 Catarina Fernandes1*
Catarina Fernandes1* Rita Costa e Sousa2Pedro Santos1Cátia Almeida2Adriana Roque2Ana Luísa Pinto3Joaquim Monteiro3Anabela Neves4Maria João Ramos5Rita Coutinho5,6,7Filipa Mousinho8Mariana Leal Fernandes9Margarida Badior10Cristina João11,12Sónia Leocádio11
Rita Costa e Sousa2Pedro Santos1Cátia Almeida2Adriana Roque2Ana Luísa Pinto3Joaquim Monteiro3Anabela Neves4Maria João Ramos5Rita Coutinho5,6,7Filipa Mousinho8Mariana Leal Fernandes9Margarida Badior10Cristina João11,12Sónia Leocádio11 Ana Luísa Tomé13Margarida Carrolo14
Ana Luísa Tomé13Margarida Carrolo14 Sara Dias12Maria Gomes da Silva1João Paulo Fernandes14
Sara Dias12Maria Gomes da Silva1João Paulo Fernandes14- 1Hematology Department, Portuguese Institute of Oncology, Lisbon, Portugal
- 2Clinical Hematology Department, Unidade Local de Saúde (ULS) Coimbra, Coimbra, Portugal
- 3Hematology Department, ULS São João, Porto, Portugal
- 4Hematology Department, ULS da Arrábida, Setúbal, Portugal
- 5Oncology Department, ULS Santo António, Porto, Portugal
- 6Department of Hematology and Bone Marrow Transplantation, Portuguese Institute of Oncology, Porto, Portugal
- 7Institute of Biomedical Sciences Abel Salazar, University of Porto, Porto, Portugal
- 8Hematology Department, Unidade Local de Saúde (ULS) Lisboa Ocidental, Lisbon, Portugal
- 9Hematology Department, ULS de São José, Lisbon, Portugal
- 10Hematology Department, ULS Gaia e Espinho, Porto, Portugal
- 11Hemato-Oncology Unit, Champalimaud Foundation, Lisbon, Portugal
- 12NOVA Medical School, Universidade Nova de Lisboa, Lisbon, Portugal
- 13Hemato-Oncology Department, ULS Almada-Seixal, Lisbon, Portugal
- 14Hemato-Oncology Unit, Hospital CUF, Lisbon, Portugal
Background: Mantle cell lymphoma is usually characterized by an aggressive and recurrent course. Clinical trials and real-world series have demonstrated clinical benefits with the use of ibrutinib as a second-line treatment, compared to later relapses.
Objective: To evaluate the Portuguese experience with the use of ibrutinib in patients with relapsed or refractory mantle cell lymphoma since its approval in the country.
Methods: A multicenter retrospective cohort of patients with mantle cell lymphoma who received ibrutinib between 2015 and 2020 was studied.
Results: Ninety-five patients treated at 11 hospitals were included. At the ibrutinib starting date, 51% of patients had high-risk simplified mantle cell lymphoma international prognostic index, 9% had central nervous system involvement, and 21% had Eastern Cooperative Oncology Group performance status ≥2. The median treatment duration was 10 (<1-75) months. The overall response rate was 66%, including 36% with complete responses. After 18 months of follow-up, seventy-two patients (76%) had discontinued ibrutinib, mainly due to progressive disease (61%) and toxicity (21%). At the last follow-up, 24% of patients were still on ibrutinib, and 60% had died, mostly (65%) due to lymphoma progression.
Conclusions: In this real-world series, the safety of ibrutinib is similar to the results described in clinical trials. However, new strategies are needed for the treatment of acquired resistance to ibrutinib.
1 Introduction
Mantle cell lymphoma (MCL) is a rare and aggressive subtype of B cell non-Hodgkin lymphoma (NHL) and accounts for approximately 5 to 7% of all NHL, with an incidence rate of 0.45 cases per 100, 000 person-years in Europe (1, 2). Most patients are diagnosed at an older age (median 65 years), making them unsuitable candidates for aggressive treatment, which may contribute to unsatisfactory clinical outcomes. Most patients have a multiple relapsing clinical course (3, 4).
Ibrutinib (IBT), a first-generation, once-daily, oral, covalently binding inhibitor of Bruton’s tyrosine kinase (BTK) has revolutionized the care of patients with relapsed or refractory (R/R) MCL and is currently established as standard-of-care in this setting since its approval in 2013 (5, 6). It has been associated with response rates of 54%–72% in patients with R/R MCL, with complete response (CR) rates in the 19%–23% range (7). Although no trials have compared it with immunochemotherapy, BTK inhibitors are now well accepted as standard second line therapy. A pooled analysis of three clinical trials in patients with R/R MCL treated with IBT demonstrated a significant benefit in progression-free survival (PFS) and overall survival (OS) for patients treated at first relapse (median PFS 25.4 months) compared to those treated at later relapses (median PFS 10.3 months), suggesting that earlier treatment with IBT may offer greater benefit (6, 8, 9). This is further demonstrated by the MANTLE-FIRST study that showed that IBT was associated with improved outcomes in patients with early progression of disease (10). Additionally, recent findings from the LATE-POD study showed improved outcomes in younger patients with MCL with late relapses also, with a more favorable response to IBT than immunochemotherapy in a non-randomized comparison (11).
In this real-world retrospective study, we describe the clinical characteristics, management and outcomes of patients with R/R MCL receiving IBT in a real-world setting.
2 Materials and methods
Eleven Portuguese centers were involved in this multicenter retrospective study. Eligibility criteria included patients diagnosed with MCL that started IBT between January 2015 and December 2020 for R/R disease. Data was collected from medical records concerning clinical characteristics at diagnosis, pathology and imaging data and therapies used pre-IBT. Response data were provided according to the Lugano classification (12). The safety profile of IBT was also evaluated based on the adverse events, according to CTCAE v5.0, reported during treatment with IBT, and the dose modifications and treatment discontinuations due to adverse events.
The clinical outcomes included overall response rate (ORR), CR rate, time to next treatment (TTNT), PFS and OS. ORR was defined as the proportion of patients achieving CR or partial response (PR) per investigator assessment according to standard criteria. TTNT was defined as the interval from day 1 of IBT therapy to the day 1 of the next line of treatment, whichever occurred first. PFS was defined as the time from day 1 of IBT therapy to disease progression or death from any cause, whichever occurred first. OS was defined as the time from day 1 of IBT therapy to death from any cause. Progression of disease (POD) after frontline treatment was categorized as occurring within 24 months (POD24) or later. Patients without an event were censored at the date of last follow-up. Discontinuation due to toxicity or stem-cell transplantation was treated as a censoring event at the corresponding date.
Survival curves were estimated using the Kaplan–Meier method, and differences between groups were compared using the log-rank test. The median survival times and 95% confidence intervals (CIs) were reported from the Kaplan–Meier estimates. To adjust for potential confounders [age, Eastern Cooperative Oncology Group performance status (ECOG PS), simplified mantle cell lymphoma international prognostic index (sMIPI), blastoid morphology, POD24, and prior lines of therapy], Cox proportional hazards regression models were fitted to estimate hazard ratios (HRs) with corresponding 95% CIs. The proportional hazards assumption was verified by examining Schoenfeld residuals and log–log survival plots. In analyses with competing events (e.g., non–disease-related death), competing risks models were applied using the Fine–Gray subdistribution hazard approach. The median follow-up time was estimated using the reverse Kaplan–Meier method, considering censoring as the event.
Statistical analyses were conducted with Stata BE version 18.0 (StataCorp, College Station, TX, USA). Two-sided p < 0.05 was considered statistically significant.
All patient data were anonymized and treated according to the principles of the declaration of Helsinki.
3 Results
3.1 Patient characteristics
Ninety-five eligible patients were included. At diagnosis, the median age was 66 years (range: 32-86) and 72% were male. Eighty-eight (96%) had stage III–IV disease, 17% (13/78) presented a blastoid histology and 48% (24/50) had a Ki-67 expression ≥ 30% (Table 1).
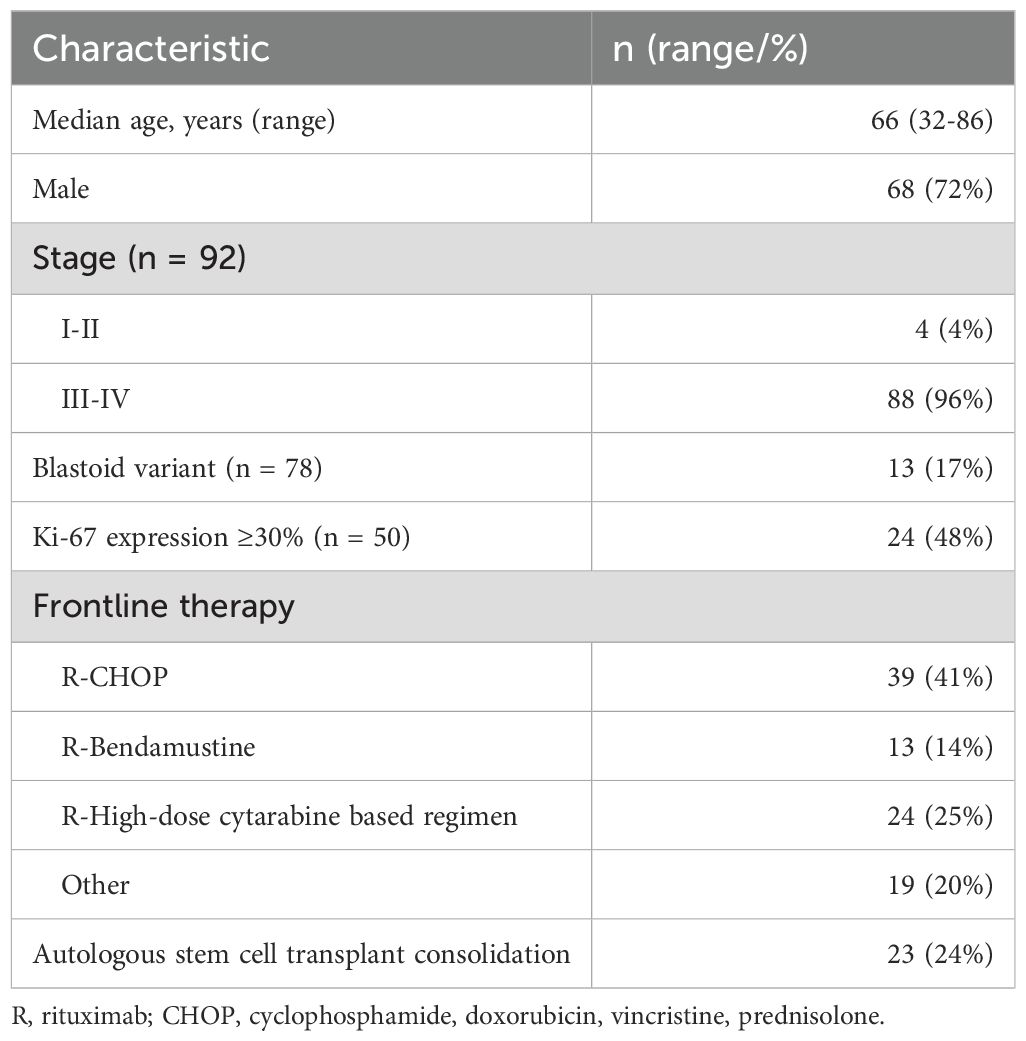
Table 1. Patients baseline characteristics at diagnosis (n=95).
Regarding pre-IBT therapy, 45% of patients were treated with only one line before IBT. As to the first line, 80% of patients received up-front conventional immunochemotherapy. Twenty-five percent received rituximab combined with high-dose cytarabine-based frontline therapy (Table 1). The most frequent conventional non-intensive regimen was R-CHOP (41%) followed by R-Bendamustine (14%) (Table 1). Nineteen percent of patients had a primary refractory disease. Twenty-four percent of patients received autologous hematopoietic stem cell transplant (ASCT) as a first-line consolidation therapy (Table 1) and 33% received rituximab maintenance.
3.2 Ibrutinib therapy
The median time from diagnosis to the start of IBT was 31 months (range: 2-158). After the end of first-line therapy, 53% (23/43) patients relapsed within the first 2 years (POD24).
The median age at IBT start was 70 years old (range: 37–87). The ECOG PS at this time was 0–1 in 79% (60/76) of the patient and sMIPI was high in 51% (39/76). Central nervous system (CNS) involvement was demonstrated in 9% (7/76). In the subgroup who had CNS involvement, 71% had one prior line, 71% presented with primary refractory disease and 5/7 relapsed within the first 2 years (POD24).
In the subgroup who had one prior line of treatment, the median age at start of IBT was 72 years (range: 37–87), 46% (15/33) had high risk sMIPI, 53% (23/43) were POD24, 19% (8/43) had a primary refractory disease and 15% (5/33) had ECOG PS 2-4.
Forty-one percent of patients started IBT less than 24 months after the diagnosis of MCL, independently of the number of prior lines of treatment.
With a median treatment duration of 10 months (range: <1-75), the ORR of IBT was 66% (95%CI 56-75) (62/94) with CR in 36% (95%CI 27-46) (34/94).
The median duration of follow-up was 22.6 months (95% CI, 33.8-52.0).
The median OS was 23.3 months (95% CI 8.6-NR) (Figure 1). In univariate analysis, only ECOG PS>=2 (HR 2.18, 95% CI 1.13-4.20; p=0.020), sMIPI high risk (vs low/moderate) (HR 2.08, 95% CI 1.12-3.88; p=0.021) (Figure 1), POD24 (HR 2.29, 95% CI 1.33-3.94; p=0.003) and Ki-67 expression >30% (HR 5.78, 95% CI 2.34-14.26; p<0.001) were significantly associated with inferior OS. There was a trend toward worse OS with an increasing number of previous treatment lines (2 lines: HR 1.50, 95% CI 0.78-2.89; p=0.224; ≥3 lines: HR 1.67, 95% CI 0.88-3.19; p=0.119) (Figure 1). Age and blastoid morphology were not significantly associated with outcome (p=0.112 and 0.231, respectively).

Figure 1. Overall survival of relapsed and/or refractory mantle cell lymphoma patients treated with ibrutinib (A). Overall survival of relapsed and/or refractory mantle cell lymphoma patients from the initiation of ibrutinib treatment by number of previous lines (B). Overall survival of relapsed and/or refractory mantle cell lymphoma patients from the initiation of ibrutinib treatment according sMIPI (C).
After multivariate Cox regression model, POD24 (HR 6.59, 95% CI 1.69-25.69; p= 0.007) and Ki-67 expression (HR 12.02; 95% CI 4.46-32.90; p<0.001) remained independent predictors of inferior overall survival.
The median PFS was 12.9 months (95% CI 2.9-34.1) (Figure 2). In the univariate analysis, older age (HR = 1.03; 95% CI 1.01-1.06; p=0.011), ECOG PS ≥2 (HR 2.19; 95% CI 1.20-3.99; p=0.010), POD24 (HR 2.02; 95% CI 1.23-3.31; p=0.006), and Ki-67 expression >30% (HR 4.96; 95% CI 2.26-10.86; p<0.001) were significantly associated with inferior PFS. A trend toward shorter PFS was also observed in patients with ≥3 treatment lines (HR 1.78; 95% CI 1.00-3.18; p= 0.051) (Figure 2) and in those with blastoid morphology (HR 1.87; 95% CI 0.98-3.56; p=0.056), whereas s-MIPI was not significantly associated with PFS (p=0.244) (Figure 2).
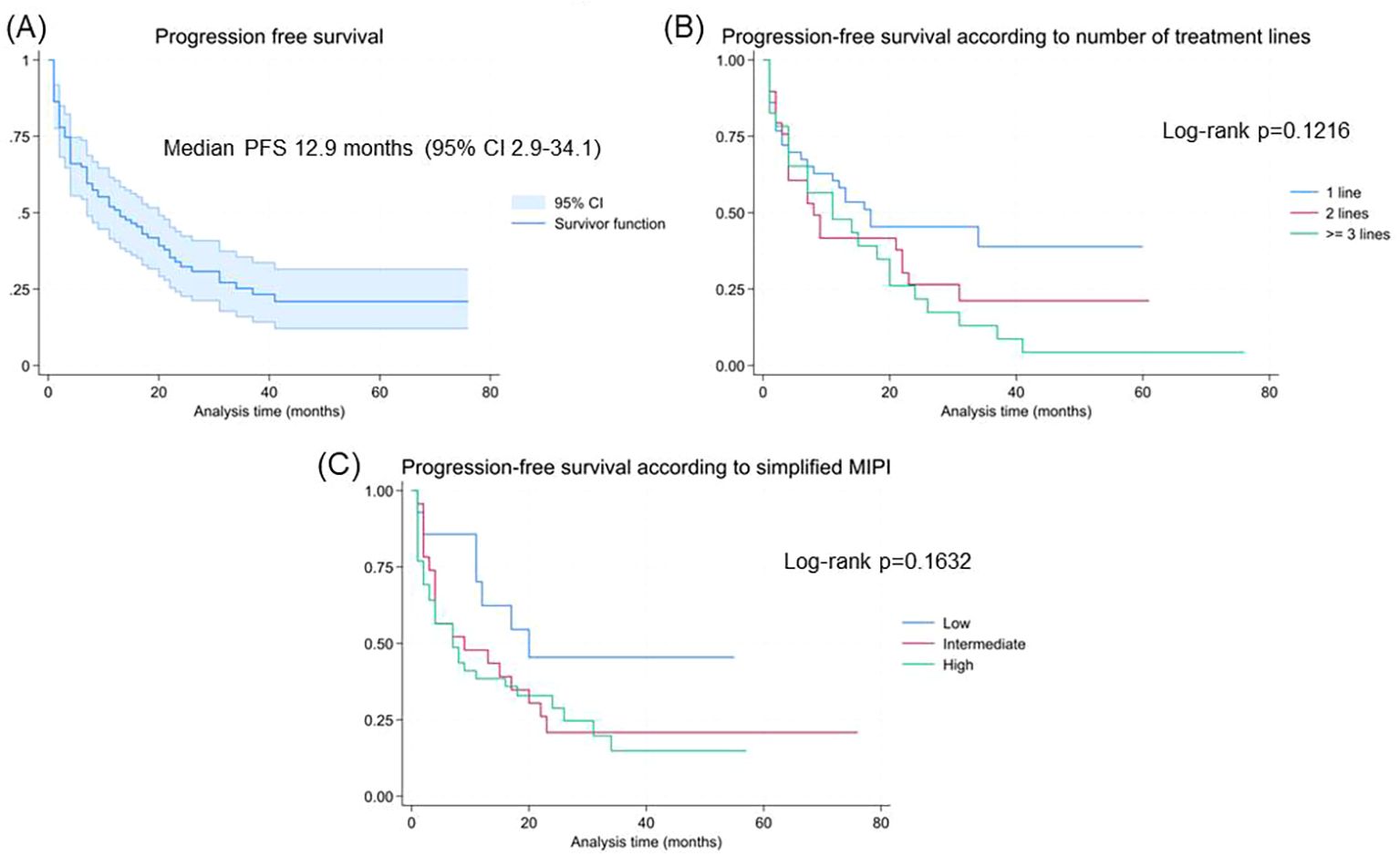
Figure 2. Progression-free survival of relapsed and/or refractory mantle cell lymphoma patients treated with ibrutinib (A). Progression-free survival of relapsed and/or refractory mantle cell lymphoma patients from the initiation of ibrutinib treatment by number of previous lines (B). Progression-free survival of relapsed and/or refractory mantle cell lymphoma patients from the initiation of ibrutinib treatment according sMIPI (C).
In the multivariate Cox regression model for PFS, POD24 (HR 5.03; 95% CI 1.84-13.97; p=0.002) and Ki-67 expression >30% (HR 9.30; 95% CI 2.11-40.95; p=0.003) remained independent predictors of inferior PFS.
3.3 Safety
At the time of last follow-up, 23 patients (24%) were still on treatment and 76% patients stopped IBT, 21% due to adverse event.
Thirty-five (36%) patients had grade 3/4 adverse events. The most frequent toxicities were hematological in 17% of patients, followed by infectious (9%), gastrointestinal (4%) and musculoskeletal (4%) (Table 2). Dose reductions of IBT were required in 25 (26%) patients.
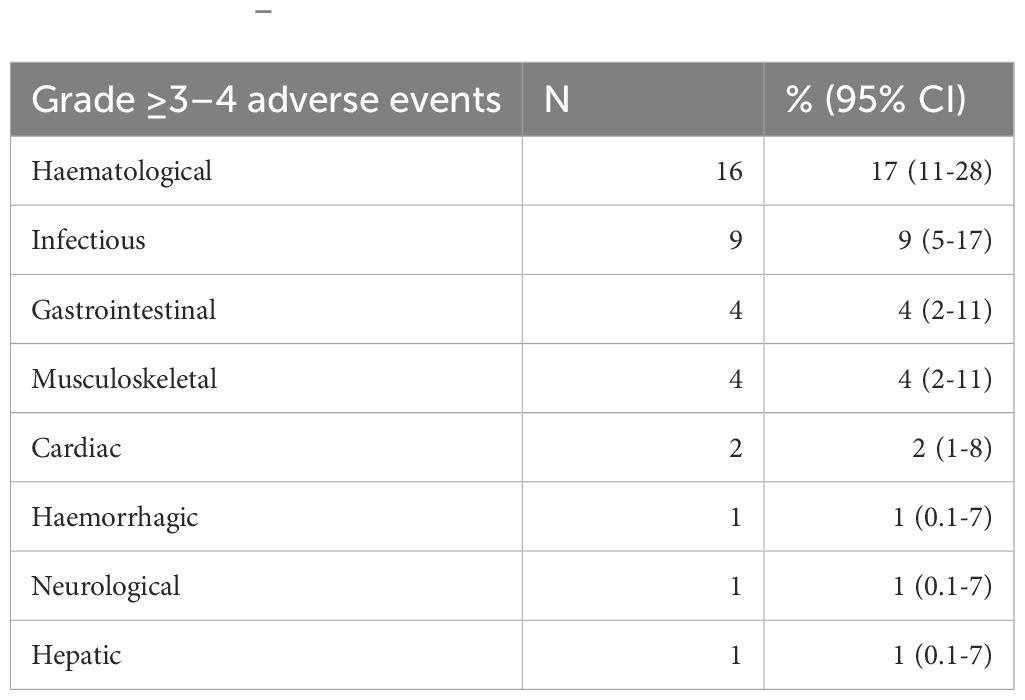
Table 2. Grade 3–4 adverse events during treatment with ibrutinib.
At the time of last follow-up, 57 (60%) patients died because of progressive disease (65%), toxicity (11%) or unknown causes (25%).
3.4 Post-ibrutinib treatment
At the time of last follow-up, 76% patients discontinued IBT: 61% due to progressive disease, 21% due to adverse event, 7% to receive consolidation with allogeneic SCT and 11% for unknown causes.
Forty-six percent of patients received subsequent therapy for MCL after discontinuation of IBT, with a median TTNT of 25.9 months (95% CI, 9.3-NR).
The first subsequent therapies used after IBT consisted of rituximab, bendamustine, cytarabine (R-BAC)-like regimens (26%), R-bendamustine regimens (24%), lenalidomide-based regimens (13%), R-CHOP-like regimens (5%), palliative care regimens (24%) and others (8%).
4 Discussion
This multicentric Portuguese retrospective analysis centered in the use of IBT in the management of patients with R/R MCL supports the tolerability and effectiveness of IBT in MCL in a real-world context.
This series is enriched with high-risk MCL patients, displaying distinct characteristics when compared to other real-world series: our cohort included 96% of patients with advanced-stage MCL, a significantly higher percentage compared to the 78.3% reported by Cencini et al. (13). CNS involvement was observed in 9%, markedly higher than the 4% reported by McCulloch et al. (4). High sMIPI was present in 51% of our cohort, considerably more than the 30.4% in Cencini et al. (13) and the 26.3% in the PCYC-1104, SPARK, and RAY trials (8). In our study, 21% of patients had a ECOG PS ≥2. This specific variable is not directly compared in the cited studies, but underscores the frailty of our cohort. The blastoid/pleomorphic variant was identified in 17% of our patients, higher than the 10.2% reported by Cencini et al. (13). In our study, 55% of patients had received ≥2 prior lines of therapy, in contrast to McCulloch et al. (4), where all patients had only one prior line of therapy. Our cohort included elderly patients, reflected in the high proportion of non-intensively pre-treated individuals. These significant differences in patient characteristics likely may explain the lower median PFS observed in our study in comparison with previously reported real-world series. Despite these challenges, we observed favorable outcomes with IBT treatment, with an ORR of 66% and an OS of 23.3 months, consistent with results from other real-world retrospective analyses (4, 13, 14).
Given the sample size of our study population, no significant benefit in PFS and OS was observed for treatment with IBT at first relapse compared to latter lines. The median PFS was longer in patients at first relapse compared with those in later treatment lines. This finding may be explained by more aggressive disease characteristics in this group, including POD24, elevated Ki-67 expression, poor ECOG PS and an elderly population.
Despite 35% of the toxicities being grade 3-4, they were manageable. The majority of those were hematological, highlighting the low cardiovascular and hemorrhagic toxicities observed in this series.
In this study, 7% of patients were consolidated with allogeneic SCT, supporting the use of IBT as a possible bridging therapy to allogeneic SCT in R/R MCL, and leading us to hypothesize that a similar or higher proportion would have been candidates to cellular therapy (not approved in Portugal at that time).
Sixty-one per cent of the patients stopped IBT because of disease progression, demonstrating the need for new treatments and combinations in this population. In this setting, CAR-T cell therapy (15) and bispecific antibodies (16) have proven to be promising approaches. The results of phase 3 TRIANGLE trial (17) can change the paradigm of first line treatment of MCL by demonstrating that high-dose regimens are not superior to IBT-containing regimen without ASCT as consolidation. This will most probably have consequences upon second line treatment options and the role of T cell engaging therapies in the treatment algorithm.
This study has several limitations, including missing data inherent to its retrospective nature, the lack of central histological and response evaluation review and the absence of data on high-risk characteristics, including TP53 mutations and deletions. Despite these limitations, this study provides real-world evidence on the use of IBT in R/R MCL in clinical practice, with 24% of the patients still in remission at last follow-up.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comissão de Ética da ULS Coimbra Unidade Local de Saúde de Coimbra. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
CF: Writing – original draft, Writing – review & editing. RC: Writing – original draft, Writing – review & editing. PS: Writing – review & editing. CA: Writing – review & editing. AR: Writing – review & editing. AP: Writing – review & editing. JM: Writing – review & editing. AN: Writing – review & editing. MR: Writing – review & editing. RC: Writing – review & editing. FM: Writing – review & editing. MF: Writing – review & editing. MB: Writing – review & editing. CJ: Writing – review & editing. SL: Writing – review & editing. AT: Writing – review & editing. MC: Writing – review & editing. SD: Writing – review & editing. Md: Writing – review & editing. JF: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
The authors thank the following healthcare professionals for assisting with the data collection for this study. They would also like to thank the Portuguese Lymphoma Group for supporting this project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Armitage JO and Longo DL. Mantle-cell lymphoma. N Engl J Med. (2022) 386:2495–506. doi: 10.1056/NEJMra2202672
2. Sant M, Allemani C, Tereanu C, De Angelis R, Capocaccia R, Visser O, et al. Incidence of hematologic Malignancies in Europe by morphologic subtype: results of the HAEMACARE project. Blood. (2010) 116:3724–34. doi: 10.1182/blood-2010-05-282632
3. Broccoli A, Casadei B, Morigi A, Sottotetti F, Gotti M, Spina M, et al. Italian real life experience with ibrutinib: results of a large observational study on 77 relapsed/refractory mantle cell lymphoma. Oncotarget. (2018) 9:23443–50. doi: 10.18632/oncotarget.25215
4. McCulloch R, Lewis D, Crosbie N, Eyre TA, Bolam S, Arasaretnam A, et al. Ibrutinib for mantle cell lymphoma at first relapse: a United Kingdom real-world analysis of outcomes in 211 patients. Br J Haematol. (2021) 193:290–8. doi: 10.1111/bjh.17363
5. Zelenetz AD, Gordon LI, Chang JE, Christian B, Abramson JS, Advani RH, et al. NCCN guidelines® Insights: B-cell lymphomas, version 5.2021. J Natl Compr Canc Netw. (2021) 19:1218–30. doi: 10.6004/jnccn.2021.0054
6. Dreyling M, Goy A, Hess G, Kahl BS, Hernández-Rivas J, Schuier N, et al. Long-term outcomes with ibrutinib treatment for patients with relapsed/refractory mantle cell lymphoma: A pooled analysis of 3 clinical trials with nearly 10 years of follow-up. HemaSphere. (2022) 6:e712. doi: 10.1097/HS9.0000000000000712
7. Dreyling M, Jurczak W, Jerkeman M, Silva RS, Rusconi C, Trneny M, et al. Ibrutinib versus temsirolimus in patients with relapsed or refractory mantle-cell lymphoma: an international, randomised, open-label, phase 3 study. Lancet. (2016) 387:770–8. doi: 10.1016/S0140-6736(15)00667-4. Erratum in: Lancet. 2016 Feb 20;387(10020):750.
8. Rule S, Dreyling M, Goy A, Hess G, Auer R, Kahl B, et al. Outcomes in 370 patients with mantle cell lymphoma treated with ibrutinib: a pooled analysis from three open-label studies. Br J Haematol. (2017) 179:430–8. doi: 10.1111/bjh.14870
9. Rule S, Dreyling M, Goy A, Hess G, Auer R, Kahl B, et al. Ibrutinib for the treatment of relapsed/refractory mantle cell lymphoma: extended 3.5-year follow up from a pooled analysis. Haematologica. (2019) 104:e211–e4. doi: 10.3324/haematol.2018.205229
10. Visco C, Di Rocco A, Evangelista A, Quaglia FM, Tisi MC, Morello L, et al. Outcomes in first relapsed-refractory younger patients with mantle cell lymphoma: results from the MANTLE-FIRST study. Leukemia. (2021) 35:787–95. doi: 10.1038/s41375-020-01013-3. Erratum in: Leukemia. 2021 Mar;35(3):932. doi: 10.1038/s41375-020-01119-8.
11. Malinverni C, Bernardelli A, Glimelius I, Mirandola M, Smedby KE, Tisi MC, et al. Outcomes of younger patients with mantle cell lymphoma experiencing late relapse (>24 months): the LATE-POD study. Blood. (2024) 144:1001–9. doi: 10.1182/blood.2023023525
12. Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. (2014) 32:3059–68. doi: 10.1200/JCO.2013.54.8800
13. Cencini E, Mecacci B, Morelli F, Ghio F, Romano I, Birtolo S, et al. Ibrutinib in patients with relapsed/refractory mantle cell lymphoma: a real-life, retrospective, multicenter trial on behalf of the "RTL" (regional Tuscan lymphoma network). Am J Blood Res. (2021) 11:373–83.
14. Karimi MA, Norooziseyedhosseini H, Khademi R, Ghajary A, Kargar H, Abdollahi SS, et al. Real world results of ibrutinib in patients with relapsed or refractory chronic lymphocytic leukemia: a meta-analysis of clinical studies. BMC Pharmacol Toxicol. (2025) 26:43. doi: 10.1186/s40360-024-00832-9
15. Wang M, Munoz J, Goy A, Locke FL, Jacobson CA, Hill BT, et al. KTE-X19 CAR T-cell therapy in relapsed or refractory mantle-cell lymphoma. N Engl J Med. (2020) 382:1331–42. doi: 10.1056/NEJMoa1914347
16. Phillips TJ, Dickinson M, Morschhauser F, Bachy E, Crump M, Trněný M, et al. Glofitamab monotherapy induces high complete response rates in patients with heavily pretreated relapsed or refractory mantle cell lymphoma. Blood. (2022) 140:178–80. doi: 10.3324/haematol.2023.283802
17. Dreyling M, Doorduijn JK, Gine E, Jerkeman M, Walewski J, Hutchings M, et al. Efficacy and safety of ibrutinib combined with standard first-line treatment or as substitute for autologous stem cell transplantation in younger patients with mantle cell lymphoma: results from the randomized triangle trial by the european MCL network. Blood. (2022) 140:1–3. doi: 10.1182/blood-2022-163018
Keywords: ibrutinib, mantle cell lymphoma, relapse/refractory disease, real-world, Portuguese
Citation: Fernandes C, Costa e Sousa R, Santos P, Almeida C, Roque A, Pinto AL, Monteiro J, Neves A, Ramos MJ, Coutinho R, Mousinho F, Fernandes ML, Badior M, João C, Leocádio S, Tomé AL, Carrolo M, Dias S, da Silva MG and Fernandes JP (2025) Portuguese real-world experience with ibrutinib for the treatment of relapsed/refractory mantle cell lymphoma. Front. Hematol. 4:1702446. doi: 10.3389/frhem.2025.1702446
Received: 09 September 2025; Accepted: 27 October 2025;
Published: 13 November 2025.
Edited by:
Paolo Strati, University of Texas MD Anderson Cancer Center, United StatesReviewed by:
Efthymia Vlachaki, Aristotle University of Thessaloniki, GreeceMohammad Amin Karimi, Shahid Beheshti University of Medical Sciences, Iran
Copyright © 2025 Fernandes, Costa e Sousa, Santos, Almeida, Roque, Pinto, Monteiro, Neves, Ramos, Coutinho, Mousinho, Fernandes, Badior, João, Leocádio, Tomé, Carrolo, Dias, da Silva and Fernandes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catarina Fernandes, Y3NvZmlhLmRtZkBnbWFpbC5jb20=