 Marco A. Arizmendi-Villarreal1,†
Marco A. Arizmendi-Villarreal1,† Alejandro Diaz Gonzalez-Colmenero1,†
Alejandro Diaz Gonzalez-Colmenero1,† Jorge A. Cantú-Hernández1
Jorge A. Cantú-Hernández1 Javier Sanchez-Maldonado2Gerardo E. Muñoz-Maldonado1Edelmiro Perez-Rodriguez2Homero A. Zapata-Chavira2Rene Rodriguez-Gutierrez3,4Francisco J. Reyna-Sepulveda2*
Javier Sanchez-Maldonado2Gerardo E. Muñoz-Maldonado1Edelmiro Perez-Rodriguez2Homero A. Zapata-Chavira2Rene Rodriguez-Gutierrez3,4Francisco J. Reyna-Sepulveda2*
- 1Department of General Surgery, Hospital Universitario “Dr. José Eleuterio González”, Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 2Department of Transplantation, Hospital Universitario “Dr. José Eleuterio González”, Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 3Department of Endocrinology, Hospital Universitario “Dr. José Eleuterio González”, Universidad Autónoma de Nuevo León, Monterrey, Mexico
- 4Plataforma INVEST Medicina UANL – KER Unit Mayo Clinic (KER Unit México), Universidad Autónoma de Nuevo León, Monterrey, Mexico
Introduction: Warm ischemia during kidney transplantation contributes to graft dysfunction. External cooling devices have been developed to preserve graft during anastomosis, with promising results in experimental models. A systematic review and meta-analysis were conducted to evaluate the effectiveness of renal cooling devices.
Methods: A comprehensive search of seven databases was performed from inception to January 6, 2023. Eligible studies were randomized, prospective, and included a control group. Four studies met the inclusion criteria. The protocol was registered in PROSPERO (CRD42023409480).
Results: All studies reported significantly lower reperfusion temperatures in kidneys treated with cooling devices compared to controls. Histological graft injury, showed no statistically significant difference (SMD −0.95; 95% CI −10.74 to 8.83). However, post-transplant urinary output was significantly higher in the cooling device groups (SMD 0.49; 95% CI 0.10 to 0.88).
Discussion: The overall risk of bias across included studies was high. Cooling devices effectively lower graft temperature and may improve early functional outcomes. However, evidence of histological benefit remains inconclusive. Further clinical trials are needed to confirm efficacy and standardize device implementation in human transplantation.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42023409480, PROSPERO CRD42023409480.
1 Introduction
Kidney transplantation is the most frequently performed organ transplant, accounting for 102,090 procedures worldwide and representing 65% of all solid organ transplants (1). Maintaining the function of the transplanted kidney is essential in kidney transplantation. The outcome of graft function is affected by the duration of the transplant, and the type of ischemia, especially in marginal organs, which have a higher rate of developing delayed graft function (2–4).
Ischemia in the organ can be classified into cold ischemia time (CIT), which is the time from exsanguination and immersion in cold solutions for preservation until the graft exits hypothermia. Warm ischemia time (WIT) is recognized in two phases: the first occurs during procurement, and the second develops during the vascular anastomosis in the recipient (5, 6).
It is recommended to limit the WIT to 30 min in order to reduce the risk of interstitial fibrosis, tubular atrophy, delayed graft function, graft failure, patient mortality, and long-term survival outcomes (7–10). In open surgical techniques, vascular anastomosis typically takes approximately 45 min (4). With the introduction of minimally invasive techniques in renal transplant (robotic and laparoscopic), the anastomosis time has been further extended compared to the open technique (11).
There are currently hypothermic technologies to maintain and even improve the condition of the organ prior to transplantation (12). Multiple methods have focused on organ preservation during transport, including advancing perfusion machines. However, the strategies to induce CIT involve direct interaction with either the preservation environment (e.g., cold static storage) or the vascular system (e.g., perfusion machines), making them inapplicable during the transplantation itself (13).
Traditionally, the most common strategy is the installation of ice water around the kidney, which is a rudimentary and ineffective (14). This has triggered a window of opportunity for developing techniques and devices to mitigate warm ischemia during anastomosis. In response, a range of novel cooling devices have emerged, from frozen pads to pumped cooling systems have been designed to reduce tissue injury (4, 5). Given the increasing diversity and clinical interest in these technologies, the aim of this systematic review is to evaluate all the cooling devices available to avoid warm ischemia time injury during kidney transplantation.
2 Materials and methods
The protocol for this systematic review and meta-analysis was registered within the International Prospective Register of Systematic Reviews (PROSPERO) on April 25th, 2024 (protocol ID: CRD42023409480), and it is based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines (15). The Cochrane Handbook for Systematic Reviews of Interventions, version 6.3.2, was thoroughly followed throughout all stages of the study (16).
2.1 Literature search
An experienced investigator screened the potential research studies by running a search strategy from inception to January 6, 2023, in seven electronic databases: MEDLINE, Embase, Web of Science, Scopus, Cochrane Central Register of Controlled Trials, EBSCOhost, and Latin American and Caribbean Health Sciences Literature Database (LILACS). The search strategy involved employing both keywords and free-text terms to explore relevant studies about external cooling devices to preserve a kidney graft during a transplant procedure. Both studies that tested a cooling device (CD) in vivo animal models or human patients were included. Terms such as “graft, kidney”, “cooling system”, “cooling apparatus” and “cooling device” were used during the search strategy. The results were complemented by screening reference lists, grey literature, and contacting experts in the field. The full search strategy is presented in Supplementary Material.
2.2 Eligibility criteria
Studies with a randomized, interventional, and comparative design were included. For studies conducted with animal models, they were considered eligible if: (1) used swine as animal models, since they have numerous anatomical and functional similarities with humans, (2) maintained the animal subjects under standard conditions, with water and food provided ad libitum, (3) average weight for their age, and (4) were submitted to the transplant procedure under an appropriate anesthesia protocol. Common inclusion criteria included: (1) the use of an external cooling device during the kidney transplant in at least one of the study groups, and (2) at least one study group underwent the kidney transplant without the external cooling device, independently of the technique used (standard, robot-assisted, or laparoscopic). Studies were excluded if they had a single-arm design, compared two or more external cooling devices without including a control group, were an ex vivo animal model study, or had no outcomes of interest reported by the authors. We avoid including case-control studies, systematic reviews, meta-analyses, case reports, basic science research, conference abstracts, letters to the editor, and literature reviews. Studies were not excluded by terms of subjects' sex, year of publication, language, study setting, or time frame.
Studies without a control group were excluded to ensure the methodological integrity of the review and allow for valid comparisons of outcomes. The absence of a comparator group limits the ability to isolate the effect of the cooling intervention from confounding variables or natural variability in perioperative care. Including only comparative studies enhances internal validity and facilitates a more accurate assessment of the effectiveness and safety of external cooling devices during kidney transplantation.
2.3 Selection process
Before every screening phase was conducted, a pre-screening pilot phase was carried out among four independent reviewers to adjust their attachment to the selection criteria. Between reviewers' agreement was estimated using the Fleiss' Kappa index, considering a value ≥0.70 as an acceptable cut-off value. The reviewers systematically screened all the studies, independently and blinded, by their abstracts and full text. Any disagreement was solved by consulting an additional reviewer who is an expert in the field (FRS). A detailed graphical representation of the global screening process is shown in (Figure 1).
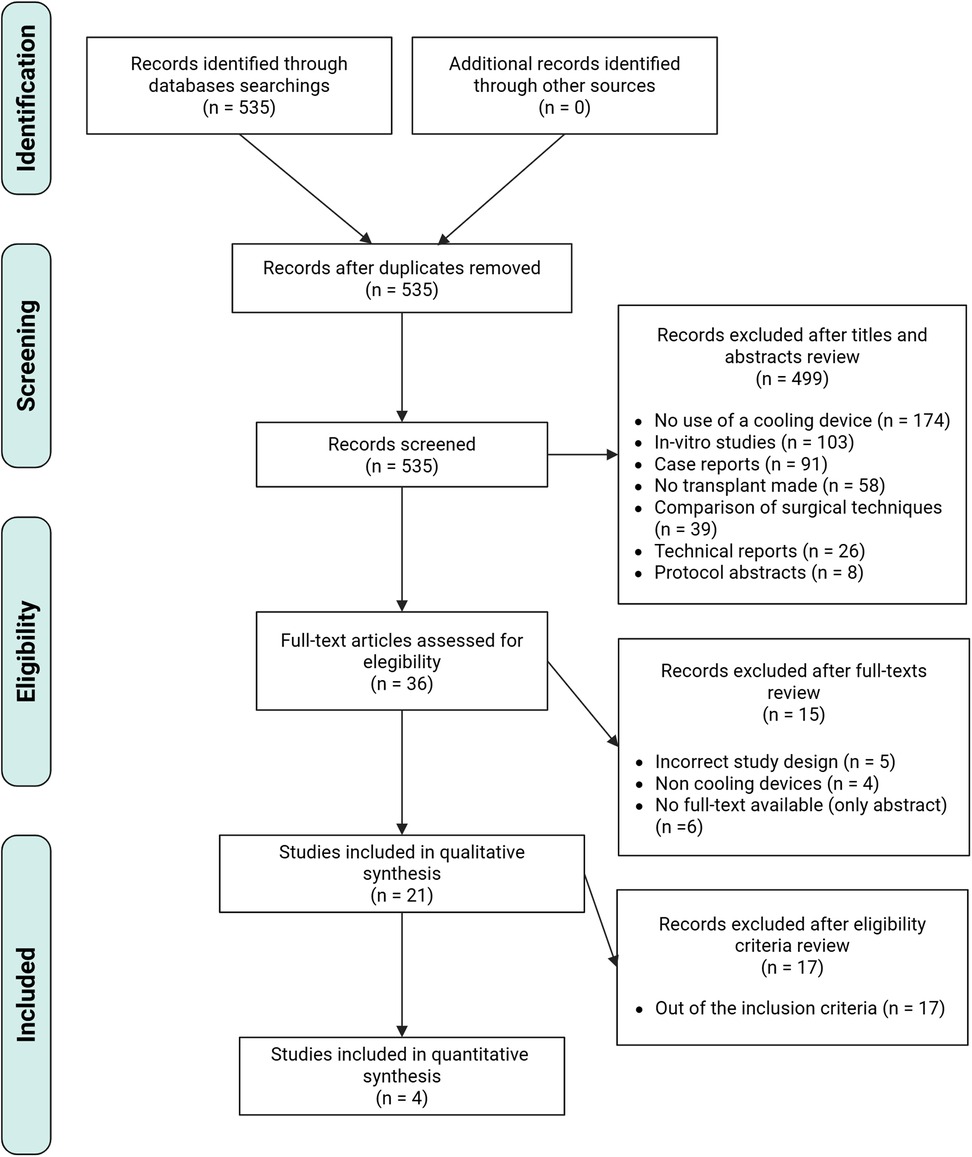
Figure 1. PRISMA flow chart. Overview of all the studies identified, screened and included in the analysis.
2.4 Data extraction, synthesis, and analysis
A pre-designed extensive database was used for data extraction, based on the specifications described in the Cochrane Handbook for Systematic Reviews (16). For each reference included, descriptive and outcome-related data were extracted. In cases where data was only available in graphic resources (e.g., plots), a web-based digital tool (“WebPlotDigitizer”, https://apps.automeris.io/wpd/) was used to extract quantitative data.
Outcome-related data from primary and secondary outcomes were extracted as Mean ± Standard Deviation (SD) of the scores from the clinical tools used for their assessment. When data was reported as Mean ± Standard Estimate Mean (SEM), SD was obtained by multiplying the SEM by the square root of the sample size n of the group (17):
Incase a study omitted or unclearly reported an outcome, a letter was sent via email to the corresponding author to make contact and retrieve missing data.
2.5 Outcomes of interest
Primary outcomes assessment included objective indicators of the kidney graft's functionality and integrity, such as histological preservation of the nephron, and urinary output after the transplant procedure.
These outcomes were evaluated through:
1. Goujon's score: originally evaluated eight histopathological parameters (apical cytoplasm vacuolization, tubular necrosis, tubular dilatation, cell detachment, brush border integrity, intracellular edema, denuded basement membrane, mitochondria integrity) using an ordinal scale from 1 to 5, and consist in the following criteria: 1, no abnormality; 2, mild lesions affecting 10% or less of kidney samples; 3, lesions affecting 25% of kidney samples; 4, lesions affecting 50% of kidney samples; and 5, lesions affecting 75% or more of kidney samples (18). This score, and its modified version, which uses the same scale, but only assesses four histopathological parameters (percentage of glomerular flocculus retraction in Bowman's space, brush border loss, lumina of tubules with cellular debris, and tubular dilatation) are widely used for the histological integrity assessment of renal tissue, specifically after and intervention for its preservation is made.
2. Urinary output: Measured as the milliliters per hour produced by the transplanted kidney during the postoperative period of the study subjects.
Secondary outcomes include graft management and indirect preservation indicators, such as surgical time, warm and cold ischemia time, graft temperature during and after the transplant procedure, and time of anastomosis. These were measured in controlled conditions, in a standardized fashion described by each author. All outcomes were extracted as means and standard deviations.
2.6 Assessing the risk of bias
Two reviewers independently assessed the risk of bias from the selected studies through one of two possible tools. For studies conducted in animal models, the Systematic Review Centre for Laboratory Animal Experimentation (SYRCLE tool) was used (19, 20). This tool is composed of ten signaling questions, which assess methodological bias in six domains (selection, performance, detection, attrition, reporting, and other type of bias).
2.7 Published specifications of experimental cooling devices
We evaluated the studies reporting the use of renal cooling devices, regardless of whether a control group was included, surgical approach, experimental model, and outcome. For each study, we identified and compiled the technical specifications and reported properties of the cooling devices, as described by the inventors or authors. This approach allowed us to compare the various techniques implemented to protect the kidney from warm ischemia. The following characteristics were assessed: device material, manufacturing process, tubing configuration, sterilization methods, type of flow control system, coolant type, temperature monitoring mechanisms, presence of a hilum access window, compatibility with different surgical approaches, and the experimental model in which the device was tested.
2.8 Statistical analysis
Analysis of the overall histological preservation was made by pooling the weighted mean treatment effect, based on the standardized mean difference (between-groups Hedge's g) between the Goujon scores (simple or modified) obtained by both intervention and control groups at follow-up. The mean difference was standardized using the pooled SDΔ and corrected for bias due to small sample size. For the interpretation of the effect's magnitude, the following cut-off values were considered (Cohen, 1988): ≥0.8 = large; 0.2–0.5 = medium; and ≤0.2 = small. Since significant heterogeneity between studies was expected due to numerous methodological aspects, a Random-Effects Model was used to pool all overall outcomes.
For the secondary outcomes, the analysis of the weighted mean treatment differences in the evaluation of other functional indicators of the graft (urinary output) and surgical management (surgical time, time of anastomosis, length of cold and warm ischemia periods, and graft temperature at reperfusion) was made through the pooling of the standardized mean difference between measures obtained by both intervention and control groups.
To appraise heterogeneity, Cochran's Q-statistic was employed, adopting a significance threshold of p < 0.10. Additionally, the I2-statistic quantified the proportion of variability attributed to heterogeneity, with values surpassing 50% denoting substantial heterogeneity. Forest plots were used to represent the calculated mean differences graphically. No sensitivity or subgroup analyses were made due to the restricted number of articles used for quantitative analysis. Data analysis was made using meta and dmetar packages in the R statistical version R.4.2.3 software (Posit PBC, Boston, United States).
3 Results
We identified 535 studies after the electronic search. After the abstract screening phase, we included 36 studies to evaluate the full manuscript. We excluded 15 studies and finally included 21 studies (3, 4, 11, 21–38) for the qualitative synthesis, and 4 studies (4, 11, 21, 22) included in quantitative synthesis. Further details are shown in (Figure 1) using the PRISMA flow chart. Four studies included animal model. In total, 70 animals were in the quantitative studies.
3.1 Study characteristics
A general description of the included studies is presented in (Table 1). All animal models used a porcine model. Three studies included a cooling jacket device with a cold between 0 and 4°C liquid infusion circuit to preserve temperature. One study used an isolation bag preservation (organ pocket), the solutions varied between studies. From the animal studies, 2 used an open technique and 2 used minimal-invasive techniques, including robotic and laparoscopic techniques. Only two animal studies used a direct measurement technique to describe the mean renal temperature after reperfusion. The surgical time in the animal models was similar between groups. Warm ischemia time was reported in all animal studies. Histological outcomes were reported in two of the animal studies using the Goujon score.
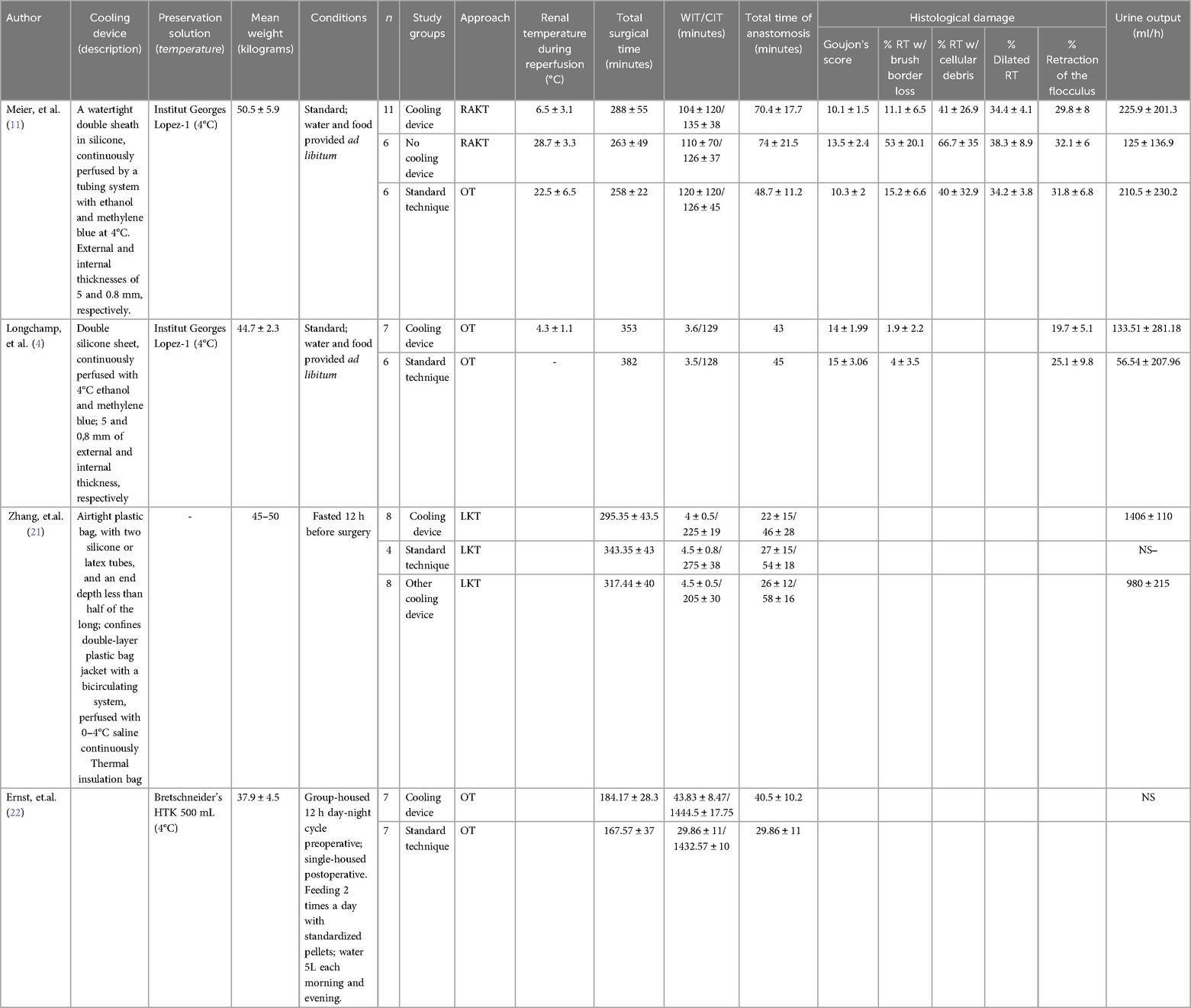
Table 1. Characteristics of animal model articles.
3.1.1 Histological outcomes
Two animal studies reported the Goujon score (30 porcine models: Cooling device: 18 Non-cooling devices: 12). There was no difference between cooling device and non-cooling device [SMD −0.95 (−10.7–8.8)] with high heterogeneity (I = 71%, p. 0.06) (Figure 2).
![Forest plot showing standardized mean difference for studies by Meier et al. and Longchamp et al. Both studies favor omitting the cooling device. Meier et al. has an SMD of -1.74 with a 95% confidence interval of [-2.94, -0.55] and a weight of 48.7%. Longchamp et al. has an SMD of -0.20 with a 95% confidence interval of [-1.30, 0.89] and a weight of 51.3%. Combined random effects model shows an SMD of -0.95 [-10.74, 8.83] with a heterogeneity of I² = 71% and p = 0.06.](https://www.frontiersin.org/files/Articles/1600784/fmedt-07-1600784-HTML/image_m/fmedt-07-1600784-g002.jpg)
Figure 2. General description of the difference in Goujon score (histopathological damage).
3.1.2 Urine outcomes
Two animal studies reported the total urine volume after auto-transplant (30 porcine models: Cooling device: 18 non-cooling devices: 12). The meta-analysis reported a positive difference favoring the cooling device group. [SMD 0.50 (0.1–0.89)] with no heterogeneity (I = 0%, p = 0.9) (Figure 3).
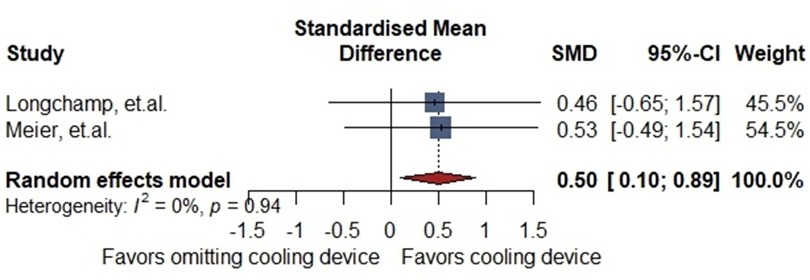
Figure 3. General description of the difference in post-transplant urinary volume.
3.2 Risk of bias
The quality assessment of animal studies is demonstrated (Table 2). Only one of the animal studies generated a random sequence with unknown allocation concealment; moreover, only one study used blinding for the intervention.
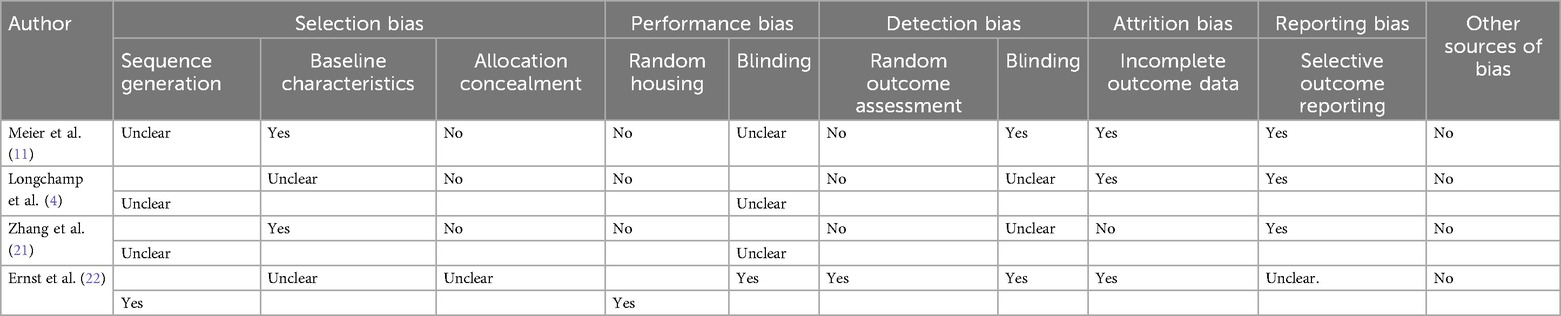
Table 2. Risk of bias for animal model studies (SYRCLE tool).
3.3 Published general characteristics of experimental cooling devices
Across the 36 studies reviewed, we identify 21 with a relevant description. A considerable variability in the design and reporting of renal cooling devices. Common materials included plastic polymers (silicone, polyethylene, polylactic acid), with one using aluminum (38). Manufacturing processes were inconsistently detailed; some used 3D printing (31, 35) or homemade sealed bags (21, 31, 34). Silicone or latex tubing was prevalent, but tubing configurations and flow control systems varied, ranging from manual irrigation to peristaltic pumps. Ice-cold saline was the standard coolant. Hilum access windows were frequently included. Devices were tested with open, laparoscopic, or robotic approaches and tested in animal or human models. Renal temperature monitoring during surgery was assessed using different methods across studies (Table 3).
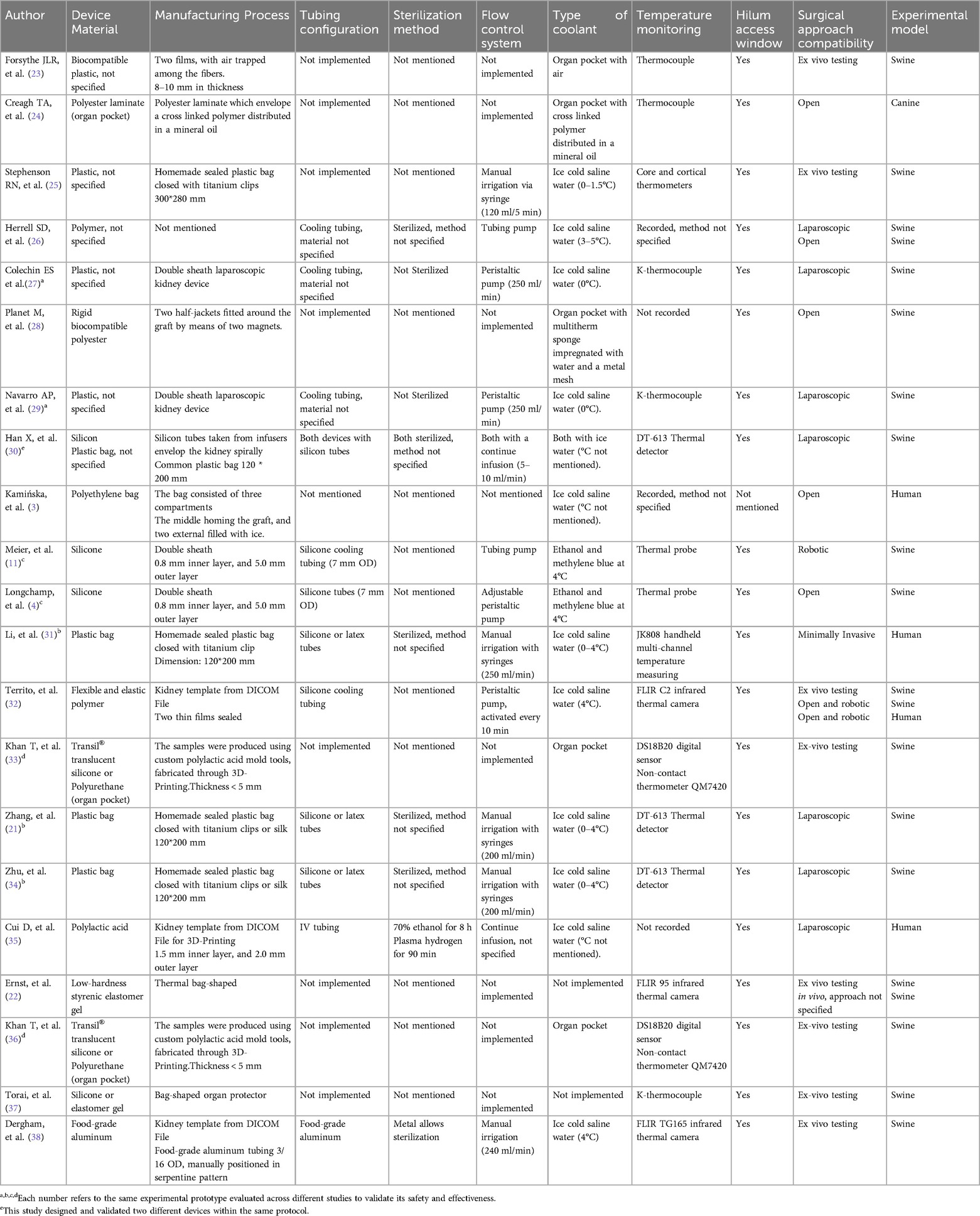
Table 3. Published general characteristics of experimental kidney cooling devices.
4 Discussion
Preclinical studies included in this systematic review did not demonstrate significant histological or clinical differences between groups receiving a cooling device and those undergoing standard procedures during kidney transplantation. Nevertheless, in all animal studies utilizing a cooling device, renal surface temperatures during vascular anastomosis were consistently maintained below 20°C, underscoring the device's effectiveness in mitigating warm ischemia (11, 21, 22). To further assess its impact, we conducted two meta-analyses—one evaluating histological injury scores and the other analyzing urine output in swine models. While histological findings did not differ significantly between groups, the use of cooling devices was associated with a notable increase in post-reperfusion urine production, suggesting improved early graft function.
Comparative analyses across surgical approaches—open, laparoscopic, and robotic—revealed no significant differences in temperature, histological, and clinical outcomes demonstrating the usefulness of these devices for minimally invasive transplant techniques. A previous systematic review identified 3 studies using cooling jackets with cold solution flow in robotic and laparoscopic kidney transplants. While these studies reported adequate surface cooling and acceptable anastomotic times, their lack of control groups limits the strength of the evidence and precludes firm conclusions regarding efficacy (14).
Previous experimental data have identified a critical thermal threshold between 15°C and 20°C, beyond which graft function may be compromised. It is well established that for every additional 10 min of exposure to temperatures above this threshold, the risk of delayed graft function (DGF) and acute rejection increases proportionally in human studies (39, 40). Based on the translation potential of this technology, we found only one clinical study that included 46 kidney transplant recipients using a cooling device with an ice-cooled sterile saline solution in an open technique, utilizing a paired-donor allograft model and control group. The cooling device showed a significantly lower rate of detrimental events (delayed graft function and/or acute rejection) as well a higher glomerular filtration rate on day 14 and a greater decrease of MMP9 and LCN2 gene expression, they demonstrated a statistically significant benefit from using a cooling device compared to the control group (3). No statistically significant difference in the main histological features and Remuzzi score with the cooling device and without it (2.4 ± 1.5 vs. 2.6 ± 1.6).
No included study provided a direct comparison between different cooling device designs, and there is currently no evidence supporting the superiority of one configuration over another. The clinical implementation of renal cooling devices faces significant logistical barriers due to the lack of standardization in design, sterilization protocols, and surgical compatibility and minimal time of use per surgery, which complicates routine use. Cost limitations arise from high production expenses, absence of scalable manufacturing, and an unclear cost-benefit ratio given the limited clinical outcome data. From a safety perspective, insufficient reporting on biomaterials, sterilization methods, and adverse events raises concerns about patient risk and regulatory approval. Finally, effectiveness remains uncertain, as no study directly compares devices or provides robust evidence on long-term graft outcomes, hindering the establishment of a superior technique.
To our knowledge, this is the first systematic review focus specifically on purpose-designed cooling devices to prevent warm ischemia in kidney transplants evaluated under standardized experimental conditions with appropriate control arms. In contrast, the review by Andras et al. included studies of a broader array of interventions, including slush ice, cold saline, gauze jackets, and cooling jackets, and most of the studies lacked design specificity or translational potential (14). In contrast, our review exclusively included cooling devices intended for clinical application and supported by preclinical evidence of thermal transfer, histological, and clinical outcomes.
The emergence of robotic and laparoscopic techniques in renal transplantation, while offering numerous surgical advantages, has been associated with prolonged vascular anastomosis times and, consequently, extended warm ischemia periods (41). Cooling devices present a promising and safe intervention to mitigate the adverse impact of this limitation on graft function. Future clinical studies should aim to identify the most effective device configurations and evaluate their application in minimally invasive settings. Moreover, these technologies hold particular promise for high-risk subpopulations predisposed to longer anastomosis times, such as obese recipients or those receiving right-sided donor kidneys (42). To establish the role of cooling devices as a standard of care during vascular anastomosis, robust evidence from randomized controlled trials is essential. One such trial, currently underway, is a single-center study evaluating the Kidney Skin System, registered on ClinicalTrials.gov with a projected two-year duration. The results of this trial may provide critical insight into the clinical utility and standardization of cooling devices in contemporary transplant surgery.
4.1 Limitations
This study has several limitations. First, the evidence based on preclinical studies with animal models, which may not be replicated in clinical studies, particularly for the lack of long-term follow-up. While a high number of single-arm studies and case series don't report adverse outcomes using cooling devices, the absence of randomized controlled trials limits the strength of the conclusions that can be drawn. Second, we have excluded a high amount of studies due to the strict criteria of inclusion of studies with the intervention without a control group. This, means that we only obtained a four preclinical studies in animals, limiting the performance of the meta-analysis. Third, the screened records exhibited a high risk of outcome reporting bias, which may impact the reliability of our findings. To mitigate this during the study selection process, we employed a comprehensive and systematic approach based on predefined inclusion criteria. Specifically, we included all studies that reported any clinical or experimental evaluation of cooling devices, irrespective of whether the outcomes were positive, negative, or inconclusive. Additionally, none of the studies have explored the short-term and long-term security profile of the devices including the prolonged anastomosis time, increased risk of wound infection, elevated costs, or other associated complications. Finally, a significant limitation across the included studies is the insufficient reporting of key technical aspects of the cooling devices. Most publications lacked detailed descriptions of the device design, the biomaterials employed, sterilization methods. Also, the high variety of strategies used to monitor thermal transfer at the renal surface. This lack of standardized reporting impairs the ability to critically assess the safety and efficacy of the inventions.
5 Conclusion
Our systematic review underscores a critical gap in high-quality, controlled human studies evaluating the efficacy and safety of cooling devices in renal transplantation. Although animal models suggest these devices may enhance early graft function, particularly through increased urine output and protection from warm ischemia, the extrapolation of these findings to clinical practice remains speculative. A major limitation across the literature is the lack of standardized and detailed descriptions regarding device design, functional mechanisms, biomaterials used, and sterilization protocols. This absence of transparency hinders reproducibility, regulatory evaluation, and the development of a consensus process on its implementation. Moreover, the current lack of comparative analyses between device models limits the identification of an optimal design. As minimally invasive techniques continue to extend warm ischemia times, the role of cooling devices may become increasingly critical. The transplantation community must now critically examine if we are ready to embrace these innovations without first demanding standardization, transparency, and evidence of long-term safety.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
MA-V: Conceptualization, Investigation, Writing – original draft. ADG-C: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. JC-H: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. JS-M: Investigation, Project administration, Writing – original draft. GM-M: Funding acquisition, Writing – review & editing. EP-R: Funding acquisition, Writing – review & editing. HZ-C: Funding acquisition, Writing – review & editing. RR-G: Formal analysis, Methodology, Validation, Writing – review & editing. FR-S: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
Our deepest gratitude to the authorities involved in the development of this work for all the resources and the access to the information. To our tutors, we extend our sincere gratitude for their invaluable guidance and constant support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmedt.2025.1600784/full#supplementary-material
Abbreviations
BPAR, biopsy proven acute rejection; CD, cooling device; CIT, cold ischemia time; DGF, delayed graft function; OT, open transplant; PRISMA, preferred reporting items for systematic review and meta-analysis; RAKT, robot assisted kidney transplant; SD, standard deviation; SEM, standard estimate mean; SYRCLE, systematic review center for laboratory animals experimentation; WIT, warm ischemia time.
References
1. World Health Organization. Global Observatory on Donation and Transplantation. Geneva: World Health Organization (2022). Available online at: https://www.transplant-observatory.org/wp-content/uploads/2023/11/2022-data-global-report_VF_2.pdf (Accessed January 14, 2025).
2. Hellegering J, Visser J, Kloke HJ, D'Ancona FC, Hoitsma AJ, van der Vliet JA, et al. Deleterious influence of prolonged warm ischemia in living donor kidney transplantation. Transplant Proc. (2012) 44(5):1222–6. doi: 10.1016/j.transproceed.2012.01.118
3. Kamińska D, Kościelska-Kasprzak K, Chudoba P, Hałoń A, Mazanowska O, Gomółkiewicz A, et al. The influence of warm ischemia elimination on kidney injury during transplantation - clinical and molecular study. Sci Rep. (2016) 6, 36118. doi: 10.1038/srep36118
4. Longchamp A, Meier RPH, Colucci N, Balaphas A, Orci LA, Nastasi A, et al. Impact of an intra-abdominal cooling device during open kidney transplantation in pigs. Swiss Med Wkly. (2019) 149:w20143. doi: 10.4414/smw.2019.20143
5. Oweira H, Ramouz A, Ghamarnejad O, Khajeh E, Ali-Hasan-Al-Saegh S, Nikbakhsh R, et al. Risk factors of rejection in renal transplant recipients: a narrative review. J Clin Med. (2022) 11(5):1392. doi: 10.3390/jcm11051392
6. Marzouk K, Lawen J, Alwayn I, Kiberd BA. The impact of vascular anastomosis time on early kidney transplant outcomes. Transplant Res. (2013) 2:1–5. doi: 10.1186/2047-1440-2-8
8. Tennankore KK, Kim SJ, Alwayn IP, Kiberd BA. Prolonged warm ischemia time is associated with graft failure and mortality after kidney transplantation. Kidney Int. (2016) 89(3):648–58. doi: 10.1016/j.kint.2015.09.002
9. Heylen L, Naesens M, Jochmans I, Monbaliu D, Lerut E, Claes K, et al. The effect of anastomosis time on outcome in recipients of kidneys donated after brain death: a cohort study. Am J Transplant. (2015) 15(11):2900–7. doi: 10.1111/ajt.13397
10. Weissenbacher A, Oberhuber R, Cardini B, Weiss S, Ulmer H, Bösmüller C, et al. The faster the better: anastomosis time influences patient survival after deceased donor kidney transplantation. Transpl Int. (2015) 28(5):535–43. doi: 10.1111/tri.12516
11. Meier RPH, Piller V, Hagen ME, Joliat C, Buchs JB, Nastasi A, et al. Intra-abdominal cooling system limits ischemia-reperfusion injury during robot-assisted renal transplantation. Am J Transplant. (2018) 18(1):53–62. doi: 10.1111/ajt.14399
12. Higashi Y, Homma J, Sekine H, Yago H, Kobayashi E, Shimizu T. External pressure dynamics promote kidney viability and perfusate filtration during ex vivo kidney perfusion. Sci Rep. (2022) 12(1):21564. doi: 10.1038/s41598-022-26147-5
13. Zulpaite R, Miknevicius P, Leber B, Strupas K, Stiegler P, Schemmer P. Ex-vivo kidney machine perfusion: therapeutic potential. Front. Med. (2021) 8:808719. doi: 10.3389/fmed.2021.808719
14. Andras I, Piana A, Verri P, Telecan T, Gallioli A, Prudhomme T, et al. Systematic review of techniques and devices used to avoid warm ischemia time injury during kidney transplantation. World J Urol. (2023) 41(4):993–1003. doi: 10.1007/s00345-023-04328-9
15. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. (2021) 134:103–12. doi: 10.1016/j.jclinepi.2021.02.003
16. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Chichester: John Wiley & Sons (2019).
17. Thalheimer W, Cook S. How to Calculate Effect Sizes from Published Research: A Simplified Methodology. Somerville, MA: Work-Learning Research, Inc. (2009). Published online.
18. Goujon JM, Hauet T, Menet E, Levillain P, Babin P, Carretier M. Histological evaluation of proximal tubule cell injury in isolated perfused pig kidneys exposed to cold ischemia. J Surg Res. (1999) 82(2):228–33. doi: 10.1006/jsre.1998.5526
19. Hooijmans CR, Rovers MM, de Vries RB, Leenaars M, Ritskes-Hoitinga M, Langendam MW. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. (2014) 14(1):43. doi: 10.1186/1471-2288-14-43
20. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
21. Zhang P, Han X, Zhang X, Zhu X, Li T, Li Y, et al. A controllable double-cycle cryogenic device inducing hypothermia for laparoscopic orthotopic kidney transplantation in swine. Transl Androl Urol. (2021) 10(7):3046–55. doi: 10.21037/tau-21-544
22. Ernst L, Czigany Z, Paschenda P, Schulz M, Breuer L, Kunczik J, et al. A proof-of-concept preclinical study using a novel thermal insulation device in a porcine kidney auto-transplantation model. Int J Mol Sci. (2022) 23(22):13806. doi: 10.3390/ijms232213806
23. Forsythe JL, Dunnigan PM, Proud G, Lennard TW, Taylor RM. Reducing renal injury during transplantation. Br J Surg. (1989) 76(10):999–1001. doi: 10.1002/bjs.1800761004
24. Creagh TA, McLoughlin F, Broe PJ, McLean PA, Murphy DM, Bouchier-Hayes DJ. A novel method of induced renal hypothermia. J Urol. (1992) 147(1):249–52. doi: 10.1016/S0022-5347(17)37207-5
25. Stephenson RN. A cooling jacket to reduce renal damage during transplantation. Br J Urol. (1993) 71(4):384–7. doi: 10.1111/j.1464-410X.1993.tb15977.x
26. Herrell SD, Jahoda AE, Husain AN, Albala DM. The laparoscopic cooling sheath: novel device for hypothermic preservation of kidney during temporary renal artery occlusion. J Endourol. (1998) 12(2):155–61. doi: 10.1089/end.1998.12.155
27. Colechin ES, Riddle J, Navarro AP, Soomro NA, Griffiths C. Laparoscopic renal cooling device. Med Biol Eng Comput. (2008) 46(12):1219–25. doi: 10.1007/s11517-008-0378-z
28. Planet M, Desgrandchamps F, Hauet T, Gourmel B, Goujon B, Carretier M, et al. Experimental study of a cooling jacket in renal transplantation. Transplant Proc. (2000) 32(2):493–5. doi: 10.1016/S0041-1345(00)00821-6
29. Navarro AP, Sohrabi S, Colechin E, Griffiths C, Talbot D, Soomro NA. Evaluation of the ischemic protection efficacy of a laparoscopic renal cooling device using renal transplantation viability assessment criteria in a porcine model. J Urol. (2008) 179(3):1184–9. doi: 10.1016/j.juro.2007.10.025
30. Han X, Zhang B, Yan W, Zhao Z, Gao Q, Zhang Y. Comparison of 2 devices in pigs to induce hypothermia in laparoscopic orthotopic kidney transplant. Exp Clin Transplant. (2012) 10(6):573–8. doi: 10.6002/ect.2012.0005
31. Li Y, Han X, Dagvadorj BU, Zhao Y, Zhang X, Zhu X, et al. An effective cooling device for minimal-incision kidney transplantation. Ann Transplant. (2020) 25:e928773. doi: 10.12659/AOT.928773
32. Territo A, Piana A, Fontana M, Diana P, Gallioli A, Gaya JM, et al. Step-by-step development of a cold ischemia device for open and robotic-assisted renal transplantation. Eur Urol. (2021) 80(6):738–45. doi: 10.1016/j.eururo.2021.05.026
33. Khan T, Kwarcinski J, Pang T, Hameed A, Boughton P, O'Grady G, et al. Protection from the second warm ischemic injury in kidney transplantation using an ex vivo porcine model and thermally insulating jackets. Transplant Proc. (2021) 53(2):750–4. doi: 10.1016/j.transproceed.2021.01.037
34. Zhu X, Zhao Y, Han X, Li Y, Zhang P, Wang S, et al. Extraperitoneal laparoscopic kidney transplantation: preliminary clinical experiences from China. Adv Ther. (2021) 38(3):1677–89. doi: 10.1007/s12325-021-01639-4
35. Cui D, Wu B, He D, Wang Y, Jiao Y, Zhang B. 3D-Printed cold preservation device in renal autotransplantation for the treatment of a patient with renal artery stenosis. Front Bioeng Biotechnol. (2022) 9:738434. doi: 10.3389/fbioe.2021.738434
36. Khan T, Kwarcinski J, Boughton P, Yoon P, Hameed A, Singla A, et al. Insulating jackets thermally protect kidneys in an ex vivo model of second warm ischemia. Artif Organs. (2023) 47(6):1038–45. doi: 10.1111/aor.14488
37. Torai S, Kurauchi K, Kobayashi E. Evaluating a new device for reducing second warm ischemia during organ transplantation in a porcine model of kidney, heart, and pancreas transplantation. Transplant Proc. (2023) 55(4):997–1004. doi: 10.1016/j.transproceed.2023.03.052
38. Dergham A, Witherspoon L, Power L, Nashed JY, Skinner TAA. A novel cooling device for kidney transplant surgery. Surg Innov. (2024) 31(4):400–6. doi: 10.1177/15533506241260087
39. Kuipers TG, Hellegering J, El Moumni M, Krikke C, Haveman JW, Berger SP, et al. Kidney temperature course during living organ procurement and transplantation. Transpl Int. (2017) 30(2):162–9. doi: 10.1111/tri.12892
40. Feuillu B, Cormier L, Frimat L, Kessler M, Amrani M, Mangin P, et al. Kidney warming during transplantation. Transpl Int. (2003) 16(5):307–12. doi: 10.1111/j.1432-2277.2003.tb00305.x
41. Wagenaar S, Nederhoed JH, Hoksbergen AWJ, Bonjer HJ, Wisselink W, van Ramshorst GH. Minimally invasive, laparoscopic, and robotic-assisted techniques versus open techniques for kidney transplant recipients: a systematic review. Eur Urol. (2017) 72(2):205–17. doi: 10.1016/j.eururo.2017.02.020
Keywords: ischemia-reperfusion injury, cold ischemia time, warm ischemia time, kidney transplantation, organ preservation
Citation: Arizmendi-Villarreal MA, Diaz Gonzalez-Colmenero A, Cantú-Hernández JA, Sanchez-Maldonado J, Muñoz-Maldonado GE, Perez-Rodriguez E, Zapata-Chavira HA, Rodriguez-Gutierrez R and Reyna-Sepulveda FJ (2025) Cooling devices used to avoid warm ischemia time injury during kidney transplantation. Systematic review and meta-analysis. Front. Med. Technol. 7:1600784. doi: 10.3389/fmedt.2025.1600784
Received: 26 March 2025; Accepted: 24 July 2025;
Published: 13 August 2025.
Edited by:
Laszlo Piros, Semmelweis University, HungaryReviewed by:
George Emilian Nita, Liverpool University Hospitals NHS Foundation Trust, United KingdomCseprekal Orsolya, Semmelweis University, Hungary
Copyright: © 2025 Arizmendi-Villarreal, Diaz Gonzalez-Colmenero, Cantú-Hernández, Sanchez-Maldonado, Muñoz-Maldonado, Perez-Rodriguez, Zapata-Chavira, Rodriguez-Gutierrez and Reyna-Sepulveda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francisco J. Reyna-Sepulveda, ZnJhbmNpc2NvLnJleW5hc0B1YW5sLmVkdS5teA==
†These authors have contributed equally to this work and share first authorship