 Nicolò Danesin1,2†
Nicolò Danesin1,2† Giovanni Leone1,2†
Giovanni Leone1,2† Mattia D’Antiga1,2
Mattia D’Antiga1,2 Marco Carraro1,2Greta Scapinello1,2
Marco Carraro1,2Greta Scapinello1,2 Livio Trentin1,2
Livio Trentin1,2 Francesco Piazza1,2*
Francesco Piazza1,2*- 1Department of Medicine, University of Padova, Padova, Italy
- 2Hematology Unit, Azienda Ospedale Università Padova, Padova, Italy
Waldenström Macroglobulinemia (WM) is a rare, indolent B-cell lymphoma that primarily affects elderly individuals. Although frontline chemoimmunotherapy and Bruton’s tyrosine kinase inhibitors (BTKi) can provide durable responses, most patients eventually relapse, posing ongoing clinical challenges. This review outlines the current therapeutic landscape for relapsed and refractory (R/R) WM, with a focus on emerging treatment strategies. While the efficacy of chemoimmunotherapy and targeted agents in the frontline setting is well established, the management of relapsed disease largely relies on early-phase clinical trials, often involving heterogeneous populations. Covalent BTKi (cBTKi), including ibrutinib, zanubrutinib, and acalabrutinib, remain the cornerstone of R/R WM therapy, with varying safety and efficacy profiles. Resistance to cBTKi, frequently associated with the BTK C481 mutation, confers poor survival outcomes. The development of non-covalent BTKi (ncBTKi) and BTK degraders as promising alternatives. In this setting, the molecular profile-particularly mutations in MYD88, CXCR4, and TP53-plays a pivotal role in predicting treatment response and prognosis. BCL-2 inhibitors, such as venetoclax, are also under investigation. A phase II trial of venetoclax monotherapy demonstrated encouraging response rates in heavily pretreated patients, underscoring its potential in BTKi-resistant or intolerant cases. Additional novel therapies under evaluation include proteasome inhibitors, PI3K inhibitors, and immunotherapeutic approaches like CAR-T cells and bispecific antibodies. While early results are promising, larger studies are needed to validate these strategies. In addition, consolidation or salvage with hematopoietic stem cell transplantation could be considered in young heavily pretreated patients, especially in the context of BTKi refractoriness. It is therefore important to underline that given the chronic, relapsing course of WM, personalized treatment sequencing-accounting for comorbidities and prior therapies-is essential for optimizing outcomes. In conclusion, although significant advancements have been made in the management of R/R WM, continued research through randomized trials and biomarker-driven approaches is critical for refining the treatment strategies and improving long-term survival in this challenging disease.
1 Introduction
Waldenstrom Macroglobulinemia (WM) is a subtype of Non-Hodgkin Lymphoma that primarily affects elderly individuals and typically follows an indolent course (1). These features allow to carefully plan the sequencing of therapies, considering each patient’s distinctive factors, such as tolerability, comorbidities and age. However, a small subset of patients affected by lymphoplasmacytic lymphoma (LPL)/WM experiences a more severe disease course, characterized by lower response rates and inferior tolerability to standard frontline therapies (2). These cases are usually, but not always, associated with advanced age at diagnosis, extranodal involvement and adverse molecular or cytogenetic features (3–6).
For the first-line treatment, both chemoimmunotherapy regimens and Bruton’s Tyrosine Kinase (BTK) inhibitors are well tolerated and widely used, demonstrating high response rates and favorable long-term outcomes, as demonstrated by phase II trials and indirect comparisons (7, 8). In contrast, current evidence concerning second-line and later therapies comes primarily from Phase I/II clinical trials, which often include heterogeneous patient populations in terms of clinical, molecular, and prior treatment characteristics. In this evolving landscape, multiple agents have been tested both in frontline and subsequent lines however there is still a lack of prospective randomized studies validating clinical decisions. Nevertheless, it has been demonstrated that targeted therapies may contribute to a chemo-free treatment approach particularly beneficial for patients who are intolerant or refractory to conventional chemotherapy (9).
This review aims at providing a comprehensive overview of WM management, with a particular focus on advanced-line treatment strategies. Given the efficacy of frontline therapies and the aging WM population, the need for a well-planned treatment sequencing is becoming increasingly relevant. Thus, it is emphasized that a modern WM management must consider to balance patient-tailored approaches with a wise usage of novel agents.
2 Disease characteristics
LPL is a malignant clonal disorder of memory B cells, characterized by a distinctive bone marrow infiltration pattern that differentiates it from monoclonal gammopathy of undetermined significance. In the majority of cases, a circulating serum monoclonal IgM component is detectable, fulfilling the diagnostic criteria for WM. However, in a small subset of patients (5–10%), the monoclonal component is of non-IgM type (LPL non-IgM) (10). Additionally, current classifications recognize other rare LPL subtypes, including cases without a detectable monoclonal component or those presenting as exclusively extramedullary disease (11).
Most patients harbors the L265P mutation in the MYD88 gene, while nearly half of WM cases exhibit mutations in the CXCR4 gene. To date, over 40 different CXCR4 mutations have been identified, with the S338X mutation being the most common (12, 13).
Both MYD88 and CXCR4 play crucial roles in the Toll-like receptor (TLR) signaling pathway, ultimately influencing NF-κB activation. It is well established that the mutational status of these genes significantly impacts treatment response, particularly to Bruton’s tyrosine kinase inhibitors (BTKi).
Additionally, TP53 mutations and/or 17p deletions have been associated with adverse outcomes and increased chemoresistance, consistent with findings in other hematologic malignancies (14).
No cytogenetic aberrations have been definitively established as disease-defining in WM. However, 6q deletion has been associated with the inflammatory subtype of WM and has been linked to adverse clinical outcomes (15, 16). The complexity of the karyotype appears to increase with advancing age at diagnosis (4). Recently, novel subtypes of WM have been identified through integrative data studies, describing distinct molecular and clinical subtypes of the disease (17).
In line with this, multi-omics approaches are being explored across different referral centers.
The signs and symptoms of WM are often related to the presence of the paraprotein, leading to autoimmune hemolytic anemia, neuropathy, or cryoglobulinemia, or to bone marrow infiltration, resulting in cytopenias (2). In a minority of cases splenomegaly and lymphadenopathy may be present. Life expectancy in symptomatic WM ranges from 5 to 15 years, depending on the IPSSWM risk score, with a median age at diagnosis of approximately 70 years (2).
3 Frontline therapy
Historically, frontline treatment for WM has been based on the combination of a chemotherapy agent and an anti-CD20 monoclonal antibody. The choice to use Bendamustine-Rituximab (BR) or Rituximab-Cyclophosphamide-Dexamethasone (DRC) largely depends on local policies and patient tolerability (18, 19). While no direct comparison between these regimens has been conducted, real-world data suggest better outcomes with the BR regimen, despite its lower feasibility and more frequent need for dose adjustments (8). These regimens appear unaffected by the mutational status of MYD88 and CXCR4 (7). However, recent studies indicate that WM patients with TP53 mutations are less responsive to conventional chemoimmunotherapy. In such cases, a BTKi until disease progression is the preferred approach. Similarly, BTKi therapy is recommended for WM patients who are ineligible for chemoimmunotherapy (14, 20). Fitness to chemotherapy, albeit it has not been precisely defined and therefore validated in prospective studies in WM, generally is defined by an age < 80 years and no significant comorbidities and organ dysfunction (21). Given these insights, an accurate diagnostic workup, including assessment of MYD88, CXCR4 and TP53 mutational status, is highly recommended, as recently outlined in a guideline paper (9).
Currently, the most promising approaches under consideration in clinical trials are focused on the combination of BTKi with chemoimmunotherapy, IMIDs, or targeted agents. One such study, led by the Canadian group for WM, investigates the role of 6 cycles of BR, followed by 1 year of Acalabrutinib in WM patients (22, 23).
Similarly, Xiong et al. designed a Phase II clinical trial to investigate the effect of 6 cycles of BR combined with 12 months of Zanubrutinib (24).
Along the same line, Buske et al. included Bortezomib, Ibrutinib and Rituximab for 6 cycles, followed by 24 months of maintenance with Rituximab plus Ibrutinib. This regimen led to rapid, deep responses, though it was associated with a high mortality rate, likely due to COVID-19 infections during pandemic era (25).
A randomized ongoing trial comparing Carfilzomib in combination with Ibrutinib until disease progression, versus Ibrutinib monotherapy in both frontline and relapsed settings is currently recruiting (26).
Lastly, Castillo et al. conducted a Phase II prospective trial to evaluate the combination of Ibrutinib and the BCL2 inhibitor (BCL2i) Venetoclax in previously untreated WM. This trial excluded MYD88 wild-type patients. Preliminary results were promising in terms of response rates but the study was prematurely closed due to a 9% incidence of ventricular arrhythmias, including two grade 5 AEs whose cause is still to be determined (27, 28).
4 Current evidence for the management of relapsed/refractory WM cases
4.1 BTKi and BCL2i based clinical trials
4.1.1 Bruton kinase inhibitors
BTKi have demonstrated a favorable safety, tolerability, and efficacy profile. These inhibitors are now considered the standard of care for relapsed/refractory (R/R) WM, as well as in the frontline setting for patients who are not fit for standard chemoimmunotherapy (29, 30). Covalent BTK inhibitors such as Ibrutinib, Zanubrutinib, Acalabrutinib, and Orelabrutinib, bind to Cys481 (C481), which is the active site of BTK. This binding blocks the activation of BTK and suppresses its downstream signaling. Although this class of BTKi is effective in WM and other B cell malignancies, both primary and acquired resistance to these compounds is not uncommon. Progression of WM during BTKi therapy due to mutations in the binding site has been described and is one of the main mechanisms of acquired resistance (31, 32). It is known that BTKi-refractory WM cases represent a subgroup of patients with unfavorable prognosis and limited treatment options, as shown in several real-world studies. These patients, therefore, are the one that might benefit the most by the use of novel compounds, such as non-covalent BTKi, Bcl2 inhibitors or BTK degraders (33).
In the relapsed setting, the efficacy of Zanubrutinib was tested in the ASPEN trial (30) (Table 1).
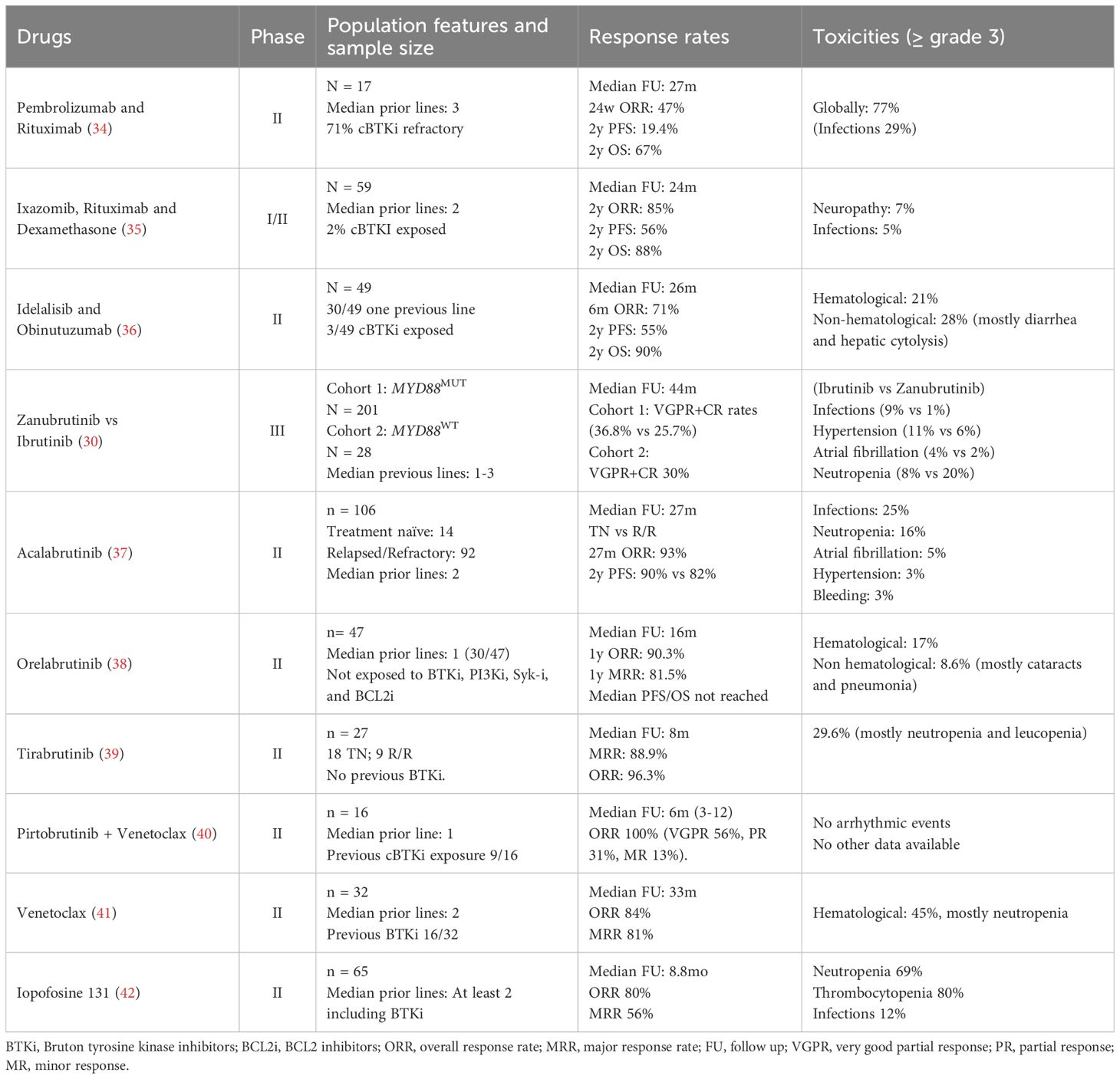
Table 1. Ongoing and concluded trials with novel treatment approaches in WM.
In cohort 1 of the ASPEN trial, 201 patients with treatment-naïve and relapsed/refractory MYD88L265P WM were randomized to receive either Zanubrutinib or Ibrutinib. The CXCR4 mutational status was comparable between the two groups. The results showed that the overall response rate (ORR) was 94% for Zanubrutinib and 95% for Ibrutinib, while the major response rate (MRR) was 80% and 81%, respectively, showing similar efficacy between the two agents. However, Zanubrutinib demonstrated a higher proportion of very good partial responses (VGPRs) (36%) compared to Ibrutinib (25%). Regarding safety, Grade 3/4 hypertension was more common in patients on Ibrutinib (11% vs. 6%), as well as infections (9% vs. 1%). On the other hand, neutropenia occurred more frequently in patients treated with Zanubrutinib (20% vs. 9%). No other significant safety differences were observed between the two agents. These findings suggest that both Zanubrutinib and Ibrutinib are highly effective in treating WM cases harboring MYD88 mutation, with Zanubrutinib offering a higher rate of VGPRs and a potentially better safety profile overall.
In cohort 2 of the ASPEN trial, Zanubrutinib demonstrated significant activity in patients with MYD88WT (wild-type) WM. The overall response rate (ORR) was 81%, and the major response rate (MRR) was 65%. Notably, 30% of patients with MYD88WT achieved a very good partial response (VGPR). These results highlight that Zanubrutinib is also effective in MYD88WT WM patients, providing meaningful clinical responses similar to those seen in MYD88MUT cases (9, 30). Furthermore, a subsequent biomarker analysis demonstrated superior efficacy in terms of PFS and MRR, in the TP53MUT R/R WM cohort treated with Zanubrutinib vs Ibrutinib (14).
Moving beyond the first generation of BTKi, acalabrutinib was tested in 92 relapsed/refractory (R/R) WM patients, with a median of 2 prior lines of therapy. The treatment demonstrated a 2-year progression-free survival (PFS) rate of 82%. The most frequent adverse events observed were infections of grade 3 or higher (25%), G3 neutropenia (16%), bleeding and cardiovascular events (5%) (37).
The significantly high rate of adverse events associated with first generation BTKi have led Shadman et al. to explore the potential role of Zanubrutinib after Ibrutinib as alternative BTKi, so that the treatment with a BTKi could continue while minimizing toxicities. The study highlighted the main reasons for Ibrutinib treatment discontinuation, including fatigue, arthralgia, hypertension, rash, and atrial fibrillation, which were the most commonly reported adverse events. Remarkably, these issues did not recur after patients switched to Zanubrutinib. Furthermore, Zanubrutinib therapy was able to maintain disease control in 93.8% of the cohort, suggesting that it could serve as a viable alternative treatment for those patients who are intolerant to Ibrutinib or Acalabrutinib, thus allowing to continue efficacious BTK-targeting with fewer side effects (43).
Orelabrutinib, another covalent BTKi, has demonstrated very promising results in a study after a median 1-year follow-up, with an Overall Response Rate (ORR) of 90.3% and a Major Response Rate (MRR) of 81.5%. The median duration of major response has not yet been reached but sustained responses were observed in 91.6% of patients at 12 months. Regarding the safety profile, the most frequent Grade 3 adverse events (AEs) were hematological toxicities, occurring in 17% of patients, mainly thrombocytopenia and neutropenia. Additionally, cataracts and pneumonia were reported, each in 4.3% of patients. The trial involved adult patients with relapsed/refractory WM who had adequate organ function and blood counts. Patients who had previously received BTKi, PI3K inhibitors, Syk inhibitors, or BCL2 inhibitors were excluded from the study. The median number of prior lines of therapy for these patients was 1 (30/47 patients) (38).
Tirabrutinib, a second-generation covalent BTKi, offers greater selectivity compared to Ibrutinib. Sekiguchi et al. conducted a multicenter, phase II study to evaluate its efficacy in treatment-naïve or relapsed/refractory WM patients. Patients were excluded if they had previously received another BTKi with a median of 2 prior lines reported. The study demonstrated impressive results with an ORR of 96.3% and MRR of 88.9%, meeting the primary endpoint despite the relatively short follow-up period of 30–35 weeks. Grade 3 adverse events (AEs) were primarily hematological, with neutropenia and leucopenia being the most commonly observed. Notably, 12 out of 27 patients in the cohort discontinued treatment due to AEs, most of which were skin-related (though not exceeding Grade 3 severity) (39).
The role of these latter two compounds in the current therapeutic algorithm is still under investigation. Since they were not tested in patients previously exposed to BTKi, and the follow-up is relatively short, it’s difficult to draw definitive conclusions regarding their long-term efficacy and safety. Further studies and extended follow-up are needed to better understand their place in treatment strategies for WM patients especially when BTKi exposed.
4.1.2 Future perspectives in BTK inhibition
Non-covalent BTKi bind to their target independently from the C481 site, offering a potential alternative for patients who become resistant to covalent BTKi due to C481 mutations. The Phase 1/2 BRUIN trial evaluated the efficacy of Pirtobrutinib, a non-covalent BTKi, in previously treated B-cell malignancies, including 26 patients with WM. The eligibility criteria required patients exposed at least two prior lines of therapy, with 18 out of the 26 having previously been treated with a covalent BTKi. The overall response rate (ORR) in the WM sub-population was 68% and the response seemed to be influenced by a prior exposure to BTKi. Pirtrobrutinib demonstrated a very favorable safety profile, with a lower rates of class-specific toxicities, particularly atrial arrhythmias and major bleeding as compared to covalent BTKi. This makes Pirtobrutinib a promising option for patients with covalent BTKi resistance, especially those harboring mutations at C481 site (44).
Ongoing trials are exploring the potential of novel BTKi compounds, including Nemtabrutinib, an orally bioavailable, non-covalent BTKi. A first-in-human Phase I study, conducted by Woyach et al. (NCT03162536), has demonstrated its favorable safety profile and preliminary efficacy in relapse/refractory B-cell malignancies (45). Further studies are needed to define its role in WM, particularly in patients with prior BTKi exposure or resistance to covalent BTKi. A Phase II trial (NCT04728893) is currently ongoing to evaluate the efficacy and safety on Nemtabrutinib in B-cell malignancies, including relapsed/refractory WM, in patients previously exposed to chemoimmunotherapy and BTKi (46). The results of this study will help clarify Nemtabrutinib’s role in BTKi-resistant WM cases and its potential as an alternative therapeutic option. Table 2.
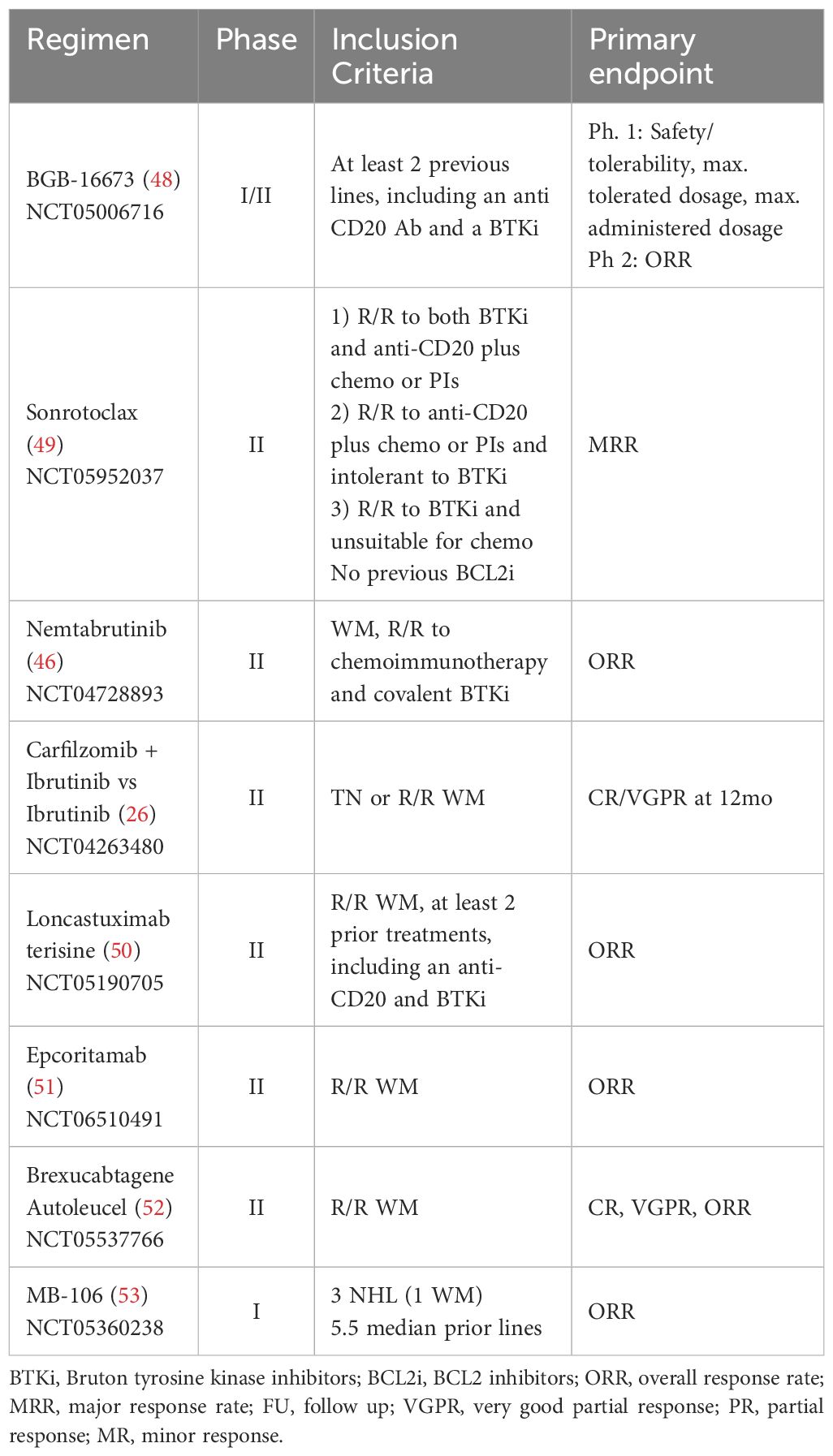
Table 2. Ongoing trials.
BGB-16673 is a novel molecule designed to degrade BTK by binding both BTK and E3 ligase, leading to BTK degradation through ubiquitination. In preclinical models it has demonstrated activity against both wild-type BTK and BTKi resistant mutant proteins, including those resistant to covalent and non-covalent BTKi. A first-in-human phase I/II trial, CaDAnCe-101, is currently ongoing to evaluate its safety, tolerability and optimal dosing in patients with relapsed/refractory B-cell malignancies, including WM. Eligible patients must have relapsed WM with at least 2 prior lines of therapy, including an anti-CD20 antibody and a covalent BTKi. Preliminary data, presented at the 2024 ASH meeting and, more recently, at EHA 2025 and 18-ICML meetings (47), included a cohort of 22 patients with a median age of 73 (range: 56–81 years) and a median number of prior therapy lines of 3.5 (range: 2-11) (48). In terms of safety and tolerability, 95% of patients experienced any-grade treatment-emergent adverse events (TEAEs). The most frequent grade 3 or higher AE was neutropenia (23%), while bruises and diarrhea were common but of lesser severity. Severe but rare AEs included three cases of grade 3 or higher infections and two deaths related to disease progression. Notably, no patients experienced atrial fibrillation, hypertension, febrile neutropenia or major hemorrhage, which are commonly associated with BTKi. Regarding efficacy, 21 patients received enough therapy to be response-evaluable, achieving an ORR of 90% and a MRR of 81%, suggesting strong antitumor activity with an acceptable safety profile. These early findings suggest promising activity, and further results will determine its potential role in the WM treatment landscape.
4.1.3 BCL2 inhibitors
Venetoclax, an oral BCL2i, is a well-established therapeutic option for chronic lymphocytic leukemia (CLL) and acute myeloid leukemia (AML). However, its role in other B-cell malignancies, including WM, remains to be fully defined. Castillo et al. conducted a multicenter, prospective phase II trial (NCT02677324) to evaluate the safety and the efficacy of Venetoclax monotherapy in relapsed/refractory WM (41). The study included 32 patients, 16 of whom had prior exposure to BTKis. All patients in the study had MYD88MUT and 17 were also CXCR4MUT. Venetoclax was administered orally at a daily dose of 800 mg for 2 years, with an initial ramp-up phase. The ORR and MRR were 84% and 81%, respectively, with lower response rates observed in refractory patients compared to those who had relapsed, as well as in individuals who had undergone extensive prior treatment (≥ 3 lines of therapy). Prior exposure to covalent BTKi was associated with a longer time to response (4.5 vs 1.4 months). The most common G3 or higher AE was neutropenia, occurring in 45% of patients.
Sonrotoclax is a second-generation BCL2i that has demonstrated the ability to overcome the G101V mutation in BCL2, showing higher selectivity in patients with chronic lymphocytic leukemia (49). This agent has demonstrated a favorable safety profile across all dose levels and strong antitumor efficacy in preliminary data from a phase 1 study conducted by Soumerai et al. (54) Currently, a phase 2 study (NCT05952037) is underway to evaluate the safety and efficacy of Sonrotoclax monotherapy in relapsed/refractory WM (55). Notably, patients with prior exposure to BCL2i were excluded from this study.
4.2 Combination therapies
Unlike in CLL, the combination of BTKi and BCL2i is not yet approved for use in WM. A Phase II trial (NCT05734495) led by Castillo et al. is currently enrolling patients to evaluate the efficacy and safety of a fixed-duration therapy combining Pirtobrutinib and Venetoclax in previously treated WM (40). The treatment schedule includes one cycle of Pirtobrutinib monotherapy, followed by a ramp-up phase of Venetoclax starting in cycle 2, with full-dose combination therapy administered from cycle 3 to 24. Preliminary data presented at the 2024 ASH meeting showed promising results in a cohort of 16 patients, with a median age of 67 years and a median of one prior line of treatment. Regarding disease characteristics, 14 patients were MYD88MUT, 6 were CXCR4MUT and 1 was TP53MUT. With a median follow-up of 6 months (range: 3-12), the ORR was 100%, including 9 VGPR, 5 PR and 2 mR. Lower VGPR rates were observed in patients with CXCR4MUT or prior BTKi exposure. Disease progression occurred in two patients within the first 6 months, both with MYD88WT WM. Regarding safety, no arrhythmias have been reported to date, and no severe cardiac events have been described. While the combination of targeted therapies represents a promising approach in WM, the overall safety profile remains to be fully characterized.
4.3 Proteasome and PI3K inhibitors
Another approach under investigation is related to the usage of alternative proteasome inhibitors instead of bortezomib with the aim to spare neurotoxicity such as the combination of Ixazomib, Rituximab, Dexamethasone.
This regimen was evaluated in a relapsed WM setting between 2015 and 2019, involving 59 patients with a median of two prior lines of therapy. Ixazomib was administered for eight cycles, while Rituximab was maintained for two years. At one-year follow up, the ORR was 85%, while at two years, the PFS and OS rates were 56% and 88%, respectively. The toxicity profile was generally acceptable, with grade 3 infections occurring in 5% of patients and grade 3 neuropathy in 7% of them. Overall, only 25 patients concluded the full treatment course (35).
PI3K/Akt/mTOR pathway and its role in the lymphomagenesis has led to the conceiving of a trial using Idealalisib in combination with the anti-CD20 monoclonal antibody Obinutuzumab. This phase II clinical trial enrolled 49 patients between 2017 and 2018, with Obinutuzumab administered for six cycles and Idelilasib given twice daily for up to two years. Most patients had received only one prior line of treatment, with limited prior exposure to cBTKI (only three patients). The cohort had unfavorable genetic features, with 56% of cases harboring CXCR4MUT and 24% TP53MUT. At six months, the ORR was 71%, while the two-year PFS rate and OS rates were 55% and 90%, respectively. However, only 9 patients completed maintenance therapy, primarily due to grade 3–4 toxicities including hematologic adverse events (21%), and non-hematologic toxicities (24%), notably diarrhea and hepatic cytolysis (36).
4.4 Immunotherapy based clinical trials
4.4.1 Checkpoint inhibitors
Ansell, Jalali and colleagues studied the PD-1/PD-L1 axis in WM highlighting its regulatory role in the tumor microenvironment and its potential as a therapeutic target (56).
In this regard the UK group recently conducted a Phase II clinical trial evaluating a combination of Pembrolizumab and Rituximab in heavily pretreated WM patients (median of three prior lines), including 71% who were refractory to cBTKi. The treatment followed a 3-week cycle, allowing up to 18 cycles. Among the 17 enrolled patients, 12 discontinued therapies, primarily due to disease progression (6/12) and adverse events (3/12). The median follow up was of 27 months. At six months, the ORR was 47%, but the PFS rate dropped significantly to 19.4% by the second year. Adverse events occurred in 94% of patients, with 77% experiencing grade 3 events—most commonly infections (29%)—though no autoimmune complications were reported (34).
4.4.2 T-cell engagers: CAR-T and bispecific antibodies
Regarding CD19-directed CAR-T cell therapies which have shown strong efficacy in other NHL subtypes are now being tested also in WM; specifically a phase II study (ZUMA-25) evaluates the efficacy of Brexucabtagene Autoleucel in rare B-cell malignancies including WM but results are not available yet (52). In addition, at the 2023 ASH meeting, Shadman et al. presented preliminary data on MB-106, a third-generation CD20-directed CAR-T therapy, for the treatment of R/R indolent NHL. At the time of abstract presentation, the study had enrolled only one patient with WM and two with follicular lymphoma (FL), all of whom were heavily pretreated, with a median of 5.5 prior lines of therapy. Given the limited sample size, it is too early to draw conclusions regarding safety and efficacy. However, dose escalation is ongoing to establish the recommended phase 2 dose for a planned pivotal trial in WM (53).
Finally, as for other T-cell engagers, Epcoritamab is now being tested in a prospective phase II trial to determine its efficacy in previously treated WM (51).
4.5 Antibody drug conjugates
Preliminary results on the role of Loncastuximab Tesirine, an anti-CD19 antibody drug-conjugate, in the treatment of R/R WM were presented at the 2024 ASH meeting. A phase II trial (NCT05190705) conducted by Castillo et al. is currently enrolling patients with R/R WM who have undergone at least two prior lines of therapy, including rituximab and a BTKi. At the time of data presentation, 7 patients had been enrolled, with a median age of 70 years (range: 53-77) and a median of four prior lines of therapy (range: 2-5). All patients carried the MYD88MUT, while 6 out of 7 also had CXCR4MUT and 4 out of 7 had TP53MUT. The treatment regimen consists of six cycles, administered every 28 days. Thus far, four patients have completed all six cycles, two remain on therapy and one experienced disease progression after the first cycle. Among the six patients who did not progress, all achieved a response (3 VGPR, 3 PR), translating in an ORR of 86%. The safety profile was consistent with findings in other settings in which Loncastuximab Tesirine has been tested, with skin toxicity being the most common adverse event, followed by edema (including one G3 case), transient cytopenias and asymptomatic gGT elevation. Despite the short follow up period, these early results suggest promising efficacy in a small cohort of heavily pretreated patients with high-risk molecular features (50).
4.6 New compounds with novel mechanism of action
The relapsing nature of indolent lymphoproliferatives disorders, such as Waldenstrom Macroglobulinemia, underscores the need for novel therapeutic strategies—either through the development of next-generation agents targeting established pathways or the identification of new mechanisms to enhance treatment efficacy.
Iopofosine I-131 is a radiopharmaceutical consisting of a lipid raft-targeting phospholipid ether covalently bound to 131I, a beta-emitting radioisotope. A phase 2 trial conducted by Ailawadhi et al. evaluated its safety and efficacy in patients with previously treated WM (≥ 2 prior lines of therapy). The study enrolled 65 patients, with a median age of 70 years, and a median of four prior lines of therapy, 56% of whom were BTKi refractory. MYD88 and CXRC4 gene mutations were identified in 71% and 9% of cases, respectively. Preliminary results demonstrated an MRR of 56.4% and an ORR of 80%, with the median DOR not yet reached at a median follow-up of 8.8 months. The estimated 18-month PFS was 72%. Regarding safety, grade ≥3 adverse events were predominantly hematologic, with thrombocytopenia being the most frequent (80%), followed by neutropenia (including 10.8% febrile neutropenia) and anemia (42).
4.7 The role of stem cell transplantation in the era of novel drugs
A comprehensive analysis by Kyriakou et al. using data from the EBMT registry was conducted to assess the role of stem cell transplantation in WM management. From 2000 to 2021, a total of 772 patients with WM underwent autologous hematopoietic stem cell transplantation (HSCT), while 330 received allogeneic HSCT. The study highlighted the efficacy and safety of both approaches, with notably better outcomes observed in the autologous HSCT group. For patients receiving autologous HSCT, estimated overall survival (OS) rates at 2, 5, and 10 years were 89.4%, 70.4%, and 55.3%, respectively, with corresponding progression-free survival (PFS) rates of 68.2%, 46.9%, and 31.2%. In contrast, allogeneic HSCT resulted in lower OS rates of 62.9%, 54.0%, and 47.3%, and PFS rates of 58.7%, 44.6%, and 34.7% over the same time periods.
It is important to note that patients undergoing allogeneic HSCT were typically more heavily pretreated, with 68% having received three or more prior lines of therapy, including 21% who had previously failed auto-HSCT. The safety profile of the two approaches also differed significantly, with allogeneic HSCT being associated with complications such as acute and chronic graft-versus-host disease, which are absent in the autologous setting. Additionally, non-relapse mortality was considerably lower in the autologous HSCT cohort compared to the allogeneic group (7.1% versus 27.98% at 10 years, respectively) (57).
In conclusion, these findings sustain the role of autologous HSCT as a consolidative strategy only in very selected WM cases, highlighting the need for a precise patient choice followed by an appropriate risk stratification.
5 Conclusions: future perspectives for the management of relapsed/refractory WM
In this review, we provided an overview of novel therapeutic combinations in WM, with a focus on second-line and advanced treatment settings and emphasizing the evolving role of targeted therapies.
The growing body of evidence supports the efficacy and safety of next-generation covalent BTKi, along with the potential to transition from covalent to non-covalent BTKi to circumvent resistance mechanisms. These regimens not only offer durable disease control but also reduce hospitalization rates, despite requiring continuous administration until progression. As a result, long-term follow-up data on BTKi use in WM continue to yield promising and consistent outcomes. Similarly, BCL2i have demonstrated strong efficacy in relapsed/refractory WM, with a median follow-up of three years and an overall manageable safety profile. Given their complementary mechanisms of action, the combination of BTKi and BCL2i is now being explored, offering a synergistic therapeutic approach that may further improve treatment outcomes in this setting. On the other hand, the combination of targeted agents, for which the mechanisms of the synergistic/cooperative effects are not fully understood, may render difficult to unravel potential ways of resistance adopted by LPL/WM cells against the individual drugs.
A chemotherapy-free approach is generally preferred in the second line setting, as WM patients often experience relapse years after their initial treatment. With time, they may develop additional comorbidities and decreased fitness, making them less suitable for another exposure to chemotherapy. Also, it is recommended to reassess disease’s molecular status, especially seeking for TP53 mutations, as they may confer to the disease an intrinsic therapy-resistance. Nevertheless, in selected cases, chemoimmunotherapy may still be considered, particularly after a first-line BTKi-based regimen, depending on patients’ characteristics and specific disease manifestations (i.e. WM-related amyloidosis, renal involvement and/or need for rapid debulking). Unfortunately, there is limited data available on the sequencing of therapies in such cases, and real-world studies exploring this issue are needed. Furthermore, the new categorization of WM subtypes using multiomics approaches should be incorporated into clinical practice to better stratify patients based on their disease subtype and responsiveness to different therapies. In this regard, clinical trials or reanalysis of existing studies to assess drug responsiveness according to disease subtype are warranted.
In this complex landscape, the role and significance of monitoring minimal residual disease (MRD) remain controversial. Impressive MRD negativity rates have been observed in recent trials like ECWM-1, suggesting its potential utility in assessing responses in WM patients treated with therapies that do not follow a fixed-duration protocol. However, whether achieving MRD negativity early in the course of a typically indolent disease is clinically meaningful remains an open question. A clear standardization of MRD testing and interpretation needs to be completed, especially in the relapsed/refractory setting.
As previously mentioned, new target agents such as Iopofosine-131 and Loncastuximab Tesirine are showing promising efficacy, although follow-up times are not yet long enough to draw definitive conclusions. In this context, it remains uncertain whether targeting the microenvironment is a viable approach, given the poor tolerability and response outcomes associated with anti-PD1 therapies. Additionally, there is a paucity of data on T-cell engagement therapies and the results of ongoing clinical trials are eagerly awaited.
In this complex scenario, the EBMT registry data on ASCT in WM span a broad time frame (since 2000) and do not account for prior treatments with targeted therapies or immunotherapies. Stem cell transplantation should not be entirely excluded from the treatment options in WM but should be reserved for carefully selected, fit patients with multi-refractory and BTKi-exposed disease, particularly in centers with significant experience in HSCT, and only after achieving a satisfactory disease response.
In conclusion, while chemotherapy has not completely disappeared in the second line setting, the emerging combinations of second-generation inhibitors and/or non-covalent BTKi with targeted agents have the potential to significantly modify the treatment algorithm. Oral BCL2i represent a valid option in advanced lines, especially in patients with unfavorable molecular profiles or prior BTKi exposure. The role of MRD needs further exploration, with promising activity for the future, particularly with the widespread use of continuous therapies. In this setting, TP53 gene status reassessment and the search for BTK resistance mutations should be integrated, not only at the initial diagnosis but also at the time of first relapse focusing in BTKi-refractory patients (58).
Author contributions
ND: Writing – review & editing, Resources, Writing – original draft, Conceptualization. GL: Resources, Writing – review & editing, Conceptualization, Writing – original draft. MD: Writing – review & editing, Supervision. MC: Supervision, Writing – review & editing. GS: Writing – review & editing, Supervision. LT: Writing – review & editing, Supervision. FP: Supervision, Writing – review & editing, Writing – original draft, Resources, Conceptualization.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Open Access funding provided by Università degli Studi di Padova | University of Padua, Open Science Committee.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Danesin N, Lo Schirico M, Scapinello G, Grassi A, Riva M, Berno T, et al. Waldenström Macroglobulinemia in very elderly (≥75-year-old) patients: A 33-year-retrospective cohort study in an Italian university hospital. Hemasphere. (2023) 7:e964. doi: 10.1097/HS9.0000000000000964
2. Zanwar S and Kapoor P. Diagnosis and risk stratification in Waldenström Macroglobulinemia. J Natl Compr Canc Netw. (2024) 22:e247024. doi: 10.6004/jnccn.2024.7024
3. Treon SP, Xu L, Guerrera ML, Jimenez C, Hunter ZR, Liu X, et al. Genomic landscape of Waldenström Macroglobulinemia and its impact on treatment strategies. J Clin Oncol. (2020) 38:1198–208. doi: 10.1200/JCO.19.02314
4. Danesin N, Bonaldi L, Martines A, Nalio S, Bertorelle R, Compagno S, et al. Impact of the presence and number of chromosomal abnormalities on the clinical outcome in Waldenström Macroglobulinemia: a monocentric experience. Ann Hematol. (2024) 103:2961–8. doi: 10.1007/s00277-024-05770-4
5. Varettoni M, Boveri E, Zibellini S, Tedeschi A, Candido C, Ferretti VV, et al. Clinical and molecular characteristics of lymphoplasmacytic lymphoma not associated with an IgM monoclonal protein: A multicentric study of the Rete Ematologica Lombarda (REL) network. Am J Hematol. (2019) 94:1193–9. doi: 10.1002/ajh.25600
6. Danesin N, Scapinello G, Del Prete D, Naso E, Berno T, Visentin A, et al. When Waldenström Macroglobulinemia hits the kidney: Description of a case series and management of a “rare in rare” scenario. Cancer Rep (Hoboken). (2024) 7:e2062. doi: 10.1002/cnr2.2062
7. Kapoor P, Paludo J, and Abeykoon JP. Frontline management of Waldenström Macroglobulinemia with chemoimmunotherapy. Hematol Oncol Clin North Am. (2023) 37:671–87. doi: 10.1016/j.hoc.2023.04.003
8. Autore F, Tedeschi A, Benevolo G, Mattiello V, Galli E, Danesin N, et al. First-line treatment of Waldenström’s Macroglobulinemia in Italy: A multicenter real-life study on 547 patients to evaluate the long-term efficacy and tolerability of different chemoimmunotherapy strategies. Am J Hematol. (2025) 100:189–91. doi: 10.1002/ajh.27524
9. Treon SP, Sarosiek S, and Castillo JJ. How I use genomics and BTK inhibitors in the treatment of Waldenström Macroglobulinemia. Blood. (2024) 143:1702–12. doi: 10.1182/blood.2022017235
10. Castillo JJ, Itchaki G, Gustine JN, Meid K, Flynn CA, Demos MG, et al. A matched case-control study comparing features, treatment and outcomes between patients with non-IgM lymphoplasmacytic lymphoma and Waldenström Macroglobulinemia. Leuk Lymphoma. (2020) 61:1388–94. doi: 10.1080/10428194.2020.1719100
11. Alaggio R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IBO, Berti E, et al. The 5th edition of the world health organization classification of hematolymphoid tumours: lymphoid neoplasms. Leukemia. (2022) 36:1720–48. doi: 10.1038/s41375-022-01620-2
12. Treon SP, Xu L, Yang G, Zhou Y, Liu X, Cao Y, et al. MYD88 L265P somatic mutation in Waldenström’s macroglobulinemia. N Engl J Med. (2012) 367:826–33. doi: 10.1056/NEJMoa1200710
13. Hunter ZR, Xu L, Yang G, Zhou Y, Liu X, Cao Y, et al. The genomic landscape of Waldenstrom Macroglobulinemia is characterized by highly recurring MYD88 and WHIM-like CXCR4 mutations, and small somatic deletions associated with B-cell lymphomagenesis. Blood. (2014) 123:1637–46. doi: 10.1182/blood-2013-09-525808
14. Tam CS, Opat S, D’Sa S, Jurczak W, Lee HP, Cull G, et al. Biomarker analysis of the ASPEN study comparing Zanubrutinib with Ibrutinib for patients with Waldenström Macroglobulinemia. Blood Adv. (2024) 8:1639–50. doi: 10.1182/bloodadvances.2023010906
15. García-Sanz R, Dogliotti I, Zaccaria GM, Ocio EM, Rubio A, Murillo I, et al. 6q deletion in Waldenström Macroglobulinaemia negatively affects time to transformation and survival. Br J Haematol. (2021) 192:843–52. doi: 10.1111/bjh.17028
16. Elessa D, Debureaux PE, Villesuzanne C, Davi F, Bravetti C, and Harel S. Inflammatory Waldenström’s Macroglobulinaemia: A French monocentric retrospective study of 67 patients. Br J Haematol. (2022) 197:728–35. doi: 10.1111/bjh.18157
17. Mondello P, Paludo J, Novak JP, Wenzl K, Yang ZZ, Jalali S, et al. Molecular clusters and tumor-immune drivers of IgM monoclonal gammopathies. Clin Cancer Res. (2023) 29:957–70. doi: 10.1158/1078-0432.CCR-22-2215
18. Dimopoulos MA, Anagnostopoulos A, Kyrtsonis MC, Zervas K, Tsatalas C, Kokkinis G, et al. Primary treatment of Waldenström Macroglobulinemia with dexamethasone, rituximab, and cyclophosphamide. J Clin Oncol. (2007) 25:3344–9. doi: 10.1200/JCO.2007.10.9926
19. Laribi K, Poulain S, Willems L, Merabet F, Herbaux C, Roos-Weil D, et al. Long-term results of Waldenström Macroglobulinaemia treatment by bendamustine and rituximab: A study on behalf of the French Innovative Leukemia Organization (FILO). Br J Haematol. (2024) 204:2233–6. doi: 10.1111/bjh.19409
20. Buske C, Tedeschi A, Trotman J, García-Sanz R, MacDonald D, Leblond V, et al. Ibrutinib plus rituximab versus placebo plus rituximab for Waldenström’s Macroglobulinemia: final analysis from the randomized phase III iNNOVATE study. J Clin Oncol. (2022) 40:52–62. doi: 10.1200/JCO.21.00838
21. Tedeschi A, Tam CS, Owen RG, Buske C, Leblond V, Dimopoulos MA, et al. Health-related quality of life in patients with Waldenström Macroglobulinemia: results from the ASPEN trial. Future Oncol. (2024) 20:1789–98. doi: 10.1080/14796694.2024.2355079
22. Bendamustine, rituximab and acalabrutinib in Waldenstrom’s Macroglobulinemia (BRAWM)(2024). Available online at: https://clinicaltrials.gov/study/NCT04624906 (Accessed June 29, 2025).
23. A study of BR alone versus in combination with acalabrutinib in subjects with previously untreated MCL(2023). Available online at: https://clinicaltrials.gov/study/NCT04624906 (Accessed June 29, 2025).
24. A phase 2 clinical trial to evaluate zanubrutinib combined with BR (Bendamustine/Rituximab) regimen in subjects with newly-diagnosed Waldenström’s Macroglobulinemia (CZ-WM01). Available online at: https://clinicaltrials.gov/study/NCT05979948 (Accessed June 29, 2025).
25. Efficacy of first line B-RI for treatment naive Waldenström’s Macroglobulinemia(2024). Available online at: https://clinicaltrials.gov/study/NCT03620903 (Accessed June 29, 2025).
26. Efficacy and Safety of Carfilzomib in Combination With Ibrutinib vs Ibrutinib in Waldenström’s Macroglobulinemia (CZAR-1)(2024). Available online at: https://clinicaltrials.gov/study/NCT03620903 (Accessed June 29, 2025).
27. Castillo JJ, Branagan AR, Sermer D, Flynn CA, Meid K, Little M, et al. Ibrutinib and venetoclax as primary therapy in symptomatic, treatment-naïve Waldenström Macroglobulinemia. Blood. (2024) 143:582–91. doi: 10.1182/blood.2023022420
28. Tam CS, Allan JN, Siddiqi T, Kipps TJ, Jacobs R, Opat S, et al. Fixed-duration Ibrutinib plus venetoclax for first-line treatment of CLL: primary analysis of the CAPTIVATE FD cohort. Blood. (2022) 139:3278–89. doi: 10.1182/blood.2021014488
29. Treon SP, Tripsas CK, Meid K, Warren D, Varma G, and Green R. Ibrutinib in previously treated Waldenström’s Macroglobulinemia. N Engl J Med. (2015) 372:1430–40. doi: 10.1056/NEJMoa1501548
30. Tam CS, Opat S, D’Sa S, Jurczak W, Lee HP, Cull G, et al. A randomized phase 3 trial of Zanubrutinib vs Ibrutinib in symptomatic Waldenström Macroglobulinemia: the ASPEN study. Blood. (2020) 136:2038–50. doi: 10.1182/blood.2020006844
31. Gu D, Tang H, Wu J, Li J, and Miao Y. Targeting Bruton tyrosine kinase using non-covalent inhibitors in B cell Malignancies. J Hematol Oncol. (2021) 14:40. doi: 10.1186/s13045-021-01049-7
32. Tawfiq RK, Abeykoon JP, and Kapoor P. Bruton tyrosine kinase inhibition: an effective strategy to manage Waldenström Macroglobulinemia. Curr Hematol Malig Rep. (2024) 19:120–37. doi: 10.1007/s11899-024-00731-0
33. Muñoz J, Sarosiek S, and Castillo JJ. Managing ibrutinib-intolerant patients with B-cell Malignancies. Oncologist. (2023) 28:309–18. doi: 10.1093/oncolo/oyac260
34. Kothari J, Eyre T, Rismani A, Ediriwickrema K, Edwards D, Galani S, et al. PembroWM: A phase II trial to investigate the safety and efficacy of rituximab and pembrolizumab in relapsed/refractory Waldenström’s Macroglobulinaemia. Br J Haematol. (2024) 205:2273–81. doi: 10.1111/bjh.19706
35. Kersten MJ, Amaador K, Minnema MC, Vos JMI, Nasserinejad K, Kap M, et al. Combining ixazomib with subcutaneous rituximab and dexamethasone in relapsed or refractory Waldenström’s Macroglobulinemia: final analysis of the phase I/II HOVON124/ECWM-R2 study. J Clin Oncol. (2022) 40:40–51. doi: 10.1200/JCO.21.00105
36. Tomowiak C, Poulain S, Herbaux C, Perrot A, Mahé B, Morel P, et al. Obinutuzumab and idelalisib in symptomatic patients with relapsed/refractory Waldenström Macroglobulinemia. Blood Adv. (2021) 5:2438–46. doi: 10.1182/bloodadvances.2020003895
37. Owen RG, McCarthy H, Rule S, D’Sa S, Thomas SK, Tournilhac O, et al. Acalabrutinib monotherapy in patients with Waldenström Macroglobulinemia: a single-arm, multicentre, phase 2 study. Lancet Haematol. (2020) 7:e112–21. doi: 10.1016/S2352-3026(19)30210-8
38. Cao XX, Jin J, Fu CC, Yi SH, Zhao WL, Sun ZM, et al. Evaluation of Orelabrutinib monotherapy in patients with relapsed or refractory Waldenström’s Macroglobulinemia in a single-arm, multicenter, open-label, phase 2 study. EClinicalMedicine. (2022) 52:101682. doi: 10.1016/j.eclinm.2022.101682
39. Sekiguchi N, Rai S, Munakata W, Suzuki K, Handa H, Shibayama H, et al. A multicenter, open-label, phase II study of tirabrutinib (ONO/GS-4059) in patients with Waldenström’s Macroglobulinemia. Cancer Sci. (2020) 111:3327–37. doi: 10.1111/cas.14561
40. Castillo JJ, Sarosiek SR, Branagan AR, von Keudell G, Flynn CA, Budano NS, et al. A phase II study of pirtobrutinib and venetoclax in previously treated patients with Waldenström Macroglobulinemia: an interim analysis. ASH Annu meeting. (2024) 144(supplement 1):3011. doi: 10.1182/blood-2024-198297
41. Castillo JJ, Allan JN, Siddiqi T, Advani RH, Meid K, Leventoff C, et al. Venetoclax in previously treated Waldenström Macroglobulinemia. J Clin Oncol. (2022) 40:63–71. doi: 10.1200/JCO.21.01194
42. Ailawadhi S, Gavriatopoulou M, Peterson J, Ntanasis-Stathopoulos I, El-Haddad G, Grajales-Cruz A, et al. Iopofosine I 131 in previously treated patients with Waldenström Macroglobulinemia (WM): efcacy and safety results from the international, multicenter, open-label phase 2 study (CLOVER-WaMTM). ASH Annu meeting. (2024) 144(supplement 1):861. doi: 10.1182/blood-2024-200277
43. Shadman M, Flinn IW, Levy MY, Porter RF, Burke JM, Zafar SF, et al. Zanubrutinib in patients with previously treated B-cell Malignancies intolerant of previous Bruton tyrosine kinase inhibitors in the USA: a phase 2, open-label, single-arm study. Lancet Haematol. (2023) 10:e35–45. doi: 10.1016/S2352-3026(22)00320-9
44. Mato AR, Shah NN, Jurczak W, Cheah CY, Pagel JM, Woyach JA, et al. Pirtobrutinib in relapsed or refractory B-cell Malignancies (BRUIN): a phase 1/2 study. Lancet. (2021) 397:892–901. doi: 10.1016/S0140-6736(21)00224-5
45. Woyach JA, Stephens DM, Flinn IW, Bhat SA, Savage RE, Chai F, et al. First-in-human study of the reversible BTK inhibitor nemtabrutinib in patients with relapsed/refractory chronic lymphocytic leukemia and B-cell non-Hodgkin lymphoma. Cancer Discov. (2024) 14:66–75. doi: 10.1158/2159-8290.CD-23-0670
46. A phase 2 study to evaluate the efficacy and safety of MK-1026 in participants with hematologic Malignancies(2024). Available online at: https://www.clinicaltrials.gov/study/NCT04728893 (Accessed June 29, 2025).
47. Frustaci AM, Seymour JF, Cheah CY, Parrondo RD, Allan JN, Trotman J, et al. Updated efficacy & safety of BTK degrader BGB-16673 in patients (PTS) with replased/refractory Waldenström Macroglobulinemia (R/R WM): Ongoing phase 1 CaDAnCe-101 results. 18th ICML meeting. 43(S3) supplement. doi: 10.1002/hon.70093_147
48. Seymour JF, Tam CS, Cheah CY, Parrondo RD, Allan JN, Trotman J, et al. preliminary efficacy and safety of the Bruton tyrosine kinase degrader BGB-16673 in patients with relapsed or refractory Waldenström Macroglobulinemia: results from the phase 1 caDAnCe-101 study. ASH Annu meeting. (2024) 144(supplement 1):860. doi: 10.1182/blood-2024-199212
49. Liu J, Li S, Wang Q, Feng Y, Xing H, Yang X, et al. Sonrotoclax overcomes BCL2 G101V mutation-induced venetoclax resistance in preclinical models of hematologic Malignancy. Blood. (2024) 143:1825–36. doi: 10.1182/blood.2023019706
50. Castillo JJ, Treon SP, Flynn CA, Ramirez-Gamero A, Budano NS, Eurell AN, et al. A phase II trial of loncastuximab tesirine in patients with previously treated Waldenström Macroglobulinemia. ASH Annu meeting. (2024) 144(supplement 1):4404. doi: 10.1182/blood-2024-211573
51. Epcoritamab in previously treated WM. Available online at: https://clinicaltrials.gov/study/NCT06510491 (Accessed June 29, 2025).
52. Study of brexucabtagene autoleucel in adults with rare B-cell Malignancies (ZUMA-25). Available online at: https://clinicaltrials.gov/study/NCT05537766 (Accessed June 29, 2025).
53. Shadman M, Caimi PF, O’Brien SM, Reagan PM, Dezube B, Navaratnarajah P, et al. Efficacy and safety of a third generation CD20 CAR-T (MB-106) for treatment of relapsed/refractory indolent B-cell non-Hodgkin lymphoma: phase-1 results from a multicenter trial. ASH Annu meeting. (2023) 142(supplement 1):2102. doi: 10.1182/blood-2023-175007
54. Soumerai JD, Lasica M, Opat S, Cheah CY, Chan H, Verner E, et al. A phase 1 study with the novel B-cell lymphoma 2 (Bcl-2) inhibitor bgb-11417 as monotherapy or in combination with zanubrutinib (ZANU) in patients (Pts) with non-Hodgkin lymphoma (NHL) or waldenström macroglobulinemia (WM): preliminary data. ASH Annu meeting. (2022) 140(supplement 1):9326-7. doi: 10.1182/blood-2022-169664
55. Lee H-P, Opat S, Hrom J, Kliman DS, Marlton P, Liu P, et al. BGB-11417-203: An ongoing, phase 2 study of sonrotoclax (BGB-11417), a next-generation BCL2 inhibitor, in patients with Waldenström Macroglobulinemia. ASCO Annual Meeting. (2024) 42(supplement 16). doi: 10.1200/JCO.2024.42.16_suppl.TPS7090
56. Jalali S, Price-Troska T, Paludo J, Villasboas J, Kim HJ, Yang ZZ, et al. Soluble PD-1 ligands regulate T-cell function in Waldenstrom Macroglobulinemia. Blood Adv. (2018) 2:1985–97. doi: 10.1182/bloodadvances.2018021113
57. Kyriakou C, Fekom M, Khvedelidze I, Moukalled N, Serroukh YIM, Castagna L, et al. Long term outcomes of hematopoietic stem cell transplantation in patients with Waldenström’s Macroglobulinemia. Report from the lymphoma working party of the European society for blood and marrow transplantation (LWP EBMT). ASH Annu meeting. (2024) 144(supplement 1):3010. doi: 10.1182/blood-2024-197901
Keywords: Waldenstöm’s Macroglobulinemia, lymphoplasmacytic cells, non-Hodgkin lymphoma (NHL), BTK inhibition, B-cell lymphoma 2 inhibition (BCL2), target therapies
Citation: Danesin N, Leone G, D’Antiga M, Carraro M, Scapinello G, Trentin L and Piazza F (2025) The therapeutic perspective of relapsed/refractory Waldenström Macroglobulinemia: what comes next? Front. Hematol. 4:1624046. doi: 10.3389/frhem.2025.1624046
Received: 06 May 2025; Accepted: 23 June 2025;
Published: 16 July 2025.
Edited by:
Vittorio Del Fabro, Divisione Clinicizzata Di Ematologia Policlinico Di Catania, ItalyReviewed by:
Andrea Galitzia, Ospedale San Francesco, ItalySuzanne Arulogun, Guy’s and St Thomas’ NHS Foundation Trust, United Kingdom
Copyright © 2025 Danesin, Leone, D’Antiga, Carraro, Scapinello, Trentin and Piazza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Piazza, ZnJhbmNlc2NvLnBpYXp6YUB1bmlwZC5pdA==
†These authors have contributed equally to this work