 Paweł Chmara
Paweł Chmara Sabina Brazevic
Sabina Brazevic Marek Jóźwiak
Marek Jóźwiak Brian Po-Jung Chen
Brian Po-Jung Chen Faustyna Manikowska
Faustyna Manikowska- 1Gait and Motion Analysis Laboratory, Department of Pediatric Orthopedics and Traumatology, Poznań University of Medical Sciences, Poznań, Poland
- 2Motion Analysis Laboratory, Bone and Joint Research Center, Chang Gung Memorial Hospital - Linkou, Taoyuan, Taiwan
Introduction: Cerebral palsy (CP) often leads to impairments in movement and posture, limiting functional mobility. Robotic-assisted gait training (RAGT) using powered exoskeletons has emerged as a novel approach to enhance gait in individuals with CP. However, evidence regarding its effectiveness, particularly in unassisted gait performance, remains limited and inconclusive.
Methods: This study involved 44 ambulatory youth with bilateral hypertonic CP (GMFCS levels I–III), who underwent an intensive RAGT program using the EksoGT exoskeleton. The intervention consisted of 28 sessions (90 min each) over 8 weeks, with a 2 weeks mid-point break. Gait assessments were conducted before (T1) and after (T2) therapy using 3D motion analysis and the 6-minute walk test (6MWT). Primary outcomes included spatiotemporal parameters, gait symmetry, gait deviation index (GDI), and walking endurance.
Results: Following the exoskeleton training, participants demonstrated a statistically significant improvement in gait efficiency, with 6MWT distances increasing from 375 to 418 m (p < 0.01). However, no significant changes were observed in gait symmetry, spatiotemporal parameters, or GDI scores, indicating no measurable effect on unassisted gait mechanics.
Conclusion: Intensive exoskeleton therapy significantly improved walking endurance but did not alter gait symmetry or kinematics in independently ambulatory youth with hypertonic CP. These - findings suggest that while exoskeleton assisted training enhances functional endurance, its impact on gait pattern may be limited. Further research should explore its broader benefits on quality of life, participation, and psychosocial outcomes.
1 Introduction
Children with cerebral palsy (CP), resulting from a non-progressive brain lesion, present with permanent disorders of movement and posture that lead to functional disability (Rosenbaum et al., 2007). The combination of multiple impairments contributes to abnormal muscle activity and movement patterns, which can be categorized as either positive motor signs (e.g., hypertonia and involuntary movements) or negative motor signs (e.g., muscle weakness and impaired control) (Sanger et al., 2006). These motor deficits collectively limit functional performance.
Among the available interventions, task-specific functional therapy has been identified as the most effective approach for enhancing gross motor function in children with CP. This method emphasizes active participation in daily life activities that involve purposeful movement execution to improve coordination and motor performance (Christy et al., 2012; Graham et al., 2016). Active engagement, both physical and cognitive, is essential for therapeutic success. In contrast, passive interventions such as manual manipulation by a therapist or mechanical assistance using devices like exoskeletons have shown limited efficacy, potentially due to reduced engagement of both the patient and their nervous system (Graham et al., 2016).
Robotic-assisted gait training (RAGT) has emerged as a widely used rehabilitation modality to improve gait in individuals with neurological impairments. Various forms of RAGT, including driven gait orthoses and powered lower limb exoskeletons, aim to enhance voluntary movement control by adapting joint motion (e.g., at the ankle or knee), measuring human-machine interaction forces, supporting leg movement, providing body weight support, and maintaining gait trajectories. These systems have demonstrated benefits in children with CP (Banz et al., 2008; Brütsch et al., 2010; Jamwal et al., 2020). However, despite promising results, the overall evidence remains limited due to the lack of standardized outcome measures. Furthermore, the comparative efficacy of RAGT versus conventional therapy remains under debate (Bunge et al., 2021; Cortés-Pérez et al., 2022).
According to the World Health Organization’s International Classification of Functioning, Disability and Health (ICF), promoting independence in daily activities is a key therapeutic goal (Gormley, 2001; Gómez-Salgado et al., 2018). While powered exoskeletons, one of the most widely used RAGT devices, involve some degree of passive assistance, they enable overground walking that closely resembles natural daily activity and require less hands-on input from the therapist. This allows for more cognitively engaging practice, potentially enhancing therapeutic outcomes (Fasoli et al., 2012).
The aim of this study was to evaluate the effect of powered lower limb exoskeleton use on gait parameters in children with spastic CP. Specifically, the study investigated short-term changes in spatiotemporal gait parameters, gait kinematics, and gait asymmetry.
2 Materials and methods
2.1 Participants
A total of 44 subjects diagnosed with hypertonic CP were recruited for the study and underwent exoskeleton-assisted gait training (20 females, 24 males; mean age: 17.61 ± 3.95 years). The study group consisted of ambulatory individuals with bilateral lower limb involvement. All participants were able to walk independently or with assistive devices and were classified within levels I to III of the Gross Motor Function Classification System (GMFCS): Level I (n = 5), Level II (n = 31), and Level III (n = 8).
Inclusion criteria were as follows: (1) diagnosis of bilateral hypertonic CP, (2) no orthopedic surgery within the past year, (3) no botulinum toxin injections within the last 6 months, (4) ability to follow verbal instructions, and (5) a primary therapeutic goal of improving gait function. Exclusion criteria included: (1) the presence of pain, (2) fixed contractures that prevented participation in training, and (3) leg length discrepancy greater than 0.5 cm.
Gait training sessions were conducted at the outpatient clinic of a local rehabilitation hospital. All assessments were performed at the Motion Analysis Laboratory of a local orthopedic hospital. The study was approved by the appropriate Institutional Review Board. Written informed consent was obtained from all participants aged 18 years or older and from parents or legal guardians for those under 18 years of age.
2.2 Protocol
Each participant underwent a total of 28 therapy sessions of exoskeleton training over a period of 8 consecutive weeks, with a 2 weeks break at the midpoint. Each session lasted 90 min and included the following components:
1. Warm-up: Strength and balance exercises to prepare for gait training.
2. Therapy session: 40 min of walking practice using the exoskeleton device.
3. Cool-down: Stretching exercises to conclude the session.
Exoskeleton training was conducted using the EksoGT powered exoskeleton (Ekso Bionics Holdings, Inc., San Rafael, CA, United States). The device is designed for users with a body weight of up to 100 kg, a height range of 1.58–1.88 m, and a maximum hip width of 45.7 cm. The system weighs 27 kg and includes two lithium-ion batteries (2 Ah, 48.1 VDC) capable of producing a peak current of 30 A, allowing full-load operation for up to 60 min.
The EksoGT supports active hip flexion from −20° to 135° and passive hip abduction from −2° to 4°. Knee flexion is motor-assisted within a 0°–135° range, while the ankle allows passive plantarflexion from −10° to 10°. Foot stiffness can be adjusted on a scale of 1 (flexible) to 4 (rigid). The device enables a walking speed of approximately 2 km/h, with adjustable step lengths (20.3–45.7 cm), step widths (0.0–7.6 cm), and swing phase durations (0.8–2.5 s). Before the first therapy session, each participant received a 30–60 min adaptation period to become familiar with walking in the exoskeleton.
Gait performance was assessed twice for each subject: prior to the intervention (T1) and immediately after completing the 28 therapy sessions (T2). Assessments included instrumental gait analysis and the six-minute walk test (6MWT) (Enright, 2003). The 6MWT was used to evaluate gait endurance. During the test, participants walked at their maximum achievable speed along a 15 m straight course for 6 min. The course was marked on a flat surface using cones, with each meter clearly labeled. An examiner recorded the distance covered using a stopwatch, and the total distance was calculated by summing the number of completed laps and any additional meters from the final, incomplete lap.
Kinematic data were collected using an 8-camera motion capture system (six Bonita 3 and two Vero 2.2; Vicon Motion Systems Ltd., Oxford, United Kingdom) at a sampling rate of 120 Hz. Reflective markers were placed according to the standard Lower Body Plug-in-Gait protocol. All participants walked barefoot along a 10 m walkway at a self-selected speed during data collection.
2.3 Outcome measure
The primary outcome measures included the following gait spatiotemporal parameters: step time (s), step length (m), step width (m), stride time (s), stride length (m), walking speed (m/s), cadence (steps/min), single support (% of gait cycle), double support (% of gait cycle), and foot-off (% of gait cycle). In addition, the gait symmetry index (SI) was calculated for each of these parameters. Further outcome measures included the Gait Deviation Index (GDI) and the total distance covered in the 6MWT.
Gait symmetry was calculated based on the spatiotemporal parameters using the following formula: (Robinson et al., 1987)
where:
An SI value of 0 indicates perfect symmetry; negative values indicate asymmetry favoring the left side, while positive values indicate asymmetry favoring the right.
Changes in GDI values were categorized as improvement when ΔGDI ≥ 5, deterioration when ΔGDI ≤ −5, and no change when −5 < ΔGDI < 5 (Schwartz et al., 2016; Rajagopal et al., 2018).
2.4 Statistical analysis
The normality of data distribution was assessed using the Shapiro-Wilk test. For variables that were normally distributed and exhibited homogeneity of variance, paired t-tests were used to evaluate changes over time. For non-normally distributed variables or those with heterogeneous variance, the Wilcoxon signed-rank test was applied. Differences in the Gait Deviation Index (GDI) were analyzed using the Fisher-Freeman-Halton test. All statistical analyses were conducted using the Statistical software (Version 14; TIBCO Software Inc., Palo Alto, CA, United States). A p-value of < 0.05 was considered statistically significant.
3 Results
3.1 Six-minute walk test (6MWT)
Analysis of the effect of exoskeleton therapy on gait efficiency in patients with CP demonstrated a statistically significant improvement in the distance covered during the 6MWT (T1 = 375 m; T2 = 418 m; p < 0.01; normally distributed; Figure 1).
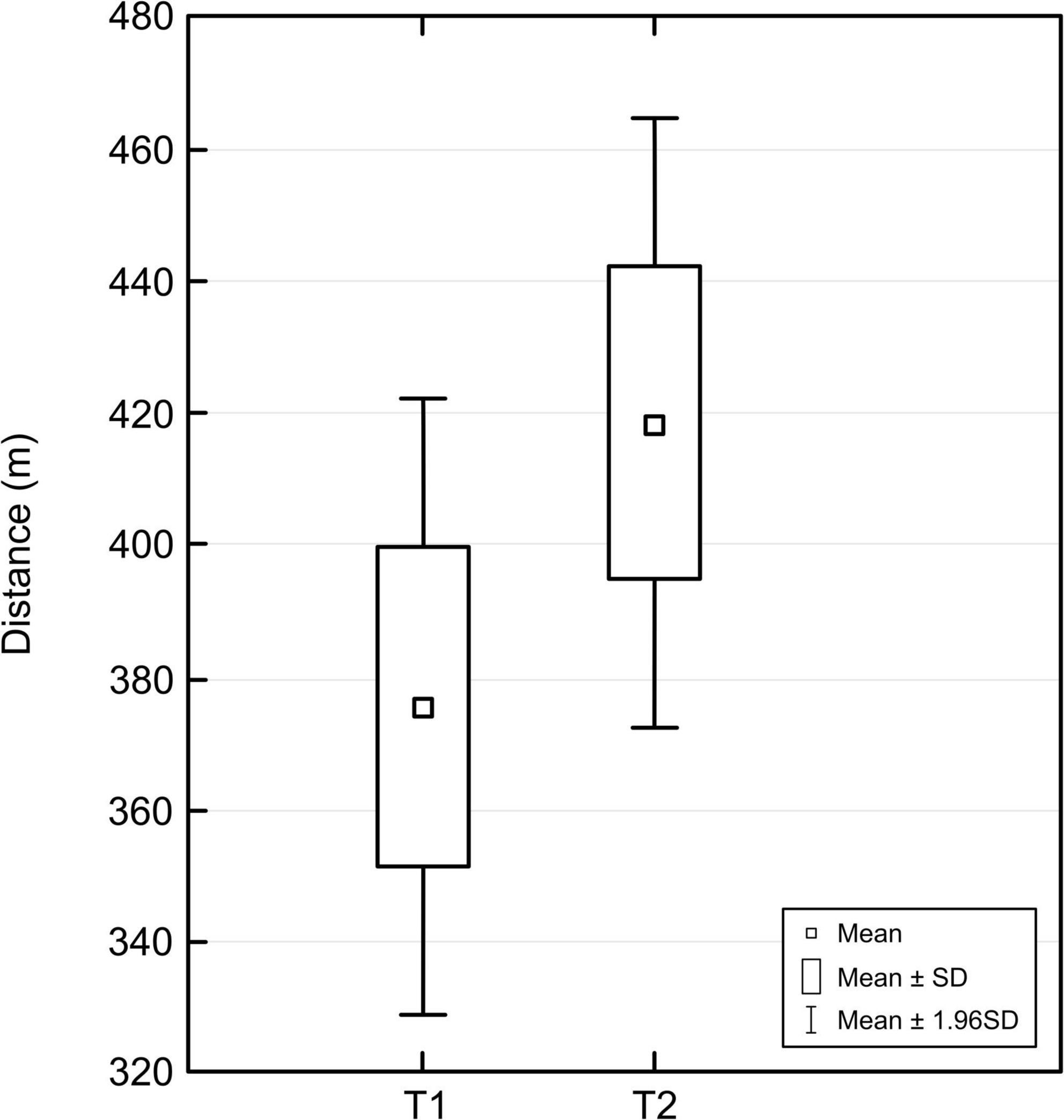
Figure 1. Changes in six-minute walk test (6MWT) distance before (T1) and after (T2) robotic-assisted gait training (RAGT).
3.2 Gait symmetry
No statistically significant changes in gait symmetry were observed following exoskeleton therapy (Table 1).
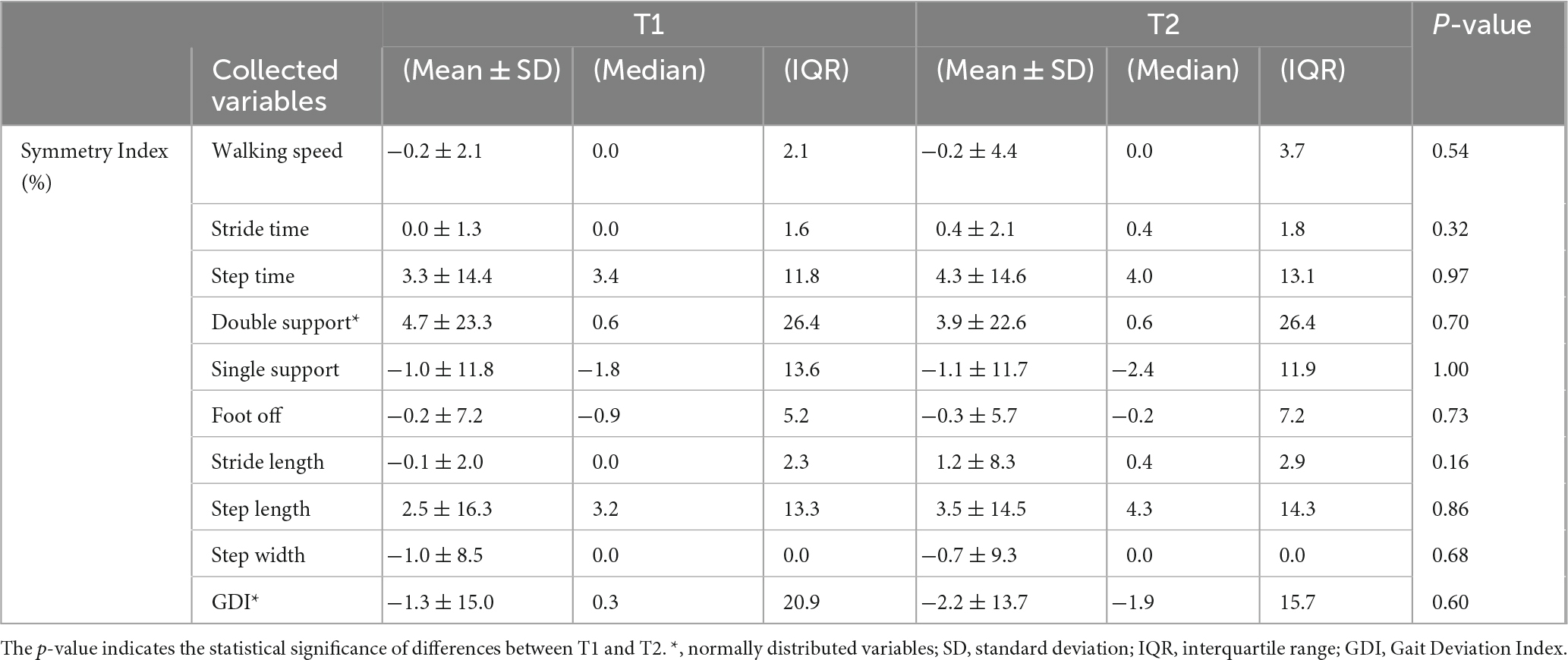
Table 1. Gait symmetry index before (T1) and after (T2) the exoskeleton therapy.
3.3 Spatiotemporal gait parameters
Analysis of spatiotemporal gait parameters revealed no statistically significant changes after the intervention (Table 2).
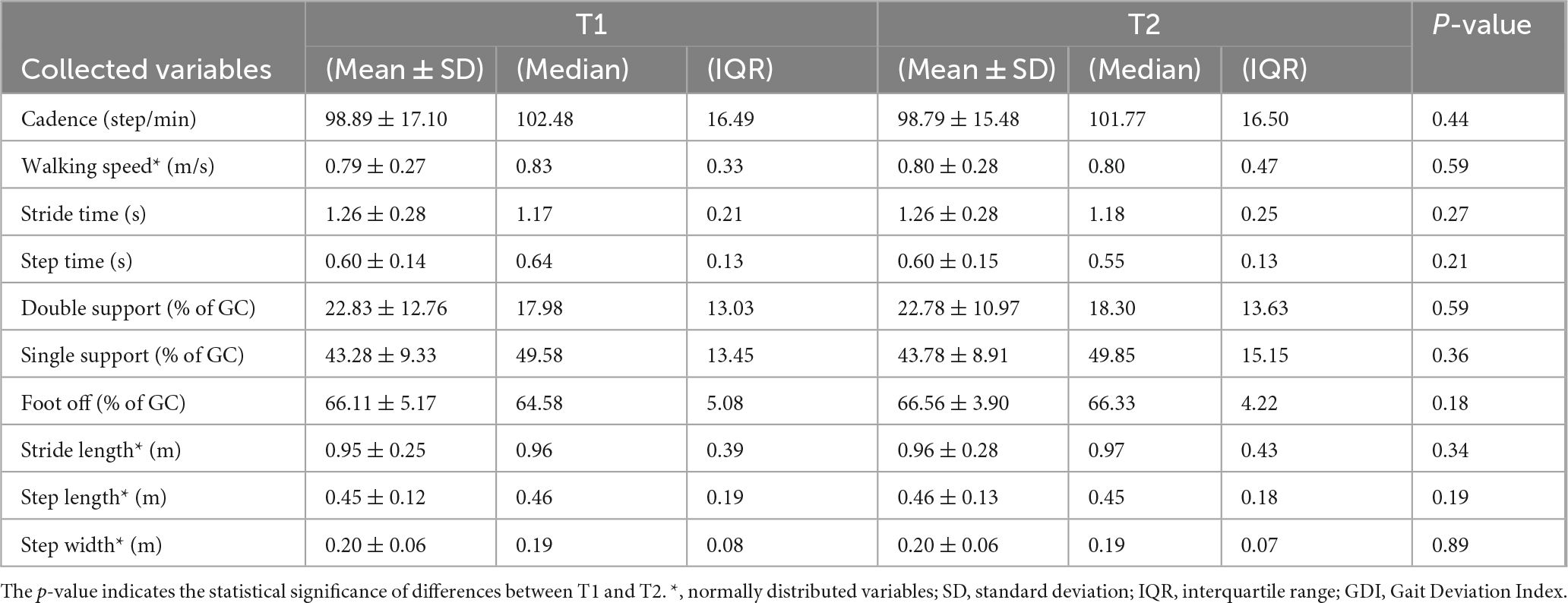
Table 2. Spatiotemporal parameters before (T1) and after (T2) the exoskeleton therapy.
3.4 Gait Deviation Index (GDI)
No statistically significant changes in gait kinematics, as measured by the Gait Deviation Index, were found following exoskeleton therapy (Table 3).
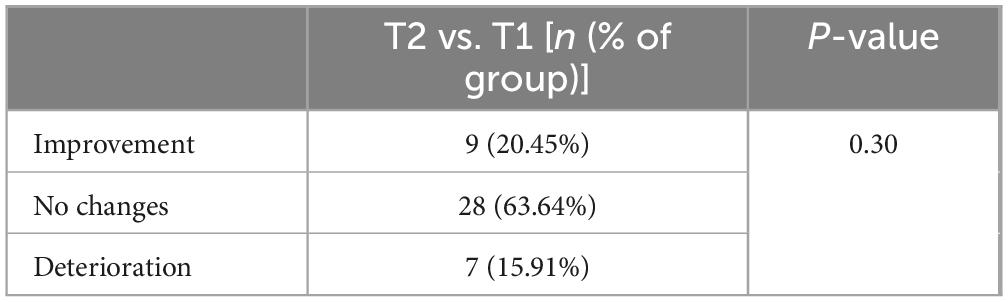
Table 3. Number of participants showing changes in Gait Deviation Index (GDI).
4 Discussions
The aim of this study was to evaluate the effectiveness of intensive exoskeleton-assisted therapy on gait in ambulatory individuals with hypertonic CP. Our findings indicate that, while this form of exoskeleton training significantly improved gait efficiency, as measured by the six-minute walk test (6MWT), it did not result in statistically significant changes in gait symmetry, spatiotemporal parameters, or kinematic patterns.
The literature on the efficacy of exoskeleton therapy in individuals with CP remains limited and highly variable in terms of methodology, participant characteristics, and outcome measures (Bunge et al., 2021; Hunt et al., 2022). Previous studies reviewed in this study have been conducted with heterogeneous samples differing in age, diagnosis, functional level, sample size, and therapy duration. Some findings are based on a single session with a single participant, making it difficult to generalize conclusions. To our knowledge, this study represents one of the largest and most homogeneous cohorts to date. We evaluated 44 youths with bilateral hypertonic CP, all ambulatory without third-party assistance (GMFCS levels I–III), and all received the same long-term, intensive exoskeletal training protocol without additional therapeutic interventions. Gait outcomes were assessed using objective, instrumented measures.
Importantly, our study cohort consisted of adolescents and young adults (mean age: 18 years), a population in which functional development and gait patterns are generally considered stable. This minimizes the confounding influence of natural developmental changes on gait, which is a significant concern in studies involving younger children. Previous research has included participants ranging from 5 to 31 years of age, making it difficult to isolate the effects of exoskeleton due to age-related variability in gait (Sutherland, 1997; Ganley and Powers, 2005).
The evidence regarding the effect of exoskeleton on spatiotemporal gait parameters is inconsistent. Some studies report significant improvements, while others find no measurable changes (Bayón et al., 2016; Lerner et al., 2017a; Mataki et al., 2018; Matsuda et al., 2018; Ueno et al., 2019; Nakagawa et al., 2020; Thurston et al., 2021). Additionally, certain studies evaluated gait parameters while participants were wearing the exoskeleton, which can introduce bias. Improvements in parameters such as walking speed, cadence, and step length have been observed in some of these studies, while others report no change, or even a decline (Robinson et al., 1987; Mileti et al., 2016; Lerner et al., 2017d,2017a,2017c; Orekhov et al., 2020). Improvements in gait symmetry and lower limb kinematics during assisted walking have also been documented. However, it is important to recognize that gait patterns induced by powered exoskeletons may not be retained once the device is removed, thus limiting the interpretation of such immediate effects as true functional gains.
Despite the absence of significant changes in kinematic data following therapy, we conducted a detailed analysis of the direction of change in the Gait Deviation Index (GDI). The results showed that GDI improved in nine subjects, declined in seven, and remained unchanged in the majority (28 subjects). Further analysis indicated that GMFCS level was not a distinguishing factor for improvement or deterioration, among those who improved, six were classified as GMFCS level II and 1 as level III.
In contrast to studies assessing gait while wearing the device, we focused on evaluating unassisted, barefoot gait before and after a full course of therapy (28 sessions). Our results did not reveal any significant changes in spatiotemporal parameters, symmetry, or kinematics, suggesting that 28-session exoskeleton training in 8 weeks may not induce lasting modifications in gait pattern among independently ambulatory youth with CP.
Despite the lack of significant changes in gait mechanics, we observed a meaningful improvement in gait efficiency, as reflected in the increased distance covered during the 6MWT. This suggests a potential training effect resulting from sustained walking with resistance. Given the 27 kg weight of the exoskeleton and the intensity of each session (40 min of active walking), it is plausible that this form of therapy contributed to improved muscular endurance and walking capacity. Prior studies have suggested that the weight of the device could impose a metabolic burden (Rossi et al., 2013; Russell Esposito et al., 2018); however, our findings align with literature indicating that resistance or strength-based training can improve function in individuals with CP and support the notion that exoskeleton use may provide a similar benefit.
Most existing studies, including ours, have focused on ambulatory individuals with CP classified as GMFCS levels I–III (Lerner et al., 2016, 2017d,2017b; 2017a; 2017c; 2018; 2019; Takahashi et al., 2018; Orekhov et al., 2020; Chen et al., 2021; Fang et al., 2022). A limited number of studies have examined the effects of exoskeleton in non-ambulatory individuals, i.e., GMFCS level IV (Smania et al., 2012; Nakagawa et al., 2019, 2020; Ueno et al., 2019). However, interpreting gait-related outcomes in non-ambulatory populations may be problematic, as these individuals are not accustomed to autonomous locomotion. In such cases, the value of exoskeleton therapy may lie more in enhancing participation and quality of life rather than altering gait patterns. While theoretical frameworks suggest that exoskeleton could facilitate community participation and mobility, empirical evidence supporting this claim is currently lacking (Bunge et al., 2021).
4.1 Limitations
A key limitation of this study is its exclusive focus on gait-related outcomes. Although gait is a critical component of functional mobility, the potential benefits of exoskeleton therapy may extend beyond biomechanics to include psychosocial domains such as participation, self-efficacy, and quality of life. These aspects were not assessed in the present study and should be a focus for future research to comprehensively evaluate the impact of exoskeleton in individuals with CP.
While the current study demonstrated the benefits of an intensive program, future research may be strengthened by incorporating longitudinal follow-up, control groups, and multidimensional outcome measures to better establish the therapeutic potential of robotic gait interventions.
Regarding the statistical analysis used to interpret our results, although appropriate analyses have been applied, additional methods, such as effect size metrics and predictive modeling, could further provide more comprehensive insights and strengthen the interpretation of the therapy program’s effectiveness.
5 Conclusion
This study demonstrates that an intensive exoskeleton program can significantly improve gait efficiency in ambulatory youth with hypertonic CP. Despite this improvement in gait endurance, no statistically significant changes were observed in gait symmetry, spatiotemporal parameters, or kinematic profiles. These findings suggest that while the powered exoskeleton may effectively enhance functional walking capacity, it does not appear to meaningfully alter unassisted gait patterns in the short term. Future research should investigate the broader impact of exoskeleton therapy, including its effects on quality of life, social participation, and psychological wellbeing, to better understand its full therapeutic potential.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethical Committee of Poznań University of Medical Sciences. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
PC: Conceptualization, Writing – review and editing, Writing – original draft, Project administration, Methodology, Data curation, Formal Analysis. SB: Writing – review and editing, Project administration, Formal Analysis, Writing – original draft, Data curation, Methodology, Conceptualization. MJ: Conceptualization, Funding acquisition, Writing – review and editing, Supervision, Writing – original draft. BC: Writing – original draft, Formal Analysis, Methodology, Writing – review and editing. FM: Project administration, Methodology, Writing – review and editing, Conceptualization, Investigation, Supervision, Funding acquisition, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by a grant from the Polish National Centre for Research and Development (NCBiR): Grant No. POIR.04.01.04-00-0035/19-00.
Acknowledgments
We would like to acknowledge the staff of Poznań University of Medical Sciences, Poland, and Chang Gung Memorial Hospital – Linkou, Taiwan, for their support and assistance in conducting this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Banz, R., Bolliger, M., Colombo, G., Dietz, V., and Lünenburger, L. (2008). Computerized visual feedback: An adjunct to robotic-assisted gait training. Phys. Ther. 88, 1135–1145. doi: 10.2522/ptj.20070203
Bayón, C., Lerma, S., Ramírez, O., Serrano, J., Del Castillo, M., Raya, R., et al. (2016). Locomotor training through a novel robotic platform for gait rehabilitation in pediatric population: Short report. J. Neuroeng. Rehabil. 13:98. doi: 10.1186/s12984-016-0206-x
Brütsch, K., Schuler, T., Koenig, A., Zimmerli, L., Koeneke, S. M., Lünenburger, L., et al. (2010). Influence of virtual reality soccer game on walking performance in robotic assisted gait training for children. J. Neuroeng. Rehabil. 7:15. doi: 10.1186/1743-0003-7-15
Bunge, L., Davidson, A., Helmore, B., Mavrandonis, A., Page, T., Schuster-Bayly, T., et al. (2021). Effectiveness of powered exoskeleton use on gait in individuals with cerebral palsy: A systematic review. PLoS One 16:e0252193. doi: 10.1371/journal.pone.0252193
Chen, J., Hochstein, J., Kim, C., Tucker, L., Hammel, L., Damiano, D., et al. (2021). A pediatric knee exoskeleton with real-time adaptive control for overground walking in ambulatory individuals with cerebral palsy. Front. Robot. AI 8:702137. doi: 10.3389/frobt.2021.702137
Christy, J., Chapman, C., and Murphy, P. (2012). The effect of intense physical therapy for children with cerebral palsy. J. Pediatr. Rehabil. Med. 5, 159–170. doi: 10.3233/PRM-2012-0208
Cortés-Pérez, I., González-González, N., Peinado-Rubia, A., Nieto-Escamez, F., Obrero-Gaitán, E., and García-López, H. (2022). Efficacy of robot-assisted gait therapy compared to conventional therapy or treadmill training in children with cerebral palsy: A systematic review with meta-analysis. Sensors 22:9910. doi: 10.3390/s22249910
Enright, P. (2003). The six-minute walk test. Respir. Care 48, 783–785. doi: 10.4187/respcare.03480783
Fang, Y., Orekhov, G., and Lerner, Z. (2022). Adaptive ankle exoskeleton gait training demonstrates acute neuromuscular and spatiotemporal benefits for individuals with cerebral palsy: A pilot study. Gait Posture 95, 256–263. doi: 10.1016/j.gaitpost.2020.11.005
Fasoli, S., Ladenheim, B., Mast, J., and Krebs, H. (2012). New horizons for robot-assisted therapy in pediatrics. Am. J. Phys. Med. Rehabil. 91, S280–S289. doi: 10.1097/PHM.0b013e31826bcff4
Ganley, K., and Powers, C. (2005). Gait kinematics and kinetics of 7-year-old children: A comparison to adults using age-specific anthropometric data. Gait Posture 21, 141–145. doi: 10.1016/j.gaitpost.2004.01.007
Gómez-Salgado, J., Jacobsohn, L., Frade, F., Romero-Martin, M., and Ruiz-Frutos, C. (2018). Applying the WHO international classification of functioning, disability and health in nursing assessment of population health. Int. J. Environ. Res. Public Health. 15:2245. doi: 10.3390/ijerph15102245
Gormley, M. (2001). Treatment of neuromuscular and musculoskeletal problems in cerebral palsy. Pediatr. Rehabil. 4, 5–16. doi: 10.1080/13638490151068393
Graham, H., Rosenbaum, P., Paneth, N., Dan, B., Lin, J., Damiano, D., et al. (2016). Cerebral palsy. Nat. Rev. Dis. Primers 2:15082. doi: 10.1038/nrdp.2015.82
Hunt, M., Everaert, L., Brown, M., Muraru, L., Hatzidimitriadou, E., and Desloovere, K. (2022). Effectiveness of robotic exoskeletons for improving gait in children with cerebral palsy: A systematic review. Gait Posture 98, 343–354. doi: 10.1016/j.gaitpost.2022.09.082
Jamwal, P., Hussain, S., and Ghayesh, M. (2020). Robotic orthoses for gait rehabilitation: An overview of mechanical design and control strategies. Proc. Inst. Mech. Eng. H 234, 444–457. doi: 10.1177/0954411919898293
Lerner, Z., Damiano, D., and Bulea, T. (2017b). Relationship between assistive torque and knee biomechanics during exoskeleton walking in individuals with crouch gait. IEEE Int. Conf. Rehabil. Robot. 2017, 491–497. doi: 10.1109/ICORR.2017.8009296
Lerner, Z., Damiano, D., and Bulea, T. (2017c). The effects of exoskeleton assisted knee extension on lower-extremity gait kinematics, kinetics, and muscle activity in children with cerebral palsy. Sci. Rep. 7:13512. doi: 10.1038/s41598-017-13554-2
Lerner, Z., Damiano, D., and Bulea, T. C. A. (2016). robotic exoskeleton to treat crouch gait from cerebral palsy: Initial kinematic and neuromuscular evaluation. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2016, 2214–2217. doi: 10.1109/EMBC.2016.7591169
Lerner, Z., Damiano, D., and Bulea, T. C. A. (2017a). lower-extremity exoskeleton improves knee extension in children with crouch gait from cerebral palsy. Sci. Transl. Med. 9:eaam9145. doi: 10.1126/scitranslmed.aam9145
Lerner, Z., Damiano, D., Park, H., Gravunder, A., and Bulea, T. C. (2017d). A Robotic exoskeleton for treatment of crouch gait in children with cerebral palsy: Design and initial application. IEEE Trans. Neural Syst. Rehabil. Eng. 25, 650–659. doi: 10.1109/TNSRE.2016.2595501
Lerner, Z., Gasparri, G., Bair, M., Lawson, J., Luque, J., Harvey, T., et al. (2018). An untethered ankle exoskeleton improves walking economy in a pilot study of individuals with cerebral palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 26, 1985–1993. doi: 10.1109/TNSRE.2018.2870756
Lerner, Z., Harvey, T., and Lawson, J. L. (2019). A battery-powered ankle exoskeleton improves gait mechanics in a feasibility study of individuals with cerebral palsy. Ann. Biomed. Eng. 47, 1345–1356. doi: 10.1007/s10439-019-02237-w
Mataki, Y., Kamada, H., Mutsuzaki, H., Shimizu, Y., Takeuchi, R., Mizukami, M., et al. (2018). Use of hybrid assistive limb (HAL®) for a postoperative patient with cerebral palsy: A case report. BMC Res. Notes 11:201. doi: 10.1186/s13104-018-3311-z
Matsuda, M., Iwasaki, N., Mataki, Y., Mutsuzaki, H., Yoshikawa, K., Takahashi, K., et al. (2018). Robot-assisted training using Hybrid Assistive Limb® for cerebral palsy. Brain Dev. 40, 642–648. doi: 10.1016/j.braindev.2018.04.004
Mileti, I., Taborri, J., Rossi, S., Petrarca, M., Patane, F., and Cappa, P. (2016). “Evaluation of the effects on stride-to-stride variability and gait asymmetry in children with Cerebral Palsy wearing the WAKE-up ankle module,” in Proceedings of the 2016 IEEE International Symposium on Medical Measurements and Applications (MeMeA), (Piscataway. NJ: IEEE). doi: 10.1109/MeMeA.2016.7533748
Nakagawa, S., Mutsuzaki, H., Mataki, Y., Endo, Y., Kamada, H., and Yamazaki, M. (2019). Improvement and sustainability of walking ability with hybrid assistive limb training in a patient with cerebral palsy after puberty: A case report. J. Phys. Ther. Sci. 31, 633–637. doi: 10.1589/jpts.31.633
Nakagawa, S., Mutsuzaki, H., Mataki, Y., Endo, Y., Matsuda, M., Yoshikawa, K., et al. (2020). Safety and immediate effects of Hybrid assistive limb in children with cerebral palsy: A pilot study. Brain Dev. 42, 140–147. doi: 10.1016/j.braindev.2019.10.003
Orekhov, G., Fang, Y., Luque, J., and Lerner, Z. (2020). Ankle exoskeleton assistance can improve over-ground walking economy in individuals with cerebral palsy. IEEE Trans. Neural Syst. Rehabil. Eng. 28, 461–467. doi: 10.1109/TNSRE.2020.2965029
Rajagopal, A., Kidziński, Ł, McGlaughlin, A. S., Hicks, J. L., Delp, S. L., and Schwartz, M. H. (2018). Estimating the effect size of surgery to improve walking in children with cerebral palsy from retrospective observational clinical data. Sci. Rep. 8:16344. doi: 10.1038/s41598-018-33962-2
Robinson, R., Herzog, W., and Nigg, B. (1987). Use of force platform variables to quantify the effects of chiropractic manipulation on gait symmetry. J. Manipulative Physiol. Ther. 10, 172–176.
Rosenbaum, P., Paneth, N., Leviton, A., Goldstein, M., Bax, M., Damiano, D., et al. (2007). A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child Neurol. Suppl. 109, 8–14. doi: 10.1111/j.1469-8749.2007.tb12610.x
Rossi, S., Colazza, A., Petrarca, M., Castelli, E., Cappa, P., and Krebs, H. (2013). Feasibility study of a wearable exoskeleton for children: Is the gait altered by adding masses on lower limbs? PLoS One 8:e73139. doi: 10.1371/journal.pone.0073139
Russell Esposito, E., Schmidtbauer, K., and Wilken, J. (2018). Experimental comparisons of passive and powered ankle-foot orthoses in individuals with limb reconstruction. J. Neuroeng. Rehabil. 15:111. doi: 10.1186/s12984-018-0455-y
Sanger, T., Chen, D., Delgado, M., Gaebler-Spira, D., Hallett, M., Mink, J., et al. (2006). Definition and classification of negative motor signs in childhood. Pediatrics 118, 2159–2167. doi: 10.1542/peds.2005-3016
Schwartz, M., Rozumalski, A., and Steele, K. (2016). Dynamic motor control is associated with treatment outcomes for children with cerebral palsy. Dev. Med. Child Neurol. 58, 1139–1145. doi: 10.1111/dmcn.13126
Smania, N., Gandolfi, M., Marconi, V., Calanca, A., Geroin, C., Piazza, S., et al. (2012). Applicability of a new robotic walking aid in a patient with cerebral palsy. Case report. Eur. J. Phys. Rehabil. Med. 48, 147–153.
Sutherland, D. (1997). The development of mature gait. Gait Posture 6, 163–170. doi: 10.1016/S0966-6362(97)00029-5
Takahashi, K., Mutsuzaki, H., Mataki, Y., Yoshikawa, K., Matsuda, M., Enomoto, K., et al. (2018). Safety and immediate effect of gait training using a Hybrid assistive limb in patients with cerebral palsy. J. Phys. Ther. Sci. 30, 1009–1013. doi: 10.1589/jpts.30.1009
Thurston, M., Kulmala, J. P., Nurminen, J., and Avela, J. (2021). Beyond orthoses: Using an exosuit to enhance the walking pattern of patients with unilateral Cerebral Palsy. Gait Posture 90, 271–273. doi: 10.1016/j.gaitpost.2021.09.141
Keywords: robotic-assisted gait training, exoskeleton, cerebral palsy, six-minute walk test, gait
Citation: Chmara P, Brazevic S, Jóźwiak M, Chen BP-J and Manikowska F (2025) Exoskeleton therapy in cerebral palsy: improved gait endurance without kinematic change. Front. Hum. Neurosci. 19:1644585. doi: 10.3389/fnhum.2025.1644585
Received: 10 June 2025; Accepted: 28 July 2025;
Published: 07 August 2025.
Edited by:
Rajat Emanuel Singh, Northwestern College, United StatesReviewed by:
Thais Raquel Martins Filippo, Universidade Federal de São Carlos, BrazilGrzegorz Sobota, The Jerzy Kukuczka Academy of Physical Education in Katowice, Poland
Copyright © 2025 Chmara, Brazevic, Jóźwiak, Chen and Manikowska. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Faustyna Manikowska, Zm9rYUBpbnRlcmlhLnBs