 Sabrina De Cillis1*†
Sabrina De Cillis1*† Daniele Amparore1†Alberto Quarà1
Daniele Amparore1†Alberto Quarà1 Enrico Checcucci2Alberto Piana1Gabriele Volpi1Federico Piramide1
Enrico Checcucci2Alberto Piana1Gabriele Volpi1Federico Piramide1 Michele Sica1Michele Ortenzi1Matteo Manfredi1Michele Di Dio3Stefano De Luca1Cristian Fiori1
Michele Sica1Michele Ortenzi1Matteo Manfredi1Michele Di Dio3Stefano De Luca1Cristian Fiori1 Francesco Porpiglia1 and on behalf of the ESUT lower Tract group
Francesco Porpiglia1 and on behalf of the ESUT lower Tract group- 1Department of Oncology, Division of Urology, University of Turin, San Luigi Gonzaga Hospital, Turin, Italy
- 2Department of Surgery, Candiolo Cancer Institute, Fondazione del Piemonte per l’Oncologia - Istituto di Ricerca e Cura a Carattere Scientifico (FPO-IRCCS), Turin, Italy
- 3Division of Urology, Department of Surgery, Annunziata Hospital, Cosenza, Italy
Introduction: This study aims to assess our first clinical experience with Aquablation in terms of perioperative and 1-year micturition outcomes, with a focus on postoperative lower urinary tract symptoms (LUTS).
Materials and methods: From 10/2018 to 07/2021, patients referred to our center with BPH-related LUTS, International Prostate Symptom Score (IPSS) ≥10, maximum urinary flow rate (Qmax) ≤12 ml/s, and prostate volume <80 ml were enrolled in this prospective study to undergo Aquablation. Demographics, perioperative data, and complications (according to the Clavien–Dindo system) were collected. Functional outcomes were assessed at 1, 3, 6, and 12 months with IPSS, IPSS quality of life (IPSS QoL), uroflowmetry, and evaluation of post void residue (PVR). The types of LUTS were classified on the basis of IPSS single question answers in filling phase LUTS and voiding phase LUTS.
Results: Sixty patients were enrolled in the study. The mean patient age was 64.9 ± 7.3 years, prostate volume was 63.5 ± 16.8) ml, Qmax was 8.4 ± 2.6 ml/s, the median (IQR) IPSS was 23 (19–26), and the IPSS QoL score was 5 (4–5). The mean Qmax at 1, 3, 6, and 12 months was 21.1 ± 11, 18.1 ± 5.4, 17.1 ± 6, and 17.8 ± 6.6 ml/s, respectively. The median IPSS urinary symptom score was 2 (2–5) one year after surgery. In parallel, the median IPSS QoL score and mean PVR reached 1 (0–1) and 23.6 ml (25.5) in the 12th month. At 1- and 3-month follow-up, filling phase symptoms were predominant in almost two-thirds of the study population. Within the patients who reported a prevalence of filling phase symptoms at 3 months, 27 of 38 (71%) reported a de novo onset of these symptoms after surgery.
Conclusion: Aquablation is a safe procedure for treating BPH-related LUTS, and it has been demonstrated to be effective up to 12 months after the procedure. LUTS of the filling phase were more prevalent than voiding phase ones in the first 3 months following surgery, but showed a self-limited fashion.
Introduction
As the global population progressively ages, benign prostatic hyperplasia (BPH) associated with lower urinary tract symptoms (LUTS) has become the most diagnosed urological condition among men aged 45–74 years (1). Transurethral resection of the prostate (TURP) holds the role of “gold standard” surgical treatment for BPH, but it is not devoid of short- and long-term complications, including perioperative and postoperative morbidity (20%), ejaculatory dysfunction (65%), erectile disorders (10%), and urethral strictures (7%) (2–4). Moreover, while most patients report a marked improvement in symptoms, up to about one-third of patients undergoing TURP complain of postoperative LUTS (5). Patients may refer to refractory or de novo symptoms often require to continue or switch medical therapy postoperatively, that typically can range across all micturition phases: filling phase (urgency, urge incontinence, pollakiuria); voiding phase (decreased force of stream, straining); post micturition (urinary retention) (6). Indeed, a non-negligible percentage of patients treated with TURP will not experience an improvement in their quality of life.
For all those reasons, in the last few decades, a tremendous effort has been made by urologists in the search for new surgical techniques to improve upon the results achieved by TURP. The impressive momentum of innovation driven by the availability of new technologies has supplied the surgical armamentarium with plenty of new techniques using different types of energy, such as lasers (Holmium, Thullim, photoselective vaporization (PVP)), water vapor thermal therapy (Rezum), temporary implantable nitinol devices (iTINDs) and prostatic urethral lift (PUL) (7–12), among others. Besides the proven safety and feasibility, the occurrence or persistence of filling phase symptoms is still an open issue.
One of the most recent introductions in the field of BPH surgery is the Aquablation system (PROCEPT BioRobotics, Redwood Shores, CA, USA) (13). This technique relies on a robotic system that uses a jet of high-velocity saline solution to ablate prostate adenoma under real-time trans-rectal ultrasound (TRUS) guidance. Since its launch in 2017, Aquablation has demonstrated shorter operating times and superior postoperative ejaculatory function compared to TURP, HoLEP, and PVP, with similar rates of short- and mid-term adverse events (14, 15). In the ongoing WATER trial, authors reported that there was no significant difference between Aquablation and TURP concerning International Prostate Symptoms Score (IPSS) reduction, improvement in quality of life (QoL) score, increase in maximum urinary flow rate (Qmax), and post-void residual (PVR) at the 3-year follow-up (16).
Along with these encouraging functional data, the mechanism of action of Aquablation involving a high-velocity low-temperature water jet raised the question of whether postoperative LUTS (particularly filling phase LUTS) existed in patients undergoing this procedure.
Analyzing postoperative LUTS in more depth, the authors found no differences in terms of urgency rate, frequency, dysuria, or incontinence between the two techniques both in the immediate postoperative period (<3 months) and beyond (p = 0.723 and 1.000, respectively (16). Moreover, the postoperative medical therapy discontinuation and starting rates were similar in both groups.
With the aim of contributing to this field of research, we report our first clinical experience as a tertiary care center with the use of Aquablation for the treatment of BPH symptoms, particularly focusing on perioperative and micturition outcomes and analyzing postoperative residual or de novo LUTS.
Materials and methods
Study design
In this prospective single-arm study, we evaluated the safety and efficacy of Aquablation for treating BPH-related LUTS. After the approval of the local ethics committee (ethics committee of San Luigi Gonzaga Hospital, registry number 132/2019), the study-enrolled patients presenting with BPH-related LUTS, IPSS ≥10, Qmax ≤12 ml/s, and prostate volume <80 ml were observed in our department for BPH surgery between October 2018 and July 2021.
Exclusion criteria included prostate cancer diagnosis, previous prostate surgery, indwelling catheter or self-catheterization, urethral stenosis, bladder stones, clinically significant bladder diverticulum, and prostatic calcifications. Men taking anticoagulants or on antiplatelet therapy that could not be discontinued were also excluded.
Surgical procedure
The Aquablation system consists of three elements: the console, the 24 Fr robotic handpiece, and the disposable probe (Figure 1). The procedures were performed via general or spinal anesthesia, according to the characteristics and preference of the patient. First, with the patient in a dorsal lithotomy position, the TRUS probe was positioned and anchored to an articulating arm mounted to the surgical table. Next, a robotically guided handpiece containing a sapphire nozzle is used to access the bladder through the urethra. The handpiece was positioned with the tip just inside the bladder before the scope was retracted to visualize the bladder neck, placed above the verumontanum and anchored to a second articulating arm. Once the handpiece was correctly positioned, the TRUS probe was inserted until the central part of the prostate was correctly visualized and could be used to compress the prostate and improve the ultrasound visualization if necessary. After placement of the TRUS probe and handpiece, the operator maps the prostate by delineating the boundaries of the area to be treated using the dedicated software. The software allows for changes in depth up to 25 mm and the angle of resection up to 225°, to adapt the delineating area to the specific anatomy of the patient. Moreover, the software allows safety areas to be demarcated. In these areas, the water jet reaches lower pressures and depths (Figure 2). Usually, these areas are located at the level of the bladder neck and verumontanum. The ablative phase could be initiated and controlled with the aid of a foot pedal. The Aquablation automatically adjusted the flow rate in each direction to alter the depth of penetration and remove the tissue following the borders outlined by the surgeon. After the first passage, additional ablation passages could be performed if necessary, depending on the shape and size of the prostate. At the end of the ablative phase, hemostasis was achieved by selective coagulation of the bleeding vessels using a bipolar resector. A 20-Fr Doufur catheter was placed at the end of the procedure with the balloon inflated accordingly to prostate size. Bladder irrigation was usually maintained for a mean of 48 h.

Figure 1 Aquablation system conformal planning unit, console, and handpiece.
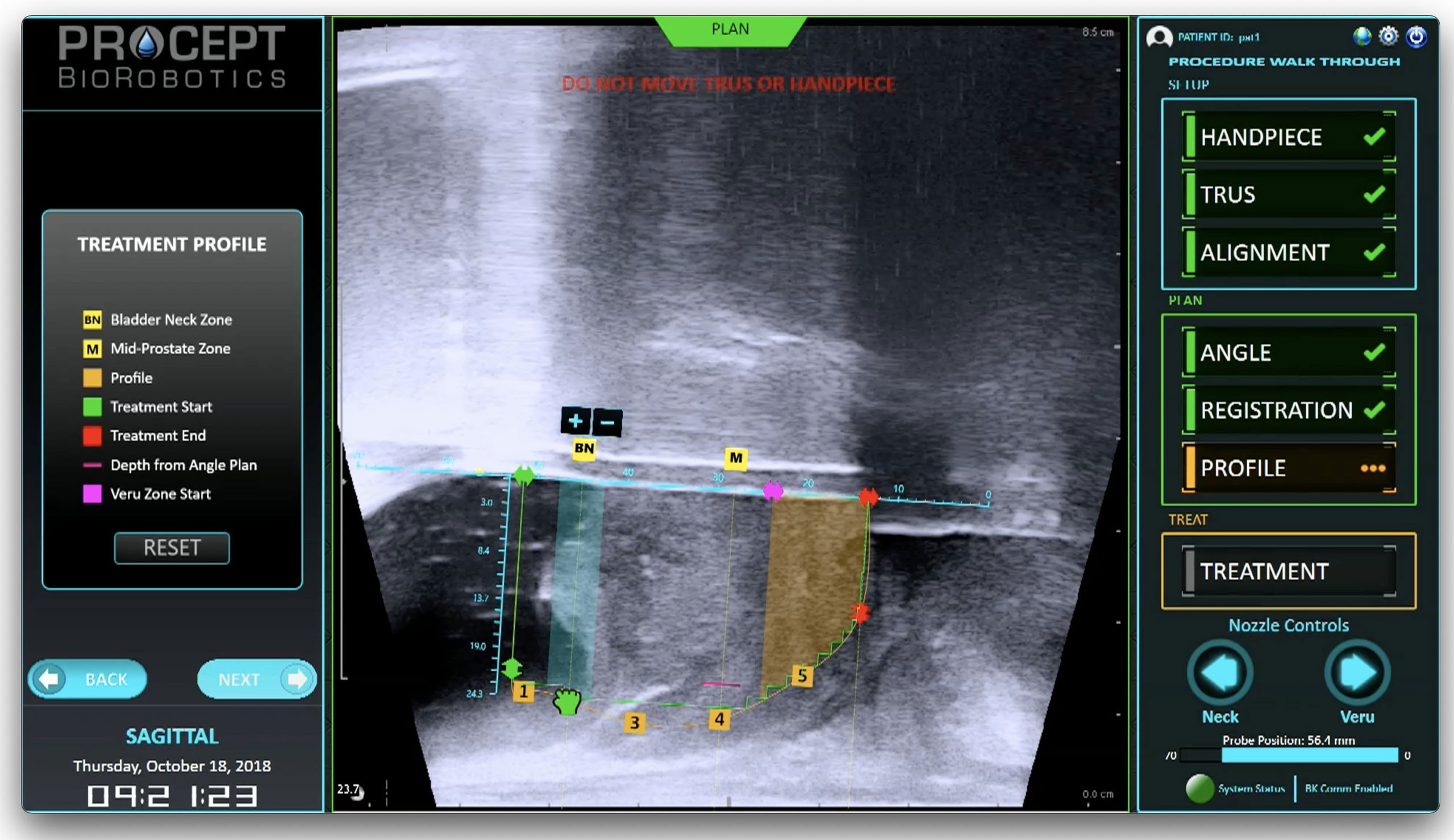
Figure 2 Aquablation display on conformal planning unit at the end of the mapping phase. Blue and orange areas represent the safety zones at the bladder neck and verumontanum.
Data collection and follow-up
Demographics, use of preoperative BPH-drugs, perioperative data, and complications (according to the Clavien–Dindo system) were collected. For the porpoise of the study, all the patients were told to discontinue previous BPH medical therapy at time of discharge and no drugs (AB, 5-ARI, AC, or B3A) were prescribed after the Aquablation procedure in order to correctly assess the presence of postoperative LUTS.
Functional outcomes were assessed at 1, 3, 6, and 12 months with IPSS, IPSS Quality of Life (IPSS Qol), uroflowmetry, and evaluation of PVR.
A detailed evaluation of the answers given to the individual questions of the IPSS questionnaire was carried out in order to classify the type of LUTS the patients were suffering from. In particular, the questions were grouped according to the category of symptoms they investigated: questions numbers 1, 3, 5, and 6 (1—how often have you had a sensation of not emptying your bladder completely after you finish urinating?; 3—how often have you found you stopped and started again several times when you urinated?; 5—how often have you had a weak urinary stream?; 6—Over the past month, how often have you had to push or strain to begin urination)? grouped under the category LUTS of voiding phase; question numbers 2, 4, and 7 (2—how often have you had to urinate again less than two hours after you have finished urinating?; 4—how often have you found it difficult to postpone urination?; 7—how many times did you most typically get up each night to urinate from the time you went to bed until the time you got up in the morning)? LUTS refers to the filling phase. Finally, we summed up the scores expressed by each patient for each symptom category and classified the patients as suffering from predominantly emptying phase or filling phase symptoms at each timepoint.
Statistical analysis
Descriptive statistics included frequencies and proportions for categorical variables and means and standard deviation or median and interquartile range for continuous ones. The means of continuous variables were compared using the paired Student’s t-test after verifying that the variables to be analyzed were approximately normally distributed. A Chi-square was used to compare the rates of LUTS symptom categories at each time point. A p <0.05 was considered to indicate statistical significance. JAMOVI version 2.0 (The Jamovi Project, 2022) was used for statistical analysis.
Results
A total of 60 patients were enrolled from October 2018 to July 2021, with a minimum of 12 months of follow-up. Demographic and perioperative data are summarized in Table 1.
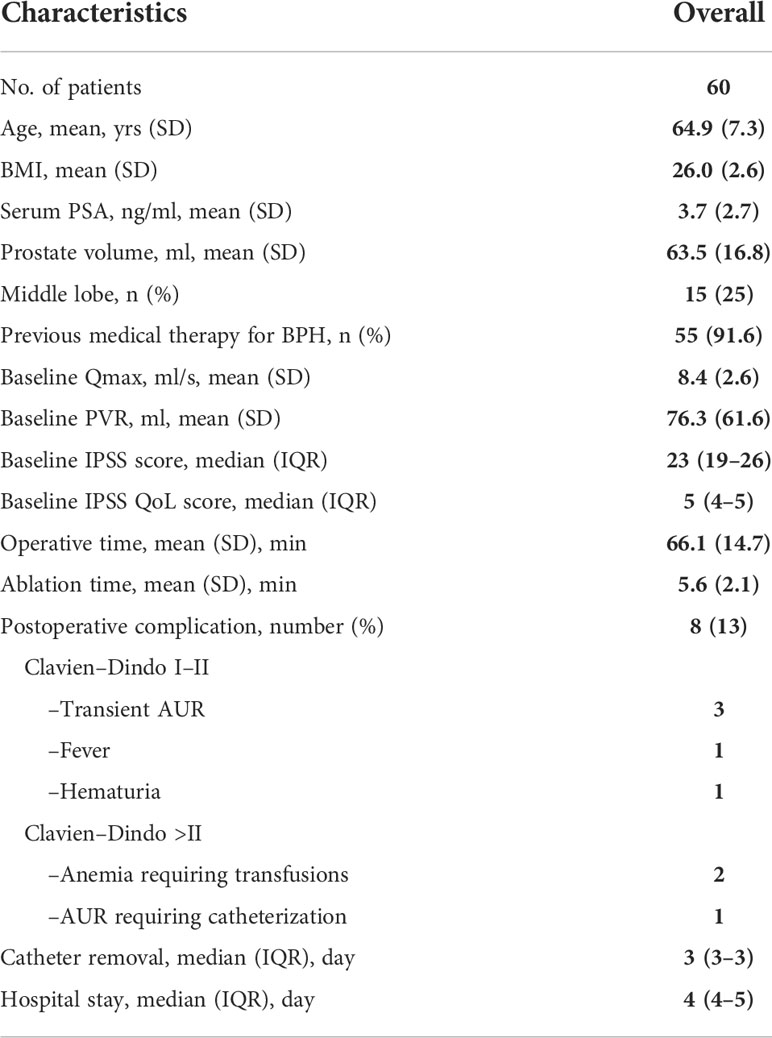
Table 1 Demographics and perioperative variables (SD, standard deviation; IQR, interquartile range; BMI, body mass index; PSA, prostate specific antigen; BPH, benign prostatic hyperplasia; Qmax, peak urinary flow; PVR, post void residual; IPSS, International Prostate Symptoms Score; IPSS QoL, International Prostate Symptoms Score Quality of Life).
The study population had a mean age of 64.9 ± 7.3 years, a prostate volume of 63.5 ± 16.8 ml, a PSA of 3.7 ± 2.7 ng/ml, a baseline Qmax of 8.4 ± 2.6 ml/s, and a PVR of 76.3 ± 61.6 ml. Fifty-five patients (91.6%) were previously on alpha-blockers (AB) or 5-alpha reductase inhibitors (5-ARI) for BPH. No patients reported preoperative therapy with anticholinergic (AC) or beta3-agonists (B3A) drugs.
At enrollment, patients reported a median IPSS of 23 (19–26), an IPSS QoL of 5 (4–5).
All the Aquablation procedures were uneventful and no intraoperative complications were observed.
A mean operative time and ablation time of 66.1 ± 14.7 and 5.6 ± 2.1 min were recorded, respectively. In all the procedures, hemostasis was achieved by focal transurethral bipolar coagulation of bleeding vessels.
Eight (13%) postoperative complications were recorded, of which three (5%) were classified as Clavien–Dindo >II (two gross hematurias requiring blood transfusions and one acute urinary retention requiring catheterization for 12 h). The remaining five (8%) complications (three transient acute urinary retentions, one fever, and one hematuria post catheter removal) were self-limited and classified as Clavien–Dindo I or II.
Median catheterization and hospitalization times were 3 (3–3) and 4 (4–5), respectively.
Concerning functional outcomes (Table 2), the mean Qmax recorded a peak at 1-month with 21.1 ± 11 ml/s and stabilized itself at 17.8 ± 6.6 ml/s at 12 months, with an improvement from baseline of 9.4 ml/s. PVR decreased by 52.7 ml from preoperative evaluation, reaching a mean of 23.6 ± 25.5 ml at 1-year follow-up. Statistically significant (p <0.001) improvements in IPSS scores from baseline were noted at each time point. Specifically, IPSS dropped from a preoperative median of 23 (19–26) to 2 (2–5) in 1 year. This improvement was coupled with a parallel decrease in the QoL score, recording a median of 1 (0–1) at 1-year, with an improvement from the baseline of 4 points. No patients reported urinary incontinence after Aquablation.
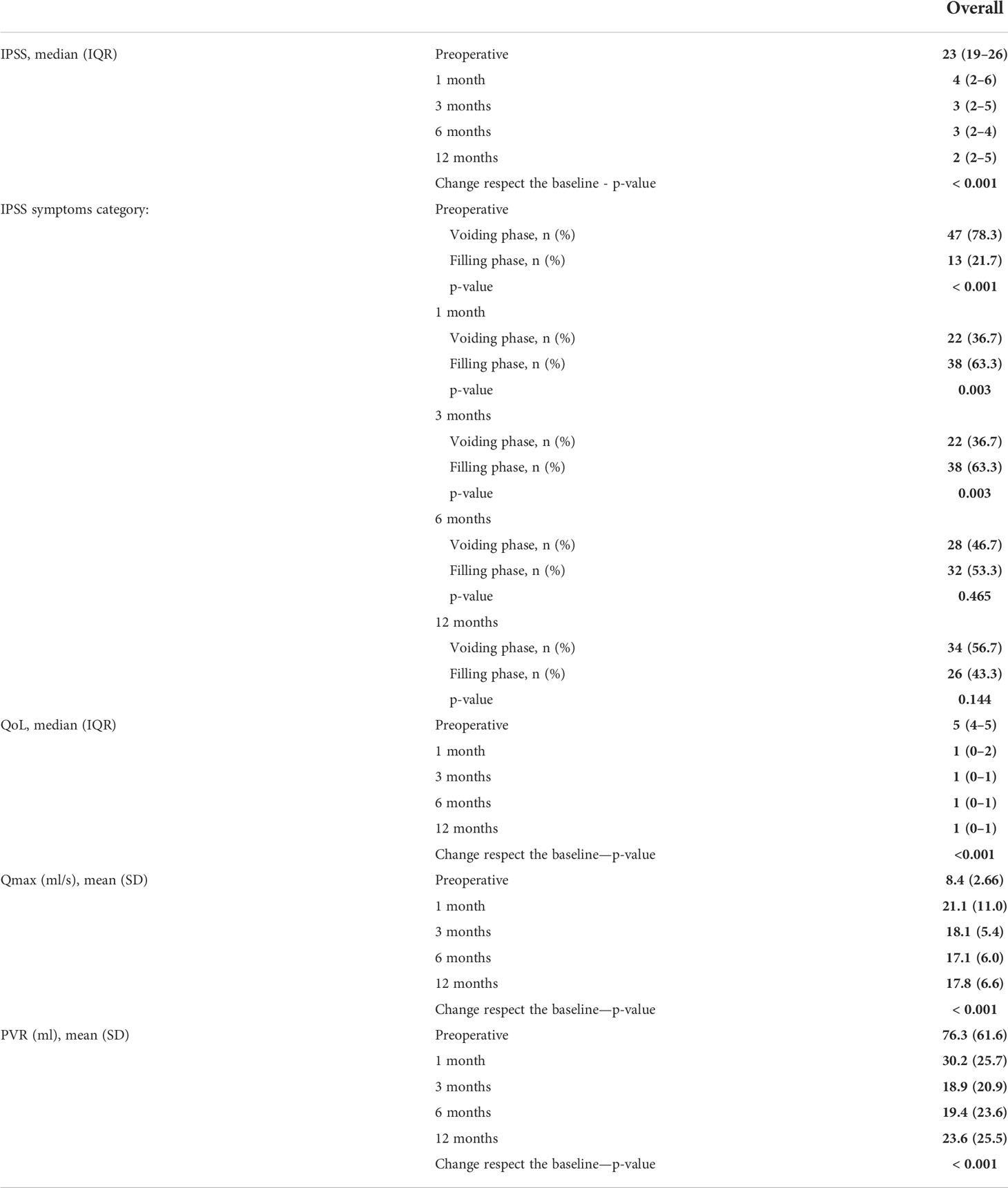
Table 2 Functional outcomes (SD, standard deviation; IQR, interquartile range; Qmax, peak urinary flow; PVR, post void residual; IPSS, International Prostate Symptoms Score; IPSS QoL, International Prostate Symptoms Score Quality of Life; AUR, acute urinary retention).
Analyzing the IPSS symptom category (Table 2), there is a reversal of symptom category prevalence rates between baseline and three months after surgery (p-value of 0.003). Specifically, as might be expected, most patients preoperatively complained more of emptying phase symptoms, whereas at one and three month follow-up after Aquablation, taking into account a significantly decreased total IPSS score, filling phase symptoms were shown to be predominant in almost two-thirds of the study population. Moreover, 27 of 38 (71%) patients with a prevalence of filling phase symptoms at 3 months reported a de novo onset of these symptoms after surgery. This portion of patients accounted for 45% (27/60) of the total study population. The difference in prevalence between symptom categories flattens out at longer time points, not reaching significance at 6- and 12-month follow-up.
Discussion
The present prospective single-arm study demonstrates that Aquablation is a safe and effective procedure for the treatment of BPH related LUTS.
Although this was the first clinical experience with this technology for our institution, the postoperative complication rate is consistent with data published in the literature for Aquabeam and other minimally or ultra-minimally invasive procedures (9, 17, 18). In addition, 1-year efficacy is demonstrated with a statistically significant improvement in urinary symptoms, quality of life, and uroflowmetry from baseline.
Nevertheless, when analyzing in detail the LUTS reported by patients in the postoperative period, a high prevalence of filling phase LUTS was found at 1 and 3 months after surgery. Seventy-one percent of patients with a higher prevalence of filling phase LUTS reported a de novo occurrence of these symptoms.
Despite the considerable burden that BPH exerts on public health, clinical research is still unable to offer an ideal treatment that meets the needs of both clinicians and patients.
In the current ‘gold standard’ surgical treatment for BPH, TURP, in 5%–35% of cases, may be followed by a persistence or de novo onset of bothersome LUTS (5), an occurrence that has a great impact on both the quality of life and public health of the patient (19).
Studies have been performed to assess the permanence or onset of de novo LUTS after surgery performed with new techniques for BPH surgeries in comparisons with TURP. Differences were found mainly in the case of laser enucleative techniques, which demonstrated a higher prevalence of filling phase LUTS than TURP in the immediate postoperative period. In a prospective, randomized controlled trial, authors compared 10-year, long-term results of TURP, contact laser prostatectomy, and photoselective vaporization of the prostate (20). No differences were found between the techniques in terms of efficacy and success rate, but patients who underwent HoLEP reported a higher rate of filling phase LUTS than TURP 1 month after surgery.
Despite it seeming logical to think that the administration of medical therapy for BPH (AB, 5-ARI, AC, and B3A) may provide further improvement in post-surgery LUTS, consensus about the actual benefit of pharmaco-therapy after BPH surgery is lacking (21, 22). As a result of these discordant data in the literature, there are no recommendations from the European Association of Urology (EAU) to guide the urologist on the use of drug therapy following surgical treatment for BPH. For all these reasons, patients should be thoroughly evaluated before undergoing surgery and, above all, properly informed about the risk of persistence or onset of de novo postoperative LUTS.
In this study, Aquablation demonstrated a low prevalence of bothersome postoperative LUTS, as evidenced by the postoperative IPSS score and IPSS QoL. Nevertheless, patients reported a prevalence of filling phase symptoms in the 3 months following the surgical procedure, accounting for 45% (27/60) of all the study population to be de novo filling phase symptoms.
These data are of primary interest to the clinician and patient, as urgency and nocturia have been referred to as the symptoms that most impair quality of life in LUTS patients (23).
Of note, these symptoms were self-limited and of medium durability, reverting to the rates of symptoms of the emptying phase at 6 months after surgery.
The pathophysiology of the development or persistence of LUTS following surgical therapy for BPH is a heterogeneous and unclear field; beyond the pre-surgical presence of overactive bladder syndrome or detrusor underactivity, the persistence of LUTS after BPH-surgery could be the result of a hypoxic insult (24), changes in neuroplasticity (25), progressive detrusor hypertrophy (26), and most importantly, it is still unclear how different energy sources and surgical techniques may affect the development of these symptoms.
Further studies are therefore needed to fully address the cause–effect relationship and allow the choice of the best surgical approach for each patient.
This study is not devoid of limitations. Firstly, the single-arm design of the study does not allow direct comparison with other surgeries for BPH or “sham,” limiting the strength of our findings.
Secondly, the duration of follow-up is short. Recruitment of patients to this study is still on-going and a longer follow-up will ensue to evaluate the efficacy and durability of the procedure.
Lastly, the lack of data from the urodynamic study may not allow the correct evaluation of the postoperative results. However, there is evidence that there is a low correlation between LUTS reported in the postoperative period and urodynamic examination results. Additionally, preoperative urodynamic investigation in patients with LUTS/BPH is only recommended by the EAU in selected cases, which were not included in our study population.
Conclusions
Aquablation is a safe and effective procedure for treating BPH related LUTS, with good urinary outcomes up to 1-year follow-up. LUTS of the filling phase were more prevalent than voiding phase ones in the first 3 months following surgery, but showed a self-limited fashion.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
This study was reviewed and approved by the Comitato Etico Interaziendale San Luigi Gonzaga. The patients/participants provided their written informed consent to participate in this study.
Author contributions
Protocol/project development: FrP, SDL, EC, DA, and SDC. Data collection or management: MS, AQ, and MO. Data analysis: SDC, AQ, FeP, AP, and GV. Manuscript writing/editing: SDC, DA, and EC. Supervision: FrP, CF, MD, MM, and SDL. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Epidemiology of clinical benign prostatic hyperplasia. Asian J Urol (2017) 4:148–51. doi: 10.1016/j.ajur.2017.06.004
2. Cornu J-N, Ahyai S, Bachmann A, de la Rosette J, Gilling P, Gratzke C, et al. A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: An update. Eur Urol (2015) 67:1066–96. doi: 10.1016/j.eururo.2014.06.017
3. Alexander CE, Scullion MM, Omar MI, Yuan Y, Mamoulakis C, N’Dow JM, et al. Bipolar versus monopolar transurethral resection of the prostate for lower urinary tract symptoms secondary to benign prostatic obstruction. Cochrane Database Syst Rev (2019) 12:CD009629. doi: 10.1002/14651858.CD009629.pub4
4. Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP)–incidence, management, and prevention. Eur Urol (2006) 50:969–79. doi: 10.1016/j.eururo.2005.12.042
5. Nitti VW, Kim Y, Combs AJ. Voiding dysfunction following transurethral resection of the prostate: symptoms and urodynamic findings. J Urol (1997) 157:600–3. doi: 10.1016/S0022-5347(01)65214-5
6. Chughtai B, Simma-Chiang V, Kaplan SA. Evaluation and management of post-transurethral resection of the prostate lower urinary tract symptoms. Curr Urol Rep (2014) 15:434. doi: 10.1007/s11934-014-0434-1
7. Rapisarda S, Russo GI, Osman NI, Chapple CR, Morgia G, Tubaro A, et al. The use of laser as a therapeutic modality as compared to TURP for the small prostate ≤40 mL: A collaborative review. Minerva Urol Nefrol (2019) 71:569–75. doi: 10.23736/S0393-2249.19.03350-2
8. Reale G, Marchioni M, Altieri V, Greco F, De Nunzio C, Destefanis P, et al. Operative profile, safety and functional outcomes after GreenLight laser prostate surgery: Results from a 12 months follow-up multicenter Italian cohort analyses. Minerva Urol Nefrol (2020) 72:622–8. doi: 10.23736/S0393-2249.20.03597-3
9. Porpiglia F, Checcucci E, Amparore D, Niculescu G, Volpi G, Piramide F, et al. Urethral-sparing robot-assisted simple prostatectomy: An innovative technique to preserve ejaculatory function overcoming the limitation of the standard millin approach. Eur Urol (2021) 80:222–33. doi: 10.1016/j.eururo.2020.09.028
10. Fiori C, De Cillis S, Volpi G, Checcucci E, Cattaneo G, Meziere J, et al. iTIND for BPH: Technique and procedural outcomes: A narrative review of current literature. Turkish J Urol (2021) 47:470–81. doi: 10.5152/tud.2021.21145
11. Jung JH, Reddy B, McCutcheon KA, Borofsky M, Narayan V, Kim MH, et al. Prostatic urethral lift for the treatment of lower urinary tract symptoms in men with benign prostatic hyperplasia. Cochrane Database Syst Rev (2019) 5:CD012832. doi: 10.1002/14651858.CD012832.pub2
12. Manfredi C, Arcaniolo D, Spatafora P, Crocerossa F, Fusco F, Verze P, et al. Emerging minimally invasive transurethral treatments for benign prostatic hyperplasia: A systematic review with meta-analysis of functional outcomes and description of complications. Minerva Urol Nephrol (2022) 74:389–99. doi: 10.23736/S2724-6051.21.04530-4
13. Fiori C, Checcucci E, Gilling P, Amparore D, Volpi G, De Cillis S, et al. All you need to know about “Aquablation” procedure for treatment of benign prostatic obstruction. Minerva Urol e Nefrol (2020) 72:152–61. doi: 10.23736/S0393-2249.20.03654-1
14. Gilling P, Barber N, Bidair M, Anderson P, Sutton M, Aho T, et al. WATER: A double-blind, randomized, controlled trial of aquablation® vs transurethral resection of the prostate in benign prostatic hyperplasia. J Urol (2018) 199:1252–61. doi: 10.1016/j.juro.2017.12.065
15. Nguyen D-D, Misraï V, Bach T, Bhojani N, Lingeman JE, Elterman DS, et al. Operative time comparison of aquablation, greenlight PVP, ThuLEP, GreenLEP, and HoLEP. World J Urol (2020) 38:3227–33. doi: 10.1007/s00345-020-03137-8
16. Gilling P, Barber N, Bidair M, Anderson P, Sutton M, Aho T, et al. Three-year outcomes after aquablation therapy compared to TURP: Results from a blinded randomized trial. Can J Urol (2020) 27:10072–9.
17. Sadri I, Arezki A, Couture F, Nguyen D-D, Schwartz R, Zakaria AS, et al. Reasons to overthrow TURP: Bring on aquablation. World J Urol (2021) 39:2291–9. doi: 10.1007/s00345-020-03390-x
18. Checcucci E, Veccia A, De Cillis S, Piramide F, Volpi G, Amparore D, et al. New ultra-minimally invasive surgical treatment for benign prostatic hyperplasia: A systematic review and analysis of comparative outcomes. Eur Urol Open Sci (2021) 33:28–41. doi: 10.1016/j.euros.2021.08.009
19. Yim PWC, Wang W, Jiang Y, Zakir HAS, Toh PC, Lopez V, et al. Health-related quality of life, psychological well-being, and sexual function in patients with benign prostatic hyperplasia after prostatic surgery. Appl Nurs Res (2015) 28:274–80. doi: 10.1016/j.apnr.2015.02.007
20. Hoekstra RJ, Van Melick HHE, Kok ET, Ruud Bosch JLH. A 10-year follow-up after transurethral resection of the prostate, contact laser prostatectomy and electrovaporization in men with benign prostatic hyperplasia; long-term results of a randomized controlled trial. BJU Int (2010) 106:822–6. doi: 10.1111/j.1464-410X.2010.09229.x
21. Tehranchi A, Rezaei Y, Shojaee R. Tolterodine to relieve urinary symptoms following transurethral resection of the prostate: a double-blind placebo-controlled randomized clinical trial. Korean J Urol (2014) 55:260–4. doi: 10.4111/kju.2014.55.4.260
22. Campbell J, Reid J, Ordon M, Welk B. The utilization of benign prostatic hyperplasia and bladder-related medications after a transurethral prostatectomy. Urology (2019) 130:126–31. doi: 10.1016/j.urology.2019.05.003
23. Irwin DE, Milsom I, Kopp Z, Abrams P, Artibani W, Herschorn S. Prevalence, severity, and symptom bother of lower urinary tract symptoms among men in the EPIC study: Impact of overactive bladder. Eur Urol (2009) 56:14–20. doi: 10.1016/j.eururo.2009.02.026
24. Mirone V, Imbimbo C, Longo N, Fusco F. The detrusor muscle: An innocent victim of bladder outlet obstruction. Eur Urol (2007) 51:57–66. doi: 10.1016/j.eururo.2006.07.050
25. Speakman MJ, Brading AF, Gilpin CJ, Dixon JS, Gilpin SA, Gosling JA. Bladder outflow obstruction–a cause of denervation supersensitivity. J Urol (1987) 138:1461–6. doi: 10.1016/s0022-5347(17)43675-5
Keywords: BPH, Aquablation, robotic surgery, LUTS, minimally-invasive
Citation: De Cillis S, Amparore D, Quarà A, Checcucci E, Piana A, Volpi G, Piramide F, Sica M, Ortenzi M, Manfredi M, Di Dio M, De Luca S, Fiori C, Porpiglia F and on behalf of the ESUT lower Tract group (2022) Evaluation of LUTS of the filling phase after Aquablation: A prospective single center experience. Front. Urol. 2:1001710. doi: 10.3389/fruro.2022.1001710
Received: 23 July 2022; Accepted: 18 August 2022;
Published: 21 September 2022.
Edited by:
Afonso Morgado, Centro Hospitalar Universitário de São João (CHUSJ), PortugalReviewed by:
Diogo Jose Nunes Carneiro, Centro Hospitalar Universitário do Porto, PortugalMargarida Manso, São João University Hospital Center, Portugal
Copyright © 2022 De Cillis, Amparore, Quarà, Checcucci, Piana, Volpi, Piramide, Sica, Ortenzi, Manfredi, Di Dio, De Luca, Fiori, Porpiglia and on behalf of the ESUT lower Tract group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sabrina De Cillis, c2FicmluYXRpdHRpLmRlY2lsbGlzQGdtYWlsLmNvbQ==
†These authors share first authorship