 Mar Hernandez-Martin
Mar Hernandez-Martin Fernando Del Ama Gonzalo
Fernando Del Ama Gonzalo Roberto Alonso González-Lezcano
Roberto Alonso González-Lezcano- 1Department of Architecture and Design, Escuela Politécnica Superior, Universidad San Pablo- CEU, CEU Universities, Montepríncipe Campus, Madrid, Spain
- 2Department of Sustainable Product Design and Architecture, Keene State College, Keene, NH, United States
Indoor environmental quality (IEQ) is an essential topic nowadays due to its direct impact on occupant health and wellbeing. Most research, however, has focused on commercial and workspace typologies, leaving residential buildings underexplored. Importantly, the effects of IEQ are not experienced uniformly across all populations. Age-related changes and cognitive function, in particular, significantly influence how occupants experience indoor environments. This makes infants and older adults and/or with disabilities especially vulnerable. Understanding these parameters is crucial to designing comfortable, healthy, and inclusive buildings for all user profiles. This review aimed to document research on IEQ, particularly concerning vulnerable populations in residential building typologies. The findings revealed how different vulnerable groups (children, elderly people, pregnant women, and people with disabilities) are affected by the main IEQ domains (thermal, air quality, lighting, acoustics). On the one hand, this relationship is essential for adopting healthy habits when using buildings as users, and on the other, for methods, factors, and strategies to consider and apply when designing healthy and inclusive buildings as architects, designers, and engineers. The quality of the indoor environment must be considered throughout the entire life cycle of a building, from decisions in the initial design stages to its maintenance.
1 Introduction
According to recent studies, most people spend approximately 80%–90% of their time indoors (Al horr et al., 2016), so the quality of the interior environment is a topic that has drawn extensive scholarly attention. Recent research aimed at enhancing Indoor Environmental Quality (IEQ) is closely associated with the increasing demand for building rehabilitation across Europe and the imperative to decrease energy consumption while promoting sustainability and efficiency (Anderson et al., 2015). The confluence of these factors highlights the critical need for ongoing investigation into the optimization of indoor environments to meet contemporary ecological and health standards (Soares et al., 2017; Ortiz et al., 2017). However, most studies and research focus on commercial typologies and workspaces, leaving the IEQ in residential buildings understudied (Al horr et al., 2016; Carton et al., 2022). The Association for Media Research (AIMC) estimates that the time spent in houses is around 65% in Spain. This percentage increases to 85% for individuals over 65 and up to 95% for those over 85 (Hughes et al., 2019).
Previous research indicates that the quality of interior environments—including thermal, acoustic, visual, humidity, air quality, odors, and vibrations—significantly impacts the comfort and health of building occupants (Apte, 2000; Wolkoff, 2018; Wu et al., 2023a). Furthermore, the relationship between the occupants’ wellbeing and satisfaction and the interior environmental quality is based on complex parameters. This complexity presents challenges in measurement and can lead to discrepancies affected by contextual factors such as local climate, building typology, and the interior layout of the structures. Additionally, the interplay between occupant wellbeing and satisfaction and the interior environment’s quality is influenced by many parameters, which can be both diverse and complex. While these contextual elements may not be explicitly categorized as determinants of interior environmental quality, they directly influence user comfort, perceptions, and how individuals inhabit and utilize the spaces within buildings (Al horr et al., 2016; Carton et al., 2022).
The quality of the interior environment affects diverse population groups in different ways. Age-related variations are particularly notable, as seen in infants and elderly individuals (Putri et al., 2023). The World Health Organization also identifies other vulnerable groups including people with reduced mobility or disabilities, as well as pregnant women. These considerations highlight how interior environments interact uniquely with the specific needs and conditions of each group.
Allab et al. (2017), Dias Pereira et al. (2017), and Zuhaib et al. (2018) addressed IEQ issues related to building energy efficiency or performance, user needs, and design strategies (Šujanová et al., 2019). Usually, only one of the aspects or parameters defining the quality of the interior environment is analyzed (Ortiz et al., 2017; Bluyssen, 2010). Understanding these parameters is essential to designing comfortable, healthy, and inclusive buildings for all user profiles. In addition, according to the WHO, healthy buildings must adapt to the future and, therefore, be protected under the now more latent criteria of sustainability, efficiency, and low consumption and cost without damaging the surrounding environment (Šujanová et al., 2019; Bluyssen, 2010).
However, the behavior of the occupants inside these buildings sometimes conflicts with the strategies designed for low energy consumption. To effectively adapt to future requirements, people’s needs must be balanced with IEQ parameters (general comfort, energy efficiency, building design, and climate control), also called quality of life indicators (Bluyssen, 2010). Thus, a three-level connection is related, as Figure 1 shows (Šujanová et al., 2019).
Figure 1. Three-level connection for efficient building design.
Besides IEQ domains, psychological and physiological aspects related to the wellbeing of occupants influence the overall perception of comfort. All of these domains must be considered to achieve the right quality of the interior environment (Bluyssen, 2010). As relevant studies show, physiological and psychological domains, such as the intrinsic characteristics of each occupant, the age range (Zalejska-Jonsson and Wilhelmsson, 2013; Frontczak et al., 2012; Chiang et al., 2001), sociocultural conditions, and the type of space (Frontczak et al., 2012; Heinzerling et al., 2013) (19) are important when evaluating IEQ and its impact. However, defining these domains can be difficult, as specific criteria for different user profiles may not always be known or considered (Bluyssen, 2010). Recent studies highlight the importance of adopting multi-domains approaches, as comfort cannot be fully understood by isolating individual parameters and factors. Instead, the interactions between IEQ domains (thermal, visual, acoustic and air quality), combined with psychological and physiological dimensions, provide a more comprehensive framework for assessing occupant wellbeing (Schweiker et al., 2020).
It is essential to consider not only all factors, but also the capacity for adaptation to change, and above all, the time frame in which it occurs, as this will be decisive. Even if actions with less impact and lower energy consumption are implemented, occupants’ behaviour and their adaptation will be uncertain, influenced by actions such as (Šujanová et al., 2019; Coccolo et al., 2016; Gunay et al., 2013):
- behavioural adjustments (change in habits or tolerance limits).
- physicals responses (level of activity, clothing use and environmental conditions)
- psychological adaptations, shaped by individual sensations and perceptions.
These actions may occur consciously, in the first case; subconsciously, in the second case, or automatically by the peripheral nervous system, in the last case.
The number of occupants in a space is another aspect to consider when measuring the IEQ. A higher occupancy can lead to increased indoor air pollution. Additionally, the interior air quality can be affected by the construction materials used and the types of equipment present within the building (Al horr et al., 2016; Bakó-Biró et al., 2004). It is, therefore, essential to accurately assess both space occupation and interior pollutants. Numerous researchers studied various types of public buildings, such as offices (Kong et al., 2022), schools (Wu et al., 2023b; Tao et al., 2022), shopping centers (Deng et al., 2022), hotels (Xu et al., 2022a; Xu et al., 2022b) and nursing homes (Wang et al., 2022). These studies have used a variety of methods, including field measurements, simulations, behavioral observations, questionnaires, and interviews, as well as tools such as virtual reality (VR) and electroencephalography (EEG) (Wu et al., 2023a). However, the relationship between the objective aspects and the perception of the environment remains unclear and undefined. There is often a discrepancy between actual conditions and how user profiles respond to or evaluate their environment (Bluyssen, 2010).
The WHO confirms that approximately a quarter of the diseases around the world are due to modifiable environmental factors (Šujanová et al., 2019). Many studies have confirmed that the quality of the interior environment is correlated with diseases, such as cardiovascular, respiratory, and reproductive conditions, which are visible both in the short and long term (Al horr et al., 2016; Wu et al., 2023a; Bluyssen, 2010; Houtman et al., 2008; Fisk et al., 2007). Assessing diseases and discomfort among different populations, particularly vulnerable individuals, is crucial for understanding their relationship with IEQ domains (Bluyssen, 2010). Air pollution occurs due to factors such as the presence of mold, dust, mites, allergens, indoor aldehydes, volatile organic compounds (VOC), airborne fungi, pesticides, tobacco smoke, lighting, air exchange or circulation rates, carbon monoxide, carbon dioxide. These elements can lead to respiratory health issues (Al horr et al., 2016; Takigawa et al., 2009). Mechanical ventilation, as opposed to natural ventilation in buildings, may increase the incidence of diseases by 30%–200%, resulting in more hospital visits, particularly among women (Al horr et al., 2016; Preziosi et al., 2004).
Sick Building Syndrome (SBS) comprises a group of health issues caused by the indoor environment of a building (Al horr et al., 2016; Takigawa et al., 2009; De Dear and Brager, 2002). Various factors contribute to SBS, including temperature, humidity, chemical and biological contamination, and physical condition and psychosocial status of the occupants (Simonson et al., 2002; Wang et al., 2007; Wolkoff and Kjærgaard, 2007; Stolwijk, 1991). People experiencing SBS can suffer eye, nose, and throat irritation, headache, cough, wheezing, cognitive disorders, depression, sensitivity to light, gastrointestinal upset, fatigue, and similar to those of the flu (Šujanová et al., 2019; WHO, 1983; Mendell and Smith, 1990).
High exposure to poorly ventilated interior spaces or areas with airborne pollutants, such as s soil fungal concentrations due to high humidity (Redd, 2002) or dust in chairs, is often associated with allergies, irritation of lung functions, asthma, and pneumonitis (Al horr et al., 2016; Redd, 2002; Fisk et al., 2007). These health issues, along with poisoning, are closely linked to indoor air quality, which is one of the leading contributors to health-related deaths (Šujanová et al., 2019; Franchi et al., 2006; WHO, 2017). The severity of these diseases depends on the intensity, duration, and source of harmful exposure (Šujanová et al., 2019). Prolonged exposure to poor Indoor Air Quality (IAQ) can lead to serious illnesses like legionellosis and CO poisoning. Although symptoms like asthma, cough, and pulmonary infiltration may appear after brief exposure, they can become chronic and acute respiratory diseases. Many of these conditions can be avoided with proper indoor air quality management (Franchi et al., 2006).
Beyond air quality, other environmental domains also have measurable health impacts. High noise levels can cause cardiovascular risks and hypertension (Šujanová et al., 2019). In addition, heart rate variability has been related to indoor air temperature and may be a predictor of mortality (Bluyssen, 2010). Thermal comfort, air quality, and noise collectively influence not only health but also concentration, and motivation (Šujanová et al., 2019; Kallio et al., 2020). For example, increased temperatures can elevate the concentration of harmful substances in the air from the devices, relating temperature dependence to indoor air quality or ventilation (Šujanová et al., 2019). On the other hand, poor ventilation or fungal concentration can also cause fatigue (Šujanová et al., 2019; Redd, 2002). High humidity worsens the quality of sleep (Wolkoff, 2018).
Lighting conditions are equally critical. Inadequate lighting disrupts sleep quality and circadian rhythms, causing discomfort throughout the day (Šujanová et al., 2019; Chang and Chen, 2005). The effects of poor lighting can vary based on gender, age, and the time of year (Serghides et al., 2015). Similarly, poor acoustic environments are associated with insomnia and alter sleep patterns (Šujanová et al., 2019), particularly among the elderly (Putri et al., 2023). High noise levels, their frequency, and sound pressure differences cause discomfort in people (Landström et al., 1995). A deficit in the optimization of indoor acoustics not only affects cognitive decline in hearing but also causes distractions, irritability, stress, discomfort, and fatigue (Al horr et al., 2016); Šujanová et al., 2019; Passero and Zannin, 2012). It can even affect the development of learning disorders, such as dyslexia or voice problems (Bottalico and Astolfi, 2012).
This systematic review aims to identify key factors affecting building environmental quality in residential buildings and their impact on different vulnerability groups. The study also examines how sensory perception, cognitive function, and building design and operation interact with building environmental quality in vulnerable people.
This review addresses vulnerable groups from an age-related perspective, considering the elderly and children as classifications recognised by the World Health Organisation. However, other vulnerable groups, such as pregnant women and people with disabilities, are also mentioned. This classification is not addressed from a socio-economic perspective or based on housing characteristics, which could be another way of classifying vulnerable groups.
2 Methodology
This literature review aimed to document the key research and theories linking IEQ to design, focusing on the most vulnerable occupants in residential building typologies.
2.1 Initial literature search
This research began with an initial bibliographic search. Since the main objective of the study was to analyse the impact of IEQ on the health and wellbeing of vulnerable occupants in residential buildings, the keywords used for the search were related to this, in addition to wellbeing buildings.
The following multiple chains were used, taking into account both IEQ in residential buildings in general and in vulnerable groups:
(“Indoor Environmental Quality” OR IEQ);
(“Indoor Environmental Quality” OR IEQ) AND (residen*);
(“Indoor Environmental Quality” OR IEQ) AND (pregnan* OR baby OR babies OR child* OR infant);
(“Indoor Environmental Quality” OR IEQ) AND (elder*);
(“Indoor Environmental Quality” OR IEQ) AND (vulnerab*);
(“Indoor Environmental Quality” OR IEQ) AND (disab*);
(Acoustic) AND (indoor) AND (residen*);
(IAQ) AND (residen*);
(“thermal comfort”) AND (indoor) AND (residen*);
(“visual comfort”) AND (indoor) AND (residen*)
Thus, an initial and rapid analysis using the Scopus search engine revealed the main trends and gaps, as well as areas that have been little explored.
It is important to recognize that the preliminary analysis has certain limitations, as the database used was not subjected to a rigorous selection process. Furthermore, the large volume of contributions prevented a thorough verification of the consistency of the dataset with the established search criteria.
The bibliography was then analysed using this data, revealing the results shown in the following figures:
Figure 2 illustrates the literature gap over time between the frequency with which the term IEQ is used in all articles versus its use alongside other terms intended for vulnerable groups, such as the elderly. Another important aspect is the comparison between all articles on IEQ and those that focus only in residential buildings. Figure 3 shows that, in the residential sector, publications with a separate domains predominate rather than considering IEQ as a whole. It can also be seen that the frequency of publications increased after the pandemic.
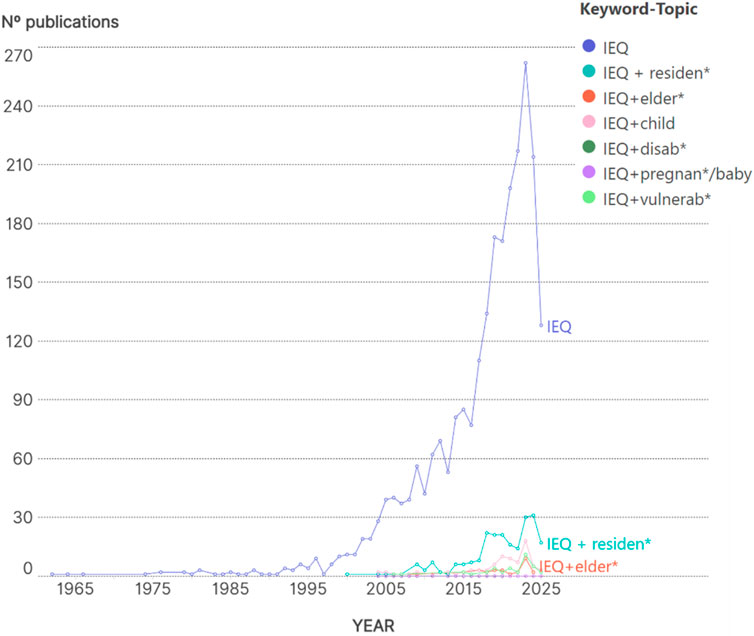
Figure 2. Frequency of articles from different decades, about the increment of IEQ versus the IEQ with different vulnerability groups.
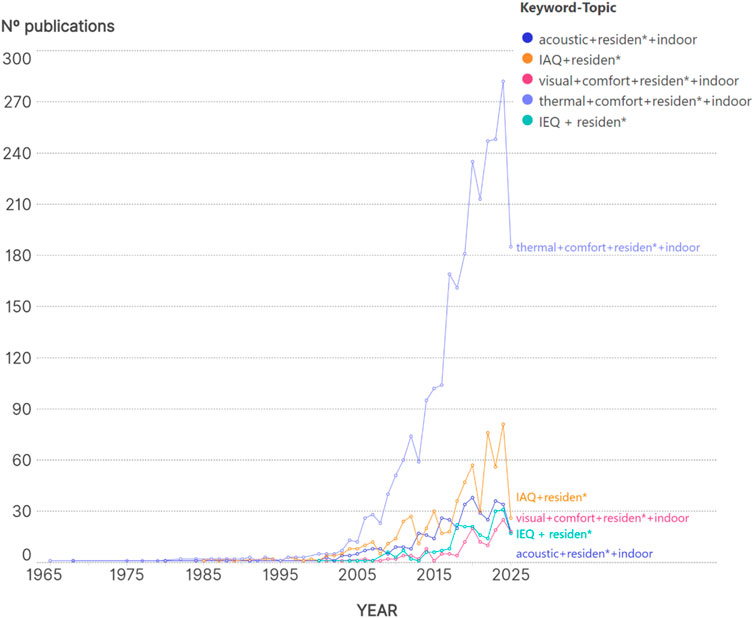
Figure 3. Frequency of articles from different decades since 1970, about the increment of IEQ domains in an individual mode versus the IEQ as a whole concept, in the residential typology.
All this information is important for future research to take into account.
Next, Figure 4 shows that when the articles are broken down by domains, the frequency of articles in their entirety (yellow) is compared to existing research on vulnerable groups by domains and on IEQ as a single concept, which is minimal. Zooming in reveals that the effect of each domain is studied more in isolation than as a whole in terms of IEQ.
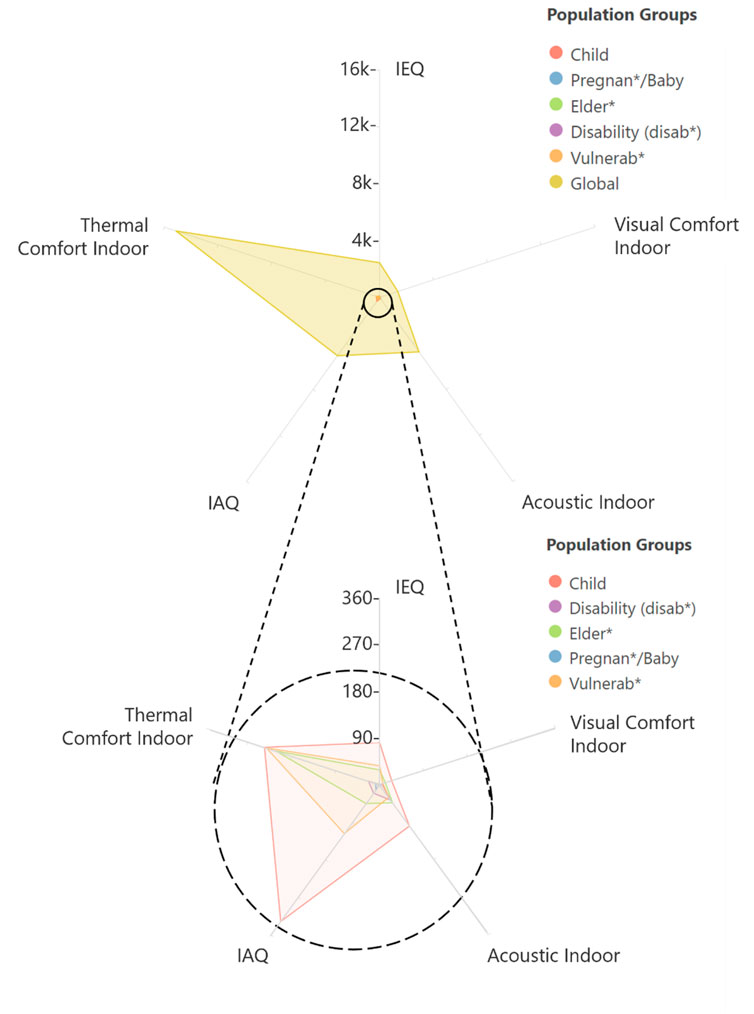
Figure 4. The overall impact of the IEQ issue is depicted, with the vulnerable groups barely visible. The frequency of items per IEQ domain is shown for each vulnerability group.
Geographically, the highest scientific output for both IEQ and each domain is concentrated in countries such as the US and China. In contrast, European countries have experienced more limited development in these areas and have tended to study the domains more separately, as illustrated in Figure 5.
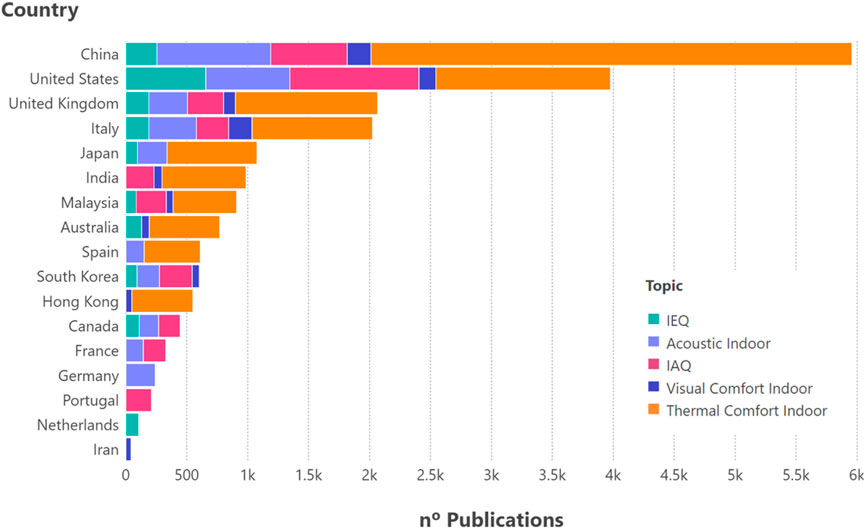
Figure 5. The frequency of articles per country is shown for both the IEQ and the individual domains that comprise it.
Finally, as illustrated in Figure 6, the five most influential authors per topic were identified in this initial search, many of whom are referenced in the bibliography.
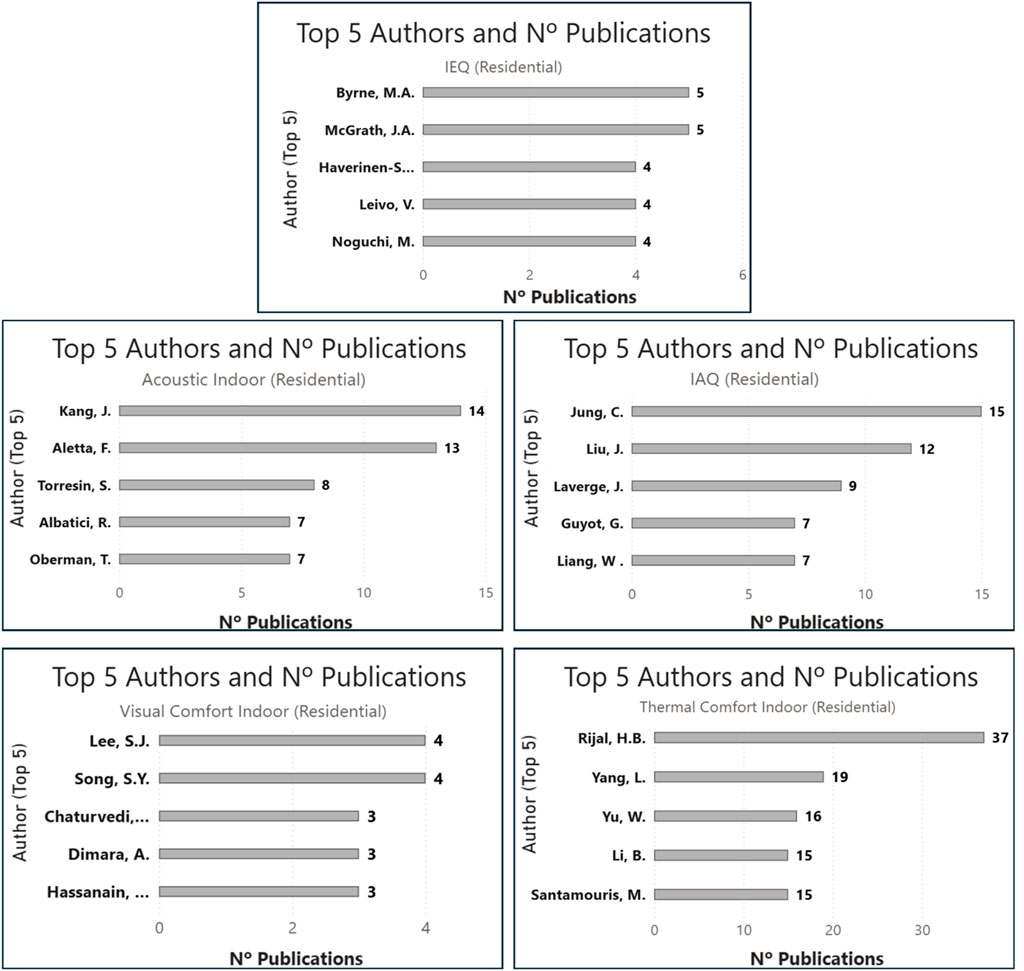
Figure 6. Authors with the most publications on IEQ in the residential sector by IEQ domain.
2.2 In-depth literature search and classification
Following the initial phase, the methodological structure of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram was adopted to systematically address, in a deeper way, this literature, identifying, evaluating and synthesising the available scientific evidence on the topic addressed in this review.
To this end, the Scopus and Web of Science scientific databases were consulted within the time range of 2000–2025.
In the context of this review, combinations of controlled terms were used alongside Boolean operators and search methods such as (*) to obtain additional words from semantic roots.
The relevant records were exported to an Excel spreadsheet for screening, in order to identify the most relevant publications.
The following inclusion and exclusion criteria were applied:
The inclusion criteria were: that there should be at least one IEQ domain—or IEQ as an overall concept—in addition to taking vulnerable groups into account, and even that it should be indoors or in a residential environment.
The following procedure was used to search for keywords in both databases, as we did in the initial search, using the same strings expressed in section 2.1.
Hoewer, this time, the exclusion criteria were: a language other than English, full text not available, main focus on medical aspects not related to IEQ (transplants, molecular studies, pharmacology, etc.) (not medicine, not transplantation, not molecules, not pacreat* not surgery not biology not cell not molecular not protein not physical not chemical), research related to an activity such as in hospitals, schools or offices, when the objective was to evaluate the functioning of the facility and not the impact on the health or wellbeing of the occupants. Also, studies that were not relevant or did not explicitly evaluate these issues.
Although this review primarily focuses on housing, it also includes articles related to schools, care facilities and offices, in order to determine symptoms and conditions, as well as important thresholds for different vulnerable groups.
Finally, the most impactful and frequently cited articles from high-quality, high-impact journals were read and included.
This review includes 138 references divided into database and grey literature.
The entire process is documented using the PRISMA diagram shown in Figure 7.
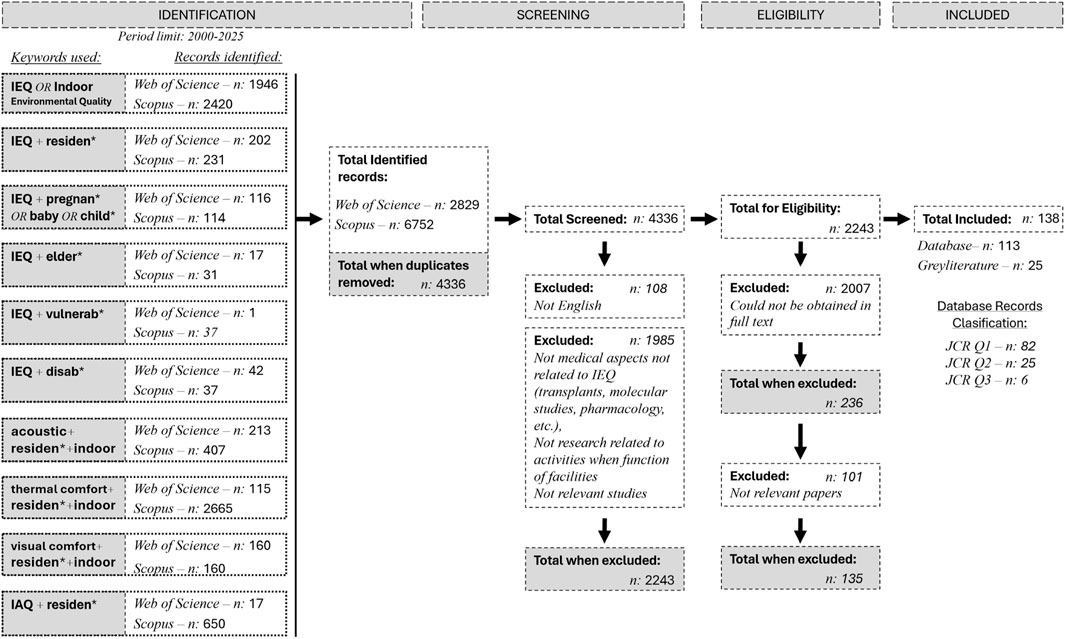
Figure 7. PRISMA Diagram of the methodology followed in the selection of scientific literature.
The final step of the process was the analysis of the downloaded papers, which allowed us to categorize the findings into specific thematic areas such as IEQ in the residential sector, air quality in the residential sector, indoor visual comfort in the residential sector, thermal comfort in the residential sector and acoustics in the residential sector.
Following the presentation of these sections, the authors address the main issues that can affect building design. Given the recent proliferation of healthy building design initiatives and the use of healthy building guidelines around the world, the discussion helps readers to establish a link between health and wellness parameters and the domains included in healthy building guidelines.
This systematisation made it possible to identify patterns, trends and areas that have been little explored in the literature, providing a solid basis for discussion and justification of the research.
In addition to taking into account the high impact of the journals analysed, the origin of the references used was also considered, which analyses the geographical framework of the research used. This distribution is shown in Figure 8, where the United States, China, and central European countries predominate.
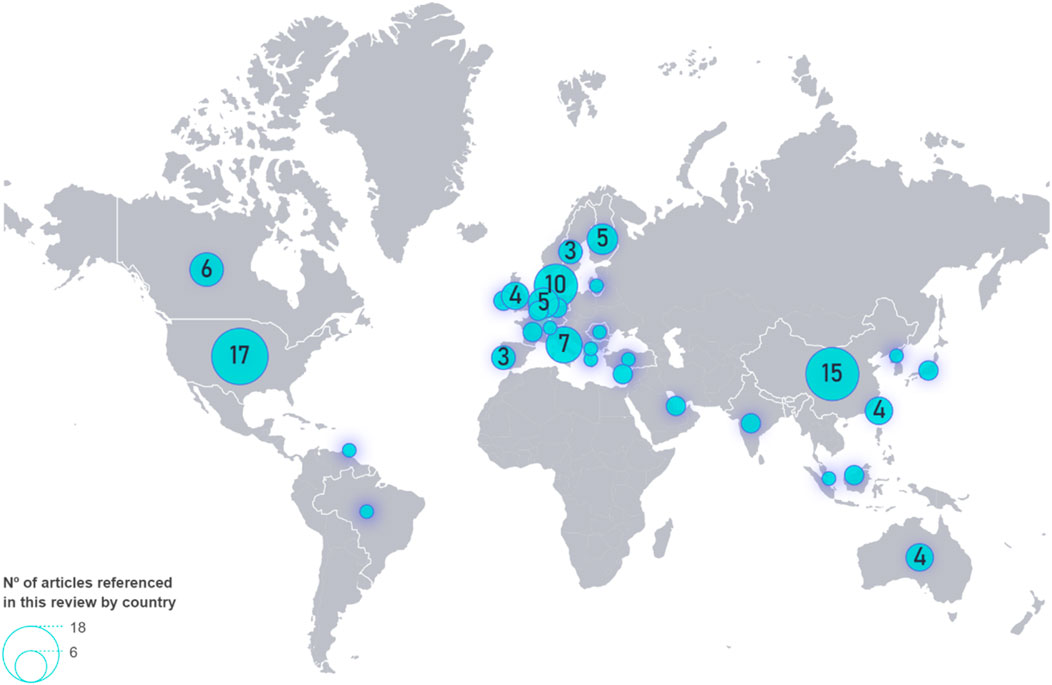
Figure 8. Geographical distribution of references used (database) in this review.
3 State of the art of the research on thermal comfort
Thermal comfort directly impacts buildings’ energy consumption. Over 60% of a building’s energy consumption is used for heating and cooling a space (Šujanová et al., 2019). Even a slight feeling of discomfort can lead users to adjust the controls to suboptimal levels (Al horr et al., 2016; Catalina and Iordache, 2012; Corgnati et al., 2009).
3.1 Thermal comfort and people’s wellbeing: sensitivity to thermal conditions, preferred temperatures, adaptability and perception of thermal comfort
Thermal comfort can be defined depending on more specific patterns known as climate, geographic location, the design typology of the building, and the time of year, which are determined using air temperature, radiant temperature, relative humidity, and the speed of the air (Al horr et al., 2016; Šujanová et al., 2019; Frontczak and Wargocki, 2011). Beyond these parameters, the most important and variable element is personal thermal adaptation theory, which relies on behavioral, psychological, and physiological aspects (Zhou et al., 2023). The assessment of those parameters includes habits and behaviors, as well as intrinsic characteristics of the individual, such as gender, race, and age (Al horr et al., 2016; Quang et al., 2014), along with metabolic rates (activity levels) and insulation provided by clothing (Clo value) (Šujanová et al., 2019; Katafygiotou and Serghides, 2015). Four environmental variables are also assessed: air temperature, air speed, humidity, and radiant temperature. The most recurring method for measuring thermal comfort is Fanger’s PMV-PPD model, using metrics either by expected average vote (PMV) or by the expected percentage of dissatisfaction (PPD), which depends on user responses (Hughes et al., 2019; Zhou et al., 2023; Ole Fanger and Toftum, 2002; Papadopoulos et al., 2008).
Physiologically, temperature perception is detected by cutaneous sensory fibers, which respond to cold and heat. Cold perception is felt at temperatures ranging from 17 °C to 34 °C, whereas heat receptors are activated from 33 °C to 46 °C. The point that is considered neutral is a temperature of 32 °C. Temperatures below 17 °C and above 46 °C are considered harmful if there is a long time exposure. The maximum sun exposure is 3,500 W/m2 (Šujanová et al., 2019).
Regarding body temperature, human bodies stay around 37 °C through the heat exchange from the human body and the environment through radiation, convection, and evaporation, as explained in ASHRAE 55. These regulations, together with ISO 7730 (1994) and ISO 17772-1, define thermal comfort and serve as a reference for the design of buildings worldwide (Al horr et al., 2016) (Šujanová et al., 2019). If body temperature exceeds 40 °C, there would be a risk of heart attack, and below 35 °C, there would be a risk of hypothermia (Šujanová et al., 2019; Noonan et al., 2012). Adjustments to thermal factors generally produce slow physiological responses, and their effects tend to manifest over the long term (Šujanová et al., 2019).
3.2 Effect of hygrothermal variables on age, gender and disability
Hygrometric variables are among the key factors that influence user perceptions based on gender and age (Smolander, 2002; Nicol and Humphreys, 2002). As the body undergoes physiological changes over the years, it adapts to different thermal conditions. A weak self-regulation of thermal comfort (thermoregulation) is observed, resulting in less precision in assessing comfort levels. Consequently, older adults tend to have a broader range of comfort temperatures than young adults. Studies indicate that older individuals demonstrate lower thermal sensitivity, especially in cold environments. A primary factor driving these age-related differences is the metabolic rate, typically 5%–30% slower in older adults than in sedentary young adults (40.6–55.1 W/m2) due to loss of muscle tissue and neurological changes. Besides, older adults commonly experience a decrease in body temperature and an increase in body fat and overall weight, which enhances the body’s thermal insulation.
As a consequence, the elderly produce less metabolic heat, resulting in a lower heart rate and cardiac output—between 3.4% and 40% less than that in young adults and, therefore, a slower response to cold. The thresholds for the start of vasodilation and sweating are also different, as they approach 0.5 °C and 0.21 °C, respectively. Due to these differences, sweating begins at higher temperatures due to reduced sweat secretion rate, and tremors or chills occur at lower temperatures due to less effective peripheral vasoconstriction. When evaluating this parameter, other behavioral and psychological aspects must be considered (Zhou et al., 2023).
These age-related changes in thermal perception have significant health implications. Older adults may not adequately adapt to their environment, increasing their vulnerability to cold and related health risks, such as arthritis, respiratory conditions as lung diseases, and even higher mortality rates. The WHO recommends a temperature of 18 °C in rooms. However, if the occupants are older, the recommended temperature rises to 20 °C–21 °C (Hughes et al., 2019). In the case of infants, there is a lack of emphasis on thermal comfort, so the space is adapted for the comfort of a young adult. On the other hand, infants spend their time at a lower height and are more vulnerable to diseases like influenza because their immune system is not fully developed. The space temperature must be set at 26 °C–28 °C in summer and 20 °C–23 °C in winter, with a humidity of 60% for optimal health outcomes for this demographic (Genjo, 2022).
In the thermal comfort domain, as shown in Table 1, the literature focus on established metrics and standards, such as ASHRAE 55, and on reviewing approaches to energy efficiency and wellbeing. Though energy consumption and sustainability have been linked to thermal comfort through a multitude of studies, still remains a normative and generalist view that address contextual variations or the specific needs of different environments and housing types. Moreover, although advances have been made in incorporating psychological and social aspects, studies remain fragmented and limited in terms of the diversity of populations analysed, especially vulnerable groups such as children and older adults. It is evident that there is a clear need for more research should connect standardised metrics with physiological and psychological parameters that have yet to be fully explored.
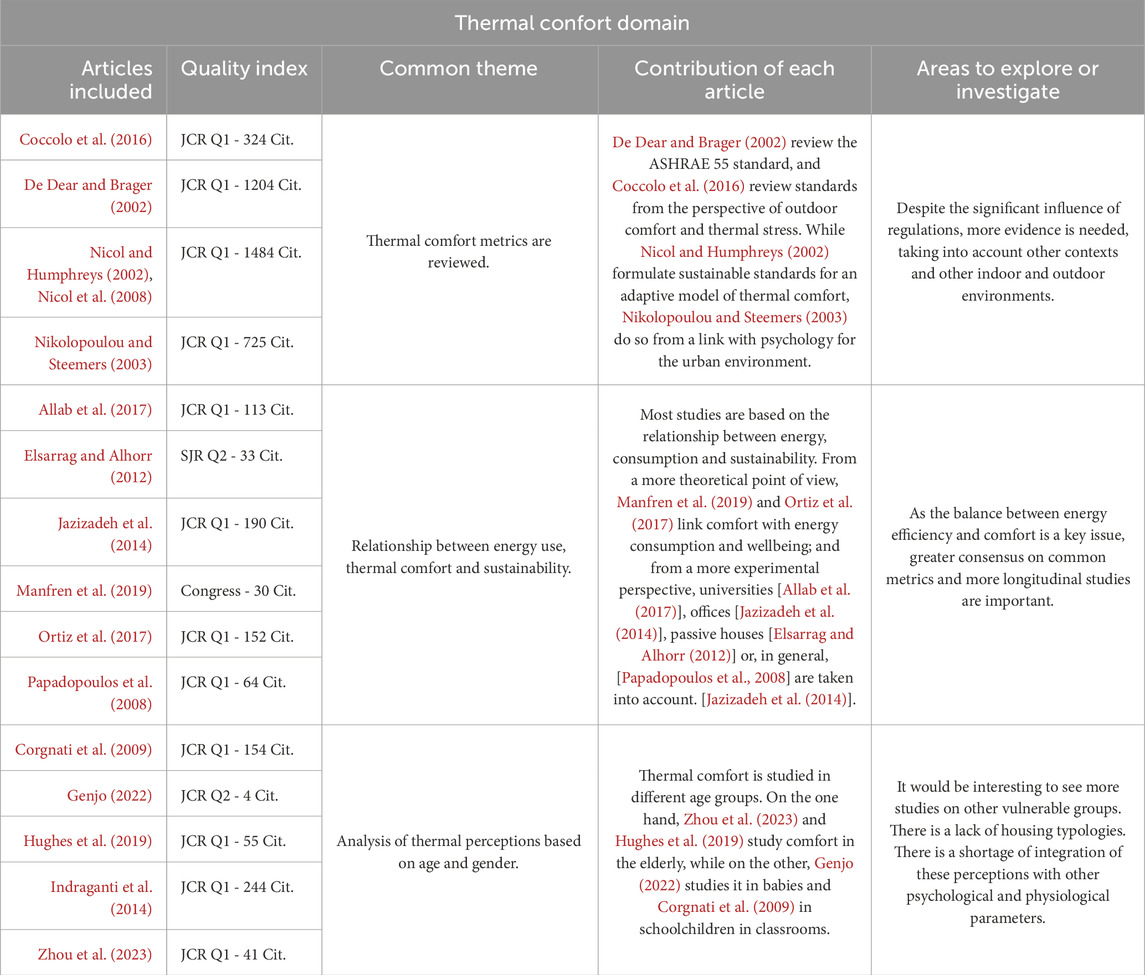
Table 1. Critical synthesis across studies in thermal comfort domain. Main advances in research, common themes, differences and areas where further research is needed.
4 State of the art of the research on indoor air quality
Indoor air quality (IAQ) impacts the health of the building occupants in the short and long term (Simonson et al., 2002; Wargocki et al., 2002). Addressing IAQ comprises three critical factors: external weather conditions, air renewal rates, which directly affect the consumption of HVAC systems (Mancini et al., 2020) and a comprehensive assessment of various air quality parameters. The complexity of pollutant selection goes beyond simple measurements of air temperature and relative humidity, which are typically reported. The wide range of pollutants found in indoor environments complicates the identification of any single pollutant as a sole indicator of IAQ (Ortiz et al., 2017; Wong et al., 2016).
The scientific literature shows that the most prevalent indoor air pollutants include volatile organic compounds (VOC), detected in 84% of cases; carbon dioxide (CO2), present in 65%; asbestos in 45%; particulate matter (PM10 or PM2.5) in 16% (Karami et al., 2018). Other studies consider the former factors and add environmental parameters such as temperature (T) and relative humidity (RH) (Vilčeková et al., 2017), highlighting the close relationship between environmental conditions and thermal comfort (Šujanová et al., 2019). In addition to the pollutants already mentioned, several other airborne particles adversely affect occupant health. Tobacco smoke, mites, pet allergens, cockroaches, mold, pollen, nitrogen oxide, formaldehyde, radon, and mineral fibers must be mitigated by adequate ventilation and air quality management strategies (Franchi et al., 2006).
These parameters are classified into intervals by classes, depending on the different contaminants obtained from the EN 13779: 2007 standard and their relationship to temperature and relative humidity. Table 2 illustrates the relationship of these parameters.

Table 2. Saad et al., 2017; Mancini et al., 2020.
An acceptable concentration of CO2 indoors is usually up to 1,000 ppm (Lai et al., 2009). However, the concentration levels of pollutants usually differ in summer and winter and in different rooms (Zhang et al., 2022). Under external weather conditions, the interior air relative humidity usually goes unnoticed. Not only does relative humidity affect thermal comfort, but it also affects IAQ and the occupants’ health (Simonson et al., 2002). Previous research states that high relative humidity implies a higher formaldehyde concentration. Some material finishes of walls and floors can also produce volatile organic compounds (VOCs) emissions, contributing to unpleasant odors and the perception of stale air (Wolkoff and Kjærgaard, 2007). It is also important to consider air filtration systems, heat gains, airflow patterns, and pressure ratios (Šujanová et al., 2019). The tightness of the building and the use of synthetic construction or furniture materials also impact air quality (Lai et al., 2009). Occupants’ habits and ventilation methods can also be relevant in maintaining good IAQ. Poor ventilation is a significant issue that typically leads to unhealthy indoor air conditions (Zhang et al., 2022).
Recommended values for IAQ can be found in standard EN 16798-3 for non-residential buildings, ASHRAE 62.1 and 62.2, and CR 1752. These standards outline ventilation requirements and offer guidance for designing buildings with adaptable 1AQ. IAQ control can be achieved through natural ventilation or mechanical systems for air renewal (Šujanová et al., 2019).
4.1 Initiative indoor air quality and people’s wellbeing: vulnerability in children, respiratory health in adults, sensitivity in the elderly, and cognitive function
Bluyssen et al. (2011b) and Bluyssen et al. (2011a) state that it is necessary to study the psychological and physiological state of the occupants and its impact on the way the human body reacts to IAQ. Consequently, it is essential to correlate the measurements of the IAQ factors with occupant satisfaction surveys (Andersen et al., 2009).
A perception of dryness, experienced through the mucosal surfaces of the eyes and nose, is exceptionally responsive to irritants and odors (Šujanová et al., 2019). This sensation mostly occurs due to a lack of relative or absolute humidity in indoor environments (Wolkoff, 2018; Wolkoff and Kjærgaard, 2007).
Moreover, a high accumulation of humidity due to a low ventilation rate can favor the transmission of viruses, lengthen their lives, and worsen people’s sleep quality (Wolkoff, 2018; Zhang et al., 2022). In addition, exposure to moisture can cause an increase of 30%–50% in respiratory problems, and, notably, respiratory distress and asthma usually occur slightly more in children than in young adults (Fisk et al., 2007). More aged people will be more sensitive to moisture levels, as there is less mucociliary activity, and they develop eye irritation more rapidly when relative humidity is low (Wolkoff and Kjærgaard, 2007).
Respiratory symptoms and other diseases have often appeared due to poor IAQ (Koponen et al., 2001). Numerous studies show that elevated carbon dioxide (CO2) concentrations have been positively correlated with ocular and nasal symptoms and respiratory conditions such as cough, asthma, fatigue, and headache. Furthermore, these symptoms were most evident when mechanical ventilation or air conditioning was used, compared to natural ventilation (Apte, 2000). These effects are especially harmful among vulnerable populations, including pregnant women and children (Zhang et al., 2022).
Prolonged exposure to indoor air with CO2 concentrations ranging from 1,000 to 2,000 parts per million (ppm) has been associated with drowsiness, while short-term exposure to concentrations around 10,000 ppm can induce respiratory toxicity in adults (Zhang et al., 2022). The high concentrations of PM2.5 and PM10 cause arterial problems and a reduction in life expectancy by 8.6 months (Zhang et al., 2022). Other particles, such as VOCs, can become carcinogenic (Wang et al., 2007). Acknowledging the external pollutants transported indoors, which must be filtered, is also crucial (Koponen et al., 2001). A controlled ventilation rate is essential in environments with children or babies, trying to reach less than 1,000 ppm (Genjo, 2022).
As shown in Table 3, related to the IAQ domain, most studies concentrate on the effects of ventilation and air pollution on health, with a particular emphasis on offices and institutional spaces. Although risks associated with chemical pollutants, particulate matter and humidity are identified, the approaches remain partial and lack a more robust integration between chemical and biological pollutants, as well as psychosocial and behavioural parameters that condition the perception of air quality. Furthermore, there is a significant limitation in the differentiation of vulnerable populations, particularly women, children and the elderly, which reduces the applicability of the findings in more general housing scenarios. The lack of international comparisons and methodological standardisation restricts the transferability of results to different contexts. To address this, studies need to connect scientific evidence with diverse realities and practical strategies for improving IAQ in residential and urban environments.
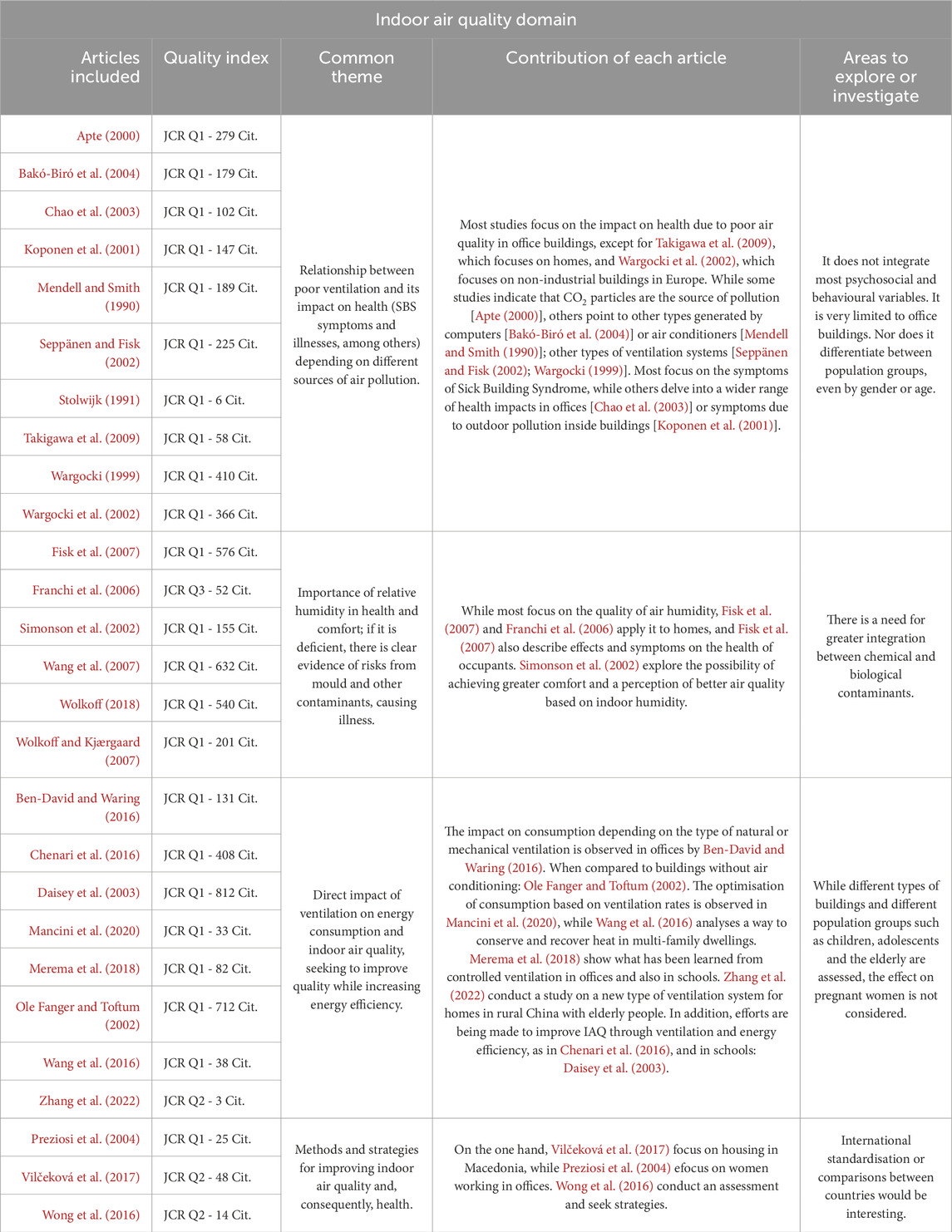
Table 3. Critical synthesis across studies in IAQ domain. Main advances in research, common themes, differences and areas where further research is needed.
5 State of the art of the research on lighting and visual comfort
Good visual comfort is beneficial for users’ wellbeing, who also achieve greater comfort (Serghides et al., 2015; Leech et al., 2002; Veitch, 2001). To ensure this wellbeing through visual comfort, it is crucial to consider the lighting conditions and views of the interior space. These aspects are likely to cause a significant therapeutic impact (Al horr et al., 2016; Aries, 2005; Aries et al., 2010).
5.1 Lighting conditions, glare, contrast and visual clarity, and visual comfort
Consequently, artificial and natural light, along with glare and visual comfort, must be analyzed together to achieve optimal lighting conditions (Al horr et al., 2016; Yun et al., 2012; Van Den Wymelenberg and Inanici, 2014; Huang et al., 2012). Attenuation controls could enhance visual comfort in users (Newsham et al., 2004). When evaluating lighting conditions, it is essential to analyze quantitative measurements of the light environment and qualitative aspects of vision. The former includes light flow, intensity, illuminance, luminance, availability of natural light, sunlight exposure, and glare. The latter comprise light uniformity, light sources, distribution, the intended use of interior spaces, chromatic reproduction, and the spectral composition of radiation (Putri et al., 2023; Šujanová et al., 2019).
For these measurements, we can rely on the EN 12665 standard. International standards are only based on the photopic sensitivity (diurnal) of the human eye, unknown scotopic vision (nighttime), and non-visual effects of light (Šujanová et al., 2019; Alrubaih et al., 2013). Melatonin segregation is important due to the influence of light since it invites us to sleep when it occurs. This hormone stops when humans are exposed to light, primarily to blue wavelengths, which also predominate at night (Bluyssen, 2010). Exposure to light or darkness influences sleep cycles, memory formation, immune response, and metabolic health due to its connection to circadian rhythms (Altomonte et al., 2020).
Improvements made to enhance visual comfort can produce rapid results (14). These improvements can positively affect occupants’ wellbeing and reduce the total energy consumption of the building or house by up to 25% (Costa et al., 2013; Energy Efficiency, 2008; Von Neida et al., 2001).
5.2 Effect of lighting on older people and issues such as age, gender and disability
The human visual system is sensitive to wavelengths of visible radiation ranging from approximately 370 nm–730 nm, with peak sensitivity at around 555 nm. However, empirical evidence indicates that the optical performance of the human eye tends to diminish with advancing age (Šujanová et al., 2019). Additionally, luminous flux and light intensity significantly affect sleep quality in older people (Putri et al., 2023). It is essential to consider major lighting components in relation to melatonin and serotonin production. Current estimates suggest that at least 2.2 billion people experience visual disabilities, which include 1.8 billion with presbyopia and 196 million with macular degeneration. These visual disorders have become a global health problem as the numbers grow gradually with aging (Wu et al., 2022a). The interior spaces must adapt to the deterioration of visual capacity suffered by the elderly (Fu et al., 2022). At earlier stages of life, good lighting or natural light positively affects visual capacity, immune system improvement, and comfort (Optimizing et al., 2022).
In Table 4 (visual comfort domain), we observe that research focuses on the influence of lighting and the visual environment on health, performance and psychological perception, as well as on the development of technological systems and metrics to evaluate this comfort. However, studies remain fragmented between technical (lighting systems, energy optimization) and perceptual approaches (influence of natural light, circadian rhythms, subjective perception), with little integration between the two. Also, there is a lack of validation in different building types and specific populations, such as people with visual impairments, which limits the applicability of the results. The absence of standardization in indicators, as well as the link between objective metrics and subjective perceptions, limits the findings’ capacity to establish universal design criteria. It is therefore essential to adopt more robust comparative methodologies that can translate this evidence into practical guidelines that can be applied in a range of building contexts.
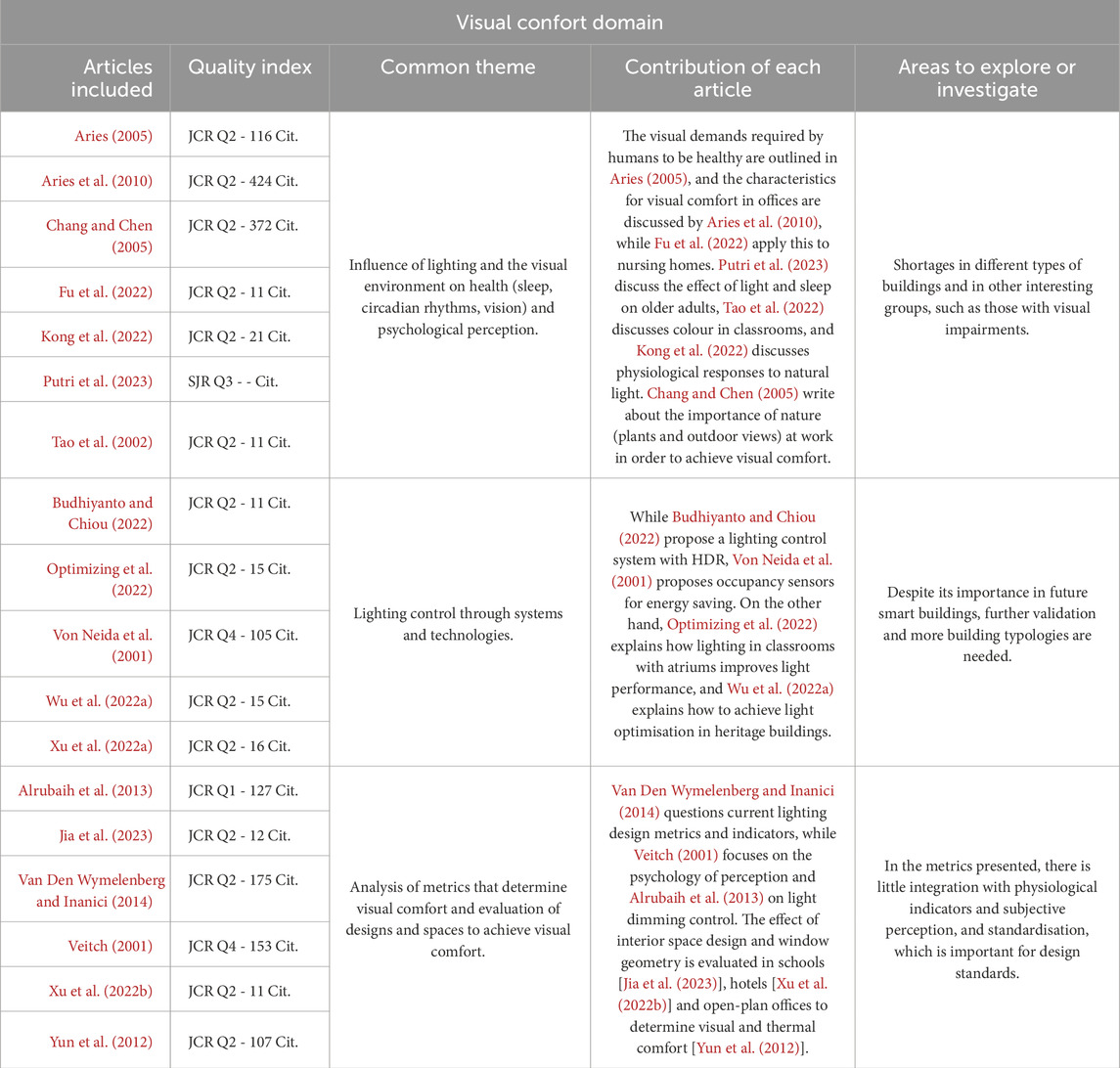
Table 4. Critical synthesis across studies in Visual Comfort domain. Main advances in research, common themes, differences and areas where further research is needed.
6 State of the art of the research on acoustic comfort
To maintain good quality of the indoor environment, it is essential to protect users from noise and provide a comfortable acoustic environment. Indoor spaces must be protected from outdoor noise and noise generated by neighboring equipment or facilities (Al horr et al., 2016). Sound perception depends not only on the intensity of the sound and its temporal and spectral characteristics but also on the individual’s activities, psychological state, and a variety of other contextual factors (Šujanová et al., 2019).
6.1 Conditions for noise perception, acoustic comfort, and speech intelligibility
A high noise level, spectrum, and variation over time influence the level of disturbance and can be perceived as a lack of privacy in communication (Al horr et al., 2016). Continuous and regular sound patterns are less disruptive than noise emanating from various sources and irregular sounds (Veitch et al., 2002). Therefore, a thorough analysis of indoor acoustics must include indoor sound frequency and pressure, sound insulation, acoustic absorption, and reverberation time. In addition, the acoustic quality is multidimensional since it comprises three main variables: sound field, auditory evaluation, and auditory perception (Šujanová et al., 2019). Some standards outlining measurement procedures and associated guidelines include ISO 10140, ISO 717, ISO 3382, and ISO 12354. The auditory system can perceive volume, 1300 tones, intervals, and timbre, as well as the spatial perception of the source in direction and distance (Zhong et al., 2014).
6.2 Effect on the wellbeing of elderly people who are exposed to loud noise. Impact of age, gender, and disability
Humans can perceive vibrations and resonances even in the fetal stage ranging from 10-5 Pa to 100P a (with 0 dB being the hearing threshold and 120 dB the pain threshold) and in a frequency spectrum from 20 Hz to 20 kHz. However, the upper-frequency limit is often reduced with age to 16 kHz (Šujanová et al., 2019). This age-related decline in the auditory range explains that satisfaction with the noise level is higher for elderly people (Zalejska-Jonsson and Wilhelmsson, 2013; Frontczak et al., 2012; Chiang et al., 2001). Nonetheless, the acoustic quality of the current environment is inappropriate for the elderly with hearing loss (Fu et al., 2022). In addition to auditory decline, other issues such as tinnitus, sleep disturbances, hypertension, and cardiovascular diseases may arise, and, in the case of children, cognitive decline (Altomonte et al., 2020). Therefore, ensuring an adequate acoustic environment is critical in the presence of children and babies engaged in crucial stages of speech intelligibility development. The World Health Organization (WHO) recommends that background noise levels should not exceed 35 dB to foster an optimal auditory environment (Genjo, 2022), in contrast to the higher tolerable noise level of up to 80 dB reported by young adults (Altomonte et al., 2020).
In the Acoustic domain, as shown in Table 5, research has been conducted on the impact of noise on health, productivity and cognitive function, with a particular focus on educational settings, offices and specialized residences. However, literature is limited in terms of replication and geographical scope, which weakens the robustness of the conclusions. Furthermore, although architectural and technological solutions for acoustic control are recognized, the studies lack comparative integration that would allow for an evaluation of the joint effectiveness of these strategies in different types of buildings. Another significant gap is the lack of attention to populations with specific vulnerabilities, including people with hearing loss. Therefore, there is a need to move towards interdisciplinary and comparative research that allows for an understanding of the acoustic impact in a greater diversity of contexts and users, contributing to more inclusive and applicable design guidelines.
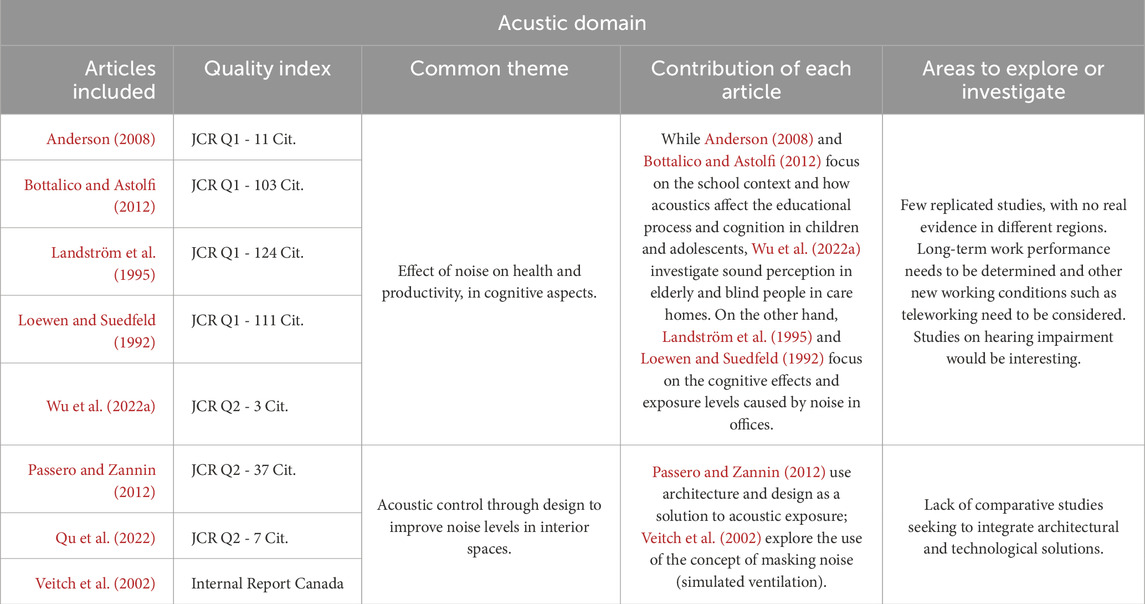
Table 5. Critical synthesis across studies in Acoustic domain. Main advances in research, common themes, differences, and areas where further research is needed.
7 Interaction between sensory perception, cognitive function and design and IEQ in vulnerable groups
Although there is still a limited understanding of human perception’s neurological and biological mechanisms, it is necessary and beneficial to understand how humans perceive and what effects it brings to the environment. Researchers must address psychological and sociological methodologies (Wu et al., 2023a). Indoor natural light landscapes can influence physiological indicators (Kong et al., 2022), while colors can affect emotional indicators (Tao et al., 2022). These findings provide supporting data for future developments in the therapeutic effects of indoor environments on health (Wu et al., 2023a). In addition, natural or biophilic elements, vegetation, and even artificial greenery are incorporated into buildings to improve mental health, help stress, and achieve cognitive recovery and mental fatigue. Being surrounded by plants causes positive stimulation that favors the recovery of diseases (Chang and Chen, 2005).
When analysing the four domains of environmental comfort (Tables 1, 3, 4, 5)—thermal, visual, acoustic and indoor air quality—together, it is evident that, although there is a solid base of studies addressing metrics, standards and effects on health and wellbeing, research remains fragmented and with significant gaps. Each domain focuses on a limited set of technical variables, leaving integration with the psychological, social and behavioural aspects that are essential to understanding the actual experience of occupants in the background. Furthermore, the diversity of contexts and populations is underrepresented: studies favour offices, schools or institutional environments, while vulnerable groups—such as children, older adults, or people with disabilities—receive little attention.
Even in Table 6 (Critical synthesis across studies in IEQ), research lacks of consensus and standardisation in metrics and indices across studies. This limits comparisons between building types, cultural contexts and population groups:
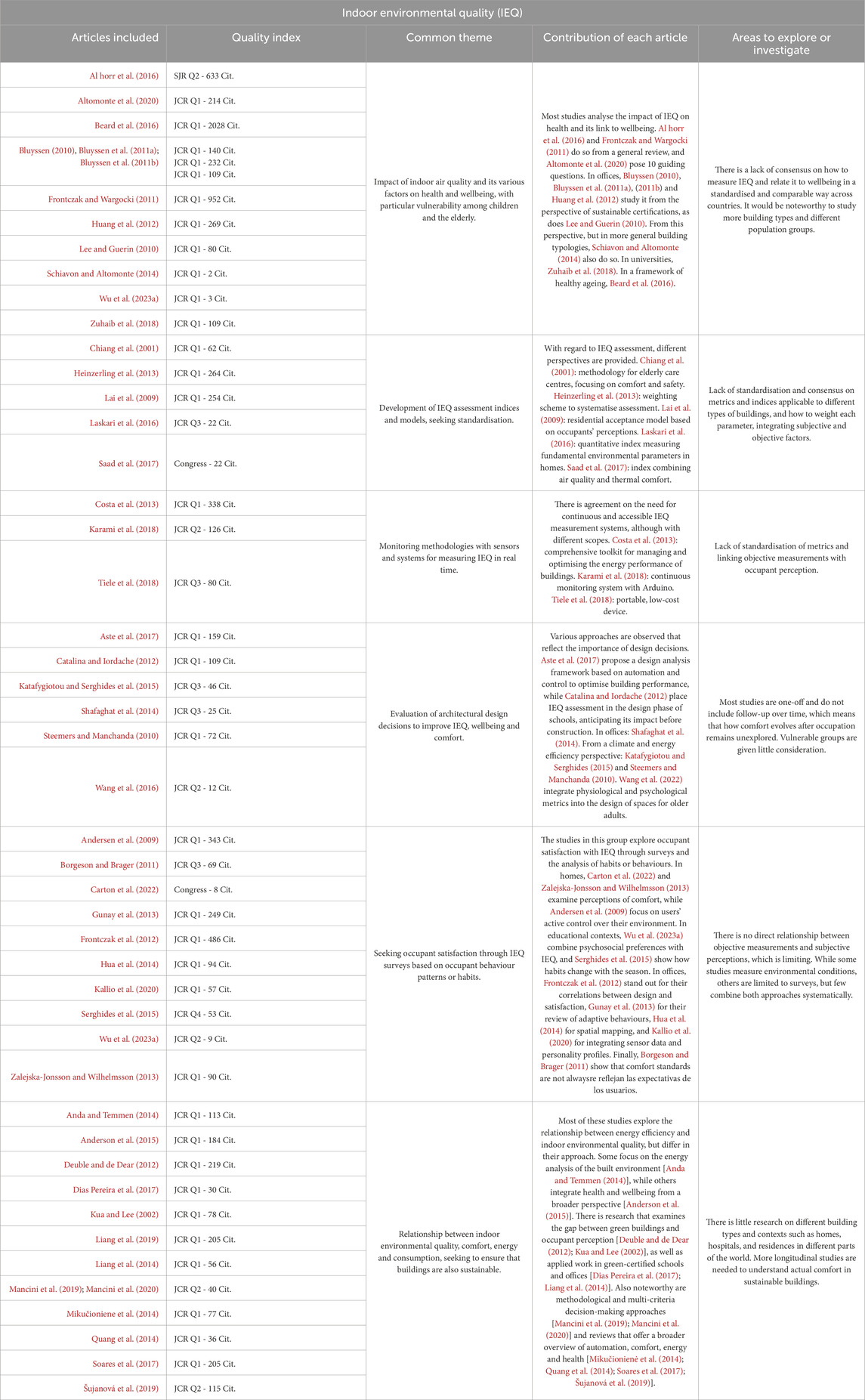
Table 6. Critical synthesis across studies in IEQ. Main advances in research, common themes, differences and areas where further research is needed.
Lack of standardized metrics and methodologies, along with limited international comparability, restricts the application of results of practical design and regulatory criteria.
7.1 Thresholds for vulnerable population according to regulations
Reviewing different regulations enables us to identify certain reference thresholds applicable to groups not considered vulnerable. Therefore, the values for vulnerable groups in Table 7 are estimates, as they are not specifically defined and do not apply to each group. Further research is needed in this regard to determine whether the domains are relevant, or whether it would be more advisable to propose adjustments for a more accurate and consistent representation of vulnerability conditions based not only on global regulations and find standardised metrics applicable worldwide.
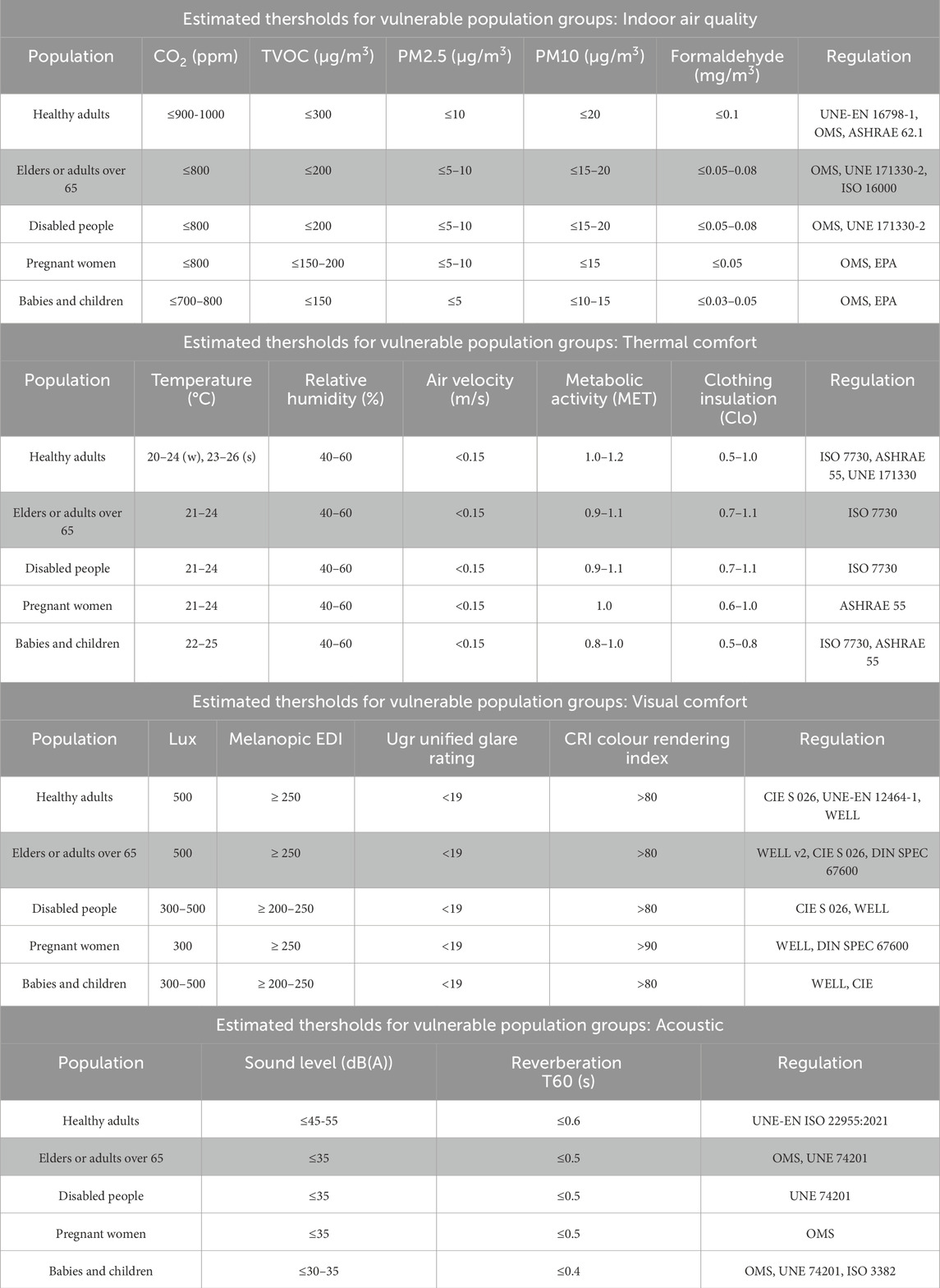
Table 7. Estimated thresholds for vulnerable population according to regulations. Four most important domains within IEQ.
8 Design of healthy and inclusive buildings
The World Health Organization (WHO) defined healthy buildings in 1990. In many investigations, wellbeing is related to the design of buildings and quality standards. However, to achieve and seek objectives to improve the interior environment’s quality, it is important to formulate pertinent inquiries that facilitate effective design strategies to promote wellbeing and accommodate forthcoming factors (Bluyssen, 2010; Altomonte et al., 2020). Attributes of the building, such as the construction materials, the climatic conditions, or those related to users (gender and age, needs and comfort) (95) must be considered at early design stages since they affect the quality of the interior environment (Frontczak et al., 2012). Additionally, economic factors—about financing and the final valuation—coupled with environmental considerations, such as resource utilization, sustainable management practices, and life cycle assessments, must also be incorporated (Bluyssen, 2010). These behavioral aspects remain absent in building certifications such as LEED, BREEAM, or CASBEE. The challenges in defining a healthy building may be due to the conflicting interests between sustainability and the quality of life of the occupants, among others (Bluyssen, 2010; Hua et al., 2014; Schiavon and Altomonte, 2014). This review observes a scarcity of literature that connects IEQ with energy efficiency (Manfren et al., 2019; Lee and Guerin, 2010).
Renovation projects provide clear opportunities to improve building efficiency, including upgrades such as window replacement, roof and wall insulation, renewable energy integration, and the installation of adapted heating or indoor humidity control systems for enhanced thermal comfort (De Santoli et al., 2018; Mikučioniene et al., 2014). In contrast, in new buildings, there must also be a physical adaptation of the environment at the early stages of the design, avoiding the inefficiency and cost associated with renovations (Jazizadeh et al., 2014; Indraganti et al., 2014; Lozinsky et al., 2025). In this adaptation, it is important to consider the climate and the influence of culture (Lovins, 1992). For instance, mechanical cooling is necessary in the Middle East to maintain an optimal level of comfort for occupants (Nicol et al., 2008), whereas, in tropical climates, natural ventilation consumes significantly less energy and provides users with a closer connection to nature (Fisher, 2000).
Design strategies to achieve thermal comfort have evolved to adapt to environmental variability (Table 8). These strategies include operable windows, blinds devices, or automated controls that change their settings in response to changing weather conditions. Among sustainable design strategies, natural ventilation and other passive climate approaches have proven to be the most effective (Deuble and de Dear, 2012). Other factors determining the occupant’s final perception are behavior, physiological adaptation, and psychological expectation (Bluyssen, 2010; Nikolopoulou and Steemers, 2003). As a reference for the design, the ASHRAE 55 and the ISO 7730 standards (1994) define thermal comfort worldwide.
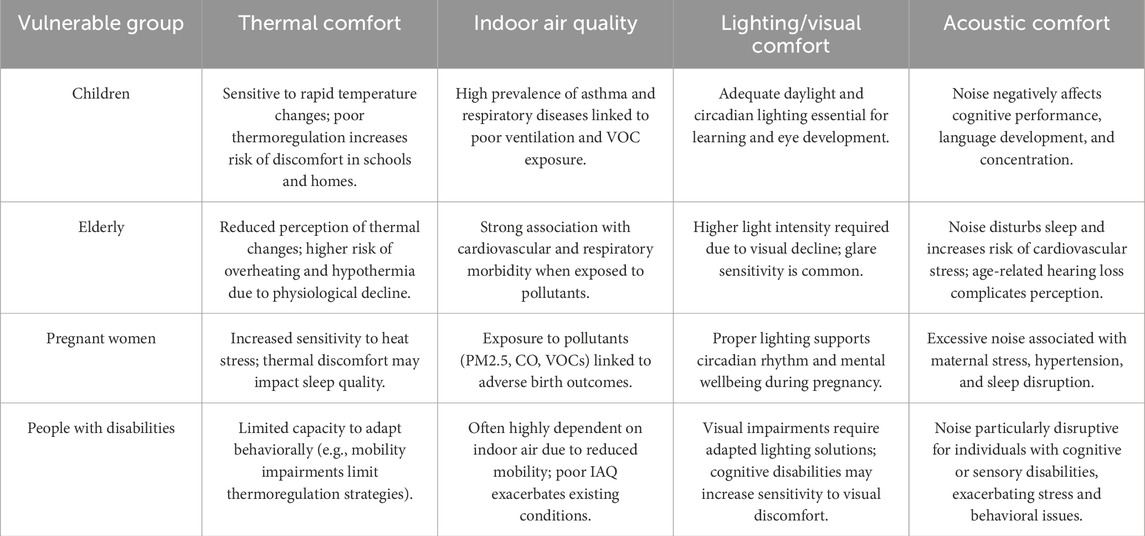
Table 8. Comparative framework: the impact of different IEQ domains on different vulnerable groups.
IAQ is a more complex problem because it depends on external weather conditions and air renewal rates, which directly affect the consumption of HVAC systems (Mancini et al., 2020). Energy-saving strategies must include building design, the implementation of demand-controlled ventilation (DCV) (Merema et al., 2018), or building automation and control systems (BACs). These systems optimize HVAC operation by regulating airflow rates and employing diverse ventilation methodologies (Chenari et al., 2016; Ben-David and Waring, 2016; Mancini et al., 2019; Aste et al., 2017). At the time of day, intelligent or Smart control systems control airflow, temperature, and humidity, among others. Another way to control humidity is by selecting suitable building materials capable of moisture retention, such as wood, which is an alternative approach to humidity control (Simonson et al., 2002).
In building design, the most effective strategies for improving IAQ involve either increasing the ventilation rate, reducing air pollutants (Daisey et al., 2003), or minimizing pollution sources inside and outside the building (Wargocki, 1999). Another passive strategy is the use of natural ventilation (Al horr et al., 2016; Chenari et al., 2016), which can significantly lower cooling energy costs and reduce instances of Sick Building Syndrome (SBS) among occupants (Borgeson and Brager, 2011; Seppänen and Fisk, 2002).
Nevertheless, natural ventilation is not always adequate if there is a significant temperature difference between the indoors and outdoors, which limits its effectiveness in removing indoor pollutants (Zhang et al., 2022). Other passive ventilation systems include solar chimneys on the facade or roof, Trombe walls, and pipes with geothermal air, which are based on solar energy and the residual heat of buildings, increasing the ventilation rate and air temperature. However, those strategies are ineffective in eliminating indoor pollutants and depend on an unstable value of variable solar radiation (Zhang et al., 2022). A more reliable solution may be mechanical ventilation. This solution controls the airflow and starts and stops ventilation to control the pollutants. Additionally, underground ducts can help preheat incoming cold air using the ground’s temperature, improving air quality and enhancing the overall benefits of the ventilation system (Bluyssen, 2010; Wang et al., 2016).
It is essential to ensure visual comfort inside buildings, as it affects the wellbeing of users throughout the day. Some researchers estimate that 30% of energy consumption corresponds to building lighting (Budhiyanto and Chiou, 2022). Decisions such as the geometry and location of windows, surface photometry, the amount of glass, the dense distribution of space, the use of colors, and shading devices are critical for achieving high-quality interior lighting (Al horr et al., 2016; Serghides et al., 2015). By focusing on these elements, building designers can avoid some of the negative impacts associated with poor lighting, such as compromised sleep quality, vision loss, and glare (Chang and Chen, 2005; Serghides et al., 2015; Veitch, 2001). Natural light is considered an essential factor to consider when designing buildings (Optimizing et al., 2022). It not only enhances aesthetic appeal but also reduces the energy demand for electric lighting (Wu et al., 2022b). In renovations, especially in protected facades, the entry of natural light through ceiling openings must be incorporated whenever possible (Wu et al., 2022a). Light control sensors are a system that is implemented in building design, which achieves optimal results and reduces consumption by up to 60% (Jia et al., 2023).
An effective interior design must balance visual comfort with acoustic design without neglecting key acoustic control methods in the form of physical barriers, which often occur in open spaces (98). The geometry of a room plays a significant role. A square area will provide greater acoustic comfort than a long, narrow one, creating a “bowling alley” effect and causing the sound to bounce between the walls (Acoustics in Educational Settings, 2005). ASHRAE Standard 50 recommends minimizing hard surfaces, as these can reduce sound absorption and increase interior noise levels (Anderson, 2008). Therefore, traditional methods include using sound-absorbing materials such as textiles on ceilings, walls, and floors to enhance the acoustic environment.
The selection of appropriate building materials is essential for ensuring good IEQ (Takigawa et al., 2009). The selected materials can significantly impact a space’s thermal, visual, and acoustic comfort (Al horr et al., 2016).
Acoustics is an essential domain to avoid problems in the health and comfort of users (Andersen et al., 2009; Anderson, 2008). A comprehensive assessment of acoustic performance must encompass internal and external noise factors and consider anticipated occupancy patterns within the rooms (Bluyssen et al., 2011a; Bluyssen et al., 2011b). Different strategies can be adopted depending on the source of the noise. If the noise comes from outside, using absorbent materials and acoustic insulation in the ceiling, façade, and windows is advisable. Incorporating absorbent materials and acoustic insulation in the ceiling, façades, and window assemblies is recommended for external noise sources (Qu et al., 2022). If the noise comes from the interior space, physical barriers such as panels in the distribution or electronic sound masking techniques will be used (Loewen and Suedfeld, 1992). The volume, spatial configuration, and the selection of materials or barriers are decisive in achieving acoustic comfort (Šujanová et al., 2019). Despite an increasing emphasis on acoustic comfort factors, the criteria for efficient certifications are often not mandatory in this area, and their indications and guidelines are often incomplete (Schiavon and Altomonte, 2014).
9 Discussion
A building design process that integrates social, environmental, and economic factors into the building can lead to enhanced energy performance and improve IEQ (Steemers and Manchanda, 2010; Kua and Lee, 2002; Iwaro and Mwasha, 2013). However, a conflict between these buildings’ performance and users’ wellbeing remains. A lower ventilation rate means high energy efficiency but also increases the concentration of suspended particles indoors (Lai et al., 2009; Koponen et al., 2001). Moreover, optimizing ventilation rates to prioritize occupants’ comfort might increase acoustic issues due to airflow background noise (Deuble and de Dear, 2012). Decisions regarding ventilation and choices about materials, lighting levels, and other factors ultimately affect occupant wellbeing. Unfortunately, it is a general practice for building designers to promote energy efficiency over the wellbeing of the user (Lai et al., 2009; Koponen et al., 2001; Liang et al., 2014). This practice often leads to pursuing certifications for sustainable design, such as LEED, BREEAM, and GSAS, at the expense of the user’s experience (Elsarrag and Alhorr, 2012).
The use of these certifications generates a contemporary metric depending on the energy efficiency of the building, thanks to simulation tools of the proposed design (WBDG Home), which prioritizes low energy consumption (Šujanová et al., 2019). Usually, one-third of the buildings with these certifications consume more energy than those that do not have it because they typically fail to account for the behavioral patterns of the building’s occupants (Liang et al., 2014; Liang et al., 2019). The introduction of smart controls could lead to a reduction in energy consumption by as much as 10% (Costa et al., 2013; Dean et al., 2016; Anda and Temmen, 2014), compared with the percentage of consumption in the sector in developed countries (Šujanová et al., 2019; Liang et al., 2014). The implementation of renewable energy could favor these buildings since results yielded that 15% of the energy demand is consumed in residential buildings in the European Union (Šujanová et al., 2019).
A building can only be deemed genuinely energy efficient when it neither induces nor exacerbates health issues among its occupants, concurrently ensuring their comfort while minimizing energy expenditures to achieve optimal conditions, as outlined by the Health Optimization Protocol for Energy Efficient Buildings (HOPE) (Cox, 2025).
According to HOPE (Health Optimization Protocol for Energy Efficient Buildings), a building can only be deemed energy efficient when it does not cause or aggravate health issues among its occupants, guarantees comfort, and minimizes the use of energy to achieve the desired conditions (Cox, 2025). The building must be used consciously, without exceeding the occupation, and using efficient technology for its maintenance (Costa et al., 2013; Liang et al., 2019). The IEQ must be evaluated throughout the building’s life cycle, with sustainable strategies at the early design stages and appropriate maintenance of this building until the disposal of materials at the end of its cycle (Al horr et al., 2016). This evaluation must focus on the occupants, considering various user profiles influencing needs based on gender, age, and vulnerabilities. In addition, the quality of the interior environment has been related not only to the wellbeing of these users but also to its impact on health and diseases in the short and long term, being relevant to the development of adequate actions to reduce or eliminate harmful effects on health (Srinivasan et al., 2003).
Despite the advances summarised in this review, it is important to recognise the limitations that make it difficult to draw definitive conclusions about the relationship between IEQ and the health of vulnerable populations. Firstly, the observed associations and relationships may be influenced by uncontrolled confounding factors with a significant impact on indoor environments, which are rarely considered in studies. These factors include external variables, such as outdoor air quality, the presence of urban vegetation or proximity to sources of pollution; internal variables related to the use of everyday items, such as air fresheners or recent renovations; and other factors, such as exposure to electromagnetic fields generated by devices both indoors and in the immediate outdoor vicinity. Secondly, the heterogeneity in the classification and definition of vulnerable groups, as well as in measurement methods, makes it difficult to compare results. Future research must consider these factors in order to reduce bias, improve the validity of findings and establish a more accurate framework.
10 Conclusion
It is important to bear in mind the heterogeneity that exists between the different types of groups considered vulnerable, as well as within each of them. Table 8 contrasts how different vulnerable groups (children, elderly people, pregnant women, and people with disabilities) are affected by the main IEQ domains (thermal, air quality, lighting, acoustics). While there is a significant impact at different stages of life, children are affected in their cognitive development, while older people suffer from chronic diseases. All groups are highly sensitive to poor air quality.
In the case of older people, for example, age is not the only parameter to consider; other parameters must also be taken into account, such as lifestyle, home characteristics, gender, and physiological characteristics such as mobility and chronic diseases (Beard et al., 2016). This highlights the need for an IEQ index model adapted to this heterogeneity, incorporating weights for both variability and environmental domains. While some studies (Laskari et al., 2016; Tiele et al., 2018) have begun to propose such indices and interpret the related weights, further research is needed.
The elderly population is significantly vulnerable due to limited mobility and the high prevalence of chronic diseases. However, there is insufficient scientific literature connecting IEQ with its effects on the physical health of older adults. Building designers need to tackle variables affecting indoor and outdoor environments, as these domains significantly impact the health of vulnerable adults. For instance, studies have shown the importance of bedrooms, indoor gardens, green roofs, and patios, but evidence in this area is limited. Besides involving vulnerable adults in creating inclusive buildings, additional studies need to establish assessment criteria and monitoring standards that can lead to well-rounded design recommendations for housing where vulnerable adults reside. Empirical research on social and economic impacts will help facilitate the sustainable development of aging societies and create more inclusive and healthy designs.
Beyond the energy credentials granted to green and sustainable buildings, specific considerations are required, often insufficient to guarantee user comfort and wellbeing. This document presents a review of current knowledge on user wellbeing and comfort related to IEQ. To address existing research gaps and challenges, a holistic framework for building environment design guidelines should be developed, in addition to future lines of research. These guidelines should provide recommendations for building designers and urban planners that are applicable across various contexts rather than confined to specific locations.
1. Building designs for vulnerable people should prioritize spatial distribution, focusing on places such as bedrooms, dining areas, and other rooms frequented by occupants, ensuring thermal comfort, adequate ventilation, and natural lighting. Future research should prioritize establishing the quantitative relationship between IEQ, comfort conditions, and occupant health, as this remains unclear.
Quantifying the spatial distribution of green spaces in relation to air pollution and extreme heat is imperative, as they act as comfort modulators. In addition, it is a priority to optimise ventilation and air quality through hybrid systems that combine natural and mechanical ventilation to ensure adequate levels of air renewal in spaces that are used for long periods of time. Similarly, the thermal design of buildings should be based on passive strategies, such as insulation, cross ventilation and solar protection, complemented by low-energy technologies. Specific comfort ranges must be defined that take into account the greater sensitivity of certain groups. Lighting is another fundamental aspect: natural light should be encouraged in frequently used rooms and supplemented with adjustable artificial lighting that respects circadian rhythms and reduces glare, thereby contributing to the visual health and rest of the occupants. At the same time, noise exposure must be reduced through more stringent acoustic standards, the use of insulating materials, and landscaping solutions that act as sound barriers.
2. Environmental monitoring and modelling methods can be used to verify and improve the building environment. This can be achieved by installing low-cost, accessible sensors that allow residents to monitor the environmental quality of their homes in real time.
3. It is essential to consider the perspectives of vulnerable individuals through systematic surveys in order to identify the needs and habits of occupants and adjust design solutions accordingly. This information can then be used to establish reference limits and comfort ranges adapted to the vulnerability of occupants, as well as to create design guidelines applicable to vulnerable groups with an adapted IEQ index.
4. Future findings should not only be applied to new constructions, but also to housing renovations and energy efficiency. This will ensure that comfort and health are not neglected in favour of energy-saving criteria.
5. Further studies should be conducted to measure the impact of poor IEQ on the health of vulnerable groups and its relationship with their habits. Generating quantitative models that integrate IEQ, health and occupant habits will help formulate new regulatory frameworks.
6. Finally, it is a priority to develop systematic guidelines with generic conclusions that can be transferred between different climatic and social contexts, and that support the creation of inclusive societies adapted to ageing. To this end, it is necessary to link IEQ research with urban, social, and public health policies at multiple scales, which can be explored in future research.
Author contributions
MH-M: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft, Writing – review and editing. FD: Conceptualization, Data curation, Formal Analysis, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. RG-L: Conceptualization, Data curation, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The authors wish to thank CEU San Pablo University Foundation for the funds dedicated to the ARIE Research Group through the Project “IEQ to guarantee the health and wellbeing of vulnerable people in multi-family homes” of the Call for “Knowledge Generation Projects” within the framework of the State Plan 2021–2023. The project reference is PID2023-151422OB-I00 and was funded by the Ministry of Science, Innovation and Universities of Spain and the European Regional Development Fund (ERDF) of the European Union.
Acknowledgements
The authors would like to thank the CEU San Pablo University Foundation for the funds dedicated to the ARIE Research Group: Architecture, Efficient Installation. Registration number: G20/6-06 of CEU San Pablo University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Acoustics in Educational Settings (2005). Technical report ASHA working group on classroom acoustics. Available online at: http://www.asha.org/members/deskref-journals/deskref/default (Accessed May 30, 2025).
Al horr, Y., Arif, M., Katafygiotou, M., Mazroei, A., Kaushik, A., and Elsarrag, E. (2016). Impact of indoor environmental quality on occupant well-being and comfort: a review of the literature. Int. J. Sustain. Built Environ. 5, 1–11. doi:10.1016/j.ijsbe.2016.03.006
Allab, Y., Pellegrino, M., Guo, X., Nefzaoui, E., and Kindinis, A. (2017). Energy and comfort assessment in educational building: case study in a French University Campus. Energy Build. 143, 202–219. doi:10.1016/J.ENBUILD.2016.11.028
Alrubaih, M. S., Zain, M. F. M., Alghoul, M. A., Ibrahim, N. L. N., Shameri, M. A., and Elayeb, O. (2013). Research and development on aspects of daylighting fundamentals. Renew. Sustain. Energy Rev. 21, 494–505. doi:10.1016/J.RSER.2012.12.057
Altomonte, S., Allen, J., Bluyssen, P. M., Brager, G., Heschong, L., Loder, A., et al. (2020). Ten questions concerning well-being in the built environment. Build. Environ. 180, 106949. doi:10.1016/j.buildenv.2020.106949
Anda, M., and Temmen, J. (2014). Smart metering for residential energy efficiency: the use of community based social marketing for behavioural change and smart grid introduction. Renew. Energy 67, 119–127. doi:10.1016/J.RENENE.2013.11.020
Andersen, R. V., Toftum, J., Andersen, K. K., and Olesen, B. W. (2009). Survey of occupant behaviour and control of indoor environment in Danish dwellings. Energy Build. 41 (1), 11–16. doi:10.1016/J.ENBUILD.2008.07.004
Anderson, K. L. (2008). Classroom acoustics: a first step toward education for all. J. Acoust. Soc. Am. 124 (4_Suppl.), 2587. doi:10.1121/1.4783202
Anderson, J. E., Wulfhorst, G., and Lang, W. (2015). Energy analysis of the built environment—A review and outlook. Renew. Sustain. Energy Rev. 44, 149–158. doi:10.1016/J.RSER.2014.12.027
Apte, M. G., Fisk, W. J., and Daisey, J. M. (2000). Associations between indoor CO2 concentrations and sick building syndrome symptoms in U.S. office buildings: an analysis of the 1994–1996 BASE study data. Indoor Air 10 (4), 246–257. doi:10.1034/J.1600-0668.2000.010004246.X
Aries, M. B. C. (2005). Human lighting demands: healthy lighting in an office environment. PhD Thesis 1 (Research TU/e / Graduation TU/e), Built Environment. Netherland: Technische Universiteit Eindhoven. doi:10.6100/IR594257
Aries, M. B. C., Veitch, J. A., and Newsham, G. R. (2010). Windows, view, and office characteristics predict physical and psychological discomfort. J. Environ. Psychol. 30 (4), 533–541. doi:10.1016/J.JENVP.2009.12.004
Aste, N., Manfren, M., and Marenzi, G. (2017). Building automation and control systems and performance optimization: a framework for analysis. Renew. Sustain. Energy Rev. 75, 313–330. doi:10.1016/J.RSER.2016.10.072
Bakó-Biró, Z., Wargocki, P., Weschler, C. J., and Fanger, P. O. (2004). Effects of pollution from personal computers on perceived air quality, SBS symptoms and productivity in offices. Indoor Air 14 (3), 178–187. doi:10.1111/j.1600-0668.2004.00218.x
Beard, J. R., Officer, A., De Carvalho, I. A., Sadana, R., Pot, A. M., Michel, J. P., et al. (2016). The world report on ageing and health: a policy framework for healthy ageing. Lancet 387 (10033), 2145–2154. doi:10.1016/S0140-6736(15)00516-4
Ben-David, T., and Waring, M. S. (2016). Impact of natural versus mechanical ventilation on simulated indoor air quality and energy consumption in offices in fourteen U.S. cities. Build. Environ. 104, 320–336. doi:10.1016/J.BUILDENV.2016.05.007
Bluyssen, P. M. (2010). Towards new methods and ways to create healthy and comfortable buildings. Build. Environ. 45 (4), 808–818. doi:10.1016/J.BUILDENV.2009.08.020
Bluyssen, P. M., Aries, M., and van Dommelen, P. (2011a). Comfort of workers in office buildings: the European HOPE project. Build. Environ. 46 (1), 280–288. doi:10.1016/J.BUILDENV.2010.07.024
Bluyssen, P. M., Janssen, S., van den Brink, L. H., and de Kluizenaar, Y. (2011b). Assessment of wellbeing in an indoor office environment. Build. Environ. 46 (12), 2632–2640. doi:10.1016/J.BUILDENV.2011.06.026
Borgeson, S., and Brager, G. (2011). Comfort standards and variations in exceedance for mixed-mode buildings. Build. Res. Inf. 39 (2), 118–133. doi:10.1080/09613218.2011.556345
Bottalico, P., and Astolfi, A. (2012). Investigations into vocal doses and parameters pertaining to primary school teachers in classrooms. J. Acoust. Soc. Am. 131 (4), 2817–2827. doi:10.1121/1.3689549
Budhiyanto, A., and Chiou, Y. S. (2022). Prototyping a lighting control system using LabVIEW with real-time high dynamic range images (HDRis) as the luminance sensor. Buildings 2022, 650. doi:10.3390/BUILDINGS12050650
Carton, Q., Kolarik, J., and Breesch, H. (2022). “Analysis of occupant satisfaction with IEQ in residential buildings,” in CLIMA 2022 conference. doi:10.34641/clima.2022.125
Catalina, T., and Iordache, V. (2012). IEQ assessment on schools in the design stage. Build. Environ. 49 (1), 129–140. doi:10.1016/J.BUILDENV.2011.09.014
Chang, C. Y., and Chen, P. K. (2005). Human response to window views and indoor plants in the workplace. HortScience 40 (5), 1354–1359. doi:10.21273/HORTSCI.40.5.1354
Chao, H. J., Schwartz, J., Milton, D. K., and Burge, H. A. (2003). The work environment and workers’ health in four large office buildings. Environ. Health Perspect. 111 (9), 1242–1248. doi:10.1289/ehp.5697
Chenari, B., Dias Carrilho, J., and Gameiro Da Silva, M. (2016). Towards sustainable, energy-efficient and healthy ventilation strategies in buildings: a review. Renew. Sustain. Energy Rev. 59, 1426–1447. doi:10.1016/J.RSER.2016.01.074
Chiang, C. M., Chou, P. C., Lai, C. M., and Li, Y. Y. (2001). A methodology to assess the indoor environment in care centers for senior citizens. Build. Environ. 36 (4), 561–568. doi:10.1016/S0360-1323(00)00024-X
Coccolo, S., Kämpf, J., Scartezzini, J. L., and Pearlmutter, D. (2016). Outdoor human comfort and thermal stress: a comprehensive review on models and standards. Urban Clim. 18, 33–57. doi:10.1016/J.UCLIM.2016.08.004
Corgnati, S. P., Ansaldi, R., and Filippi, M. (2009). Thermal comfort in Italian classrooms under free running conditions during mid seasons: assessment through objective and subjective approaches. Build. Environ. 44 (4), 785–792. doi:10.1016/J.BUILDENV.2008.05.023
Costa, A., Keane, M. M., Torrens, J. I., and Corry, E. (2013). Building operation and energy performance: monitoring, analysis and optimisation toolkit. Appl. Energy 101, 310–316. doi:10.1016/J.APENERGY.2011.10.037
Cox, C. (2025). HOPE: health optimisation protocol for energy-efficient buildings pre-normative and socio-economic research to create healthy and energy-efficient buildings. doi:10.13140/RG.2.2.33658.80328
Daisey, J. M., Angell, W. J., and Apte, M. G. (2003). Indoor air quality, ventilation and health symptoms in schools: an analysis of existing information. Indoor Air 13 (1), 53–64. doi:10.1034/j.1600-0668.2003.00153.x
De Dear, R. J., and Brager, G. S. (2002). Thermal comfort in naturally ventilated buildings: revisions to ASHRAE standard 55. Energy Build. 34 (6), 549–561. doi:10.1016/S0378-7788(02)00005-1
De Santoli, L., Garcia, D. A., Groppi, D., Bellia, L., Palella, B. I., Riccio, G., et al. (2018). “A general approach for retrofit of existing buildings towards NZEB: the windows retrofit effects on indoor air quality and the use of low temperature district heating,” in Proceedings - 2018 IEEE international conference on environment and electrical engineering and 2018 IEEE industrial and commercial power systems Europe, EEEIC/I and CPS Europe 2018. doi:10.1109/EEEIC.2018.8493730
Dean, B., Dulac, J., Petrichenko, K., and Graham, P. (2016). Towards zero-emission efficient and resilient buildings. Global status report. Brazil: Global Alliance for Buildings and Construction.
Deng, H., Xu, Y., and Deng, Y. (2022). Is the shortest path always the best? Analysis of general demands of indoor navigation system for shopping malls. Buildings 12 (10), 1574. doi:10.3390/BUILDINGS12101574
Deuble, M. P., and de Dear, R. J. (2012). Green occupants for green buildings: the missing link? Build. Environ. 56, 21–27. doi:10.1016/J.BUILDENV.2012.02.029
Dias Pereira, L., Neto, L., Bernardo, H., and Gameiro da Silva, M. (2017). An integrated approach on energy consumption and indoor environmental quality performance in six Portuguese secondary schools. Energy Res. Soc. Sci. 32, 23–43. doi:10.1016/J.ERSS.2017.02.004
Elsarrag, E., and Alhorr, Y. (2012). Modelling the thermal energy demand of a Passive-House in the gulf region: the impact of thermal insulation. Int. J. Sustain. Built Environ. 1 (1), 1–15. doi:10.1016/J.IJSBE.2012.07.002
Fisher, T. R. (2000). In the scheme of things: alternative thinking on the practice of architecture. NED-New edition. United States: University of Minnesota Press, 155. Available online at: http://www.jstor.org/stable/10.5749/j.ctttt25c.
Fisk, W. J., Lei-Gomez, Q., and Mendell, M. J. (2007). Meta-analyses of the associations of respiratory health effects with dampness and mold in homes. Indoor Air 17 (4), 284–296. doi:10.1111/J.1600-0668.2007.00475.X
Franchi, M., Carrer, P., Kotzias, D., Rameckers, E. M. A. L., Seppänen, O., Van Bronswijk, J. E. M. H., et al. (2006). Working towards healthy air in dwellings in Europe. Allergy 61 (7), 864–868. doi:10.1111/J.1398-9995.2006.01106.X
Frontczak, M., and Wargocki, P. (2011). Literature survey on how different factors influence human comfort in indoor environments. Build. Environ. 46 (4), 922–937. doi:10.1016/J.BUILDENV.2010.10.021
Frontczak, M., Schiavon, S., Goins, J., Arens, E., Zhang, H., and Wargocki, P. (2012). Quantitative relationships between occupant satisfaction and satisfaction aspects of indoor environmental quality and building design. Indoor Air 22 (2), 119–131. doi:10.1111/j.1600-0668.2011.00745.x
Fu, Y., Wu, Y., Gao, W., and Hui, R. (2022). The effect of daylight illumination in nursing buildings on reading comfort of elderly persons. Buildings 12 (2), 214. doi:10.3390/BUILDINGS12020214
Genjo, K. (2022). Assessment of indoor climate for infants in nursery school classrooms in mild climatic areas in Japan. Buildings 12 (7), 1054. doi:10.3390/BUILDINGS12071054
Gunay, H. B., O’Brien, W., and Beausoleil-Morrison, I. (2013). A critical review of observation studies, modeling, and simulation of adaptive occupant behaviors in offices. Build. Environ. 70, 31–47. doi:10.1016/J.BUILDENV.2013.07.020
Heinzerling, D., Schiavon, S., Webster, T., and Arens, E. (2013). Indoor environmental quality assessment models: a literature review and a proposed weighting and classification scheme. Build. Environ. 70, 210–222. doi:10.1016/J.BUILDENV.2013.08.027
Houtman, I., Douwes, M., de Jong, T., Meeuwsen, J. M., Brekelmans, F., Nieboer-Op de Weegh, M., et al. (2008). New forms of physical and psychosocial health risks at work. doi:10.13140/RG.2.2.21037.79845
Hua, Y., Göçer, Ö., and Göçer, K. (2014). Spatial mapping of occupant satisfaction and indoor environment quality in a LEED platinum campus building. Build. Environ. 79, 124–137. doi:10.1016/J.BUILDENV.2014.04.029
Huang, L., Zhu, Y., Ouyang, Q., and Cao, B. (2012). A study on the effects of thermal, luminous, and acoustic environments on indoor environmental comfort in offices. Build. Environ. 49 (1), 304–309. doi:10.1016/J.BUILDENV.2011.07.022
Hughes, C., Natarajan, S., Liu, C., Chung, W. J., and Herrera, M. (2019). Winter thermal comfort and health in the elderly. Energy Policy 134, 110954. doi:10.1016/j.enpol.2019.110954
Indraganti, M., Ooka, R., Rijal, H. B., and Brager, G. S. (2014). Adaptive model of thermal comfort for offices in hot and humid climates of India. Build. Environ. 74, 39–53. doi:10.1016/J.BUILDENV.2014.01.002
Iwaro, J., and Mwasha, A. (2013). The impact of sustainable building envelope design on building sustainability using integrated performance model. Int. J. Sustain. Built Environ. 2 (2), 153–171. doi:10.1016/J.IJSBE.2014.03.002
Jazizadeh, F., Ghahramani, A., Becerik-Gerber, B., Kichkaylo, T., and Orosz, M. (2014). User-led decentralized thermal comfort driven HVAC operations for improved efficiency in office buildings. Energy Build. 70, 398–410. doi:10.1016/J.ENBUILD.2013.11.066
Jia, Y., Liu, Z., Fang, Y., Zhang, H., Zhao, C., and Cai, X. (2023). Effect of interior space and window geometry on daylighting performance for terrace classrooms of universities in severe cold regions: a case study of Shenyang, China. Buildings 13 (3), 603. doi:10.3390/BUILDINGS13030603
Kallio, J., Vildjiounaite, E., Koivusaari, J., Räsänen, P., Similä, H., Kyllönen, V., et al. (2020). Assessment of perceived indoor environmental quality, stress and productivity based on environmental sensor data and personality categorization. Build. Environ. 175, 106787. doi:10.1016/J.BUILDENV.2020.106787
Karami, M., McMorrow, G. V., and Wang, L. (2018). Continuous monitoring of indoor environmental quality using an Arduino-based data acquisition system. J. Build. Eng. 19, 412–419. doi:10.1016/J.JOBE.2018.05.014
Katafygiotou, M. C., and Serghides, D. K. (2015). Bioclimatic chart analysis in three climate zones in Cyprus. Indoor Built Environ. 24 (6), 746–760. doi:10.1177/1420326X14526909
Kong, Z., Hou, K., Wang, Z., Chen, F., Li, Y., Liu, X., et al. (2022). Subjective and physiological responses towards interior natural lightscape: influences of aperture design, window size and sky condition. Buildings 12 (10), 1612. doi:10.3390/BUILDINGS12101612
Koponen, I. K., Asmi, A., Keronen, P., Puhto, K., and Kulmala, M. (2001). Indoor air measurement campaign in Helsinki, Finland 1999 – the effect of outdoor air pollution on indoor air. Atmos. Environ. 35 (8), 1465–1477. doi:10.1016/S1352-2310(00)00338-1
Kua, H. W., and Lee, S. E. (2002). Demonstration intelligent building—a methodology for the promotion of total sustainability in the built environment. Build. Environ. 37 (3), 231–240. doi:10.1016/S0360-1323(01)00002-6
Lai, A. C. K., Mui, K. W., Wong, L. T., and Law, L. Y. (2009). An evaluation model for indoor environmental quality (IEQ) acceptance in residential buildings. Energy Build. 41 (9), 930–936. doi:10.1016/J.ENBUILD.2009.03.016
Landström, U., Åkerlund, E., Kjellberg, A., and Tesarz, M. (1995). Exposure levels, tonal components, and noise annoyance in working environments. Environ. Int. 21 (3), 265–275. doi:10.1016/0160-4120(95)00017-F
Laskari, M., Karatasou, S., and Santamouris, M. (2016). A methodology for the determination of indoor environmental quality in residential buildings through the monitoring of fundamental environmental parameters: a proposed Dwelling Environmental Quality Index. Indoor Built Environ. 26 (6), 813–827. doi:10.1177/1420326X16660175
Lee, Y. S., and Guerin, D. A. (2010). Indoor environmental quality differences between office types in LEED-certified buildings in the US. Build. Environ. 45 (5), 1104–1112. doi:10.1016/J.BUILDENV.2009.10.019
Leech, J. A., Nelson, W. C., Burnett, R. T., Aaron, S., and Raizenne, M. E. (2002). It’s about time: a comparison of Canadian and American time-activity patterns. J. Expo. Analysis Environ. Epidemiol. 12 (6), 427–432. doi:10.1038/sj.jea.7500244
Liang, H. H., Chen, C. P., Hwang, R. L., Shih, W. M., Lo, S. C., and Liao, H. Y. (2014). Satisfaction of occupants toward indoor environment quality of certified green office buildings in Taiwan. Build. Environ. 72, 232–242. doi:10.1016/J.BUILDENV.2013.11.007
Liang, J., Qiu, Y., and Hu, M. (2019). Mind the energy performance gap: evidence from green commercial buildings. Resour. Conservation Recycl. 141, 364–377. doi:10.1016/J.RESCONREC.2018.10.021
Loewen, L. J., and Suedfeld, P. (1992). Cognitive and arousal effects of masking office noise. Environ. Behav. 24 (3), 381–395. doi:10.1177/0013916592243006
Lovins, A. (1992). Air-conditioning comfort: behavioral and cultural issues. Boulder, CO: IE Source, Inc.
Lozinsky, C. H., Casquero-Modrego, N., and Walker, I. S. (2025). The health and indoor environmental quality impacts of residential building envelope retrofits: A literature review. Build. Environ. 270, 112568. doi:10.1016/J.BUILDENV.2025.112568
Mancini, F., Basso, G. L, and Santoli, L. d. (2019). Energy use in residential buildings: impact of building automation control systems on energy performance and flexibility. Energies 12 (15), 2896. doi:10.3390/EN12152896
Mancini, F., Nardecchia, F., Groppi, D., Ruperto, F., and Romeo, C. (2020). Indoor environmental quality analysis for optimizing energy consumptions varying air ventilation rates. Sustain. Switz. 12 (2), 482. doi:10.3390/su12020482
Manfren, M., Nastasi, B., Piana, E., and Tronchin, L. (2019). On the link between energy performance of building and thermal comfort: An example. AIP Conf. Proc. 2123 (1). doi:10.1063/1.5116993
Mendell, M. J., and Smith, A. H. (1990). Consistent pattern of elevated symptoms in air-conditioned office buildings: a reanalysis of epidemiologic studies. Am. J. Public Health 80 (10), 1193–1199. doi:10.2105/ajph.80.10.1193
Merema, B., Delwati, M., Sourbron, M., and Breesch, H. (2018). Demand controlled ventilation (DCV) in school and office buildings: lessons learnt from case studies. Energy Build. 172, 349–360. doi:10.1016/J.ENBUILD.2018.04.065
Mikučioniene, R., Martinaitis, V., and Keras, E. (2014). Evaluation of energy efficiency measures sustainability by decision tree method. Energy Build. 76, 64–71. doi:10.1016/J.ENBUILD.2014.02.048
Newsham, G., Veitch, J., Arsenault, C., and Duval, C. (2004). “Effect of dimming control on office worker satisfaction and performance,” in Proceedings of the IESNA annual conference, 19–41.
Nicol, J. F., and Humphreys, M. A. (2002). Adaptive thermal comfort and sustainable thermal standards for buildings. Energy Build. 34 (6), 563–572. doi:10.1016/S0378-7788(02)00006-3
Nicol, F., Humphreys, M., and Rijal, H. (2008). Allowing for thermal comfort in free-running buildings in the new European Standard EN 1 525 1. Available online at: https://www.aivc.org/resource/allowing-thermal-comfort-free-running-buildings-neweuropean-standard-en-1-525-1.
Nikolopoulou, M., and Steemers, K. (2003). Thermal comfort and psychological adaptation as a guide for designing urban spaces. Energy Build. 35 (1), 95–101. doi:10.1016/S0378-7788(02)00084-1
Noonan, B., Bancroft, R. W., Dines, J. S., and Bedi, A. (2012). Heat- and cold-induced injuries in athletes: evaluation and management. J. Am. Acad. Orthop. Surg. 20 (12), 744–754. doi:10.5435/JAAOS-20-12-744
Ole Fanger, P., and Toftum, J. (2002). Extension of the PMV model to non-air-conditioned buildings in warm climates. Energy Build. 34 (6), 533–536. doi:10.1016/S0378-7788(02)00003-8
Optimizing, Q., Wu, Y., Liu, Z., Kong, Z., Ma, J., and Yang, Q. (2022). Optimizing annual daylighting performance for atrium-based classrooms of primary and secondary schools in Nanjing, China. Buildings 13 (1), 11. doi:10.3390/BUILDINGS13010011
Ortiz, M. A., Kurvers, S. R., and Bluyssen, P. M. (2017). A review of comfort, health, and energy use: understanding daily energy use and wellbeing for the development of a new approach to study comfort. Energy Build. 152, 323–335. doi:10.1016/J.ENBUILD.2017.07.060
Papadopoulos, A. M., Oxizidis, S., and Papandritsas, G. (2008). Energy, economic and environmental performance of heating systems in Greek buildings. Energy Build. 40 (3), 224–230. doi:10.1016/J.ENBUILD.2007.02.019
Passero, C. R. M., and Zannin, P. H. T. (2012). Acoustic evaluation and adjustment of an open-plan office through architectural design and noise control. Appl. Ergon. 43 (6), 1066–1071. doi:10.1016/J.APERGO.2012.03.007
Preziosi, P., Czernichow, S., Gehanno, P., and Hercberg, S. (2004). Workplace air-conditioning and health services attendance among French middle-aged women: a prospective cohort study. Int. J. Epidemiol. 33 (5), 1120–1123. doi:10.1093/IJE/DYH136
Putri, A. H., Satino, S., Rifai, A., and Widodo, W. (2023). Effect light-intensity on sleep quality in elderly. JKG J. Keperawatan Glob., 89–97. doi:10.37341/jkg.v8i2.858
Qu, T., Wang, B., and Min, H. (2022). Lightweight composite partitions with high sound insulation in hotel interior spaces: design and application. Buildings 12 (12), 2184. doi:10.3390/BUILDINGS12122184
Quang, T. N., He, C., Knibbs, L. D., De Dear, R., and Morawska, L. (2014). Co-optimisation of indoor environmental quality and energy consumption within urban office buildings. Energy Build. 85, 225–234. doi:10.1016/J.ENBUILD.2014.09.021
Redd, S. C. (2002). Mold: state of the science on molds and human health. Available online at: https://stacks.cdc.gov/view/cdc/142218 (Accessed May 30, 2025).
Saad, S. M., Shakaff, A. Y. M., Saad, A. R. M., Yusof, A. M., Andrew, A. M., Zakaria, A., et al. (2017). Development of indoor environmental index: air quality index and thermal comfort index. AIP Conf. Proc. 1808 (1). doi:10.1063/1.4975276/795703
Schiavon, S., and Altomonte, S. (2014). Influence of factors unrelated to environmental quality on occupant satisfaction in LEED and non-LEED certified buildings. Build. Environ. 77, 148–159. doi:10.1016/J.BUILDENV.2014.03.028
Schweiker, M., Ampatzi, E., Andargie, M. S., Andersen, R. K., Azar, E., Barthelmes, V. M., et al. (2020). Review of multi-domain approaches to indoor environmental perception and behaviour. Build. Environ. 176, 106804. doi:10.1016/J.BUILDENV.2020.106804
Seppänen, O., and Fisk, W. J. (2002). Association of ventilation system type with SBS symptoms in office workers. Indoor Air 12 (2), 98–112. doi:10.1034/J.1600-0668.2002.01111.X
Serghides, D. K., Chatzinikola, C. K., and Katafygiotou, M. C. (2015). Comparative studies of the occupants’ behaviour in a university building during winter and summer time. Int. J. Sustain. Energy 34 (8), 528–551. doi:10.1080/14786451.2014.905578
Shafaghat, A., Keyvanfar, A., Lamit, H., Mousavi, S. A., and Majid, M. Z. A. (2014). Open plan office design features affecting staff’s health and well-being status. J. Teknol. Sci. Eng. 70 (7), 83–88. doi:10.11113/JT.V70.3583
Simonson, C. J., Salonvaara, M., and Ojanen, T. (2002). The effect of structures on indoor humidity – possibility to improve comfort and perceived air quality. Indoor Air 12 (4), 243–251. doi:10.1034/J.1600-0668.2002.01128.X
Smolander, J. (2002). Effect of cold exposure on older humans. Int. J. Sports Med. 23 (2), 86–92. doi:10.1055/s-2002-20137
Soares, N., Bastos, J., Pereira, L. D., Soares, A., Amaral, A. R., Asadi, E., et al. (2017). A review on current advances in the energy and environmental performance of buildings towards a more sustainable built environment. Renew. Sustain. Energy Rev. 77, 845–860. doi:10.1016/J.RSER.2017.04.027
Srinivasan, S., O’Fallon, L. R., and Dearry, A. (2003). Creating healthy communities, healthy homes, healthy people: initiating a research agenda on the built environment and public health. Am. J. Public Health 93, 1446–1450. doi:10.2105/AJPH.93.9.1446
Steemers, K., and Manchanda, S. (2010). Energy efficient design and occupant well-being: case studies in the UK and India. Build. Environ. 45 (2), 270–278. doi:10.1016/J.BUILDENV.2009.08.025
Stolwijk, J. A. J. (1991). Sick-building syndrome. Environ. Health Perspect. 95, 99–100. doi:10.1289/EHP.919599
Šujanová, P., Rychtáriková, M., Sotto Mayor, T., and Hyder, A. (2019). A healthy, energy-efficient and comfortable indoor environment, a review. Energies 12 (8), 1414. doi:10.3390/en12081414
Takigawa, T., Wang, B. L., Sakano, N., Wang, D. H., Ogino, K., and Kishi, R. (2009). A longitudinal study of environmental risk factors for subjective symptoms associated with sick building syndrome in new dwellings. Sci. Total Environ. 407 (19), 5223–5228. doi:10.1016/J.SCITOTENV.2009.06.023
Tao, W., Wu, Y., Li, W., and Liu, F. (2022). Influence of classroom colour environment on college students’ emotions during campus lockdown in the COVID-19 post-pandemic Era—A case study in Harbin, China. Buildings 12 (11), 1873. doi:10.3390/BUILDINGS12111873
Tiele, A., Esfahani, S., and Covington, J. (2018). Design and development of a low-cost, portable monitoring device for indoor environment quality. J. Sensors 2018, 1–14. doi:10.1155/2018/5353816
Van Den Wymelenberg, K., and Inanici, M. (2014). A critical investigation of common lighting design metrics for predicting human visual comfort in offices with daylight. LEUKOS - J. Illum. Eng. Soc. N. Am. 10 (3), 145–164. doi:10.1080/15502724.2014.881720
Veitch, J. A. (2001). Psychological processes influencing lighting quality. J. Illum. Eng. Soc. 30 (1), 124–140. doi:10.1080/00994480.2001.10748341
Veitch, J. A., Bradley, J. S., Legault, L. M., Norcross, S. G., and Svec, J. M. (2002). Masking speech in open-plan offices with simulation ventilation noise: noise-level and spectral composition effects on acoustic satisfaction,” in Internal report. Canada: National Research Council of Canada. Institute for Research in Construction. doi:10.4224/20386334
Vilčeková, S., Apostoloski, I. Z., Mečiarová, Ľ., Burdová, E. K., and Kiseľák, J. (2017). Investigation of indoor air quality in houses of Macedonia. Int. J. Environ. Res. Public Health 14 (1), 37. doi:10.3390/IJERPH14010037
Von Neida, B., Manicria, D., and Tweed, A. (2001). An analysis of the energy and cost savings potential of occupancy sensors for commercial lighting systems. J. Illum. Eng. Soc. 30 (2), 111–125. doi:10.1080/00994480.2001.10748357
Wang, S., Ang, H. M., and Tade, M. O. (2007). Volatile organic compounds in indoor environment and photocatalytic oxidation: state of the art. Environ. Int. 33 (5), 694–705. doi:10.1016/J.ENVINT.2007.02.011
Wang, Q., Ploskić, A., Song, X., and Holmberg, S. (2016). Ventilation heat recovery jointed low-temperature heating in retrofitting—An investigation of energy conservation, environmental impacts and indoor air quality in Swedish multifamily houses. Energy Build. 121, 250–264. doi:10.1016/J.ENBUILD.2016.02.050
Wang, H., Hou, K., Kong, Z., Guan, X., Hu, S., Lu, M., et al. (2022). “In-between area” design method: an optimization design method for indoor public spaces for elderly facilities evaluated by STAI, HRV and EEG. Buildings 12 (8), 1274. doi:10.3390/BUILDINGS12081274
Wargocki, P., Wyon, D. P., Baik, Y. K., Clausen, G., and Fanger, P. O. (1999). Perceived air quality, sick building syndrome (SBS) symptoms and productivity in an office with two different pollution loads. Indoor Air 9 (3), 165–179. doi:10.1111/j.1600-0668.1999.t01-1-00003.x
Wargocki, P., Sundell, J., Bischof, W., Brundrett, G., Fanger, P. O., Gyntelberg, F., et al. (2002). Ventilation and health in non-industrial indoor environments: report from a European Multidisciplinary Scientific Consensus Meeting (EUROVEN). Indoor Air 12 (2), 113–128. doi:10.1034/J.1600-0668.2002.01145.X
WBDG Home (n.d.). WBDG - whole building design guide. Available online at: https://www.wbdg.org/ (Accessed June 13, 2025).
WHO. World Health Organization (1983). Assessment of exposure to indoor air pollutants. Euro-Reports and Studies No. 78. Ed.
Wolkoff, P. (2018). Indoor air humidity, air quality, and health – an overview. Int. J. Hyg. Environ. Health 221 (3), 376–390. doi:10.1016/J.IJHEH.2018.01.015
Wolkoff, P., and Kjærgaard, S. K. (2007). The dichotomy of relative humidity on indoor air quality. Environ. Int. 33 (6), 850–857. doi:10.1016/J.ENVINT.2007.04.004
Wong, L.-T., Mui, K.-W., Tsang, T.-W., Cincinelli, A., and Martellini, T. (2016). Evaluation of indoor air quality screening strategies: a step-wise approach for IAQ screening. Int. J. Environ. Res. Public Health 13 (12), 1240. doi:10.3390/IJERPH13121240
World Health Organization (WHO) (2017). Preventing noncommunicable diseases (NCDs) by reducing environmental risk factors. Available online at: https://www.who.int/publications/i/item/WHO-FWC-EPE-17.01 (Accessed May 30, 2025).
Wu, Y., Huo, S., Mu, J., and Kang, J. (2022a). Sound perception of blind older adults in nursing homes. Buildings 12 (11), 1838. doi:10.3390/BUILDINGS12111838
Wu, Y., Liu, Z., Kong, Z., Piraei, F., Matusiak, B., and Lo Verso, V. R. M. (2022b). Evaluation and optimization of daylighting in Heritage buildings: a case-study at high latitudes. Buildings 12 (12), 2045. doi:10.3390/BUILDINGS12122045
Wu, Y., Liu, Z., and Kong, Z. (2023a). Indoor environmental quality and occupant comfort. Buildings 13 (6), 1400. doi:10.3390/buildings13061400
Wu, Y., Liu, Z., Kong, Z., Hamida, A., Eijkelenboom, A., and Bluyssen, P. M. (2023b). Profiling students based on the overlap between IEQ and psychosocial preferences of study places. Buildings 13 (1), 231. doi:10.3390/BUILDINGS13010231
Xu, J., Li, M., Cao, K., Zhou, F., Lv, B., Lu, Z., et al. (2022a). A VR experimental study on the influence of Chinese hotel interior color design on customers’ emotional experience. Buildings 12 (7), 984. doi:10.3390/BUILDINGS12070984
Xu, J., Li, M., Huang, D., Wei, Y., and Zhong, S. (2022b). A comparative study on the influence of different decoration styles on subjective evaluation of hotel indoor environment. Buildings 12 (11), 1777. doi:10.3390/BUILDINGS12111777
Yun, G. Y., Kong, H. J., Kim, H., and Kim, J. T. (2012). A field survey of visual comfort and lighting energy consumption in open plan offices. Energy Build. 46, 146–151. doi:10.1016/J.ENBUILD.2011.10.035
Zalejska-Jonsson, A., and Wilhelmsson, M. (2013). Impact of perceived indoor environment quality on overall satisfaction in Swedish dwellings. Build. Environ. 63, 134–144. doi:10.1016/J.BUILDENV.2013.02.005
Zhang, B., Cai, X., Liu, M., Wu, Y., Liu, Z., Kong, Z., et al. (2022). Study on a new type of ventilation system for rural houses in winter in the severe cold regions of China. Buildings 12 (7), 1010. doi:10.3390/BUILDINGS12071010
Zhong, X., Xie, B., Zhong, X., and Xie, B. (2014). Head-Related transfer functions and virtual auditory display. Soundscape Semiotics - Localisation Categ 6. doi:10.5772/56907
Zhou, S., Li, B., Du, C., Liu, H., Wu, Y., Hodder, S., et al. (2023). Opportunities and challenges of using thermal comfort models for building design and operation for the elderly: a literature review. Renew. Sustain. Energy Rev. 183, 113504. doi:10.1016/j.rser.2023.113504
Keywords: indoor environmental quality, vulnerable people, healthy architecture, inclusive housing, elderly people, healthy buildings
Citation: Hernandez-Martin M, Del Ama Gonzalo F and González-Lezcano RA (2025) Indoor environmental quality to ensure the health and wellbeing of vulnerable people in residential buildings: a systematic review. Front. Built Environ. 11:1652527. doi: 10.3389/fbuil.2025.1652527
Received: 23 June 2025; Accepted: 29 September 2025;
Published: 07 November 2025.
Edited by:
Ilaria Pigliautile, University of eCampus, ItalyReviewed by:
Sahar Zahiri, Oxford Brookes University, United KingdomYijun Chen, Cardiff University, United Kingdom
Copyright © 2025 Hernandez-Martin, Del Ama Gonzalo and González-Lezcano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mar Hernandez-Martin, bWFyLmhlcm5hbmRlem1hcnRpbkBjZXUuZXM=