 Friederike Poppenborg1
Friederike Poppenborg1 Hans Christian Reinhardt
Hans Christian Reinhardt Ferras Alashkar
Ferras Alashkar- 1Department of Hematology and Stem Cell Transplantation, West German Cancer Center, University Hospital Essen, Essen, Germany
- 2Medical Care Centre (MVZ) Dr. Eberhard & Partner Dortmund, Dortmund, Germany
Introduction: The marketing authorization for crizanlizumab (Adakveo®), indicated for the prevention of recurrent vaso-occlusive crises (VOCs) in sickle cell patients (pts) aged ≥16, was revoked by the European Medicines Agency (EMA) as the STAND study did not demonstrate a significant difference between crizanlizumab and placebo in annualized rates of VOCs.
Methods: This is a retrospective, monocentric analysis of adult pts with sickle cell disease (SCD) (age (median) 29 years, range 19-42, annual VOC rate 3, range 1-5, homozygous SCD (HbS/S) 50.0% (4/8)) receiving crizanlizumab as monotherapy at the University Hospital of Essen between Dec 2020 to May 2023 (observation time (median) 17.5 months, range 4.8-27.3). The results were compared to hydroxycarbamide (HC)-treated pts at maximum tolerated dose (MTD).
Results: At 6, 9, and 12 months, mean VOC rate was 1.5 (range 0-3; N=6), 1.8 (range 0-3; N=5) and 4.0 (range 3-5; N=3), indicating a time-dependent increase in VOCs in crizanlizumab-treated pts (6-9 months: p=0.039; 6-12 months: p=0.008) (mean VOC rate in HC-treated pts: 6 months: 0.38, range 0-1 (N=8); 9 months: 0.50, range 0-2 (N=8); 12 months: 0.63, range 0-3 (N=8)). Serious adverse events were mandatory in 7 pts, resulting in 12 inpatient-admissions (acute chest syndrome (N=2), VOC-related pain crisis (N=9), infusion-related VOC (N=1)).
Conclusion: These findings, together with the high economic burden of crizanlizumab in contrast to HC, do further support the revocation of crizanlizumab in Europe in our opinion. Physicians should consider the potential risks when making a therapeutic decision regarding the use of crizanlizumab outside of Europe.
Introduction
Sickle cell disease (SCD) is an autosomal recessive, monogenic disorder associated with early age morbidity and mortality. Both of which are related to acute and chronic disease-associated complications (1). SCD comprises a group of disorders caused by two beta (β)-globin gene (HBB) pathogenic variants, of which at least one is the characteristic substitution of glutamic acid for valine at residue 6 on the β-chain of adult hemoglobin (HbA), resulting in sickle cell hemoglobin (HbS) production (2). HbS polymerization upon deoxygenation is considered central to the disease pathology, contributing to hemolysis with chronic anemia and recurrent vaso-occlusive crises (VOCs) with ischemia-reperfusion injury, in addition to chronic endothelial dysfunction and sterile inflammation, resulting in a viscous cycle (3).
On November 15, 2019, the dual functional, first-in-class humanized immunoglobulin G2 (IgG2)-kappa, anti-P-selectin monoclonal antibody crizanlizumab (Adakveo®) was first approved by the US Food and Drug Administration (FDA) (4, 5). Crizanlizumab was indicated to reduce the frequency of VOCs in older adolescent and adult patients, aged 16 years (yrs) and older suffering from SCD. The approval was based on the positive results observed in the phase 2, double-blind, randomized, placebo-controlled SUSTAIN Trial (NCT01895361) (6–11). In the per-protocol population (N=125), defined as patients who underwent randomization, and who received at least 12 of the 14 scheduled crizanlizumab doses (5.0 mg/kg body weight (BW)), a 52.3% reduction in the annual VOC rate was observed (median, 1.04 vs 2.18 crises per year; p=0.02) (12). In this study, the overall benefit of crizanlizumab was irrespective of concomitant hydroxycarbamide (HC) therapy and/or past VOCs, and incidences of adverse events (AEs) and serious adverse events (SAEs) were similar among patients treated with crizanlizumab and placebo-treated patients (11–13).
On July 23, 2020, the European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) issued a positive opinion for crizanlizumab, resulting in a conditional marketing authorization valid in Europe on October 28, 2020 (11). In Europe, crizanlizumab was indicated for the prevention of recurrent VOCs in SCD patients ≥16 yrs of age at a dose of 5.0 mg/kg BW, given either as an add-on therapy to HC or as a monotherapy in patients in whom the use of HC was inappropriate or inadequate. However, data obtained from the confirmatory STAND Trial (CSEG101A2301; NCT03814746) were requested by the EMA as part of the conditions for approval (11).
On May 26, 2023, the CHMP recommended to revoke the conditional marketing authorization for crizanlizumab in the European Union (EU) (14). This recommendation was based on the preliminary results of the STAND Trial, as no difference between crizanlizumab (5.0 mg/kg BW) (2.49; 95% confidence interval (CI) [1.90; 3.26]) and placebo (2.30; 95% CI [1.75; 3.01]) in the annual VOC rate leading to a physician visit in the first year following randomization (primary endpoint) was observed (rate ratio 1.08; 95% CI [0.76; 1.55]). The adjusted annual rate, estimated by negative binomial regression, for VOCs that resulted in a physician visit and were treated at home (main secondary endpoint) was 4.70; 95% CI [3,60; 6,14] in the crizanlizumab 5.0 mg/kg arm versus (vs) 3.87; 95% CI [3,00; 5,01] in the placebo arm (rate ratio 1.21, 95% CI [0,87; 1,70]). In crizanlizumab-treated patients’, higher rates of grade ≥3 treatment-related adverse events (TAEs) were further reported; however, no new safety concerns were raised (14, 15).
Therefore, the conditional marketing authorization for crizanlizumab in the EU was revoked on May 26, 2023 (Article 20 of Regulation European Commission (EC) No 726/2004), in consultation with the EMA and the Paul Ehrlich Institute (PEI) as the risk-benefit ratio could no longer be considered positive (14, 15).
Materials and methods
Study design and patients
This is a single-centre, retrospective analysis evaluating the efficacy and safety of crizanlizumab in adult SCD patients (≥18 yrs of age) treated at the Adult Hemoglobinopathy Outpatient Unit (AHO) of the University Hospital Essen at the Department of Hematology and Stem Cell Transplantation. In accordance to the SUSTAIN and STAND studies following patient groups were excluded: 1) patients on chronic partial exchange transfusions with crizanlizumab being infused following exchange transfusions, as no stable crizanlizumab plasma concentration could be ensured and 2) patients suffering from ≥10 opioid-dependent VOCs/yr (N=1). Concomitant treatment with HC and/or voxelotor (N=1), including add-on therapy following crizanlizumab induction, was allowed aiming for maximum tolerated dose (MTD) in HC-treated patients during follow-up. Patients not receiving ≥2 crizanlizumab infusions (saturation phase) were further excluded from data analysis, whereas, if this was due to an infusion-related AE, patients were found eligible for evaluation. Patients enrolled in the STAND Trial (N=5) had to be excluded.
The findings were compared to HC-adherent patients dosed at MTD (cross-sectional cohort treated at the AHO). In these patients HC at MTD was achieved and maintained for ≥3 months prior to analysis.
Methods, disease-related definitions, and treatment
Methods
Following capillary electrophoresis (CE), diagnosis of SCD was confirmed according to international standards via molecular genetic analyses of the HBB gene by polymerase chain reaction (PCR), Sanger sequencing and/or multiplex ligation-dependent probe amplification (MLPA) at the Medical Care Centre Dr. Eberhard & Partner Dortmund, Dortmund.
Sickle cell-associated definitions
An acute pain crisis (APC) or uncomplicated VOC was defined as an acute onset of pain for which there was no other medical explanation other than vaso-occlusion and which required either enteral or parenteral analgetic treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) and/or metamizole and required no inpatient admission. A complicated VOC was defined by requiring either enteral or parenteral analgetic treatment with opioids and/or required inpatient admission for treatment. Acute chest syndrome (ACS) or splenic sequestration were referred to as complicated VOCs. ACS was defined based on the finding of a new pulmonary infiltrate in the presence of other signs and symptoms: chest pain, a temperature of ≥38.5°C, tachypnoea, wheezing or cough. Splenic sequestration was defined on the basis of left upper quadrant pain, an enlarged spleen, and an acute decrease in hemoglobin (Hb) concentration (i.e., a decrease in Hb concentration of 2 g/dL from baseline).
Treatment
Crizanlizumab was administered according to the prescribing information at a dose of 5.0 mg/kg BW by intravenous infusion over a period of 30 minutes on week (wk) 0, wk 2, and every 4 wks thereafter. If a dose was missed within 2 wks after a missed visit, the treatment schedule was continued according to the patient’s original visit. If crizanlizumab was administered for more than 2 wks after a missed visit, treatment was continued every 28 days thereafter.
Analysis
Descriptive statistics were applied, summarizing the data following one year of crizanlizumab therapy in adult SCD patients over HC-treated patients at MTD as control group. The data analysis was performed using T-Test at an alpha (α) level of α <0.05 (16).
Results
From December 2020 to December 2022, 11 patients consented to treatment with crizanlizumab (age (median) 29 yrs, range 19 to 42 yrs; homozygous sickle cell disease (HbS/S) 54.5% (6/11)). The annual VOC rate (both, uncomplicated and complicated VOCs) prior to crizanlizumab induction was 2 (median), range 1 to 11. In total, three patients were excluded from data analysis, of which 2 (both, HbS/S) did not receive ≥2 crizanlizumab infusions as they were lost to follow-up due to change of residence. The third patient (sickle beta (β)-thalassemia, HbS/β) who was excluded from evaluation according to study definitions, suffered from ≥10 opioid-dependent VOCs/yr, requiring both, partial manual exchange transfusions every 4 wks in addition to HC (MTD 25 mg/kg BW) for ≥12 months prior to crizanlizumab induction.
In total, 8 patients were eligible for evaluation, of which 7 patients [age (median) 29 yrs, range 25 to 42 yrs; HbS/S 57.1% (4/7)] received ≥2 crizanlizumab infusions, as in one sickle hemoglobin C disease (HbS/C) patient treatment discontinuation was secondary to an infusion-related VOC requiring inpatient admission. In the remaining 7 crizanlizumab-treated patients, median observation time was 17.5 months, range 4.8 to 27.3, with a median number of 12 crizanlizumab infusions (range 5 to 26) being infused. During follow-up, patients were adherent to treatment, resulting in no substantial delay over time. Patients’ baseline characteristics are presented in Table 1. Both patient groups were well balanced [i.e., annual VOC rates prior to treatment in the crizanlizumab group was 3, range 1 to 5, likewise to HC-treated patients (3, range 1 to 4)].
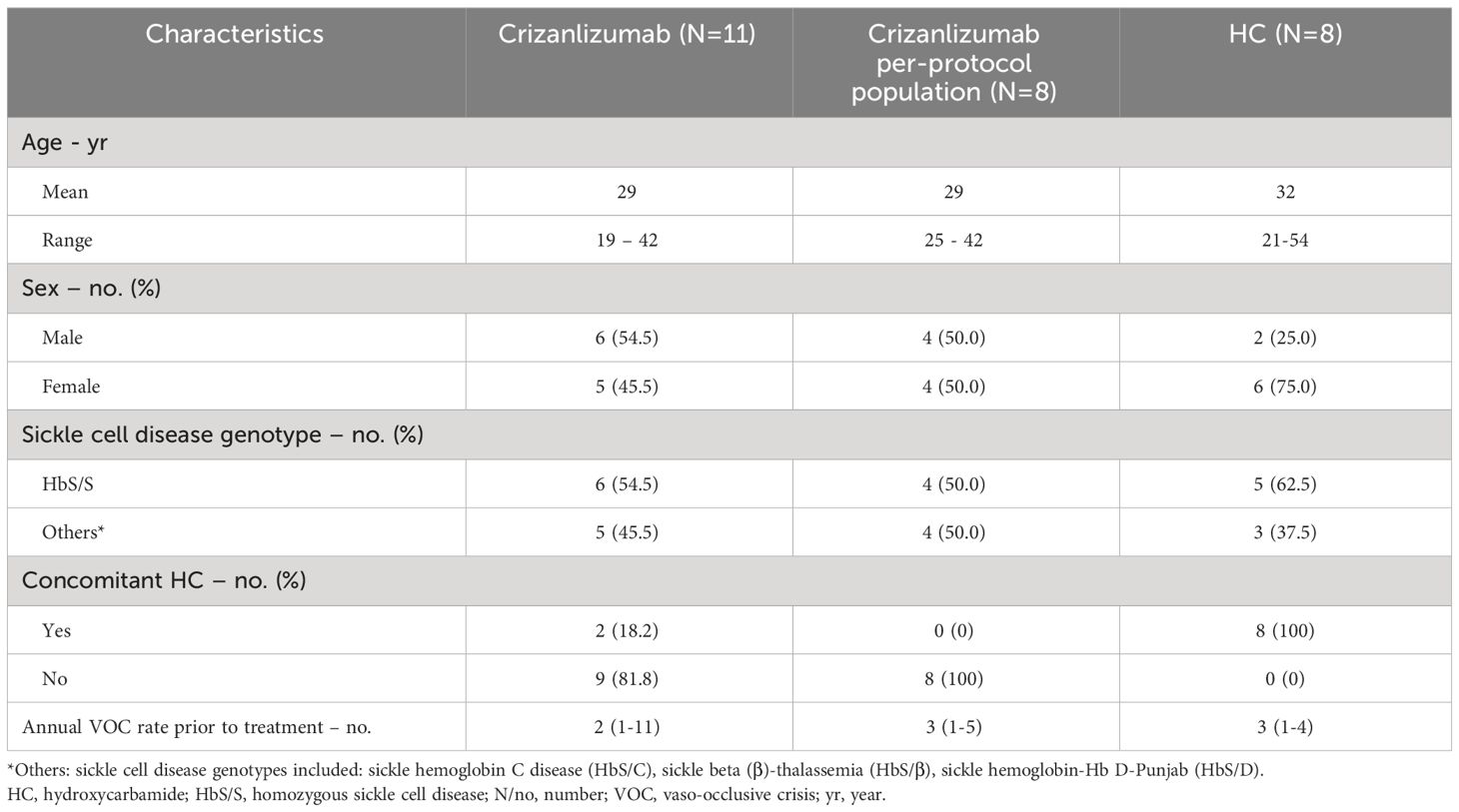
Table 1 Baseline characteristics (N=19).
Therapeutic modalities at baseline and during follow-up
Prior to crizanlizumab, only 1 (HbS/S) patient out of the 7 patients had exposure to HC. However, HC-free interval in this patient was >12 months at baseline. Barriers to the therapeutic use of HC in SCD patients were concerns of HC-associated potential side effects [i.e., fertility concerns (males)]. During follow-up, 2 patients (both, females) consented to add-on treatment with HC due to persistence of VOCs [month 9 (HbS/β) and 20 (HbS/S)] following crizanlizumab induction, respectively. Of note, one of them suffered from a voxelotor-associated allergic reaction prior to HC induction.
Clinical efficacy
At 6, 9, and 12 months, mean VOC rate (both, uncomplicated and complicated) was 1.5 (range 0 to 3; N=6), 1.8 (range 0 to 3; N=5) and 4.0 (range 3 to 5; N=3). The increase in VOCs was time-dependent in crizanlizumab-treated patients (6 to 9 months: p=0.039; 6 to 12 months: p=0.008). In contrast, in HC-treated patients dosed at MTD (reference group), a VOC rate of 0.38 (mean) (range 0 to 1; N=8) at 6 months was observed [(9 months: 0.50 (mean), range 0 to 2 (N=8); 12 months: 0.63 (mean), range 0 to 3 (N=8)] (Figure 1). A VOC rate of zero at 9.1 months (last date of follow-up) was observed in only one male patient (HbS/S, 36 yrs-of-age, annual VOC rate prior to crizanlizumab induction: 1 (complicated VOC), 8 crizanlizumab infusions). In 2 (both, HbS/S) out of the 6 crizanlizumab-treated patients (33.3%), a reduction in the need for opioid analgesics was further documented.
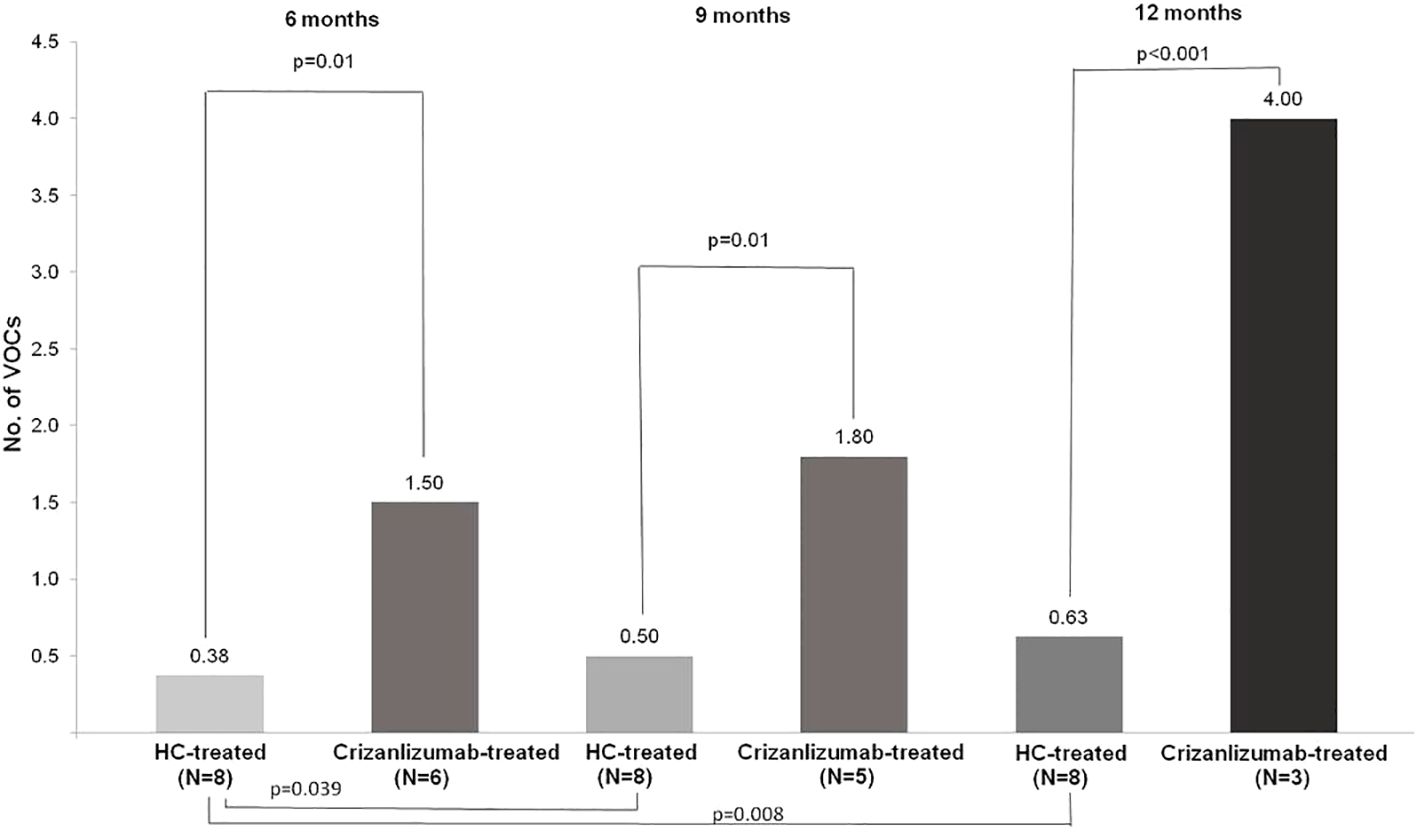
Figure 1 Vaso-occlusive rates in crizanlizumab- and HC-treated adult patients with sickle cell disease at 6, 9, and 12 months. HC, hydroxycarbamide; N/no, number; VOCs, vaso-occlusive crises.
In the present analysis, VOC rates were independent of SCD-genotype at 6 months (N=6) (Figure 2). Despite an overall increase in VOCs in crizanlizumab-treated patients, for both, uncomplicated and complicated VOCs, no significance was observed (Figure 3).
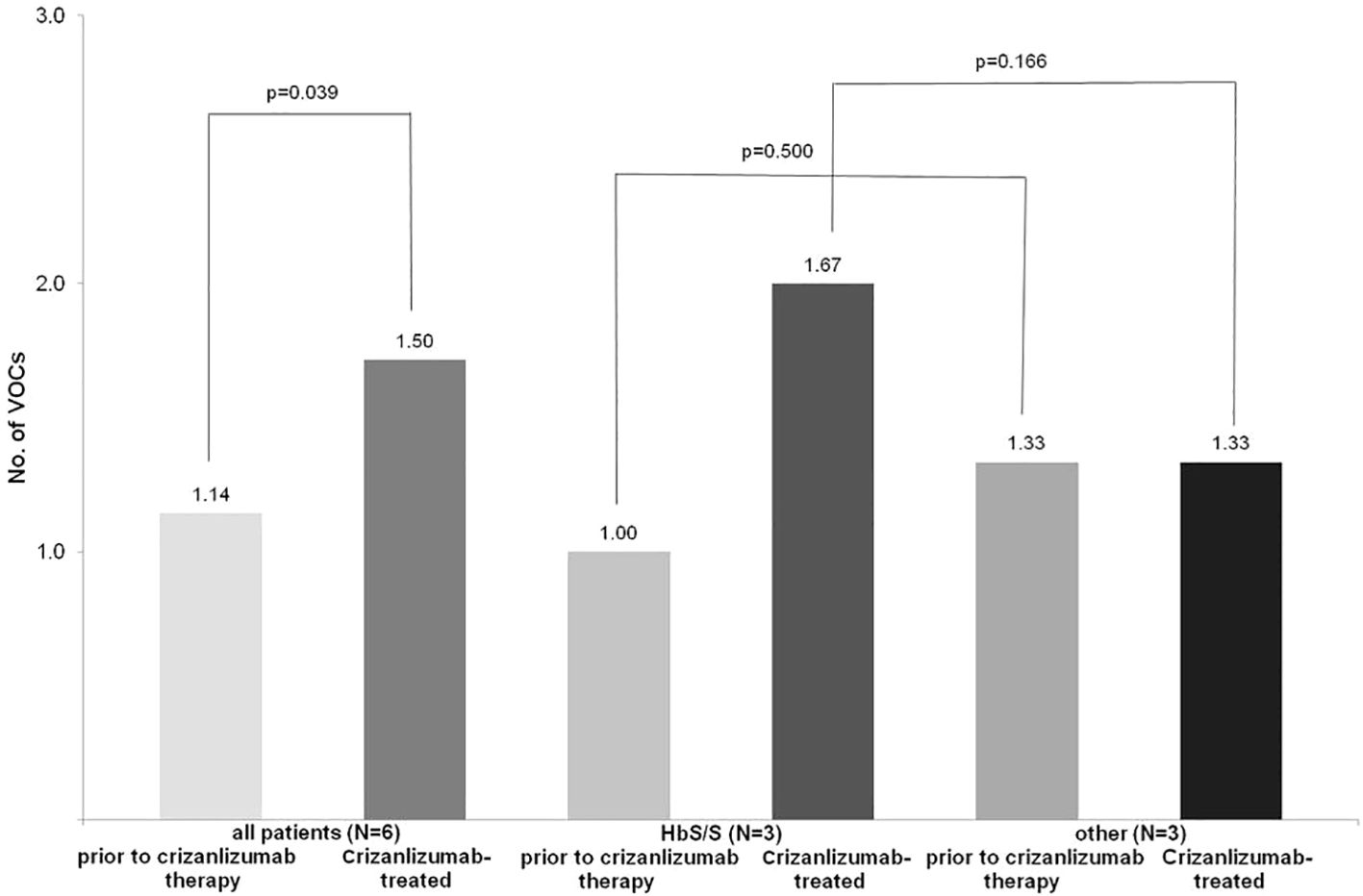
Figure 2 Vaso-occlusive rates at 6 months in crizanlizumab-treated adult patients with sickle cell disease in dependence of genotype. HC, hydroxycarbamide; HbS/S, homozygous sickle cell disease; other: sickle beta (β)-thalassemia (HbS/β), sickle hemoglobin-Hb D-Punjab (HbS/D); N/no, numberVOCs, vaso-occlusive crises.
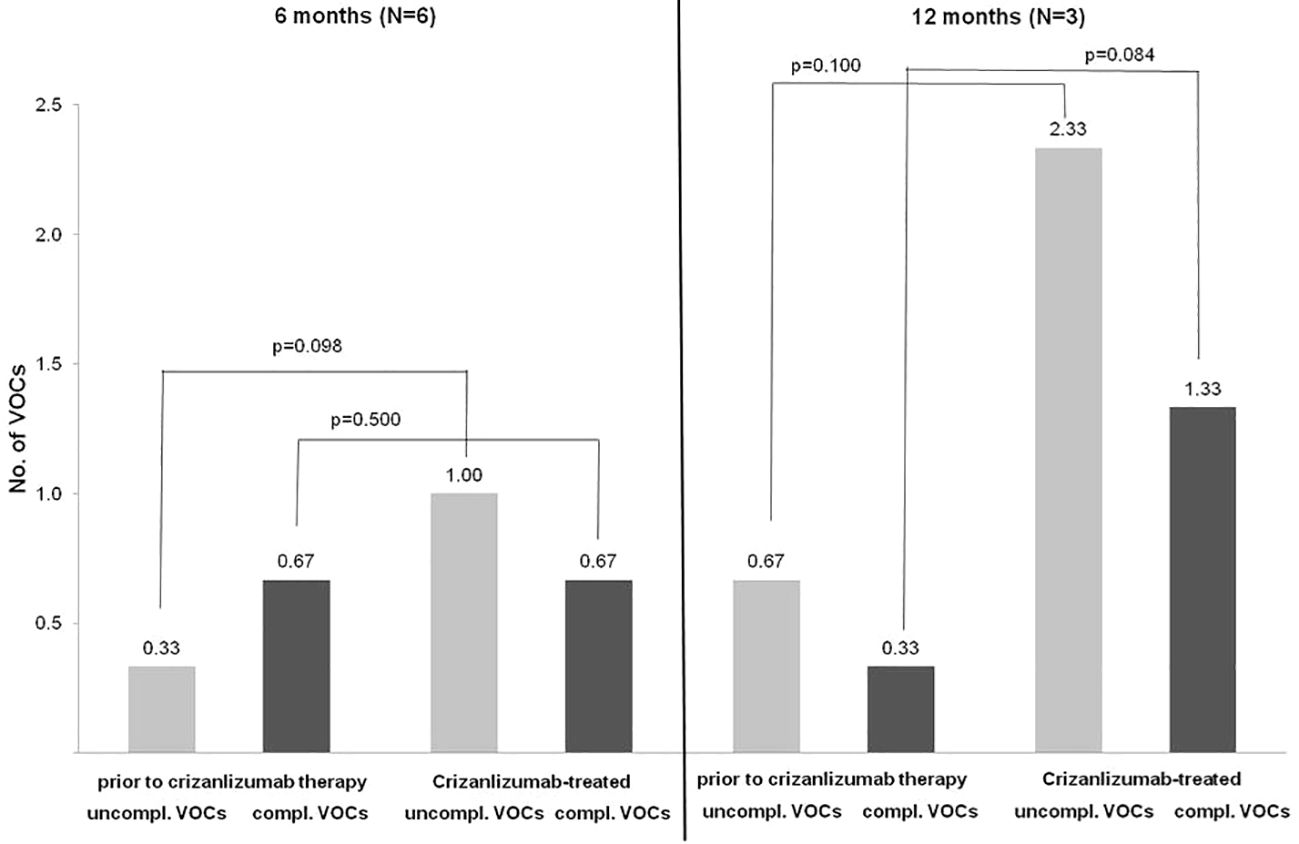
Figure 3 Uncomplicated and complicated vaso-occlusive crises at 6 (N=6) and 12 months (N=3) in crizanlizumab-treated adult patients with sickle cell disease (add-on therapy allowed (N=2)) compl., complicated; N/no, number; VOCs, vaso-occlusive crises; uncompl., uncomplicated.
Safety
None of the patients died throughout observation period. SAEs, requiring in-patient admissions, were observed in 7 crizanlizumab-treated patients resulting in overall 12 inpatient-admissions [(infectious-related) acute chest syndrome (N=2), (infectious-related) VOC-related pain crisis (N=9), infusion-related VOC (N=1)]. All safety data are listed in Table 2.
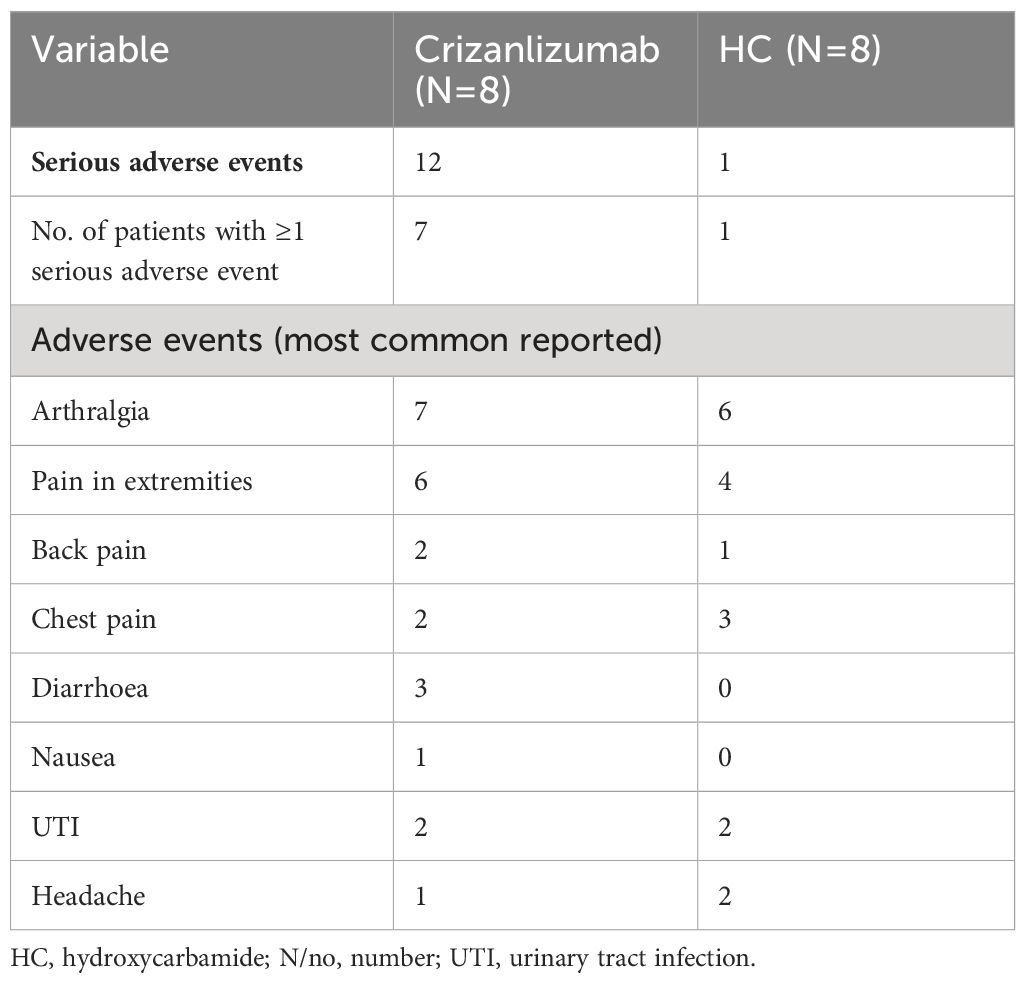
Table 2 (Serious) adverse events (N=16).
Discussion
SCD is considered a rare disease in Germany with an estimated number of at least 2.000 affected patients (17). Besides the monocentric character of the present analysis with a resulting low number of crizanlizumab-treated patients at AHO at the University Hospital of Essen and no placebo-matched control group, our data support the preliminary findings observed within in the STAND Trial (18), resulting in no significant benefit of crizanlizumab in reducing (annual) VOCs rates in addition to a high rate of (S)AEs in these patients. Furthermore, standard HC therapy at a MTD proved to be superior to crizanlizumab-monotherapy in the studied patients.
(Minor) differences were applied for the definition of VOCs in contrast to both crizanlizumab studies. In the present analysis add-on therapy with HC, including subsequent dose titration, and voxelotor was allowed throughout observation time. These therapeutic attempts represent what we consider to be more accurate in daily practice.
In the SUSTAIN Study a -32.1% lower rate in the median crisis rate/yr was observed in patients receiving HC and crizanlizumab (13). Unfortunately, none of the patients treated in the present analysis did consent to prior HC treatment despite experiencing high rates of VOCs that required frequent hospitalizations. Therefore, a (potentially) synergistic effect cannot be excluded. During follow-up, however, two crizanlizumab-treated patients consented to add-on HC therapy, as no reduction in VOCs was observed. Add-on therapy with HC in these patients, likewise to the HC-control group, was well tolerated during follow-up (on average 10 months), resulting in an overall improvement of patients’ daily physical activities with no need for VOC-related in-patient admissions at data cut-off.
To date, no HC dosing data (mg/kg BW) are reported in both crizanlizumab studies (SUSTAIN and STAND). This, together with the fact, that a HC dose titration was excluded, will further not answer the question of a (potentially) synergistic effect at a HC-MTD pattern. Furthermore, no data supporting the adherence of patients to HC can be drawn from these two trials in our opinion. Considering the divergent results observed within these studies, in addition to the data observed within the present analysis, a (partial) poor adherence to HC in patients treated within the STAND Trial might potentially be assumed. Although the selected control group within this present analysis might represent a comparative group of only limited significance, this comparison allows to highlight the efficacy of HC in patients with good adherence to HC at a MTD in comparison to crizanlizumab monotherapy.
These findings, together with the overall high economic burden of crizanlizumab treatment ranging between $7,071 to $9,428/month ($84,852 and $113,135/year) in contrast to the cost-effectiveness of HC monotherapy, does further support EMA’s decision in our opinion to revoke the conditional approval of crizanlizumab in Europe (19–23). Following the withdrawal of the marketing authorization for crizanlizumab in Europe, the question of further therapeutic options (cell-based gene therapies excluded) for patients who have benefited from a crizanlizumab-based therapy remains unanswered, as it is obvious that most of these patients will have already refused therapy with HC (24). Regarding ongoing trial data assessment, physicians outside Europe should consider the potential risks when making a therapeutic decision regarding the use of crizanlizumab.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the University of Duisburg-Essen (23-11246-BO). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
FP: Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft. AR: Formal analysis, Validation, Writing – review & editing. RY: Formal analysis, Methodology, Validation, Writing – review & editing. HCR: Formal analysis, Validation, Writing – review & editing. FA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was founded by HCR.
Conflict of interest
FA received honorarium for participation in advisory boards from Novartis, Global Blood Therapeutics/Pfizer, Bristol Myers Squibb, and Vertex Pharmaceuticals, received a speaker honorarium from Novartis, Global Blood Therapeutics/Pfizer, Agios Pharmaceuticals, and Vertex Pharmaceuticals, and received an honorarium from Novartis, Bristol Myers Squibb, Global Blood Therapeutics/Pfizer, and Vertex Pharmaceuticals for consultancy. HCR received consulting and lecture fees from AbbVie, AstraZeneca, Roche, Janssen-Cilag, Novartis, Vertex, and Merck, received research funding from Gilead and AstraZeneca. HCR is a co-founder of CDL Therapeutics GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kavanagh PL, Fasipe TA, Wun T. Sickle cell disease: A review. JAMA. (2022) 328:57–68. doi: 10.1001/jama.2022.10233
2. Brandow AM, Liem RI. Advances in the diagnosis and treatment of sickle cell disease. J Hematol Oncol. (2022) 15:20. doi: 10.1186/s13045-022-01237-z
3. Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. (2010) 376:2018–31. doi: 10.1016/S0140-6736(10)61029-X
4. Kutlar A, Kanter J, Liles DK, Alvarez OA, Cançado RD, Friedrisch JR, et al. Effect of crizanlizumab on pain crises in subgroups of patients with sickle cell disease: A SUSTAIN study analysis. Am J Hematol. (2019) 94(1):55–61. doi: 10.1002/ajh.25308
5. Sy SKB, Tanaka C, Grosch K. Population pharmacokinetics and pharmacodynamics of crizanlizumab in healthy subjects and patients with sickle cell disease. Clin Pharmacokinet. (2023) 62:249–66. doi: 10.1007/s40262-022-01193-4
6. Karki NR, Kutlar A. P-selectin blockade in the treatment of painful vaso-occlusive crises in sickle cell disease: A spotlight on crizanlizumab. J Pain Res. (2021) 14:849–56. doi: 10.2147/JPR.S278285
7. Delgado J, Voltz C, Stain M, Lapveteläinen T, Urach S, Lähteenvuo J, et al. The european medicines agency review of crizanlizumab for the prevention of recurrent vaso-occlusive crises in patients with sickle cell disease. Hemasphere. (2021) 5(7):e604. doi: 10.1097/HS9.0000000000000604
8. Han J, Saraf SL, Gordeuk VR. Systematic review of crizanlizumab: A new parenteral option to reduce vaso-occlusive pain crises in patients with sickle cell disease. Pharmacotherapy. (2020) 40:535–43. doi: 10.1002/phar.2409
9. Chan KH, Buddharaju R, Idowu M. Real-world experience of patients with sickle cell disease treated with crizanlizumab. J Investig Med. (2024) 72(2):242–7. doi: 10.1177/10815589231220592
10. National Libary of Medicine. Study to Assess Safety and Impact of SelG1 With or Without Hydroxyurea Therapy in Sickle Cell Disease Patients With Pain Crises (SUSTAIN). Available online at: https://classic.clinicaltrials.gov/ct2/show/NCT01895361.
11. European Medicines Agency. Adakveo (crizanlizumab), EMA/446082/2020 EMEA/H/C/004874 . Available online at: https://ema.europa.eu/medicines/human/orphan-designations/eu3121034.
12. Ataga KI, Kutlar A, Kanter J, Liles D, Cancado R, Friedrisch J, et al. Crizanlizumab for the prevention of pain crises in sickle cell disease. N Engl J Med. (2017) 376(5):429–39. doi: 10.1056/NEJMoa1611770
13. Ataga KI, Kutlar A, Kanter J, Liles D, Cancado R, Friedrisch J, et al. SUSTAIN: A multicenter, randomized, placebo-controlled, double-blind, 12-month study to assess safety and efficacy of SelG1 with or without hydroxyurea therapy in sickle cell disease patients with sickle cell-related pain crises. Blood. (2016) 128(22):1. doi: 10.1182/blood.V128.22.1.1
14. European Medicines Agency. ADAKVEO (crizanlizumab): revocation of EU marketing authorisation due to lack of therapeutic efficacy. (2023). Available online at: https://www.ema.europa.eu/en/news/revocation-authorisation-sickle-cell-disease-medicine-adakveo.
15. CHMP. Adakveo - EMEA/H/A-20/1525/C/4874/0013. (2023). Available online at: https://www.ema.europa.eu/en/medicines/human/referrals/adakveo.
16. Planing P. Statistik Grundlagen, T-Test (2023). Available online at: https://statistikgrundlagen.de/ebook/chapter/t-test_t-tests/.
17. Kunz JB, Lobitz S, Grosse R, Oevermann L, Hakimeh D, Jarisch A, et al. German sickle cell disease registry. Sickle cell disease in Germany: Results from a national registry. Pediatr Blood Cancer. (2020) 67(4):e28130. doi: 10.1002/pbc.28130
18. National Institute of Health (NIH). Study of Two Doses of Crizanlizumab Versus Placebo in Adolescent and Adult Sickle Cell Disease Patients (STAND). Available online at: https://classic.clinicaltrials.gov/ct2/show/NCT03814746.
19. Moore RD, Charache S, Terrin ML, Barton FB, Ballas SK. Cost-effectiveness of hydroxyurea in sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea in Sickle Cell Anemia. Am J Hematol. (2000) 64:26–31. doi: 10.1002/(ISSN)1096-8652
20. Joana Carvalho P. FDA Approves Novartis’ Adakveo, 1st Treatment for Pain Crises in Teens and Adults with SCD. Available online at: https://sicklecellanemianews.com/news/fda-approves-adakveo-novartis-scd-pain-crises-treatment-adults-teens/.
21. Stallworth JR, Jerrell JM, Tripathi A. Cost-effectiveness of hydroxyurea in reducing the frequency of pain episodes and hospitalization in pediatric sickle cell disease. Am J Hematol. (2010) 85:795–7. doi: 10.1002/ajh.21772
22. John CC, Opoka RO, Latham TS, Hume HA, Nabaggala C, Kasirye P, et al. Hydroxyurea dose escalation for sickle cell anemia in sub-saharan Africa. N Engl J Med. (2020) 382(26):2524–33. doi: 10.1056/NEJMoa2000146
23. Steinberg MH, Barton F, Castro O, Pegelow CH, Ballas SK, Kutlar A, et al. Effect of hydroxyurea on mortality and morbidity in effect of hydroxyurea on mortality and morbidity in adult sickle cell anemia, risks and benefits up to 9 years of treatment. JAMA. (2003) 289(13):1645–51. doi: 10.1001/jama.289.13.1645
Keywords: crizanlizumab, hydroxycarbamide, sickle cell disease, vaso-occlusive crises, health economics
Citation: Poppenborg F, Röth A, Yamamoto R, Reinhardt HC and Alashkar F (2024) Crizanlizumab in adult patients with sickle cell disease: a retrospective German analysis. Front. Hematol. 3:1374181. doi: 10.3389/frhem.2024.1374181
Received: 21 January 2024; Accepted: 23 April 2024;
Published: 10 May 2024.
Edited by:
Anna Rita Migliaccio, Campus Bio-Medico University, ItalyReviewed by:
Gil Cunha De Santis, Hemocentro Foundation of Ribeirão Preto, BrazilNoel Scott Reading, ARUP Laboratories, United States
Copyright © 2024 Poppenborg, Röth, Yamamoto, Reinhardt and Alashkar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ferras Alashkar, ZmVycmFzLmFsYXNoa2FyQHVrLWVzc2VuLmRl