 Philipp Faustmann1*
Philipp Faustmann1* Jan C. Schroeder1
Jan C. Schroeder1 Andreas Riedel1
Andreas Riedel1 Christian M. Schürch2,3Simon Killinger1Laurent Phely1
Christian M. Schürch2,3Simon Killinger1Laurent Phely1 Lucas Mix1Claudia Lengerke1,4Max-Felix Häring1
Lucas Mix1Claudia Lengerke1,4Max-Felix Häring1- 1Internal Medicine II – Hematology, Oncology, Clinical Immunology, Rheumatology, University Hospital Tuebingen, Tuebingen, Germany
- 2Department of Pathology and Neuropathology, University Hospital and Comprehensive Cancer Center Tuebingen, Tuebingen, Germany
- 3Cluster of Excellence Ifit (EXC 2180) “Image-Guided and Functionally Instructed Tumor Therapies”, University of Tübingen, Tübingen, Germany
- 4German Cancer Consortium (DKTK), partner side Tuebingen, a partnership between DKFZ and University Hospital Tuebingen, Tuebingen, Germany
Relapsed or refractory (r/r) nodal T-follicular helper cell lymphoma of the angioimmunoblastic type is a rare disease with a dismal prognosis. This disease usually harbors mutations in epigenetic modifiers. A standard of treatment for an r/r disease is not known. Here, we report real-world data of 11 patients with a median age of 73 years, treated with azacitidine, a hypomethylating agent. Overall survival was 182 days. Five patients died from progressive disease; three were in complete remission after allogeneic stem cell transplantation; two were in complete remission, still receiving azacytidine; and one was under treatment for relapse. The treatment was well-tolerated despite the advanced age, and there was a high burden of comorbidities with a median hematopoietic cell transplantation-specific comorbidity index (HCT-CI) of 5, a score for identifying relevant comorbidities. However, a grade 3 or 4 hematological toxicity occurred in nine patients. Azacitidine may be a suitable treatment option for some patients with r/r nodal T-follicular helper cell lymphoma.
1 Introduction
Peripheral T-cell lymphomas (PTCLs) account for 5%–10% of all non-Hodgkin lymphomas (NHLs) (1, 2). Nodal T-follicular helper cell lymphoma (TFH lymphoma) is a rare subtype of PTCL, accounting for 18.5% of all PTCLs or approximately 2% of all lymphomas (2, 3). Subtypes are classified into angioimmunoblastic, follicular, and not otherwise specified (NOS) (4, 5). The median age at diagnosis is 65 years, and 56% of patients are men (3). Approximately one-third of patients have bone marrow involvement.
Thus far, the outcome for this is poor. The 5-year overall survival (OS) for TFH lymphoma of the angioimmunoblastic type after anthracycline-based chemotherapy is approximately 32% (6). Nevertheless, anthracycline-based regimens like CHOP or CHOEP (cyclophosphamide, doxorubicin, vincristine, prednisone with or without etoposide) remain the standard of care in the first-line setting (7–9). The median OS of relapsed or refractory (r/r) disease is 7.7 months without stem cell transplantation (10). For relapsed or refractory disease, there is currently no established standard of care. One approach is conventional chemotherapy. Combination chemotherapy regimens like GDP (gemcitabine, cisplatin, dexamethasone), ICE (ifosfamide, carboplatin, etoposide), and DHAP (dexamethasone, high-dose cytarabine, cisplatin) or single-agent chemotherapy with gemcitabine or etoposide is commonly applied (10, 11). Another approach is the use of novel therapeutics like romidepsin, pralatrexate, and belinostat, which have demonstrated efficacy (12–15) but are not approved in many countries.
TFH lymphoma of the angioimmunoblastic type harbors mutations in the genes DNMT3A, IDH2, RHOA, and TET2 in 26%–39%, 20%–45%, 53%–72%, and 33%–82% of cases, respectively (16–22). DNMT3A, IDH2, and TET2 are involved in DNA and histone methylation, and recurrent mutations in these genes are key drivers of epigenetic deregulation in hematological malignancies.
Azacitidine (aza) acts as a hypomethylating agent and thus partially counteracts these epigenetic changes (23) and has been successfully applied to treat myeloid neoplasms (24, 25). Aza is available as an oral or subcutaneous formulation. The rationale behind this therapy is that hypermethylation silences tumor suppressors and aza reverses this effect. Furthermore, it was shown in a gene expression profile analysis that, especially in combination with romidepsin, aza changes the transcriptome, for example, through downregulation of metabolism or upregulation of genes involved in cell cycle arrest (26). Therefore, aza was tested for the treatment of r/r disease. Lemonnier et al. conducted a retrospective study demonstrating a median OS of 21 months in 12 patients receiving subcutaneous aza (27). Another retrospective analysis showed an OS of 10.5 months for 15 patients with r/r TFH lymphoma (28). Recently, Dupuis et al. reported a progression-free survival (PFS) of 5.6 months and a median OS of 18.4 months in a phase 3 study of oral aza in patients with r/r TFH lymphoma (29). In this prospective trial, grade 3 or 4 adverse events were seen in 76% of patients. The most common events were hematological side effects (anemia, thrombocytopenia, neutropenia). Others were infections, gastrointestinal disorders, and metabolism/nutrition disorders. Febrile neutropenia was only seen in one patient.
Furthermore, aza has been tested in combination with romidepsin, polychemotherapy (CHOP), or chidamide in combination or without gemcitabine/oxaliplatin with promising results (30–34).
Given the low incidence of TFH lymphoma, further real-world data on the safety and efficacy of aza are urgently needed. We address this need by reporting on 11 patients with TFH lymphoma of the angioimmunoblastic type, treated with aza at our institution.
2 Materials and methods
All patients who were diagnosed with TFH lymphoma and were treated with aza between 2019 and April 2025 were included. The diagnosis was made using the immunohistochemistry panel staining CD3, CD4, CD8, PD-1, ICOS, CD10, BCL6, CXCL13, and EBV (for example, see the Supplementary Data). CD30 was stained in special situations. Confirmation of diagnosis was by reference pathology. Next-generation sequencing was performed for typical mutations, but clonal hematopoiesis was not tested in routine diagnostics. Aza was administered subcutaneously at a dose of 75 mg/m² for 7 days of each 28-day cycle in 10 patients, unless adverse events necessitated discontinuation. One patient received 300 mg of aza orally together with his DLBCL treatment.
Demographic and clinicopathologic variables were collected. These included age, sex, medical comorbidities, performance status, laboratory results, immunophenotype, cytogenetic and molecular genetic aberrations, organs involved, treatment line, treatment duration, post-remission, and relapse treatments. Outcome measures included best response as assessed by computed tomography (CT) or positron emission tomography (PET-CT), duration of response, OS as defined by time from start of treatment to death from any cause, PFS as defined by time from start of treatment to progression, recurrence, cause of death, and type and severity of adverse events according to the Common Terminology Criteria for Adverse Events (CTCAE v5.0). Data lock was on 16 May 2025. This analysis was reviewed and approved by our institutional ethics committee (#469/2024BO2).
For descriptive statistics, absolute frequencies and percentages were used for categorical variables, and the median, arithmetic mean, and range were used for continuous variables. The Kaplan–Meier estimator was used to analyze the probability of OS and PFS.
3 Results
3.1 Patient characteristics
Eleven patients have been treated with aza for r/r TFH lymphoma at our institution. Nine suffered from the angioimmunoblastic subtype, and two from the NOS subtype. The median age was 73 years. For detailed information about the patient characteristics, see Table 1.
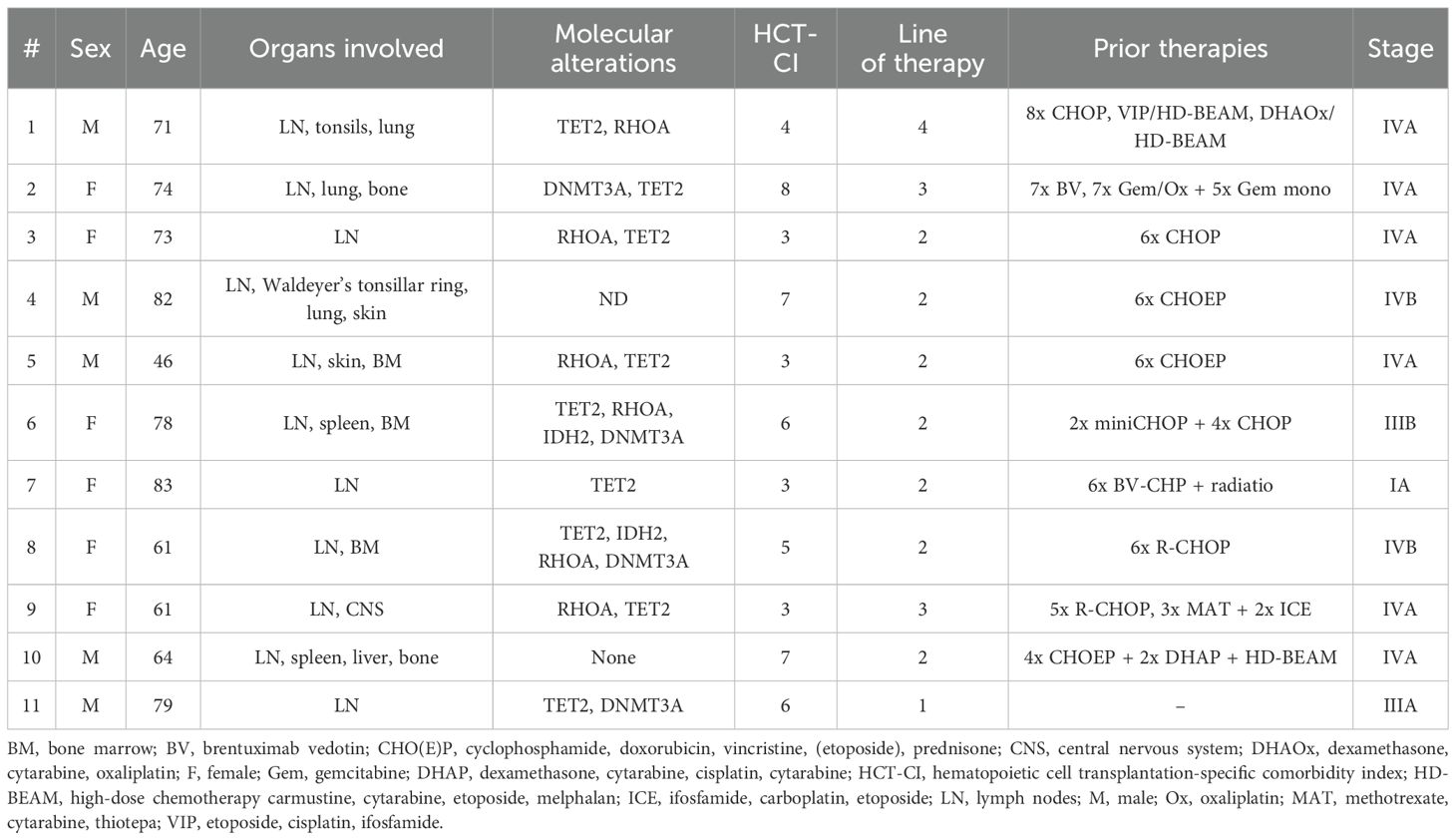
Table 1. Patient characteristics.
The median hematopoietic cell transplantation-specific comorbidity index (HCT-CI) was 5 (range 3–8). One patient suffered from two other lymphomas prior to the start of aza (PTCL, NOS, and EBV-positive atypical B-cell proliferation). Both cancers were in remission when aza was administered. Four patients suffered from EBV-positive diffuse large B-cell lymphoma (DLBCL) simultaneously with TFH lymphoma. In one of these patients, THF lymphoma and DLBCL were treated simultaneously with aza and rituximab. In another patient, TFH lymphoma and DLBCL were treated simultaneously with pola-R-CHP (polatuzumab vedotin, rituximab, cyclophosphamide, doxorubicin, prednisolone) and oral aza. One patient with concomitantly diagnosed myelodysplastic syndrome (MDS) was treated with venetoclax in combination with aza.
3.2 Treatment
All patients received aza for relapsed or refractory disease off-label for this indication. The median number of treatment lines was 2 (range 2–4).
The median cycles of aza were 3 (range 1–10), and the median duration of aza treatment was 74 days (range 6–277 days). To date, two patients are still receiving aza. Three patients were treated with an allogeneic hematopoietic stem cell transplantation (alloHCT) for consolidation. Two were transplanted in partial remission (PR) and one in complete response (CR).
3.3 Safety and efficacy
In general, treatment with aza was well-tolerated. Eight patients developed neutropenia grade 3 or 4, four patients thrombocytopenia grade 3 or 4, and two patients anemia grade 3, respectively. Two patients suffered from a urinary tract infection. One patient had CMV reactivation and oral and esophageal candidiasis. The other patients did not develop major complications.
The complete response rate (CRR) was 36% and the overall response rate (ORR) was 64%. The median PFS was 149 days, and the median overall survival was 236 days (Figure 1). The patients treated with an alloHCT are still alive without relapse. Two patients are still under treatment with aza and in CR after 5 and 10 cycles, respectively (Figure 2). These patients are 78 and 79 years old and have an HCT-CI of 6, which renders them ineligible for intensive chemotherapy or alloHCT. For progressive/relapsed disease under treatment with aza, the response to treatment was poor. All six patients had progressive disease after further treatment. They received between one and four lines of therapy after aza (Table 2).
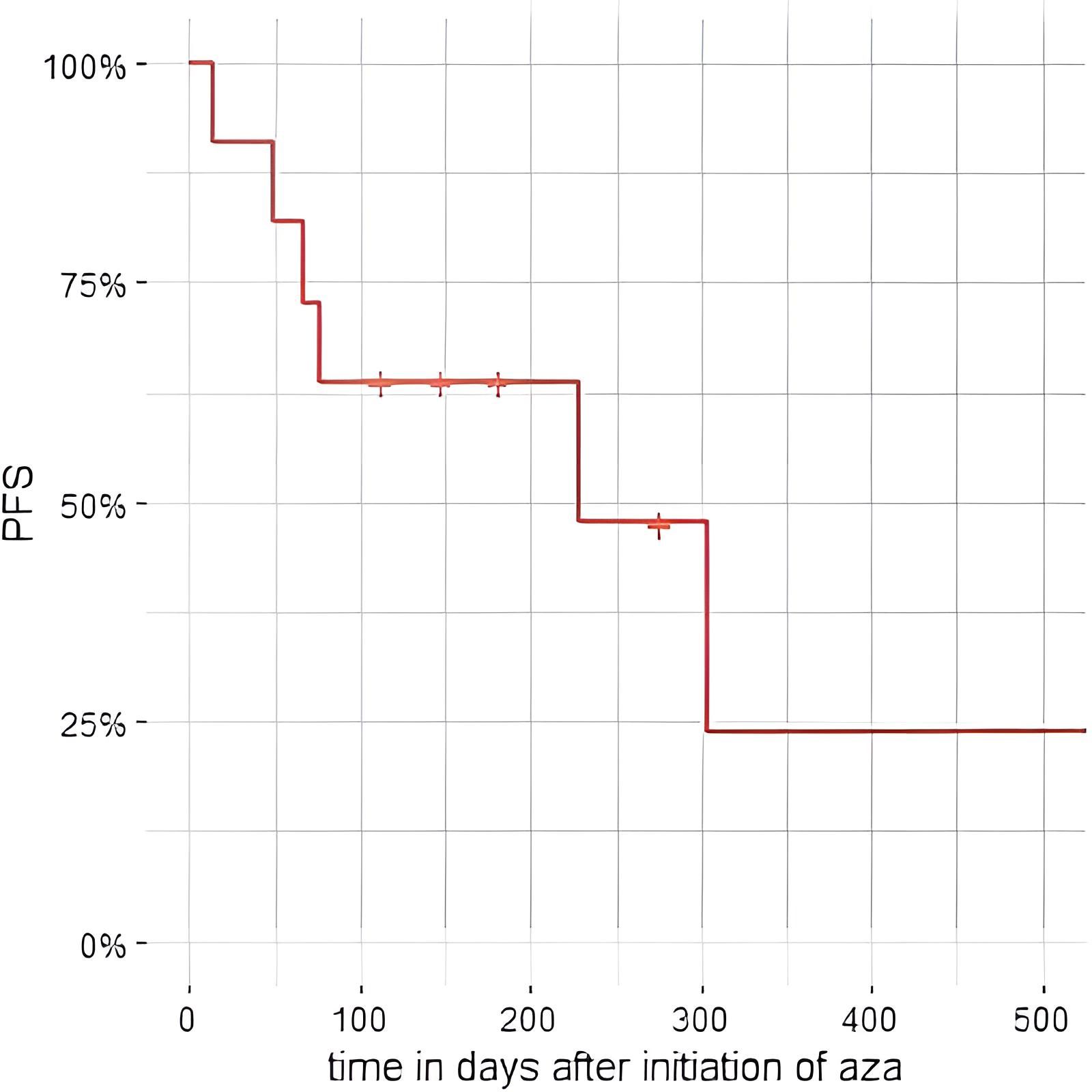
Figure 1. Progression-free survival in % from initiation of azacitidine. PFS, progression-free survival.
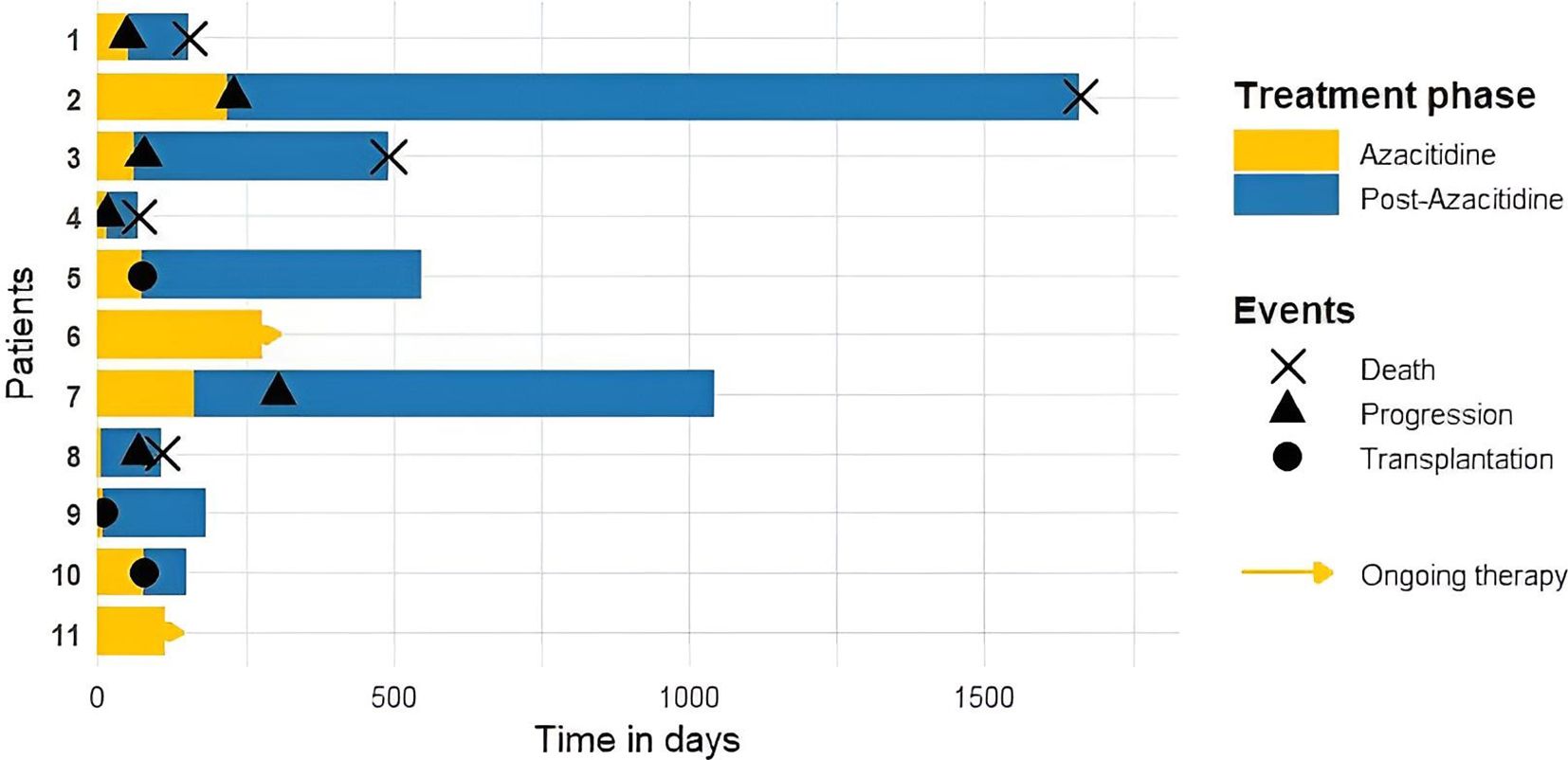
Figure 2. A swimmer plot showing azacitidine treatment, post-azacitidine time, allogeneic stem cell transplantation, progress, and death.
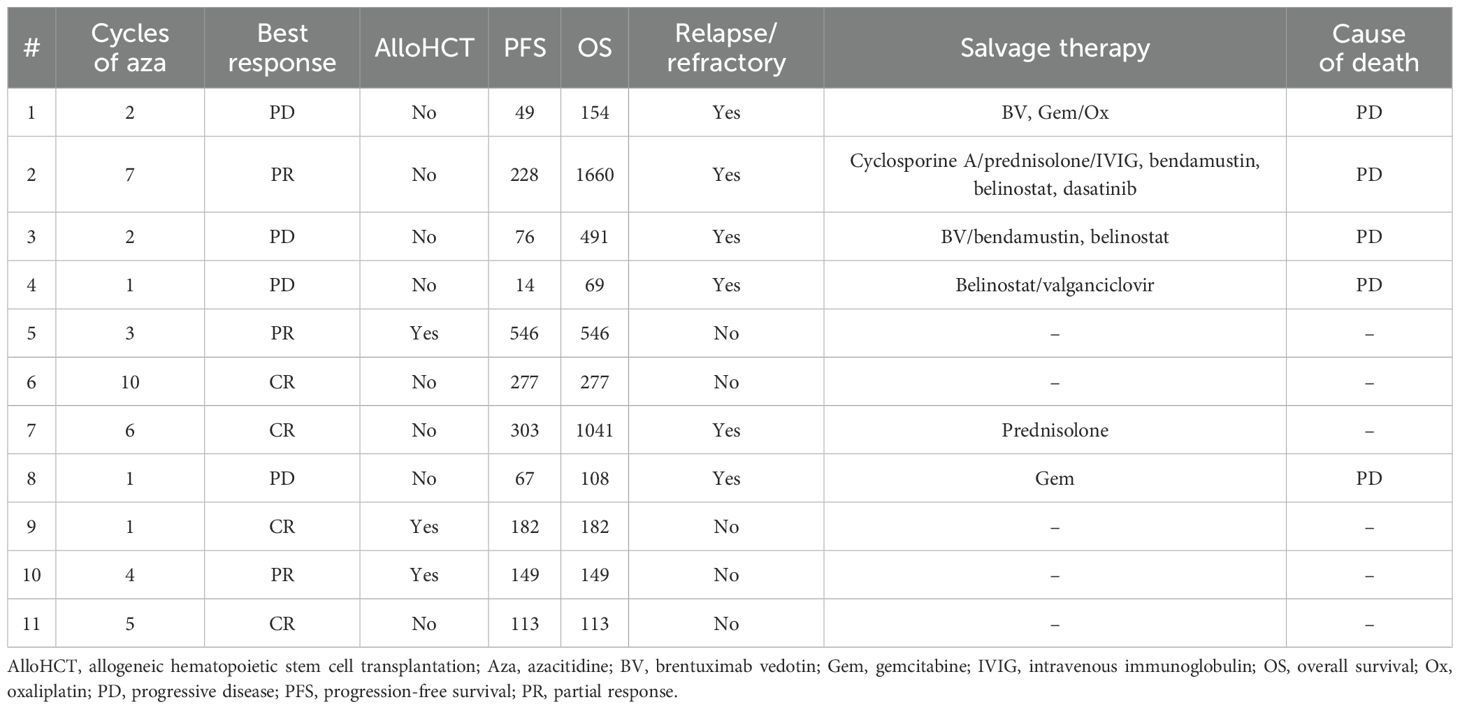
Table 2. Outcome and relapse therapy.
4 Discussion
In our cohort, we observed worse PFS and OS than in the phase 3 study of Dupuis et al. However, our cohort showed a more advanced age (73 vs. 69 years). Our patients also had significant comorbidities (median HCT-CI 5), and eight patients suffered from stage IV disease. Grade 3 or 4 hematologic events occurred in nine patients. However, only one patient suffered from serious infections (CMV reactivation and Candida infection). Interestingly, this patient is still alive and in CR after alloHCT, underscoring the importance of alloHCT for consolidation.
The two patients who are still under treatment with aza without relapse were not eligible for intensive chemotherapy or alloHCT due to their age and comorbidities, underscoring the role of aza in this patient collective.
Retrospective and uncontrolled prospective studies show that despite the dismal prognosis of peripheral T-cell lymphoma, some patients achieve a long-term remission after alloHCT (35, 36). The only patients in our study being in CR after discontinued treatment received alloHCT, which is in line with our knowledge about the value of alloHCT.
The major limitation of our study is the small number of patients. Nevertheless, our study showed the clinical benefit of aza for patients with acceptable tolerability, and aza should be considered as an option for patients with r/r TFH lymphoma of the angioimmunoblastic type, especially if they are ineligible for intensive therapy.
Alternative therapies for patients who are ineligible for intensive chemotherapy and alloHCT are romidepsin, belinostat, and brentuximab vedotin. Romidepsin and belinostat are not approved in Europe for any indication, while brentuximab vedotin like aza is only approved for other indications. Therefore, in addition to the expected efficacy, availability must also be considered. While no head-to-head comparisons are available, the published retrospective series do not suggest a clearly superior choice among these agents. Belinostat showed an ORR of 25% with a median OS of 7.9 months in patients with a variety of PTCLs (12). In patients with THF lymphoma of the angioimmunoblastic type, the ORR was 54% and the PFS was 6.7 months for brentuximab vedotin (37). Romidepsin showed an ORR of 30% for this entity and a PFS of 4 months for all tested PTCLs (13). For aza, the results seem to be similar regarding PFS (5.6 months), but OS seems to be better (18.4 months) in a phase 3 trial (29). Nevertheless, our results did not prove these results. It should also be considered that comparisons between different studies can only be made with caution.
Because of the dismal prognosis of r/r TFH lymphoma of the angioimmunoblastic type and the lack of standard treatments, the approach of using the hypomethylating agent aza for a disease with mutations in epigenetic modifiers should be considered for combination therapy with other therapies to increase the survival of patients, either as a bridge to transplant for patients, who are eligible for alloHCT, or as palliative treatment for patients, who are ineligible for alloHCT.
Further research for the treatment of r/r TFH lymphoma is necessary. Aza offers a treatment approach, and some patients could benefit from aza or combinations of aza with other therapies.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethik-Kommission an der Medizinischen Fakultät der Eberhard-Karls-Universität und am Universitätsklinikum Tübingen. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
PF: Methodology, Formal analysis, Writing – original draft, Data curation, Investigation, Visualization, Writing – review & editing. JS: Methodology, Writing – review & editing, Validation. AR: Writing – review & editing. CS: Writing – review & editing, Methodology. SK: Writing – review & editing. LP: Writing – review & editing. LM: Writing – review & editing. CL: Funding acquisition, Resources, Writing – review & editing. M-FH: Writing – review & editing, Supervision, Validation, Resources, Project administration, Conceptualization.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
JS was supported by the MINT-Clinician Scientist Program of the Medical Faculty Tübingen, funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation)—493665037; AR received funding from the Medical Faculty of Tübingen Junior Clinician Scientist Program—524-0-0. LM received funding from the Medical Faculty of Tübingen Junior Clinician Scientist Program—522-0-0. We acknowledge the support from the Open Access Publication Fund of the University of Tübingen.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhem.2025.1638236/full#supplementary-material
References
1. Anderson JR, Armitage JO, and Weisenburger DD. Epidemiology of the non-Hodgkin’s lymphomas: Distributions of the major subtypes differ by geographic locations. Ann Oncol. (1998) 9:717–20. doi: 10.1023/A:1008265532487
2. Laurent C, Baron M, Amara N, Haioun C, Dandoit M, Maynadié M, et al. Impact of expert pathologic review of lymphoma diagnosis: study of patients from the french lymphopath network. JCO. (2017) 35:2008–17. doi: 10.1200/JCO.2016.71.2083
3. Vose J, Armitage J, and Weisenburger D. International peripheral T-cell and natural killer/T-cell lymphoma study: pathology findings and clinical outcomes. JCO. (2008) 26:4124–30. doi: 10.1200/JCO.2008.16.4558
4. Campo E, Jaffe ES, Cook JR, Quintanilla-Martinez L, Swerdlow SH, Anderson KC, et al. The international consensus classification of mature lymphoid neoplasms: a report from the clinical advisory committee. Blood. (2022) 140:1229–53. doi: 10.1182/blood.2022015851
5. Alaggio R, Amador C, Anagnostopoulos I, Attygalle AD, Araujo IBDO, Berti E, et al. The 5th edition of the world health organization classification of haematolymphoid tumours: lymphoid neoplasms. Leukemia. (2022) 36:1720–48. doi: 10.1038/s41375-022-01620-2
6. AbouYabis AN, Shenoy PJ, Sinha R, Flowers CR, and Lechowicz MJ. A systematic review and meta-analysis of front-line anthracycline-based chemotherapy regimens for peripheral T-cell lymphoma. ISRN Hematology. (2011) 2011:1–14. doi: 10.5402/2011/623924
7. Carson KR, Horwith SM, Pinter-Brown LC, Rosen ST, Pro B, Hsi ED, et al. A prospective cohort study of patients with peripheral T-cell lymphoma in the United States. Cancer. (2016) 123:1174–83. doi: 10.1002/cncr.30416
8. Lunning MA and Vose JM. Angioimmunoblastic T-cell lymphoma: the many-faced lymphoma. Blood. (2017) 129:1095–102. doi: 10.1182/blood-2016-09-692541
9. d’Amore F, Gaulard P, Trümper L, Corradini P, Kim WS, Specht L, et al. Peripheral T-cell lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2015) 26:v108–15. doi: 10.1093/annonc/mdv201
10. Mak V, Hamm J, Chhanabhai M, Shenkier T, Klasa R, Sehn LH, et al. Survival of patients with peripheral T-cell lymphoma after first relapse or progression: spectrum of disease and rare long-term survivors. JCO. (2013) 31:1970–6. doi: 10.1200/JCO.2012.44.7524
11. Dreyling M, Thieblemont C, Gallamini A, Arcaini L, Campo E, Hermine O, et al. ESMO Consensus conferences: guidelines on Malignant lymphoma. part 2: marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann Oncol. (2013) 24:857–77. doi: 10.1093/annonc/mds643
12. O’Connor OA, Horwitz S, Masszi T, Van Hoof A, Brown P, Doorduijn J, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: results of the pivotal phase II BELIEF (CLN-19) study. JCO. (2015) 33:2492–9. doi: 10.1200/JCO.2014.59.2782
13. Coiffier B, Pro B, Prince HM, Foss F, Sokol L, Greenwood M, et al. Results from a pivotal, open-label, phase II study of romidepsin in relapsed or refractory peripheral T-cell lymphoma after prior systemic therapy. JCO. (2012) 30:631–6. doi: 10.1200/JCO.2011.37.4223
14. Piekarz RL, Frye R, Prince HM, Kirschbaum MH, Zain J, Allen SL, et al. Phase 2 trial of romidepsin in patients with peripheral T-cell lymphoma. Blood. (2011) 117:5827–34. doi: 10.1182/blood-2010-10-312603
15. O’Connor OA, Pro B, Pinter-Brown L, Bartlett N, Popplewell L, Coiffier B, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. JCO. (2011) 29:1182–9. doi: 10.1200/JCO.2010.29.9024
16. Lemonnier F, Couronné L, Parrens M, Jaïs JP, Travert M, Lamant L, et al. Recurrent TET2 mutations in peripheral T-cell lymphomas correlate with TFH-like features and adverse clinical parameters. Blood. (2012) 120:1466–9. doi: 10.1182/blood-2012-02-408542
17. Sakata-Yanagimoto M, Enami T, Yoshida K, Shiraishi Y, Ishii R, Miyake Y, et al. Somatic RHOA mutation in angioimmunoblastic T cell lymphoma. Nat Genet. (2014) 46:171–5. doi: 10.1038/ng.2872
18. Palomero T, Couronné L, Khiabanian H, Kim MY, Ambesi-Impiombato A, Perez-Garcia A, et al. Recurrent mutations in epigenetic regulators, RHOA and FYN kinase in peripheral T cell lymphomas. Nat Genet. (2014) 46:166–70. doi: 10.1038/ng.2873
19. Cairns RA, Iqbal J, Lemonnier F, Kucuk C, De Leval L, Jais JP, et al. IDH2 mutations are frequent in angioimmunoblastic T-cell lymphoma. Blood. (2012) 119:1901–3. doi: 10.1182/blood-2011-11-391748
20. Quivoron C, Couronné L, Della Valle V, Lopez CK, Plo I, Wagner-Ballon O, et al. TET2 inactivation results in pleiotropic hematopoietic abnormalities in mouse and is a recurrent event during human lymphomagenesis. Cancer Cell. (2011) 20:25–38. doi: 10.1016/j.ccr.2011.06.003
21. Wang C, McKeithan TW, Gong Q, Zhang W, Bouska A, Rosenwald A, et al. IDH2 R172 mutations define a unique subgroup of patients with angioimmunoblastic T-cell lymphoma. Blood. (2015) 126:1741–52. doi: 10.1182/blood-2015-05-644591
22. Yoo HY, Sung MK, Lee SH, Kim S, Lee H, Park S, et al. A recurrent inactivating mutation in RHOA GTPase in angioimmunoblastic T cell lymphoma. Nat Genet. (2014) 46:371–5. doi: 10.1038/ng.2916
23. Stresemann C and Lyko F. Modes of action of the DNA methyltransferase inhibitors azacytidine and decitabine. Int J Cancer (2008) 123:8–13. doi: 10.1002/ijc.23607
24. Fenaux P, Mufti GJ, Hellstrom-Lindberg E, Santini V, Finelli C, Giagounidis A, et al. Efficacy of azacitidine compared with that of conventional care regimens in the treatment of higher-risk myelodysplastic syndromes: a randomised, open-label, phase III study. Lancet Oncol. (2009) 10:223–32. doi: 10.1016/S1470-2045(09)70003-8
25. Dombret H, Seymour JF, Butrym A, Wierzbowska A, Selleslag D, Jang JH, et al. International phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. (2015) 126:291–9. doi: 10.1182/blood-2015-01-621664
26. Marchi E, Zullo KM, Amengual JE, Kalac M, Bongero D, McIntosh CM, et al. The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol. (2015) 171:215–26. doi: 10.1111/bjh.13566
27. Lemonnier F, Dupuis J, Sujobert P, Tournillhac O, Cheminant M, Sarkozy C, et al. Treatment with 5-azacytidine induces a sustained response in patients with angioimmunoblastic T-cell lymphoma. Blood. (2018) 132:2305–9. doi: 10.1182/blood-2018-04-840538
28. Yoon SE, Cho J, Kim YJ, Kim SJ, and Kim WS. Real-world efficacy of 5-azacytidine as salvage chemotherapy for angioimmunoblastic T-cell lymphoma. Clin Lymphoma Myeloma Leukemia. (2022) 22:e972–80. doi: 10.1016/j.clml.2022.07.009
29. Dupuis J, Bachy E, Morschhauser F, Cartron G, Fukuhara N, Daguindau N, et al. Oral azacitidine compared with standard therapy in patients with relapsed or refractory follicular helper T-cell lymphoma (ORACLE): an open-label randomised, phase 3 study. Lancet Haematology. (2024) 11:e406–14. doi: 10.1016/S2352-3026(24)00102-9
30. Ruan J, Moskowitz AJ, Mehta-Shah N, Sokol L, Chen Z, Kotlov N, et al. Multicenter Phase 2 Study of Oral azacitidine (CC-486) plus CHOP as initial treatment for peripheral T-cell lymphoma. Blood. (2023) 141:2194–205. doi: 10.1182/blood.2022018254
31. Kalac M, Jain S, Tam CS, Xiao Z, Montanari F, Kanakry J, et al. Real-world experience of combined treatment with azacitidine and romidepsin in patients with peripheral T-cell lymphoma. Blood Advances. (2023) 7:3760–3. doi: 10.1182/bloodadvances.2022009445
32. Falchi L, Ma H, Klein S, Lue JK, Montanari F, Marchi E, et al. Combined oral 5-azacytidine and romidepsin are highly effective in patients with PTCL: a multicenter phase 2 study. Blood. (2021) 137:2161–70. doi: 10.1182/blood.2020009004
33. Ding K, Liu H, Yang H, Zhu H, Ma J, Peng H, et al. A prospective phase 2 study of combination epigenetic therapy against relapsed/refractory peripheral T cell lymphoma. Med. (2024) 5:1393–401.e2. doi: 10.1016/j.medj.2024.07.007
34. O’Connor OA, Falchi L, Lue JK, Marchi E, Kinahan C, Sawas A, et al. Oral 5-azacytidine and romidepsin exhibit marked activity in patients with PTCL: a multicenter phase 1 study. Blood. (2019) 134:1395–405. doi: 10.1182/blood.2019001285
35. Corradini P, Dodero A, Zallio F, Caracciolo D, Casini M, Bregni M, et al. Graft-versus-lymphoma effect in relapsed peripheral T-cell non-hodgkin’s lymphomas after reduced-intensity conditioning followed by allogeneic transplantation of hematopoietic cells. JCO. (2024) 22:2172–6.
36. Kyriakou C, Canals C, Finke J, Kobbe G, Harousseau JL, Kolb HJ, et al. Allogeneic stem cell transplantation is able to induce long-term remissions in angioimmunoblastic T-cell lymphoma: A retrospective study from the lymphoma working party of the european group for blood and marrow transplantation. JCO. (2009) 27:3951–8. doi: 10.1200/JCO.2008.20.4628
Keywords: azacitidine, PTCL, orphan disease, nodal T-follicular helper cell lymphoma, angioimmunoblastic T-cell lymphoma, T-cell lymphoma
Citation: Faustmann P, Schroeder JC, Riedel A, Schürch CM, Killinger S, Phely L, Mix L, Lengerke C and Häring M-F (2025) Real-world data of azacitidine for relapsed/refractory nodal T-follicular helper cell lymphoma in 11 patients. Front. Hematol. 4:1638236. doi: 10.3389/frhem.2025.1638236
Received: 30 May 2025; Accepted: 18 August 2025;
Published: 25 September 2025.
Edited by:
Bhavana Bhatnagar, West Virginia University, United StatesReviewed by:
Pier Paolo Piccaluga, University of Bologna, ItalyMarzia Palma, Karolinska Institutet (KI), Sweden
Copyright © 2025 Faustmann, Schroeder, Riedel, Schürch, Killinger, Phely, Mix, Lengerke and Häring. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Philipp Faustmann, UGhpbGlwcC5mYXVzdG1hbm5AbWVkLnVuaS10dWViaW5nZW4uZGU=