 Véronique De Gucht
Véronique De Gucht Dion H. A. Woestenburg2†
Dion H. A. Woestenburg2† Vesna Vrecko Pizzulin
Vesna Vrecko Pizzulin- 1Research Group of Health, Medical and Neuropsychology, Institute of Psychology, Leiden University, Leiden, Netherlands
- 2Methodology and Statistics Research Unit, Institute of Psychology, Leiden University, Leiden, Netherlands
- 3Division of Surgery, University Medical Centre Ljubliana, Ljubliana, Slovenia
- 4Fresenius Medical Care Deutschland GmbH, Global Medical Office, Bad Homburg, Germany
- 5Department of Psychosomatic Medicine, Center of Internal Medicine and Dermatology, Charité Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin, Berlin Institute of Health, Berlin, Germany
- 6Center for Patient Centered Outcomes Research, Charité Universitätsmedizin Berlin (CPCOR), Berlin, Germany
Introduction: Fatigue is a prevalent and burdensome symptom in Chronic Kidney Disease (CKD), with major impact on Health-Related Quality of Life (HRQoL). Physical activity has been linked to improvements in both fatigue and HRQoL. This study examined whether physical activity relates to HRQoL indirectly through fatigue and whether this relationship is moderated by sleep quality.
Methods: A total of 465 CKD patients (mean age = 53.78 years; 50% female) participated in the study. Fatigue, physical activity, HRQoL, and sleep quality were assessed and compared to general population norms and across treatment modalities using t-tests and ANCOVAs. Mediation, moderation, and moderated mediation analyses were conducted.
Results: CKD patients reported lower physical activity levels, HRQoL, and sleep quality, and higher fatigue than the general population (all ps <.001). Among treatment groups, transplant recipients showed the most favorable outcomes, while patients without renal replacement therapy reported the poorest. Higher levels of physical activity were associated with better HRQoL indirectly through fatigue, with small to moderate effect sizes. Stronger associations observed in those reporting better sleep quality.
Discussion: These findings indicate that physical activity is associated with better HRQoL in CKD patients through its relationship with fatigue, particularly among those with good sleep quality. Future research should explore fatigue across CKD stages to optimize interventions that target both physical activity and sleep.
Introduction
Fatigue appears to be the main complaint in chronic kidney disease (CKD). In a healthy population, fatigue is reported in 5% to 45% of the cases (1). The prevalence of (chronic) fatigue in CKD is substantially higher and varies depending on the study from about 50% to 89% in hemodialysis (HD) (2). Very few studies focused however on peritoneal dialysis and transplant populations (3). Given its prevalence and burdensome nature, fatigue has been identified as a highly prioritized symptom to treat and investigate (4).
The biopsychosocial model of fatigue in CKD patients (5) hypothesizes fatigue is precipitated by physiological factors [uremia, anemia, blood pressure, inflammation (2, 6, 7)] and may be perpetuated by psycho-behavioral [psychological distress, sleep disturbances, physical activity, smoking, and cognitions (2)], and social factors (e.g. social support). However, specific determinants and causal mechanisms of fatigue in CKD patients are not well understood due to its complex multifaceted etiology (2, 8, 9) and the lack of longitudinal studies (2).
Fatigue has a profound direct and indirect negative effect on individuals’ functioning and quality of life. Consequences of fatigue are directly reflected in impaired functionality (10), disease progression, increased risk of hospitalization (11), and lower physical and mental Health-Related Quality of Life (HRQoL) (2, 12–14). Indirectly, fatigue may predict mortality through distress, impaired functioning and its consequences (15). It should, however, be noted that both fatigue and HRQOL differ by CKD treatment and modality (16, 17).
Poor sleep quality proved to be associated with more fatigue in patients on maintenance hemodialysis, while prolonged fatigue in these patients was associated with mortality (13). According to a review in hemodialysis patients, fatigue is especially related to poor physical HRQoL (18). Fatigue in patients with CKD, especially in patients on long-term dialysis, also leads to muscle wasting, resulting in inactivity or reduced physical activity which are in turn related to mortality (19, 20).
Experiential evidence shows physical activity decreases fatigue in CKD patients (9) and improves HRQoL (21). It is hypothesized physical activity has a positive, multifaceted effect (9) on fatigue due to its beneficial effect on pathophysiologic mechanisms of fatigue in CKD populations such as improved mental health, a positive effect on the cardiovascular and muscular system and reduced inflammation (9, 22, 23) which are evident across the whole spectrum of CKD (19). In addition, a systematic review by Zhao et al. (24), based on 13 randomized controlled trials, demonstrated that exercise interventions have a positive impact on fatigue as well as on both physical and mental HRQoL in CKD. Therefore, physical activity could be a promising target to alleviate fatigue in this population (9).
Sleep has an important regenerative and restorative function in an individual’s health (25). Unhealthy sleep, characterized as inappropriate length or quality, results in a myriad of negative consequences such as impaired daily functioning, poor quality of life (26), reduced well-being (25), and disease progression (27). Diminished sleep quality is assumed to be a significant determinant of fatigue in CKD patients (13, 28, 29).
Evidence suggests that physical activity benefits both fatigue and HRQoL in patients with CKD, and studies in healthy populations indicate that the association between physical activity and fatigue depends on sleep quality (30, 31). Yet, despite the high prevalence of fatigue and its association with poor sleep in CKD, little research has examined how these factors jointly shape the relationship between physical activity and HRQoL, leaving an important gap in understanding their combined roles.
Based on previous studies in healthy and CKD samples, we hypothesize that physical activity is indirectly associated with better physical and mental HRQoL through lower fatigue, and that this indirect association is stronger among CKD patients reporting better sleep quality.
The current study focuses on the following research questions (RQs):
● RQ-A: Compare fatigue, sleep, physical activity, and physical and mental HRQoL between patients with CKD and the general population.
● RQ-B: Compare fatigue, sleep, physical activity, and physical and mental HRQoL between treatment modalities within the CKD population.
● RQ-C: Investigate whether fatigue mediates the relationship between physical activity and physical and mental HRQoL.
● RQ-D: Investigate whether sleep moderates the relationship between physical activity and fatigue.
● RQ-E: If RQ-C and RQ-D are confirmed, examine whether sleep moderates the indirect relationship—mediated by fatigue—between physical activity and HRQoL.
Materials and methods
Study design
The study employed a cross-sectional design. Patients were recruited through the official German national patient association for kidney disease (Bundesverband Niere e.V.), in cooperation with Fresenius Medical Care Germany. An information letter, informed consent form, and the study questionnaire were published in the association’s quarterly journal Der Nierenpatient. Patients could detach the questionnaire from the journal, sign the informed consent form prior to completing it, and return both anonymously in a prepaid envelope to the patient association. Alternatively, after providing informed consent, participants had the option to complete the survey online via the survey tool LimeSurvey. Thus, participants could choose their preferred mode of participation and were given ten weeks to respond following publication in the journal. Inclusion criteria were age ≥18 years, a diagnosis of CKD, and residence in Germany. CKD status and treatment modality were self-reported.
A power analysis was conducted using GPower (32). Under a significant level of.05, a power of 95%, in total four covariates and medium effect size, a minimum of total 357 participants was required.
Ethical approval for the study was obtained from the Psychology Research Ethics Committee of Leiden University (proposal number CEP 18-0516/257). Data will be shared upon reasonable request to the first author.
Measures
The Short Form (SF)-12 (33) was used to assess physical and mental HRQoL. Twelve statements with varying response categories were converted into physical and mental standardized values. From the standardized values, a norm-based T-score is calculated for the physical and mental component, with higher scores indicating a better HRQoL. The SF-12 demonstrated good reliability, construct validity, and responsiveness (34) and test-retest reliability was supported in clinical patients (35).
Physical activity was assessed with the International Physical Activity Questionnaire-Short Form (IPAQ-SF), a valid and reliable tool (36) providing information on the time spent on moderate and vigorous-intensive physical activity, walking and sitting.
Fatigue was measured using the 20-item Multidimensional Fatigue Inventory (MFI-20) (37), consisting of five scales: general fatigue, physical fatigue, mental fatigue, reduced activity, and reduced motivation. A total MFI score can also be computed. Items were scored on a five-point scale (1 = not true, …, 5 = true). Reversely stated items were recoded and a higher score indicates more fatigue. The instrument has adequate reliability and validity (38). In the current study, reliability is good for all subscales (α = 0.77–0.84) except for reduced motivation (α = 0.61), which has acceptable internal consistency reliability.
Sleep quality was assessed with the 4-item sleep scale of the Kidney Disease Quality of Life - Short Form (KDQOL-SF) (39). Participants rated their sleep quality on a 0 to 10 scale (0 = bad, …, 10 = excellent) and three statements on other sleep problems in the last four weeks using a 6-point scale (1 = never, …, 6 = always). Scores were transformed and summed on a 0 to 100 scale. In the current study, internal consistency reliability is good (α = 0.75). Quantity of sleep was measured by self-reported effective sleeping time in hours.
Statistical analysis
Normative data of the healthy German population on physical and mental HRQoL (40), physical activity (41), fatigue (42) and sleep quantity (43), was compared with the sample data of the study (RQ-A). For the total sample and across gender groups, the average HRQoL score was tested against the population mean using one-sample T-tests. A one-sample Wilcoxon signed-rank test was used to evaluate physical activity against the reported median of the German population. Norm scores for fatigue were reported across age and gender, and were compared within each subgroup using two-samples T-tests. No norm-reference data was available on sleep quality. For the purpose of comparison, sleep quantity (effective sleeping time) of CKD patients was transformed into the categories “short”, “optimal” and “long” as Schlack and colleagues (43) only provided categorical reference data. This study’s sample distribution was tested against their reported percentages using a multinomial goodness-of-fit Chi-squared test. As measure of effect size, the Cohen’s d was used when applying T-tests (≥ 0.20 as “small”; ≥ 0.50 as “medium”; ≥ 0.8 as “large”); phi was used when a Chi-squared test was conducted (0.10 ~ small; 0.30 ~ medium; 0.50 ~ large). To control for multiple testing, p-values were adjusted using Bonferroni corrections.
For the multivariate analyses, a logarithmic transformation was applied to the physical activity variable in accordance with the recommendations of Tabachnick and Fidell (44). To compare fatigue, sleep, physical activity, and physical and mental HRQoL between treatment modalities, ANCOVAs were conducted. The PROCESS macro developed by Hayes (45) was used to test mediation (RQ-C), moderation, and moderated mediation (RQ-D and RQ-E). These analyses, were performed for each aspect of fatigue separately to avoid issues of collinearity among the different MFI (sub)scales. All multivariate analyses were controlled for gender, age, comorbidity, and disease duration. For each model, the assumptions of linearity, homoscedasticity, and normality of residuals were inspected using residual-versus-fitted plots and partial regression plots. Variance Inflation Factor values indicated no problems with multicollinearity (all VIFs < 2). Missing data were handled using pairwise deletion, so that all available data for each analysis could be included.
Statistical analyses were conducted using IBM SPSS Statistics version 22 with the PROCESS macro version 4.2 (45).
Results
Subjects
A total of 465 patients participated in the study. The average age was 53.78 years (SD = 15.00); 50.3 percent were women. Demographic and medical characteristics of the patient sample can be found in Table 1.
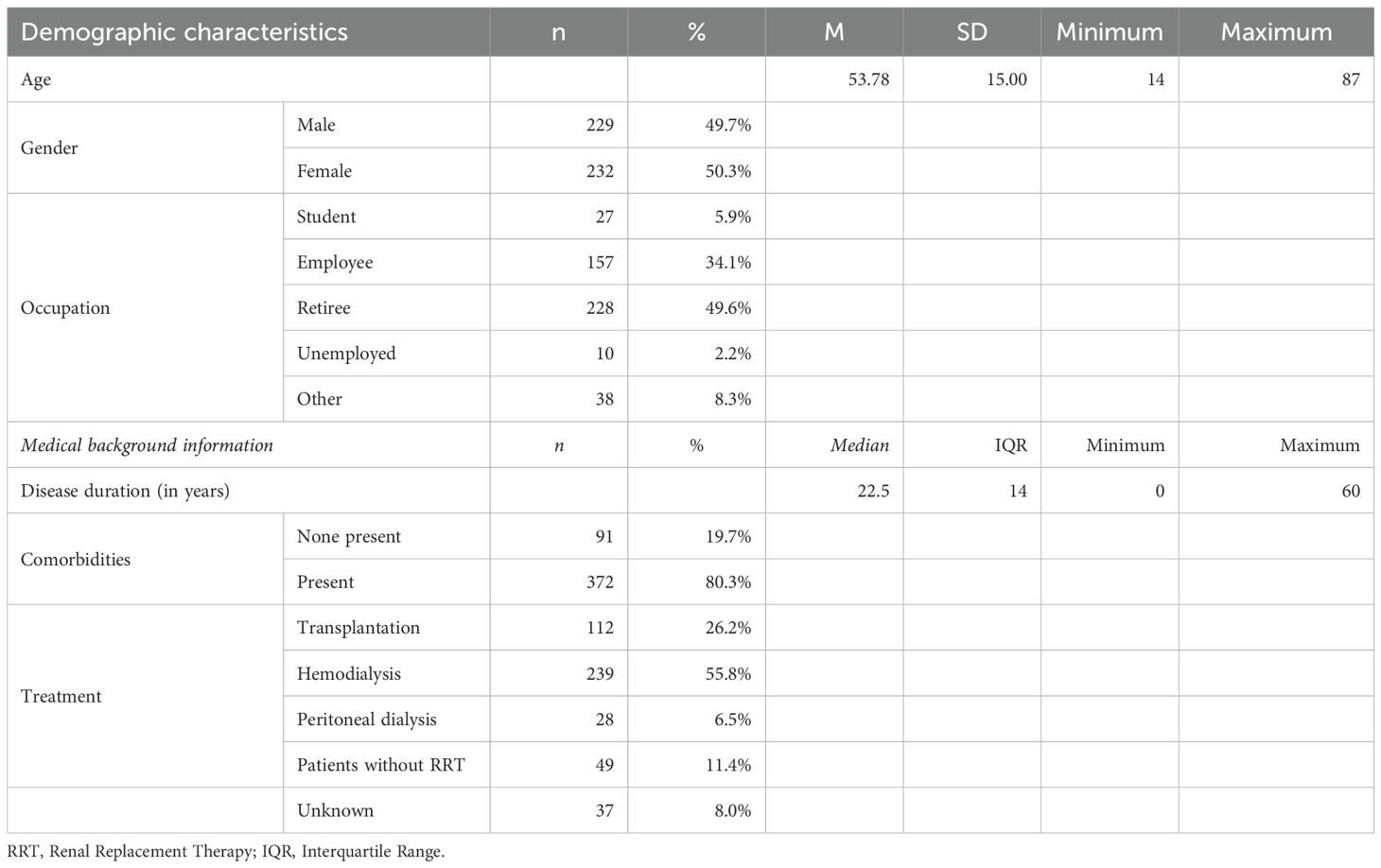
Table 1. Demographic and medical characteristics of the sample (N = 465).
Norm-comparisons of CKD patients with the German population
In the CKD patient group, the mean HRQoL scores were significantly lower than the normative means for the physical (M = 39.32 vs. 51.40) and mental component (M = 45.55 vs. 49.30). The associated effect size was medium to large for the physical (d = -1.13), and small for the mental component (d = -0.33). The same pattern of differences was found within the female and male subsamples, respectively (all ps <.001).
Physical activity was significantly lower in the patient group than in the general population. The median score in the patient sample was 2091 (IQR = 3412), which is significantly lower than the median of 5070 reported by Rütten et al. (41) (p <.001). The CKD sample mean (M = 3249.7, SD = 3925.1) was also substantially lower than the reported population mean (M = 8534.2, SD = 9024.5).
An overview of norm comparisons of the MFI subscales, stratified by gender and age, is presented in Figure 1. Higher fatigue was reported in the sample of CKD patients, except for reduced motivation and mental fatigue for the oldest group of women and mental fatigue for the oldest group of men. With respect to the age-groups, the largest differences were found in younger men and women (≤ 40 years; Cohen’s d = 1.02–1.97). With respect to gender, a similar pattern was found for females and males. With respect to the MFI-subscales, overall, the largest differences were found for general fatigue (d = 0.71–1.97), followed by reduced activity (d = 0.62–1.97) and physical fatigue (d = 0.55–1.68); the differences for reduced motivation (d = 0.24–1.44) and mental fatigue (d = 0.13–1.21) were smaller.
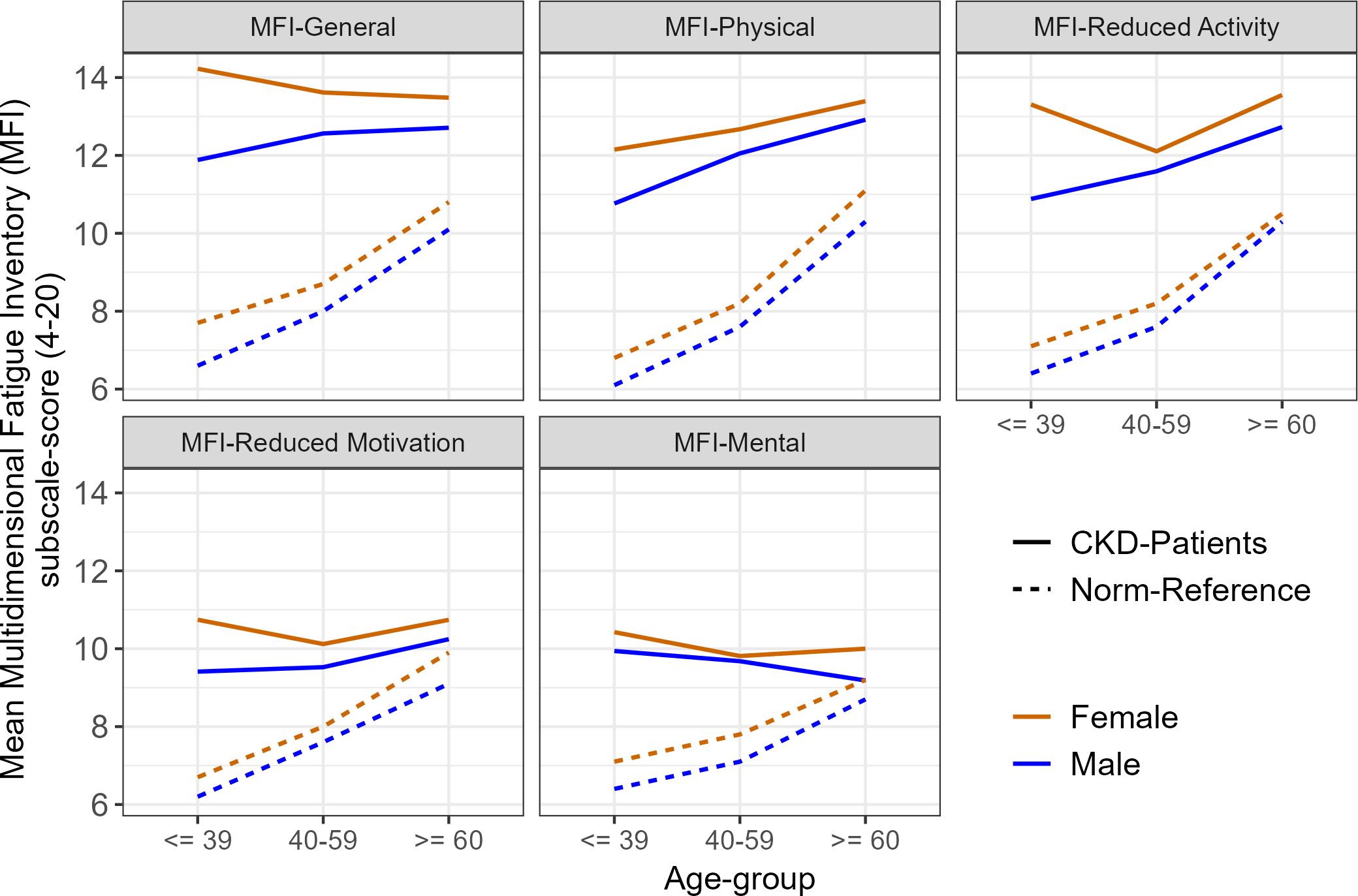
Figure 1. Means of MFI-subscale scores in the CKD sample compared to norm-reference values within age and gender groups.
A significant difference in sleeping time was found between the CKD sample and the healthy German population, χ²(2) = 32.52, p <.001; φ = 0.27. Short sleep (≤ 5 hours) was more common in the CKD group (21.1% vs. 12.3%), while optimal sleep was less frequent (72.2% vs. 81.6%). Long sleep (≥ 9 hours) occurred at similar rates (6.2% vs. 6.1%). This pattern was significant for both females, χ²(2) = 36.36, p <.001, φ = 0.40, and males, χ²(2) = 6.05, p = .049, φ = 0.17, with a larger effect for females. Female patients reported optimal sleep less often (68.4%) than male patients (76.6%) compared to the norm (80.5%).
Comparisons across modalities of treatment
Table 2 shows results of mean comparison tests across treatment modalities. Overall, transplant patients had the highest sleep quality, the lowest levels of (general) fatigue and reduced motivation, and the highest mental HRQoL, followed by hemodialysis patients. In contrast, the lowest sleep quality and mental HRQoL, and the highest (general) fatigue was found in the group of patients without RRT. Level of physical activity, physical fatigue, reduced activity, mental fatigue and the physical component of HRQoL was not significantly different across treatment modalities.
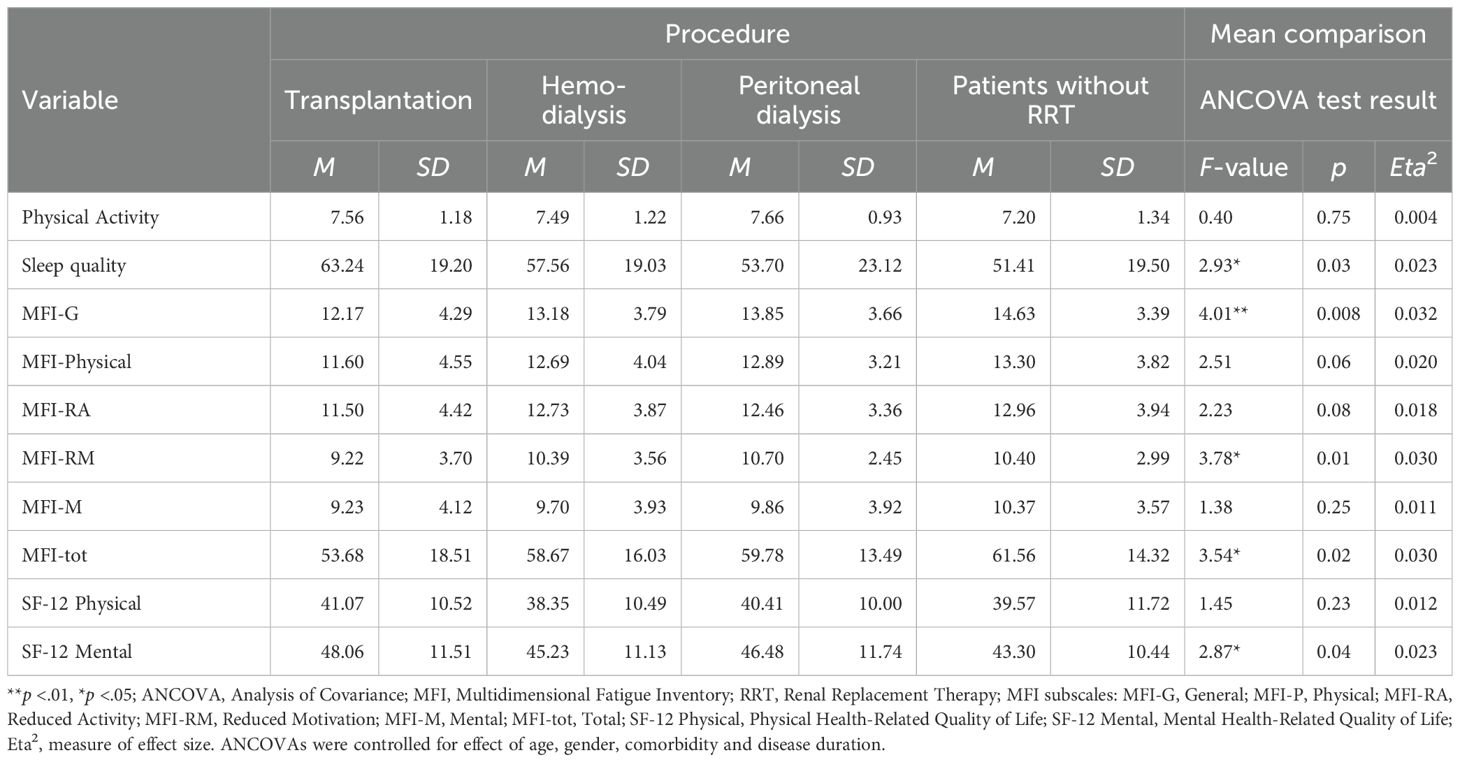
Table 2. Differences between treatment modalities for physical activity, sleep, fatigue and health-related quality of life.
Fatigue as a mediator of the effect of physical activity on HRQoL
In Table 3 (Panel A), the results of the mediation analysis are presented. The indirect effects were all significantly positive. Patients who were physically more active, had a lower level of fatigue, which in turn was related to better physical and mental HRQoL. For physical quality of life, physical fatigue showed the strongest indirect association (β = 0.195); for the mental component of HRQoL, total fatigue showed the largest indirect association (β = 0.243). The smallest indirect effects were found for reduced motivation and mental fatigue. To illustrate the mediating effect of fatigue, results for general fatigue (MFI-G) are presented in Figure 2.
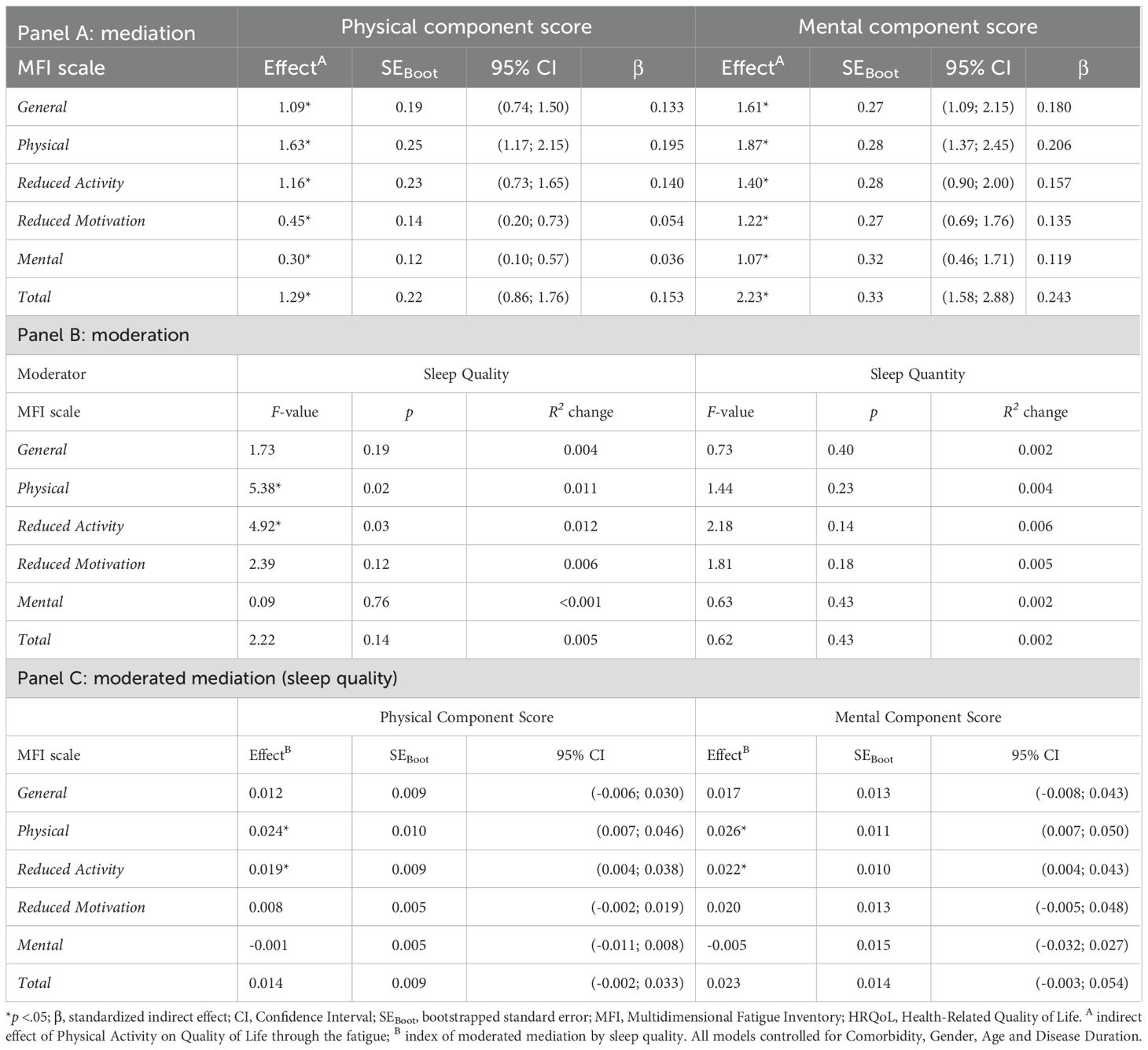
Table 3. Indirect effects of physical activity on HRQoL for each of the fatigue scales as mediator.
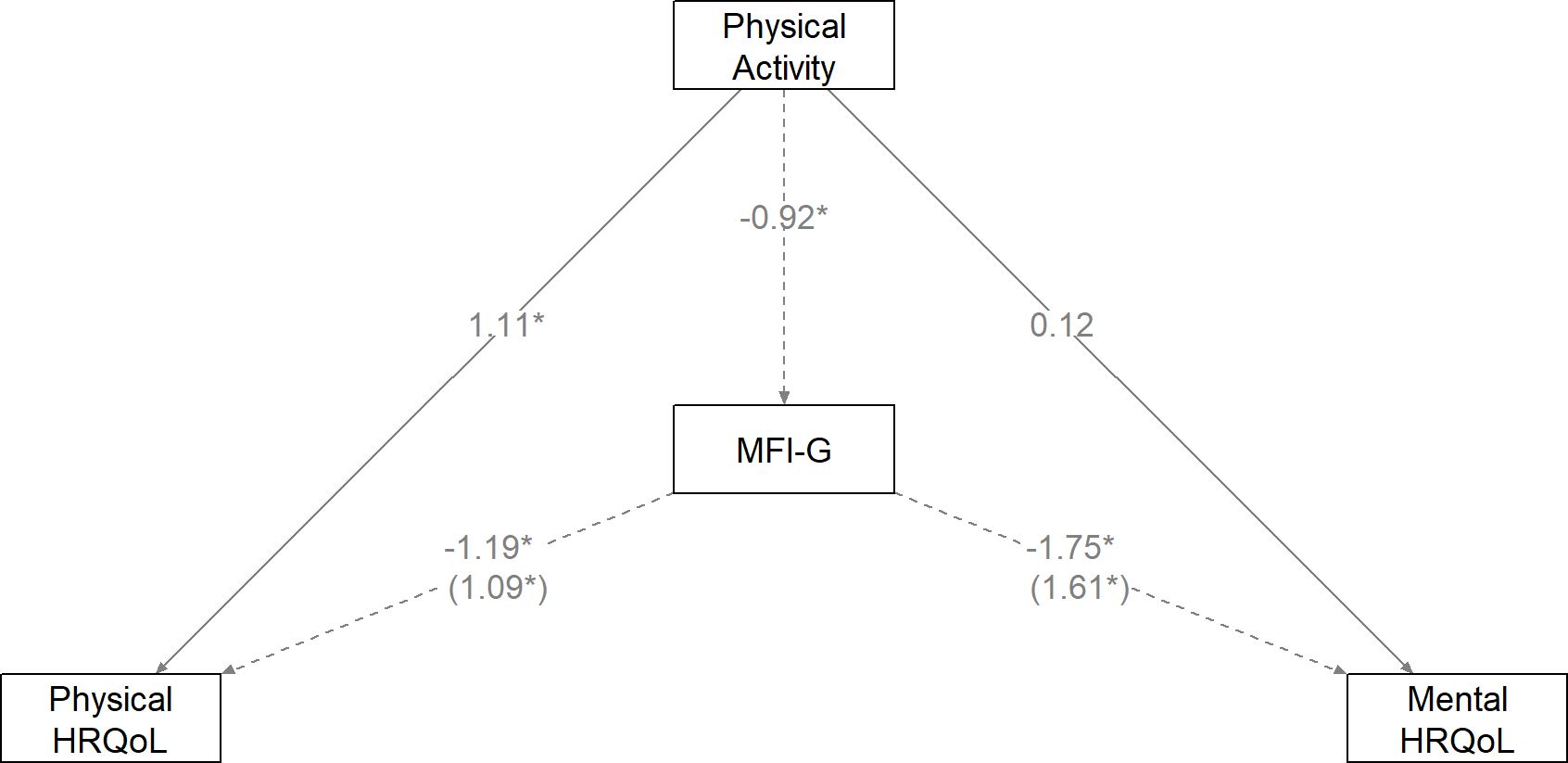
Figure 2. Unstandardized path coefficients of the mediating effect of fatigue (MFI-total) on the effect of physical activity on (the physical and mental component of) Health-Related Quality of Life (HRQoL). The indirect effects are shown in parenthesis (*p <.05).
Sleep as a moderator of the effect of physical activity on fatigue
Panel B (Table 3) gives an overview of the moderating effects of sleep quality and sleep quantity. For patients reporting better sleep quality, the association between physical activity and physical fatigue was stronger, indicating a moderating effect of sleep quality (see Figure 3, left). A similar moderating effect was observed for the MFI subscale measuring reduced activity: patients with better sleep quality and higher physical activity levels showed more favorable scores on this subscale (see Figure 3, right). By contrast, sleep quantity did not significantly moderate the association between physical activity and fatigue.
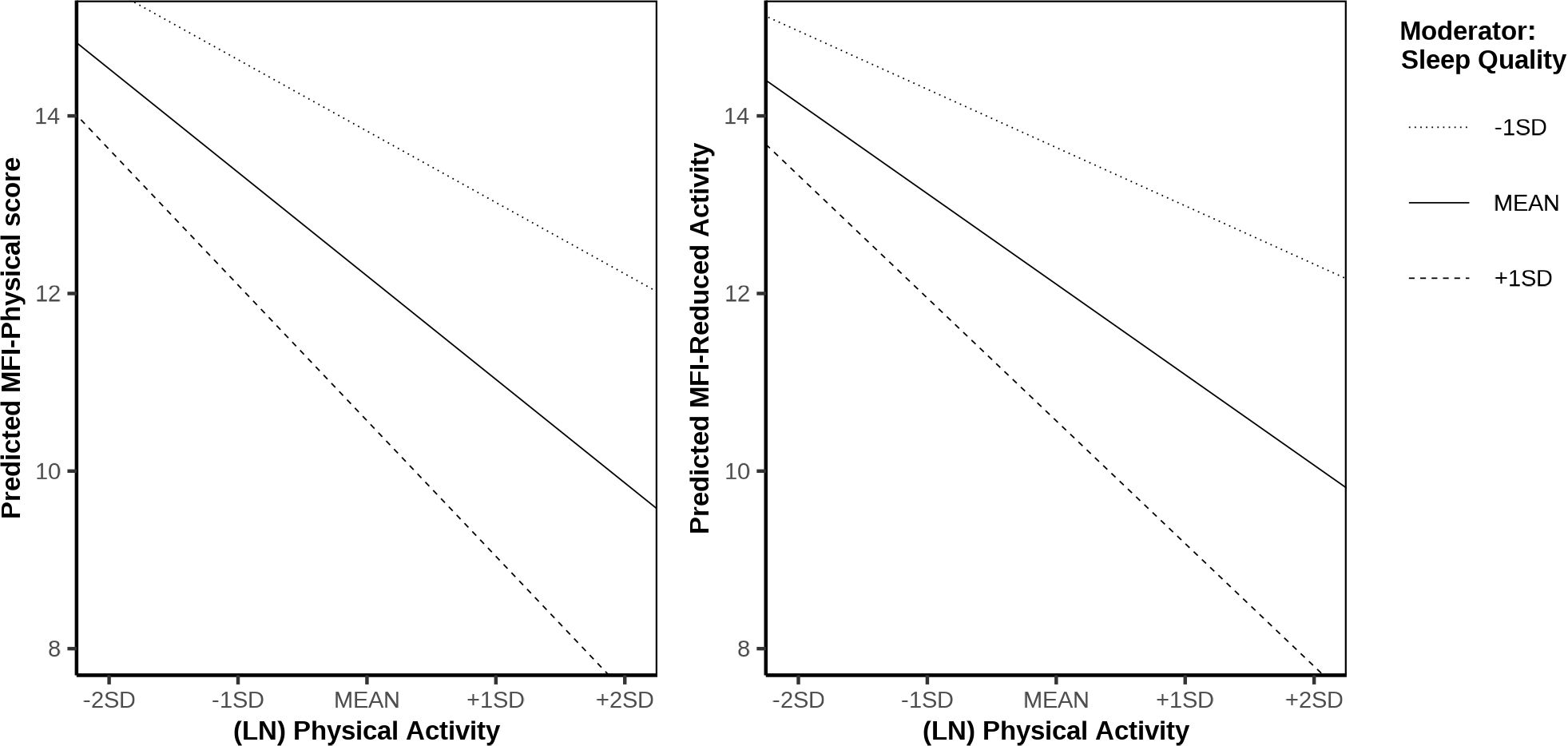
Figure 3. Interaction plots of physical activity × sleep quality on the MFI-physical subscale (left) and physical activity × sleep quality on the MFI-reduced activity subscale score (right).
Sleep quality as a moderator of the indirect effect of physical activity on physical and mental HRQoL via fatigue
The results of the analysis are shown in Table 3 (Panel C). The indirect association between physical activity and physical and mental HRQoL via physical fatigue was moderated by sleep quality. Specifically, for patients with better sleep quality, the negative association between physical activity and physical fatigue was stronger, which in turn was related to higher HRQoL. A similar moderated mediation was observed for the MFI subscale measuring reduced activity: patients with higher sleep quality and greater physical activity reported less reduced activity, which was associated with higher physical and mental HRQoL.
Discussion
The results of the current study indicate that CKD patients report lower mental and physical HRQoL compared to a sample from the general population, with the largest difference observed for physical HRQoL. CKD patients also report lower levels of physical activity and higher levels of fatigue. The greatest differences in fatigue were found among patients younger than 40 years. In addition, a larger proportion of participants in our sample reported short sleep duration (less than five hours per night) compared to data from the general population.
A comparison between the different treatment modalities shows that transplant patients report the best sleep quality, the least fatigue (with respect to general fatigue and reduced motivation) and the best mental HRQoL, followed by the hemodialysis patients. Patients without RRT are doing worse on each of these dimensions. No differences were found for degree of physical activity, the physical component of quality of life, and the other dimensions of fatigue.
Results further indicate that higher physical activity is linked to lower fatigue, which in turn is associated with better mental and physical HRQoL. For the mental component, the strongest indirect association was with total fatigue, whereas for the physical component it was with physical fatigue. The association between higher physical activity and lower fatigue (physical fatigue and reduced activity), which in turn is related to higher HRQoL, appeared more pronounced in patients reporting better sleep quality, with somewhat stronger effects for mental than for physical HRQoL.
The finding that CKD patients experience more fatigue than the general population is consistent with the existing literature on the subject (2, 3). However, the present study shows that the largest differences between CKD patients and the general population occur in a younger age group, an effect that, to our knowledge, has not been described before. A possible explanation for our finding is that younger patients may experience a heavier impact of the disease on their functioning and, as a consequence, hold more negative thoughts about their condition and related symptoms, which in turn may cause them to experience more severe fatigue. The latter is consistent with the biopsychosocial model of fatigue in CKD patients, which implies that psychological factors, including cognitions, play an important role in the perpetuation of fatigue (2, 5).
The comparison of the different treatment modalities shows that transplant patients do better whereas patients without RRT do worse than the other subgroups in a number of respects. The finding regarding transplant patients is consistent with previous studies (17, 46). That patients not yet on RRT do worse may seem counterintuitive. It can however be explained by the fact that these patients already experience symptoms due to deteriorating kidney function but are not yet receiving treatment that can adequately alleviate these symptoms (47). The null findings for degree of physical activity, the physical component of quality of life, and the other dimensions of fatigue may indicate that such differences truly do not exist between treatment modalities, or they may reflect limitations of the study. In particular, some subgroups (e.g., patients on peritoneal dialysis or not yet on RRT) were relatively small, which reduces statistical power and sensitivity to detect potential differences. It is therefore possible that the study was underpowered to capture more subtle contrasts. Nevertheless, future research with larger and more balanced samples across treatment modalities will be important to clarify whether such group differences are truly absent or simply not detected in the current study.
Previous research has reported positive associations between physical activity and both fatigue (9) and quality of life in CKD patients (21). In addition, fatigue in CKD patients has been shown to be associated with lower quality of life (18). However, to our knowledge, this is the first study to examine these relationships together and to suggest that fatigue may serve as a pathway linking physical activity with quality of life, that is, the association between physical activity and HRQoL may be explained, at least in part, by fatigue.
Although earlier studies have shown that poorer sleep quality is associated with higher patient-reported fatigue (13, 28, 29), as well as lower quality of life (23) in CKD patients, the question of whether sleep quality modifies the relationship between physical activity, fatigue, and HRQoL has not previously been examined. The present study’s finding that the strength of the association between physical activity and fatigue (and thereby HRQoL) appears to vary depending on sleep quality is therefore noteworthy and aligns with findings in non-clinical populations (30, 31).
Strengths and weaknesses
A major strength of the study is that physical activity, fatigue, and sleep, factors that are all known to influence HRQoL as well as disease progression and mortality in CKD patients (18, 20, 27), were examined together. Another strength is the inclusion of a heterogeneous CKD population, consisting of patients on hemodialysis, peritoneal dialysis, and kidney transplantation, as well as patients not yet receiving RRT. This contrasts with most prior studies, which have typically focused only on hemodialysis populations.
At the same time, several limitations should be acknowledged. First, while mediation and moderation analyses provide valuable insights into potential pathways, the cross-sectional design of the study does not allow conclusions regarding temporal sequence or causality. Longitudinal studies are needed to establish causal inferences. Second, recruitment took place via a patient association newsletter and an anonymous online survey, which may have introduced self-selection bias, for example, by attracting more motivated or health-literate patients. This, in turn, may limit the generalizability of our findings. Third, physical activity was measured using the IPAQ-SF, a widely used tool, but one known to overestimate activity and subject to recall bias. Similarly, sleep was assessed with the abbreviated 4-item KDQOL sleep scale, which may not fully capture all dimensions of sleep quality. Fourth, all measures in the study - including CKD status and treatment modality - were self-reported; no objective measures such as actigraphy for activity (using an accelerometer) or polysomnography for sleep were employed. Additional medical information such as CKD stage and medication use was not available, nor were bloodwork and clinical data (e.g., hemoglobin, eGFR), as the study was conducted anonymously in collaboration with a patient organization. This limits the ability to account for important medical confounders; for instance, anemia or uremic toxins may contribute to fatigue independently of physical activity or sleep. Finally, some CKD subgroups were relatively small, which may have reduced the sensitivity to detect subtle differences across treatment modalities.
Suggestions for future research and potential clinical implications
Beyond statistical significance, the present findings also have clinical relevance. Fatigue and sleep quality emerged as important factors associated with physical activity and HRQoL in patients with CKD. Although some of the observed effect sizes were modest, they highlight domains directly relevant to patients’ daily functioning and well-being. For example, even small improvements in sleep quality may strengthen the association between physical activity and reduced fatigue, which can translate into better energy levels, adherence to treatment, and overall quality of life. Building on this, the results suggest that interventions incorporating physical activity could be a promising strategy to address both fatigue and quality of life in CKD patients.
At the same time, prescribing exercise to fatigued patients with poor sleep quality may be challenging in practice. Tailored approaches that account for sleep quality, and that integrate sleep-focused strategies before or alongside physical activity, may therefore be more feasible. While previous studies have established that fatigue is related to lower QoL and that exercise is associated with reduced fatigue in CKD (24), the present study extends this work by examining mediated and moderated associations. These findings underscore the relevance of fatigue as a potential pathway and sleep quality as a potential modifier in the relationship between physical activity and HRQoL. To investigate these relationships more rigorously, it will be important to conduct longitudinal studies to further examine the observed associations and to establish temporal sequence and causality. In addition, the use of objective measures for physical activity and sleep would strengthen the validity of future findings. Subsequently, intervention studies are needed to test whether interventions targeting sleep and physical activity have the desired effect on reducing fatigue.
The results also show a substantial gap in fatigue between younger CKD patients and their peers in the general population, suggesting that younger patients may be a primary target group for intervention development. Moreover, the impact of untreated fatigue on later treatment outcomes has not yet been adequately studied from earlier stages of CKD through to renal replacement therapy. Addressing this gap would allow for the more targeted development of interventions across the disease trajectory.
For future research, it will be important to include biological indicators of renal function in addition to the psychosocial variables examined here. This would make it possible to investigate a broader range of factors within the biopsychosocial model of fatigue in CKD patients.
Data availability statement
The datasets presented in this article are not readily available because they contain potentially identifiable participant information. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Psychology Research Ethics Committee of Leiden University (nr. of proposal CEP 18-0516/257). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
VDG: Investigation, Methodology, Conceptualization, Writing – original draft. DW: Data curation, Methodology, Formal Analysis, Writing – original draft. VP: Data curation, Writing – review & editing, Formal Analysis. KC: Writing – review & editing, Investigation.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Ethical approval for the study was obtained from the Psychology Research Ethics Committee of Leiden University (proposal number CEP 18-0516/257).
Acknowledgments
The present study was supported by the German patient organization, Bundesverband Niere e.V., Ms. Jennifer Kloes, as well as the peritoneal dialysis center at the University Clinics Giessen. Thanks to all survey participants for sharing their time and experience.
Conflict of interest
Author KC was employed by the company Fresenius Medical Care Deutschland GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Finsterer J and Mahjoub SZ. Fatigue in healthy and diseased individuals. Am J Hospice Palliative Med. (2014) 31:562–75. doi: 10.1177/1049909113494748, PMID: 23892338
2. Artom M, Moss-Morris R, Caskey F, and Chilcot J. Fatigue in advanced kidney disease. Kidney Int. (2014) 86:497–505. doi: 10.1038/ki.2014.86, PMID: 24694985
3. Joshwa B and Campbell ML. Fatigue in patients with chronic kidney disease: evidence and measures. Nephrol Nurs J. (2017) 44:337–44., PMID: 29160968
4. Ju A, Unruh M, Davison S, Dapueto J, Dew MA, Fluck R, et al. Establishing a core outcome measure for fatigue in patients on hemodialysis: A standardized outcomes in nephrology–hemodialysis (SONG-HD) consensus workshop report. Am J Kidney Dis. (2018) 72:104–12. doi: 10.1053/j.ajkd.2017.12.018, PMID: 29551585
5. Picariello F, Moss-Morris R, Macdougall IC, and Chilcot J. The role of psychological factors in fatigue among end-stage kidney disease patients: A critical review. Clin Kidney J. (2017) 10:79–88. doi: 10.1093/ckj/sfw113, PMID: 28638608
6. Romagnani P, Remuzzi G, Glassock R, Levin A, Jager KJ, Tonelli M, et al. Chronic kidney disease. Nat Rev Dis Primers. (2017) 3:e17088. doi: 10.1038/nrdp.2017.88, PMID: 29168475
7. Davey CH, Webel AR, Sehgal AR, Voss JG, and Huml A. Fatigue in individuals with end stage renal disease. Nephrol Nurs J: J Am Nephrol Nurses’ Assoc. (2019) 46:497–508.
8. Bossola M, Arena M, Urciuolo F, Antocicco M, Pepe G, Calabrò GE, et al. Fatigue in kidney transplantation: A systematic review and meta-analysis. Diagnostics. (2021) 11(5):833. doi: 10.3390/diagnostics11050833, PMID: 34063041
9. Gregg LP, Bossola M, Ostrosky-Frid M, and Hedayati SS. Fatigue in CKD. Clin J Am Soc Nephrol. (2021) 16:1445–55. doi: 10.2215/CJN.19891220, PMID: 33858827
10. Bonner A, Wellard S, and Caltabiano M. The impact of fatigue on daily activity in people with chronic kidney disease. J Clin Nurs. (2010) 19:3006–15. doi: 10.1111/j.1365-2702.2010.03381.x, PMID: 21040007
11. Gregg LP, Jain N, Carmody T, Minhajuddin AT, Rush AJ, Trivedi MH, et al. Fatigue in nondialysis chronic kidney disease: correlates and association with kidney outcomes. Am J Nephrol. (2019) 50:37–47. doi: 10.1159/000500668, PMID: 31167183
12. Bonner A, Caltabiano M, and Berlund L. Quality of life, fatigue, and activity in Australians with chronic kidney disease: A longitudinal study. Nurs Health Sci. (2013) 15:360–7. doi: 10.1111/nhs.12038, PMID: 23480135
13. Jhamb M, Pike F, Ramer S, Argyropoulos C, Steel J, Dew MA, et al. Impact of fatigue on outcomes in the hemodialysis (HEMO) study. Am J Nephrol. (2011) 33:515–23. doi: 10.1159/000328004, PMID: 21555875
14. Brys ADH, Lenaert B, Van Heugten CM, Gambaro G, and Bossola M. Exploring the diurnal course of fatigue in patients on hemodialysis treatment and its relation with depressive symptoms and classical conditioning. J Pain Symptom Manage. (2019) 57:890–8. doi: 10.1016/j.jpainsymman.2019.02.010, PMID: 30776536
15. Picariello F, Norton S, Moss-Morris R, Macdougall IC, and Chilcot J. Fatigue in prevalent haemodialysis patients predicts all-cause mortality and kidney transplantation. Ann Behav Med. (2019) 53:501–14. doi: 10.1093/abm/kay061, PMID: 30020399
16. SChade van Westrum E, Hoogeveen EK, Broekman BFP, Siegert CEH, Keurhorst D, Annema C, et al. Fatigue across different chronic kidney disease populations: experiences and needs of patients. Clin Kidney J. (2025) 18:sfaf118. doi: 10.1093/ckj/sfaf118, PMID: 40599823
17. Maglakelidze N, Pantsulaia T, Tchokhonelidze I, Managadze L, and Chkhotua A. Assessment of health-related quality of life in renal transplant recipients and dialysis patients. Transplant Proc. (2011) 43:376–9. doi: 10.1016/J.TRANSPROCEED.2010.12.015, PMID: 21335226
18. Kraus MA, Fluck RJ, Weinhandl ED, Kansal S, Copland M, Komenda P, et al. Intensive hemodialysis and health-related quality of life. Am J Kidney Dis. (2016) 68:33–42. doi: 10.1053/j.ajkd.2016.05.023, PMID: 27772641
19. Kosmadakis GC, Bevington A, Smith AC, Clapp EL, Viana JL, Bishop NC, et al. Physical exercise in patients with severe kidney disease. Nephron - Clin Pract. (2010) 115:7–16. doi: 10.1159/000286344, PMID: 20173344
20. Zelle DM, Klaassen G, Van Adrichem E, Bakker SJL, Corpeleijn E, and Navis G. Physical Inactivity: A risk factor and Target for Intervention in Renal Care. Nat Rev Nephrol. (2017) 13:152–68. doi: 10.1038/nrneph.2016.187, PMID: 28138130
21. Barcellos FC, Santos IS, Umpierre D, Bohlke M, and Hallal PC. Effects of exercise in the whole spectrum of chronic kidney disease: a systematic review. Clin Kidney J. (2015) 8:753–65. doi: 10.1093/ckj/sfv099, PMID: 26613036
22. Bündchen DC, Sousa H, Afreixo V, Frontini R, Ribeiro O, Figueiredo D, et al. Intradialytic exercise in end-stage renal disease: an umbrella review of systematic reviews and/or meta-analytical studies. Clin Rehabil. (2021) 35:812–28. doi: 10.1177/0269215520986784, PMID: 33530715
23. Yamamoto R, Ito T, Nagasawa Y, Matsui K, Egawa M, Nanami M, et al. Efficacy of aerobic exercise on the cardiometabolic and renal outcomes in patients with chronic kidney disease: A systematic review of randomized controlled trials. J Nephrol. (2021) 34:155–64. doi: 10.1007/s40620-020-00865-3, PMID: 33387341
24. Zhao Q-G, Zhang H-R, Wen X, Wang Y, Chen X-M, Chen N, et al. Exercise interventions on patients with end-stage renal disease: a systematic review. Clin Rehabil. (2019) 33:147–56. doi: 10.1177/0269215518817083, PMID: 30789077
25. Roumelioti M-E, Argyropoulos CP, and Unruh ML. Sleep disorders in patients with CKD and ESRD. In: Cukor D, Cohen SD, and Kimmel PL, eds. Psychosocial Aspects of Chronic Kidney Disease. Cambridge, MA: Academic Press (Elsevier) (2021). p. 183–212. doi: 10.1016/B978-0-12-817080-9.00009-9
26. Elder SJ, Pisoni RL, Akizawa T, Fissell R, Andreucci VE, Fukuhara S, et al. Sleep quality predicts quality of life and mortality risk in haemodialysis patients: results from the dialysis outcomes and practice patterns study (DOPPS). Nephrol Dialysis Transplant. (2008) 23:998–1004. doi: 10.1093/ndt/gfm630, PMID: 17911092
27. Yamamoto R, Shinzawa M, Isaka Y, Yamakoshi E, Imai E, Ohashi Y, et al. Sleep quality and sleep duration with CKD are associated with progression to ESKD. Clin J Am Soc Nephrol. (2018) 13:1825–32. doi: 10.2215/CJN.01340118, PMID: 30442866
28. Jhamb M, Liang K, Yabes J, Steel JL, Dew MA, Shah N, et al. Prevalence and correlates of fatigue in chronic kidney disease and end-stage renal disease: are sleep disorders a key to understanding fatigue? Am J Nephrol. (2013) 38:489–95. doi: 10.1159/000356939, PMID: 24335380
29. Brys ADH, Stifft F, Van Heugten CM, Bossola M, Gambaro G, and Lenaert B. mHealth-based experience sampling method to identify fatigue in the context of daily life in haemodialysis patients. Clin Kidney J. (2021) 14:245–54. doi: 10.1093/ckj/sfaa124, PMID: 33564425
30. Miller M, Lee-Chambers J, Cooper B, Boolani A, and Jansen E. Associations between physical activity and energy and fatigue depend on sleep quality. Fatigue: Biomed Health Behav. (2020) 8:193–204. doi: 10.1080/21641846.2020.1843790
31. Herring MP, Monroe DC, Kline CE, O’Connor PJ, and MacDonncha C. Sleep quality moderates the association between physical activity frequency and feelings of energy and fatigue in adolescents. Eur Child Adolesc Psychiatry. (2018) 27:1425–32. doi: 10.1007/s00787-018-1134-z, PMID: 29508054
32. Faul F, Erdfelder E, Buchner A, and Lang AG. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav Res Methods. (2009) 41:1149–60. doi: 10.3758/BRM.41.4.1149, PMID: 19897823
33. Ware JE, Kosinski M, and Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. (1996) 34:220–33. doi: 10.1097/00005650-199603000-00003, PMID: 8628042
34. Luo X, George ML, Kakouras I, Edwards CL, Pietrobon R, Richardson W, et al. Reliability, validity, and responsiveness of the short form 12-item survey (SF-12) in patients with back pain. Spine. (2003) 28:1739–45. doi: 10.1097/01.BRS.0000083169.58671.96, PMID: 12897502
35. Bohannon RW, Maljanian R, and Landes M. Test-retest reliability of short form (SF)-12 component scores of patients with stroke. Int J Rehabil Res. (2004) 27:149–50. doi: 10.1097/01.MRR.0000127350.25287.08, PMID: 15167113
36. Sember V, Meh K, Sorić M, Jurak G, Starc G, and Rocha P. Validity and reliability of international physical activity questionnaires for adults across EU countries: systematic review and meta analysis. Int J Environ Res Public Health. (2020) 17:7161. doi: 10.3390/IJERPH17197161, PMID: 33007880
37. Smets EMA, Garssen B, Bonke B, and De Haes JCJM. The multidimensional fatigue inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. (1995) 39:315–25. doi: 10.1016/0022-3999(94)00125-O, PMID: 7636775
38. Hinz A, Benzing C, Brähler E, Zenger M, Herzberg PY, Finck C, et al. Psychometric properties of the multidimensional fatigue inventory (MFI-20), derived from seven samples. J Pain Symptom Manage. (2020) 59:717–23. doi: 10.1016/J.JPAINSYMMAN.2019.12.005, PMID: 31837450
39. Hays RD, Kallich JD, Mapes DL, Coons SJ, and Carter WB. Development of the kidney disease quality of life (KDQOL) instrument. Qual Life Res: Int J Qual Life Aspects Treatment Care Rehabil. (1994) 3:329–38. doi: 10.1007/BF00451725, PMID: 7841967
40. Ellert U and Kurth BM. Gesundheitsbezogene lebensqualität bei erwachsenen in Deutschland. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz. (2013) 56:643–9. doi: 10.1007/s00103-013-1700-y, PMID: 23703481
41. Rütten A, Ziemainz H, Schena F, Stahl T, Stiggelbout M, Auweele Y, et al. Using different physical activity measurements in eight european countries. Results of the European physical activity surveillance system (EUPASS) time series survey. Public Health Nutr. (2003) 6:371–6. doi: 10.1079/phn2002450, PMID: 12795825
42. Schwarz R, Krauss O, and Hinz A. Fatigue in the general population. Onkologie. (2003) 26:140–4. doi: 10.1159/000069834, PMID: 12771522
43. Schlack R, Hapke U, Maske U, Busch M, and Cohrs S. Häufigkeit und Verteilung von Schlafproblemen und Insomnie in der deutschen Erwachsenenbevölkerung. Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz. (2013) 56:740–8. doi: 10.1007/s00103-013-1689-2, PMID: 23703493
44. Tabachnick BG and Fidell LS. Using multivariate statistics. 7th ed. New York, NY: Pearson (2019).
45. Hayes AF. An index and test of linear moderated mediation. Multivariate Behav Res. (2015) 50:1–22. doi: 10.1080/00273171.2014.962683, PMID: 26609740
46. Fujisawa M, Ichikawa Y, Yoshiya K, Isotani S, Higuchi A, Nagano S, et al. Assessment of health-related quality of life in renal transplant and hemodialysis patients using the SF-36 health survey. Urology. (2000) 56:201–6. doi: 10.1016/S0090-4295(00)00623-3, PMID: 10925078
47. Grams ME, Surapaneni A, Appel LJ, Lash JP, Hsu J, Diamantidis CJ, et al. Clinical events and patient-reported outcome measures during CKD progression: findings from the chronic renal insufficiency cohort study. Nephrol Dialysis Transplant. (2021) 36:1685–93. doi: 10.1093/NDT/GFAA364, PMID: 33326030
Keywords: chronic kidney disease, fatigue, sleep, physical activity, HRQoL, renal transplantation, renal replacement therapy, dialysis
Citation: De Gucht V, Woestenburg DHA, Pizzulin VV and Cromm K (2025) Fatigue and quality of sleep jointly influence the association between physical activity and health-related quality of life in patients with chronic kidney disease: a cross-sectional study. Front. Nephrol. 5:1649578. doi: 10.3389/fneph.2025.1649578
Received: 18 June 2025; Accepted: 29 September 2025;
Published: 18 November 2025.
Edited by:
Michal Nowicki, Medical University of Lodz, PolandReviewed by:
Pedro Paulo Gattai Gomes, University of São Paulo, BrazilMani Abdul Karim, XIM University, India
L. Manju, Kerala University of Health Sciences, India
Copyright © 2025 De Gucht, Woestenburg, Pizzulin and Cromm. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Véronique De Gucht, ZGVndWNodEBmc3cubGVpZGVudW5pdi5ubA==
†ORCID: Véronique De Gucht, orcid.org/0000-0001-5155-0983
Dion H. A. Woestenburg, orcid.org/0000-0001-6143-1101
Krister Cromm, orcid.org/0000-0002-5324-0695