 Barbara Naeme de Lima Cordeiro1
Barbara Naeme de Lima Cordeiro1 Jader Vinicius Da Silva Rocha1Elizangela Kuster1Aurore Thibauth2Lucas Rodrigues Nascimento1Chad Swank3
Jader Vinicius Da Silva Rocha1Elizangela Kuster1Aurore Thibauth2Lucas Rodrigues Nascimento1Chad Swank3 Guilherme Peixoto Tinoco Arêas4
Guilherme Peixoto Tinoco Arêas4 Walter Gomes da Silva Filho1Carolina Fiorin Anhoque1Wellingson Silva Paiva5Jéssica Costa Buarque6
Walter Gomes da Silva Filho1Carolina Fiorin Anhoque1Wellingson Silva Paiva5Jéssica Costa Buarque6 Fernando Zanela Arêas1,3*
Fernando Zanela Arêas1,3*- 1Neurorehabilitation and Neuromodulation Laboratory, Federal University of Espirito Santo, Vitória, Brazil
- 2Coma Science Group, GIGA Consciousness, University of Liège, Liège, Belgium
- 3Baylor Scott & White Research Institute (BSWRI), Dallas, TX, United States
- 4Physiological Sciences Laboratory, Federal University of Amazonas, Manaus, Brazil
- 5Division of Neurosurgery, Hospital das Clinicas, University of São Paulo, São Paulo, Brazil
- 6Neurorehabilitation and Neuromodulation Laboratory, Federal University of Espirito Santo, Vitória, Brazil
The aim of this study is to report clinical cases of patients with severe traumatic brain injury (TBI) who underwent transcranial direct current stimulation (tDCS) in the subacute phase. We hypothesize that tDCS will improve the functional and cognitive recovery of patients. 5 men, admitted with severe TBI, and Glasgow Coma Scale (GCS) score ≤ 8 on admission or at some point during hospitalization, were in the subacute phase of the trauma (between 2 and 16 weeks). Participants received 5 sessions of tDCS every day. The results were measured at the beginning and at the end of the 5 sessions. The application of tDCS with an active electrode (anode) was applied to the region of the left dorsolateral prefrontal cortex (LPFC - F3) and the cathode was positioned over the contralateral supraorbital area. Clinical outcomes were measured through cognitive assessment, Mini Mental State Examination (MMSE), mental health and depression, Hospital Anxiety and Depression Scale (HADS-A), pain, visual analogue scale (VAS), Functional Independence Measure (FIM), Rancho Los Amigos Scale (RLAS) and Glasgow Outcome Scale - Extended (GOS-E), were applied to classify the patient’s condition. For characteristics of participants and findings results, descriptive statistics were presented as mean ± Standard Deviation (SD). The results after the tDCS intervention show substantial improvement in the assessed. The research demonstrates the potential benefits of using tDCS in patients with TBI, but also provides a practical basis for applying these techniques in clinical settings.
Introduction
Traumatic brain injury (TBI) is a global health problem and has been one of the main causes of morbidity, disability and mortality, especially in adults young people. Worldwide, more than 50 million individuals suffer a TBI each year (Bruns and Hauser, 2003). In Brazil, it is an important public health problem due to the high rate of disability in the young population, causing these individuals to interrupt their professional activities early (Areas et al., 2019). Damage to neuronal tissues associated with TBI falls into two categories: (I) primary injury, which is caused directly by mechanical forces during the initial insult; and (II) secondary injury, which refers to the cascade of cellular and molecular processes initiated by the primary injury. The immediate impact of different mechanical traumas to the brain can cause two types of primary lesions: focal and diffuse brain lesions. Axonal injury is the most common consequence of diffuse trauma, accounting for approximately 70% of cases TBI cases. TBI is complex and dynamic and results in changes in the function and structure of practically all elements of the brain. A proportion of survivors of severe TBI, after prolonged hospital care, require special attention and may experience disorders long-term physical, cognitive and psychological. Among the disabilities, cognitive dysfunction is a consequence of brain injury that affects a large proportion of those who survive after moderate to severe injury (Newcombe et al., 2011). A scale widely used during the initial examination to estimate the severity of TBI is the Glasgow Coma Scale, which consists of a quick and reproducible scoring system. A score of 13 to 15 indicates mild TBI; 9 to 12 moderate TBI and 8 or less severe TBI.
Non-invasive brain stimulation (NIBS) techniques have shown potential as therapeutic options for neuropsychiatric conditions, including TBI sequelae. A widely used technique is transcranial direct current stimulation (tDCS), which has the potential to modify and modulate the polarity of the neuron’s membrane current. tDCS has been tested in some diseases including TBI. Its principle is based on the application of a low intensity electrical current that flows from the anode to the cathode to modify the resting potential of the membrane and modulate the level of activity of spontaneous excitatory neurons through two electrodes positioned on the individual’s scalp (Fregni and Pascual-Leone, 2007).
Research has demonstrated positive results from the application of tDCS after stroke, such as improved motor and cognitive function, when tDCS was combined with other therapies. Other studies have mainly explored the use of non-invasive brain stimulation on psychiatric disorders and in healthy individuals (for performance evaluation). However, previous studies have failed to report conclusive evidence to support or refute the use of tDCS after TBI (Hong-Yu et al., 2023; González-Rodriguez et al., 2022). Factors related to biological systems and individual variability are the main reasons underlying some of these inconsistencies. Studies showing positive results from tDCS after TBI were carried out on individuals in the chronic phase of trauma (Yan et al., 2020), revealing a lack of studies examining tDCS in the acute phase of TBI, which would be clinically relevant as studies suggest that early interventions are optimal for optimal recovery. According to Zaninotto et al. (2019) combining tDCS with cognitive and/or physical training can increase long-term potentiation (LTP). In view of the above, there is a need to carry out more studies in the acute or subacute phase of TBI since, to date, there is no publication of studies in these initial phases using non-invasive brain stimulation (tDCS).
Therefore, the objective of this study is to bring clinical case reports of patients with severe traumatic brain injury (TBI) who underwent tDCS in the sub-acute phase. The investigation sought to understand the therapeutic effects of tDCS on the functional and cognitive recovery of these patients, identify possible variations in results depending on the individual characteristics of the patients and the stimulation protocol used, and evaluate the safety and tolerability of the method. Furthermore, the study aims to contribute to the development of evidence-based clinical guidelines for the application of tDCS in patients with TBI.
Case description
This is a prospective, single-group forecasting study with a pre-test, post-test and follow-up, which follows the CONSORT (Consolidated Reporting Standards) extension for planned pilot testing and forecasting.
The sample consisted of 5 men with a mean age of 35.2 ± 18.75, admitted to the State Hospital for Urgency and Emergency, located in the city of Vitória, Espirito Santo, Brazil.
Patients underwent screening, which included anamnesis and assessment of inclusion and exclusion criteria.
Participants were included if they: had severe TBI, had a Glasgow Coma Scale (GCS) score ≤ 8 on admission or at some point during hospital stay, were in the subacute phase of the trauma (between 2 and 16 weeks), were between 15 and 80 years old.
They were excluded if they had: craniectomy, cranioplasty, previous neurological diseases, epidural hematoma, epilepsy and pain or bedsores that prevented the application of tDCS or that did not voluntarily accept to participate in the research.
Treatment
Participants received 5 tDCS sessions every day. The results were measured at the beginning and end of the 5 sessions. The application of tDCS was with an intensity of 2 mA. The Stimulator (DC Plus stimulator, Neuroconn, Ilmenau, Germany) provided direct current through a pair of electrodes. Surface (electrode size 35 cm2), spongy, soaked in 0.9% saline solution. The active electrode (anode) was applied to the region of the left dorsolateral prefrontal cortex (CPFDLE - F3) based on the study of Kolskar (Kolskår et al., 2021) according to the international system 10–20 and the cathode was positioned over the contralateral supraorbital area (Figure 1).
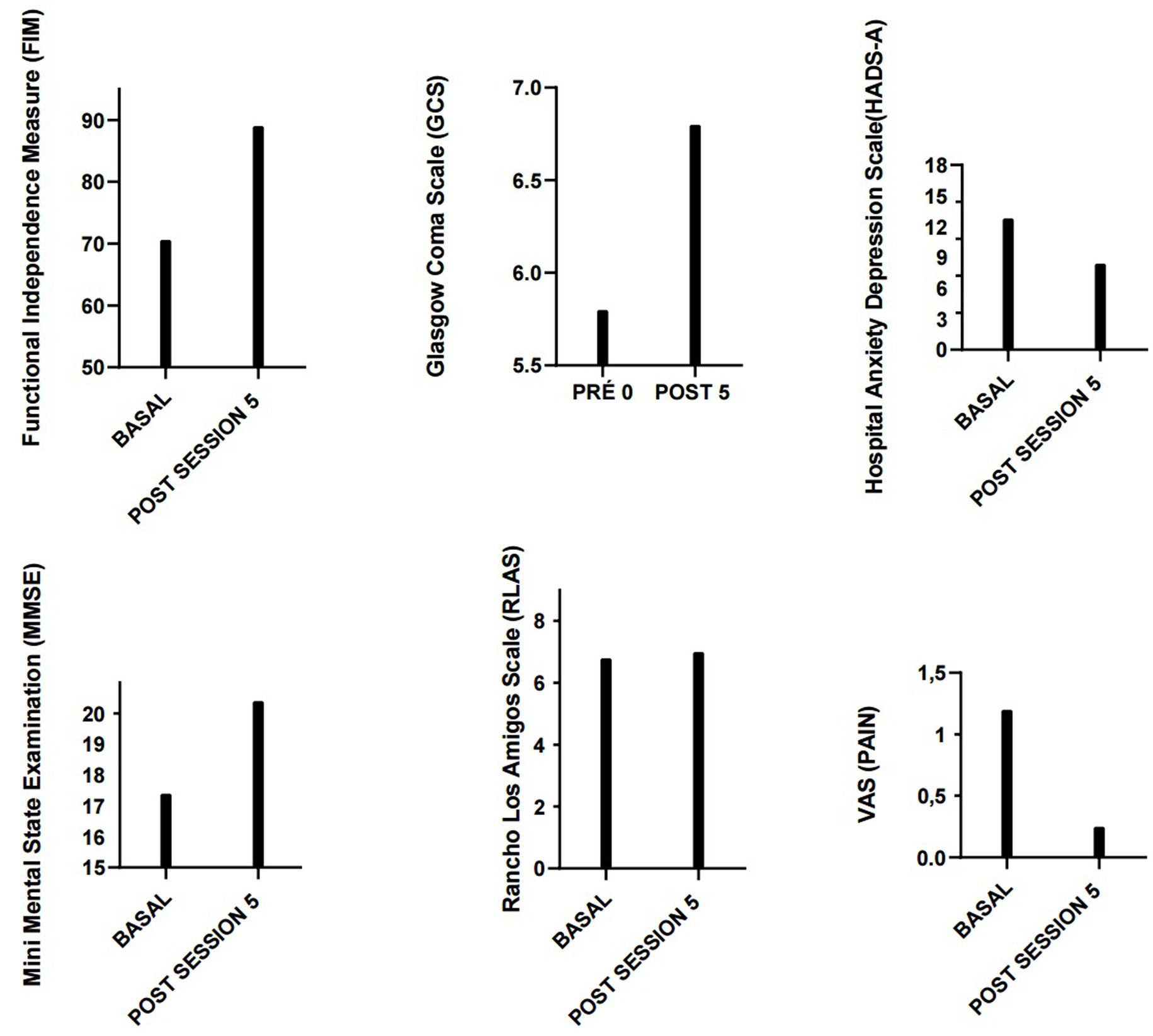
Figure 1. Results.
Clinical outcomes were measured using cognitive assessment, the Mini Mental State Examination (MMSE), mental health and depression, the Hospital Anxiety and Depression Scale (HADS-A), MMSE scores can be influenced by factors such as educational level, age, language, and ethnicity (Crum et al., 1993; Scazufca et al., 2009). Furthermore, the ability of the MMSE to identify patients with mild cognitive impairment has been considered limited (Pendlebury et al., 2010). Based on this, we used another cognitive test, the Hospital Anxiety and Depression Scale (HADS), which is widely used in clinical research. In addition, it is important to include assessments of patients’ mental state regarding symptoms of anxiety and depression, which can provide a more comprehensive view of their clinical condition.
In addition, we assessed pain, using the visual analogue scale (VAS-PAIN), Functional Independence Measure (FIM). In addition to the study results, two scales, Rancho Los Amigos Scale (RLAS) and Glasgow Outcome Scale-Extended (GOS-E), were applied to classify the patient’s condition.
The study obtained ethical approval from the Research Ethics Committee (CAAE32061920.6.0000.5060) of the Federal University of Espírito Santo, Vitória, Brazil. All study procedures remain in accordance with the Declaration of Helsinki. Informed consent was obtained.
Results
Due to the nature of an estimation study, no formal sample size calculation was performed. And, it did not have the statistical power to detect clinically significant differences in the progress assessed. For characteristics of participants and findings results, descriptive statistics were presented as mean ± Standard Deviation (SD).
Patients were assessed using scales before and after 5 days of tDCS intervention. The average evaluation results are presented below. Data reveals significant mean improvements across all scales assessed following tDCS intervention:
Mini Mental State Examination (MMSE): The average score increased from 17.2 to 20.4, indicating an improvement in cognitive function.
Hospital Anxiety and Depression Scale - Anxiety Subscale (HADS-A): The average score decreased from 12.8 to 8.4, suggesting a reduction in anxiety levels.
Visual Analogue Scale (VAS): The average score decreased from 1.2 to 0.25, indicating a reduction in pain perception.
Functional Independence Measure (FIM): The average score increased from 70.6 to 89, reflecting an improvement in patients’ functional independence.
Rancho Los Amigos Scale (RLAS): The average score increased slightly from 6.8 to 7, suggesting a small improvement in cognitive and behavioral responsiveness.
Glasgow Outcome Scale - Extended (GOS-E): The average score increased from 5.8 to 6.8, indicating an improvement in the patients’ overall outcome.
Discussion
In a sample of five patients, we tested the effect of tDCS in patients with sub-acute TBI. To our knowledge, no prior studies have examined effects of tDCS on sub-acute patients with TBI.
The results observed after the tDCS intervention, such as the increase in the MMSE score, which suggests an improvement in the patients’ cognitive abilities, were previously described by Wang et al. (2022). The substantial improvement in the evaluated areas, as observed in this study, corroborates the previously reported findings, reinforcing the effectiveness of the intervention.
The reduction in HADS-A and VAS scores indicates a significant decrease in anxiety levels and pain perception, respectively, suggesting an improvement in overall quality of life. As observed in this study, these findings are consistent with previous research, further reinforcing the effectiveness of the intervention (Starkstein and Hayhow, 2019).
The notable improvement in the FIM score points to an increase in patients’ functional independence, which is crucial for rehabilitation (Dong et al., 2021). Although improvements in the RLAS and GOS-E scales are less pronounced, they still indicate a positive trend in patient recovery.
Direct comparison between studies is complicated due to differences in protocols, regarding both electrode montage and location (both in terms of the cathode and anode), stimulation frequency, number of sessions, and current amperage. There might be greater treatment benefit with higher number of sessions and increased stimulation intensity (Charvet et al., 2018).
Some preliminary studies have shown beneficial effects of tDCS on cognitive function in healthy individuals as well as in stroke patients and these studies demonstrate good tolerability and safety in patients (Kazuta et al., 2017). Moreover, tDCS treatment response may interact with individual characteristics such as time since stroke onset, lesion location, or lesion size.
Conclusion
This study investigated the effects of transcranial direct current stimulation (tDCS) in patients with subacute traumatic brain injury (TBI), exploring this approach in patients with this specific condition. The results found suggest that tDCS may have a positive impact on the recovery of these patients, evidenced by the improvement in all assessed scores.
Although there is little evidence on the effects of tDCS in acute stroke patients, the results of this study suggest that tDCS may be a promising intervention, with the potential to benefit the recovery of patients with subacute TBI. However, it is essential to consider individual patient characteristics, such as time since injury onset, location and size of the lesion, when planning tDCS treatments.
Future studies with larger sample sizes and long-term follow-ups are needed to confirm these results and better understand the neurophysiological mechanisms underlying the observed improvements.
The positive results observed may guide healthcare professionals to adopt similar transcranial direct current stimulation (tDCS) protocols in their clinical practices. This can standardize treatments and improve outcomes for TBI patients. Furthermore, this research provides a basis for future studies that could explore different parameters of tDCS, such as duration and intensity of stimulation, as well as its combination with other therapeutic interventions.
Strength and limitation
Our case report highlights several strengths, including be first study to explore tDCS in the subacute phase of TBI, offering potential for early intervention, use of multiple outcome measures (cognitive, functional, psychological). Have clinical relevance conducted in a real-world hospital setting, making the results applicable to clinical practice. However, it does have some limitations, such short intervention duration, only five tDCS sessions, which may not capture long-term effects, lack of statistical power to detect significant differences, requiring further research to confirm findings.
Data availability statement
The datasets presented in this article are not readily available because requests to access the datasets should be directed to ZmVybmFuZG96YW5lbGFAaG90bWFpbC5jb20=.
Ethics statement
The studies involving humans were approved by the Universidade Federal do Espirito Santo. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
BC: Data curation, Investigation, Methodology, Writing – original draft. JR: Conceptualization, Data curation, Writing – original draft. EK: Conceptualization, Data curation, Writing – original draft. AT: Conceptualization, Methodology, Writing – review & editing. LN: Formal analysis, Writing – original draft. CS: Methodology, Validation, Visualization, Writing – original draft. GA: Writing – review & editing. WSF: Data curation, Formal analysis, Writing – original draft. CA: Investigation, Resources, Validation, Visualization, Writing – review & editing. WSP: Conceptualization, Methodology, Supervision, Validation, Visualization, Writing – review & editing. JB: Writing – review & editing. FA: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Areas, F. Z. S., Schwarzbold, M. L., Diaz, A. P., Rodrigues, I. K., Sousa, D. S., Ferreira, C. L., et al. (2019). Predictors of hospital mortality and the related burden of disease in severe traumatic brain injury: a prospective multicentric study in Brazil. Front. Neurol. 10, 1–8. doi: 10.3389/fneur.2019.00432
Bruns, J. Jr., and Hauser, W. A. (2003). The epidemiology of traumatic brain injury: a review. Epilepsia 44, 2–10. doi: 10.1046/j.1528-1157.44.s10.3.x
Charvet, L. E., Dobbs, B., Shaw, M. T., Bikson, M., Datta, A., and Krupp, L. B. (2018). Remotely supervised transcranial direct current stimulation for the treatment of fatigue in multiple sclerosis: results from a randomized, sham-controlled trial. Mult. Scler. J. 24, 1760–1769. doi: 10.1177/1352458517732842
Crum, R. M., Anthony, J. C., Bassett, S. S., and Folstein, M. F. (1993). Population-based norms for the Mini-mental state examination by age and educational level. JAMA 269, 2386–2391. doi: 10.1001/jama.1993.03500180078038
Dong, K., Meng, S., Guo, Z., Zhang, R., Xu, P., Yuan, E., et al. (2021). The effects of transcranial direct current stimulation on balance and gait in stroke patients: a systematic review and Meta-analysis. Front. Neurol. 12:650925. doi: 10.3389/fneur.2021.650925
Fregni, F., and Pascual-Leone, A. (2007). Technology insight: noninvasive brain stimulation in neurology-perspectives on the therapeutic potential of rTMS and tDCS. Nat. Clin. Pract. Neurol. 3, 383–393. doi: 10.1038/ncpneuro0530
González-Rodriguez, B., Serradell-Ribé, N., Viejo-Sobera, R., Romero-Muñoz, J. P., and Marron, E. M. (2022). Transcranial direct current stimulation in neglect rehabilitation after stroke: a systematic review. J. Neurol. 269, 6310–6329. doi: 10.1007/s00415-022-11338-x
Hong-Yu, L., Zhi-Jie, Z., Juan, L., Ting, X., Wei-Chun, H., and Ning, Z. (2023). Effects of cerebellar transcranial direct current stimulation in patients with stroke: a systematic review. Cerebellum 22, 973–984. doi: 10.1007/s12311-022-01464-7
Kazuta, T., Takeda, K., Osu, R., Tanaka, S., Oishi, A., Kondo, K., et al. (2017). Transcranial direct current stimulation improves Audioverbal memory in stroke patients. Am. J. Phys. Med. Rehabil. 96, 565–571. doi: 10.1097/PHM.0000000000000686
Kolskår, K. K., Richard, G., Alnaes, D., Dørum, E. S., Sanders, A. M., Ulrichsen, K. M., et al. (2021). Reliability, sensitivity, and predictive value of fMRI during multiple object tracking as a marker of cognitive training gain in combination with tDCS in stroke survivors. Hum. Brain Mapp. 42, 1167–1181. doi: 10.1002/hbm.25284.3321640845
Newcombe, V. F., Outtrim, J. G., Chatfield, D. A., Manktelow, A., Hutchinson, P. J., Coles, J. P., et al. (2011). Parcellating the neuroanatomical basis of impaired decision making in traumatic brain injury. Brain 134, 759–768. doi: 10.1093/brain/awq388
Pendlebury, S. T., Cuthbertson, F. C., Welch, S. J., Mehta, Z., and Rothwell, P. M. (2010). Underestimation of cognitive impairment by Mini-mental state examination versus the Montreal cognitive assessment in patients with transient ischemic attack and stroke: a population-based study. Stroke 41, 1290–1293. doi: 10.1161/STROKEAHA.110.579888
Scazufca, M., Almeida, O. P., Vallada, H. P., Tasse, W. A., and Menezes, P. R. (2009). Limitations of the Mini-mental state examination for screening dementia in a community with low socioeconomic status: results from the Sao Paulo Ageing & Health Study. Eur. Arch. Psychiatry Clin. Neurosci. 259, 8–15. doi: 10.1007/s00406-008-0827-6
Starkstein, S. E., and Hayhow, B. D. (2019). Treatment of post-stroke depression. Curr. Treat. Options Neurol. 21:31. doi: 10.1007/s11940-019-0570-5
Wang, Y., Xu, N., Wang, R., and Zai, W. (2022). Systematic review and network meta-analysis of effects of noninvasive brain stimulation on post-stroke cognitive impairment. Front. Neurosci. 16:1082383. doi: 10.3389/fnins.2022.1082383
Yan, R. B., Zhang, X. L., Li, Y. H., Hou, J. M., Chen, H., and Liu, H. L. (2020). Effect of transcranial direct-current stimulation on cognitive function in stroke patients: a systematic review and meta-analysis. PLoS One 15:e0233903. doi: 10.1371/journal.pone.0233903
Zaninotto, A. L., El-Hagrassy, M. M., Green, J. R., Babo, M., Paglioni, V. M., Benute, G. G., et al. (2019). Transcranial direct current stimulation (tDCS) effects on traumatic brain injury (TBI) recovery: a systematic review. Dement Neuropsychol. 13, 172–179. doi: 10.1590/1980-57642018dn13-020005.31285791
Keywords: neuromodulation, traumatic brain injury, tDCS, reahabilitation, case report
Citation: Cordeiro BNdL, Rocha JVDS, Kuster E, Thibauth A, Nascimento LR, Swank C, Arêas GPT, da Silva Filho WG, Anhoque CF, Silva Paiva W, Buarque JC and Arêas FZ (2025) Transcranial direct current stimulation in individuals with severe traumatic brain injury in the subacute phase: a case series. Front. Hum. Neurosci. 19:1552387. doi: 10.3389/fnhum.2025.1552387
Edited by:
Jeffrey Cheng, Harvard Medical School, United StatesReviewed by:
Thais Raquel Martins Filippo, Universidade Nove de Julho, BrazilJustin R. Deters, The University of Iowa, United States
Copyright © 2025 Cordeiro, Rocha, Kuster, Thibauth, Nascimento, Swank, Arêas, da Silva Filho, Anhoque, Silva Paiva, Buarque and Arêas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fernando Zanela Arêas, ZmVybmFuZG96YW5lbGFAaG90bWFpbC5jb20=