 Oscar MacCormac1,2*
Oscar MacCormac1,2* Conor C. Horgan1,3
Conor C. Horgan1,3 Dale Waterhouse1,3Philip Noonan1,3Mirek Janatka1,3Richard Miles1,3Jaco Jacobs3Cameron Dockerill1,3Théo Trotouin1,3Alexis Schizas4
Dale Waterhouse1,3Philip Noonan1,3Mirek Janatka1,3Richard Miles1,3Jaco Jacobs3Cameron Dockerill1,3Théo Trotouin1,3Alexis Schizas4 Barbara Seeliger5,6,7Sebastien Ourselin1,3Michael Ebner1,3
Barbara Seeliger5,6,7Sebastien Ourselin1,3Michael Ebner1,3 Tom Vercauteren1,3
Tom Vercauteren1,3 Jonathan Shapey1,2,3
Jonathan Shapey1,2,3
- 1School of Biomedical Engineering & Imaging Science, King’s College London, London, United Kingdom
- 2Department of Neurosurgery, King’s College Hospital, London, United Kingdom
- 3Hypervision Surgical Limited, London, United Kingdom
- 4Department of General Surgery, St Thomas’ Hospital, London, United Kingdom
- 5Institute of Image-Guided Surgery, IHU Strasbourg, Strasbourg, France
- 6Department of Digestive and Endocrine Surgery, University Hospitals of Strasbourg, Strasbourg, France
- 7ICube, UMR 7357, CNRS, INSERM U1328 RODIN, University of Strasbourg, Strasbourg, France
Background: Ischaemia is a critical complication, and can result in poor surgical outcomes. While intra-operative overt ischaemia can be perceived with the naked eye, timely recognition of borderline perfusion can prevent post-operative ischaemic complications, which is particularly relevant for colorectal anastomoses. Consequently, there is a clinical need for new technologies to intra-operatively assess tissue oxygenation (indicative of end organ perfusion), with minimal disruption to the surgical workflow. Here we present a hyperspectral imaging (HSI) system for laparoscopic surgery. This system provides live, easy to interpret, tissue oxygenation (StO2) maps with associated quantitative values.
Methods: White light view and tissue oxygenation maps were reconstructed from a protoype laparoscopic Hyperspectral Surgical System (HSS). First, in a live porcine model (55 kg female), the mesentery of a small bowel loop was temporarily occluded with a laparoscopic grasper, then released whilst being imaged with HSI. The quantitative StO2 values obtained from the HSS were compared with those of a non-invasive tissue oximetry probe (Moor VMS-Oxy, Moor Instruments Ltd, United Kingdom). Secondly, mimicking a laparoscopic colon resection and anastomosis, the colorectal junction was mobilised laparoscopically, exteriorised, transected, anastomosed and repositioned in the abdominal cavity. In order to compare healthy and ischaemic colon, the distal part was intentionally devascularised. Tissue oxygenation maps were compared with indocyanine green fluorescence angiography (ICG-FA) of the anastomotic region.
Results: The HSS was used as the primary scope to complete a laparoscopic colorectal anastomosis, providing a simultaneous white light view and hyperspectral information. Quantitative results from small bowel imaging were shown to correlate with measurements from the superficial tissue oximetry probe. Real-time tissue oxygenation maps were shown to visually correlate with ICG-FA.
Conclusion: The HSS can guide laparoscopic surgical procedures whilst providing visual and quantitative tissue oxygenation information in a live animal model. This paves the way for further studies to assess clinical applications.
1 Introduction
Laparoscopic surgery has long proven to be safe and cost effective, resulting in reduced recovery times when compared to open surgery (1, 2). For optimal surgical vision, there has been continuous improvement in the associated visual technology over the last three decades, now with ultra-HD/4K and 3D laparoscopy systems being used (3). Furthermore, these improved imaging techniques have been associated with improved surgical outcomes (4, 5). Despite these significant improvements in standard white light imaging on conventional red, green and blue (RGB) camera systems, there remain invisible tissue parameters that may have significant impact on the success of the surgery. One such parameter is tissue oxygenation (StO2), and its impairment has been demonstrated to be an important factor in the aetiology of surgical complications, including anastomotic leakage (AL) (6).
Bowel anastomoses are a common procedure, particularly following oncological abdominal surgery (6), with nearly 85% of colorectal resections resulting in primary anastomosis in the UK (7). Whilst AL incidence is usually as low as 6%–7%, it can be as high as 19% in colorectal anastomoses (6, 8–12). When AL does occur, it carries a significant morbidity of up to 98%, with a long-term mortality as high as 36.4% (11, 13, 14). Moreover, it is associated with a significantly increased local tumour recurrence in colorectal cancer resections (9, 15–18).
For uncomplicated healing of a bowel anastomosis, adequate blood supply is considered essential to avoid AL (8, 13, 14, 19–21). Appropriate delivery of nutrients, in particular oxygen (22, 23), is essential for cellular homeostasis, function and wound healing (24). In ambient air, oxygen is delivered to tissue via blood, principally (98%) reversibly bound to haemoglobin in red blood cells (measured as oxygen saturation), and only a little dissolved in blood plasma. However, oxygen delivery also depends on other factors i.e., increased temperature, decreased pH and increased carbon dioxide () facilitate offloading of oxygen from haemoglobin. This is referred to as a ‘right shift’ in the oxygen dissociation curve (25). Aside from such general and systemic factors, it is generally assumed that a tissue that is well perfused receives an adequate oxygen supply. Detailed assessment of perfusion via blood flow or tissue oxygenation measurements could provide complementary information, particularly in situations of hypoxia or reduced oxygen carrying capability (low haemoglobin) (26).
Unfortunately, visualising bowel perfusion and oxygenation remains a challenge to predict anastomotic blood supply or tissue oxygenation (27). A number of approaches have been proposed to improve perfusion assessment with associated evidence to demonstrate improved patient outcomes, including indocyanine green fluorescence angiography (ICG-FA), laser speckle contrast imaging (LSCI) and Hyperspectral Imaging (HSI) (14).
Indocyanine green (ICG) fluorescence angiography (ICG-FA) is the method described most in the literature (14) and is likely the most familiar amongst general surgeons (28, 29). ICG is a fluorophore with an excitation peak within the near infra-red (NIR) spectrum (780 nm) and has an excellent safety profile (30, 31). It can be injected systemically into the bloodstream, or locally delivered via the urethra or submucosally depending on the organ/tissue of interest to be visualised (32).
Laser speckle contrast imaging (LSCI) is a wide-field technique for visualising microvascular perfusion in near real-time (33, 34). LSCI has only recently been integrated into a minimally invasive (laparoscopic) surgical setup (35, 36).
Unfortunately, neither ICG-FA nor LSCI are able to directly quantify StO2 information with currently commercialised systems, but rely on measuring tissue perfusion, from which oxygen supply may be inferred.
Hyperspectral imaging (HSI) is a wide-field, spectral imaging technique that is capable of obtaining specific tissue information depending on the optical properties of the structure in question, especially its scattering and absorption (37). By returning spatially-resolved, multi-channel spectral information, where each channel corresponds to a narrow wavelength band, each pixel in the image will have its own spectral signature as illustrated in Figure 1. Snapshot hyperspectral imaging captures the entire spatio-spectral data cube in a single image, meaning it can image in real-time, albeit with some compromises to spatial and spectral resolution, making it particularly suitable for clinical applications where live, real-time imaging is essential (38).
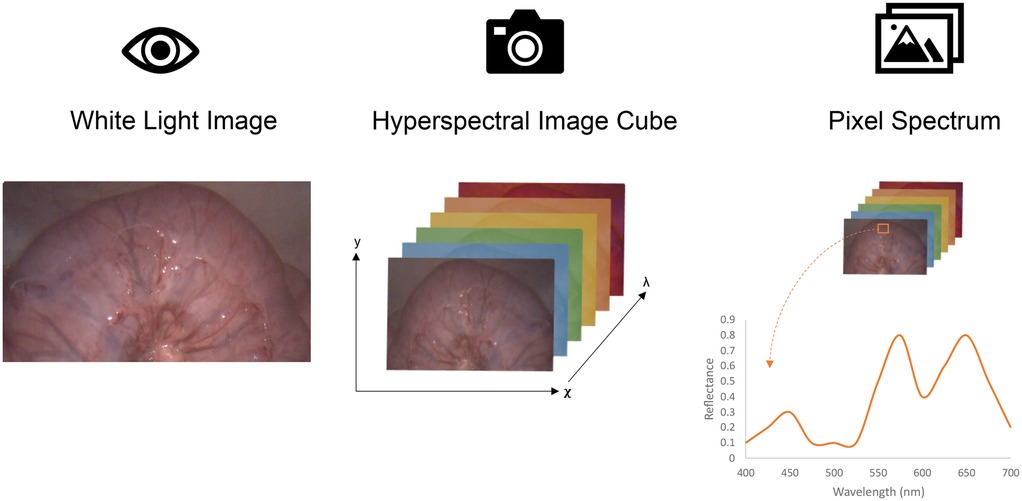
Figure 1. (Left) Simple 2D white light image. (Middle) 3D (two spatial: and one spectral: ) HSI image, resulting in a complete hypercube. (Right) Schematic representation of a HSI generated spectral curve from defined region of interest.
More specifically, snapshot mosaic HSI is a camera-based method by which each pixel has a single optical band-pass filter, allowing collection of a single channel per spatial location in one image (39, 40). Spectral filters are arranged in a repeating mosaic fashion, usually 4 4 or 5 5 pixels resulting in a lower spatial resolution per spectral channel and misalignment across spectral channels (39). Post-processing steps can infer the complete spatio-spectral data from the sampled pixels, improving the overall spectral and spatial resolution (41, 42). By simultaneously combining snapshot mosaic HSI with computational post-processing steps, it has been demonstrated as a feasible, real-time method for providing tissue differentiation and oxygenation measurement capabilities in surgery (43–47).
Hyperspectral imaging offers the potential for label-free, real-time, high-resolution imaging and tissue oxygenation information intra-operatively without many of the limitations described for ICG-FA (48–51). However, much of the current clinical literature pertaining to intra-operative HSI systems has so far been limited to open surgical techniques (52). This is due to the size of previous HSI cameras, as well as slow acquisition times, making these systems generally unsuitable for laparoscopic/minimally invasive surgery (MIS) (53). Diaspective Vision have made way towards overcoming these initial obstacles by developing an intra-operative laparoscopic HSI system (TIVITA Mini) that has demonstrated feasibility for in vivo use (53–55). Ayala et al. (43) have also taken promising steps towards addressing some of the challenges associated with intra-operative MIS HSI and have published the only clinical study in the literature reporting a laparoscopic HSI system capable of acquiring real-time tissue perfusion information, albeit in conjunction with a standard white light laparoscope (43). However, neither of these systems are yet able to provide truly quantitative and real-time StO2 information and simultaneously be used to guide entire laparoscopic procedures.
Further developments have been made to improve upon these promising starts towards hyperspectral-guided laparoscopic surgery (41, 45). An early prototype laparoscopic hyperspectral surgical system (HSS), provided by Hypervision Surgical Ltd, utilises a snapshot mosaic camera integrated with a standard laparoscopic setup and is able to provide real-time, high resolution (1,088 pixels 2,043 pixels), hyperspectral generated RGB video as well as simultaneous real-time tissue oxygenation (StO2) information.
The aims of this proof of concept study are to assess the reliability and feasibility of the HSS to guide laparoscopic abdominal surgery by performing a laparoscopic rectal mobilisation with externalised anastomosis, compare real-time StO2 information with the current clinical standard (ICG-FA), demonstrate the HSS capability to provide quantitative StO2 information by inducing small bowel ischaemia in a live porcine model and obtain initial surgeon feedback regarding the usability of the system.
2 Materials and methods
2.1 Equipment used
To enable simultaneous real-time white light imaging and quantitative imaging of superficial tissue oxygenation, this study used a prototype laparoscopic hyperspectral imaging system (Hypervision Surgical Ltd) with manual focus and fixed magnification. The sensor is a snapshot mosaic sensor with wavelengths covering the visible range. This system provides simultaneous real-time (60 fps) acquisition and processing of white light images alongside superficial tissue oxygenation visualisation based on computational hyperspectral imaging using proprietary artificial intelligence (AI) driven algorithms. A standard sterile camera drape was used to cover the HSS camera head and was coupled with a standard sterile laparoscopic telescope (Hopkins laparoscope, Karl Storz, Germany). This ensured sterility of the overall imaging system as per standard clinical practice. The display, Sunoptic Titan X450 Xenon light source (Sunoptic Technologies, Jacksonville, USA) and computer system were mounted on a standard medical cart to allow bedside positioning of the system. For ICG imaging, an independent commercially-available ICG imaging system (EleVision IR platform, Medtronic, USA) was deployed alongside the HSS.
2.2 Experimental animal procedure
On 12th June 2023, a female 55 kg Landrace pig was anaesthetised using Zoletil™ 2.2 mg/kg and medetomidine 0.02 mg/kg administered intramuscularly. General anaesthesia was induced with oxygen over isoflurane via a close fitting face mask, before intubation with a cuffed endotracheal tube (ETT). Anaesthesia was then maintained with oxygen over isoflurane via the ETT and respiration controlled via a ventilator. The animal was then positioned supine and the ambient lighting was switched off whilst the HSS was white balanced. A small (15 mm) midline incision was made and a 12 mm trocar placed under direct vision before peritoneal insufflation with CO2 to a pressure of 12 mm Hg. The laparoscopic HSS was inserted via this port and two further 12 mm ports along with one 5 mm port were placed under direct vision, using the real-time RGB video display from HSS, as per standard laparoscopic surgery procedure. Inside the abdomen, the surgeon selected a suitable small bowel loop and its corresponding mesentery was occluded with a laparoscopic grasper. Raw HSI data was recorded throughout the procedure, and simultaneous RGB and StO2 information was reconstructed for display to guide the procedure. The grasper was then released and reperfusion imaged and recorded using the HSS. A point-based superficial tissue oximetry probe (Moor VMS-Oxy, Moor Instruments Ltd, United Kingdom) was used to obtain quantitative StO2 measurements from relevant tissues during the procedure, based on the work published by Saito and Yamaguchi (56). The tissue oximetry probe was introduced into the abdomen alongside a standard laparoscopic grasper via a 12 mm port (Figure 2) and manipulated with the grasper.

Figure 2. Tissue oximetry probe secured to a Johan laparoscopic grasper and passed via a 12 mm laparoscopic port.
Once the tissue oximetry probe was positioned onto the same selected small bowel loop, the HSS light source was switched off to ensure accurate readings from the tissue oximetry probe. The tissue oximetry probe was held steady and StO2 readings were recorded (phase i). The HSS light source was then switched back on and the mesentery was temporarily occluded under direct vision, (phase ii). The HSS light source was switched off once again with the tissue oximetry probe held in the same position. StO2 readings were recorded until no further oxygenation decrease was observed (phase iii). The HSS light source was then switched on, with RGB visualisation of the ischaemic segment, and the mesentery released (phase iv), with the tissue oximetry probe then being positioned again and the HSS light source switched off. The tissue oximetry probe recorded StO2 measurements following reperfusion (phase v).
This process was repeated using the HSS. However, phase ii and iv were not required, given that recording of well perfused tissue (phase i), mesentery occlusion and ischaemia (phase iii) and reperfusion/return to normal values following mesentery release (phase v) could be carried out entirely under the visual guidance of the continuous wide field imaging of HSS. This process is summarised in Table 1.
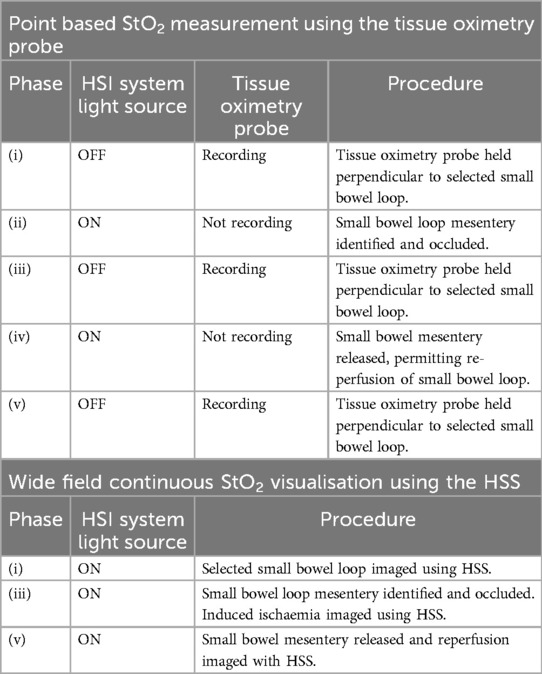
Table 1. Table outlining the procedure for tissue oximetry probe recordings and HSS recordings before, during and after induced small bowel ischaemia.
In total, two epsiodes of ischaemia were induced for the same segment of small bowel, one with the HSS light source predominantly off (tissue oximetry probe recording) and one with the HSS light source predominantly on (HSS recording).
Following this, a HSI laparoscope guided colorectal anastomosis was performed. The colorectal junction was mobilised laparoscopically and subsequently exteriorised via a mini laparotomy. The colon was transected and a continuity re-established with a hand sewn anastomosis prior to returning the colon to to the abdominal cavity. StO2 was not monitored during the exteriorised, hand-sewn anastomosis creation. The mini laparotomy was closed with silk sutures to maintain peritoneal insufflation thereafter. Subsequently, the porcine cranial rectal artery, which is equivalent to the human superior rectal artery (57), was occluded using Ethicon Ligaclips under HSI laparoscopic guidance and the marginal vasculature divided along the rectum, with StO2 information displayed and recorded using the HSS. This resulted in a near total devascularisation of the rectum, which facilitated a clear delineation between well perfused colon proximal and ischaemic distal to the anastomosis.
In order to create a comparison with ICG, a NIR compatible laparoscope (EleVision system) was used via a port adjacent to the HSS. ICG solution was prepared and injected intravenously at a dose of 0.2 mg/kg and the NIR system laser switched on, whilst the HSS light source was switched off. ICG-FA video was recorded up to to 5 min following ICG injection.
2.2.1 Comparison with ICG
Once the colorectal junction was mobilised laparoscopically, exteriorised, transected, anastomosed and repositioned in the abdominal cavity, the HSS was used to visualise StO2 in the well perfused tissue proximal to the anastomosis and the poorly perfused tissue distal to the anastomosis. Following injection of ICG, the Medtronic EleVision system was used to visualise ICG fluorescence in the same regions. Recordings were taken from each system, and a direct visual comparison was made.
2.2.2 HSI guided laparoscopic surgery
The surgical procedure was conducted by a qualified general surgeon with vast experience in laparoscopic surgery. Following the procedure, a short interview was conducted with the surgeon. He was asked to comment on the image quality, colour matching and usability of the HSS compared to the current clinical standard for laparoscopic imaging. Since a single surgeon operated on a single animal, no formal analysis of the surgeon feedback was performed. The interview was taken as an initial indication of system potential and usability by a single end user.
Following the experimental procedure, the pig was immediately euthanised with intravenous sodium pentobarbitone 140 mg/kg, in accordance with UK schedule 1 methodology.
IRB approval and written consent were not required for this study, as this study did not involve human participants.
3 Results
The HSS was used to successfully complete the experimental procedure as planned. There were no procedure related complications during this study, with no bleeding or initial indicators of anastomotic leakage.
3.1 visualisation in small bowel
Under laparoscopic vision with the HSS, hyperspectral-based reconstruction of RGB video was used to guide identification and occlusion of a small bowel mesentery. Figures 3A, C demonstrates the hyperspectral-based reconstruction of RGB video that was used to guide identification and occlusion of a small bowel mesentery. Whilst slight colour changes may be appreciated in the RGB images following occlusion of the mesentery, the HSS generated StO2 colour map demonstrated a more distinct and objective visualisation of the reduction in bowel StO2 (Figures 3B, D).
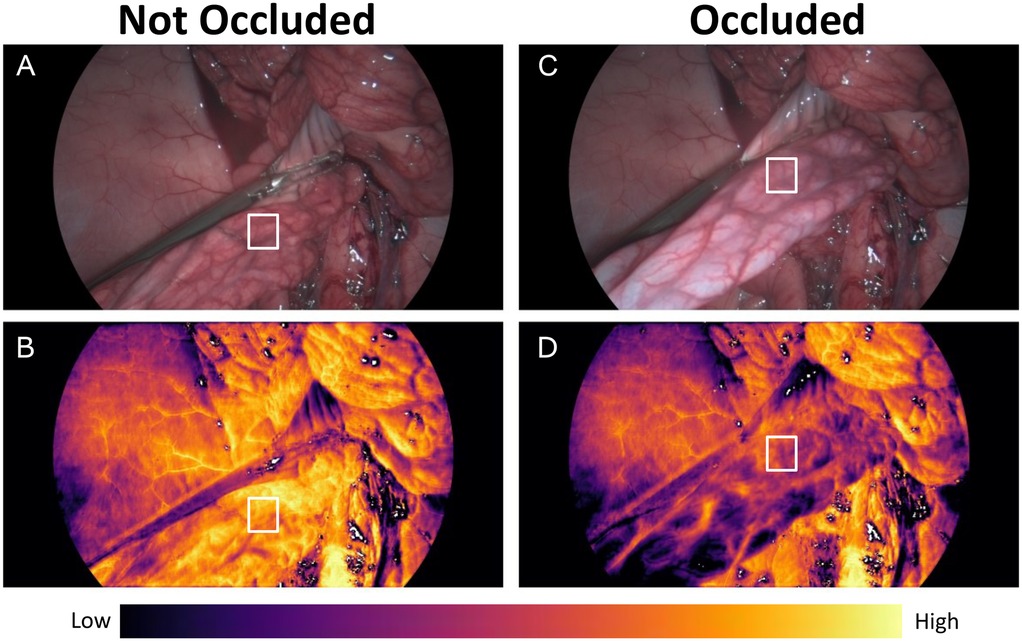
Figure 3. (A) Small bowel with open grasper and mesentery not occluded in RGB. (B) Small bowel with mesentery not occluded in StO2 vision. (C) Small bowel with closed grasper and mesentery occluded in RGB. (D) Small bowel with mesentery occluded in StO2 vision. Tissue oxygenation map colour bar denotes areas corresponding to low and high StO2. White square denotes the region at which the tissue oximetry probe was placed to generate the graph seen in Figure 4.
The region of interest (RoI) highlighted by the white rectangle in Figure 3 represents the tissue oximetry probe measurement area, providing reference readings for bowel StO2 during ischaemia and reperfusion as shown in Figure 4.
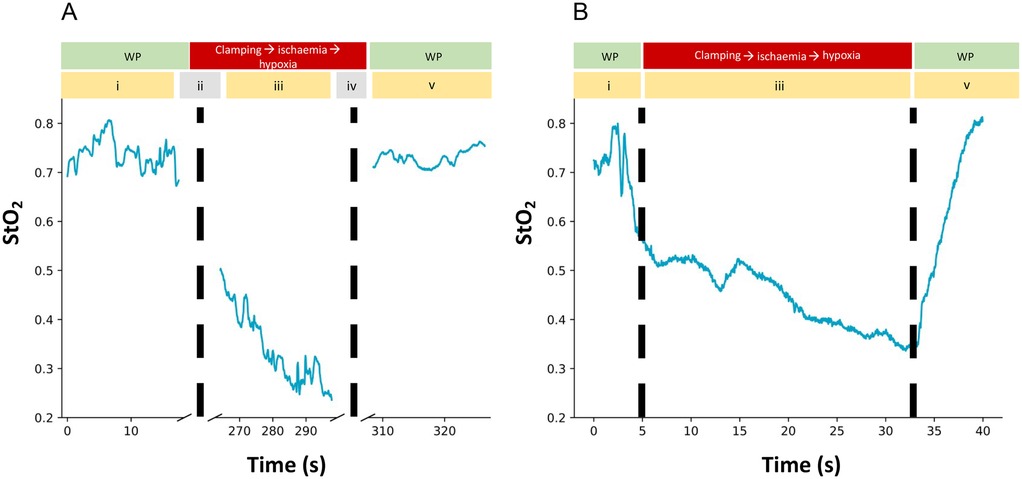
Figure 4. (A) tissue oximetry probe readings from well perfused (WP) small bowel (phase i), during induced ischaemia and reperfusion (phase iii) and following reperfusion (phase v). Dotted lines represent the clamping (phase ii) and release (phase iv) of the small bowel mesentery, during which no StO2 data could be recorded because the HSS light source was switched on for visualisation of the grasper. (B) HSS generated quantitative StO2 readings from well perfused (WP) small bowel (phase i), during induced ischaemia (phase iii) and reperfusion of the small bowel (phase v). Dotted lines represent the time points where the small bowel mesentery was occluded and released.
3.2 Comparison with ICG
Following completion of the colon anastomosis, with intentional devascularisation of the distal colon/rectum, the HSS was capable of providing StO2 information for the deoxygenated rectal tissue distal to the anastomosis as shown in Figure 5.
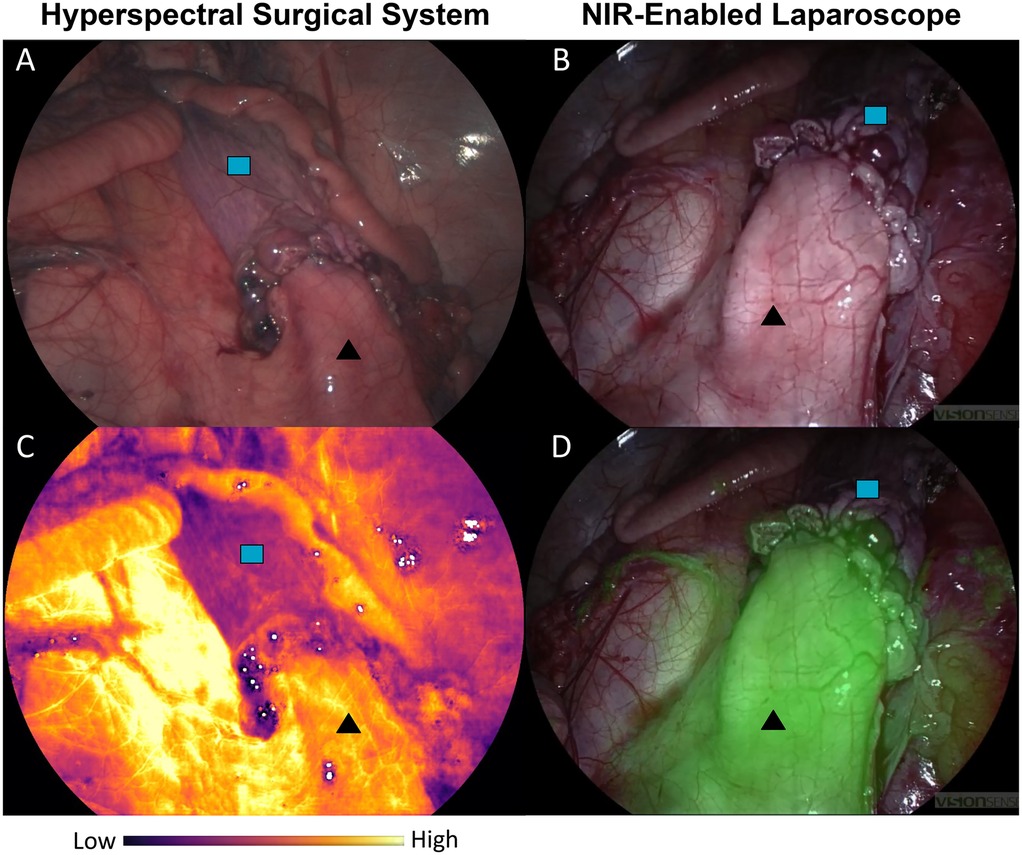
Figure 5. Comparison of ischaemic  rectum and well perfused
rectum and well perfused  colon. (A) HSI-generated RGB. (B) Near-infrared (NIR) enabled laparoscope RGB. (C) HSI-generated StO2 map. (D) NIR overlay of the same anastomotic region. Different viewpoints of the anastomosis are due to imaging via different ports to accommodate both the HSS and laparoscope (Ele Vision).
colon. (A) HSI-generated RGB. (B) Near-infrared (NIR) enabled laparoscope RGB. (C) HSI-generated StO2 map. (D) NIR overlay of the same anastomotic region. Different viewpoints of the anastomosis are due to imaging via different ports to accommodate both the HSS and laparoscope (Ele Vision).
Whilst colour differences can be perceived in the HSI-generated RGB in Figures 5A, B, the visual (non-quantitative) assessment of the ICG-FA view in Figure 5D also demonstrates the ischaemic boundary. The HSI-based StO2 map illustrated the well oxygenated and deoxygenated regions comparatively clearly in Figure 5C.
3.3 HSI-guided laparoscopic surgery
The HSS was successfully used to carry out laparoscopic surgery as it displayed real-time HSI-generated RGB images (akin to standard white light imaging), whilst simultaneously displaying real-time StO2 information next to the RGB feed as illustrated in Figure 6.
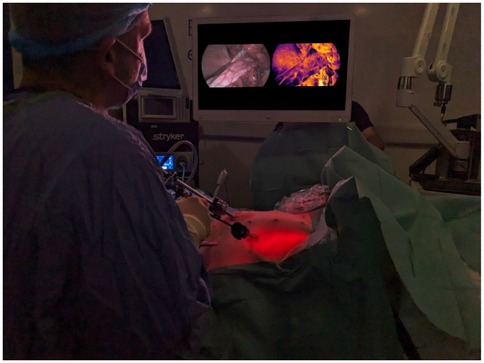
Figure 6. Use of the HSS for laparoscopic surgery. It simultaneously provides the RGB view generated from hyperspectral information (left on the display monitor) as well as the StO2 colour map display (right on the display monitor). The image displayed on the screen has been replaced to better represent the visualised StO2 map.
During the post-procedure interview with the lead surgeon, points highlighted were that the system was “easy to use, handle and not heavy,” as well as “The frame rate is good without perceptible lag.” Additionally, the operating surgeon felt that “the colours with the HSS RGB seem more accurate than that of the laparoscopic system,” referring to the ICG imaging system used in this study. Areas to improve in the pre-commercial HSS used in this early study were that “the [image] definition is closer to standard definition than high definition” and that “the [image] definition is not as good when viewing at a distance.” These have been elaborated on further in Section 6.
4 Study limitations
Whilst we feel that this study shows promising early results, it is important to emphasise its limitations. Firstly, this is a proof of concept using a single animal, with a single independent operating surgeon. The qualitative feedback was also from this one surgeon. Formal qualitative assessments would need to be carried out to thoroughly assess this technology, its usability and its impact on the wider operating theatre team, akin to those performed with other, similar hyperspectral systems (58).
Additionally, whilst every effort was made to create the same surgical environment when data was being collected using the point based tissue oximetry probe and the HSS, the steps outlined in Table 1 meant that the time points for each method were not the same, as evidenced in Figure 4. This means that a meaningful statistical analysis was not able to be performed on the single set of results obtained and further studies would need to be carried out to facilitate a detailed statistical analysis.
A further limitation of this proof-of-concept study is that it was designed to compare StO2 visualisation of ischaemic and oxygenated bowel following the anastomosis. Further studies will be required to assess the system’s ability to detect more subtle and transitional ischaemic changes, such as those observed in the ischaemia-reperfusion StO2 curves, as well as to inform clinical decision making and assess the impact of such image guidance on the clinical outcome.
5 Barriers to uptake of new surgical technology
When considering developing a new technology, it is important to consider perceived barriers to adoption, which have been well described. From an individual perspective, how useful the technology is and how well it integrates into an individual surgeon’s practice has been shown to be a key factor (59, 60), as opposed to how easy the technology is to use, which plays less of a role (60). As well as this, lengthy training time has been demonstrated to reduce uptake of new surgical technologies (59), which we feel is unlikely to play a significant role with the HSS given the fact that our system uses already familiar laparoscopes. Finally, lack of clear benefits to patients is a significant barrier to uptake, which is why further work is required to establish the tangible impact of the HSS on our patient population. We are addressing this by undertaking a multi-centre trial in human participants (LapHSI Clinical Trial Number NCT06700317), due to begin recruitment in 2025.
6 Discussion
Our study aimed to demonstrate the reliability and feasibility of a novel HSI system that can provide real-time quantitative StO2 information in bowel tissue alongside conventional RGB vision for surgical guidance. This system is also the first system that we are aware of that utilises HSI-generated RGB to guide the entire surgical procedure, without reliance on an additional RGB imaging system.
This study has demonstrated that the HSS is capable of laparoscopic surgical guidance, as well as displaying accurate bowel StO2 information to the surgeon in real-time. The HSS HSI generated RGB visualisation was able to guide the surgery throughout the procedure. HSI-generated quantitative StO2 results showed a good correlation with readings taken using the tissue oximetry probe, although it is important to note that the probe was used outside of its intended use (FDA cleared for non-invasive use). Similarly, the visual StO2 map was comparable to the ICG-FA perfusion display, as can be seen in Figure 5.
In terms of limitations reported by the lead surgeon, image definition is an important factor to consider for improvement, with the goal of full HD (1080 1920) visualisation desired as a minimum for surgery. From the computational perspective, image resolution improvements are expected by deploying dedicated super-resolution methods. From the hardware perspective, further improvements could also be achieved by using an improved sensor with a greater pixel density.
Related to the above, some feedback from the surgeon detailed in Section 3 suggested that imaging from a greater working distance resulted in slightly poorer image definition. This may be a limitation of the system’s hardware, for example the optical quality of the camera coupler. Similarly, the current HSS utilises a manually adjustable focus that some surgeons may be unaccustomed to. Whilst the system has a large depth of field, focus may need to be adjusted manually to achieve in-focus images at different working distances. Our surgeon typically operates using state-of-the-art 4 K robotic systems with in-built autofocus (Da Vinci Xi); systems typically present in world-class teaching and research hospitals. However, many centers that offer laparoscopic surgery still use standard definition (SD) cameras with manual focus as standard of care. Moreover, the image quality of future systems may be improved by enabling a greater depth of field and integrating an autofocus capability (61, 62), in line with recent MIS system developments.
However, the HSS demonstrates a promising advancement in the field of laparoscopic HSI-enabled surgical vision, in line with the progress made by Diaspective Vision. Their MIS HSI system (TIVITA-Mini) has been compared with their open surgical system, which has been shown to accurately detect bowel ischaemia, surpassing quantitative ICG-FA in predicting local capillary lactate levels as a marker of ischaemia (49, 63). Correlation has been shown between intra-operative StO2 measurements taken using the TIVITA Mini and the open TIVITA system, albeit with a mean absolute error (MAE) between 12.6% and 17.7% (53). However, it is important to note that this correlation was achieved during open surgery, and the response of the system when used as intended inside the abdominal cavity may be different to the response measured outside of it. For example, the presence of multiple distinct tissue types within the same field of view, as well as the enclosure of the system in a semi-opaque cavity will almost certainly affect the optical properties of the system by introducing differences in light scattering, absorption and reflectance when compared to the open surgical environment. Another important limitation with the TIVITA Mini is the fact that a laparoscopic holder was required for stabilization as the handheld system created too much motion blur (53). Whilst using a laparoscope holder is technically feasible in MIS surgery, it might significantly impact the surgical workflow when the system is used throughout multi-quadrant procedures. Furthermore, the reported HSI image acquisition time for the TIVITA Mini was between 4.6 s (54) and 7 s (53), which complicates a seamless integration into the surgical workflow.
Ayala et al. (43) have reported a clinical study in which a laparoscopic multispectral imaging (MSI)/HSI system capable of providing real-time StO2 information has been evaluated. However, in their work, they relied on a proposed ischaemic index as opposed to an absolute StO2 value. This means the results are somewhat binary as the tissue is considered either perfused or ischaemic. Whilst certainly beneficial in the context of establishing whether renal blood flow has confidently been occluded, this may not be as helpful in other surgical applications, such as bowel anastomoses, where the StO2 changes can be more subtle. Furthermore, the study required an additional standard laparoscopic camera to carry out the surgery, meaning multiple camera removal and insertions as well as frequent alterations to the laparoscopic light source, resulting in a negative impact on the surgical workflow
Whilst our study focuses on HSI to guide surgery and its ability to provide StO2 information, it should be noted that concurrent approaches are being pursued for obtaining tissue perfusion information in laparoscopic surgery. However, as per Section 1, both ICG-FA and LSCI come with their own limitations.
In the context of digestive anastomoses, ICG requires preparation by an anaesthetist and is generally administered as an intravenous bolus when requested by the surgeon (64). However, the protocols worldwide are not fully standardised and assessment is time-dependent (14). Colonic fluorescence is generally monitored for two minutes following injection with the laparoscopic NIR camera/mode. This can also be performed in open surgery with a dedicated camera system provided ambient lighting is switched off (64). There are also further limitations to ICG image analysis. Firstly, it remains subjective. The operating surgeon will need to decide whether the fluorescence visualised is representative of adequate blood supply or (borderline) ischaemia and this is often unclear (16, 65). Whilst steps have been made in correlating certain parameters of the ICG intensity curve, such as maximum fluorescence () and the time to maximum fluorescence (), with AL (16, 66–71), there have been inconsistent results in studies thus far (16). Attempts have also been made to use computer software to quantify fluorescence dynamics (51, 65, 72–75), although these remain in the development phase and are not yet available for clinical use outside of clinical study protocols. Repeated doses are often required throughout a surgical procedure to confirm adequate perfusion (76), but background fluorescence from prior injections can hinder visual assessment and poses further challenges for potential quantitative evaluation (77). Conditional factors such as distance of the camera from region of interest (RoI), ambient lighting conditions (64) and patient specific factors such as hypertension/portal hypertension (65) can also affect the fluorescence intensity and time to (peak) fluorescence, making this technique challenging to standardise. Indeed, the ICG-FA shown in Figure 5C could be biased by highlighting the region closest to the camera in green, with a potentially weaker signal imperceptible in the overlay for the distal rectum.
LSCI has only recently been integrated into a minimally invasive (laparoscopic) surgical setup (35, 36, 78). LSCI achieves tissue perfusion monitoring by measuring the interference pattern caused by scattered light from a tissue surface that has been illuminated by a laser (34, 79); the so called “speckle” pattern. When there is motion within the illuminated surface, particularly at a rate equal to or greater than the image exposure time (e.g., blood flow) then this speckle pattern will become blurred (34). This blurring, or contrast loss, can be correlated with tissue perfusion (34, 36). As with ICG-FA, there are also limitations with LSCI. For example, as LSCI relies on the movement of blood, it is also susceptible to other forms of motion such as breathing or peristalsis (80) and is bound to qualitative measurements with very limited inter-patient comparability (34). LSCI is also susceptible to specular reflection and differences in camera angulation, making it subject to inconsistencies when used in the abdominal cavity where surfaces are curved and often reflective (14, 65, 80, 81).
7 Conclusion
This presented prototype HSS has enabled the first fully HSI-driven laparoscopic surgery. It is capable of simultaneously providing standard surgical visualisation and simultaneously displaying tissue StO2 information to the surgeon. We have shown that the HSS HSI-derived StO2 values align well with reference values recorded with a tissue oximetry probe and that it compares favourably with ICG-FA within the confines of this study. This paves the way for further development and future work to demonstrate the utility of the HSS in patients undergoing laparoscopic bowel surgery is planned.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The animal study was approved by The Griffin Institute Animal Welfare Ethical Review Body (AWERB): AWERB_023Project License Number: P14B07C34. The study was conducted in accordance with the local legislation and institutional requirements.
Author contributions
OMC: Data curation, Formal analysis, Methodology, Writing – original draft. CCH: Formal analysis, Methodology, Software, Writing – review & editing. DW: Writing – review & editing. PN: Software, Writing – review & editing. MJ: Visualization, Writing – review & editing. RM: Software, Writing – review & editing. JJ: Funding acquisition, Resources, Writing – review & editing. CD: Project administration, Resources, Writing – review & editing. TT: Project administration, Validation, Writing – review & editing. AS: Data curation, Writing – review & editing. BS: Writing – review & editing; SO: Supervision, Writing – review & editing. ME: Funding acquisition, Resources, Writing – review & editing. TV: Supervision, Writing – review & editing. JS: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by Hypervision Surgical, Ltd (85 Great Portland Street, First Floor, London, W1W 7LT, United Kingdom) who also provided the HSS. OM is funded by the EPSRC Research Council, part of the EPSRC DTP, Grant Ref: [EP/T517963/1]. This work was supported by core funding from the Wellcome/EPSRC [WT203148/Z/16/Z; NS/A000049/1]. TV is supported by a Medtronic/RAEng Research Chair [RCSRF1819734]. CH is supported by an InnovateUK Secondment Scholars Grant (Project Number 75124). CD was supported by the UK Medical Research Council [MR/N013700/1] and the King’s College London MRC Doctoral Training Partnership in Biomedical Sciences For the purpose of open access, the authors have applied a CC-BY public copyright license to any Author Accepted Manuscript version arising from this submission. This work was also supported by French state funds managed by the ANR within the ‘Programme d'investissements d'avenir’ France 2030 (reference ANR-10-IAHU-02).
Acknowledgments
We would like to acknowledge the staff members at The Griffin Institute, Harrow, London, without whom this work would not be possible. We would like to acknowledge Navodini Wijethilake and Zhonghao Wang of King’s College London for their assistance with LaTeX during the writing of this manuscript.
Conflict of interest
The authors declare that the research was conducted in collaboration between Hypervision Surgical and King’s College London. Authors ME, PN, MJ, CH, TT, JJ, CD, DW are all paid employees of Hypervision Surgical Ltd. ME, TV, SO and JS are shareholders and co-founders of Hypervision Surgical Ltd. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmedt.2025.1549245/full#supplementary-material
References
1. Ates M, Coban S, Sevil S, Terzi A. The efficacy of laparoscopic surgery in patients with peritonitis. Surg Laparosc Endosc Percutan Tech. (2008) 18:453–6. doi: 10.1097/SLE.0b013e31817f4624
2. Murray AC, Lourenco T, De Verteuil R, Hernández RA, Fraser MF, McKinley AJ, et al. Clinical effectiveness and cost-effectiveness of laparoscopic surgery for colorectal cancer: systematic reviews and economic evaluation. Health Technol Assess (Rockv). (2006) 10(45):1–141, iii-iv. doi: 10.3310/hta10450
3. Singla V, Bhattacharjee HK, Gupta E, Singh D, Mishra AK, Kumar D. Performance of three-dimensional and ultra-high-definition (4K) technology in laparoscopic surgery: a systematic review and meta-analysis. J Minim Access Surg. (2022) 18:167. 10.4103/jmas.jmas_122_2135313429
4. Mari GM, Crippa J, Achilli P, Miranda A, Santurro L, Riggio V, et al. 4K ultra HD technology reduces operative time and intraoperative blood loss in colorectal laparoscopic surgery. F1000Research. (2020) 9:106. doi: 10.12688/f1000research.21297.1
5. Zhang L, Hong H, Zang L, Dong F, Lu A, Feng B, et al.Application value of 4K high-definition system in laparoscopic gastrectomy: preliminary results and initial experience. J Laparoendosc Adv Surg Tech. (2022) 32:137–41. doi: 10.1089/lap.2020.0931
6. Marland JR, Gray ME, Argyle DJ, Underwood I, Murray AF, Potter MA. Post-operative monitoring of intestinal tissue oxygenation using an implantable microfabricated oxygen sensor. Micromachines. (2021) 12:810. doi: 10.3390/mi12070810
7. Janardhanan P, Khalid A, Anwaar M, Williams R, Timms E, Ward S, et al. The “hub” model for colorectal surgery: a viable paradigm shift? Ann R Coll Surg Engl. (2025). doi: 10.1308/rcsann.2024.0003
8. Kingham PT, Pachter LH. Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg. (2009) 208:269–78. doi: 10.1016/j.jamcollsurg.2008.10.015
9. Koedam TW, Bootsma BT, Deijen CL, van de Brug T, Kazemier G, Cuesta MA, et al. Oncological outcomes after anastomotic leakage after surgery for colon or rectal cancer: increased risk of local recurrence. Ann Surg. (2022) 275:e420–7. doi: 10.1097/SLA.0000000000003889
10. McDermott F, Heeney A, Kelly M, Steele R, Carlson G, Winter D. Systematic review of preoperative, intraoperative and postoperative risk factors for colorectal anastomotic leaks. Br J Surg. (2015) 102:462–79. doi: 10.1002/bjs.9697
11. Turrentine FE, Denlinger CE, Simpson VB, Garwood RA, Guerlain S, Agrawal A, et al. Morbidity, mortality, cost, and survival estimates of gastrointestinal anastomotic leaks. J Am Coll Surg. (2015) 220:195–206. doi: 10.1016/j.jamcollsurg.2014.11.002
12. Wan Y, Lim S, Riebman J, Jamous N, Gao X. Pwe-024 clinical and economic burden associated with anastomotic leak after colorectal surgeries in the United Kingdom. Gut. (2014) 63:A132.1. doi: 10.1136/gutjnl-2014-307263.284
13. Choi H-K, Law W-L, Ho JW. Leakage after resection and intraperitoneal anastomosis for colorectal malignancy: analysis of risk factors. Dis Colon Rectum. (2006) 49:1719–25. doi: 10.1007/s10350-006-0703-2
14. Renna MS, Grzeda MT, Bailey J, Hainsworth A, Ourselin S, Ebner M, et al. Intraoperative bowel perfusion assessment methods and their effects on anastomotic leak rates: meta-analysis. Br J Surg. (2023) 110(9):1131–42. doi: 10.1093/bjs/znad154
15. Ha GW, Kim JH, Lee MR. Oncologic impact of anastomotic leakage following colorectal cancer surgery: a systematic review and meta-analysis. Ann Surg Oncol. (2017) 24:3289–99. doi: 10.1245/s10434-017-5881-8
16. Iwamoto M, Ueda K, Kawamura J. A narrative review of the usefulness of indocyanine green fluorescence angiography for perfusion assessment in colorectal surgery. Cancers. (2022) 14:5623. doi: 10.3390/cancers14225623
17. Karim A, Cubas V, Zaman S, Khan S, Patel H, Waterland P. Anastomotic leak and cancer-specific outcomes after curative rectal cancer surgery: a systematic review and meta-analysis. Tech Coloproctol. (2020) 24:513–25. doi: 10.1007/s10151-020-02153-5
18. Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased local recurrence and reduced survival from colorectal cancer following anastomotic leak: systematic review and meta-analysis. Ann Surg. (2011) 253:890–9. doi: 10.1097/SLA.0b013e3182128929
19. Kojima S, Sakamoto T, Nagai Y, Matsui Y, Nambu K, Masamune K. Laser speckle contrast imaging for intraoperative quantitative assessment of intestinal blood perfusion during colorectal surgery: a prospective pilot study. Surg Innov. (2019) 26:293–301. doi: 10.1177/1553350618823426
20. Rutegård M, Rutegård J. Anastomotic leakage in rectal cancer surgery: the role of blood perfusion. World J Gastrointest Surg. (2015) 7:289. doi: 10.4240/wjgs.v7.i11.289
21. Vignali A, Gianotti L, Braga M, Radaelli G, Malvezzi L, Carlo VD. Altered microperfusion at the rectal stump is predictive for rectal anastomotic leak. Dis Colon Rectum. (2000) 43:76–82. doi: 10.1007/BF02237248
22. Gottrup F. Physiology and measurement of tissue perfusion. Ann Chir Gynaecol. (1994) 83:183–9.7857061
23. Seiler A, Blockley NP, Deichmann R, Nöth U, Singer OC, Chappell MA, et al. The relationship between blood flow impairment and oxygen depletion in acute ischemic stroke imaged with magnetic resonance imaging. J Cereb Blood Flow Metab. (2019) 39:454–65. doi: 10.1177/0271678X17732448
24. Castilla DM, Liu Z-J, Velazquez OC. Oxygen: implications for wound healing. Adv Wound Care. (2012) 1:225–30. doi: 10.1089/wound.2011.0319
26. Bhutta BS, Alghoula F, Berim I. Hypoxia. In: StatPearls. Tampa, FL, USA: StatPearls Publishing (2022).
27. Karliczek A, Harlaar N, Zeebregts C, Wiggers T, Baas P, Van Dam G. Surgeons lack predictive accuracy for anastomotic leakage in gastrointestinal surgery. Int J Colorectal Dis. (2009) 24:569–76. doi: 10.1007/s00384-009-0658-6
28. Borg L, Portelli M, Testa L, Andrejevic P. The use of indocyanine green for colorectal anastomoses: a systematic review and meta-analysis. Ann R Coll Surg Engl. (2024). doi: 10.1308/rcsann.2024.0002
29. Singaravelu A, Entee PDM, Boland PA, Moynihan A, McCarrick C, Vahrmeijer AL, et al. Colorectal surgeons’ perspectives on the efficacy of intraoperative bowel perfusion technology with a focus on indocyanine green fluorescence angiography. Langenbecks Arch Surg. (2025) 410:73. doi: 10.1007/s00423-025-03640-9
30. Hope-Ross M, Yannuzzi LA, Gragoudas ES, Guyer DR, Slakter JS, Sorenson JA, et al. Adverse reactions due to indocyanine green. Ophthalmology. (1994) 101:529–33. doi: 10.1016/S0161-6420(94)31303-0
31. Wang X, Zhang Y, Yang H, Xu Y. Maternal–fetal transfer of indocyanine green: a systematic review. J Matern-Fetal Neonatal Med. (2022) 35:8181–5. doi: 10.1080/14767058.2021.1966410
32. Garoufalia Z, Wexner SD. Indocyanine green fluorescence guided surgery in colorectal surgery. J Clin Med. (2023) 12:494. doi: 10.3390/jcm12020494
33. Allen J, Howell K. Microvascular imaging: techniques and opportunities for clinical physiological measurements. Physiol Meas. (2014) 35:R91. doi: 10.1088/0967-3334/35/7/R91
34. Heeman W, Steenbergen W, van Dam GM, Boerma EC. Clinical applications of laser speckle contrast imaging: a review. J Biomed Opt. (2019) 24:080901. doi: 10.1117/1.JBO.24.8.080901
35. Heeman W, Wildeboer AC, Al-Taher M, Calon JE, Stassen LP, Diana M, et al. Experimental evaluation of laparoscopic laser speckle contrast imaging to visualize perfusion deficits during intestinal surgery. Surg Endosc. (2023) 37:950–7. doi: 10.1007/s00464-022-09536-9
36. Wildeboer A, Heeman W, van der Bilt A, Hoff C, Calon J, Boerma EC, et al. Laparoscopic laser speckle contrast imaging can visualize anastomotic perfusion: a demonstration in a porcine model. Life. (2022) 12:1251. doi: 10.3390/life12081251
37. Jacques SL. Optical properties of biological tissues: a review. Phys Med Biol. (2013) 58:R37–R61. doi: 10.1088/0031-9155/58/11/R37
38. Clancy NT, Jones G, Maier-Hein L, Elson DS, Stoyanov D. Surgical spectral imaging. Med Image Anal. (2020) 63:101699. doi: 10.1016/j.media.2020.101699
39. Bahl A, Horgan CC, Janatka M, MacCormac OJ, Noonan P, Xie Y, et al. Synthetic white balancing for intra-operative hyperspectral imaging. J Med Imaging. (2023) 10:046001. doi: 10.1117/1.JMI.10.4.046001
40. Geelen B, Tack N, Lambrechts A. A compact snapshot multispectral imager with a monolithically integrated per-pixel filter mosaic. In: Advanced Fabrication Technologies for Micro/Nano Optics and Photonics VII. SPIE (2014). Vol. 8974. p. 80–7.
41. Li P, Asad M, Horgan C, MacCormac O, Shapey J, Vercauteren T. Spatial gradient consistency for unsupervised learning of hyperspectral demosaicking: application to surgical imaging. Int J Comput Assist Radiol Surg. (2023) 18(6):981–8. doi: 10.1007/s11548-023-02865-7
42. Pichette J, Goossens T, Vunckx K, Lambrechts A. Hyperspectral calibration method for CMOS-based hyperspectral sensors. In: Photonic Instrumentation Engineering IV. SPIE (2017). Vol. 10110. p. 132–44.
43. Ayala L, Adler TJ, Seidlitz S, Wirkert S, Engels C, Seitel A, et al. Spectral imaging enables contrast agent–free real-time ischemia monitoring in laparoscopic surgery. Sci Adv. (2023) 9:eadd6778. doi: 10.1126/sciadv.add6778
44. Chalopin C, Nickel F, Pfahl A, Köhler H, Maktabi M, Thieme R, et al. Künstliche intelligenz und hyperspektrale bildgebung zur bildgestützten assistenz in der minimal-invasiven chirurgie. Die Chir. (2022) 93:940–7. doi: 10.1007/s00104-022-01677-w
45. Ebner M, Nabavi E, Shapey J, Xie Y, Liebmann F, Spirig JM, et al. Intraoperative hyperspectral label-free imaging: from system design to first-in-patient translation. J Phys D: Appl Phys. (2021) 54:294003. doi: 10.1088/1361-6463/abfbf6
46. Jansen-Winkeln B, Holfert N, Köhler H, Moulla Y, Takoh J, Rabe S, et al. Determination of the transection margin during colorectal resection with hyperspectral imaging (HSI). Int J Colorectal Dis. (2019) 34:731–9. doi: 10.1007/s00384-019-03250-0
47. MacCormac O, Horgan C, Noonan P, Janatka M, Trotouin T, Jacobs J, et al. Real-time intra-operative hyperspectral imaging derived tissue properties in neurosurgery: a first in human case series (ideal 1 and 2a). Brain Spine. (2024) 4:103594. doi: 10.1016/j.bas.2024.103594
48. Akbari H, Kosugi Y, Kojima K, Tanaka N. Detection and analysis of the intestinal ischemia using visible and invisible hyperspectral imaging. IEEE Trans Biomed Eng. (2010) 57:2011–7. doi: 10.1109/TBME.2010.2049110
49. Barberio M, Felli E, Seyller E, Longo F, Chand M, Gockel I, et al. Quantitative fluorescence angiography versus hyperspectral imaging to assess bowel ischemia: a comparative study in enhanced reality. Surgery. (2020) 168:178–84. doi: 10.1016/j.surg.2020.02.008
50. Holmer A, Marotz J, Wahl P, Dau M, Kämmerer PW. Hyperspectral imaging in perfusion and wound diagnostics–methods and algorithms for the determination of tissue parameters. Biomed Tech (Berl). (2018) 63:547–56. doi: 10.1515/bmt-2017-0155
51. Son GM, Nazir AM, Yun MS, Lee IY, Im SB, Kwak JY, et al. The safe values of quantitative perfusion parameters of ICG angiography based on tissue oxygenation of hyperspectral imaging for laparoscopic colorectal surgery: a prospective observational study. Biomedicines. (2023) 11:2029. doi: 10.3390/biomedicines11072029
52. Shapey J, Xie Y, Nabavi E, Bradford R, Saeed SR, Ourselin S, et al. Intraoperative multispectral and hyperspectral label-free imaging: a systematic review of in vivo clinical studies. J Biophotonics. (2019) 12:e201800455. doi: 10.1002/jbio.201800455
53. Thomaßen MT, Köhler H, Pfahl A, Stelzner S, Mehdorn M, Thieme R, et al. In vivo evaluation of a hyperspectral imaging system for minimally invasive surgery (HSI-MIS). Surg Endosc. (2023) 37(5):3691–700. doi: 10.1007/s00464-023-09874-2
54. Köhler H, Kulcke A, Maktabi M, Moulla Y, Jansen-Winkeln B, Barberio M, et al. Laparoscopic system for simultaneous high-resolution video and rapid hyperspectral imaging in the visible and near-infrared spectral range. J Biomed Opt. (2020) 25:086004. doi: 10.1117/1.JBO.25.8086004
55. Pfahl A, Köhler H, Thomaßen MT, Maktabi M, Bloße AM, Mehdorn M, et al. Video: clinical evaluation of a laparoscopic hyperspectral imaging system. Surg Endosc. (2022) 36:7794–9. doi: 10.1007/s00464-022-09282-y
56. Saito T, Yamaguchi H. Optical imaging of hemoglobin oxygen saturation using a small number of spectral images for endoscopic application. J Biomed Opt. (2015) 20:126011. doi: 10.1117/1.JBO.20.12.126011
57. Hasegawa H, Takeshita N, Ito M. Novel oxygen saturation imaging endoscopy to assess anastomotic integrity in a porcine ischemia model. BMC Surg. (2020) 20:1–8. doi: 10.1186/s12893-020-00913-6
58. Elliot M, Al Banna Q, Payne MA, MacCormac O, Patel MS, Wang Z, et al. The development and validation of an intra-operative hyperspectral imaging system for neurosurgery: embedding human factors in the design phase of novel surgical technology. Brain Spine. (2024) 4:103616. doi: 10.1016/j.bas.2024.103616
59. BenMessaoud C, Kharrazi H, MacDorman KF. Facilitators and barriers to adopting robotic-assisted surgery: contextualizing the unified theory of acceptance and use of technology. PLoS One. (2011) 6:e16395. doi: 10.1371/journal.pone.0016395
60. Chau PY, Hu PJ. Examining a model of information technology acceptance by individual professionals: an exploratory study. J Manage Inf Syst. (2002) 18:191–229. doi: 10.1080/07421222.2002.11045699
61. Budd C, Qiu J, MacCormac O, Huber M, Mower C, Janatka M, et al.. Deep reinforcement learning based system for intraoperative hyperspectral video autofocusing. In: International Conference on Medical Image Computing and Computer-Assisted Intervention. Springer (2023). p. 658–67.
62. Katz JI, Lee S-y., Hua H. Improved multi-resolution foveated laparoscope with real-time digital transverse chromatic correction. Appl Opt. (2020) 59:G79–G91. doi: 10.1364/AO.393088
63. Barberio M, Longo F, Fiorillo C, Seeliger B, Mascagni P, Agnus V, et al.. Hyperspectral enhanced reality (hyper): a physiology-based surgical guidance tool. Surg Endosc. (2020) 34:1736–44. doi: 10.1007/s00464-019-06959-9
64. Son GM, Ahn H-M, Lee IY, Ha GW. Multifunctional indocyanine green applications for fluorescence-guided laparoscopic colorectal surgery. Ann Coloproctol. (2021) 37:133. doi: 10.3393/ac.2021.05.07
65. Serra-Aracil X, García-Nalda A, Serra-Gómez B, Serra-Gómez A, Mora-López L, Pallisera-Lloveras A, et al.. Experimental study of the quantification of indocyanine green fluorescence in ischemic and non-ischemic anastomoses, using the SERGREEN software program. Sci Rep. (2022) 12:13120. doi: 10.1038/s41598-022-17395-6
66. Amagai H, Miyauchi H, Muto Y, Uesato M, Ohira G, Imanishi S, et al.. Clinical utility of transanal indocyanine green near-infrared fluorescence imaging for evaluation of colorectal anastomotic perfusion. Surg Endosc. (2020) 34:5283–93. doi: 10.1007/s00464-019-07315-7
67. Gomez-Rosado J-C, Valdes-Hernandez J, Cintas-Catena J, Cano-Matias A, Perez-Sanchez A. Feasibility of quantitative analysis of colonic perfusion using indocyanine green to prevent anastomotic leak in colorectal surgery. Surg Endosc. (2022) 36(2):1688–95. doi: 10.1007/s00464-021-08918-9
68. Hayami S, Matsuda K, Iwamoto H, Ueno M, Kawai M, Hirono S, et al. Visualization and quantification of anastomotic perfusion in colorectal surgery using near-infrared fluorescence. Tech Coloproctol. (2019) 23:973–80. doi: 10.1007/s10151-019-02089-5
69. Iwamoto H, Matsuda K, Hayami S, Tamura K, Mitani Y, Mizumoto Y, et al. Quantitative indocyanine green fluorescence imaging used to predict anastomotic leakage focused on rectal stump during laparoscopic anterior resection. J Laparoendosc Adv Surg Tech. (2020) 30:542–6. doi: 10.1089/lap.2019.0788
70. Son GM, Kwon MS, Kim Y, Kim J, Kim SH, Lee JW. Quantitative analysis of colon perfusion pattern using indocyanine green (ICG) angiography in laparoscopic colorectal surgery. Surg Endosc. (2019) 33:1640–9. doi: 10.1007/s00464-018-6439-y
71. Wada T, Kawada K, Takahashi R, Yoshitomi M, Hida K, Hasegawa S, et al. ICG fluorescence imaging for quantitative evaluation of colonic perfusion in laparoscopic colorectal surgery. Surg Endosc. (2017) 31:4184–93. doi: 10.1007/s00464-017-5475-3
72. Diana M, Noll E, Diemunsch P, Dallemagne B, Benahmed MA, Agnus V, et al. Enhanced-reality video fluorescence: a real-time assessment of intestinal viability. Ann Surg. (2014) 259:700–7. doi: 10.1097/SLA.0b013e31828d4ab3
73. Galema HA, Meijer RP, Lauwerends LJ, Verhoef C, Burggraaf J, Vahrmeijer AL, et al. Fluorescence-guided surgery in colorectal cancer; a review on clinical results and future perspectives. Eur J Surg Oncol. (2022) 48:810–21. doi: 10.1016/j.ejso.2021.10.005
74. Haslik W, Pluschnig U, Steger GG, Zielinski CC, Schrögendorfer K, Nedomansky J, et al. Indocyanine green video angiography predicts outcome of extravasation injuries. PLoS One. (2014) 9:e103649. doi: 10.1371/journal.pone.0103649
75. Moyer HR, Losken A. Predicting mastectomy skin flap necrosis with indocyanine green angiography: the gray area defined. Plast Reconstr Surg. (2012) 129:1043–8. doi: 10.1097/PRS.0b013e31824a2b02
76. Wexner S, Abu-Gazala M, Boni L, Buxey K, Cahill R, Carus T, et al. Use of fluorescence imaging and indocyanine green during colorectal surgery: results of an intercontinental Delphi survey. Surgery. (2022) 172:S38–S45. doi: 10.1016/j.surg.2022.04.016
77. Seeliger B, Walz MK, Alesina PF, Agnus V, Pop R, Barberio M, et al. Fluorescence-enabled assessment of adrenal gland localization and perfusion in posterior retroperitoneoscopic adrenal surgery in a preclinical model. Surg Endosc. (2020) 34:1401–11. doi: 10.1007/s00464-019-06997-3
78. Liu YZ, Shah SK, Sanders CM, Nwaiwu CA, Dechert AF, Mehrotra S, et al. Utility and usability of laser speckle contrast imaging (LSCI) for displaying real-time tissue perfusion/blood flow in robot-assisted surgery (RAS): comparison to indocyanine green (ICG) and use in laparoscopic surgery. Surg Endosc. (2023) 37:4803–11. doi: 10.1007/s00464-022-09590-3
79. Bunke J, Sheikh R, Reistad N, Malmsjö M. Extended-wavelength diffuse reflectance spectroscopy for a comprehensive view of blood perfusion and tissue response in human forearm skin. Microvasc Res. (2019) 124:1–5. doi: 10.1016/j.mvr.2019.02.001
80. Zötterman J, Mirdell R, Horsten S, Farnebo S, Tesselaar E. Methodological concerns with laser speckle contrast imaging in clinical evaluation of microcirculation. PLoS One. (2017) 12:e0174703. doi: 10.1371/journal.pone.0174703
Keywords: hyperspectral imaging, laparoscopy, minimally invasive surgery, tissue oxygenation, StO2, anastomosis
Citation: MacCormac O, Horgan CC, Waterhouse D, Noonan P, Janatka M, Miles R, Jacobs J, Dockerill C, Trotouin T, Schizas A, Seeliger B, Ourselin S, Ebner M, Vercauteren T and Shapey J (2025) Hyperspectral abdominal laparoscopy with real-time quantitative tissue oxygenation imaging: a live porcine study. Front. Med. Technol. 7:1549245. doi: 10.3389/fmedt.2025.1549245
Received: 20 December 2024; Accepted: 20 May 2025;
Published: 5 June 2025.
Edited by:
Michael Liebman, IPQ Analytics, United StatesReviewed by:
Nicole Buote, College of Veterinary Medicine, Cornell University, United StatesJames A. Bailey, University of Nottingham, United Kingdom
Joel Cazares, School of Medicine, Juntendo University, Japan
Copyright: © 2025 MacCormac, Horgan, Waterhouse, Noonan, Janatka, Miles, Jacobs, Dockerill, Trotouin, Schizas, Seeliger, Ourselin, Ebner, Vercauteren and Shapey. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oscar MacCormac, b3NjYXIuai5tYWNjb3JtYWNAa2NsLmFjLnVr