 Nina Marie Birk1†
Nina Marie Birk1† Katrine Kielsen1,2,3*†
Katrine Kielsen1,2,3*† Özcan Met4,5Eva Kannik Haastrup6
Özcan Met4,5Eva Kannik Haastrup6 Thomas M. Hulen4Cecilie Ø. Madsen4,5
Thomas M. Hulen4Cecilie Ø. Madsen4,5 Torben Barington7,8Jonas Nielsen9
Torben Barington7,8Jonas Nielsen9 Kristian Schønning10Søren Lykke Petersen11‡
Kristian Schønning10Søren Lykke Petersen11‡ Marianne Ifversen1‡
Marianne Ifversen1‡- 1Department of Pediatrics and Adolescent Medicine, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
- 2Institute for Inflammation Research, Department of Rheumatology and Spine Diseases, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
- 3Department of Immunology and Microbiology, University of Copenhagen, Copenhagen, Denmark
- 4National Center for Cancer Immune Therapy, Department of Oncology, Copenhagen University Hospital, Herlev, Denmark
- 5Department of Health Technology, Technical University of Denmark, Kongens Lyngby, Denmark
- 6Cell Therapy Facility, The Blood Bank, Department of Clinical Immunology, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
- 7Centre for Cellular Immunotherapy of Haematological Cancer Odense (CITCO), Odense University Hospital and University of Southern Denmark, Odense, Denmark
- 8Department of Clinical Immunology, Odense University Hospital, Odense, Denmark
- 9Department of Intensive care, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark
- 10Department of Clinical Microbiology, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
- 11Department of Hematology, Copenhagen University Hospital Rigshospitalet, Copenhagen, Denmark
We report a case of severe encephalitis caused by human herpes virus 6 (HHV-6) following CD19 chimeric antigen receptor T (CAR-T) cell therapy. Rapid expansion of circulating T-lymphocytes and high HHV-6 viral load (4,500,000 DNA copies/mL) early after CAR-T infusion suggested HHV-6 transferal from autologous CAR-T cells. To investigate this hypothesis, we retrospectively analyzed cryo-preserved patient samples for HHV-6. HHV-6 was undetectable in the apheresis product, transduced CAR-T cells, and in vitro activated CAR-T cells. In conclusion, despite strong clinical suspicion, we found no evidence to substantiate the infused CAR-T cells as the source of the severe HHV-6 infection.
Introduction
Neurotoxicity is a well-known risk following chimeric antigen receptor T-cell (CAR-T) therapy. In particular, immune effector cell-associated neurotoxicity syndrome (ICANS) occurs shortly after CAR-T infusion with symptoms varying from difficulties in word finding, headache, confusion, and impaired fine motor skills to seizures, coma, and cerebral edema (1–3). Although ICANS has been associated with increased cytokine levels in cerebrospinal fluid (CSF) and disruption of the blood-brain barrier, the etiology is still unknown (2, 4). Infections are common in the early period after CAR-T infusion and may lead to pathogen-induced inflammation, potentially contributing to the pathogenesis of ICANS (5). Additionally, infections with neurological manifestations such as viral encephalitis are diagnostically challenging after CAR-T due to overlapping symptoms with ICANS. Since ICANS is a clinical diagnosis, and cerebrospinal fluid (CSF) analysis for viral pathology may not be available, the initiation of targeted treatment may be delayed.
Primary infection of HHV-6 usually occurs during childhood and manifests typically as roseola infantum with high fever and exanthema. HHV-6 can infect various human cells (including central-nervous system tissue, germ cells, endothelial cells, lymph nodes, and leukocytes) (6) and is known to remain latent within specific leukocyte subsets, including T cells (7). Latently infected cells carry HHV-6 chromosomally integrated in the telomeres. Infected germ cells allow vertical transmission of HHV-6, resulting in individuals carrying a chromosomally integrated HHV-6 genome in every nucleated cell (8). HHV-6 comprises two related viruses, HHV-6A and HHV-6B, which are collectively referred to as HHV-6 in this case report. Both are responsible for chromosomally integrated HHV-6, while HHV-6B is primarily associated with the development of neurological complications such as encephalitis and febrile seizures (9–12).
Reactivation of latent HHV-6 may occur after severe immunosuppression, particularly after allogeneic hematopoietic stem cell transplantation (HSCT), where up to 30–70% of patients with long-term T-cell depletion may develop HHV-6 reactivation (13–15). Although HHV-6 reactivation is often asymptomatic, HHV-6 encephalitis is reported in up to 1.4-4.1% of patients after HSCT and is often associated with irreversible memory loss and significant mortality (13, 16, 17).
HHV-6 reactivation following CAR-T therapy is likely less common with a reported cumulative incidence of 6% within 12 weeks after CD19 or BCMA-targeted CAR-T cell therapy (18). Evidence of severe HHV-6 disease after CAR-T therapy is limited to case reports of HHV-6 encephalitis (19–23) and a single case of fatal HHV-6 myelitis (24), and a recent retrospective cohort study suggests that HHV-6 encephalitis is rare (18).
The mechanism and cellular source of severe HHV-6 reactivation following CAR-T therapy remain unexplored. Here, we present a case of severe HHV-6 encephalitis occurring shortly after anti-CD19 CAR-T therapy coinciding with an atypical surge in lymphocytes. We hypothesize that the autologous T cells harbored latent HHV-6, which during CAR-T cell manufacturing or proliferation post-infusion led to a high viral load, causing encephalitis. Here, the academical production of the CAR-T cells allowed for detailed analysis of T cells during manufacturing and after infusion.
Case description
A 58-year-old woman with a prior history of antithrombin III deficiency and depression was treated with CAR-T therapy for a refractory transformed follicular lymphoma as part of a clinical trial investigating an academical autologous 4-1BB anti-CD19 CAR-T product (CTIS # 2024-515174-27-00). She was initially treated with R-CHOP for follicular lymphoma, and upon lymphoma transformation, she was refractory to treatment with ICE and received two courses of DHAX as bridging to CAR-T therapy. Before lymphodepleting chemotherapy, the patient had a limited tumor burden with multiple small PET-positive lymph nodes above and below the diaphragm, but only a single enlarged lymph node (1.1 x 1.5 cm). The bone marrow was without evidence of lymphoma cells, and lactate dehydrogenase was 338 U/L. She was neuropsychologically healthy without any focal neurological deficits at the neurological examination before CAR-T infusion.
The CAR-T cell product was manufactured from a fresh apheresis product using a lentiviral vector carrying a 4-1BB anti-CD19 CAR transgene on the CliniMACS Prodigy platform (Miltenyi, San José, CA, USA). The production process spanned 12 days and met all predefined release criteria. The patient received standard lymphodepleting chemotherapy consisting of cyclophosphamide (2 doses of 500 mg/m2) and fludarabine (4 doses of 30 mg/m2) before infusion of 2.6 x106/kg fresh CAR-T cells with a CD4/CD8 CAR-T cell ratio of 9:1 (Figure 1).
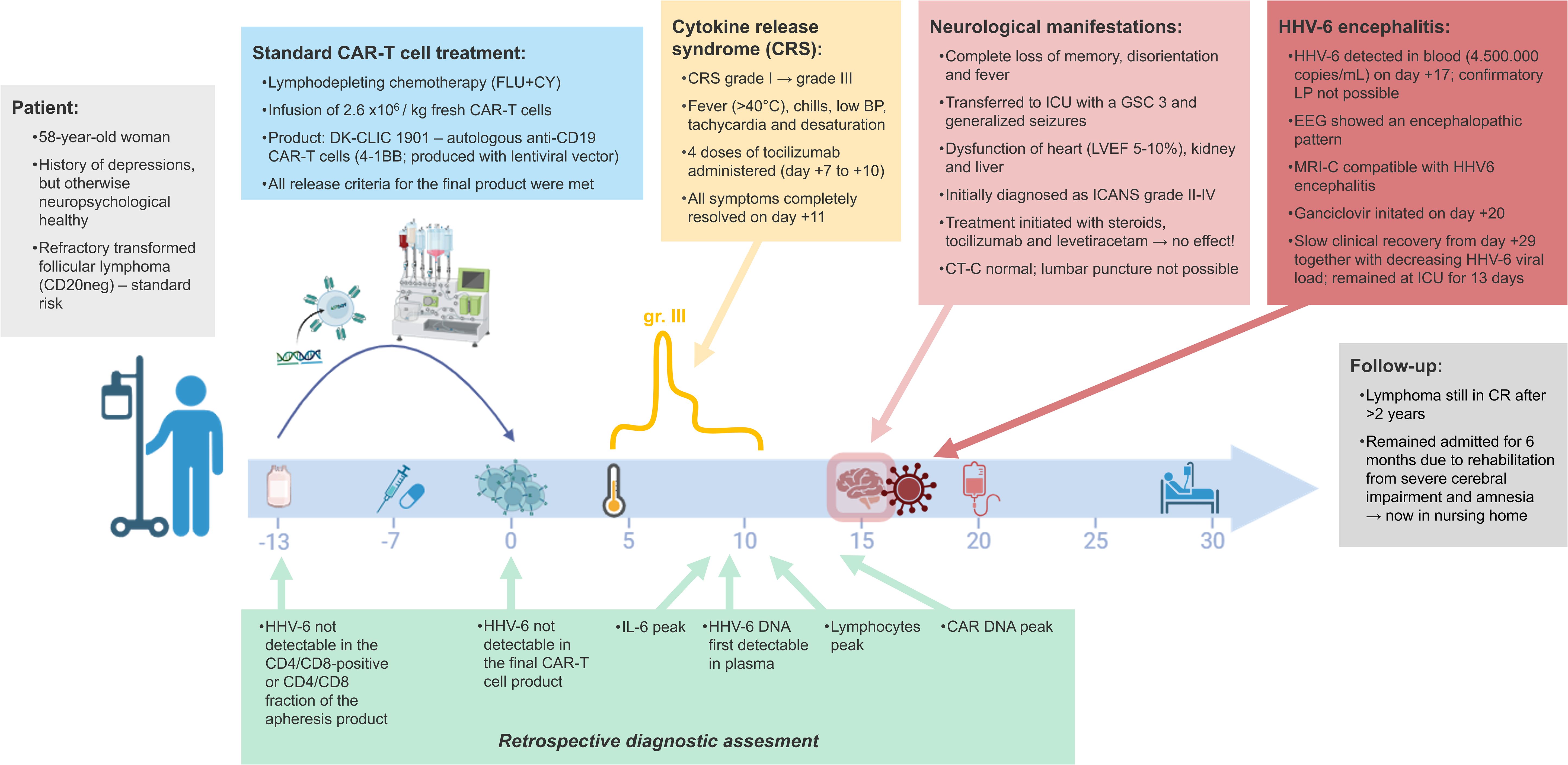
Figure 1. Patient timeline with symptoms, diagnostic findings and treatment from day of apheresis (day -13) to day +30 after anti-CD19 CAR-T cell therapy. Day 0 mark the infusion of CAR-T cells. Retrospective diagnostic analyses are presented below the timeline for comparison with the clinical findings.
Four days after CAR-T infusion, the patient presented with fever >40 °C and chills, and later hypotension (systolic BP 100-110), tachycardia (100 bpm), and hypoxia (oxygen requirement of 6–10 L) consistent with cytokine release syndrome (CRS) grade III. Treatment with tocilizumab was initiated, and a total of 4 doses were administered from day +6 to 9. All symptoms were completely resolved on day +11 post-infusion without administration of methylprednisolone. The CRS episode was paralleled by increasing absolute lymphocyte counts from 0.5 x109/L to 5.6 x109/L from day +8 to +11, indicating a rapid proliferation of CAR-T cells.
On day +15, the patient became increasingly confused, followed by a sudden onset of complete loss of memory, disorientation, recurrent fever, and three episodes of generalized seizures. The symptoms were initially categorized as ICANS grade II (with ICE score 8) and upgraded to grade IV (ICE score 6) on day +16, and she was transferred to the intensive care unit with a Glasgow Coma Score of 3. Myocarditis (left ventricular ejection fraction of 5-10%), and affection of kidney (estimated glomerular filtration rate of 16), liver (alanine transaminase of 128 U/L, alkaline phosphatase of 209 U/L, LDH of 512 U/L, pancreas amylase of 206 U/L) and coagulation system (INR of 3.8, hypofibrinogenemia of 2.5 µmol/L, and Fibrin D-dimer of 1.9 FEU/L) developed in parallel, while fever resolved. Treatment with dexamethasone (10 mg x4 daily), tocilizumab (x1 initially due to fever) and levetiracetam for ICANS was commenced, however, this did not relieve the symptoms. Computed tomography scan with angiography of the brain was normal, whereas electroencephalography showed an encephalopathic pattern (Supplementary Figure 1). A lumbar puncture was not performed due to thrombocytopenia and coagulation disorders, but viral reactivation in plasma was investigated for alternative causes of the neurological symptoms.
On day +20, plasma analysis for viral reactivations from day +17 revealed a viral load of 4.5 x106 HHV-6 copies/ml, indicating that HHV-6 reactivation and encephalitis were a likely cause of the patient’s condition. Although HHV-6 could not be confirmed in CSF, a contrasted MRI scan on day +22 supported the diagnosis of infectious encephalitis, including bilateral hippocampal involvement (Supplementary Figure 2). Prophylactic acyclovir was immediately substituted with ganciclovir treatment (5 mg/kg twice daily). Slow clinical recovery was observed from day +25, and on day +29 she was able to recognize hospital staff, attempted to speak to relatives, and could move her upper extremities. The clinical improvement was mirrored by decreasing viral load over the following weeks with HHV-6 negativity obtained from day +43, and antiviral medication was discontinued after 38 days. No other microbial agents were detected, including no reactivation of cytomegalovirus and Epstein-Barr virus. Ferritin and CRP levels remained low to normal. Dexamethasone treatment was gradually tapered and discontinued after 5 weeks. The patient was shortly on mechanical ventilation due to hypoxia (from day +20-25), and the heart failure gradually improved within a few weeks supported by antidiuretics and inotropes.
At the time of this report, the patient has been in complete remission from lymphoma for more than two years following CAR-T cell therapy. She was hospitalized for six months after the CAR-T infusion due to prolonged rehabilitation for cerebral impairment and amnesia. However, she continues to experience severe neurophysiological sequelae, including short-term memory loss and epileptic seizures, with disabilities corresponding to a modified Rankin Scale score of 4, and therefore resides permanently in a nursing home.
Diagnostic assessment
To investigate whether the HHV-6 infection resulted from reactivation of latent HHV-6 in the patient’s harvested lymphocytes, we retrospectively analyzed cryopreserved samples of cells (106 cells pr. test) from both the apheresis product and the final CAR-T product, and plasma samples collected from before lymphodepleting therapy to day +21 after CAR-T infusion. All samples were tested for HHV-6 DNA in triplicates by real-time quantitative polymerase chain reaction (qPCR) using the commercial HHV-6 R-GENE® kit (bioMérieux, Argene Varilhes, France) with a detection limit of 200 copies/mL (25). This analysis detects HHV-6A as well as HHV-6B, the latter being the endemic HHV-6 virus in Northern Europe (26).
HHV-6 DNA was not detected in either plasma from the patient prior to lymphodepleting chemotherapy, in cryo-preserved cells from the CD4/CD8 negative and the CD4/CD8 positive fraction of the apheresis product, or in the final product of transduced and expanded CAR-T cells. After CAR-T infusion, HHV-6 DNA was positive in plasma from day +9 and peaked on day +17 with 4.5 x106 HHV-6 copies/ml (Figure 2A). The increase in HHV-6 DNA levels was paralleled by a rapid increase in lymphocytes, primarily due to an unusual surge in CD4+ T cells (Figures 2A, B).
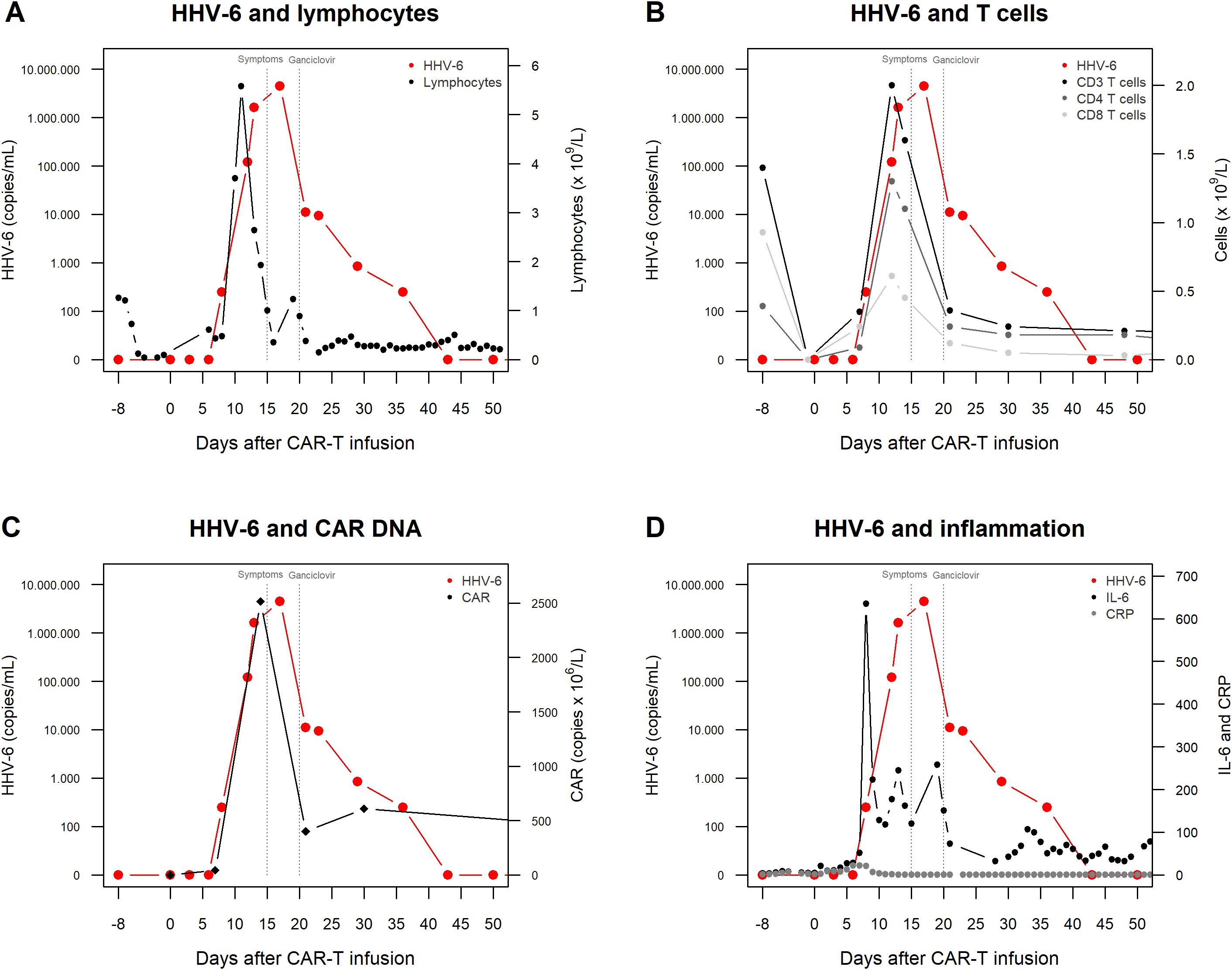
Figure 2. HHV-6 reactivation, T-cell recovery and inflammatory measures from before lymphodepleting chemotherapy (day -8) to day +50 after CAR-T cell infusion in our case patient with severe HHV-6 encephalitis. (A) Circulating lymphocytes and HHV-6 viral load in plasma. (B) T cells and HHV-6 viral load in plasma. NK cell counts were below 0.075 x109 cells/L and B-cells were undetectable at all time points. (C) CAR DNA copies and HHV-6 viral load in plasma. (D) IL-6 (ng/L), CRP (mg/L), and HHV-6 viral load in plasma. Dotted vertical lines indicate the beginning of CNS symptoms and administration of ganciclovir, respectively.
The number of circulating CAR-T cells was assessed in whole blood (cell bound leukocyte DNA) using an in-house qPCR-based assay targeting the region that encodes the single-chain variable fragment (scFv) domain of the CD19 CAR-T cells, established at Department of Clinical Immunology, Odense University Hospital, Denmark. CAR DNA copies were measurable from day +7 after CAR-T infusion showing a sharp increase and peaking at 2515 x106 copies/L on day +14 before gradually declining (Figure 2C). Routine inflammatory markers showed a transient rise in circulating Interleukin 6 (IL-6) peaking on day +8 (maximum 635 ng/L), thus preceding HHV-6 reactivation and clinical symptoms, while c-reactive protein (CRP) levels remained close to normal (between 0–22 mg/L) (Figure 2D).
In summary, HHV-6 DNA was retrospectively detected in plasma from day +9 after CAR-T infusion, peaking on day +17. This was accompanied by a parallel increase in circulating T-cell counts and CAR DNA copy numbers, however, HHV-6 DNA was undetectable in the apheresis product as well as in the manufactured CAR-T cell product.
We then set up an in vitro activation assay to simulate the interaction between CAR-T cells and tumor cells expressing their target antigen CD19 to investigate whether stimulation and expansion of CAR-T cells from the patient’s infusion product led to HHV-6 reactivation. Cryo-preserved CAR-T cells from the patient’s infusion product were thawed and seeded in 24-well plates at a density of 2×106 cells per well. Three conditions were created: (a) co-culture with CD19+ Daudi cells at a 3:1 effector-to-target ratio, (b) plate-bound human CD3 (Miltenyi Biotec, 170-076-124) and CD28 (Miltenyi Biotec, 170-076-117) T cell agonistic antibodies (300 ng/mL), and (c) CAR-T cells alone (Figure 3A). After day 0, the CAR-T cells were serially activated again in their respective conditions at days +3 and +7. CAR-T cells were harvested after +1, +4, and +8 days of co-culture, corresponding to the time to HHV-6 reactivation in the patient. Harvested cells underwent either flow cytometry for T cell phenotyping and multicytokine intracellular staining (Agilent Novocyte Quanteon with NovoExpress v1.6.2, processed in FlowJo v10.8.1), or real-time PCR for HHV-6 detection. The patient’s CAR-T cells expressed an activated T-cell phenotype (Figure 3B) with reactivity in response to the CD19-positive cell line as measured by the production of two or more cytokines, including CD107a, CD137, TNF-α, and/or IFN-γ (Figures 3C, D). However, HHV-6 remained undetectable by real-time PCR in the stimulated CAR-T cells from the patient’s infusion product at all time points.
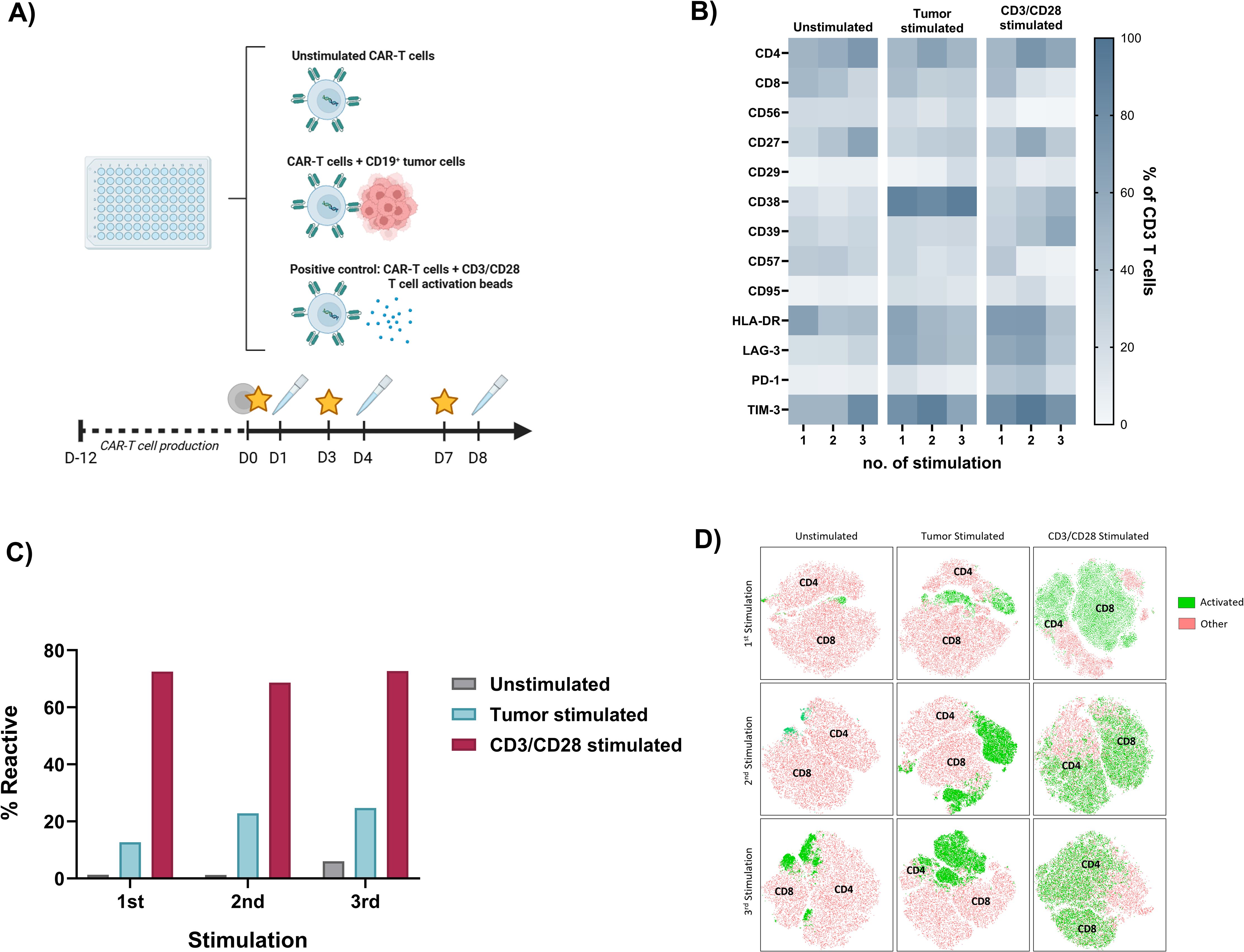
Figure 3. (A) Tumor killing assay mimicking the activation of CAR-T cells by their target tumor cells. CAR-T cells from the infusion product from our case patient were thawed and incubated either alone, co-cultured with CD19+ Daudi cells, or activated with Human CD3/CD28 T cell Activation Beads. Stars indicate the time of CAR-T cell stimulation 1-3 (addition of Daudi cells or beads), and pipettes indicate the time of cell harvest. (B) Heatmap showing T cell phenotypes as the proportion of CD3+ T cells expressing different T cell activation and exhaustion surface markers after 1–3 stimulations of the CAR-T cell infusion product in the tumor killing assay. (C) Barplot of the proportion of CD3+ T cells from the CAR-T infusion product that produces ≥2 cytokines (CD107 α, CD137, TNF-α or IFN-γ) after 1–3 stimulation cycles in the tumor killing assay. The infusion product consisted of 35.7% living CAR-T cells, nearly corresponding to the proportion of activated cells after incubation with CD19+ Daudi cells. (D) Uniform manifold approximation and projection map of CD4+ and CD8+ activated cells measured by multicytokine intracellular staining after 1–3 stimulation cycles in the tumor killing assay. Green color illustrates activated T-cells (production of ≥2 cytokines: CD107 α, CD137, TNF-α or IFN-γ), while red color indicates other cells.
Discussion
We report a case of severe clinical encephalitis with persistent neurological sequelae following anti-CD19 CAR-T cell therapy. Neurological symptoms appeared on day +15 shortly after complete recovery from CRS and were initially thought to be caused by ICANS. However, symptoms such as confusion, severe amnesia and repeated seizures, together with later onset, slower progression and the limited effect of treatment with steroids and tocilizumab were atypical for ICANS. On day +20, the patient was diagnosed with HHV-6 driven encephalitis based on high viral load of HHV-6 in plasma (4.5 x106 copies/mL) together with EEG and MRI scan consistent with infectious encephalitis (27).
We hypothesized that the HHV-6 virus was latently residing in the patient’s autologous T cells and that proliferation during manufacturing or after CAR-T cell infusion caused the clinical infection. Retrospective laboratory analyses of cryopreserved patient samples showed that circulating HHV-6 DNA was present from day +9 and peaked at day +17 after CAR-T infusion, corresponding to the clinical course. This HHV-6 kinetic was associated with a simultaneous rise in circulating lymphocyte counts, and the patients’ condition improved upon treatment with ganciclovir while HHV-6 copies decreased, indicating a clinical association.
Our patient’s clinical course is similar to previous case reports of HHV-6-related encephalitis following CAR-T cell therapy. Consistent symptoms include acute memory loss, confusion, disorientation, and seizures, typically occurring within 5–14 days after CAR-T infusion and often preceded by CRS. Outcome after HHV-6 encephalitis ranges from complete resolution of symptoms to severe sequelae or death (19, 21–23, 28, 29).
In allogeneic HSCT, monitoring of HHV-6 DNA in the peripheral blood in high-risk settings are conducted in some centers, but pre-emptive treatment is currently challenged by no established thresholds and insufficient data regarding efficacy (30). Incidence of HHV-6 encephalitis up to 4% is reported after HSCT, especially in settings with long-term T-cell depletion such as cord blood transplantations or T-cell-depleted haploidentical HSCT (12, 16, 17, 31). In HSCT, a high viral load of HHV-6 in plasma remains a risk factor for encephalitis (13, 15, 31, 32). Thus, one study demonstrated that only patients with circulating HHV-6 DNA levels above 104 copies/mL developed CNS-related symptoms with incidences of HHV-6 encephalitis of 21% and 50% in patients with a maximal HHV-6 level ≥104 and ≥105 copies/mL plasma, respectively (33).
In the only prospective cohort study of HHV-6 following CD19- or BCMA-directed CAR-T cell therapy (n=89), an incidence of 6% HHV-6 reactivation was reported at median day +21 (range: 2–6 weeks) (18). However, viral loads were low with a median of 435 copies/mL (all <104 copies/mL) and none had clinical features of encephalitis. In the same paper, the course of CAR-T cell treatment of 626 patients was retrospectively reviewed for possible HHV-6 encephalitis. Only few were tested for HHV-6 (CFS: n=34; peripheral blood: n=24), and only one patient had detectable HHV-6 at day +32 with a low viral load (<2 x103 copies/ml), without typical features of HHV-6 encephalitis and not requiring antiviral treatment. This suggests that HHV-6 encephalitis is rare after CAR-T cell therapy, and the authors suggest that routine HHV-6 monitoring may not be necessary (18).
In comparison, HHV-6 reactivation occurred considerably earlier after CAR-T infusion and with a higher viral peak load in our and other case reports of clinically significant HHV-6 encephalitis. We further demonstrated that in our patient, circulating HHV-6 DNA was detectable already 6 days before the debut of neurological symptoms with a rapid increase to 4.5 x 106 copies/ml. We suggest that early HHV-6 reactivation during lymphopenia may possess a greater risk of clinical progression to encephalitis, potentially due to co-occurring systemic inflammation from CRS or ICANS. Increased proinflammatory cytokines are considered to play pathogenic roles in the development of CNS manifestations in various viral infections, including primary HHV-6 infection (34). In a study of HSCT recipients, longitudinal analyses of patients with high HHV-6 viral loads suggested that transiently increased plasma concentration of IL-6 predicted the development of HHV-6 encephalitis (33). A similar pattern of high IL-6 levels, peaking at day +8 at the time of first HHV-6 reactivation, was found in our patient one week before neurological symptoms, and IL-6 remained markedly elevated through approximately two weeks. High IL-6 levels are suggested to mediate the pathogenesis of HHV-6 encephalitis through epithelial or endothelial injury, increased permeability of the blood–brain barrier, or induction of apoptosis in the cerebrum (33). It can be speculated that the pronounced CD4+ T cell activation in our patient further contributed to the rapid progression of HHV-6 disease, as the receptor for HHV-6B (OX40) is known to be specifically upregulated during CD4+ T cell activation (35).
The biological background for HHV-6 reactivation after CAR-T cell therapy is, to our knowledge, still unknown. While HHV-6 disease in other settings is usually associated with severe T and B-cell depletion (e.g. HSCT), patients treated with CAR-T therapy only experience a transient decrease in T-cell numbers following the lymphodepleting chemotherapy (36). In our patient, the neurological symptoms from day +15 were preceded by a remarkable expansion of lymphocytes from day +8 to +11, mainly due to expansion of CD4+ T cells coinciding with the increase in HHV-6 DNA. The high CD4/CD8 ratio of 9.1 in the infused CAR-T cell product further suggested an HHV-6-driven proliferation of activated CD4+ T cells during manufacturing (11). However, HHV-6 DNA was undetectable in the CD4/CD8 negative and CD4/CD8 positive fractions of the apheresis product as well as in the final CAR-T cell product.
In a recent study, HHV-6 was shown to reactivate in cultures of human allogeneic CAR-T cells after approximately 2 weeks, initiated by viral spreading from a rare subset of HHV-6-positive CD4+ CAR-T cells and driven by T-cell activation, proliferation, and culture duration. Furthermore, the authors show that HHV-6 can be transcriptionally detected in autologous CAR-T cells in vitro or in vivo between 2 and 3 weeks after the start of CAR-T cell manufacturing, suggesting that reactivation would first be present after CAR-T infusion and that screening at early time points may miss virus-positive cells (35). Based on these findings, we conducted an in vitro tumor-killing assay to mimic the CAR-T cell activation occurring in vivo in our patient to assess whether this could lead to reactivation of latent HHV-6 potentially contained in the CAR-T cell product. However, HHV-6 remained undetectable also in the in vitro activated CAR-T cells after up to 8 days of exposure to CD19-positive tumor cells. With the sensitivity of the HHV-6 kit, HHV-6 should have been detectable in the 1x106 CAR-T cells tested, if these were the cause of the HHV-6 reactivation. Thus, we could not confirm that HHV-6 reactivation originated from the patient’s CAR-T cell product and it might instead reflect a reactivation of latent infection due to the temporary lymphodepletion given prior to CAR-T cell infusion.
In conclusion, we report a case of severe HHV-6-associated encephalitis following autologous anti-CD19 CAR-T therapy. In this patient, the source of HHV-6 reactivation could not be linked to CAR-T cell manufacturing, as HHV-6 was undetectable in the apheresis product, the final CAR-T cell product, and in CAR-T cells following in vitro T-cell activation in a tumor killing assay. Future studies involving larger patient cohorts are needed to further explore the biological mechanism of HHV-6 reactivation and encephalitis, including potential contributing factors such as IL-6 levels and rapid CD4+ proliferation. Nevertheless, our case indicates that viral screening may be critical for a timely initiation of antiviral treatment in patients with HHV-6-mediated disease early after CAR-T infusion.
Patient perspective
This case highlights HHV-6 encephalitis as a serious yet diagnostically challenging complication following CAR-T therapy. While the patient remains in sustained complete remission from cancer, the severe cognitive impairment resulting from viral encephalitis has significantly impacted her quality of life. Although HHV-6 encephalitis is a rare complication after CAR-T treatment, early diagnosis and prompt intervention should be prioritized in patients presenting with atypical neurological symptoms to mitigate long-term sequela. Additionally, the potential consequences of viral encephalitis should be considered alongside other CAR-T-related toxicities when assessing the risk-benefit profile of this therapy.
Data availability statement
The datasets presented in this article are not readily available because of ethical/privacy restrictions. Requests to access the datasets should be directed to Katrine Kielsen, a2F0cmluZWtpZWxzZW5AZGFkbG5ldC5kaw==.
Ethics statement
The studies involving humans were approved by Danish National Committee on Health Research, Ørestads Boulevard 5, 2300 Copenhagen, Denmark. The studies were conducted accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent obtained from the individual(s) for the publication of potentially identifiable images or data included in this article.
Author contributions
NB: Formal analysis, Writing – original draft, Visualization, Investigation. KK: Resources, Writing – original draft, Formal analysis, Visualization, Conceptualization, Methodology, Investigation. ÖM: Conceptualization, Funding acquisition, Resources, Writing – review & editing, Methodology, Supervision. EH: Resources, Writing – review & editing. TH: Investigation, Visualization, Formal analysis, Writing – review & editing. CM: Formal analysis, Visualization, Writing – review & editing, Investigation. TB: Writing – review & editing, Methodology, Resources, Investigation. JN: Writing – review & editing, Resources. KS: Resources, Investigation, Methodology, Writing – review & editing. SP: Conceptualization, Resources, Writing – review & editing, Funding acquisition. MI: Funding acquisition, Writing – original draft, Resources, Conceptualization, Project administration, Supervision.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This research was supported by the Danish Childhood Cancer Foundation and the BRIDGE – Translational Excellence Programme at the Faculty of Health and Medical Sciences, University of Copenhagen, funded by the Novo Nordisk Foundation (grant agreement #NNF23SA0087869).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhem.2025.1628552/full#supplementary-material
Supplementary Figure 1 | Representative images of the electroencephalography (EEG) performed on day +20 after CAR-T infusion. At the time of the recording, the patient was comatose and not receiving sedation. The EEG demonstrated a theta-predominant background with Bilateral Independent Periodic Discharges (BiPDs), maximally expressed in both temporal regions. The BiPDs exhibited a stable frequency of 0.7–1 Hz. Although the pattern showed some fluctuation in the following EEG, it met criteria for the ictal-interictal continuum but did not unequivocally qualify as a definite electrographic seizure or non-convulsive status epilepticus. The presence of BiPDs on EEG provides crucial information regarding bilateral brain injury and suggests that both cerebral hemispheres are at risk for seizure generation. This observation aligns with previous studies that have associated BiPDs with worse neurological status (typically coma) and poorer outcomes when compared to patients exhibiting Lateralized Periodic Discharges (LPDs) (Hirsch and Brenner’s Atlas of EEG in Critical Care). Human Herpesvirus 6 (HHV-6) encephalitis has previously been associated with a broader spectrum of EEG findings, including focal slowing, focal electrographic seizures, LPDs, Generalized Periodic Discharges (GPDs), and BiPDs (27). (A) The EEG in this panel was recorded with the following filter settings: Timebase: 30 mm/s; High Pass: 25 Hz; Low Pass: 1 Hz; Sensitivity: 100 µV/cm; Notch filter: On. A Common Average Montage was employed. This tracing clearly displays Bilateral Independent Periodic Discharges (BiPDs), with maximal amplitude in the temporal regions. The discharges recur at an interval of 0.7–1 per second, showing no clear evolution or significant fluctuation. The background activity between these discharges is characterized by low-frequency rhythms, approximately 4–5 Hz. (B) This panel, utilizing a Longitudinal Montage with the same filter settings as described for A, highlights distinct and independent periodic discharges (BiPDs) within the yellow boxes, without any additional modifiers.
Supplementary Figure 2 | Representative images of the MRI scan of the cerebrum performed on day +22 after CAR-T infusion, supporting the diagnosis of encephalitis. The MRI demonstrates symmetric signal changes on Diffusion Weighted Imaging (DWI), with associated thickening of the hippocampus, the uncus and amygdala bilaterally, as well as thickening of the right insular cortex. These findings were not confirmed on Apparent Diffusion Coefficient (ADC) imaging. The overall pattern is most consistent with encephalitis. No other pathological findings are observed. (A) T2-weighted sequence. (B) Fluid-Attenuated Inversion Recovery (FLAIR) sequence. (C) Diffusion Weighted Imaging (DWI) sequence.
Abbreviations
HHV-6, Human herpes virus 6; CAR-T, Chimeric antigen receptor T cells; ICANS, Immune effector cell-associated neurotoxicity syndrome; CSF, Cerebrospinal fluid; HSCT, Hematopoietic stem cell transplantation; CRS, Cytokine release syndrome; ICU, Intensive care unit; PCR, Polymerase chain reaction; IL-6, Interleukin 6; CRP, C-reactive protein.
References
1. Lee DW, Santomasso BD, Locke FL, Ghobadi A, Turtle CJ, Brudno JN, et al. ASTCT consensus grading for cytokine release syndrome and neu-rologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant. (2019) 25:625–38. doi: 10.1016/j.bbmt.2018.12.758
2. Tallantyre EC, Evans NA, Parry-Jones J, Morgan MPG, Jones CH, and Ingram W. Neurological updates: neurological complications of CAR-T therapy. J Neurol. (2021) 268:1544–54. doi: 10.1007/s00415-020-10237-3
3. Neill L, Rees J, and Roddie C. Neurotoxicity-CAR T-cell therapy: what the neurologist needs to know. Pract Neurol. (2020) 20:285–93. doi: 10.1136/practneurol-2020-002550
4. Sterner RC and Sterner RM. Immune effector cell associated neurotoxicity syndrome in chimeric antigen re-ceptor-T cell therapy. Front Immunol. (2022) 13:879608. doi: 10.3389/fimmu.2022.879608
5. Gea-Banacloche JC. Infectious complications of chimeric antigen receptor (CAR) T-cell therapies. Semin Hematol. (2023) 60:52–8. doi: 10.1053/j.seminhematol.2023.02.003
6. Agut H, Bonnafous P, and Gautheret-Dejean A. Roseoloviruses: Human Herpesviruses 6A, 6B, and 7. Microbiol Spectr. (2016). 4(3). doi: 10.1002/9780470741405.ch10
7. Sultanova A, Cistjakovs M, Gravelsina S, Chapenko S, Roga S, Cunskis E, et al. Association of active human herpesvirus-6 (HHV-6) infection with autoimmune thyroid gland diseases. Clin Microbiol Infection. (2017) 23:50.e1–5. doi: 10.1016/j.cmi.2016.09.023
8. Aimola G, Beythien G, Aswad A, and Kaufer BB. Current understanding of human herpesvirus 6 (HHV-6) chromosomal integration. Antiviral Res. (2020) 176:104720. doi: 10.1016/j.antiviral.2020.104720
9. Komaroff AL, Pellett PE, and Jacobson S. Human herpesviruses 6A and 6B in brain diseases: association versus causation. Clin Microbiol Rev. (2020) 34:e00143–20. doi: 10.1128/CMR.00143-20
10. Eliassen E, Hemond CC, and Santoro JD. HHV-6-associated neurological disease in children: epidemiologic, clinical, diagnostic, and treatment considerations. Pediatr Neurol. (2020) 105:10–20. doi: 10.1016/j.pediatrneurol.2019.10.004
11. Wood ML, Bell AJ, Young R, Brownlie C, Orr N, Campbell A, et al. Inherited chromosomally integrated human herpesvirus 6: regional variation in prevalence, association with angina, and identification of ancestral viral lineages in two large UK studies. J Virol. (2025) 5:e0216024. doi: 10.1128/jvi.02160-24
12. Aswad A, Aimola G, Wight D, Roychoudhury P, Zimmermann C, Hill J, et al. Evolutionary history of endogenous human herpesvirus 6 reflects human migration out of Africa. Mol Biol Evol. (2021) 38:96–107. doi: 10.1093/molbev/msaa190
13. Ljungman P, Wang FZ, Clark DA, Emery VC, Remberger M, Ringdén O, et al. High levels of human herpesvirus 6 DNA in peripheral blood leucocytes are correlated to platelet engraftment and disease in allogeneic stem cell transplant patients. Br J Haematol. (2000) 111:774–81. doi: 10.1111/j.1365-2141.2000.02422.x
14. Yoshikawa T, Asano Y, Ihira M, Suzuki K, Ohashi M, Suga S, et al. Human herpesvirus 6 viremia in bone marrow transplant recipients: clinical features and risk factors. J Infect Dis. (2002) 185:847–53. doi: 10.1086/339411
15. Zerr DM, Corey L, Kim HW, Huang ML, Nguy L, and Boeckh M. Clinical outcomes of human herpesvirus 6 reactivation after hematopoietic stem cell transplantation. Clin Infect Dis. (2005) 40:932–40. doi: 10.1086/428060
16. Hill JA, Koo S, Guzman Suarez BB, Ho VT, Cutler C, Koreth J, et al. Cord-blood hematopoietic stem cell transplant confers an increased risk for human herpesvirus-6-associated acute limbic encephalitis: a cohort analysis. Biol Blood Marrow Transplant. (2012) 18:1638–48. doi: 10.1016/j.bbmt.2012.04.016
17. Ogata M, Satou T, Kadota J, Saito N, Yoshida T, Okumura H, et al. Human herpesvirus 6 (HHV-6) reactivation and HHV-6 encephalitis after allogeneic hematopoietic cell transplantation: a multicenter, prospective study. Clin Infect Dis. (2013) 57:671–81. doi: 10.1093/cid/cit358
18. Kampouri E, Krantz EM, Xie H, Ibrahimi SS, Kiem ES, Sekhon MK, et al. Human herpesvirus 6 reactivation and disease are infrequent in chimeric antigen receptor T-cell therapy recipients. Blood. (2024) 144:490–5. doi: 10.1182/blood.2024024145
19. Baird JH, Epstein DJ, Tamaresis JS, Ehlinger Z, Spiegel JY, Craig J, et al. Immune reconstitution and infectious complications following axicabtagene ciloleucel therapy for large B-cell lymphoma. Blood Adv. (2021) 5:143–55. doi: 10.1182/bloodadvances.2020002732
20. Kampouri E, Little JS, Rejeski K, Manuel O, Hammond SP, and Hill JA. Infections after chimeric antigen receptor (CAR)-T-cell therapy for hematologic Malignancies. Transpl Infect Dis. (2023) 25 Suppl 1:e14157. doi: 10.1111/tid.14157
21. Rebechi MT, Bork JT, and Riedel DJ. HHV-6 encephalitis after chimeric antigen receptor T-cell therapy (CAR-T): 2 case reports and a brief review of the literature. Open Forum Infect Dis. (2021) 8:ofab470. doi: 10.1093/ofid/ofab470
22. Shah M, Kuhnl A, Shields G, Sudhanva M, Metaxa V, Wong S, et al. Human herpesvirus 6 encephalitis following axicabtagene ciloleucel treatment for refractory diffuse large B cell lymphoma. Hemasphere. (2021) 5:e535. doi: 10.1097/HS9.0000000000000535
23. Handley G, Hasbun R, and Okhuysen P. Human herpesvirus 6 and central nervous system disease in oncology patients: A retrospective case series and literature review. J Clin Virol. (2021) 136:104740. doi: 10.1016/j.jcv.2021.104740
24. Handley G, Khawaja F, Kondapi DS, Lee HJ, Kaufman GP, Neelapu SS, et al. Human herpesvirus 6 myelitis after chimeric antigen receptor T-cell therapy. Int J Infect Dis. (2021) 112:327–9. doi: 10.1016/j.ijid.2021.09.061
25. Deback C, Agbalika F, Scieux C, Marcelin AG, Gautheret-Dejean A, Cherot J, et al. Detection of human herpesviruses HHV-6, HHV-7 and HHV-8 in whole blood by real-time PCR using the new CMV, HHV-6, 7, 8 R-gene kit. J Virol Methods. (2008) 149:285–91. doi: 10.1016/j.jviromet.2008.01.026
26. Ablashi D, Agut H, Alvarez-Lafuente R, Clark DA, Dewhurst S, DiLuca D, et al. Classification of HHV-6A and HHV-6B as distinct viruses. Arch Virol. (2014) 159:863–70. doi: 10.1007/s00705-013-1902-5
27. Yassin A, Al-Mistarehi AH, El-Salem K, Momani A, Al Qawasmeh M, Rodriguez R, et al. Clinical, radiological, and electroencephalographic features of HHV-6 encephalitis following hematopoietic stem cell transplantation. Ann Med Surg. (2020) 60:81–6. doi: 10.1016/j.amsu.2020.10.022
28. Spanjaart AM, van der Valk FM, van Rooijen G, Brouwer MC, and Kersten MJ. Confused about confusion. N Engl J Med. (2022) 386:80–7. doi: 10.1056/NEJMcps2114818
29. Yi F, Qin N, and Wang L. Human herpesvirus 6 (HHV-6) encephalitis secondary to chimeric antigen receptor (CAR)-T cell therapy. Neurol Sci. (2024) 46(3):1323–7. doi: 10.1007/s10072-024-07860-7
30. Kampouri E, Handley G, Phan TL, Lee YJ, Shaw R, Carpenter PA, et al. American society for transplantation and cellular therapy series 9: management of human herpesvirus 6B after hematopoietic cell transplantation and chimeric antigen receptor-T-cell therapy. Transplant Cell Ther. (2025) 31(8):480–93. doi: 10.1016/j.jtct.2025.05.001
31. Yamane A, Mori T, Suzuki S, Mihara A, Yamazaki R, Aisa Y, et al. Risk factors for developing human herpesvirus 6 (HHV-6) reactivation after allogeneic hematopoietic stem cell transplantation and its association with central nervous system disorders. Biol Blood Marrow Transplant. (2007) 13:100–6. doi: 10.1016/j.bbmt.2006.09.003
32. Ogata M, Satou T, Kawano R, Goto K, Ikewaki J, Kohno K, et al. Plasma HHV-6 viral load-guided preemptive therapy against HHV-6 encephalopathy after allogeneic stem cell transplantation: a prospective evaluation. Bone Marrow Transplant. (2008) 41:279–85. doi: 10.1038/sj.bmt.1705907
33. Ogata M, Satou T, Kawano R, Takakura S, Goto K, Ikewaki J, et al. Correlations of HHV-6 viral load and plasma IL-6 concentration with HHV-6 encephalitis in allogeneic stem cell transplant recipients. Bone Marrow Transplant. (2010) 45:129–36. doi: 10.1038/bmt.2009.116
34. Ichiyama T, Ito Y, Kubota M, Yamazaki T, Nakamura K, and Furukawa S. Serum and cerebrospinal fluid levels of cytokines in acute encephalopathy associated with human herpesvirus-6 infection. Brain Dev. (2009) 31:731–8. doi: 10.1016/j.braindev.2008.11.005
35. Lareau CA, Yin Y, Maurer K, Sandor KD, Daniel B, Yagnik G, et al. Latent human herpesvirus 6 is reactivated in CAR T cells. Nature. (2023) 623:608–15. doi: 10.1038/s41586-023-06704-2
Keywords: CAR-T therapy, HHV-6, encephalitis, ICANS, neurotoxicity
Citation: Birk NM, Kielsen K, Met Ö, Haastrup EK, Hulen TM, Madsen CØ, Barington T, Nielsen J, Schønning K, Petersen SL and Ifversen M (2025) Case Report: Severe HHV-6-related encephalitis following anti-CD19 CAR-T therapy with no evidence of HHV-6 reactivation in transduced CAR-T cells. Front. Hematol. 4:1628552. doi: 10.3389/frhem.2025.1628552
Received: 15 May 2025; Accepted: 08 August 2025;
Published: 19 September 2025.
Edited by:
Stella Bouziana, King’s College Hospital NHS Foundation Trust, United KingdomReviewed by:
Toshiki Terao, Okayama University, JapanFelix Fischbach, University Medical Center Hamburg-Eppendorf, Germany
Joseph Sassine, University of Oklahoma Health Sciences, United States
Copyright © 2025 Birk, Kielsen, Met, Haastrup, Hulen, Madsen, Barington, Nielsen, Schønning, Petersen and Ifversen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katrine Kielsen, a2F0cmluZWtpZWxzZW5AZGFkbG5ldC5kaw==
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship