 Aaron Shield
Aaron Shield- Department of Speech Pathology and Audiology, Miami University, Oxford, OH, United States
Introduction: It is often assumed that sign language may be a more accessible alternative to speech for autistic children who have minimally expressive spoken language. However, this hypothesis remains largely untested in children exposed to both modalities from birth. This case series describes the developmental, cognitive, and language profiles of seven hearing autistic children of Deaf parents (CODAs) with native exposure to American Sign Language (ASL) and English.
Methods: Standardized assessments of receptive language, nonverbal cognition, and autism characteristics were collected alongside observational and parent-report data.
Results: Results revealed substantial individual variation: some children showed delays in both ASL and English; others showed slightly better ASL comprehension; and still others were clearly dominant in English, despite early access to ASL. Notably, no child demonstrated a consistent sign-language advantage.
Discussion: These findings challenge the assumption that sign is inherently more accessible to autistic children and highlight the need for individualized, modality-sensitive assessment. This study provides the first in-depth look at bimodal bilingualism in autism, offering a novel perspective on bilingual language acquisition in autism.
Introduction
The question of whether exposure to more than one language presents challenges or benefits for autistic children has received increasing scientific attention over the past decades. Historically, clinicians and educators often advised families to limit autistic children to a single language, fearing that bilingual exposure might confuse the child or exacerbate language delays (Kay-Raining Bird et al., 2012; Kremer-Sadlik, 2005; Yu, 2013). However, these recommendations were largely speculative and not grounded in empirical data.
A systematic review of eight studies on the language development of bilingual autistic children concluded that bilingualism does not negatively affect language outcomes (Drysdale et al., 2015). Across the 182 children included in the review, bilingual-exposed autistic children had similar language outcomes as monolingual autistic peers. One study within the review (Valicenti-McDermott et al., 2013) found that bilingual toddlers with autism were more likely than their monolingual peers to vocalize and use gestures—behaviors foundational to language acquisition and social engagement. Despite these findings, three of the studies reviewed reported that parents had been advised by professionals not to use more than one language with their autistic children, highlighting a continued disconnect between evidence and clinical practice.
Further support for the safety—and potential benefits—of bilingualism in autism comes from Beauchamp and MacLeod (2017), who concluded that bilingual exposure does not harm autistic children's language development and may actually support their socio-communicative abilities. Other, more recent studies have found that bilingualism neither impedes nor enhances linguistic (pronoun use) or cognitive (theory of mind) outcomes in bilingual-exposed autistic children (Meir and Novogrodsky, 2019). Other recent work has found that bilingual-exposed autistic children outperform monolingual autistic children on theory of mind and executive function tasks (Peristeri et al., 2021, 2024), suggesting that bilingualism may confer specific cognitive benefits on autistic children.
Taken together, these findings strongly support the conclusion that bilingualism does not hinder—and may even benefit—autistic children's development. Bilingual autistic children demonstrate equal or better outcomes in language, gesture use, social engagement, and ToM performance compared to monolingual autistic peers.
To date nearly all of this work has focused on unimodal bilingualism (i.e., two spoken languages). Little is known about the intersection of bimodal bilingualism (exposure to a signed language and a spoken language) with autism.
Bimodal bilingualism
Bimodal bilingualism differs fundamentally from traditional spoken-language bilingualism in that the two languages are produced and perceived through different modalities: the visual-gestural modality for sign and the vocal-auditory modality for speech. Bimodal bilinguals acquire sign and spoken language milestones on a timeline comparable to monolingual peers in each modality (van den Bogaerde, 2000; Petitto et al., 2001). Studies have shown that while some bimodal bilinguals develop native-like proficiency in both ASL and English, others exhibit dominance in one language over the other (Petitto et al., 2001; Lillo-Martin et al., 2014). Speech tends to become dominant as bimodal bilinguals mature, especially when English is reinforced through education and peer interactions, even if ASL is the primary home language (Petitto et al., 2001; Emmorey et al., 2013).
Moreover, bimodal bilingualism has been linked to certain cognitive benefits, especially in visual-spatial skills which benefit from exposure to a signed language, such as generating and transforming mental images (Emmorey et al., 1993) and completing spatial arrays (Keehner and Gathercole, 2007). However, bimodal bilingualism does not confer the same executive function advantages sometimes observed in unimodal bilinguals, likely because simultaneous production reduces the need for inhibitory control (Emmorey et al., 2008a). Because the articulatory and perceptual systems do not compete for processing resources, bimodal bilinguals sometimes produce elements of both languages simultaneously in a phenomenon known as code-blending (Emmorey et al., 2008b; Petitto et al., 2001). This suggests that bimodal bilinguals develop two distinct but interconnected language systems, capable of both independent and coordinated use.
In sum, the existing literature paints a picture of linguistically and cognitively robust development in typical bimodal bilinguals. These children successfully acquire two languages without confusion or delay, often with high degrees of flexibility and cross-modal coordination. However, the specific profile of language use—and which language becomes dominant—varies based on the input environment and social context. This growing body of research provides a foundation for comparison with atypical development in bimodal bilinguals, such as those with autism, whose social-communicative differences may interact with the demands of bilingualism and bimodal processing in complex ways.
Bimodal bilingual exposure in autistic children
To our knowledge, there is only one published study examining language development in a bimodal bilingual child with autism (Shield et al., 2020), and that study only documented the child's ASL development, not his spoken language development. The authors tracked the child's articulation of signs over a ten-year span (from 4;11 to 14;11) and showed that his articulation of handshape, location, and movement of signs improved over time, yet he showed a persistent pattern of reversing the direction of his palm while signing. This unusual pattern is thought to be a manifestation of imitation differences which then result in signs being articulated with a reversed palm orientation—a pattern that has been found in numerous deaf, ASL-exposed autistic children (Shield and Meier, 2012). However, since the authors did not analyze this child's spoken language development, there are currently no published reports of the bimodal-bilingual development of any autistic children.
Why study bimodal bilinguals with autism?
This population—hearing autistic children with native exposure to both ASL and English—is virtually absent from the scientific literature. Yet it offers a unique opportunity to test hypotheses and clinical assumptions about how autism interacts with language modality. It is often suggested—by clinicians, educators, and caregivers—that sign language may be more accessible to autistic children than spoken language, especially for those with limited expressive speech. Indeed, hypotheses advanced in the literature about a possible sign advantage for learners with developmental disabilities include:
1) Increased iconicity in sign language may scaffold children's vocabulary acquisition (Konstantareas et al., 1982);
2) A preference for visual over auditory stimuli (Lovaas and Schreibman, 1971; Lovaas et al., 1971; Pronovost et al., 1966; Rincover and Koegel, 1975; Salvin et al., 1977) may make signs preferable to words for some learners;
3) The unimodal nature of sign (mapping of visual linguistic symbols to objects) compared to the cross-modal nature of speech (mapping of auditory linguistic symbols to visually-perceived objects) may facilitate the learning of labels in children for whom sensory integration is at issue (Fulwiler and Fouts, 1976; Rogers and Ozonoff, 2005; Webster et al., 1973);
4) Manual gestures are more easily prompted and reinforced through touch than words, since the articulators (e.g., hands) are external (Stull et al., 1979);
5) The relatively slow rate of signing compared to speech (Klima and Bellugi, 1979) could allow learners more processing time;
6) Signs can be held in a static position, allowing for additional processing time, while speech sounds cannot be held static for any significant time without losing intelligibility (Jordan, 1990).
These hypothesized advantages have led researchers to ask whether exposing autistic and intellectually disabled children to signs could facilitate their speech development. Indeed, there is a large literature from the 1970s and 1980s in which autistic children were exposed to signs as an alternative or in addition to speech, with some success. Some studies found that participating in simultaneous sign and speech training led to a benefit to oral language skills in autistic children (e.g., Carr, 1979; Fulwiler and Fouts, 1976; Layton and Baker, 1981; Salvin et al., 1977; Schaeffer, 1980) or to some functional use of signs to communicate (Bonvillian et al., 1981). However, these interventions did not consist of exposure to a full human signed language such as American Sign Language (ASL), rather consisting of mostly single signs. Thus, the proposition that a signed language (rather than a simplified system of single signs as an alternative to or in addition to words) may be more accessible to some autistic children than a spoken language remains largely untested in the scientific literature.
This case series represents a first step toward answering that question by examining a rare but theoretically important population: hearing autistic children born to Deaf parents. These children—commonly referred to as CODAs (Children of Deaf Adults)—grow up in bimodal bilingual environments, acquiring ASL at home and spoken English in the surrounding community. They thus receive early and rich input in both modalities. As such, they offer a unique opportunity to ask whether a signed language is, in fact, more accessible than a spoken language for (some) autistic children when both are equally available from birth. We describe the developmental and language profiles of seven autistic bimodal bilingual children, all of whom were exposed to both ASL and English from birth. Although we offer details on expressive language whenever possible, our analysis focuses particularly on receptive language–at least in terms of formal assessments. The motivation for this choice is that measures of comprehension are more likely to accurately reflect the actual competence of autistic children, since expressive language can be complicated by difficulties with motor planning, recall, retrieval, and execution.
Research aims
This study addresses two related aims:
1. To document the receptive language profiles of autistic bimodal bilinguals exposed from birth to both ASL and English.
2. To determine whether there is evidence that ASL may be more accessible than spoken English for these children.
By systematically documenting each child's developmental history, standardized test scores, and autism characteristics, this study provides a first-of-its-kind empirical look at bimodal bilingualism in autism.
Methods
Participants
This study draws on data from a nationwide project in the United States investigating language, cognition, and social development in autistic children born to Deaf parents. Several previous papers have described various aspects of this population (e.g., Shield and Meier, 2012; Shield et al., 2015, 2016, 2017a,b), and several papers have included some of the participants described herein as part of the exploration of the effects of autism on ASL development (e.g., Shield et al., 2020). However, previous studies have not sought to compare the spoken language and signed language skills of these children, nor have they focused on the hearing children in the sample, as nearly all of the children in these studies were themselves deaf.
In the current study, all participants were hearing children of at least one Deaf parent and full, native exposure to ASL (n = 7; age range: 5;3-14;11). Children were recruited using social media, parent networks, and community organizations across the United States. Institutional Review Boards approved the research and all parents granted written informed consent prior to participation. See Table 1 for an overview of child characteristics and measures administered.
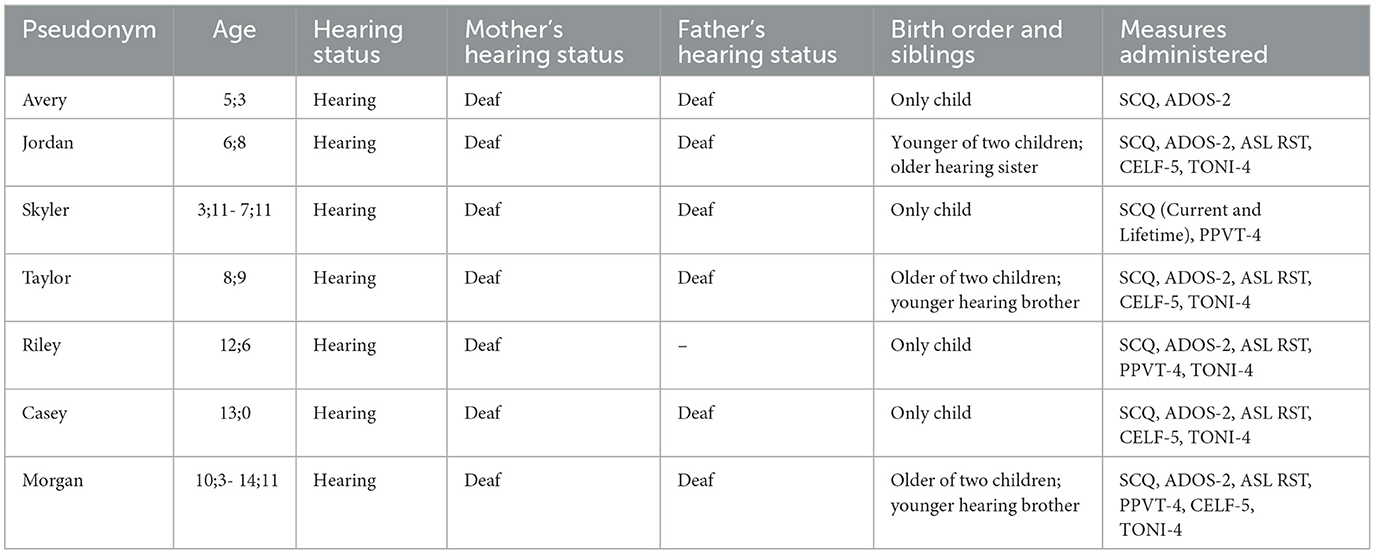
Table 1. Participant characteristics and measures administered.
Measures
Autism diagnosis
Autism diagnoses were confirmed either through direct assessment, parent-report screeners, or both. The Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012) was administered by a research-reliable clinician fluent in ASL to six of the seven children.
In addition, all caregivers (n = 7) completed the Social Communication Questionnaire (SCQ; Rutter et al., 2003), a validated ASD screener designed to assess social communication, play, and repetitive behaviors. A score of 15 or greater is commonly considered to be indicative of symptoms consistent with autism.
Nonverbal cognitive ability
Test of Nonverbal Intelligence – Fourth Edition (TONI-4). The Test of Nonverbal Intelligence, Fourth Edition (TONI-4; Brown et al., 2010) is a standardized, language-free measure of general intelligence and problem-solving ability. Designed for individuals aged 6 to 89 years, the TONI-4 assesses abstract reasoning using a series of visual analogies and pattern completion tasks. It requires no spoken, signed, or written language, making it especially useful for evaluating cognitive abilities in individuals with speech, language, hearing, or motor impairments. The test yields a standard score with a mean of 100 and a standard deviation of 15, and is commonly used in clinical, educational, and research settings to estimate nonverbal IQ.
ASL comprehension
ASL comprehension was assessed using the ASL Receptive Skills Test (ASL RST; Enns et al., 2013). The ASL RST assesses core grammatical structures in ASL and provides norm-referenced scores based on a large sample of deaf children exposed to ASL in early childhood (77 native signers of Deaf parents and 126 non-native signers with early ASL exposure). The test requires no expressive language and yields both standard scores (mean of 100; standard deviation of 15) and age equivalents for ASL comprehension.
English comprehension
Receptive spoken language competence was assessed using either the Clinical Evaluation of Language Fundamentals-Fifth Edition (CELF-5; Wiig et al., 2013) or the Peabody Picture Vocabulary Test-Fourth Edition (PPVT-4; Dunn and Dunn, 2007). Measures varied across participants due to the study being carried out over the course of a number of years and in a variety of settings; however, both assessments are widely believed to yield good estimates of English comprehension.
Clinical Evaluation of Language Fundamentals – Fifth Edition (CELF-5). The CELF-5 (Wiig et al., 2013) is a comprehensive, standardized assessment (mean = 100; standard deviation = 15) used to evaluate a wide range of receptive and expressive language skills in children and adolescents aged 5 to 21 years. It includes subtests that assess core language domains such as syntax, semantics, morphology, and memory for language, providing composite scores for Core Language, Receptive Language, Expressive Language, and Language Content. The CELF-5 is widely used in both clinical and research settings to diagnose language disorders and guide intervention planning. In this study, the subtests of the Receptive Language Index (RLI) were administered in order to yield an estimate of participants' English language comprehension.
Peabody Picture Vocabulary Test – Fourth Edition (PPVT-4). The PPVT-4 (Dunn and Dunn, 2007) is a norm-referenced, untimed test that measures receptive vocabulary for Standard American English. Participants are shown a series of images and asked to point to the picture that best represents a spoken word. The PPVT-4 is suitable for individuals aged 2 years 6 months through 90+ years, and is commonly used to assess language comprehension, estimate verbal ability, and support the identification of language impairments.The PPVT-4 yields standard scores with a mean of 100 and standard deviation of 15.
Other measures
When available, we report the results of prior evaluations when available, such as earlier medical or neuropsychological reports provided to us by children's parents.
Results
For this case series, we grouped the seven children into three categories based on their relative language abilities across modalities:
(1) children with significant language delay in both modalities,
(2) children with comparable delays across modalities, with a slight ASL advantage, and
(3) children who were clearly dominant in English despite early access to ASL.
Group 1: significant language delay in both modalities
Avery (age 5;3)
Avery, a hearing male born to two Deaf parents, was diagnosed with Pervasive Developmental Disorder–Not Otherwise Specified (PDD-NOS) at 18 months. A developmental evaluation conducted at 32 months documented persistent communication delays, motor challenges, and sensory preferences. Avery had passed a hearing screening and was receiving a comprehensive intervention program including speech-language therapy, occupational therapy, and applied behavior analysis (ABA) therapy three times per week. His mother reported gradual progress in therapy but noted that Avery could be aggressive and loud at home, and was often resistant to basic routines such as haircuts and tooth brushing. Although he did not initiate single words spontaneously, he occasionally repeated words when prompted. He was not yet independently using a fork but would feed himself if the utensil was placed in his hand. He showed limited engagement with toys, including non-verbal manipulatives, and preferred outdoor sensory activities.
At home, Avery demonstrated stronger responsiveness to his father and was able to interact playfully with a younger cousin. However, he appeared overwhelmed in group settings such as daycare, where he typically played alone and did not initiate peer interaction. Although he was showing improvement in joint attention and eye contact, he remained difficult to engage in structured developmental tasks. His physical exam at that time revealed intermittent eye contact and limited responsiveness to developmental probes. Recommendations included continued early intervention services, ABA therapy, and supplementary supports such as a sensory diet, hippotherapy, and aqua therapy.
At age 5;3, Avery's mother completed the SCQ, Current Form, obtaining a score of 15. The SCQ responses indicated significant deficits in communication and social interaction: Avery was not yet producing short phrases in speech or sign, exhibited echolalic behaviors (e.g., insisting others repeat words/signs), and frequently used others' hands as tools. He demonstrated limited play and social engagement—failing to initiate pretend or cooperative play, showing little interest in peers, and avoiding most social games. He did not use language to be friendly, imitate others spontaneously, or respond positively when approached by children. Notably, he showed a range of preserved or emerging social-emotional strengths, including spontaneous pointing, appropriate use of head gestures (e.g., nodding, shaking head), eye contact during communication, reciprocal smiling, and behaviors consistent with shared attention and empathy (e.g., showing objects, offering comfort, requesting help, sharing enjoyment). These strengths suggested the presence of some foundational social-affective skills despite his overall language and interactional delays.
The ADOS-2, Module 1 was administered by a trained examiner fluent in ASL and English. Avery received a total algorithm score of 19 (Social Affect = 17; Restricted and Repetitive Behavior = 2), with a calibrated severity score of 6, placing him in the moderate range for autism symptom severity. During the assessment, Avery demonstrated no spontaneous spoken or signed language and did not direct vocalizations to others. He did not respond to his name, initiate joint attention, or engage in social overtures beyond isolated instrumental behaviors. Although he gave a balloon to the examiner once, this was not part of a sustained social exchange. He followed a point on one occasion, suggesting emerging responsiveness to joint attention.
His eye contact was inconsistently modulated and not used effectively to regulate interaction. Avery showed minimal interest in toys or social routines, did not request help appropriately, and required significant effort from the examiner to remain engaged. Functional play was limited to cause-and-effect behaviors (e.g., pushing a car, using a dump truck), and no pretend play was observed. Although no sensory-seeking or repetitive behaviors were noted during the session, he did display hand and finger mannerisms that interfered with parts of the assessment. Notably, there were no signs of overactivity, anxiety, or aggression during the session.
An attempt was made by the study team to administer the TONI-4, the PPVT-4, and the ASL RST. However, Avery did not respond to any of the prompts or items, leading to discontinuation of each measure without yielding an interpretable score.
Taken together, Avery's developmental history and diagnostic assessment reflect a profile of significant social-communicative delay with limited expressive language in both modalities (sign and speech). His case is characterized by a clear divergence between his impaired expressive language and more intact—but still emerging—social-emotional signals, such as eye gaze, smiling, and shared affect. These features suggest a communicative profile in which the foundations for social connection are present but underutilized in linguistic contexts.
Skyler (ages 3;11-7;11)
Skyler, a hearing female born to two Deaf parents, was diagnosed with autism spectrum disorder (ASD) at age 3. At age 3;11, Skyler's mother completed the SCQ, Current Form, yielding a total score of 26, well above the threshold for autism risk. At that time, Skyler was able to speak in short phrases or sentences but could not maintain a back-and-forth conversation. Her speech was marked by echolalic patterns—saying the same phrases repetitively and in the same intonation—and by the presence of neologisms. Her mother also reported ritualistic behavior, such as strict adherence to routines, and instrumental use of others' hands, a common early sign of atypical communication.
Several restricted and repetitive behaviors were noted: preoccupying and intense sensory interests, a strong focus on parts of toys or objects, and unusual motor behaviors, including both hand/finger stereotypies and broader body movements. Skyler was described as carrying around preferred objects, a behavior she insisted on. Socially, she showed limited reciprocity: she did not spontaneously imitate others, point, or gesture meaningfully. She failed to exhibit behaviors such as shared attention (e.g., showing), offering to share, shared enjoyment, comforting others, or reciprocal smiling. She avoided eye contact when speaking, did not shake her head no, and did not join in cooperative or pretend play with peers. Nonetheless, she did demonstrate some foundational skills, including talking to others to be friendly, gesturing to get attention, and a normal range of facial expressions, suggesting that the building blocks of social communication were present but inconsistently deployed.
At age 4;2, Skyler was administered the PPVT-4, obtaining a raw score of 9, which corresponds to an estimated standard score of 50–55 (≤ 1st percentile). This placed her performance in the “extremely low” range, indicating severe receptive language impairment. Her receptive vocabulary was thus markedly delayed relative to age expectations, despite being exposed to both a signed and spoken language from birth.
By age 7;11, Skyler's mother completed the SCQ Lifetime Form. Many of the core features observed earlier persisted: Skyler continued to produce short phrases and sentences, without the capacity for sustained reciprocal conversation. Her language remained idiosyncratic, including invented words and repetitive speech patterns. She maintained a reliance on rituals and instrumental use of others' hands, and was still drawn to object parts and intense sensory experiences. However, new concerns emerged, including self-injurious behavior, not previously reported. She continued to insist on carrying objects with her.
Importantly, several positive changes were noted. While early social communication was minimal, by age 7;11 her mother reported that Skyler now spontaneously imitated, pointed, and gestured. She showed reciprocal smiling, shared objects to gain attention, and wanted to share enjoyment with others, although she still did not offer to share or comfort others when distressed. Her facial expressiveness remained intact, and she had begun to join in social and make-believe games, a developmental milestone that had been absent in toddlerhood. Though still selective in her peer engagement, she now appeared interested in unfamiliar same-age peers and responded positively when approached. She paid attention when others initiated interaction and was willing to engage in social games, though imaginative or cooperative play with peers remained limited. These gains suggest increasing social responsiveness and participation in structured and unstructured social contexts.
An attempt was made by the study team to administer the TONI-4, CELF-5, and the ASL RST. However, Skyler did not respond to any of the prompts or items, so the measures were discontinued. Thus, it is unclear how much ASL she was able to understand, or how her English receptive abilities had changed in the four years since our first visit. However, we did not observe any expressive language in either modality.
In summary, Skyler presents a case of early-diagnosed autism in a bimodal bilingual child with significant language delays—most notably in receptive vocabulary—and pronounced early social-communicative difficulties. Her expressive speech was echolalic and constrained, and her early engagement with others was marked by reduced eye contact, imitation, and shared attention. Nonetheless, her profile at age 7;11 demonstrates developmental growth in a number of key areas, including gesture use, pretend play, and social responsiveness.
Morgan (age 10;3-14;11)
Morgan, a hearing male born to two Deaf parents, was diagnosed with PDD-NOS at age 2;10 and has since exhibited a stable profile of global developmental delay with moderate autism severity. His developmental history is characterized by early and persistent delays in language, cognition, and adaptive functioning, along with the emergence of core features of ASD.
Morgan's earliest evaluations began at age 2;5. According to reports provided to us by his parents, on the Mullen Scales of Early Learning (MSEL; Mullen, 1995), he exhibited developmental levels well below age expectations: Gross Motor (t = 33, ~22 months), Problem Solving (t = 31, ~21 months), Receptive Language (t = 29, ~19 months), and Expressive Language (t = 36, ~22 months). Fine Motor was not scored. The Rossetti Infant-Toddler Language Scale (Rossetti, 2006) revealed receptive and expressive language scattered between the 15–21 month range. His performance on the Early Intervention Developmental Profile indicated relative strength in Socialization (27 months) but significant delays in Feeding (18 months) and Dressing/Hygiene (19 months).
At age 2;10, Morgan underwent a comprehensive psychological evaluation. On the Childhood Autism Rating Scale (CARS; Schopler et al., 1980), he received a score of 32.5, consistent with an autism diagnosis. Adaptive functioning measured by the Vineland Adaptive Behavior Scales yielded uniformly low scores: Communication = 69, Daily Living Skills = 69, Socialization = 69, Motor Skills = 72. The Bayley Scales of Infant Development, Second Edition (Bayley-II; Bayley, 1993) indicated a developmental quotient below 50, with an estimated mental age of 17 months.
At age 10;3, Morgan was administered the PPVT-4 and received a raw score of 65, corresponding to a standard score of 46 (1st percentile), indicating severe impairment in receptive spoken vocabulary. Shortly thereafter, at age 10;6, Morgan underwent an ADOS-2 (Module 1) assessment. His overall total was 15 (Social Affect = 7, Restricted and Repetitive Behaviors = 8), with a calibrated severity score of 6, indicating moderate autism severity.
During the ADOS-2, Morgan used a mix of short spoken phrases and ASL signs. Examples of spontaneous spoken language produced were: what's that, careful, of course you can, drum, no wait, more, no please, it's okay, again, no I can't, yes of course, all done work, and have some. He echoed words and phrases regularly, producing echoes from TV, and frequently produced stereotyped phrases, including sleep well, of course you can, and yes of course. He also produced some spontaneous single signs such as MORE, AGAIN, SCARED, and FLOWER, as well as code-blends in which English words and ASL signs were produced at the same time or in very close proximity. These included really/TRUE, day/DAY, somewhere/WHERE, people/PEOPLE, yeah/YES, Toy Story/TOY STORY, soon/SOON, watch Toy Story/WATCH TOY STORY, and wait/WAIT. He also produced one code-switch, responding with the ASL sign YES to the examiner's question in English Do you see all the people? Finally, he produced one English phrase using ASL-like syntax, all done work.
Socially, Morgan's engagement was mixed. He showed some shared enjoyment, responded to name, followed gaze, and offered spontaneous joint attention, but was limited in giving, showing, and varied emotional expressiveness. His eye contact was poorly modulated and his interactions were at times one-sided. His overtures to the examiner were often slightly unusual and his responses to social cues were sometimes restricted or out of context. Functional and pretend play were observed, although not with imaginative extension or symbolic substitution.
Morgan's repetitive and sensory behaviors were prominent during the ADOS-2. He displayed frequent motor stereotypies, including rocking and flapping, unusual gestural mannerisms (“sign-like” movements near his face), and intense interest in string and a slinky, which interfered with assessment tasks. He also showed mild anxiety, particularly in response to specific tasks or unfamiliar toys.
By adolescence (age 14;2-14;11), Morgan's language and cognitive profile remained significantly delayed across both modalities. On the TONI-4, he obtained a standard score of 86 (17th percentile), placing him in the low-average range of nonverbal intelligence. His CELF-5 Receptive Language Index, derived from subtests assessing word knowledge, paragraph comprehension, and semantic reasoning, yielded a standard score of 45 (below the 1st percentile). His ASL RST raw score was 12 (standard score <70; age equivalent 4;6), also indicative of significant impairment in the comprehension of ASL.
At age 14;2, his mother completed the SCQ Lifetime Form, reporting an SCQ score of 16. He was reported to speak in short sentences and maintain simple reciprocal conversations, though his speech included odd phrases, repetition, pronoun confusion, and socially inappropriate comments. He was noted to have friends, appropriate facial expressions, and no preoccupying interests or rituals. He exhibited motor mannerisms and whole-body movements, but no self-injury or compulsions. He did not spontaneously initiate interaction or use gesture, but he demonstrated several social-emotional strengths: reciprocal smiling, joint attention, sharing and showing, comforting others, pretend play, and cooperative games. While imaginative social play was limited, he did participate in structured peer activities like hide-and-seek and ball games.
In summary, Morgan is a hearing adolescent with ASD exposed to English and ASL from birth whose developmental history reflects severe and persistent impairments in both signed and spoken language, moderate cognitive delay, and a stable profile of autistic social and behavioral features. His expressive language is marked by repetitiveness and echolalia, as well as ASL-English code-blends. His receptive language remains significantly delayed in both languages despite early access to both ASL and English.
Group 2: comparable delays in sign and speech, with slight ASL advantage
Jordan (age 6;8)
Jordan, a hearing male born to two Deaf parents, was diagnosed with ASD at age 2;6 and received an additional diagnosis of attention-deficit/hyperactivity disorder (ADHD) at age 6. Jordan's mother completed multiple parent-report measures at the time of testing. On the SCQ, Lifetime Form, he obtained a score of 14, just below the typical threshold for autism risk, but clinical observations and the ADOS confirmed ongoing social-communicative challenges. According to the SCQ, Jordan could use short phrases and hold simple conversations, but also exhibited several behaviors consistent with ASD. These included repetitive or idiosyncratic language, insistence on rituals, the use of socially inappropriate statements, and a reliance on others' hands as tools. He had intense interests and was unusually drawn to sensory stimuli. His mother reported that he had no particular friends, engaged only intermittently with other children, and did not typically participate in imaginative or cooperative play. Nonetheless, Jordan demonstrated several important social strengths: he used spontaneous pointing and gestures, modulated head movements to indicate yes/no, looked others in the face during conversation, and responded to social overtures with reciprocal smiling. He showed things to others to share attention, expressed shared enjoyment, and made efforts to get others' attention through words or gestures.
The ADOS-2, Module 3, was administered by a trained examiner fluent in ASL and English. Jordan received a total algorithm score of 15 (Social Affect = 14, Restricted and Repetitive Behavior = 1), and a calibrated severity score of 9, indicating high severity of autism-related symptoms for his age and language level. His expressive spoken language was notable for relatively complex utterances, including some multi-clause sentences. However, his speech was slow and halting, and his prosody was atypical. He demonstrated occasional echolalia and used language in somewhat repetitive or formal ways. Although he provided reasonable accounts of routine events and occasionally offered information, his spontaneous contributions were often limited to personal interests, and he rarely asked questions or showed reciprocal curiosity.
Jordan demonstrated reduced conversational reciprocity, often following his own train of thought rather than engaging in mutual exchange. His gestures were limited and tended to occur only during structured tasks. Eye contact was inconsistently modulated and did not effectively support social engagement. Although he showed fleeting enjoyment in a single interaction, he generally lacked insight into others' emotions or social roles, and his responses were at times restricted or odd. His attempts to direct the examiner's attention were often tied to a specific interest—in this case, asking the examiner to read a book aloud multiple times. He demonstrated some reciprocal social communication, but it was reduced in both frequency and contextual diversity.
In terms of play and restricted interests, Jordan displayed some imaginative capacity, demonstrated by pretend behavior (e.g., declaring “I'm a friendly dinosaur”), though this was context-bound and limited in scope. No unusual sensory interests, repetitive behaviors, compulsions, or signs of anxiety or agitation were observed during the session. He remained seated and regulated throughout the assessment, with no evidence of aggression, overactivity, or emotional dysregulation.
On the TONI-4, Jordan obtained a standard score of 120, placing him in the 91st percentile for his age and indicating above-average nonverbal intelligence. Despite this cognitive strength, his receptive language scores were well below average in both modalities. On the ASL RST, he earned a raw score of 8, corresponding to a standard score of 85—within the low average range. In contrast, his comprehension of spoken English, measured by the Receptive Language Index of the CELF-5, yielded a standard score of 73 (4th percentile), reflecting significantly impaired spoken language comprehension relative to age peers.
In sum, Jordan presents a complex profile: a cognitively capable child with substantial social-communicative challenges, atypical prosody and pragmatic language use, and receptive language delays in both ASL and English, which are slightly more pronounced in English.
Riley (age 12;6)
Riley, a hearing male born to a single Deaf mother, was diagnosed with autistic disorder at age 3. At the time of evaluation at 12;6, Riley demonstrated a profile consistent with moderate to severe autism. His mother completed the SCQ Lifetime Form, yielding a total score of 19. According to her responses, Riley was able to speak or sign in short phrases and hold basic reciprocal conversations, but frequently used unusual or repetitive language. He invented neologisms, engaged in ritualistic behaviors (especially involving his train collection), and used others' hands instrumentally. He showed strong preoccupying interests, particularly in trains, and was fascinated with the parts of objects, such as wheels or small mechanical components. Riley also displayed sensory-seeking behaviors and engaged in pacing, though no hand stereotypies or self-injury were reported.
His social behavior was uneven. He did not have close friends and was largely uninterested in peers, typically not responding positively when approached by unfamiliar children. Nonetheless, Riley did engage in social behaviors with familiar adults: he spoke/signaled to be friendly, used gestures and pointing, nodded and shook his head to communicate, and showed objects to others to gain their attention. He spontaneously copied actions, used facial expressions (albeit inconsistently), and occasionally offered to share or engage. However, reciprocal smiling, comforting others, and spontaneous make-believe or cooperative play were largely absent.
The ADOS-2, Module 3 was administered by a trained examiner fluent in ASL and English. Riley obtained a total algorithm score of 20 (Social Affect = 14; Restricted and Repetitive Behaviors = 6), with a calibrated severity score of 10, indicating high severity of autism symptoms. He used relatively complex spoken language, occasionally producing multi-clause utterances, but his speech was marked by flat intonation and frequent stereotyped or echolalic phrases. He produced thirteen echoed utterances, which were partial or total echoes of the examiner's previous utterance. He also produced a number of stereotyped/scripted phrases, often having to do with the Thomas the Tank Engine series (one of his intense, restricted interests). When asked What do you like doing that makes you feel happy, he responded I'm cheerful like Percy (a reference to Percy the Small Engine); when asked What makes you mad, he replied Diesel tells his lies (a reference to the “Devious” Diesel engine character). He produced one code-blend: the ASL lexical sign (TWELVE) was produced spontaneously in response to a question in English (how old are you?) and in conjunction with the English word twelve.
Riley spontaneously offered personal information (e.g., about Disney), asked the examiner questions, and reported on past events not related to his preoccupations—demonstrating genuine, if limited, narrative and reciprocal language use. He used descriptive gestures (e.g., gestures for “fly,” “digest”) during conversation and structured tasks.
With regard to morphosyntax, Riley produced several English grammatical errors. He made one irregular verb tense error (flied instead of flew) and two auxiliary verb tense errors (Have you been gone to Walt Disney World before; have you been seen Disney Junior live on stage). He also used the present tense when talking about a past experience, which could also be considered a tense error on an irregular verb (I ride on Casey Junior). He made an error with a preposition in the sentence the boulder is chasing to Percy; the verb chase does not take a preposition before its object. Finally, he added an [s] to the end of the word “myself” in the sentence I will change myselfs in response to the question What would you change about yourself?
Socially, Riley exhibited poorly modulated eye contact and minimal facial expression directed at the examiner. He displayed little shared enjoyment, although he showed visible pleasure when speaking about his interests. His social overtures were often inappropriate or one-sided, and his responses to social cues were frequently restricted or odd. Nonetheless, he demonstrated some understanding of emotion in others and attempted to maintain interaction through topic continuation and visual bids (e.g., pointing and saying “look”).
Riley's restricted and repetitive behaviors were salient during the ADOS-2. He displayed strong sensory interests (e.g., peering intently at the tops of objects), persistent references to his train-related interests, and ritualistic patterns that were evident in his conversational content and object handling. No compulsions, motor stereotypies, or self-injury were observed during the assessment, and Riley was calm, compliant, and not anxious or disruptive.
On the TONI-4, Riley obtained a standard score of approximately 69 (2nd−3rd percentile), placing him in the low-average range. In terms of receptive language, Riley's profile showed a slight asymmetry across modalities. On the PPVT-4, he obtained a standard score of 72, indicating significant delay in receptive spoken vocabulary (≈3rd percentile). On the vocabulary check portion of the ASL RST, Riley produced fourteen of twenty lexical signs and fingerspelled four others. He was able to select the correct picture for the six signs that he did not produce, indicating that he recognized the signs. On the comprehension portion, he earned a raw score of 17 (out of 34 total items), which corresponded to a standard score of 79. According to the age norms provided in the ASL RST manual, his ASL comprehension was equivalent to that of a typical five-year-old.
In summary, Riley is a bimodal bilingual boy with ASD who presents with moderate to high symptom severity, low-average cognitive functioning, significantly delayed receptive language in both ASL and English, morphosyntactic difficulties in expressive English, circumscribed interests, and marked impairments in social reciprocity and imaginative play. Despite limited insight into typical peer interactions, Riley showed strengths in verbal labeling, routine-based conversation, and retained a desire to engage with others, particularly around his interests.
Group 3: English-dominant profiles
Taylor (age 8;9)
Taylor, a hearing female born to two Deaf parents, was diagnosed with ASD at 30 months of age. Her behavioral profile—as documented in the SCQ, Lifetime Form (score of 26)—reflected a high degree of autistic traits across social, communicative, and behavioral domains. According to her mother's SCQ responses, Taylor spoke in phrases or full sentences and was capable of engaging in conversational turn-taking, but her expressive language was idiosyncratic: she frequently used odd phrases, inappropriate statements, and neologisms. Socially, Taylor demonstrated both limitations and emerging strengths. She did not use appropriate facial expressions, and had difficulty with basic nonverbal behaviors such as pointing, head nodding, eye contact, and reciprocal smiling. She did not comfort others or offer to share, nor did she engage in cooperative or pretend play with peers. She lacked close friendships and did not respond positively to other children her age. Nonetheless, she did spontaneously imitate, use gestures, and show things to others as a way of initiating joint attention, suggesting an emerging awareness of and desire to share experiences with others.
The ADOS-2, Module 3, was administered by a trained examiner fluent in ASL and English. Her overall algorithm score was 8 (Social Affect = 7; RRB = 1), with a calibrated severity score of 5, indicating a moderate level of autism symptoms. During the assessment, Taylor used relatively complex speech with some grammatical errors, and her prosody was slightly atypical, described as flat with limited pitch variation. While she did not demonstrate echolalia or significantly restricted language, her use of language included stereotyped or formal expressions. Despite these mild pragmatic anomalies, she was able to offer information, ask questions, and build on conversation initiated by the examiner, demonstrating fluid and flexible use of language in a structured setting.
Taylor's social communication behaviors were uneven. She showed some awareness of others' emotions, including appropriate emotional labeling and contextual responses. She also displayed creative pretend play, such as inventing a story involving dinosaurs and naming objects with imaginative labels (e.g., “Mrs. Ponytail”). However, her eye contact remained poorly modulated, and her facial expressions were limited. She exhibited occasional unusual sensory interests, such as spinning a disk, but no repetitive behaviors, rituals, or motor mannerisms were observed. She remained engaged and well-regulated throughout the session, with no signs of overactivity, aggression, or anxiety.
Taylor's nonverbal intelligence, measured by the TONI-4, was a notable strength: she obtained a standard score of 129, placing her in the 97th percentile for her age. Her spoken English receptive language, measured using the Receptive Language Index of the CELF-5, was in the average range (standard score = 96, 39th percentile), while her comprehension of ASL on the ASL RST yielded a raw score of 14, corresponding to a standard score of 85 (low average range). Thus, although her English was somewhat stronger, Taylor's receptive language in both modalities fell within the broadly average range.
In summary, Taylor is a cognitively able bimodal bilingual girl with ASD who demonstrates average to low-average receptive language in both sign and speech, with somewhat higher scores in English.
Casey (age 13;0)
Casey, a 13-year-old hearing male born to two Deaf parents, was diagnosed with PDD-NOS at 30 months. His parents report using a combination of ASL, spoken English, and Total Communication strategies at home. Interestingly, Casey's mother reported on his screening form that he had difficulty understanding or using ASL, even though it had been the primary language used in the home since birth. In contrast, she described him as a fluent English speaker, indicating an asymmetrical bilingual profile that favors the spoken modality.
Casey's mother completed the SCQ Lifetime Form, yielding a score of 21. She reported that Casey was able to engage in reciprocal conversations and did not demonstrate many of the hallmark features of autism, such as neologisms, pronoun errors, inappropriate statements, or instrumental use of others' hands. He did not exhibit rituals, self-injury, or preoccupying interests, though she did note a tendency to focus on the parts of objects and intensely pursue certain interests, both of which are sometimes associated with ASD. Socially, Casey had friends, showed appropriate facial expressions, and was generally communicative. However, his mother also noted that as a young child, his social delays included limited spontaneous pointing, poor facial engagement, lack of shared enjoyment, and minimal imaginative or cooperative play. Although he responded positively to peers, he did not initiate typical social behaviors or respond to caregivers' bids for interaction at that age.
Casey's ADOS-2 (Module 3) was administered at age 13;0. His total algorithm score was 7 (Social Affect = 6; RRB = 1), with a calibrated severity score of 4, placing him within the “Autism Spectrum” classification but at the low end of the severity range. His spoken language was grammatically correct and included some complex sentence structures, with occasional stereotyped phrasing and slightly atypical intonation described as flat or mechanical. He spontaneously offered personal information, reported on real-world events, and asked the examiner questions about their interests, showing intact narrative and reciprocal discourse skills. He also made use of descriptive and conventional gestures, such as pointing and miming actions.
In terms of social behavior, Casey demonstrated some difficulties with eye contact and facial expression. His gaze was described as poorly modulated, and while he did direct facial expressions to the examiner, these were limited in range. His nonverbal communicative behaviors (gesture, gaze, and facial expression) were less frequent or appropriately coordinated than expected for his age and language level. He displayed some spontaneous shared enjoyment and correct labeling of others' emotions, and he demonstrated insight into typical social relationships, including his own role within them. His social overtures were occasionally unusual, but he frequently attempted to engage the examiner and responded appropriately to social bids, resulting in a generally comfortable and fluid interaction.
No restricted or repetitive behaviors were observed during the ADOS-2 session. Casey showed no signs of sensory-seeking, compulsive behaviors, motor mannerisms, or intense preoccupations. He remained engaged, seated, and calm throughout the assessment, with no signs of agitation, anxiety, or behavioral dysregulation.
Casey's nonverbal intelligence, as measured by the TONI-4, was a significant strength: he obtained a standard score of 121, placing him in the 92nd percentile for his age. His spoken English receptive language was also strong, with a Receptive Language Index standard score of 112 on the CELF-5 (79th percentile). These results indicate above-average general reasoning skills and well-developed comprehension of spoken language.
In contrast, Casey's receptive skills in ASL were markedly weaker. On the ASL RST, he obtained a raw score of 17, corresponding to a standard score of 77, in the borderline range. Notably, in the ASL RST's vocabulary check—designed to assess recognition of basic signs—Casey was only able to produce 7 of the 20 target signs, failing to generate common signs such as car, ball, school, dog, book, and game. This stark difference between his performance in English and ASL suggests that Casey, despite early exposure, had not acquired functional receptive ASL proficiency, reinforcing his mother's concern and raising questions about modality-specific language access in autistic children exposed to signed language from birth.
Taken together, Casey presents as a cognitively able autistic adolescent with strong spoken language and social-cognitive skills, but a distinct modality-specific language profile. His limited ASL proficiency is especially striking given his native exposure to sign from birth, and stands in contrast to his age-appropriate (and even advanced) abilities in spoken English.
Synthesis of case series findings
The seven children in this case series, all hearing children of Deaf parents with lifelong exposure to both ASL and English, illustrate a range of language, cognitive, and social-communicative profiles within the broader context of autism. Despite shared access to bimodal linguistic input, outcomes varied considerably across individuals and modalities. Three children (Avery, Skyler, and Morgan) exhibited profound delays in both spoken and signed language, with minimal expressive language. Two children (Jordan and Riley) showed significantly impaired language in both modalities, but their ASL comprehension scores were slightly higher than their English scores. The final two children (Taylor and Casey) showed dominance in English over ASL, with Casey demonstrating the clearest disconnect between the two languages, with superior comprehension of English and marked impairment in ASL. Table 2 summarizes the participants' scores on standardized autism, nonverbal intelligence, ASL and English comprehension measures. Table 3 summarizes participants' overall language and developmental profile.
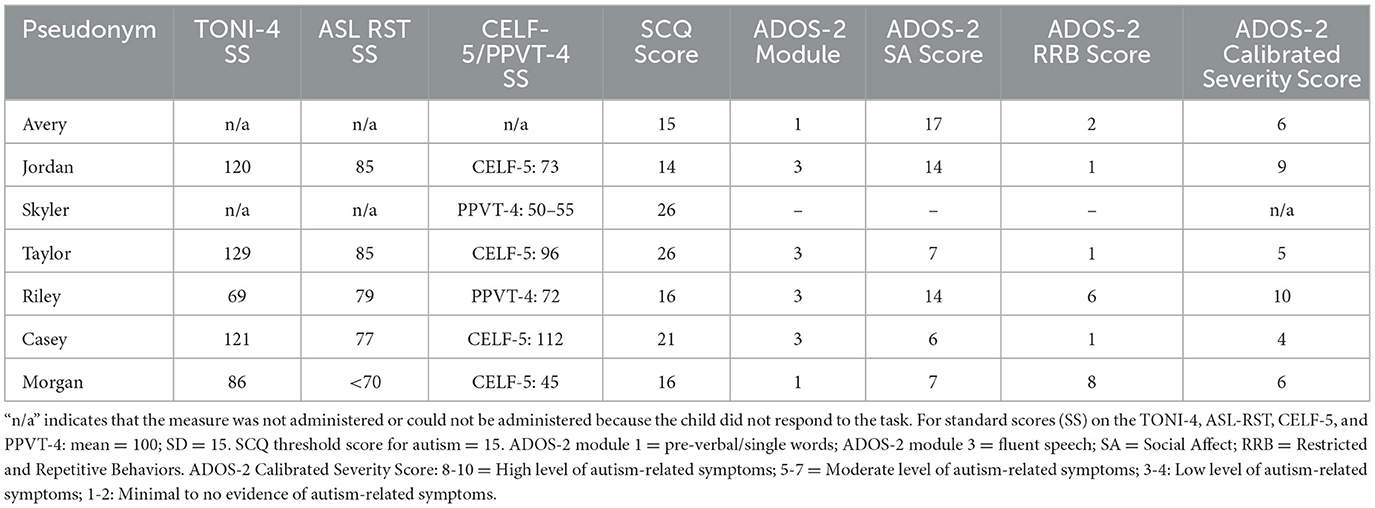
Table 2. Scores on standardized measures.
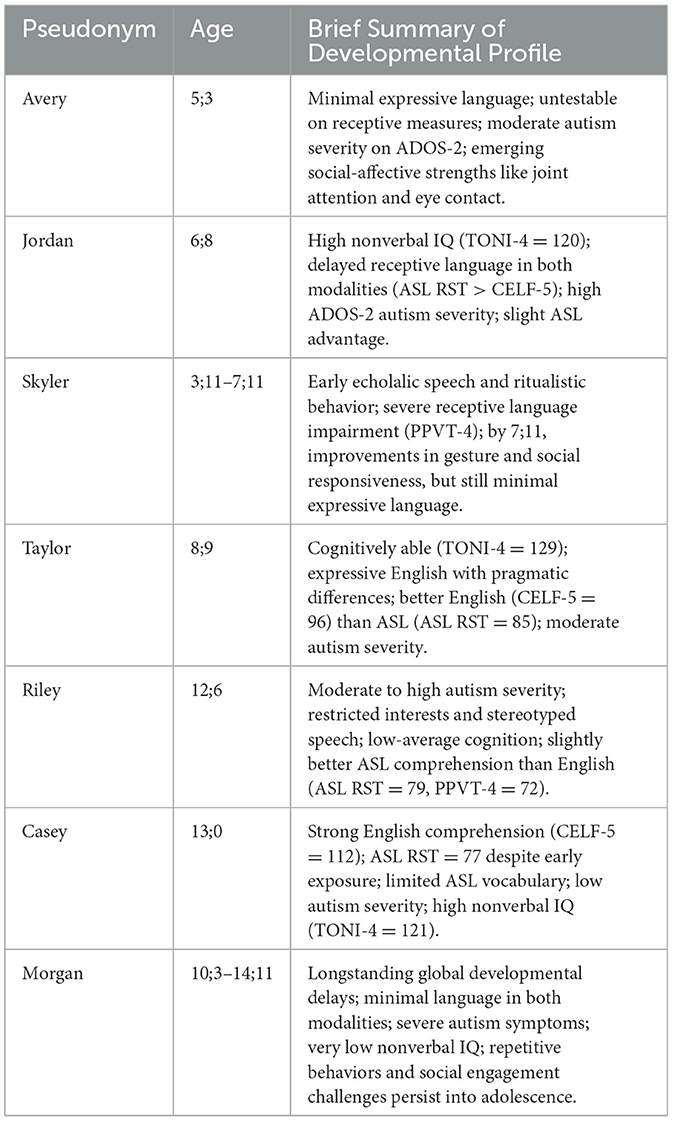
Table 3. Participant profiles and developmental summaries.
Discussion
This case series examined seven hearing children of Deaf parents (CODAs), all diagnosed with ASD and exposed to ASL and spoken English from birth. This group represents a uniquely under-documented and theoretically important population: bimodal bilingual autistic children with native, early, and sustained access to two languages across different modalities. Their profiles allow us to directly test assumptions about bilingualism in autism, particularly the widespread clinical belief that signed languages may be inherently more accessible than spoken languages.
We now return to the two guiding aims posed at the outset.
1. To document the receptive language profiles of bimodal bilinguals autistic children with early exposure to ASL and English.
2. To determine whether there is evidence that ASL is more accessible than spoken English for these children.
All seven children had access to fluent sign models in the home and opportunities for English exposure in the broader community. Despite this shared bimodal bilingual environment, their language profiles revealed substantial heterogeneity—not only in the degree of delay, but in the balance between modalities, the depth of receptive language development, and the broader social-communicative context in which language emerged.
Across the sample, three broad language profiles emerged:
1. Minimal language in both modalities: Three children (Avery, Skyler, and Morgan) demonstrated serious challenges with both modalities and delays in receptive language in both ASL and English. Their early histories included very limited expressive language and marked social-communicative difficulties. Their delayed receptive language, despite early and rich exposure, highlights that some autistic children with access to both signed and spoken language may nonetheless struggle to acquire either to age-expected levels.
2. Delayed language in both modalities, with possible ASL advantage: Two children (Jordan and Riley) showed delayed but roughly parallel receptive abilities in both ASL and English, with a possible but slight advantage in ASL comprehension. Although neither child was in the typical range in either ASL or English for a child their age, their standard scores were slightly higher on the ASL RST than on the CELF-5/PPVT-4 (12 points higher for Jordan and 7 points higher for Riley). More research is needed to confirm whether such a difference really indicates an advantage for sign, but these two children show that it is at least possible that ASL may be more accessible than English for some autistic children. However, our data indicate that any advantage for ASL is slight at best.
3. English-dominant profiles: Two children (Taylor and Casey) showed strong nonverbal cognitive scores and above-average spoken English comprehension, but significantly weaker ASL skills. Casey, in particular, had a CELF-5 receptive standard score of 112 and a TONI-4 score of 121, but failed to recognize or produce many basic ASL signs, scoring in the borderline range on the ASL RST (SS = 77), a 44-point difference. His mother's report also emphasized limited ability to use or understand ASL, despite being raised in a Deaf household where ASL was the primary language. For Taylor, the difference was not as stark, with an 11-point advantage in English comprehension over ASL comprehension. These profiles suggest that even when sign language is available from birth, autistic children may preferentially acquire spoken language—or may find sign less accessible due to modality differences, social-cultural factors, or challenges with the social-cognitive skills that are required for sign-language comprehension (e.g., eye contact, facial expressions, perspective-taking). This tendency of some codas to develop a preference for spoken language over sign is in line with previous research on typically-developing codas (Petitto et al., 2001; Emmorey et al., 2013).
The range of profiles observed in this study reflects both the diversity of autism and the complexity of language acquisition across modalities. Autistic children exhibit considerable heterogeneity in language development, with some acquiring age-appropriate skills and others remaining minimally verbal despite early access and intervention (Kjelgaard and Tager-Flusberg, 2001; Pickles et al., 2014; Tager-Flusberg and Kasari, 2013; Tek et al., 2014). While all children had early exposure to ASL and English, the degree to which they accessed, processed, and acquired each language varied widely. We attribute these differences to the innate linguistic capacities as well as the individual learning styles of each child. The finding that some children (e.g., Casey) acquired fluent or near-fluent spoken English but did not acquire basic receptive (or expressive) ASL skills challenges assumptions that Deaf-parented children will naturally acquire sign language, and is in line with prior work on typically-developing CODAs who demonstrate English dominance over ASL (Petitto et al., 2001; Emmorey et al., 2013). This result also underscores the fact that language input alone does not guarantee language acquisition, particularly in the context of autism. This has important implications for assessment and support: professionals should not assume that Deaf parents' use of ASL ensures their autistic child's sign fluency, nor that spoken English will be uniformly inaccessible. Instead, individualized language assessment across both modalities is critical, especially for children navigating two linguistic systems in different sensory channels. Professionals assessing bimodal bilingual autistic children should be knowledgeable about ASL and not assume parity across modalities.
A widely held clinical assumption is that sign may be more accessible than spoken language for autistic children, particularly those with limited expressive speech. However, this case series provides little support for that claim. Among the seven children studied, no consistent “sign advantage” emerged—despite all having early, rich exposure to ASL from Deaf parents. Only two children (Jordan and Riley) showed slightly stronger ASL comprehension, but even that advantage was modest. Two children (Taylor and Casey) demonstrated notably stronger performance in spoken English, including fluent comprehension and age-appropriate or above-average receptive language scores, despite reported difficulty with or disinterest in ASL. In contrast, several children (Avery, Skyler, Morgan) showed significant delays in both modalities, including minimal expressive signing despite native exposure. These findings suggest that for many autistic bimodal bilinguals, access alone is not sufficient for the development of sign language fluency, and that sign is not uniformly more accessible than speech. Indeed, the social skills needed to acquire a signed language (such as the ability to look at others' faces, make eye contact, understand facial expressions, and take the differing visual perspectives of others) may make the acquisition of sign particularly difficult for some autistic children. That said, given the variability observed in autism, it is still possible that manual signing systems (particularly simplified signing systems) may be an effective alternative means of communication for hearing autistic children, particularly those who struggle with speech due to oral-motor difficulties.
Novelty and contributions
This study makes several unique contributions. First, it provides the first known descriptions of bimodal bilingual autistic children raised from birth with access to ASL and English. We add to the growing literature on bilingual-exposed autistic children as well as to the literature on bimodal-bilingual children, complementing existing studies of typical development. Bimodal bilingualism differs substantially in nature from spoken language bilingualism: the two languages are perceived through different senses and produced using different articulators. As such, they rely on different cognitive and social resources and mechanisms. While the underlying difficulties associated with autism remain the same, each language modality places different emphasis on specific social skills. For example, while facial expressions produced during speech can lend nuance to the comprehension of spoken utterances, facial expressions also carry grammatical functions in signed languages. For autistic children with an aversion to face gaze, comprehension of signed utterances will be specifically impacted.
Second, our results challenge the presumption on the part of some clinicians that sign language may be inherently more accessible to autistic individuals than spoken language, or that sign-language training will necessarily succeed if speech remains out of reach for some autistic children. Sign language acquisition offers its own challenges: in addition to the universal obstacles of mastering a complicated linguistic system with its own phonology, morphology, and syntax, signed languages require learners to engage in joint attention, eye contact, visual perspective-taking, imitation, gesture, pointing, and facial expressions—all skills that are known areas of difficulty for autistic learners. These factors do not make sign learning impossible, but learners may struggle to acquire sign if one or more of these skills is impaired. Still, this fact should in no way be interpreted to mean that sign language should be withheld from deaf (or hearing) autistic children. Bimodal bilingual exposure is not harmful, and – in the case of deaf children – can ensure against the risk of language deprivation.
Third, our study documents substantial heterogeneity in outcomes, even within a relatively homogeneous input environment (hearing children of Deaf parents with early exposure to ASL and English). Clinicians should be sensitive to the specific linguistic, social, and cognitive profiles of children in choosing the best course of therapy and intervention. This work highlights that language modality does not override the core developmental differences associated with autism, and that early input—while critical—is not always sufficient for fluent bilingual development, especially in the context of neurodevelopmental differences.
Limitations and future directions
As a case series, this study is exploratory and descriptive. It includes a small number of participants and relies primarily on in-depth clinical, observational, and parent-report data. We focused on receptive language, but there are many questions that remain about bimodal bilingual's expressive abilities in ASL and English. Future work should more systematically explore if there are analogous or different expressive profiles in this population, incorporate longitudinal naturalistic observations, and compare autistic children with non-autistic bimodal bilingual peers.
Additionally, a few methodological limitations bear mentioning. First, we were not able to get measures for every child in both ASL and English. Two children (Avery and Skyler) did not respond to either receptive language measure, so it is unclear what their true abilities may be. Second, there was some variation in the English-language measure given, with some children receiving the PPVT-4 and others the CELF-5. Although both are standardized, the PPVT-4 is a measure of receptive vocabulary while the CELF-5 receptive language index assesses the child's ability to understand English morphosyntax and semantic relationships between words. The use of different measures for different children could have influenced our results, and future work should include multiple measures for a fuller picture of children's linguistic abilities.
Finally, while these children had full access to ASL and English, the quantity and quality of input in each modality may have varied—particularly in households using Total Communication or Sign Supported Speech. Future research should explore how input quality, parental language use, and social interactional context interact with autistic learning profiles to shape bilingual language development.
Conclusion
This case series offers the first detailed look at autistic hearing children exposed from birth to both ASL and English. It is thus the first detailed description of a novel research population, with the potential to inform and enrich our understanding of bilingualism in autism. Our results also show that sign is not universally more accessible than speech for autistic learners. Despite rich, early exposure to both languages, outcomes varied widely across children and modalities, likely due to individual differences in the cognitive and linguistic abilities of the children.
Ultimately, this study highlights the need for modality-sensitive, individualized approaches to assessment and intervention. Understanding how autistic children navigate language across modalities not only informs clinical best practice but also expands our theoretical models of bilingualism, language development, and neurodiversity.
Data availability statement
The datasets presented in this article are not readily available because of the sensitive nature of the participant information and the small size of the sample, which could compromise confidentiality. Participants are members of a small and identifiable population (hearing children of Deaf adults), and despite de-identification, there remains a risk of deductive disclosure. As such, data sharing is not possible under the terms of our ethical approval. Requests to access the datasets should be directed to Aaron Shield, c2hpZWxkYUBtaWFtaW9oLmVkdQ==.
Ethics statement
The studies involving humans were approved by Boston University Institutional Review Board (2471e) and Miami University Institutional Review Board (01375). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants‘ legal guardians/next of kin. Written informed consent was obtained from the minor(s)' legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
AS: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was supported by a grant from NIDCD (Grant #1F32 DC0011219) and an Advancing Academic-Research Careers (AARC) Award from the American Speech-Language-Hearing Association (ASHA).
Acknowledgments
The author would like to thank Helen Tager-Flusberg and Karen Emmorey for mentorship on the research projects that led to the production of this manuscript. The author thanks the children and families who participated in this research.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Gen AI was used in the creation of this manuscript. Portions of this manuscript were prepared with the assistance of OpenAI's ChatGPT. The author reviewed, edited, and takes full responsibility for the content of the final manuscript. No AI tools were used to generate, interpret, or analyze the study data.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bayley, N. (1993). Bayley Scales of Infant Development (2nd ed.). San Antonio, TX: Psychological Corporation.
Beauchamp, M. L., and MacLeod, A. A. N. (2017). Bilingualism in children with autism spectrum disorder: making evidence-based recommendations. Can. Psychol. 58, 250–262. doi: 10.1037/cap0000122
Bonvillian, J. D., Nelson, K. E., and Rhyne, J. M. (1981). Sign language and autism. J. Autism Dev. Disord. 11, 125–137. doi: 10.1007/BF01531345
Brown, L., Sherbenou, R. J., and Johnsen, S. K. (2010). Test of Nonverbal Intelligence (4th ed.). Austin, TX: Pro-Ed.
Carr, E. G. (1979). Teaching autistic children to use sign language: some research issues. J. Autism Dev. Disord. 9, 345–359. doi: 10.1007/BF01531444
Drysdale, H., van der Meer, L., and Kagohara, D. (2015). Children with autism spectrum disorder from bilingual families: a systematic review. Rev. J. Autism Dev. Disord. 2, 26–38. doi: 10.1007/s40489-014-0032-7
Dunn, L. M., and Dunn, D. M. (2007). Peabody Picture Vocabulary Test (4th ed.). Minneapolis, MN: Pearson Assessments. doi: 10.1037/t15144-000
Emmorey, K., Borinstein, H. B., Thompson, R., and Gollan, T. H. (2008a). Bimodal bilingualism. Bilingual. Lang. Cogn. 11, 43–61. doi: 10.1017/S1366728907003203
Emmorey, K., Kosslyn, S. M., and Bellugi, U. (1993). Visual imagery and visual-spatial language: enhanced imagery abilities in deaf and hearing ASL signers. Cognition 46, 139–181. doi: 10.1016/0010-0277(93)90017-P
Emmorey, K., Luk, G., Pyers, J. E., and Bialystok, E. (2008b). The source of enhanced cognitive control in bilinguals: evidence from bimodal bilinguals. Psychol. Sci. 19, 1201–1206. doi: 10.1111/j.1467-9280.2008.02224.x
Emmorey, K., Petrich, J. A. F., and Gollan, T. H. (2013). Bimodal bilingualism and the frequency-lag hypothesis. J. Deaf Stud. Deaf Educ. 18, 1–11. doi: 10.1093/deafed/ens034
Enns, C., Zimmer, K., and Domitrovich, S. (2013). ASL Receptive Skills Test. Winnipeg: Northern Signs Research, Inc.
Fulwiler, R. L., and Fouts, R. S. (1976). Acquisition of American sign language by a noncommunicating autistic child. J. Autism Child. Schizop. 6, 43–51. doi: 10.1007/BF01537941
Jordan, R. (1990). Me and you: a problem for autism. Proceedings of the Durham Conference on Autism: Experimental Psychology. Autism Research Unit, University of Sunderland, pp. 157–171.
Kay-Raining Bird, E., Lamond, E., and Holden, J. (2012). Survey of bilingualism in autism spectrum disorders: Bilingualism and autism: a survey study. Int. J. Lang. Commun. Disord. 47, 52–64. doi: 10.1111/j.1460-6984.2011.00071.x
Keehner, M., and Gathercole, S. E. (2007). Cognitive adaptations arising from nonnative experience of sign language in hearing adults. Memory Cogn. 35, 752–761. doi: 10.3758/BF03193312
Kjelgaard, M. M., and Tager-Flusberg, H. (2001). An investigation of language impairment in autism: Implications for genetic subgroups. Lang. Cogn. Proces. 16, 287–308. doi: 10.1080/01690960042000058
Klima, E. S., and Bellugi, U. (1979). The Signs of Language. Cambridge, MA: Harvard University Press.
Konstantareas, M. M., Oxman, J., and Webster, C. D. (1982). Simultaneous communication with autistic and other severely dysfunctional nonverbal children. J. Commun. Disord. 10, 267–282. doi: 10.1016/0021-9924(77)90006-5
Kremer-Sadlik, T. (2005). “To be or not to be bilingual: Autistic children from multilingual families,” in ISB4: Proceedings of the 4th International Symposium on Bilingualism eds. J. Cohen, K. T. McAlister, K. Rolstad, and J. MacSwan (Massachusetts: Cascadilla Press), pp. 1225–1234.
Layton, T. L., and Baker, B. L. (1981). Development of semantic–syntactic relations in an autistic child. J. Autism Dev. Disord. 11, 385–399. doi: 10.1007/BF01531614
Lillo-Martin, D., de Quadros, R. M., Chen Pichler, D., and Fieldsteel, Z. (2014). Language choice in bimodal bilingual development. Front. Psychol. 5:1163. doi: 10.3389/fpsyg.2014.01163
Lord, C., Rutter, M., DiLavore, P. C., Risi, S., Gotham, K., and Bishop, S. L. (2012). Autism Diagnostic Observation Schedule, Second Edition (ADOS-2). Torrance, CA: Western Psychological Services.
Lovaas, O. I., and Schreibman, L. (1971). Stimulus overselectivity of autistic children in a two-stimulus situation. Behav. Res. Therapy 9, 305–309. doi: 10.1016/0005-7967(71)90042-8
Lovaas, O. I., Schreibman, L., Koegel, R. L., and Rehm, R. (1971). Selective responding by autistic children to multiple sensory input. J. Abnormal Psychol. 77, 211–218. doi: 10.1037/h0031015
Meir, N., and Novogrodsky, R. (2019). Prerequisites of third-person pronoun use in monolingual and bilingual children with autism and typical language development. Front. Psychol. 10:2289. doi: 10.3389/fpsyg.2019.02289
Peristeri, E., Baldimtsi, E., Tsimpli, I. M., and Durrleman, S. (2024). “Bilingualism matters: a study of children with autism spectrum disorder and developmental language disorder,” in Multifaceted Multilingualism eds. K. K. Grohmann (Amsterdam: John Benjamins Publishing Company) 204–231. doi: 10.1075/sibil.66.08per
Peristeri, E., Baldimtsi, E., Vogelzang, M., Tsimpli, I. M., and Durrleman, S. (2021). The cognitive benefits of bilingualism in autism spectrum disorder: Is theory of mind boosted and by which underlying factors? Autism Res. 14, 1695–1709. doi: 10.1002/aur.2542
Petitto, L. A., Katerelos, M., Levy, B. G., Gauna, K., Tétreault, K., and Ferraro, V. (2001). Bilingual signed and spoken language acquisition from birth: implications for the mechanisms underlying early bilingual language acquisition. J. Child Lang. 28, 453–493. doi: 10.1017/S0305000901004718
Pickles, A., Anderson, D. K., and Lord, C. (2014). Heterogeneity and plasticity in the development of language: a 17-year follow-up of children referred early for possible autism. J. Child Psychol. Psych. Allied Discipl. 55, 1354–1362. doi: 10.1111/jcpp.12269
Pronovost, W., Wakstein, M. P., and Wakstein, D. J. (1966). A longitudinal study of the speech behavior and language comprehension of fourteen children diagnosed as autistic. Except. Child. 33, 19–26. doi: 10.1177/001440296603300104
Rincover, A., and Koegel, R. L. (1975). Setting generality and stimulus control in autistic children. J. Appl. Behav. Anal. 8, 235–246. doi: 10.1901/jaba.1975.8-235
Rogers, S. J., and Ozonoff, S. (2005). Annotation: What do we know about sensory dysfunction in autism? A critical review of the empirical evidence. J. Child Psychol. Psych. 46, 1255–1268. doi: 10.1111/j.1469-7610.2005.01431.x
Rutter, M., Bailey, A., and Lord, C. (2003). Social Communication Questionnaire: Manual. Los Angeles, CA: Western Psychological Services.
Salvin, A., Routh, D. K., Foster, R. E., and Lovejoy, K. M. (1977). Acquisition of modified American sign language by a mute autistic child. J. Autism Child. Schizophrenia 7, 359–71. doi: 10.1007/BF01540394
Schaeffer, B. (1980). Teaching signed speech to nonverbal children: theory and method. Sign. Lang. Stud. 26, 29–63. doi: 10.1353/sls.1980.0015
Schopler, E., Reichler, R. J., DeVellis, R. F., and Daly, K. (1980). Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J. Autism Dev. Disord. 10, 91–103. doi: 10.1007/BF02408436
Shield, A., Cooley, F., and Meier, R. P. (2017a). Sign language echolalia in deaf children with autism spectrum disorder. J. Speech Lang. Hear. Res. 60, 1622–1634. doi: 10.1044/2016_JSLHR-L-16-0292
Shield, A., Igel, M., Randall, K., and Meier, R. P. (2020). The source of palm orientation errors in the signing of children with ASD: Imitative, motoric, or both? Brain Sci. 10:258. doi: 10.3390/brainsci10050268
Shield, A., Knapke, K., Henry, M., Srinivasan, S., and Bhat, A. (2017b).Impaired praxis in gesture imitation by deaf children with autism spectrum disorder. Autism Dev. Lang. Impair. 2. doi: 10.1177/2396941517745674
Shield, A., and Meier, R. P. (2012). Palm reversal errors in native-signing children with autism. J. Commun. Disord. 45, 439–454. doi: 10.1016/j.jcomdis.2012.08.004
Shield, A., Meier, R. P., and Tager-Flusberg, H. (2015). The use of sign language pronouns by native-signing children with autism. J. Autism Develop. Disord. 45, 2128–2145. doi: 10.1007/s10803-015-2377-x
Shield, A., Pyers, J., Martin, A., and Tager-Flusberg, H. (2016). Relations between language and cognition in native-signing children with autism spectrum disorder. Autism Res. 9, 1304–1315. doi: 10.1002/aur.1621
Stull, S., Edkins, C., Krause, M., McGavin, G., Brand, L. H., and Webster, C. D. (1979). Sign language as a means of communicating with autistic and mentally handicapped children. Child Youth Care Forum 8, 143–147. doi: 10.1007/BF01554714
Tager-Flusberg, H., and Kasari, C. (2013). Minimally verbal school-aged children with autism spectrum disorder: the neglected end of the spectrum. Autism Res. 6, 468–478. doi: 10.1002/aur.1329
Tek, S., Mesite, L., Fein, D., and Naigles, L. (2014). Longitudinal analyses of expressive language development reveal two distinct language profiles among young children with autism spectrum disorders. J. Autism Dev. Disord. 44, 75–89. doi: 10.1007/s10803-013-1853-4
Valicenti-McDermott, M., Tarshis, N., Schouls, M., Galdston, M., Hottinger, K., Seijo, R., et al. (2013). Language differences between monolingual English and bilingual English–Spanish young children with autism spectrum disorders. J. Child Neurol. 28, 945–948. doi: 10.1177/0883073812453204
van den Bogaerde, B. (2000). Input and interaction in deaf families. [Thesis, Universiteit van Amsterdam]. IFOTT/LOT. doi: 10.1075/sll.3.1.12bog
Webster, C. D., McPherson, H., Sloman, L., Evans, M. A., and Kuchar, E. (1973). Communicating with an autistic boy by gestures. J. Autism Dev. Disord. 3, 337–346. doi: 10.1007/BF01538541
Wiig, E. H., Semel, E., and Secord, W. (2013). Clinical Evaluation of Language Fundamentals (5th ed.). San Antonio, TX: Pearson.
Keywords: autism spectrum disorder, bimodal bilingualism, sign language, receptive language, language acquisition
Citation: Shield A (2025) Language development in bimodal bilingual autistic children: a case series of hearing children with deaf signing parents. Front. Lang. Sci. 4:1671297. doi: 10.3389/flang.2025.1671297
Received: 22 July 2025; Accepted: 07 October 2025;
Published: 27 October 2025.
Edited by:
Mark Antoniou, Western Sydney University, AustraliaReviewed by:
Diane Lillo-Martin, University of Connecticut, United StatesZhonghua Wu, Hangzhou City University, China
Copyright © 2025 Shield. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aaron Shield, c2hpZWxkYUBtaWFtaW9oLmVkdQ==