS patients showed median S-Endocan values higher than 8 ng/ml throughout hospitalization. We hypothesize that in our patient groups, endocan kinetics could be more delayed than in the cases of sepsis already described, being specifically related to cardiovascular pathophysiology as evidenced by its linear association with ventricular dysfunction, but presenting similar prognostic implications.
Our results might indicate a perpetuation of endothelial dysfunction and inflammation in AHF and CS patients (Reina-Couto et al., 2021), reflecting the “non-resolving” course typical of this condition with high incidence of re-hospitalization and worse outcomes of AHF, as verified also in our population with median survival time of 13 months. This is in accordance with previous evidence in AHF patients showing that neurohormones and inflammatory biomarkers remain elevated 48h to 5 days after the acute event or even for longer periods (Milo et al., 2003; Gheorghiade et al., 2005a; Cotter et al., 2008). The persistence of these neurohormonal and inflammatory responses may be responsible for the high rehospitalization rates of this syndrome. So far, no therapeutic drug is well established as securely modifying prognosis in AHF (McDonagh et al., 2021) but current guidelines recommend decongestive therapy and eventually vasodilators for AHF patients who present with pulmonary edema or inotropes/vasopressors for CS patients (McDonagh et al., 2021). In fact, AHF or CS pharmacotherapy may be part of the problem. AHF pharmacological treatment may contribute to heightened neurohormonal activation (Goldsmith et al., 2018). Furthermore, the use of catecholamines as inotropes and/or vasopressors for the management of CS patients may further worsen cardiac and renal function (Amado et al., 2016; Tarvasmaki et al., 2016). Sympathetic activation is known to be associated with both inflammation and endothelial dysfunction and may underlie the unresolved inflammatory and endothelial responses in AHF and CS patients (Marvar and Harrison, 2012; Johansson et al., 2015; Ziegler et al., 2018). The therapeutic modulation of endocan has been explored in some studies as recently reviewed by our group (Bessa et al., 2020). However, as far as we know, no studies analysed the effects of mainstay pharmacotherapies for AHF (diuretics, vasodilators) or CS (inotropes, vasopressors) specifically on endocan. Regarding other drug treatments used in patients with cardiovascular disease, there is some evidence that RAAS inhibitors, statins and P2Y12 receptor antagonists can reduce endocan (Celik et al., 2015; Wei et al., 2017; Gao et al., 2018; Tuncez et al., 2019). However, in our study, only prior RAAS inhibitor treatment significantly decreased serum endocan and this was just observed for CS patients at admission. Treatment with statins or antiplatelet agents throughout hospitalization did not seem to affect serum or urinary endocan values in AHF or CS patients.
Endothelial dysfunction is poorly characterized in humans on mechanical circulatory support. In our study, we performed an extensive evaluation of endothelial and inflammatory biomarkers. Nevertheless, although the time frame selected in our study seemed adequate based on a previous study (Frerou et al., 2021), a more prolonged evaluation period might be required for VA-ECMO patients, ideally comparing pre- and post-cannulation. Indeed, during the first week of hospitalization, we could not observe any differences in the endothelial or inflammatory biomarkers in VA-ECMO patients compared to the conventional treatment group, with the exception of a tendential rise in S-CRP in the VA-ECMO group at days 5–8. These results are in contrast to a recent study describing that CS patients on VA-ECMO had higher values of plasma IL-6 and TNF-α within 24 h of VA-ECMO initiation compared to CS patients without VA-ECMO. Nevertheless, similarly, the authors could not find differences in these parameters between groups on day 4 after VA-ECMO initiation (Frerou et al., 2021). So far, from the scarce evidence found, there is still no consensus on the impact of ECMO on endothelial dysfunction and inflammation. Persistently high IL-6 concentrations in VA-ECMO patients were shown to be associated with poor prognosis (Risnes et al., 2008; Al-Fares et al., 2019), but in studies conducted in experimental models to investigate endothelial cell dysfunction associated with prolonged contact of blood components with synthetic surfaces, plasma from the ECMO experiments did not induce ICAM-1 expression in human umbilical vein endothelial cells during the 8 h of exposure (Graulich et al., 2000).
Major strengths of our study include an ICU population sample in “real-world conditions”, particularly CS and VA-ECMO patients, which are scarcely studied in the literature, as well as an extensive panel of endothelial and inflammatory biomarkers and the most commonly used clinical and echocardiographic prognostic indicators, including ICU APACHE II and SAPS II scores. Furthermore, our cohort appears to be representative of the mortality rate described in the literature for both AHF and CS (Chioncel et al., 2017b; Thiele et al., 2021). The small size of sample population and the unicentric character of this study are important limitations to point out that might limit the ability to generalize our results in terms of prognosis. Nevertheless, our results provide important clues of endocan usefulness as a prognostic marker in AHF and CS. We believe that endocan relation with mortality deserves to be explored in larger studies for its potential impact on disease management and prognosis. A further long-term prospective study should also be conducted after hospital discharge in patients presenting to ambulatory HF clinic since the results obtained throughout 1 week of hospitalization suggest that endothelitis might be a valuable therapeutic target in these patients.
In conclusion, admission concentrations of serum and urinary endocan significantly increase across AHF spectrum, but there is no reduction in the values of endocan or of other endothelial and inflammatory markers throughout hospitalization, suggesting a perpetuation of endothelial dysfunction and inflammation in these patients that could be related with the poor prognosis of this condition. Importantly, serum endocan appears to be a potential new biomarker of endothelitis and a putative therapeutic target in AHF and CS, being closely associated with LVEF impairment, BNP and prognostic scores.
Data Availability statement
The raw data supporting the conclusion of this article will be made available on request by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Comissão de Ética para a Saúde do Centro Hospitalar Universitário São João. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MR-C contributed to conceptualization, investigation, methodology, formal analysis and data interpretation, writing—original draft and writing—review and editing. CS-P and PP-T contributed to investigation, methodology, formal analysis and writing—review and editing. JQ-S and JB contributed to investigation, methodology and writing—review and editing; PS, JA, and SM contributed to investigation and methodology. CCD contributed to investigation, methodology, formal analysis and writing—review and editing. MM contributed to investigation, data interpretation and writing–review and editing. JTG contributed to investigation, methodology, resources, writing—review and editing. RRA contributed to investigation, methodology, resources and writing—review and editing. JAP contributed to conceptualization, investigation, methodology, resources, data interpretation, writing - review and editing and supervision. AA-T and TS were responsible for conceptualization, investigation, methodology, resources, funding acquisition, project administration, data interpretation, writing—review and editing and supervision. All authors read and approved the submitted version.
Funding
This work was supported by FEDER funds via COMPETE, Portugal 2020—Operational Programme for Competitiveness and Internationalization (POCI) (POCI-01-0145-FEDER-032188) and by national funds through the Portuguese Foundation for Science and Technology (FCT) (RIFF-HEART project: PTDC/MEC-CAR/32188/2017). CS-P is a recipient of a Ph.D. fellowship from FCT and MedInUP (UI/BD/150816/2020).
Acknowledgments
The authors wish to thank the blood donors, medical doctors and nurses from the Service of Immunohemotherapy, CHUSJ, and to the nurses from the Service of Intensive Care Medicine, CHUSJ, for their collaboration in our study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphys.2022.965611/full#supplementary-material
References
Al-Fares A., Pettenuzzo T., Del Sorbo L. (2019). Extracorporeal life support and systemic inflammation. Intensive Care Med. Exp. 7 (Suppl. 1), 46. doi:10.1186/s40635-019-0249-y
Alem M. M. (2019). Endothelial dysfunction in chronic heart failure: Assessment, findings, significance, and potential therapeutic targets. Int. J. Mol. Sci. 20 (13), 3198. doi:10.3390/ijms20133198
Amado J., Gago P., Santos W., Mimoso J., de Jesus I. (2016). Cardiogenic shock: Inotropes and vasopressors. Rev. Port. Cardiol. 35 (12), 681–695. doi:10.1016/j.repc.2016.08.004
Benjamin E. J., Muntner P., Alonso A., Bittencourt M. S., Callaway C. W., Carson A. P., et al. (2019). Heart disease and stroke statistics-2019 update: A report from the American Heart Association. Circulation 139 (10), e56–e528. doi:10.1161/CIR.0000000000000659
Bessa J., Albino-Teixeira A., Reina-Couto M., Sousa T. (2020). Endocan: A novel biomarker for risk stratification, prognosis and therapeutic monitoring in human cardiovascular and renal diseases. Clin. Chim. Acta. 509, 310–335. doi:10.1016/j.cca.2020.07.041
Bonderman D., Ghio S., Felix S. B., Ghofrani H. A., Michelakis E., Mitrovic V., et al. (2013). Riociguat for patients with pulmonary hypertension caused by systolic left ventricular dysfunction: A phase IIb double-blind, randomized, placebo-controlled, dose-ranging hemodynamic study. Circulation 128 (5), 502–511. doi:10.1161/CIRCULATIONAHA.113.001458
Bougle A., Allain P. A., Favard S., Ait Hamou N., Carillion A., Leprince P., et al. (2018). Postoperative serum levels of Endocan are associated with the duration of norepinephrine support after coronary artery bypass surgery. Anaesth. Crit. Care Pain Med. 37 (6), 565–570. doi:10.1016/j.accpm.2018.02.013
Braunwald E. (2015). The war against heart failure: The Lancet lecture. Lancet 385 (9970), 812–824. doi:10.1016/S0140-6736(14)61889-4
Celik T., Balta S., Karaman M., Ahmet Ay S., Demirkol S., Ozturk C., et al. (2015). Endocan, a novel marker of endothelial dysfunction in patients with essential hypertension: comparative effects of amlodipine and valsartan. Blood Press. 24 (1), 55–60. doi:10.3109/08037051.2014.972816
Chioncel O., Collins S. P., Greene S. J., Pang P. S., Ambrosy A. P., Antohi E. L., et al. (2017a). Predictors of post-discharge mortality among patients hospitalized for acute heart failure. Card. Fail. Rev. 3 (2), 122–129. doi:10.15420/cfr.2017:12:1
Chioncel O., Mebazaa A., Harjola V. P., Coats A. J., Piepoli M. F., Crespo-Leiro M. G., et al. (2017b). Clinical phenotypes and outcome of patients hospitalized for acute heart failure: The ESC heart failure long-term registry. Eur. J. Heart Fail. 19 (10), 1242–1254. doi:10.1002/ejhf.890
Chioncel O., Mebazaa A., Maggioni A. P., Harjola V. P., Rosano G., Laroche C., et al. (2019). Acute heart failure congestion and perfusion status - impact of the clinical classification on in-hospital and long-term outcomes; insights from the ESC-EORP-HFA Heart Failure Long-Term Registry. Eur. J. Heart Fail. 21 (11), 1338–1352. doi:10.1002/ejhf.1492
Chong A. Y., Freestone B., Patel J., Lim H. S., Hughes E., Blann A. D., et al. (2006a). Endothelial activation, dysfunction, and damage in congestive heart failure and the relation to brain natriuretic peptide and outcomes. Am. J. Cardiol. 97 (5), 671–675. doi:10.1016/j.amjcard.2005.09.113
Chong A. Y., Lip G. Y., Freestone B., Blann A. D. (2006b). Increased circulating endothelial cells in acute heart failure: Comparison with von Willebrand factor and soluble E-selectin. Eur. J. Heart Fail. 8 (2), 167–172. doi:10.1016/j.ejheart.2005.06.010
Colombo P. C., Doran A. C., Onat D., Wong K. Y., Ahmad M., Sabbah H. N., et al. (2015). Venous congestion, endothelial and neurohormonal activation in acute decompensated heart failure: cause or effect? Curr. Heart Fail. Rep. 12 (3), 215–222. doi:10.1007/s11897-015-0254-8
Colombo P. C., Onat D., Harxhi A., Demmer R. T., Hayashi Y., Jelic S., et al. (2014). Peripheral venous congestion causes inflammation, neurohormonal, and endothelial cell activation. Eur. Heart J. 35 (7), 448–454. doi:10.1093/eurheartj/eht456
Colombo P. C., Onat D., Sabbah H. N. (2008). Acute heart failure as "acute endothelitis"--Interaction of fluid overload and endothelial dysfunction. Eur. J. Heart Fail. 10 (2), 170–175. doi:10.1016/j.ejheart.2007.12.007
Cotter G., Felker G. M., Adams K. F., Milo-Cotter O., O'Connor C. M. (2008). The pathophysiology of acute heart failure--is it all about fluid accumulation? Am. Heart J. 155 (1), 9–18. doi:10.1016/j.ahj.2006.02.038
De Freitas Caires N., Gaudet A., Portier L., Tsicopoulos A., Mathieu D., Lassalle P., et al. (2018). Endocan, sepsis, pneumonia, and acute respiratory distress syndrome. Crit. Care 22 (1), 280. doi:10.1186/s13054-018-2222-7
De Freitas Caires N., Legendre B., Parmentier E., Scherpereel A., Tsicopoulos A., Mathieu D., et al. (2013). Identification of a 14 kDa endocan fragment generated by cathepsin G, a novel circulating biomarker in patients with sepsis. J. Pharm. Biomed. Anal. 78-79, 45–51. doi:10.1016/j.jpba.2013.01.035
De Keulenaer G. W., Segers V. F. M., Zannad F., Brutsaert D. L. (2017). The future of pleiotropic therapy in heart failure. Lessons from the benefits of exercise training on endothelial function. Eur. J. Heart Fail. 19 (5), 603–614. doi:10.1002/ejhf.735
Demissei B. G., Valente M. A., Cleland J. G., O'Connor C. M., Metra M., Ponikowski P., et al. (2016). Optimizing clinical use of biomarkers in high-risk acute heart failure patients. Eur. J. Heart Fail. 18 (3), 269–280. doi:10.1002/ejhf.443
El Halim A. A., Sayed M. (2015). Serum endocan role in diagnosis and prognosis of ventilator associated pneumonia. Egypt. J. Chest Dis. Tuberc. 64 (4), 865–869. doi:10.1016/j.ejcdt.2015.05.015
Flather M. D., Shibata M. C., Coats A. J., Van Veldhuisen D. J., Parkhomenko A., Borbola J., et al. (2005). Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital admission in elderly patients with heart failure (SENIORS). Eur. Heart J. 26 (3), 215–225. doi:10.1093/eurheartj/ehi115
Frerou A., Lesouhaitier M., Gregoire M., Uhel F., Gacouin A., Reizine F., et al. (2021). Venoarterial extracorporeal membrane oxygenation induces early immune alterations. Crit. Care 25 (1), 9. doi:10.1186/s13054-020-03444-x
Gao C. Z., Ma Q. Q., Wu J., Liu R., Wang F., Bai J., et al. (2018). Comparison of the effects of ticagrelor and clopidogrel on inflammatory factors, vascular endothelium functions and short-term prognosis in patients with acute ST-segment elevation myocardial infarction undergoing emergency percutaneous coronary intervention: A pilot study. Cell. Physiol. Biochem. 48 (1), 385–396. doi:10.1159/000491768
Gaudet A., Chenevier-Gobeaux C., Parmentier E., Delobel J. E., Dubucquoi S., Mathieu D., et al. (2017). Endocan is a stable circulating molecule in ICU patients. Clin. Biochem. 50 (15), 870–877. doi:10.1016/j.clinbiochem.2017.04.011
Gheorghiade M., Gattis Stough W., Adams K. F., Jaffe A. S., Hasselblad V., O'Connor C. M. (2005a). The pilot randomized study of nesiritide versus dobutamine in heart failure (PRESERVD-HF). Am. J. Cardiol. 96 (6A), 18G-25G. doi:10.1016/j.amjcard.2005.07.017
Gheorghiade M., Greene S. J., Butler J., Filippatos G., Lam C. S., Maggioni A. P., et al. (2015). Effect of vericiguat, a soluble guanylate cyclase stimulator, on natriuretic peptide levels in patients with worsening chronic heart failure and reduced ejection fraction: The SOCRATES-REDUCED randomized trial. JAMA 314 (21), 2251–2262. doi:10.1001/jama.2015.15734
Gheorghiade M., Zannad F., Sopko G., Klein L., Pina I. L., Konstam M. A., et al. (2005b). Acute heart failure syndromes: current state and framework for future research. Circulation 112 (25), 3958–3968. doi:10.1161/CIRCULATIONAHA.105.590091
Goldsmith S. R., Bart B. A., Pin A. I. (2018). Neurohormonal imbalance: A neglected problem-and potential therapeutic target-in acute heart failure. Curr. Probl. Cardiol. 43 (7), 294–304. doi:10.1016/j.cpcardiol.2017.12.002
Graulich J., Walzog B., Marcinkowski M., Bauer K., Kossel H., Fuhrmann G., et al. (2000). Leukocyte and endothelial activation in a laboratory model of extracorporeal membrane oxygenation (ECMO). Pediatr. Res. 48 (5), 679–684. doi:10.1203/00006450-200011000-00021
Groenewegen A., Rutten F. H., Mosterd A., Hoes A. W. (2020). Epidemiology of heart failure. Eur. J. Heart Fail. 22 (8), 1342–1356. doi:10.1002/ejhf.1858
Harjola V. P., Lassus J., Sionis A., Kober L., Tarvasmaki T., Spinar J., et al. (2015). Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur. J. Heart Fail. 17 (5), 501–509. doi:10.1002/ejhf.260
Harjola V. P., Mullens W., Banaszewski M., Bauersachs J., Brunner-La Rocca H. P., Chioncel O., et al. (2017). Organ dysfunction, injury and failure in acute heart failure: From pathophysiology to diagnosis and management. A review on behalf of the Acute Heart Failure Committee of the Heart Failure Association (HFA) of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 19 (7), 821–836. doi:10.1002/ejhf.872
Hayek A., Paccalet A., Mechtouff L., Da Silva C. C., Ivanes F., Falque H., et al. (2021). Kinetics and prognostic value of soluble VCAM-1 in ST-segment elevation myocardial infarction patients. Immun. Inflamm. Dis. 9 (2), 493–501. doi:10.1002/iid3.409
Hsiao S. Y., Kung C. T., Tsai N. W., Su C. M., Huang C. C., Lai Y. R., et al. (2018). Concentration and value of endocan on outcome in adult patients after severe sepsis. Clin. Chim. Acta. 483, 275–280. doi:10.1016/j.cca.2018.05.007
Ioakeimidou A., Pagalou E., Kontogiorgi M., Antoniadou E., Kaziani K., Psaroulis K., et al. (2017). Increase of circulating endocan over sepsis follow-up is associated with progression into organ dysfunction. Eur. J. Clin. Microbiol. Infect. Dis. 36 (10), 1749–1756. doi:10.1007/s10096-017-2988-6
Johansson P. I., Bro-Jeppesen J., Kjaergaard J., Wanscher M., Hassager C., Ostrowski S. R., et al. (2015). Sympathoadrenal activation and endothelial damage are inter correlated and predict increased mortality in patients resuscitated after out-of-hospital cardiac arrest. a post Hoc sub-study of patients from the TTM-trial. PLoS One 10 (3), e0120914. doi:10.1371/journal.pone.0120914
Kosir G., Jug B., Novakovic M., Mijovski M. B., Ksela J. (2019). Endocan is an independent predictor of heart failure-related mortality and hospitalizations in patients with chronic stable heart failure. Dis. Markers 2019, 9134096. doi:10.1155/2019/9134096
Lassalle P., Molet S., Janin A., Heyden J. V., Tavernier J., Fiers W., et al. (1996). ESM-1 is a novel human endothelial cell-specific molecule expressed in lung and regulated by cytokines. J. Biol. Chem. 271 (34), 20458–20464. doi:10.1074/jbc.271.34.20458
Lassus J., Gayat E., Mueller C., Peacock W. F., Spinar J., Harjola V. P., et al. (2013). Incremental value of biomarkers to clinical variables for mortality prediction in acutely decompensated heart failure: The multinational observational cohort on acute heart failure (MOCA) study. Int. J. Cardiol. 168 (3), 2186–2194. doi:10.1016/j.ijcard.2013.01.228
Levey A. S., Stevens L. A., Schmid C. H., Zhang Y. L., Castro A. F., Feldman H. I., et al. (2009). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 150 (9), 604–612. doi:10.7326/0003-4819-150-9-200905050-00006
Lino D. O. C., Freitas I. A., Meneses G. C., Martins A. M. C., Daher E. F., Rocha J. H. C., et al. (2019). Interleukin-6 and adhesion molecules VCAM-1 and ICAM-1 as biomarkers of post-acute myocardial infarction heart failure. Braz J. Med. Biol. Res. 52 (12), e8658. doi:10.1590/1414-431X20198658
Madhivathanan P. R., Fletcher N., Gaze D., Thomson R., Chandrasekaran V., Al-Subaie N., et al. (2016). Perioperative kinetics of endocan in patients undergoing cardiac surgery with and without cardiopulmonary bypass. Cytokine 83, 8–12. doi:10.1016/j.cyto.2016.03.006
Mangat M., Amalakuhan B., Habib S., Reyes L. F., Hinojosa C. A., Rodriguez A. H., et al. (2017). High endocan levels are associated with the need for mechanical ventilation among patients with severe sepsis. Eur. Respir. J. 50 (1), 1700013. doi:10.1183/13993003.00013-2017
Marti C. N., Gheorghiade M., Kalogeropoulos A. P., Georgiopoulou V. V., Quyyumi A. A., Butler J., et al. (2012). Endothelial dysfunction, arterial stiffness, and heart failure. J. Am. Coll. Cardiol. 60 (16), 1455–1469. doi:10.1016/j.jacc.2011.11.082
Marvar P. J., Harrison D. G. (2012). “Inflammation, immunity and the autonomic nervous system,” in Primer on the autonomic nervous system. Editors D. Robertson, I. Bioagionni, G. Burnstock, P. A. Low, and J. F. R. Paton. Third Edition (Cambridge, Massachusetts: Academic Press), 325–329.
McDonagh T. A., Metra M., Adamo M., Gardner R. S., Baumbach A., Bohm M., et al. (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 42 (36), 3599–3726. doi:10.1093/eurheartj/ehab368
McMurray J. J., Packer M., Desai A. S., Gong J., Lefkowitz M. P., Rizkala A. R., et al. (2014). Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 371 (11), 993–1004. doi:10.1056/NEJMoa1409077
Mentz R. J., O'Connor C. M. (2016). Pathophysiology and clinical evaluation of acute heart failure. Nat. Rev. Cardiol. 13 (1), 28–35. doi:10.1038/nrcardio.2015.134
Metra M., Nodari S., Parrinello G., Specchia C., Brentana L., Rocca P., et al. (2007). The role of plasma biomarkers in acute heart failure. Serial changes and independent prognostic value of NT-proBNP and cardiac troponin-T. Eur. J. Heart Fail. 9 (8), 776–786. doi:10.1016/j.ejheart.2007.05.007
Metra M., Teerlink J. R. (2017). Heart failure. Lancet 390 (10106), 1981–1995. doi:10.1016/S0140-6736(17)31071-1
Milo O., Cotter G., Kaluski E., Brill A., Blatt A., Krakover R., et al. (2003). Comparison of inflammatory and neurohormonal activation in cardiogenic pulmonary edema secondary to ischemic versus nonischemic causes. Am. J. Cardiol. 92 (2), 222–226. doi:10.1016/s0002-9149(03)00545-9
Nault J. C., Guyot E., Laguillier C., Chevret S., Ganne-Carrie N., N'Kontchou G., et al. (2013). Serum proteoglycans as prognostic biomarkers of hepatocellular carcinoma in patients with alcoholic cirrhosis. Cancer Epidemiol. Biomarkers Prev. 22 (8), 1343–1352. doi:10.1158/1055-9965.EPI-13-0179
O'Connor C. M., Abraham W. T., Albert N. M., Clare R., Gattis Stough W., Gheorghiade M., et al. (2008). Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the organized program to initiate lifesaving treatment in hospitalized patients with heart failure (OPTIMIZE-HF). Am. Heart J. 156 (4), 662–673. doi:10.1016/j.ahj.2008.04.030
Pang P. S., Fermann G. J., Hunter B. R., Levy P. D., Lane K. A., Li X., et al. (2019). TACIT (High Sensitivity Troponin T Rules Out Acute Cardiac Insufficiency Trial). Circ. Heart Fail. 12 (7), e005931. doi:10.1161/CIRCHEARTFAILURE.119.005931
Pauly D., Hamed S., Behnes M., Lepiorz D., Lang S., Akin I., et al. (2016). Endothelial cell-specific molecule-1/endocan: Diagnostic and prognostic value in patients suffering from severe sepsis and septic shock. J. Crit. Care 31 (1), 68–75. doi:10.1016/j.jcrc.2015.09.019
Perrotti A., Chenevier-Gobeaux C., Ecarnot F., Bardonnet K., Barrucand B., Flicoteaux G., et al. (2018). Is endocan a diagnostic marker for pneumonia after cardiac surgery? The ENDOLUNG study. Ann. Thorac. Surg. 105 (2), 535–541. doi:10.1016/j.athoracsur.2017.07.031
Premer C., Kanelidis A. J., Hare J. M., Schulman I. H. (2019). Rethinking endothelial dysfunction as a crucial target in fighting heart failure. Mayo Clin. Proc. Innov. Qual. Outcomes 3 (1), 1–13. doi:10.1016/j.mayocpiqo.2018.12.006
Redfield M. M., Chen H. H., Borlaug B. A., Semigran M. J., Lee K. L., Lewis G., et al. (2013). Effect of phosphodiesterase-5 inhibition on exercise capacity and clinical status in heart failure with preserved ejection fraction: A randomized clinical trial. JAMA 309 (12), 1268–1277. doi:10.1001/jama.2013.2024
Reina-Couto M., Pereira-Terra P., Quelhas-Santos J., Silva-Pereira C., Albino-Teixeira A., Sousa T. (2021). Inflammation in human heart failure: Major mediators and therapeutic targets. Front. Physiol. 12, 746494. doi:10.3389/fphys.2021.746494
Risnes I., Wagner K., Ueland T., Mollnes T., Aukrust P., Svennevig J., et al. (2008). Interleukin-6 may predict survival in extracorporeal membrane oxygenation treatment. Perfusion 23 (3), 173–178. doi:10.1177/0267659108097882
Sabbah H. N. (2017). Pathophysiology of acute heart failure syndrome: A knowledge gap. Heart Fail. Rev. 22 (6), 621–639. doi:10.1007/s10741-017-9651-2
Salah K., Stienen S., Pinto Y. M., Eurlings L. W., Metra M., Bayes-Genis A., et al. (2019). Prognosis and NT-proBNP in heart failure patients with preserved versus reduced ejection fraction. Heart 105 (15), 1182–1189. doi:10.1136/heartjnl-2018-314173
Shantsila E., Wrigley B. J., Blann A. D., Gill P. S., Lip G. Y. (2012). A contemporary view on endothelial function in heart failure. Eur. J. Heart Fail. 14 (8), 873–881. doi:10.1093/eurjhf/hfs066
Simera I., Moher D., Hoey J., Schulz K. F., Altman D. G. (2010). A catalogue of reporting guidelines for health research. Eur. J. Clin. Invest. 40 (1), 35–53. doi:10.1111/j.1365-2362.2009.02234.x
Smart L., Bosio E., Macdonald S. P. J., Dull R., Fatovich D. M., Neil C., et al. (2018). Glycocalyx biomarker syndecan-1 is a stronger predictor of respiratory failure in patients with sepsis due to pneumonia, compared to endocan. J. Crit. Care 47, 93–98. doi:10.1016/j.jcrc.2018.06.015
Solomon S. D., Dobson J., Pocock S., Skali H., McMurray J. J., Granger C. B., et al. (2007). Influence of nonfatal hospitalization for heart failure on subsequent mortality in patients with chronic heart failure. Circulation 116 (13), 1482–1487. doi:10.1161/CIRCULATIONAHA.107.696906
Tang L., Zhao Y., Wang D., Deng W., Li C., Li Q., et al. (2014). Endocan levels in peripheral blood predict outcomes of acute respiratory distress syndrome. Mediat. Inflamm. 2014, 625180. doi:10.1155/2014/625180
Tarvasmaki T., Lassus J., Varpula M., Sionis A., Sund R., Kober L., et al. (2016). Current real-life use of vasopressors and inotropes in cardiogenic shock - adrenaline use is associated with excess organ injury and mortality. Crit. Care 20 (1), 208. doi:10.1186/s13054-016-1387-1
Thiele H., de Waha-Thiele S., Freund A., Zeymer U., Desch S., Fitzgerald S., et al. (2021). Management of cardiogenic shock. EuroIntervention. 17 (6), 451–465. doi:10.4244/EIJ-D-20-01296
Thiele H., Ohman E. M., de Waha-Thiele S., Zeymer U., Desch S. (2019). Management of cardiogenic shock complicating myocardial infarction: an update 2019. Eur. Heart J. 40 (32), 2671–2683. doi:10.1093/eurheartj/ehz363
Tomasoni D., Adamo M., Lombardi C. M., Metra M. (2019). Highlights in heart failure. Esc. Heart Fail. 6 (6), 1105–1127. doi:10.1002/ehf2.12555
Triposkiadis F., Butler J., Abboud F. M., Armstrong P. W., Adamopoulos S., Atherton J. J., et al. (2019). The continuous heart failure spectrum: moving beyond an ejection fraction classification. Eur. Heart J. 40 (26), 2155–2163. doi:10.1093/eurheartj/ehz158
Tuncez A., Altunkeser B. B., Ozturk B., Ates M. S., Tezcan H., Aydogan C., et al. (2019). Comparative effects of atorvastatin 80 mg and rosuvastatin 40 mg on the levels of serum endocan, chemerin, and galectin-3 in patients with acute myocardial infarction. Anatol. J. Cardiol. 22 (5), 240–249. doi:10.14744/AnatolJCardiol.2019.64249
Velazquez E. J., Morrow D. A., DeVore A. D., Duffy C. I., Ambrosy A. P., McCague K., et al. (2019). Angiotensin-neprilysin inhibition in acute decompensated heart failure. N. Engl. J. Med. 380 (6), 539–548. doi:10.1056/NEJMoa1812851
Wachter R., Senni M., Belohlavek J., Straburzynska-Migaj E., Witte K. K., Kobalava Z., et al. (2019). Initiation of sacubitril/valsartan in haemodynamically stabilised heart failure patients in hospital or early after discharge: Primary results of the randomised TRANSITION study. Eur. J. Heart Fail. 21 (8), 998–1007. doi:10.1002/ejhf.1498
Walczak M., Suraj J., Kus K., Kij A., Zakrzewska A., Chlopicki S., et al. (2015). Towards a comprehensive endothelial biomarkers profiling and endothelium-guided pharmacotherapy. Pharmacol. Rep. 67 (4), 771–777. doi:10.1016/j.pharep.2015.06.008
Wei P., Han B., Zhang W. J., Bai J., Jiang C. Y., Qiu C. R., et al. (2017). Effect of ticagrelor on the serum level of hs-CRP, ESM-1 and short-term prognosis of patients with acute STEMI. Exp. Ther. Med. 13 (2), 604–608. doi:10.3892/etm.2016.3987
Wrigley B. J., Shantsila E., Tapp L. D., Lip G. Y. (2013). Increased expression of cell adhesion molecule receptors on monocyte subsets in ischaemic heart failure. Thromb. Haemost. 110 (1), 92–100. doi:10.1160/TH13-02-0088
Zhang H., Shen Y. W., Zhang L. J., Chen J. J., Bian H. T., Gu W. J., et al. (2021). Targeting endothelial cell-specific molecule 1 protein in cancer: A promising therapeutic approach. Front. Oncol. 11, 687120. doi:10.3389/fonc.2021.687120
Zhao R., Dong S. (2017). Clinical value of serum endocan and procalcitonin in early diagnosis and prognosis evaluation of sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 29 (4), 321–326. doi:10.3760/cma.j.issn.2095-4352.2017.04.007
Ziaee M., Mashayekhi S., Ghaffari S., Mahmoudi J., Sarbakhsh P., Garjani A., et al. (2019). Predictive value of endocan based on TIMI risk score on major adverse cardiovascular events after acute coronary syndrome. Angiology 70 (10), 952–959. doi:10.1177/0003319718815241
Ziegler K. A., Ahles A., Wille T., Kerler J., Ramanujam D., Engelhardt S., et al. (2018). Local sympathetic denervation attenuates myocardial inflammation and improves cardiac function after myocardial infarction in mice. Cardiovasc. Res. 114 (2), 291–299. doi:10.1093/cvr/cvx227
Zuchi C., Tritto I., Carluccio E., Mattei C., Cattadori G., Ambrosio G., et al. (2020). Role of endothelial dysfunction in heart failure. Heart fail. Rev. 25 (1), 21–30. doi:10.1007/s10741-019-09881-3
Glossary
5-PL five parameter logistic
AHF acute heart failure
APACHE II Acute Physiology And Chronic Health Evaluation II
ARDS acute respiratory distress syndrome
AUC area under curve;
CHUSJ Centro Hospitalar Universitário São João
CKD-EPI Chronic Kidney Disease Epidemiology Collaboration
CMT conventional medical therapy
CS cardiogenic shock
DBP diastolic blood pressure
ECMO extracorporeal membrane oxygenation
eGFR estimated glomerular filtration rate
ELISA enzyme-linked immunosorbent assay
ESM-1 endothelial cell-specific molecule-1
HF heart failure
ICU Intensive Care Unit
LV left ventricular
LVEF left ventricular ejection fraction
NO nitric oxide
P-BNP plasma B-type natriuretic peptide
P-hs-trop I plasma high-sensitivity troponin I
RAAS renin-angiotensin-aldosterone system
ROC receiver operating characteristic
SAPS II Simplified Acute Physiology Score II
SBP systolic blood pressure
S-CRP serum C-reactive protein
SEM standard error of the mean
S-Endocan serum endocan
S-E-Selectin serum E-Selectin
S-ICAM-1 serum intercellular adhesion molecule one
S-IL-1β serum interleukin one beta
S-IL-6 serum interleukin six
S-TNF-α serum tumour necrosis factor alpha
S-Urea serum urea
S-VCAM-1 serum vascular cell adhesion molecule one
sVCAM-1 soluble vascular cell adhesion molecule-1
U-Endocan urinary endocan
VA-ECMO veno-arterial extracorporeal membrane oxygenation
VCAM-1R integrin-receptor to vascular cell adhesion molecule 1
Keywords: endocan, endothelitis, acute heart failure, cardiogenic shock, biomarker
Citation: Reina-Couto M, Silva-Pereira C, Pereira-Terra P, Quelhas-Santos J, Bessa J, Serrão P, Afonso J, Martins S, Dias CC, Morato M, Guimarães JT, Roncon-Albuquerque R, Paiva J-A, Albino-Teixeira A and Sousa T (2022) Endothelitis profile in acute heart failure and cardiogenic shock patients: Endocan as a potential novel biomarker and putative therapeutic target. Front. Physiol. 13:965611. doi: 10.3389/fphys.2022.965611
Received: 09 June 2022; Accepted: 05 July 2022;
Published: 11 August 2022.
Edited by:
Luciana Venturini Rossoni, University of São Paulo, BrazilReviewed by:
Jose Geraldo Mill, Federal University of Espirito Santo, BrazilVicente Lahera, Complutense University of Madrid, Spain
Copyright © 2022 Reina-Couto, Silva-Pereira, Pereira-Terra, Quelhas-Santos, Bessa, Serrão, Afonso, Martins, Dias, Morato, Guimarães, Roncon-Albuquerque, Paiva, Albino-Teixeira and Sousa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teresa Sousa, dHNvdXNhQG1lZC51cC5wdA==
†These authors have contributed equally to this work and share last authorship