 Eduardo López-Caneda
Eduardo López-Caneda Natália Almeida-Antunes
Natália Almeida-Antunes- 1Psychological Neuroscience Laboratory (PNL), Research Center in Psychology (CIPsi), School of Psychology, University of Minho, Braga, Portugal
- 2RISE-Health, Center for Translational Health and Medical Biotechnology Research (TBIO), ESS, Polytechnic of Porto, Porto, Portugal
Forgetting as an adaptive human mechanism
“If we remembered everything, we should on most occasions be as ill off as if we remembered nothing” (James, 1890). This phrase by James, like many others found in his masterpiece, The Principles of Psychology, perfectly encapsulates the idea that forgetting, contrary to common perception, is (in most cases) not a negative phenomenon, but serves essential adaptive functions in human life.
Indeed, forgetting may be essential for mental health, as it helps regulate negative emotions by limiting access to unpleasant or embarrassing memories, thereby fostering subjective wellbeing and emotional resilience (Nørby, 2018). It also plays a crucial role in learning, facilitating the transition from detailed episodic memories to more generalized and efficient knowledge. An extreme example of the challenges associated with remembering vast amounts of information is the famous case of Solomon Shereshevsky, a Russian journalist with an extraordinary memory who was unable to forget irrelevant details, often becoming overwhelmed by excessive mental associations, as beautifully documented by Alexander Luria in the second half of the 20th century (Luria, 1968; also see Fawcett and Hulbert, 2020; Price and Davis, 2008). Moreover, forgetting ensures that our cognitive processing remains relevant to the present and future, as it filters out outdated information, enabling us to adapt flexibly to new situations and make better-guided decisions (Kuhl et al., 2007; Richards and Frankland, 2017). Thus, forgetting proves to be not only a necessary process for maintaining a healthy emotional state but also an essential mechanism for efficient cognition and dynamic adaptation to an ever-changing environment.
Cognitive and neural mechanisms underlying memory suppression
The examination of the ability to voluntarily suppress memories has garnered increasing interest over the past two decades, partly due to the groundbreaking work by Anderson and Green (2001). In their seminal study, they developed the Think/No-Think (TNT) task, which was adapted from the classical Go/No-Go paradigm to investigate the suppression of unwanted memories. This task, designed to replicate situations in which individuals encounter reminders of unpleasant memories, requires participants to either recall (Think) or suppress (No-Think) paired word items. The study showed that suppressing memories through executive control processes significantly impairs the recall of suppressed items compared to baseline and actively recalled items (Anderson and Green, 2001). Subsequent research has expanded on this work, demonstrating that suppression-induced forgetting extends beyond neutral word pairs to emotional (Noreen and MacLeod, 2013, 2014) and immoral (Satish et al., 2022, 2024) autobiographical memories, motor actions (Schmidt et al., 2023) and even fearful imaginings about the future (Benoit et al., 2016). Additional studies have also identified the neural mechanisms underlying memory suppression, highlighting the role of prefrontal regions such as the dorsolateral prefrontal (DLPC) cortex and the inferior frontal gyrus (Anderson et al., 2004; Apšvalka et al., 2022; Depue et al., 2007; Paz-Alonso et al., 2013), which exert control over hippocampal and parahippocampal activity, inhibiting/preventing the retrieval of memories or the reinstatement of sensory information related to the learned material (Gagnepain et al., 2014; Mary et al., 2020; Schmitz et al., 2017; Yang et al., 2021). This top-down inhibitory control signal from prefrontal regions not only targets the hippocampus but also modulates other brain regions based on the content of the avoided memories, such as the amygdala for emotional content (Depue et al., 2007; Gagnepain et al., 2017) and the fusiform cortex for visual information (Gagnepain et al., 2014). Altogether, this emerging body of research has supported the view of memory suppression as an integral cognitive process within executive functions, specifically within the domain of inhibitory control (Diamond, 2013), sharing common neuroanatomical structures and neural pathways (Castiglione et al., 2019; Depue, 2012; Wessel and Anderson, 2024).
Memory suppression and addiction: theoretical perspectives and model integration
Unwanted or intrusive thoughts are considered a hallmark of several psychiatric disorders, such as depression and anxiety, posttraumatic stress disorder, and obsessive-compulsive disorder (Clark, 2018; Ehlers et al., 2004; Harrington and Blankenship, 2002; Julien et al., 2007). While limited in number, studies on these clinical conditions suggest a reduced capacity to effectively suppress unwanted thoughts or memories in individuals affected by some of these psychiatric conditions (Catarino et al., 2015; Depue et al., 2010; Diwadkar et al., 2017; Marzi et al., 2014; Storm and White, 2010; Sullivan et al., 2019). However, the role of memory suppression mechanisms in addiction—a clinical condition characterized by maladaptive and persistent substance-related thoughts that often drive compulsive use (Kavanagh et al., 2005)—remains largely underexplored. This gap in research is particularly concerning given the potential implications for understanding and treating addiction, where the inability to suppress maladaptive memories may contribute to the cycle of craving, relapse, and compulsive consumption (Almeida-Antunes et al., 2024b).
This recurring cycle underscores the chronic and progressive nature of substance abuse, which is commonly understood as a condition that evolves from impulsive to compulsive behavior. According to one of the most influential neurobiological models of addiction (Le Moal and Koob, 2007; Koob and Volkow, 2010) this transition unfolds through a spiraling cycle of three stages—binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation (see Figure 1A). The binge/intoxication stage involves the acute effects of substance use, characterized by the activation of the brain's reward systems leading to the experience of euphoria and the formation of habitual patterns of use. This is followed by the withdrawal/negative affect stage, during which the absence of the substance triggers a negative emotional state, including anxiety, dysphoria, and irritability. The persistence of drug-related memories appears to be intimately linked to the preoccupation/anticipation stage, which is marked by intensified craving, heightened sensitivity to substance-related cues, and impaired executive control—factors that significantly contribute to relapse (Koob and Le Moal, 2005; Koob and Volkow, 2016). Indeed, evidence suggests that drug-related memories play a crucial role in sustaining drug use and driving high relapse rates in substance use disorders (SUDs), as they can be triggered by drug-associated cues, eliciting cravings, impulsive behaviors and reduced self-control (Milton and Everitt, 2012; Wise and Koob, 2013; Everitt and Robbins, 2016; Hogarth, 2020; Lüscher et al., 2020). Accordingly, the craving phenomenon and drug-related memories are deeply intertwined, reinforcing each other in a self-perpetuating cycle (Ekhtiari et al., 2016). In this sense, craving is a learned response that connects drug use and its context to pleasurable or relief experiences, driving drug-seeking behavior, and can be elicited by external or internal cues, including memory retrieval (see Figure 1B). Consequently, retrieving substance-related memories can trigger the feeling of craving, which may, in turn, evoke further memories linked to consumption (Berridge and Robinson, 2016; Goldstein and Volkow, 2002). This excitatory cycle is grounded in neural mechanisms, with studies showing that both cue-elicited craving and intoxication increase activity in temporal regions, such as the inferior and middle frontal gyrus, as well as the hippocampus—a key region for retrieving drug-related memories—which may further reinforce substance-seeking behavior by facilitating the recall of substance-related memories (Langleben et al., 2008; Li et al., 2012, 2015; Volkow et al., 2004; Wei et al., 2020; Ekhtiari et al., 2016).
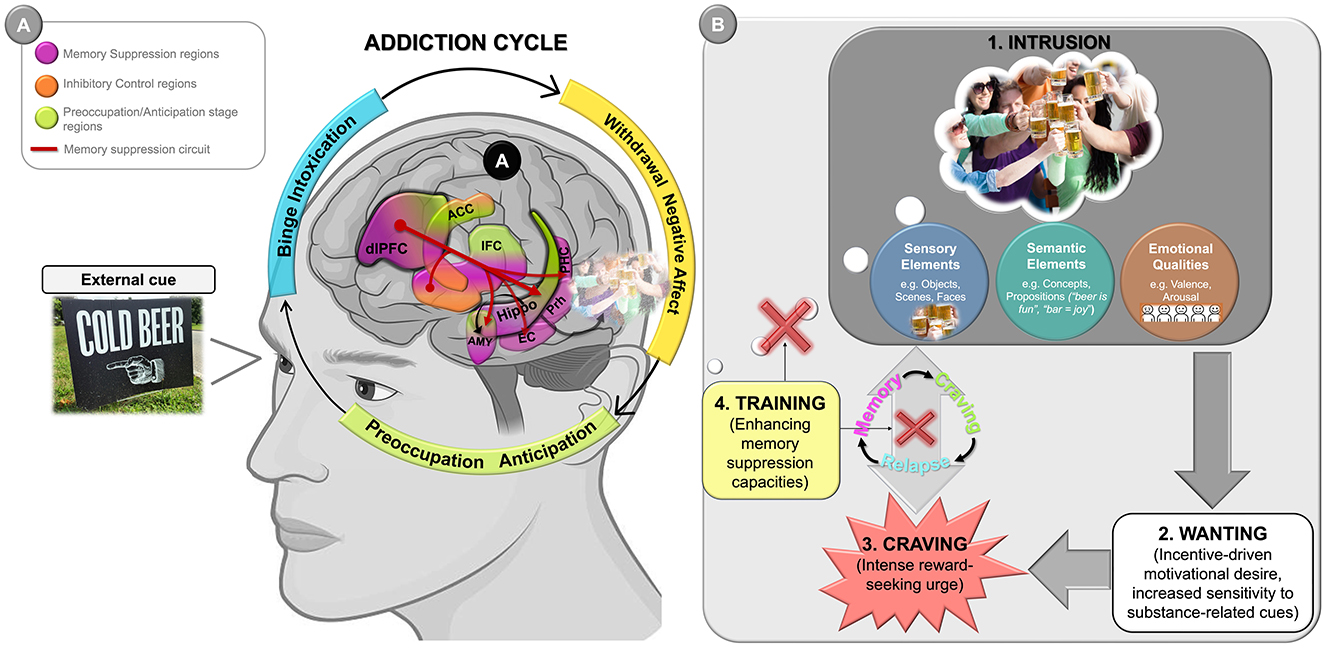
Figure 1. Graphical representation illustrating the role of drug-related memories and memory suppression in the addiction cycle. (A) According to the neurobiological model of addiction (Koob and Volkow, 2010), the transition from initial voluntary drug use to compulsive drug-seeking behavior unfolds through a spiraling cycle of three stages—binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation. In the preoccupation/anticipation stage, drug-related memories become increasingly salient, contributing to intrusive thoughts, strong craving, and heightened reactivity to substance-related cues. These processes are compounded by impaired executive control—particularly dysfunctions in prefrontal regions—undermining not only the ability to inhibit drug-seeking behavior but also the capacity to suppress recurrent, intrusive substance-related thoughts via the memory suppression circuit. (B) The conceptual framework of the preoccupation/anticipation stage closely aligns with the Elaborated Intrusion (EI) Theory of Desire (Kavanagh et al., 2005; May et al., 2015). According to this theory, craving is triggered when an initial intrusive thought—often a brief, automatic cognitive or sensory representation of the substance—emerges into consciousness. These intrusions are typically reactivated by internal (e.g., affective states, bodily sensations) or external cues (e.g., environments, people, or images associated with previous drug use), as illustrated in the photograph on the left, in part A, and are then progressively elaborated into vivid, emotionally charged mental images, often reflecting episodic memories—such as toasting with a beer at a party with friends [as depicted in (B.1)]. Once elaborated, such memory episodes may evoke wanting—that is, an incentive-driven motivational desire (Robinson and Berridge, 1993; Berridge and Robinson, 2016)—which manifests as heightened reactivity to substance-related cues and increased salience of drug-associated goals (B.2). This may, in turn, escalate into craving (B.3), experienced as an intense, reward-seeking urge that captures attention, biases decision-making, and promotes substance-seeking behavior—ultimately reinforcing the memory-craving relapse cycle. Enhancement of memory suppression capacities could eventually reduce the accessibility and impact of drug-related intrusions, thereby weakening craving episodes and lowering the risk of relapse (B.4). Photographs were obtained from the Alcohol, Tobacco, and Other Drug Public Domain Photo Database of the Journal of Studies on Alcohol and Drugs (left image), and from the Galician Beverage Picture Set (López-Caneda and Carbia, 2018; right image). ACC, anterior cingulate cortex; AMY, amygdala; EC, entorhinal cortex; dlPFC, dorsolateral prefrontal cortex; Hippo, hippocampus; PHC, parahippocampal cortex; PFC, prefrontal cortex; Prh, perirhinal cortex.
In light of this, it can be suggested that the inability to suppress such memories might potentially influence the behavior of individuals with SUDs. These difficulties could represent a key factor underlying the mechanisms involved in the preoccupation/anticipation stage, thereby contributing to the persistence of the addiction cycle (Figure 1A). A closer look at this stage reveals the engagement of a broad neurocircuitry, including regions associated with memory suppression, such as the DLPFC, hippocampus, and amygdala (Koob and Volkow, 2010). Moreover, the reduced prefrontal control inherent to this stage supports the notion of increased retrieval of drug-related memories, as diminished executive function may facilitate the automatic reactivation of these memories, reinforcing cravings and leading to further substance-seeking behavior (Noël, 2024). Specifically, hypofunction of the prefrontal cortex (PFC) may impair its control over memory-related regions, such as the hippocampus and amygdala (Depue et al., 2007; Gagnepain et al., 2017; Yang et al., 2021). Consequently, this exacerbates the occurrence of intrusive substance-related thoughts, which in turn trigger craving, as well as drug-seeking and drug-taking behaviors (Figure 1B). These behaviors perpetuate the memory-craving relapse cycle and drive progression to the binge/intoxication phase.
This conceptual framework aligns with and extends two influential motivational models of addiction: the Elaborated Intrusion (EI) Theory of Desire (Kavanagh et al., 2005; May et al., 2015) and the Incentive Salience (IS) Theory (Robinson and Berridge, 1993; Berridge and Robinson, 2016). According to the EI Theory, craving arises when an intrusive cognitive or sensory representation of the substance is elaborated into a vivid and affectively charged episode. Our proposal suggests that enhancing memory suppression may prevent such intrusions from occurring in the first place, thereby reducing the need for elaboration, and disrupting the craving episode before it consolidates. These intrusions often consist of episodic representations linked to prior drug use in emotionally salient contexts—for example, recalling the feeling of euphoria when taking cocaine in a nightclub, the sound of a beer bottle opening during a barbecue with friends, the smell of cannabis in a specific room, or the image of a particular street corner where one used to buy drugs. Such memories are typically reactivated by sensory or contextual cues and can trigger strong craving responses (May et al., 2015). Importantly, the components of intrusive desire described in the EI Theory—such as affect-laden imagery, sensory impressions, and propositional knowledge about the substance—often emerge jointly through the reactivation of episodic memories. Recent evidence indicates that suppressing such memories may reduce not only their explicit recall but also the accessibility of associated conceptual content (Taubenfeld et al., 2019; Wang et al., 2019). This suggests that memory suppression may not only interfere with the initial intrusion but also limit the availability of semantic knowledge that fuels the elaboration process. For example, suppressing the memory of drinking beer with a close friend in a particular bar may not only reduce access to that specific episodic trace, but also weaken the associated propositional beliefs such as “beer is fun” or “bar = joy,” which could otherwise contribute to the motivational amplification of craving.
In parallel, the IS Theory distinguishes between liking (the hedonic value of the substance) and wanting (the automatic motivational pull). Thus, it is possible that memory suppression acts specifically on wanting, by reducing the salience and motivational impact of substance-related cues and memories. Accordingly, several studies have showed that suppressing unwanted memories not only impairs later recall of the suppressed material, but also reduces its affective value, attentional capture, and perceptual vividness (Gagnepain et al., 2014, 2017; Harrington et al., 2021; Hertel et al., 2018; Legrand et al., 2020). In this way, the ability to suppress episodic drug-related content—along with the beliefs and semantic associations it evokes—may contribute to modulating the incentive salience of drug-associated stimuli, thereby acting as a cognitive mechanism to attenuate maladaptive motivational responses in addiction.
Emerging evidence for impaired memory suppression in alcohol misuse
Although evidence has consistently showed that individuals with drug addiction exhibit structural and functional alterations in brain regions involved in executive control—and, by extension, also implicated in memory suppression—(Goldstein and Volkow, 2011; Zilverstand et al., 2018), research on the ability to inhibit unwanted memories in SUDs remains scarce. To the best of our knowledge, only three studies have specifically examined this ability in relation to alcohol consumption patterns. Notably, all three reported impairments in both the neural correlates and/or the behavioral performance underlying the suppression of unwanted memories, including those related to alcohol (Almeida-Antunes et al., 2024a; Nemeth et al., 2014; Simeonov et al., 2022). Specifically, Nemeth et al. (2014) observed that individuals with alcohol dependence exhibited an impaired ability to suppress retrieval compared to healthy controls. Building on these findings, Simeonov et al. (2022) found that hazardous drinkers also had difficulties in suppressing retrieval, but only for alcohol-related associate pairs, suggesting a selective impairment in suppressing alcohol-related memories in this population. Extending this line of research, Almeida-Antunes et al. (2024a) found that young binge drinkers also exhibited difficulties in memory suppression mechanisms. However, they did not show impaired suppression of alcohol-related memories. Instead, they exhibited increased functional connectivity between brain regions involved in memory suppression when attempting to suppress these memories, likely reflecting heightened attention toward intrusive alcohol-related thoughts and compensatory mechanisms for potential inhibitory control deficits. Similar to alcohol-dependent individuals, binge drinkers also showed impaired suppression of non-alcohol-related memories, which was accompanied by reduced connectivity between inhibitory control and memory networks, suggesting a broader deficit in inhibitory mechanisms. Taken together, these studies indicate that individuals with problematic alcohol use patterns exhibit impairments in memory suppression abilities, particularly in relation to alcohol-related memories. However, further research is needed to better understand the mechanisms underlying these suppression deficits in population with dependent-like behaviors.
Memory suppression as a novel approach in substance use disorders treatment
The relationship between persistent drug-related memories and the emergence of craving—as described both in the preoccupation/anticipation stage of addiction and in the EI theory of desire—raises a compelling question: could targeting these memories and enhancing the ability to inhibit them offer a novel approach to breaking this cycle? Persistent, maladaptive drug-related memories pose a major challenge to maintaining abstinence, and interventions aimed at addressing these memories have been proposed as promising strategies for addiction treatment (Lee et al., 2005; Noël, 2023). However, to date, no study has investigated the potential impact of strengthening the capacity to suppress drug-associated memories in individuals with SUDs (Almeida-Antunes et al., 2022).
Interestingly, recent evidence indicates that training individuals to suppress negative thoughts improves mental health outcomes in conditions like anxiety and PTSD by reducing repetitive, intrusive thinking (Mamat and Anderson, 2023). Given that recurrent drug-related thoughts seem to be a hallmark in addiction, enhancing memory suppression abilities may similarly reduce the strength and persistence of these maladaptive memories. Additionally, training focused on attentional and executive functions, particularly when tailored to substance-related cues, has been shown to improve cognitive functions and clinical symptoms in SUDs (Bartsch et al., 2016; Nardo et al., 2022; Stein et al., 2023; Verdejo-García, 2016; Verdejo-García et al., 2024; Wiers, 2018), suggesting that drug-specific memory suppression training could significantly impact outcomes, including reducing craving and relapse (Figure 1B).
One commonly used, yet conceptually distinct, method for managing substance-related thoughts is known as thought suppression (Wenzlaff and Wegner, 2000). While this technique typically involves instructing individuals to avoid thinking about certain topics—often through vague or general directives—the memory suppression approach differs both in the type of mental content being targeted and in the nature of the suppression strategy. For example, interventions based on thought suppression in addiction contexts include instructions such as: “Try not to think about smoking. If you do happen to have thoughts about smoking this week, please, try to suppress them” or “For the next 5 minutes, please do everything you can to not think about alcohol (…) However, if you should have such a thought, please make a checkmark on this sheet of paper” (Erskine et al., 2010; Klein, 2007). In contrast, memory suppression—as conceived within the TNT framework—involves a goal-directed, item-specific effort to inhibit memory retrieval in response to specific cues. For instance, when presented with the word cue “foam,” participants are instructed to prevent the associated target image—such as people clinking beer glasses—from coming to mind, using a trained direct suppression strategy (Simeonov et al., 2022). Crucially, participants typically engage in repeated attempts to block retrieval, allowing them to improve control over intrusive content over time (Nardo and Anderson, 2024). This progressive improvement is reflected in the decreasing frequency of intrusions across suppression attempts: they occur frequently at first (around 60%), but tend to diminish with practice (~30%), reflecting the so-called intrusion-control effect (Levy and Anderson, 2012). In contrast, thought suppression paradigms usually rely on general avoidance instructions without strategic guidance or practice. These methodological differences are important, as they may account for the divergent outcomes typically associated with each approach. Whereas thought suppression has frequently been linked to ironic rebound effects and increased salience of the suppressed material (Wegner and Erber, 1992; Moss et al., 2015), recent work has questioned the generality of these findings, suggesting that such effects may stem from ambiguities in the instructions and from the interference caused by multitasking or cognitive load during suppression attempts (Mamat et al., 2024). By comparison, memory suppression tasks offer clear, reproducible instructions and engage executive mechanisms to disrupt retrieval processes at the mnemonic level, leading to suppression-induced forgetting (Anderson and Hulbert, 2021) and attenuation of the emotional or motivational salience of the suppressed content (Hu et al., 2017). As such, memory suppression constitutes a more structured and empirically supported form of inhibitory control (Wessel and Anderson, 2024), with promising implications for disrupting the memory-craving-relapse cycle in addiction.
Additionally, while models such as desire thinking (Caselli and Spada, 2016) emphasize the role of elaborative and metacognitive processes in sustaining craving, the memory suppression approach for addictive behaviors differs in two fundamental respects: it targets an earlier stage of the craving process, namely the episodic memory reactivations that often precede elaboration, and it involves the active suppression of the memory or mental image itself, rather than the modulation of cognitive elaboration or metacognitive beliefs about thinking.
Although promising, memory suppression training as a treatment for SUDs is still in its early stages. To evaluate its potential clinical impact, further research is needed to assess the type and degree of impairment (if any) in memory suppression mechanisms among individuals with SUDs, and to determine whether enhancing this ability can effectively reduce craving and relapse risk. At present, there is encouraging evidence that interventions targeting maladaptive or unwanted memories could offer an innovative therapeutic pathway (Almeida-Antunes et al., 2024b; Joormann et al., 2009; Mary et al., 2020; Nishiyama and Saito, 2022; Noël, 2023; Mamat and Anderson, 2023), although the generalization of these lab-based interventions and the durability of their effects over time remain to be systematically assessed (Fawcett et al., 2024). These approaches have the potential to complement existing strategies by addressing a crucial yet underexplored dimension of the addiction cycle, opening new avenues for more comprehensive and effective treatments.
Author contributions
EL-C: Conceptualization, Funding acquisition, Writing – original draft, Writing – review & editing. NA-A: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was conducted at the Psychology Research Center (PSI/01662), School of Psychology, University of Minho, supported by the Foundation for Science and Technology (FCT) through the Portuguese State Budget (Ref.: UIDB/PSI/01662/2020). This study was also supported by the projects PTDC/PSI-ESP/1243/2021 and 2023.14679.PEX.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. Generative AI tools were used solely to improve the clarity and grammar of the English text. The author(s) reviewed and edited all content to ensure accuracy and originality.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Almeida-Antunes, N., Antón-Toro, L., Crego, A., Rodrigues, R., Sampaio, A., López-Caneda, E., et al. (2024a). Trying to forget alcohol: brain mechanisms underlying memory suppression in young binge drinkers. Prog. Neuropsychopharmacol. Biol. Psychiatry 134:111053. doi: 10.1016/j.pnpbp.2024.111053
Almeida-Antunes, N., Sampaio, A., Crego, A., and López-Caneda, E. (2024b). Tackling addictive behaviors through memory suppression: a scoping review and perspective. Alcohol Clin. Exp. Res. 48, 1421–1442. doi: 10.1111/acer.15381
Almeida-Antunes, N., Vasconcelos, M., Crego, A., Rodrigues, R., Sampaio, A., López-Caneda, E., et al. (2022). Forgetting alcohol: a double-blind, randomized controlled trial investigating memory inhibition training in young binge drinkers. Front. Neurosci. 16:914213. doi: 10.3389/fnins.2022.914213
Anderson, M. C., and Green, C. (2001). Suppressing unwanted memories by executive control. Nature 410, 366–369. doi: 10.1038/35066572
Anderson, M. C., and Hulbert, J. C. (2021). Active forgetting: adaptation of memory by prefrontal control. Annu. Rev. Psychol. 72, 1–36. doi: 10.1146/annurev-psych-072720-094140
Anderson, M. C., Ochsner, K. N., Kuhl, B., Cooper, J., Robertson, E., Gabrieli, S. W., et al. (2004). Neural systems underlying the suppression of unwanted memories. Science 303, 232–235. doi: 10.1126/science.1089504
Apšvalka, D., Ferreira, C. S., Schmitz, T. W., Rowe, J. B., and Anderson, M. C. (2022). Dynamic targeting enables domain-general inhibitory control over action and thought by the prefrontal cortex. Nat. Commun. 13:274. doi: 10.1038/s41467-021-27926-w
Bartsch, A., Kothe, E., Allom, V., Mullan, B., and Houben, K. (2016). The effect of non-specific response inhibition training on alcohol consumption: an intervention. J. Addict. Res. Ther. 7, 260–260. doi: 10.4172/2155-6105.1000260
Benoit, R. G., Davies, D. J., and Anderson, M. C. (2016). Reducing future fears by suppressing the brain mechanisms underlying episodic simulation. Proc. Nat. Acad. Sci. 113, E8492–E8501. doi: 10.1073/pnas.1606604114
Berridge, K. C., and Robinson, T. E. (2016). Liking, wanting, and the incentive-sensitization theory of addiction. Am. Psychol. 71, 670–679. doi: 10.1037/amp0000059
Caselli, G., and Spada, M. M. (2016). Desire thinking: a new target for treatment of addictive behaviors? Int. J. Cogn. Ther. 9, 344–355. doi: 10.1521/ijct_2016_09_15
Castiglione, A., Wagner, J., Anderson, M., and Aron, A. R. (2019). Preventing a thought from coming to mind elicits increased right frontal beta just as stopping action does. Cereb. Cortex 29, 2160–2172. doi: 10.1093/cercor/bhz017
Catarino, A., Küpper, C. S., Werner-Seidler, A., Dalgleish, T., and Anderson, M. C. (2015). Failing to forget: inhibitory-control deficits compromise memory suppression in posttraumatic stress disorder. Psychol. Sci. 26, 604–616. doi: 10.1177/0956797615569889
Clark, D. A. (2018). The Anxious Thoughts Workbook: Skills to Overcome the Unwanted Intrusive Thoughts that Drive Anxiety, Obsessions, and Depression. Oakland, CA: New Harbinger Publications.
Depue, B. E. (2012). A neuroanatomical model of prefrontal inhibitory modulation of memory retrieval. Neurosci. Biobehav. Rev. 36, 1382–1399. doi: 10.1016/j.neubiorev.2012.02.012
Depue, B. E., Burgess, G. C., Willcutt, E. G., Ruzic, L., and Banich, M. (2010). Inhibitory control of memory retrieval and motor processing associated with the right lateral prefrontal cortex: evidence from deficits in individuals with ADHD. Neuropsychologia 48, 3909–3917. doi: 10.1016/j.neuropsychologia.2010.09.013
Depue, B. E., Curran, T., and Banich, M. T. (2007). Prefrontal regions orchestrate suppression of emotional memories via a two-phase process. Science 317, 215–219. doi: 10.1126/science.1139560
Diamond, A. (2013). Executive functions. Annu. Rev. Psychol. 64, 135–168. doi: 10.1146/annurev-psych-113011-143750
Diwadkar, V. A., Re, M., Cecchetto, F., Garzitto, M., Piccin, S., Bonivento, C., et al. (2017). Attempts at memory control induce dysfunctional brain activation profiles in generalized anxiety disorder: an exploratory fMRI study. Psychiatry Res. Neuroimaging 266, 42–52. doi: 10.1016/j.pscychresns.2017.05.010
Ehlers, A., Hackmann, A., and Michael, T. (2004). Intrusive re-experiencing in post-traumatic stress disorder: phenomenology, theory, and therapy. Memory 12, 403–415. doi: 10.1080/09658210444000025
Ekhtiari, H., Nasseri, P., Yavari, F., Mokri, A., and Monterosso, J. (2016). Neuroscience of drug craving for addiction medicine: from circuits to therapies. Prog. Brain Res. 223, 115–141. doi: 10.1016/bs.pbr.2015.10.002
Erskine, J. A., Georgiou, G. J., and Kvavilashvili, L. (2010). I suppress, therefore I smoke: effects of thought suppression on smoking behavior. Psychol. Sci. 21, 1225–1230. doi: 10.1177/0956797610378687
Everitt, B. J., and Robbins, T. W. (2016). Drug addiction: updating actions to habits to compulsions ten years on. Annu. Rev. Psychol. 67, 23–50. doi: 10.1146/annurev-psych-122414-033457
Fawcett, J. M., and Hulbert, J. C. (2020). The many faces of forgetting: toward a constructive view of forgetting in everyday life. J. Appl. Res. Mem. Cogn. 9, 1–18. doi: 10.1016/j.jarmac.2019.11.002
Fawcett, J. M., Taylor, T. L., Megla, E., and Maxcey, A. M. (2024). Active intentional and unintentional forgetting in the laboratory and everyday life. Nat. Rev. Psychol. 3, 652–664. doi: 10.1038/s44159-024-00352-7
Gagnepain, P., Henson, R. N., and Anderson, M. C. (2014). Suppressing unwanted memories reduces their unconscious influence via targeted cortical inhibition. Proc. Nat. Acad. Sci. 111, E1310–E1319. doi: 10.1073/pnas.1311468111
Gagnepain, P., Hulbert, J., and Anderson, M. C. (2017). Parallel regulation of memory and emotion supports the suppression of intrusive memories. J. Neurosci. 37, 6423–6441. doi: 10.1523/JNEUROSCI.2732-16.2017
Goldstein, R. Z., and Volkow, N. D. (2002). Drug addiction and its underlying neurobiological basis: neuroimaging evidence for the involvement of the frontal cortex. Am. J. Psychiatry 159, 1642–1652. doi: 10.1176/appi.ajp.159.10.1642
Goldstein, R. Z., and Volkow, N. D. (2011). Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat. Rev. Neurosci. 12, 652–669. doi: 10.1038/nrn3119
Harrington, J. A., and Blankenship, V. (2002). Ruminative thoughts and their relation to depression and anxiety 1. J. Appl. Soc. Psychol. 32, 465–485. doi: 10.1111/j.1559-1816.2002.tb00225.x
Harrington, M. O., Ashton, J. E., Sankarasubramanian, S., Anderson, M. C., and Cairney, S. A. (2021). Losing control: sleep deprivation impairs the suppression of unwanted thoughts. Clin. Psychol. Sci. 9, 97–113. doi: 10.1177/2167702620951511
Hertel, P. T., Maydon, A., Ogilvie, A., and Mor, N. (2018). Ruminators (unlike others) fail to show suppression-induced forgetting on indirect measures of memory. Clin. Psychol. Sci. 6, 872–881. doi: 10.1177/2167702618785339
Hogarth, L. (2020). Addiction is driven by excessive goal-directed drug choice under negative affect: translational critique of habit and compulsion theory. Neuropsychopharmacology 45, 720–735. doi: 10.1038/s41386-020-0600-8
Hu, X., Bergström, Z. M., Gagnepain, P., and Anderson, M. C. (2017). Suppressing unwanted memories reduces their unintended influences. Curr. Dir. Psychol. Sci. 26, 197–206. doi: 10.1177/0963721417689881
Joormann, J., Hertel, P. T., LeMoult, J., and Gotlib, I. H. (2009). Training forgetting of negative material in depression. J. Abnorm. Psychol. 118, 34–43. doi: 10.1037/a0013794
Julien, D., O'Connor, K. P., and Aardema, F. (2007). Intrusive thoughts, obsessions, and appraisals in obsessive–compulsive disorder: a critical review. Clin. Psychol. Rev. 27, 366–383. doi: 10.1016/j.cpr.2006.12.004
Kavanagh, D. J., Andrade, J., and May, J. (2005). Imaginary relish and exquisite torture: the elaborated intrusion theory of desire. Psychol. Rev. 112, 446–467. doi: 10.1037/0033-295X.112.2.446
Klein, A. A. (2007). Suppression-induced hyperaccessibility of thoughts in abstinent alcoholics: a preliminary investigation. Behav. Res. Ther. 45, 169–177. doi: 10.1016/j.brat.2005.12.012
Koob, G. F., and Le Moal, M. (2005). Plasticity of reward neurocircuitry and the 'dark side' of drug addiction. Nat. Neurosci. 8, 1442–1444. doi: 10.1038/nn1105-1442
Koob, G. F., and Volkow, N. D. (2010). Neurocircuitry of addiction. Neuropsychopharmacology 35, 217–238. doi: 10.1038/npp.2009.110
Koob, G. F., and Volkow, N. D. (2016). Neurobiology of addiction: a neurocircuitry analysis. Lancet Psychiatry 3, 760–773. doi: 10.1016/S2215-0366(16)00104-8
Kuhl, B. A., Dudukovic, N. M., Kahn, I., and Wagner, A. D. (2007). Decreased demands on cognitive control reveal the neural processing benefits of forgetting. Nat. Neurosci. 10, 908–914. doi: 10.1038/nn1918
Langleben, D. D., Ruparel, K., Elman, I., Busch-Winokur, S., Pratiwadi, R., Loughead, J., et al. (2008). Acute effect of methadone maintenance dose on brain fMRI response to heroin-related cues. Am. J. Psychiatry 165, 390–394. doi: 10.1176/appi.ajp.2007.07010070
Le Moal, M., and Koob, G. F. (2007). Drug addiction: pathways to the disease and pathophysiological perspectives. Eur. Neuropsychopharmacol. 17, 377–393. doi: 10.1016/j.euroneuro.2006.10.006
Lee J. L. C. Di Ciano P. Thomas K. L. Everitt B. J. (2005) Disrupting reconsolidation of drug memories reduces cocaine-seeking behavior. Neuron 47, 795–801. 10.1016/j.neuron.2005.08.007
Legrand, N., Etard, O., Vandevelde, A., Pierre, M., Viader, F., Clochon, P., et al. (2020). Long-term modulation of cardiac activity induced by inhibitory control over emotional memories. Sci. Rep. 10:15008. doi: 10.1038/s41598-020-71858-2
Levy, B. J., and Anderson, M. C. (2012). Purging of memories from conscious awareness tracked in the human brain. J. Neurosci. 32, 16785–16794. doi: 10.1523/JNEUROSCI.2640-12.2012
Li, Q., Li, W., Wang, H., Wang, Y., Zhang, Y., Zhu, J., et al. (2015). Predicting subsequent relapse by drug-related cue-induced brain activation in heroin addiction: an event-related functional magnetic resonance imaging study. Addict. Biol. 20, 968–978. doi: 10.1111/adb.12182
Li, Q., Wang, Y., Zhang, Y., Li, W., Yang, W., Zhu, J., et al. (2012). Craving correlates with mesolimbic responses to heroin-related cues in short-term abstinence from heroin: an event-related fMRI study. Brain Res. 1469, 63–72. doi: 10.1016/j.brainres.2012.06.024
López-Caneda, E., and Carbia, C. (2018). The Galician Beverage Picture Set (GBPS): a standardized database of alcohol and non-alcohol images. Drug Alcohol Depend. 184, 42–47. doi: 10.1016/j.drugalcdep.2017.11.022
Lüscher, C., Robbins, T. W., and Everitt, B. J. (2020). The transition to compulsion in addiction. Nat. Rev. Neurosci. 21, 247–263. doi: 10.1038/s41583-020-0289-z
Mamat, Z., and Anderson, M. C. (2023). Improving mental health by training the suppression of unwanted thoughts. Sci. Adv. 9:eadh5292. doi: 10.1126/sciadv.adh5292
Mamat, Z., Levy, D. A., and Bayley, P. J. (2024). Reconsidering thought suppression and ironic processing: implications for clinical treatment of traumatic memories. Front. Psychol. 15:1496134. doi: 10.3389/fpsyg.2024.1496134
Mary, A., Dayan, J., Leone, G., Postel, C., Fraisse, F., Malle, C., et al. (2020). Resilience after trauma: the role of memory suppression. Science 367:eaay8477. doi: 10.1126/science.aay8477
Marzi, T., Regina, A., and Righi, S. (2014). Emotions shape memory suppression in trait anxiety. Front. Psychol. 4:1001. doi: 10.3389/fpsyg.2013.01001
May, J., Kavanagh, D. J., and Andrade, J. (2015). The elaborated intrusion theory of desire: a 10-year retrospective and implications for addiction treatments. Addict. Behav. 44, 29–34. doi: 10.1016/j.addbeh.2014.09.016
Milton, A. L., and Everitt, B. J. (2012). The persistence of maladaptive memory: addiction, drug memories and anti-relapse treatments. Neurosci. Biobehav. Rev. 36, 1119–1139. doi: 10.1016/j.neubiorev.2012.01.002
Moss, A. C., Erskine, J. A., Albery, I. P., Allen, J. R., and Georgiou, G. J. (2015). To suppress, or not to suppress? That is repression: controlling intrusive thoughts in addictive behaviour. Addict. Behav. 44, 65–70. doi: 10.1016/j.addbeh.2015.01.029
Nardo, D., and Anderson, M. C. (2024). Everything you ever wanted to know about the Think/No-Think task, but forgot to ask. Behav. Res. Methods 56, 3831–3860. doi: 10.3758/s13428-024-02349-9
Nardo, T., Batchelor, J., Berry, J., Francis, H., Jafar, D., Borchard, T., et al. (2022). Cognitive remediation as an adjunct treatment for substance use disorders: a systematic review. Neuropsychol. Rev. 32, 161–191. doi: 10.1007/s11065-021-09506-3
Nemeth, V. L., Kurgyis, E., Csifcsak, G., Maraz, A., Almasi, D. A., Drotos, G., et al. (2014). The impact of intermediate-term alcohol abstinence on memory retrieval and suppression. Front. Psychol. 5:1396. doi: 10.3389/fpsyg.2014.01396
Nishiyama, S., and Saito, S. (2022). Retrieval stopping can reduce distress from aversive memories. Cogn. Emot. 36, 957–974. doi: 10.1080/02699931.2022.2071845
Noël, X. (2023). A critical perspective on updating drug memories through the integration of memory editing and brain stimulation. Front. Psychiatry 14:1161879. doi: 10.3389/fpsyt.2023.1161879
Noël, X. (2024). Leveraging memory suppression from a goal-directed perspective to regain control over alcohol consumption. Alcohol. Clin. Exp. Res. 48, 2242–2245. doi: 10.1111/acer.15462
Nørby, S. (2018). Forgetting and emotion regulation in mental health, anxiety and depression. Memory 26, 342–363. doi: 10.1080/09658211.2017.1346130
Noreen, S., and MacLeod, M. D. (2013). It's all in the detail: intentional forgetting of autobiographical memories using the autobiographical think/no-think task. J. Exp. Psychol. Learn. Mem. Cogn. 39, 375–393. doi: 10.1037/a0028888
Noreen, S., and MacLeod, M. D. (2014). To think or not to think, that is the question: individual differences in suppression and rebound effects in autobiographical memory. Acta Psychol. 145, 84–97. doi: 10.1016/j.actpsy.2013.10.011
Paz-Alonso, P. M., Bunge, S. A., Anderson, M. C., and Ghetti, S. (2013). Strength of coupling within a mnemonic control network differentiates those who can and cannot suppress memory retrieval. J. Neurosci. 33, 5017–5026. doi: 10.1523/JNEUROSCI.3459-12.2013
Price, J., and Davis, B. (2008). The woman who can't forget: The extraordinary story of living with the most remarkable memory known to science — A memoir. New York, NY: Free Press.
Richards, B. A., and Frankland, P. W. (2017). The persistence and transience of memory. Neuron 94, 1071–1084. doi: 10.1016/j.neuron.2017.04.037
Robinson, T. E., and Berridge, K. C. (1993). The neural basis of drug craving: an incentive-sensitization theory of addiction. Brain Res. Rev. 18, 247–291. doi: 10.1016/0165-0173(93)90013-P
Satish, A., Hellerstedt, R., Anderson, M. C., and Bergström, Z. M. (2022). EEG evidence that morally relevant autobiographical memories can be suppressed. Cogn. Affect. Behav. Neurosci. 22, 1290–1310. doi: 10.3758/s13415-022-01029-5
Satish, A., Hellerstedt, R., Anderson, M. C., and Bergström, Z. M. (2024). Memory control immediately improves unpleasant emotions associated with autobiographical memories of past immoral actions. Cogn. Emot. 38, 1032–1047. doi: 10.1080/02699931.2024.2342390
Schmidt, M., Anderson, M. C., and Tempel, T. (2023). Suppression-induced forgetting of motor sequences. Cognition 230:105292. doi: 10.1016/j.cognition.2022.105292
Schmitz, T. W., Correia, M. M., Ferreira, C. S., Prescot, A. P., and Anderson, M. C. (2017). Hippocampal GABA enables inhibitory control over unwanted thoughts. Nat. Commun. 8:1311. doi: 10.1038/s41467-017-00956-z
Simeonov, L., Peniket, M., and Das, R. (2022). No-think, no drink? Assessing the ability of reconsolidation interference by intentional forgetting to suppress alcohol memories in hazardous drinkers. Behav. Res. Ther. 152:104055. doi: 10.1016/j.brat.2022.104055
Stein, M., Soravia, L. M., Tschuemperlin, R. M., Batschelet, H. M., Jaeger, J., Roesner, S., et al. (2023). Alcohol-specific inhibition training in patients with alcohol use disorder: a multi-centre, double-blind randomized clinical trial examining drinking outcome and working mechanisms. Addiction 118, 646–657. doi: 10.1111/add.16104
Storm, B. C., and White, H. A. (2010). ADHD and retrieval-induced forgetting: evidence for a deficit in the inhibitory control of memory. Memory 18, 265–271. doi: 10.1080/09658210903547884
Sullivan, D. R., Marx, B., Chen, M. S., Depue, B. E., Hayes, S. M., Hayes, J. P., et al. (2019). Behavioral and neural correlates of memory suppression in PTSD. J. Psychiatr. Res. 112, 30–37. doi: 10.1016/j.jpsychires.2019.02.015
Taubenfeld, A., Anderson, M. C., and Levy, D. A. (2019). The impact of retrieval suppression on conceptual implicit memory. Memory 27, 686–697. doi: 10.1080/09658211.2018.1554079
Verdejo-García, A. (2016). Cognitive training for substance use disorders: neuroscientific mechanisms. Neurosci. Biobehav. Rev. 68, 270–281. doi: 10.1016/j.neubiorev.2016.05.018
Verdejo-García, A., Berry, J., Caracuel, A., Copersino, M. L., Field, M., Garland, E. L., et al. (2024). Clinical translation of expert-endorsed cognitive rehabilitation interventions for substance use disorders. World Psychiatry 23, 299–301. doi: 10.1002/wps.21126
Volkow, N. D., Fowler, J. S., and Wang, G. J. (2004). The addicted human brain viewed in the light of imaging studies: brain circuits and treatment strategies. Neuropharmacology 47, 3–13. doi: 10.1016/j.neuropharm.2004.07.019
Wang, Y., Luppi, A., Fawcett, J., and Anderson, M. C. (2019). Reconsidering unconscious persistence: suppressing unwanted memories reduces their indirect expression in later thoughts. Cognition 187, 78–94. doi: 10.1016/j.cognition.2019.02.016
Wegner, D. M., and Erber, R. (1992). The hyperaccessibility of suppressed thoughts. J. Pers. Soc. Psychol. 63, 903–912. doi: 10.1037/0022-3514.63.6.903
Wei, X., Li, W., Chen, J., Li, Y., Zhu, J., Shi, H., et al. (2020). Assessing drug cue-induced brain response in heroin dependents treated by methadone maintenance and protracted abstinence measures. Brain Imaging Behav. 14, 1221–1229. doi: 10.1007/s11682-019-00051-5
Wenzlaff, R. M., and Wegner, D. M. (2000). Thought suppression. Annu. Rev. Psychol. 51, 59–91. doi: 10.1146/annurev.psych.51.1.59
Wessel, J. R., and Anderson, M. C. (2024). Neural mechanisms of domain-general inhibitory control. Trends Cogn. Sci. 28, 124–143. doi: 10.1016/j.tics.2023.09.008
Wiers, R. W. (2018). Cognitive training in addiction: does it have clinical potential? Biol. Psychiatry Cogn. Neurosci. Neuroimaging 3, 101–102. doi: 10.1016/j.bpsc.2017.12.008
Wise, R. A., and Koob, G. F. (2013). The development and maintenance of drug addiction. Neuropsychopharmacology 39, 254–262. doi: 10.1038/npp.2013.261
Yang, W., Zhuang, K., Liu, P., Guo, Y., Chen, Q., Wei, D., et al. (2021). Memory suppression ability can be robustly predicted by the internetwork communication of frontoparietal control network. Cereb. Cortex 31, 3451–3461. doi: 10.1093/cercor/bhab024
Keywords: inhibitory control, memory suppression, addictive behaviors, substance use disorders (SUDs), cognitive training
Citation: López-Caneda E and Almeida-Antunes N (2025) Inhibitory control in addictive behaviors: is there room for memory suppression? Front. Hum. Neurosci. 19:1545176. doi: 10.3389/fnhum.2025.1545176
Received: 14 December 2024; Accepted: 22 May 2025;
Published: 05 June 2025.
Edited by:
Chella Kamarajan, Downstate Health Sciences University, United StatesReviewed by:
Surabhi Ramawat, Sapienza University of Rome, ItalyJohn Monterosso, University of Southern California, United States
Zulkayda Mamat, Stanford University, United States
Copyright © 2025 López-Caneda and Almeida-Antunes. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Eduardo López-Caneda, ZWR1YXJkby5sb3BlekBwc2kudW1pbmhvLnB0