 Benazir Burkhardt1
Benazir Burkhardt1 Oliver Chaudry1Stephanie Kast1,2Simon von Stengel1
Oliver Chaudry1Stephanie Kast1,2Simon von Stengel1 Matthias Kohl3
Matthias Kohl3 Frank W. Roemer1
Frank W. Roemer1 Klaus Engelke4Michael Uder1
Klaus Engelke4Michael Uder1 Wolfgang Kemmler1,2*†
Wolfgang Kemmler1,2*†- 1Institute of Radiology, University Hospital Erlangen, Erlangen, Germany
- 2Institute of Medical Physics, Friedrich-Alexander University Erlangen-Nürnberg, Erlangen, Germany
- 3Department of Medical and Life Sciences, University of Furtwangen, Schwenningen, Germany
- 4Department of Medicine III, University Hospital Erlangen, Erlangen, Germany
Introduction: Physical exercise favorably affects visceral adipose tissue (VAT), which is a risk factor for cardiometabolic diseases. However, many people are unable or unwilling to conduct frequent and intensive exercise programs that have favorable effects on VAT. The present study aimed to determine the effect of time-efficient and joint-friendly whole-body electromyostimulation (WB-EMS) technology on VAT volume in overweight-to-obese adults with osteoarthritis of the knee.
Methods: In total, 46 women and 26 men (58.4 ± 7.0 years; BMI: 30.2 ± 4.2 kg/m2) with femuro-tibial knee osteoarthritis were randomly allocated to WB-EMS (n = 36) with 1.5 × 20 min/week for 29 weeks or a usual care control group (CG: n = 36) with six sessions of physiotherapy. Magnetic resonance imaging (MRI) using a non-contrast enhanced two-point Dixon gradient echo volumetric interpolated breath-hold examination determined the VAT from mid L2 to mid L3.
Results: In summary, VAT volume increased non-significantly in the CG (p = 0.246) and decreased non-significantly in the WB-EMS group (p = 0.143). We failed to determine significant WB-EMS-induced effects, i.e., group differences for absolute changes in the VAT volume (p = 0.090). However, we observed gender differences with significantly higher effects in men than in women (p = 0.032).
Discussion: We conclude that low volume, non-superimposed WB-EMS is not a perfect tool for decreasing VAT, particularly in overweight-to-obese women.
1 Introduction
Visceral adipose tissue (VAT) is a complex and metabolically active tissue that produces different adipokines and hormones (Silveira et al., 2021). Accumulation of VAT is a strong predictor of all-cause, cardiovascular- and cancer-specific mortality (Brown et al., 2016). In addition, many studies have provided evidence that VAT is closely related to an increased risk of insulin resistance (Kim and Kim, 2023; Zhang et al., 2015), atherosclerosis (ohman et al., 2009), dyslipidemia (von Kruchten et al., 2022), hypertension (Hall et al., 2015), hepatic steatosis (Park et al., 2008), coronary heart disease (Chen et al., 2022; Silveira et al., 2021), and different types of cancer (Silveira et al., 2021). There is striking evidence that participating in exercise interventions had favorable effects on accumulated VAT (Chen et al., 2023; Lee and Lee, 2021). In summary, combined aerobic and resistance exercise seems to be particularly effective in reducing abdominal obesity in overweight/obese individuals (Batrakoulis et al., 2022). However, considering the time required for these protocols (≈2–3 × 30–45 min), many people, with or without overweight and obesity, might be unmotivated or unable to join frequent, time-consuming exercise programs. Similar to the popular high-intensity interval training (HIIT) (A'Naja et al., 2024), whole-body electromyostimulation (WB-EMS) has been recognized as a very time-efficient training technology (Kemmler et al., 2020) to address cardiometabolic conditions (Batrakoulis et al., 2021; Guretzki et al., 2024). However, in contrast to HIIT, WB-EMS is much more joint-friendly, which may particularly attract people with joint disorders. Unfortunately, there is limited evidence of the positive effects of WB-EMS on VAT. A recent study provided significant positive evidence for the WB-EMS effects on intraabdominal fat (Park et al., 2021) in obese elderly women; however, the authors applied a rather unusual (Beier et al., 2024), high-volume approach with aerobic dance superimposed by WB-EMS. As this approach differs greatly from the low-volume, non-superimposed concepts primarily applied in research (Beier et al., 2024) and commercial WB-EMS settings (Kemmler et al., 2024), the aim of the present study was to determine the effect of a time-effective, joint-friendly WB-EMS program on VAT in overweight or obese people. Since there is strong evidence that the VAT response to RT exercise is more pronounced in men (Chen et al., 2023), we also considered gender differences in our analyses of VAT changes, and we hypothesized that the low-volume, non-superimposed WB-EMS program significantly decreases VAT compared to the control group.
2 Material and methods
2.1 Study design
The randomized controlled WB-EMS trial (RCT) is part of the “electromyostimulation for the treatment of knee osteoarthritis (OA) (EMSOAT) study.” This study applied a balanced parallel group design (WB-EMS versus control group) and evaluated the effects of 7 months of WB-EMS application on outcomes related to knee osteoarthritis in middle-aged and older adults who were overweight and obese. The present study focused on WB-EMS effects on visceral adipose tissue volume. Briefly, the EMSOAT was planned, initiated, and conducted by the Institute of Radiology, University Hospital Nürnberg, Germany. The University Ethics Committee of the FAU approved this trial (No. 352_20 B), which fully complies with the Helsinki Declaration “Ethical Principles for Medical Research Involving Human Subjects”(World_Medical_Association, 2013). After receiving detailed information, all the study participants provided their written informed consent. This project was fully registered under ClinicalTrials.gov (NCT05672264).
2.1.1 Participants
Briefly, between March 2022 and June 2022, local newspapers, social media, and selected physicians disseminated our study calls, which included the core eligibility criteria. A total of 440 women and men responded via email or telephone and were provided with more detailed written study information. Potential participants who confirmed their preliminary eligibility were further checked through detailed standardized phone calls conducted by carefully briefed research assistants. Inclusion criteria were (a) age 40–70 years old; (b) overweight or obese (BMI>25 kg/m2); (c) fulfilling clinical ACR criteria for knee OA (Altman et al., 1991); and(d) osteoarthritic knee pain on at least 50% of the days during the last 3 months with an average pain intensity of >2.5 on a 0–10 numerical rating scale (Bennell et al., 2020). Exclusion criteria were (a) any WB-EMS application or regular resistance exercise (≥60 min per week) during the last 12 months; (b) glucocorticoid or opioid pain therapy; (c) trauma of the knee joint within the last 12 weeks; (d) intra-articular injections in the knee joint in the last 12 weeks; (e) conditions, diseases, and corresponding therapy with a relevant impact on our study outcomes (e.g., rheumatoid arthritis and fibromyalgia); (f) contraindications for WB-EMS (Kemmler et al., 2019) or MRI application; and (g) ≥4 weeks of absence during the 29-week conditioning and intervention phase. Lastly, the study physician verified the final eligibility. Twelve of the 84 eligible participants refused to participate predominately due to the random allocation to the study groups (WB-EMS or control). Thus, finally 72 participants were eligible and willing to participate in the present study. However, mainly due to time constraints, four participants (all CG) were unable to join the MRI assessments (i.e., baseline and 29-week control); thus, 68 participants (43 women and 25 men) with MRI data were included in the present analysis of the WB-EMS effects on visceral adipose tissue changes (Figure 1; Table 1).
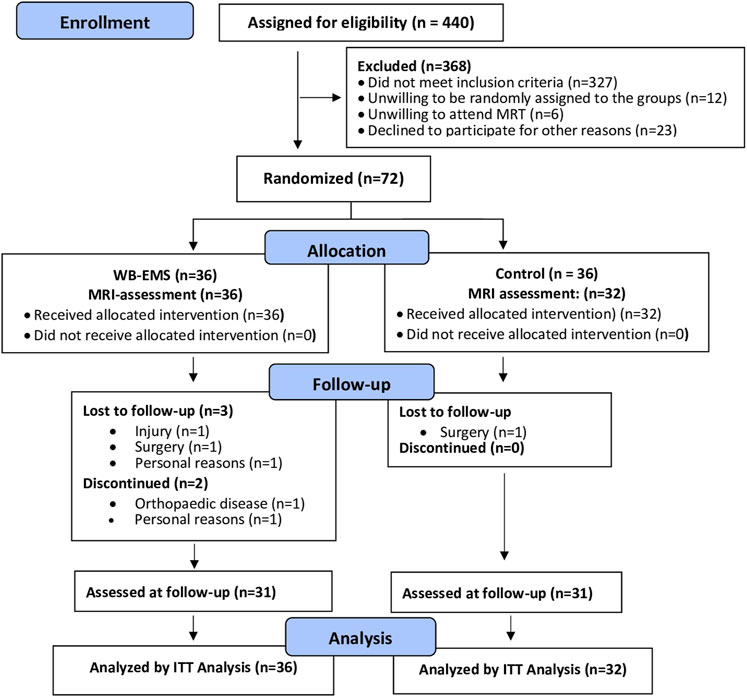
Figure 1. Participant flow throughout the study adapted for MRI assessment.
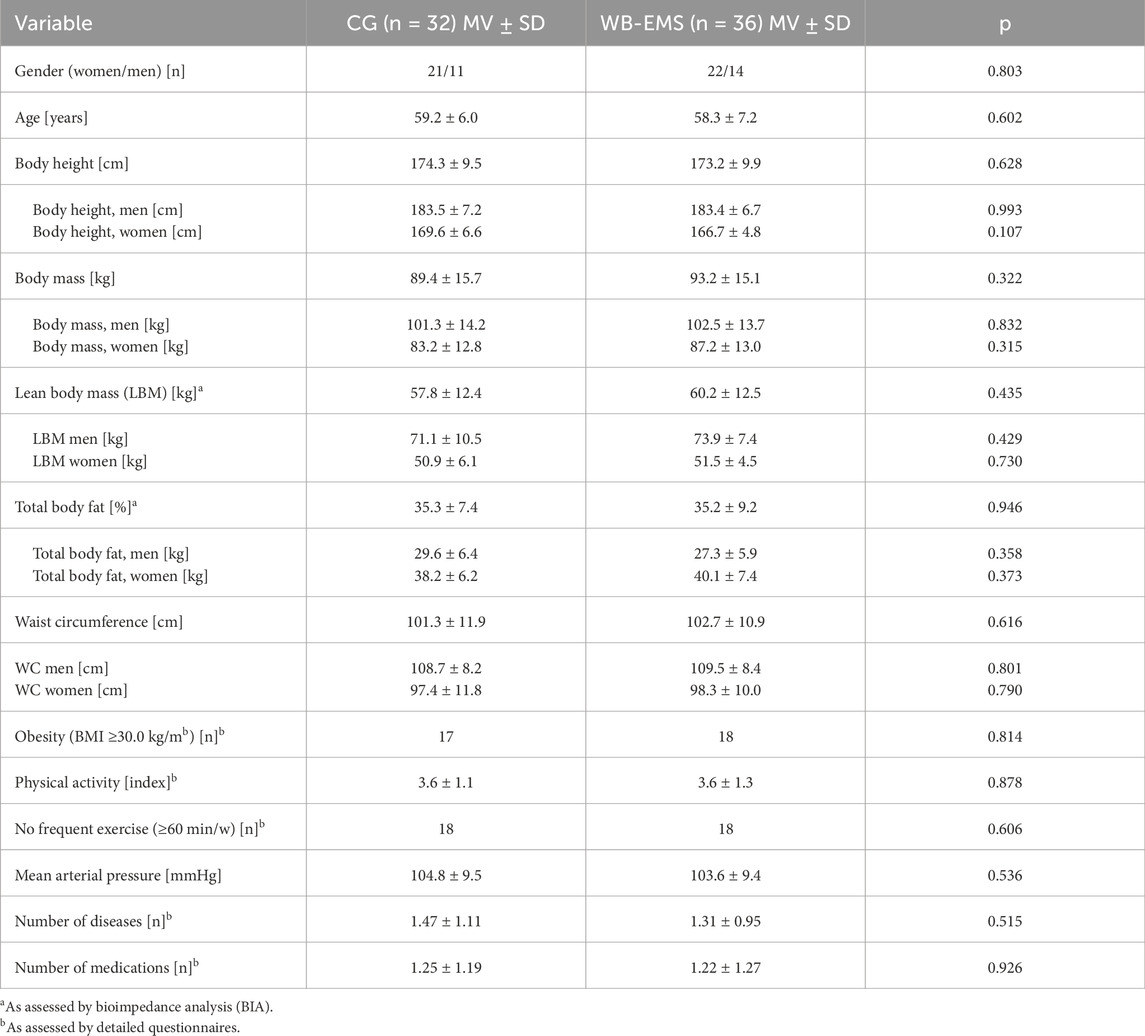
Table 1. Baseline characteristics of the study participants.
2.1.2 Randomization and blinding
Participants allocated themselves to the WB-EMS or control group by drawing lots. Lots were placed in small opaque capsules (“kinder egg”, Ferrero, Italy) and drawn from a bowl. A researcher who was not involved in the present project prepared the lots to ensure allocation concealment. After the randomization procedure, the primary investigator (SK) enrolled participants and instructed them in detail about their study status and corresponding dos and don´ts. Research assistants, testers, and outcome assessors were unaware of the participants’ group status (WB-EMS or CG) and were not allowed to ask either.
2.2 Study procedures
The WB-EMS training group (WB-EMS) conducted 7 months of WB-EMS application as described below, while the control group (CG) was provided with a “usual care” intervention (physiotherapy – see below). Furthermore, the WB-EMS and CG completed a self-management education program for knee OA. Apart from the intervention described above, participants were instructed to maintain their lifestyle, including physical activity, exercise, and dietary habits during the intervention period. There was a monthly reminder about this requirement during the self-education sessions.
2.2.1 WB-EMS intervention
We conducted a standard WB-EMS session (Beier et al., 2024; Kemmler et al., 2021) 1.5 × 20 min per week (e.g., every Monday and every second Thursday) for 29 weeks, including 4 weeks of familiarization and conditioning with the Miha Bodytec type II device (Gersthofen, Germany). Briefly, the thighs and upper arms, gluteals, abdomen, chest, lower back, latissimus, and upper back were stimulated simultaneously but with dedicated impulse intensity. Using bipolar current, the WB-EMS protocol scheduled an impulse low frequency of 85 Hz, an impulse width of 350 µs, and a direct impulse boost with 6 s of EMS stimulation intermitted by a 4 s impulse break. Based on the close interaction between the licensed trainer and a maximum of two trainees, the impulse intensity as prescribed by the rate of perceived exertion (RPE) was carefully increased to “6-7” (i.e., “hard+ to very hard”) on the Borg CR10 Scale (Borg, 2010). During the session, the impulse intensity for all electrodes was carefully adjusted every 3 min to ensure a constant impulse intensity (Kemmler et al., 2023). Video-guided low-intensity exercises (low-amplitude squat with latissimus pulleys, butterfly reverse with angled arms, straight pullovers with trunk flexion, standing trunk flexion, one-legged stand with biceps curl, side step with weight shift, and biceps curl (Weissenfels et al., 2019)) without additional load were conducted during the 6s impulse phase in a standing position. Figure 2 shows an example of a typical exercise/movement conducted during a WB-EMS session.
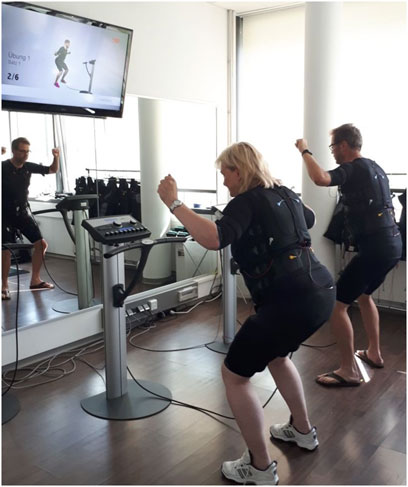
Figure 2. Example of a typical exercise/movement performed during the WB-EMS session.
2.2.2 Control intervention (physiotherapy)
As per the standard care practice in Germany, the control group was provided with six standardized physiotherapy sessions of 20 min each. Physiotherapy treatment was carried out individually in the sense of “standard care” in a diagnosis-oriented manner. The specific content was at the discretion of the treating physiotherapists and included techniques and exercises for reducing pain and detonization of the muscle tissue, increasing mobility of the knee joint, and strengthening leg muscles.
2.2.3 Self-management
A self-management program for osteoarthritis (Nelson et al., 2014) with six sessions of 60 min each was applied for both groups. Briefly, the program aimed to provide education, information, and counseling to prevent the progression of OA, reduce fear and avoidance attitudes, and improve the quality of life and mobility of the participants.
2.3 Study outcomes
As stated, the EMSOAT study predominately focuses on outcomes related to knee osteoarthritis. The present study addressed abdominal fat changes considered secondary outcomes of the EMSOAT project.
• Visceral adipose tissue (VAT) volume between baseline and 29-week follow-up (FU)
2.3.1 Explanatory outcomes
• Changes in the physical activity and exercise between baseline and 29-week FU
• Changes in the dietary intake between baseline and 29-week FU
• Changes in the medication use between baseline and 29-week FU.
2.4 Assessments
2.4.1 MRI data acquisition and examination
MRI scans were acquired at baseline and after 29 weeks of intervention. All scans were consistently acquired using a 3 T scanner (PRISMA, Siemens Healthineers, Erlangen, Germany). We applied a non-contrast-enhanced two-point Dixon Gradient Echo Volumetric Interpolated Breath-hold Examination (VIBE) sequence (TE: 1.29 ms; TR: 3.97 ms; matrix size: 320 × 260; voxel size: 1.2 × 1.2 × 3.5 mm3; and slice gap: 0.7 mm). Twelve slices covered a total length of approximately 5 cm from mid-L2 to mid-L3. Image analysis was performed using the medical image analysis framework (MIAF, Friedrich-Alexander University Erlangen-Nürnberg), as described in detail in a previous publication (Chaudry et al., 2020). The first and last slices were excluded because of intensity inhomogeneity. In the remaining ten slices, the outer contour of the body was determined automatically. The contour of the abdominal cavity was manually segmented by a supervised and trained research assistant. This was performed slice by slice using the Fiji open-source software (Schindelin et al., 2012). Between the measurements of each participant, the position of the scanned volumes was evaluated, and non-overlapping slices were cut off if necessary. In order to separate the VAT inside the abdominal cavity from the inner organs such as the kidneys, intestines, and blood vessels, we used a threshold calculated using the Otsu method (Otsu, 1979) (Figure 3).

Figure 3. Final segmentation result of VAT (yellow overlay) without inner organs and intestines, inner abdominal volume (magenta contour), and outer contour of the body (blue)”.
2.4.2 Baseline characteristics and confounding factors
Body height was assessed using a Holtain stadiometer (Crymych Dyfed, United Kingdom). Direct-segmental multi-frequency bioimpedance analysis (DSM-BIA, InBody 770, Seoul, Korea) was used to determine the body mass and body composition. Overweight (25.0–29.9 kg/m2) and (≥30.0 kg/m2) obesity were classified according to the body mass index (BMI).
At baseline, a detailed standardized questionnaire collected information on (a) demographic parameters; (b) physical limitations, diseases, operations, pharmacologic therapy, dietary supplements; and (c) lifestyle, including physical activity, exercise, and diet. After 29 weeks of intervention, all participants completed the FU questionnaire that aimed to determine changes in conditions/diseases, pharmacologic and physical therapy, physical activity, exercise, and diet, i.e., factors with a potential impact on the present outcomes. The questionnaires were carefully checked for consistency, completeness, and accuracy by the primary investigator (SK), together with the participants.
2.5 Sample size calculation
The sample size calculation was based on a parameter not addressed in the present study. Briefly, 36 participants per group were needed to determine the effects on the primary outcome, “pain of the knee joint,” as determined by the KOOS (Knee Injury and Osteoarthritis Outcome Score; (Roos and Lohmander, 2003)) questionnaire, applying a statistical power of 80%, an α-level of 5%, and a two-tailed t-test approach.
2.6 Statistical analysis
As recommended for RCTs, we applied the intention-to-treat (ITT) principle that included all participants randomly assigned to the study arms (WB-EMS vs CG), regardless of their loss to follow-up. However, as reported, due to the lack of baseline MRI and FU data, four participants in the CG could not be included in the analysis. We used R statistics software (R Development Core Team Vienna, Austria) in combination with Amelia II (Honaker et al., 2011) for multiple imputation (ITT). The full data set was used for multiple imputations, with the imputation repeated 100 times. Normal distribution was checked graphically (gg-plots and residual plots). Within-group changes were analyzed using the t-test. ANCOVA adjusted for baseline differences in VAT volume was applied to determine between-group differences (i.e., “effects”) after 29 weeks. A second ANCOVA was adjusted for baseline VAT volume and gender to determine possible gender differences. Differences in the distribution of categorical variables were analyzed using Pearson’s chi-square tests (Table 1). The standardized mean difference (SMD) was calculated using Cohen (Cohen’s d). All tests were 2-tailed, and significance was set at p < 0.05.
3 Results
Table 1 displays the baseline results of 43 women and 15 men (58.7 ± 6.9 years; BMI: 30.2 ± 4.1 kg/m2) with MRI data. In summary, no significant differences were observed between the WB-EMS and the CG at baseline.
Drop-out and loss to follow-up are displayed in Figure 1. Briefly, four participants (WB-EMS: n = 3 vs CG: n = 1) were unable to attend the 29-week FU assessment. A further two participants of the WB-EMS group quit the study due to reasons not related to the intervention. The attendance rate averaged 88% ± 10% in the WB-EMS group. Predominately due to diseases, four participants (WB-EMS) exercised, on average, less than once a week. Attendance in the physiotherapy sessions (CG) was >90%. Adherence to the WB-EMS or physiotherapy (CG) protocol did not differ significantly between the genders. Furthermore, no adverse effects or injuries were observed during the WB-EMS sessions, and (apart from occasional delayed onset muscular soreness) no participants reported any WB-EMS-related relevant discomfort during or after WB-EMS application.
3.1 Study outcome
Table 2 shows the results for VAT at baseline and the changes after 29 weeks of intervention adjusted for baseline VAT (ANCOVA). In summary, no significant WB-EMS-induced effects (p = 0.090; d’ = 0.43), i.e., group differences for absolute changes between WB-EMS and CG, on the visceral adipose tissue volume were observed. In detail, VAT volume increased non-significantly in the CG (p = 0.246) and decreased non-significantly in the WB-EMS groups (p = 0.143).

Table 2. Baseline data and changes in visceral adipose tissue parameters in the CG and WB-EMS groups. SMD: standardized mean difference;n.s.: non-significant intra-group changes.
Applying ANCOVA that adjusted for baseline VAT and gender revealed significant gender differences with significantly higher WB-EMS-induced effects in men than in women (p = 0.032, d’ = 0.67). A separate analysis of the WB-EMS effects on VAT in women and men is provided in Table 3.

Table 3. Baseline data and changes in visceral adipose tissue parameters in the CG and WB-EMS groups categorized by gender. SMD: standardized mean difference; n.s.: non-significant intra-group changes
In summary, although borderline non-significant (p = 0.052), we observed pronounced intra-group (WB-EMS vs CG) differences in men, while the effect of WB-EMS on VAT changes was negligible in women (p = 0.911).
3.2 Confounding factors
After the intervention period, no significant changes within the groups or between-group differences in physical activity (p = 0.124), exercise participation ≥60 min/w (p = 0.607), or exercise volume (p = 0.976) were reported by the participants. Five participants in the CG (three women and two men) and four participants in the WB-EMS (two women and two men) group (p = 0.794) reported changes in dietary habits, consistent with a reduction in carbohydrates/sugar and/or lower energy intake during the study period. Finally, no relevant changes in medication (e.g., glucocorticoids), conditions (e.g., eating disorders), or diseases (e.g., thyroid function) with potential impacts on abdominal adipose tissue parameters were reported.
4 Discussion
In this trial, which compared WB-EMS to a control group of standard care (physiotherapy), we could not find significant effects on VAT after 7 months of 1.5 × 20 min/week WB-EMS in overweight-to-obese adults. Reviewing the mechanisms of WB-EMS effects on body fat changes induced by increments of energy expenditure, largely comparable to conventional RT exercise, at least three effects can be identified. (a) First, acute energy expenditure during WB-EMS (Kemmler et al., 2012) is limited by the low training volume. (b) The post-exercise effect induced by energy restoration, repair, and adaptive processes post-exercise (EPOC) is particularly pronounced after WB-EMS application (Teschler et al., 2018). (c) Changes in the resting metabolic rate due to hypertrophic effects after WB-EMS (Kemmler et al., 2021).
A review of the literature shows that vigorous aerobic exercise/HIIT is particularly effective in reducing VAT in overweight-to-obese individuals (Chang et al., 2021; Chen et al., 2023; Poon et al., 2024). Aerobic exercise with low or moderate intensity, RT, or a combination of aerobic exercise and RT, on the other hand, is considered less favorable (Chang et al., 2021; Chen et al., 2023). Although there are a few exceptions (Chang et al., 2021), most meta-analyses (Chen et al., 2023; Khalafi et al., 2021; Lopez et al., 2022) reported significant (low to moderate) effect sizes for RT studies; single RCTs in the area of isolated RT and VAT rarely revealed significant effects. Thus, our results of positive, albeit non-significant findings of WB-EMS effects on VAT do not come as a surprise.
Nevertheless, a gender-specific sub-analysis of our data revealed differences with significantly more favorable, albeit still non-significant, VAT effects (WB-EMS vs CG) for the male subgroup (Tab. 3). This finding was supported by a recent network meta-analysis (Chen et al., 2023), which observed a much more pronounced VAT response to RT in men than in women. The same network meta-analysis (Chen et al., 2023) reported that in contrast to people with low body fat, RT was ineffective in reducing VAT in people with body fat rates ≥40%1. However, while only one man in the CG suffered from severe obesity, ten of the 22 women in the WB-EMS group had body fat rates ≥40%. In contrast to our finding of negligible WB-EMS effects on VAT in women, the pilot study by Park et al. (2021) reported significant positive effects on intra-abdominal fat after 8 weeks of 3 × 40 min/week of WB-EMS superimposed on aerobic dance in 30 older women with a similar body fat rate (39% ± 3%) compared to our female subgroup. Thus, there is some evidence that women need a higher training volume or/and superimposed WB-EMS to significantly affect the VAT. In contrast, a lower training volume seems to be sufficient for men for generating relevant VAT effects. This latter speculation was confirmed by a recent low-volume (2 × 40 min/week) RT trial with 43 older, predominantly overweight-to-obese men that determined similarly pronounced and (presumably due to the higher statistical power) significant net effects on VAT compared to the present male cohort (Knauer et al., 2023). In summary, adding significantly higher training frequency and strenuous voluntary exercises would not be a reasonable option, considering that the unique selling point of present WB-EMS concepts is their time-effective and joint-friendly characteristics.
Apart from cohort and exercise characteristics, one may argue that changes in dietary intake may have confounded the VAT results. Although participants were frequently instructed to maintain their dietary habits, nine of the 68 participants listed changes during the 29-week study period. As a similar number of people in the WB-EMS and CG groups reported changes in dietary habits, we feel that this aspect does not relevantly impact our findings. Undoubtedly, however, a more detailed monitoring of dietary records would have provided deeper insight into this issue.
Other limitations and peculiarities of the present trial of VAT should be addressed. (a) First, the primary outcome of this project, which included overweight and obese knee OA patients, was “pain of the knee joint”, while VAT was considered a secondary study outcome. One may argue that the alignment of the intervention was thus not customized to (optimally) address the VAT. However, the most effective WB-EMS protocol to achieve this outcome remains clear. Considering further that time efficiency is a key characteristic of WB-EMS, we applied the 20-min WB-EMS standard protocol (Beier et al., 2024; Le et al., 2024), which is known to trigger significant positive effects on a large variety of different outcomes (Kemmler et al., 2024). Another limitation of this satellite study of a larger project was the sample size analysis that did not address VAT. (b) Similarly, we did not focus on one gender but included women and men. Although the sample size of at least 32 participants/group included in the primary ITT analysis exceeds the statistical power of most RT studies with significant positive effects on VAT (Chen et al., 2023; Khalafi et al., 2021), in particular the low statistical power among the male subgroup (WB-EMS: n = 14 vs CG: n = 11) might have contributed to the borderline non-significant WB-EMS effect on VAT in men. (c) The study included adults with moderate-to-advanced knee osteoarthritis who were overweight and obese. Overweight/obesity is a strong predictor of knee OA (King et al., 2013), not only due to the higher mechanical load but also to the pro-inflammatory effects, particularly triggered by the VAT fraction (Kawai et al., 2021). Although the low-frequency, non-superimposed WB-EMS concepts might not be the most promising exercise for VAT reduction, the rationale for WB-EMS application in this cohort with OA was the opportunity for a joint-friendly protocol with low-amplitude, low-intensity movements/exercises. (d) Finally, another methodological weakness could be the lack of participant blinding. Optionally, the CG could have received the same intervention but with a pulse intensity below the motor threshold. We decided against this alternative since (a) even low stimulus intensity (e.g., low-intensity TENS) might trigger favorable effects on (knee) pain intensity (as the primary study outcome), and (b) we considered it more appropriate to provide a real-world comparison with an established therapy approach for knee OA.
In summary, we failed to determine significant positive effects of low-volume, non-superimposed WB-EMS on VAT, whether in women or (borderline) in men. Nevertheless, we are still convinced that individuals with OA will benefit from WB-EMS by improving their musculoskeletal outcomes. Although some participant characteristics might have contributed to our results, we conclude that, largely due to the low application volume, the present WB-EMS protocols applied most in scientific and commercial settings might not be the perfect tool for decreasing VAT, particularly in overweight-to-obese women.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors without undue reservation.
Ethics statement
The studies involving humans were approved by the University Ethics Committee of the Friedrich-Alexander University of Erlangen-Nürnberg (FAU), Erlangen, Germany (No. 352_20 B). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BB: conceptualization, data curation, software, visualization, writing – original draft, and writing – review and editing. OC: data curation, investigation, software, visualization, writing – original draft, and writing – review and editing. SK: data curation, investigation, project administration, resources, supervision, writing – original draft, and writing – review and editing. SV: conceptualization, funding acquisition, investigation, methodology, project administration, writing – original draft, and writing – review and editing. MK: conceptualization, formal analysis, methodology, visualization, writing – original draft, and writing – review and editing. FR: conceptualization, investigation, methodology, project administration, resources, writing – original draft, and writing – review and editing. KE: conceptualization, methodology, software, validation, visualization, writing – original draft, and writing – review and editing. MU: conceptualization, funding acquisition, methodology, resources, writing – original draft, and writing – review and editing. WK: conceptualization, data curation, funding acquisition, investigation, methodology, project administration, resources, validation, writing – original draft, and writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. We would like to thank the Else Kröner-Fresenius-Stiftung for providing funding for the present study.
Acknowledgments
The authors acknowledge the support from the non-profit organizations Else Kröner-Fresenius-Stiftung and Netzwerk Knochengesundheit Erlangen e.V., Germany. The work was performed in (partial) fulfillment of the requirements for BB to obtain the degree med. dent.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were editorial board members of Frontiers at the time of submission. This had no impact on the peer review process or the final decision.
The reviewer HK declared a past co-authorship with the authors WK and MK to the handling editor.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1However, the author had not adjusted on gender differences. Overweight and obesity thresholds vary considerably between the genders (with lower values for men) when applying body fat rate (Tomlinson et al., 2019). Thus, gender differences might have confounded the effect of body fat rate (and vice versa) on VAT changes
References
Altman R., Alarcon G., Appelrouth D., Bloch D., Borenstein D., Brandt K., et al. (1991). The American College of Rheumatology criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 34, 505–514. doi:10.1002/art.1780340502
A'Naja M. N., Batrakoulis A., Camhi S. M., McAvoy C., Sansone J. S., Reed R. (2024). 2025 ACSM worldwide fitness trends: future directions of the health and fitness industry. ACSM's Health and Fit. J. 28, 11–25. doi:10.1249/fit.0000000000001017
Batrakoulis A., Jamurtas A. Z., Fatouros I. G. (2021). High-intensity interval training in metabolic diseases: physiological adaptations. ACSM's Health and Fit. J. 25, 54–59. doi:10.1249/FIT.0000000000000703
Batrakoulis A., Jamurtas A. Z., Metsios G. S., Perivoliotis K., Liguori G., Feito Y., et al. (2022). Comparative efficacy of 5 exercise types on cardiometabolic health in overweight and obese adults: a systematic review and network meta-analysis of 81 randomized controlled trials. Circ. Cardiovasc Qual. Outcomes 15, e008243. doi:10.1161/CIRCOUTCOMES.121.008243
Beier M., Schoene D., Kohl M., von Stengel S., Uder M., Kemmler W. (2024). Non-athletic cohorts enrolled in longitudinal whole-body electromyostimulation trials - an evidence map. Sensors (Basel) 24, 972. doi:10.3390/s24030972
Bennell K. L., Nelligan R. K., Kimp A. J., Schwartz S., Kasza J., Wrigley T. V., et al. (2020). What type of exercise is most effective for people with knee osteoarthritis and co-morbid obesity?the TARGET randomized controlled trial. Osteoarthr. Cartil. 28, 755–765. doi:10.1016/j.joca.2020.02.838
Brown J. C., Harhay M. O., Harhay M. N. (2016). Visceral adipose tissue dysfunction and mortality among a population-based sample of males and females. Diabetes Metab. 42, 382–385. doi:10.1016/j.diabet.2016.05.001
Chang Y.-H., Yang H.-Y., Shun S.-C. (2021). Effect of exercise intervention dosage on reducing visceral adipose tissue: a systematic review and network meta-analysis of randomized controlled trials. Int. J. Obes. 45, 982–997. doi:10.1038/s41366-021-00767-9
Chaudry O., Grimm A., Friedberger A., Kemmler W., Uder M., Jakob F., et al. (2020). Magnetic resonance imaging and bioelectrical impedance analysis to assess visceral and abdominal adipose tissue. Obes. (Silver Spring) 28, 277–283. doi:10.1002/oby.22712
Chen Q., Wu Y., Gao Y., Zhang Z., Shi T., Yan B. (2022). Effect of visceral adipose tissue mass on coronary artery disease and heart failure: a Mendelian randomization study. Int. J. Obes. (Lond). 46, 2102–2106. doi:10.1038/s41366-022-01216-x
Chen X., He H., Xie K., Zhang L., Cao C. (2023). Effects of various exercise types on visceral adipose tissue in individuals with overweight and obesity: a systematic review and network meta-analysis of 84 randomized controlled trials. Obes. Rev. 25, e13666. doi:10.1111/obr.13666
Guretzki E., Kohl M., von Stengel S., Uder M., Kemmler W. (2024). Effects of whole-body electromyostimulation on metabolic syndrome in adults at moderate-to-high cardiometabolic risk-A systematic review and meta-analysis. Sensors 24, 6788. doi:10.3390/s24216788
Hall J. E., do Carmo J. M., da Silva A. A., Wang Z., Hall M. E. (2015). Obesity-induced hypertension: interaction of neurohumoral and renal mechanisms. Circ. Res. 116, 991–1006. doi:10.1161/CIRCRESAHA.116.305697
Honaker J., King G., Blackwell M. (2011). AmeliaII: a program for missing data, J. Stat. Softw. 45: 1–47. doi:10.18637/jss.v045.i07
Kawai T., Autieri M. V., Scalia R. (2021). Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 320, C375–C391. doi:10.1152/ajpcell.00379.2020
Kemmler W., Fröhlich M., Eifler C. (2024). “Whole-body electromyostimulation,” in Effects, limitations, perspectives of an innovative training method. Cham, Switzerland: Springer.
Kemmler W., Fröhlich M., Ludwig O., Eifler C., von Stengel S., Willert S., et al. (2023). Position statement and updated international guideline for safe and effective whole-body electromyostimulation training-the need for common sense in WB-EMS application. Front. Physiol. 14, 1174103. doi:10.3389/fphys.2023.1174103
Kemmler W., Kleinoder H., Fröhlich M. (2020). Editorial: whole-body electromyostimulation: a training technology to improve health and performance in humans? Front. Physiol. 11, 523. doi:10.3389/fphys.2020.00523
Kemmler W., Shojaa M., Steele J., Berger J., Fröhlich M., Schoene D., et al. (2021). Efficacy of Whole-Body Electromyostimulation (WB-EMS) on body composition and muscle strength in non-athletic adults. A systematic review and meta-analysis. Front. Physiol. 12, 640657. doi:10.3389/fphys.2021.640657
Kemmler W., Von Stengel S., Schwarz J., Mayhew J. L. (2012). Effect of whole-body electromyostimulation on energy expenditure during exercise. J. Strength Cond. Res. 26, 240–245. doi:10.1519/JSC.0b013e31821a3a11
Kemmler W., Weissenfels A., Willert S., Fröhlich M., Ludwig O., Berger J., et al. (2019). Recommended contraindications for the use of non-medical WB-electromyostimulation. Dtsch. Z Sportmed 70, 278–282. doi:10.5960/dzsm.2019.401
Khalafi M., Malandish A., Rosenkranz S. K., Ravasi A. A. (2021). Effect of resistance training with and without caloric restriction on visceral fat: a systemic review and meta-analysis. Obes. Rev. 22, e13275. doi:10.1111/obr.13275
Kim J., Kim K. (2023). CT-based measurement of visceral adipose tissue volume as a reliable tool for assessing metabolic risk factors in prediabetes across subtypes. Sci. Rep. 13, 17902. doi:10.1038/s41598-023-45100-8
King L. K., March L., Anandacoomarasamy A. (2013). Obesity and osteoarthritis. Indian J. Med. Res. 138, 185–193. Available online at: https://www.ncbi.nlm.nih.gov/pubmed/24056594.
Knauer K., Chaudry O., Uder M., Kohl M., Kemmler W., Bickelhaupt S., et al. (2023). Effects of high-intensity resistance training on visceral adipose tissue and abdominal aortic calcifications in older men with osteosarcopenia - results from the FrOST study. Clin. Interv. Aging 18, 71–80. doi:10.2147/CIA.S388026
Le Y. E., Schoene D., Kohl M., von Stengel S., Uder M., Kemmler W. (2024). Outcomes addressed by longitudinal whole-body electromyostimulation trials in middle aged-older adults - an evidence map. Jpn. J. Med. Sci. 2, 2024030183. doi:10.20944/preprints202403.0183.v1
Lee H. S., Lee J. (2021). Effects of exercise interventions on weight, body mass Index, lean body mass and accumulated visceral fat in overweight and obese individuals: a systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 18, 2635. doi:10.3390/ijerph18052635
Lopez P., Taaffe D. R., Galvão D. A., Newton R. U., Nonemacher E. R., Wendt V. M., et al. (2022). Resistance training effectiveness on body composition and body weight outcomes in individuals with overweight and obesity across the lifespan: a systematic review and meta-analysis. Obes. Rev. 23, e13428. doi:10.1111/obr.13428
Nelson A. E., Allen K. D., Golightly Y. M., Goode A. P., Jordan J. M. (2014). A systematic review of recommendations and guidelines for the management of osteoarthritis: the chronic osteoarthritis management initiative of the U.S. bone and joint initiative. Semin. Arthritis Rheum. 43, 701–712. doi:10.1016/j.semarthrit.2013.11.012
Ohman M. K., Wright A. P., Wickenheiser K. J., Luo W., Eitzman D. T. (2009). Visceral adipose tissue and atherosclerosis. Curr. Vasc. Pharmacol. 7, 169–179. doi:10.2174/157016109787455680
Otsu N. (1979). A threshold selection method from gray-level histograms. IEEE Trans. Syst. man, Cybern. 9, 62–66. doi:10.1109/tsmc.1979.4310076
Park B. J., Kim Y. J., Kim D. H., Kim W., Jung Y. J., Yoon J. H., et al. (2008). Visceral adipose tissue area is an independent risk factor for hepatic steatosis. J. Gastroenterol. Hepatol. 23, 900–907. doi:10.1111/j.1440-1746.2007.05212.x
Park S., Park J., Ham J. A., Jee Y. (2021). Effects of aerobic dance with electrical stimulant on body composition and radiological circumference of obese elderly women. Gazzetta Medica Ital. Arch. Sci. Mediche 180, 87–95. doi:10.23736/s0393-3660.20.04412-5
Poon E. T., Wongpipit W., Li H. Y., Wong S. H., Siu P. M., Kong A. P., et al. (2024). High-intensity interval training for cardiometabolic health in adults with metabolic syndrome: a systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 58, 1267–1284. doi:10.1136/bjsports-2024-108481
Roos E. M., Lohmander L. S. (2003). The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual. Life Outcomes 1, 64. doi:10.1186/1477-7525-1-64
Schindelin J., Arganda-Carreras I., Frise E., Kaynig V., Longair M., Pietzsch T., et al. (2012). Fiji: an open-source platform for biological-image analysis. Nat. Methods 9, 676–682. doi:10.1038/nmeth.2019
Silveira E. A., Kliemann N., Noll M., Sarrafzadegan N., de Oliveira C. (2021). Visceral obesity and incident cancer and cardiovascular disease: an integrative review of the epidemiological evidence. Obes. Rev. 22, e13088. doi:10.1111/obr.13088
Teschler M., Wassermann A., Weissenfels A., Frohlich M., Kohl M., Bebenek M., et al. (2018). Short time effect of a single session of intense whole-body electromyostimulation on energy expenditure. A contribution to fat reduction? Appl. Physiol. Nutr. Metab. 43, 528–530. doi:10.1139/apnm-2017-0602
Tomlinson D. J., Erskine R. M., Morse C. I., Onambele G. L. (2019). Body fat percentage, body mass Index, fat mass Index and the ageing bone: their singular and combined roles linked to physical activity and diet. Nutrients 11, 195. doi:10.3390/nu11010195
von Kruchten R., Lorbeer R., Muller-Peltzer K., Rospleszcz S., Storz C., Askani E., et al. (2022). Association between adipose tissue depots and dyslipidemia: the KORA-MRI population-based study. Nutrients 14, 797. doi:10.3390/nu14040797
Weissenfels A., Wirtz N., Dormann U., Kleinoder H., Donath L., Kohl M., et al. (2019). Comparison of whole-body electromyostimulation versus recognized back-strengthening exercise training on chronic nonspecific low back pain: a randomized controlled study. Biomed. Res. Int. 2019, 5745409. doi:10.1155/2019/5745409
World_Medical_Association (2013). World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. doi:10.1001/jama.2013.281053
Keywords: electromyostimulation, exercise, intra-abdominal fat, visceral fat, magnetic resonance imaging, obesity, adults
Citation: Burkhardt B, Chaudry O, Kast S, von Stengel S, Kohl M, Roemer FW, Engelke K, Uder M and Kemmler W (2025) The effect of whole-body electromyostimulation on visceral adipose tissue volume in overweight-to-obese adults with knee osteoarthritis: A randomized controlled study. Front. Physiol. 16:1544332. doi: 10.3389/fphys.2025.1544332
Received: 12 December 2024; Accepted: 24 March 2025;
Published: 15 April 2025.
Edited by:
Kyle Timmerman, Miami University, United StatesReviewed by:
Alexios Batrakoulis, Democritus University of Thrace, GreeceHeinz Kleinöder, German Sport University Cologne, Germany
Alessandra Di Cagno,Università degli Studi di Roma Foro Italico, Italy
Copyright © 2025 Burkhardt, Chaudry, Kast, von Stengel, Kohl, Roemer, Engelke, Uder and Kemmler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wolfgang Kemmler, d29sZmdhbmcua2VtbWxlckBmYXUuZGU=
†ORCID: Wolfgang Kemmler, orcid.org/0000-0003-3515-0669