 Sergio Jiménez-Rubio1
Sergio Jiménez-Rubio1 Tomás García-Calvo
Tomás García-Calvo Luis Manuel Martínez-Aranda
Luis Manuel Martínez-Aranda Javier Raya-González
Javier Raya-González- 1Sport Sciences Research Centre, Rey Juan Carlos University, Madrid, Spain
- 2Faculty of Sport Sciences, University of Extremadura, Cáceres, Spain
- 3Department of Sports and Computer Sciences, Faculty of Sports Sciences, Universidad Pablo de Olavide, Seville, Spain
- 4Science-Based Training Research Group (SEJ-680), Physical Performance and Sports Research Center, Universidad Pablo de Olavide, Seville, Spain
- 5Research Group on Sport and Physical Education for Personal and Social Development (GIDEPSO), Department of Specific Didactics, Faculty of Education Sciences and Psychology, University of Córdoba, Córdoba, Spain
Introduction: Introduction Soccer players are frequently exposed to high physical demands, which increase their risk of injury, especially anterior cruciate ligament (ACL) ruptures. Despite completing standard rehabilitation protocols, many athletes show persistent functional deficits one year after surgery. This study aimed to assess the impact of a 12-week reconditioning training program, focusing on adjacent joint mobility, neuromuscular control, plyometrics, stability-landing exercises, and strength production, of amateur soccer players 12 months after undergoing anterior cruciate ligament (ACL) surgery.
Methods: Twenty-five Spanish male amateur soccer players (age = 21.2 ± 2.4 years) participated voluntarily. All participants followed similar return-to-play guidelines and were randomly assigned to either the control group (CG, n = 13) or the experimental group (EG, n = 12). Soccer players in the EG underwent the 12-week training program (ACLrPRO), and both groups completed jump battery tests before and after the intervention period.
Results and discussion: The results showed improvements in all analyzed variables for the EG, except for the time to stabilization during the single-leg land and hold test for their non-injured leg, where the CG showed better results. Moreover, players in the CG exhibited a decline in performance related to their non-injured leg across all performed tests. The EG also demonstrated lower absence days during the experimental period compared to the CG. These findings underscore the significance of implementing a targeted neuromuscular training program for soccer players recovering from an ACL rupture, especially in enhancing performance and reducing absence days after their return to competition.
1 Introduction
Soccer is a demanding team sport characterized by a significant number of high-intensity actions, such as jumping or sprinting (Gualtieri et al., 2023). In recent years, there has been an increase in the occurrence of these high-intensity actions during soccer matches (Allen et al., 2023; Lago-Peñas et al., 2023), prompting notable changes in training methods. The main aim of this is to ensure that soccer players are well-prepared to meet these higher demands (Castillo et al., 2021) and increase the chances of success (Faude et al., 2012). However, these heightened demands are associated with an increased risk of injury in soccer players (Gabbett, 2016), making injuries a primary concern for strength and conditioning coaches in soccer (Raya-González et al., 2019). This is critical as injuries negatively impact both individual player performance (Raya-González et al., 2022) and the collective performance of the team (Hägglund et al., 2013). Moreover, injuries have adverse effects on financial aspects of clubs (Ekstrand, 2013) and on the quality of life of soccer players, sometimes leading to withdrawal from competition (Øiestad et al., 2018). These negative effects are particularly pronounced in the case of long-term injuries, with ligamentous injuries, especially ruptures of the anterior cruciate ligament (ACL) of the knee, standing out prominently.
Overall, injury incidence in professional male soccer players is stablished at 8.1 injuries/1,000 h of exposure, with a higher injury incidence during matches (36 injuries/1,000 h of exposure) compared to training sessions (3.7 injuries/1,000 h of exposure) (López-Valenciano et al., 2019). Specifically, joint injuries present an incidence of 0.4 injuries/1,000 h of exposure, with the most common ones related to knee and ankle joints having values close to 1.0 joint injury/1,000 h of exposure (López-Valenciano et al., 2019). Regarding to the ACL knee injuries, Requejo-Herrero et al. (2023) obtained an incidence of 0.0364 ACL injuries/1,000 h of exposure in professional male soccer players participating in the Spanish first division. Similarly, an incidence of 0.076 ACL injuries/1,000 h of exposure in were observed by Rekik et al. (2018) in male soccer players belonging to a Middle Eastern league. Although the incidence of ACL injuries in male soccer players is lower compared to other types of injuries, such as muscle-tendon injuries where the hamstring complex is involved (Diemer et al., 2021), the severity of ACL injuries is high. In this regard, Requejo-Herrero et al. (2023) and Rekik et al. (2018) revealed that the mean lay-off time after an ACL injury is close to 220 absence days. Given that the absence days associated with these injuries are very high, their negative impact on soccer players is excessively significant, sometimes even leading to retirement. Therefore, it seems essential to understand their impact on players and establish appropriate strategies to alleviate these effects.
After an ACL injury and subsequent surgery, it has been observed that the mechanoreceptors of the knee fail to send information for neuromuscular responses to maintain balance and joint function. This results in certain instability of the postural control system and muscle strength deficits (Negahban et al., 2014), accompanied by a decrease in quadriceps activation and increased flexor muscle activity of the knee (Nyland et al., 2016). In this context, the primary objective of rehabilitation programs for ACL injuries is to enhance the strength level, particularly of the knee extensor muscles (Buckthorpe et al., 2019). This improvement is crucial before restoring the quality of movement, functional strength, power, explosive muscle strength, and undertaking sport-specific retraining for the eventual return to sport (Buckthorpe and Roi, 2017). Consequently, resistance training becomes a pivotal component in rehabilitation programs after an ACL injury. However, a recent systematic review conducted by Nichols et al. (2021) has revealed a misalignment between the intensity prescribed during resistance training programs for ACL rehabilitation and strength and conditioning principles. Often, these programs are not optimized to develop the necessary neuromuscular qualities required for return-to-sport criteria. This contributes to suboptimal prescription of rehabilitation programs, resulting in athletes who are inadequately prepared. In this sense, Khalid et al. (2022) concluded that, compared to traditional resistance training, neuromuscular training was significantly more effective in reducing pain, improving function, quality of life, strength, and power. Current studies have validated systems for the quantification of variables related to pathologies that cause deficits in strength, stability and movement imbalance (Collings et al., 2024). Therefore, it is essential to establish rehabilitation programs that facilitate achieving the appropriate values for a safe return to sport.
Return to sport criteria following an ACL injury have been developed to objectively determine when a safe return to sport is indicated (Kyritsis et al., 2016). Regarding this, there is a consensus that passing the objective return to sport criteria is vital in reducing injury risk following an ACL injury (Losciale et al., 2019). Specifically, Kyritsis et al. (2016) found a fourfold increased risk of ACL rupture for those athletes who did not pass the return to sport criteria. Similarly, Grindem et al. (2016) estimated an 84% lower knee reinjury rate among athletes who passed return to sport criteria. However, despite compliance with established guidelines, some authors have reported functional deficits in athletes after returning to sports practice (Nagai et al., 2020). Biau et al. (2007) revealed that only 33% of ACL surgically operated patients with hamstring graft and 41% with patella graft returned to their pre-injury athletic condition, increasing the risk of reinjury. Current trends suggest extending the return to play (RTP) period to 12 months. However, a recent study (Felix et al., 2022) demonstrated that functional outcomes increased in athletes with ACL reconstruction after 12 months, but did not reach the same level as the control group. These authors found incomplete functional recovery and adaptive changes in postural control after injury, reconstruction, and return to sport. Considering this, it seems essential to apply neuromuscular programs in the 12 months following ACL surgery, even if the soccer player has satisfactorily returned to sport.
Thus, the aim of this study was to evaluate the effects of a specific reconditioning program training based on adjacent joint mobility, neuromuscular control, plyometrics, stability-landing exercises, and strength production exercises on the performance and availability of amateur soccer players applied 12 weeks after an ACL surgery. Based on prior studies (Khalid et al., 2022; Zsidai et al., 2023), we hypothesized that players in the experimental group would improve their performance related to biomechanical jump variables and would present lower absence days during the experimental period.
2 Materials and methods
2.1 Study design
A randomized-controlled trial design was applied to investigate the effects of a multicomponent training program, comprising adjacent joint mobility, neuromuscular control, plyometrics, stability-landing exercises, and strength production exercises, on the performance and availability of amateur soccer players. This training program was implemented 12 months after an ACL surgery and lasted 12 weeks (i.e., three sessions per week). Prior an after the experimental period, participants performed the following jump tests: single leg land and hold (SLLH); single leg jump (SLJ); single leg squat assessment (SLSA); drop jump (DJ), considering several biomechanical variables for each test. These jump tests were performed with both, injured and non-injured legs, Additionally, the number of absence days from regular soccer training during the experimental period was registered. Jump tests were conducted in a single session in the morning (9–11 a.m.) in a controlled indoor environment with temperatures maintained between 20°C and 23°C and humidity levels between 60% and 70%. The assessment sessions were supervised by the same strength and conditioning specialist and a standardized warm-up was completed by participants. Players were instructed to have their last meal at least 2 h before the start of the tests and to avoid consuming caffeinated beverages.
2.2 Participants
Twenty-five Spanish male amateur soccer players (age = 21.2 ± 2.4 years) voluntarily participated in the study. An a priori power analysis was performed (G*Power, v3.1.9.2, Universität Kiel, Germany), which determined that a sample size of at least 20 participants was needed to achieve a power (1-β) of 0.84, assuming an effect size (ES) of 0.90 (large effect) and alpha of 0.05. Participants belonged to different teams competing in semiprofessional league of Spain, and trained 4 times per week and played one official match during the weekend. Also, players covered the satisfactorily similar RTP guidelines prior to be allocated in any group. The inclusion criteria for the study were as follows: amateur soccer players over 18 years of age with no history of cardiovascular or metabolic pathologies, with 12 months postoperative anterior cruciate ligament injury, with the capacity to perform stability drills on one leg and without injuries during the research process. Players with 2 or more joint injuries in the 3 months prior to the investigation and with a recent history (i.e., less than 4 months) of knee surgery were excluded from the study. Participants were randomly assigned to either the control group (CG; n = 13; age: 20.2 ± 1.9 years; height: 179.0 ± 0.1 cm; body mass: 70.3 ± 2.3 kg; body mass index: 21.9 ± 0.8 kg·m−2) or to the experimental group (EG; n = 12 age: 22.2 ± 2.5 years; height: 180.0 ± 0.1 cm body mass: 70.8 ± 2.6 kg; body mass index: 21.8 ± 0.6 kg·m−2).
2.3 Procedures
During the 12-weeks intervention period, players performed their regular weekly in-season routine, with the EG performing Anterior Cruciate Ligament Reconditioning Program (ACLrPRO) 3 times per week, in addition to their regular soccer training routines. All participants were familiar with the testing protocols. Prior to the experimental sessions, players undertook a 12-min standardized warm-up consisting in 4 blocks: a) myofascial inhibition, participants used foam roller and pressure balls to facilitate the myofascial level in quadriceps, soleus and hip extensors; b) mobility, facilitated joint range of motion of the thoracic spine, ankle dorsiflexion, hip in submaximal range of flexion combined with external rotation, overhead squat and analytical facilitation of internal and external hip rotation; c) muscle activation, based on the application of tensions to the posterior chain with three exercises that combined isometric and short cycles of stretching-shortening in safe levers; and d) adaptation to stretch-shortening cycle, applying the single leg jump exercise with take-offs of only 2 cm above the surface and the countermovement jump without seeking maximum height, but rather motor control in the deceleration part.
2.3.1 Instrument
All test were completed on 2 portable force platforms (FD4000 ForceDecks dual force platforms; VALD Performance, Sydney, Australia) and neuromuscular performance techniques ForceDeck Software (version 1) at a sampling frequency of 1,000 Hz. This software detects the initiation of movement as a 30 N deviation from the initial bodyweight calculation, eccentric to concentric phase moment as the lowest center of mass displacement, and take-off as the moment the vertical forces fall 30 N below body mass. A series of metrics from ForceDecks software’s default output were analyzed to provide the end user with reliability of a multitude of metrics of interest. These metrics are defined elsewhere (Chavda et al., 2018; Heishman et al., 2020; Merrigan et al., 2020) and can also be found in the ForceDecks user guide. Raw data were analyzed via custom-designed Microsoft Excel Software (Redmond, WA) and filtered of high-frequency noise using a Butterworth low pass filter at 10 Hz.
2.3.2 Jump tests
Single Leg Land and Hold (SLLH). Players conducted four attempts with each leg, separated by 30 s of passive recovery between the two legs but continuously between repetitions of the same leg. The 2 first attempts were used to assess the Peak Drop Landing Force (PDLF) variable, both for the uninjured leg (PDLFnon) and the injured leg (PDLFinj). To measure this, participants initially weighed themselves with both feet on the platforms and then stood on a 40 cm high box. While on the box, participants placed the toes of the standing leg on the red line marked at the edge of the box. From this starting position, participants landed safely on the corresponding platform to record the peak force during this unilateral landing. To evaluate the Time to Stabilization (TSTAB) variable for both the uninjured leg (TTSnon) and the injured leg (TTSinj), participants completed other two attempts of the SLLH as follow: the participants weighed themselves with both feet on the platforms, stepped off the platforms to initiate the evaluation, and then, from a line marked 15 cm from the base of each platform, performed a single-leg landing. The time required to stabilize in a triple flexion pattern without destabilizing the platform was quantified. The ICCs and the CVs for these variables were 0.73–0.81 and 3.3–4.4, respectively.
Single Leg Jump (SLJ). Players performed two attempts with each leg, with 30 s of passive recovery between the two legs but continuous repetitions with the same leg. Firstly, the participants weighed themselves with both feet on the platforms. Then, each participant stabilized on the non-injured leg and performed a single leg squat with a stretch-shortening cycle. This was followed by a jump-push off to take off as much as possible on that platform. After finishing these 2 executions with the healthy limb, the same procedure was done with the injured limb, without the need for weighing and without modifying the registration in the software. Derived from this test, Jump Height (JH) and Peak Power Related to Body Mass (PPOW) were obtained, selecting the highest value in cm and W/kg, respectively. The ICCs and the CVs for JH were 0.64–0.78 and 5.5–5.7 respectively, while for PPOW were 0.70–0.79 and 2.2–2.5 respectively.
Single Leg Squat Assessment (SLSA). Players completed two attempts with each leg, with a 30-s passive recovery between the two legs but continuous repetitions with the same leg. After the weight measurement, with the participant in a bipodal stance, we recorded their ability to generate the maximum force in a single-legged squat without take-off. This process was repeated twice, starting with the non-injured limb and then repeating the same process to measure the maximum force produced with the injured limb. The highest values records in N for each limb was used to determine the Peak Push Force (PPFORCE). The ICCs and the CVs for this variable were 0.69–0.75 and 3.8–3.9, respectively.
Drop Jump (DJ). Players completed two bilateral DJ attempts, with a 1-min passive recovery period between them. Participants were instructed to stand in an upright position on the 30 cm box, with their feet shoulder-width apart and hands placed on their hips. Then, they were instructed to step off the box, descend to land evenly on both feet (with no heel contact allowed), and immediately perform a maximal-effort vertical jump. The best jump was selected to calculate the Reactive Strength Index (RSI) using the ratio of jump height to contact time. The ICCs and the CVs for RSI were 0.70 and 4.4 respectively.
2.3.3 Absence days
During the 12-weeks intervention period, the days on which players could not participate in the regular training soccer sessions of their team due to pain, discomfort or insecurity related to the injured leg were registered.
2.3.4 ACLrPro multicomponent training program
The training intervention lasted 12 weeks, with 3 sessions per week. The ACLrPRO incorporated mobility tasks of the ankle, hip, thoracic spine and stability in load, primarily in unilateral scenarios, implementing landings, strength and neuromuscular control drills, explosive and reactive tasks in the absorption-transmission relationship, as well as tasks emphasizing multiplanar force production. Players were introduced to the ACLrPRO exercises 1 year after surgery and only if players had satisfactorily completed the return to competition. Each training session lasted between 20 and 55 min and took place after the standardized warm-up previously explained. The ACLrPRO sessions took place four (MD-4), three (MD-3) and one (MD-1) days prior the matches. The ACLrPro sessions were supervised by a qualified strength and conditioning coach, who provided adequate feedback and instruction for correctly executing the drills. To ensure progressive improvement, a progressive overload approach was implemented, tailoring the workload for each drill based on individual capabilities (Table 1).
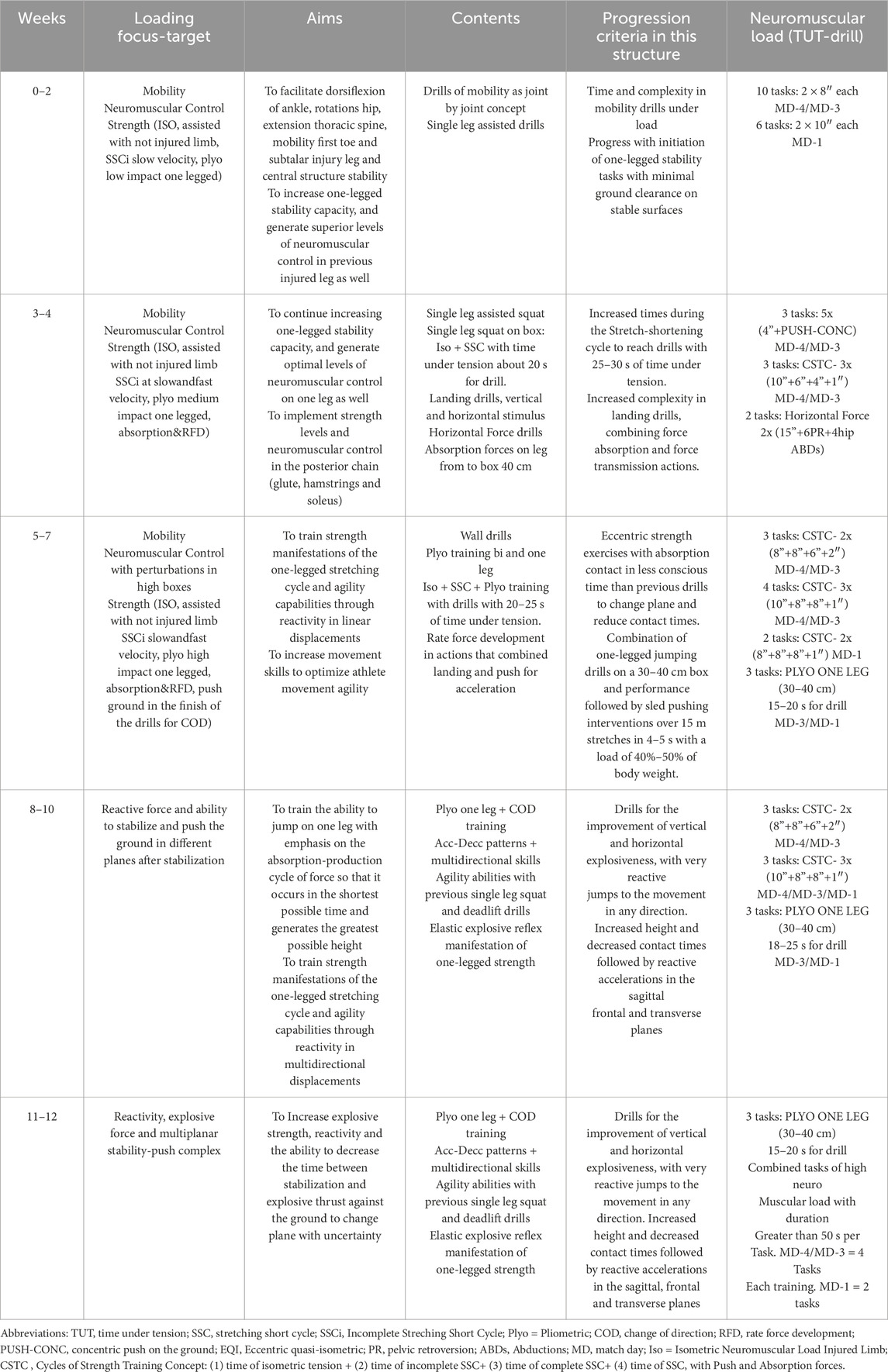
Table 1. Anterior Cruciate Ligament Reconditioning Program (ACLrPRO) applied in the experimental group.
2.4 Statistical analysis
Descriptive statistics are presented as mean ± standard deviation (SD). The Shapiro-Wilk and Levene tests were used to prove the normality of the distribution and the homogeneity of variances, respectively. A Paired-samples t-test was applied to analyze within-group differences, while the possible between-group differences were studied through an analysis of covariance (ANCOVA), including baseline values as covariates. Effect sizes (ES) were calculated using Cohen’s ES to assess the magnitude of the effects. ES were interpreted as follow: <0.2, trivial; 0.20 to 0.49, small; 0.50 to 0.80, moderate and >0.80, large (Cohen, 1988). The data analysis was carried out using the Jeffrey’s Amazing Statistics Program (JASP 0.18.1; The JASP team, Amsterdam, The Netherlands) being the statistical significance was set at p < 0.05.
3 Results
Table 2 shows the changes observed in the force platform variables related to jump after the intervention period in both groups. Within-group analysis presented significant changes in PDLFnon (p = 0.003; ES = −0.51, moderate), TSTABnon (p = 0.0042; ES = 0.67, moderate), JHnon (p = 0.001; ES = −1.07, large), PPFORCEnon (p = 0.001; ES = −1.62, large) and RSI (p = 0.002; ES = −1.20, large) for CG, while participants in EG experienced significant changes in all variables (p = 0.001; ES = −8.94 to 9.00, large) except for TSTABnon. Between-groups analysis revealed differences in favor of the EG in all variables (F = 7.10 to 81.62; p = 0.001) except for TSTABnon.
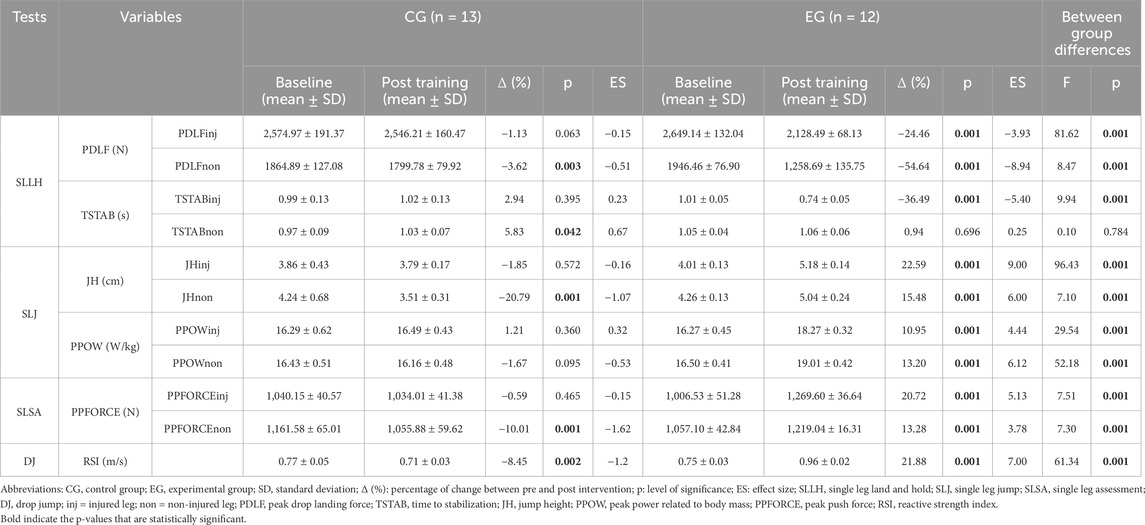
Table 2. Changes in biomechanical variables before (baseline) and after (post-training) the 12-week intervention period.
A total of 151 absence days (11.6 ± 9.7 per player) were collected for CG during the experimental period, while for the E.G., 64 absence days (5.3 ± 6.1 per player) were recorded in the same period.
4 Discussion
This study aimed to evaluate the effects of a specific reconditioning training program based on adjacent joint mobility, neuromuscular control, plyometrics, stability-landing exercises, and strength production exercises on the performance and availability of amateur soccer players applied 12 months after an ACL surgery. Despite several studies have analyzed the effectiveness of several rehabilitation programs after an ACL injury, to date, this is the first study that intervenes on the period after the return to sport, when players are fully incorporated into soccer practice. Following the program intervention, players in the EG improved all analyzed variables except for TSTABnon, obtaining better results compared to the participants in the CG. Additionally, the EG exhibited lower absence days during the experimental period compared to the CG.
Landing ability has been identified as a determinant of injury risk related to ACL injuries (Ohji et al., 2021), justifying its inclusion as a crucial component in preventive programs for this injury. However, there are several variables implicated in landing that must be considered. In this regard, PDLF holds great relevance, as reducing the impact forces during landing after an ACL injury is essential to decrease the risk of reinjury (Bressel and Cronin, 2005). In this study, significant decreases in PDLFinj and PDLFnon were observed, with better results compared to the CG, which also show a decrement in PDLFnon. These improvements, particularly in the injured leg, could be attributed to the high unilateral training load developed during the intervention period (Oliveira et al., 2022). This training program was focused on the specific needs of the injured leg, addressing aspects such as reception technique, strength, and stability. Another relevant variable during landing is the TSTAB, which measures the time it takes for an individual to return to a baseline or stable state following a jump or hop landing (Fransz et al., 2015). An increase in TSTAB, particularly related to an ACL injury, indicates dynamic postural control deficits, reflecting difficulties in controlling ground reaction forces (Webster and Gribble, 2010). Our results align with those previously obtained by Kasmi et al. (2021), who observed reductions in TSTAB after implementing a training program based on eccentric and plyometric exercises 14 weeks after ACL surgery in elite female athletes. Specifically, in our study, players in the EG improved their TSTAB in the injured leg after the experimental period. The inclusion of tasks based on the stretching-shortening cycle, emphasizing minimizing ground contact time, could explain this improvement. Conversely, no improvements in the non-injured leg were observed, although the program prevented an increase in TSTAB similar to the CG, justifying its value for both the injured and non-injured leg.
Prior studies have observed a decrease in jump performance after ACL surgery in male athletes (King et al., 2018; Kotsifaki, Whiteley, et al., 2022), possibly as a consequence of the neurophysiological alterations in the ACL following the rupture (Kakavas et al., 2020). In this regard, the SLJ test appears to be a key tool for identifying knee function deficits upon return to sport after ACL reconstruction (Kotsifaki, Van Rossom, et al., 2022). This test allows the assessment of various variables such as jump height (JH) and peak power related to body mass (PPOW), providing a comprehensive understanding of the injured leg’s status. In this study, players in the EG demonstrated improvements in both variables after the 12-week intervention period. This is particularly relevant since soccer players not only enhanced the power exerted but also exhibited improved neuromuscular performance, as evidenced by increased strength and coordination during the jump, resulting in greater jump height. Such improvements may be associated with a lower risk of reinjury, given previous findings indicating that soccer players, even though meeting RTP criteria, fail to fully regain pre-injury physical fitness values 12 months post-operation (Felix et al., 2022). Additionally, soccer players in the EG showed enhanced performance in both variables in the non-injured leg. This suggests that the applied program could significantly influence players’ overall sports performance (Zahalka et al., 2021). Conversely, players in the CG did not show improvements in either variable and, notably, experienced a significant reduction in jump height on the non-injured leg. These results provide evidence supporting the effectiveness of the program in better preparing soccer players for competition compared to those who did not undergo the intervention, despite all players having satisfactorily complied with RTP guidelines and actively participated with their teams.
The SLSA test assesses peak push force (PPFORCE) during a squat, which is closely related to the force exerted by the knee extensor apparatus in athletes who suffer an ACL rupture (Batty et al., 2019), essential during the rehabilitation process (Buckthorpe et al., 2019). After the intervention, players in the EG experienced a significant increase in the PPFORCE in their injured leg, nearly 20%, equating the PPFORCE levels to those of the uninjured leg, which also improved its performance (i.e., 13%). This finding is highly relevant, as a great force level of the knee extensors is the basis for other critical physical qualities such as quality of movement, functional strength, or power, facilitating an adequate level of physical fitness and favoring a reduced reinjury risk (Buckthorpe and Roi, 2017). Similar to JH, players in the CG worsened their performance relative to the PPFORCE in their non-injured leg, showing lower values in both legs compared to their EG counterparts after the 12-week intervention period. Some authors have reported that substantial deficits in plyometric abilities (e.g., reactive strength) are common after ACL reconstructions (Read et al., 2023). Therefore, the reactive strength index (RSI) measured during a DJ seems to be a key variable to consider when players return to play (RTP) after an ACL injury (Jarvis et al., 2022). In this sense, RSI provides a valuation of knee function regarding the stretch shortening cycle, as this metric refers to the ability of the muscle-tendon units to produce a rapid and powerful contraction immediately following a rapid eccentric action (Ramirez-Campillo et al., 2018). Improvements in RSI were observed in the EG after the application of the ACLrPRO, possibly due to a significant change in neuromuscular control and the ability to produce force. This implies an increase in the ability to apply force at high velocity through the combination of musculotendinous elasticity and contractility in a task such as the drop jump. Similar to prior variables, RSI performance also decreased in the CG, suggesting the need to implement neuromuscular training programs 12 months after ACL surgery to avoid reductions in performance that may lead to reinjuries or new associated injuries.
Previous studies have highlighted limitations in the return to play and performance, with a 15-year follow-up registering up to 35% of participants facing restrictions in returning to professional soccer (Waldén et al., 2016). Similarly, other studies with a 6-month post-surgery ACL follow-up reported 24% of participants experiencing relapses in the process. However, in this same study, it was observed that by maintaining tissue maturation until 2 years, 80.7% of participants could secure a return to play (Bodkin et al., 2022). Therefore, it appears pertinent to document the days on which players could not participate in regular soccer training sessions with their team due to pain, discomfort, or insecurity related to the injured leg to gather comprehensive information about the effectiveness of the ACLrPRO. In this context, players in the CG group experienced 151 absence days (11.6 ± 9.7 per player) during the 12-week period, while only 64 absence days (5.3 ± 6.1 per player) were recorded for players in the EG during the same period. This finding supports the assertion made by Felix et al. (2022), which claimed that soccer players exhibit incomplete functional recovery and adaptive changes in postural control after injury, reconstruction, and return to sport after 12 months of ACL reconstruction. It confirms the necessity of implementing a neuromuscular training program in this population, not only to enhance performance and reduce the reinjury risk but also to increase the availability of soccer players after their return to competition.
This study has some limitations that practitioners should be aware of. The primary limitation is the inability to control the workload covered by soccer players in their weekly microcycles with their respective clubs during the intervention period. Additionally, the sample size (n = 25) could be scarce to stablish robust conclusions. However, the analyzed topic (LCA injuries), with high number of absence days, difficult to involve a higher sample. Also, the intervention involved only male soccer players, so caution should be exercised when generalizing the findings to women’s soccer, considering the differences between the groups in terms of physical, physiological, and biomechanical factors. Finally, there was no follow-up after the 12-week intervention. Future studies should consider long-term follow-up, such as one and 2 years after completing the program, to assess the status of soccer players, the incidence of reinjuries, and possible player withdrawals.
5 Conclusion
In summary, players in the EG improved all analyzed variables except for TSTABnon, obtaining better results compared to their counterparts in the CG after performing the ACLrPRO. Additionally, players in the CG decreased their performance related to their non-injured leg in PDLF, TSTAB, JH, PPFORCE, and RSI. Finally, the EG exhibited lower absence days during the experimental period compared to the CG. These findings suggest the importance of implementing a neuromuscular training program in soccer players who suffered an ACL rupture after they returned to competition, not only to enhance their performance, reduce the reinjury risk, and increase their availability but also to avoid a decrease in performance related to the non-injured leg.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethical committee of the Universidad Rey Juan Carlos (Madrid) with internal registration number 3105202214349. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SJ-R: Investigation, Conceptualization, Formal Analysis, Writing – original draft, Methodology. TG-C: Formal Analysis, Supervision, Investigation, Resources, Writing – review and editing. LM-A: Writing – review and editing, Writing – original draft. JR-G: Resources, Formal Analysis, Supervision, Investigation, Writing – original draft, Methodology, Conceptualization, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to especially thank the players who participated in the study for their collaboration.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer AHS declared a past collaboration with the author JR-G to the handling editor at the time of the review.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Allen T., Taberner M., Zhilkin M., Rhodes D. (2023). Running more than before? The evolution of running load demands in the English premier league. Int. J. Sports Sci. and Coach. 19 (2), 779–787. doi:10.1177/17479541231164507
Batty L. M., Feller J. A., Hartwig T., Devitt B. M., Webster K. E. (2019). Single-leg squat performance and its relationship to extensor mechanism strength after anterior cruciate ligament reconstruction. Am. J. Sports Med. 47 (14), 3423–3428. doi:10.1177/0363546519878432
Biau D. J., Tournoux C., Katsahian S., Schranz P., Nizard R. (2007). ACL reconstruction: a meta-analysis of functional scores. Clin. Orthop. Relat. Res. 458, 180–187. doi:10.1097/BLO.0B013E31803DCD6B
Bodkin S. G., Hertel J., Diduch D. R., Saliba S. A., Novicoff W. M., Brockmeier S. F., et al. (2022). Predicting anterior cruciate ligament reinjury from return-to-activity assessments at 6 months postsurgery: a prospective cohort study. J. Athl. Train. 57 (4), 325–333. doi:10.4085/1062-6050-0407.20
Bressel E., Cronin J. (2005). The landing phase of a jump strategies to minimize injuries. J. Phys. Educ. Recreat. and Dance 76 (2), 30–35. doi:10.1080/07303084.2005.10607332
Buckthorpe M., Roi G. S. (2017). The time has come to incorporate a greater focus on rate of force development training in the sports injury rehabilitation process. Muscles, Ligaments Tendons J. 7 (3), 435–441. doi:10.11138/MLTJ/2017.7.3.435
Buckthorpe M., Rosa G. L., Villa F. D. (2019). Restoring knee extensor strength after anterior cruciate ligament reconstruction: a clinical commentary. Int. J. Sports Phys. Ther. 14 (1), 159–172. doi:10.26603/ijspt20190159
Castillo D., Raya-González J., Weston M., Yanci J. (2021). Distribution of external load during acquisition training sessions and match play of a professional soccer team. J. Strength Cond. Res. 35 (12), 3453–3458. doi:10.1519/jsc.0000000000003363
Chavda S., Bromley T., Jarvis P., Williams S., Bishop C., Turner A. N., et al. (2018). Force-time characteristics of the countermovement jump: analyzing the curve in excel. Strength Cond. J. 40 (2), 67–77. doi:10.1519/SSC.0000000000000353
Cohen J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, NY: L. Erlbaum Associates.
Collings T. J., Lima Y. L., Dutaillis B., Bourne M. N. (2024). Concurrent validity and test–retest reliability of VALD ForceDecks strength, balance, and movement assessment tests. J. Sci. Med. Sport 0 (0), 572–580. doi:10.1016/j.jsams.2024.04.014
Diemer W. M., Winters M., Tol J. L., Pas H. I. M. F. L., Moen M. H. (2021). Incidence of acute hamstring injuries in soccer: a systematic review of 13 studies involving more than 3800 athletes with 2 million sport exposure hours. J. Orthop. Sports Phys. Ther. 51 (1), 27–36. doi:10.2519/JOSPT.2021.9305
Ekstrand J. (2013). Keeping your top players on the pitch: the key to football medicine at a professional level. Br. J. Sports Med. 47 (12), 723–724. doi:10.1136/bjsports-2013-092771
Faude O., Koch T., Meyer T. (2012). Straight sprinting is the Most frequent action in goal situations in professional football. J. Sports Sci. 30 (7), 625–631. doi:10.1080/02640414.2012.665940
Felix E. C. R., Alonso A. C., Brech G. C., Fernandes T. L., Almeida A. M. de, Luna N. M. S., et al. (2022). Is 12 months enough to reach function after athletes’ ACL reconstruction: a prospective longitudinal study. Clinics 77, 100092. doi:10.1016/J.CLINSP.2022.100092
Fransz D. P., Huurnink A., De Boode V. A., Kingma I., Van Dieën J. H. (2015). Time to stabilization in single leg drop jump landings: an examination of calculation methods and assessment of differences in sample rate, filter settings and trial length on outcome values. Gait and Posture 41 (1), 63–69. doi:10.1016/J.GAITPOST.2014.08.018
Gabbett T. J. (2016). The training-injury prevention paradox: should athletes be training smarter and harder? Br. J. Sports Med. 12, 273–280. doi:10.1136/bjsports-2015-095788
Grindem H., Snyder-Mackler L., Moksnes H., Engebretsen L., Risberg M. A. (2016). Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br. J. Sports Med. 50 (13), 804–808. doi:10.1136/BJSPORTS-2016-096031
Gualtieri A., Rampinini E., Dello Iacono A., Beato M. (2023). High-speed running and sprinting in professional adult soccer: current thresholds definition, match demands and training strategies. A systematic review. Front. Sports Act. Living 5, 1116293. doi:10.3389/fspor.2023.1116293
Hägglund M., Waldén M., Magnusson H., Kristenson K., Bengtsson H., Ekstrand J. (2013). Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA champions league injury study. Br. J. Sports Med. 47 (12), 738–742. doi:10.1136/bjsports-2013-092215
Heishman A. D., Daub B. D., Miller R. M., Freitas E. D. S., Frantz B. A., Bemben M. G. (2020). Countermovement jump reliability performed with and without an arm swing in NCAA division 1 intercollegiate basketball players. J. Strength Cond. Res. 34 (2), 546–558. doi:10.1519/JSC.0000000000002812
Jarvis P., Turner A., Read P., Bishop C. (2022). Reactive strength index and its associations with measures of physical and sports performance: a systematic review with meta-analysis. Sports Med. Auckl. 52 (2), 301–330. doi:10.1007/S40279-021-01566-Y
Kakavas G., Malliaropoulos N., Pruna R., Traster D., Bikos G., Maffulli N. (2020). Neuroplasticity and anterior cruciate ligament injury. Indian J. Orthop. 54 (3), 275–280. doi:10.1007/S43465-020-00045-2
Kasmi S., Zouhal H., Hammami R., Clark C. C. T., Hackney A. C., Hammami A., et al. (2021). The effects of eccentric and plyometric training programs and their combination on stability and the functional performance in the Post-ACL-Surgical rehabilitation period of elite female athletes. Front. Physiology 12, 688385. doi:10.3389/FPHYS.2021.688385
Khalid K., Anwar N., Saqulain G., Afzal M. F. (2022). Neuromuscular training following anterior cruciate ligament reconstruction – pain, function, strength, power and quality of life perspective: a randomized control trial. Pak. J. Med. Sci. 38 (8), 2175–2181. doi:10.12669/PJMS.38.8.5730
King E., Richter C., Franklyn-Miller A., Daniels K., Wadey R., Moran R., et al. (2018). Whole-body biomechanical differences between limbs exist 9 months after ACL reconstruction across jump/landing tasks. Scand. J. Med. and Sci. Sports 28 (12), 2567–2578. doi:10.1111/SMS.13259
Kotsifaki A., Van Rossom S., Whiteley R., Korakakis V., Bahr R., Sideris V., et al. (2022). Single leg vertical jump performance identifies knee function deficits at return to sport after ACL reconstruction in Male athletes. Br. J. Sports Med. 56 (9), 490–498. doi:10.1136/BJSPORTS-2021-104692
Kotsifaki A., Whiteley R., Van Rossom S., Korakakis V., Bahr R., Sideris V., et al. (2022). Single leg hop for distance symmetry masks lower limb biomechanics: time to discuss hop distance as decision criterion for return to sport after ACL reconstruction? Br. J. Sports Med. 56 (5), 249–256. doi:10.1136/BJSPORTS-2020-103677
Kyritsis P., Bahr R., Landreau P., Miladi R., Witvrouw E. (2016). Likelihood of ACL graft rupture: not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br. J. Sports Med. 50 (15), 946–951. doi:10.1136/BJSPORTS-2015-095908
Lago-Peñas C., Lorenzo-Martinez M., López-Del Campo R., Resta R., Rey E. (2023). Evolution of physical and technical parameters in the Spanish LaLiga 2012-2019. Sci. and Med. Footb. 7 (1), 41–46. doi:10.1080/24733938.2022.2049980
López-Valenciano A., Ruiz-Pérez I., Garcia-Gómez A., Vera-Garcia F. J., De Ste Croix M., Myer G. D., et al. (2019). Epidemiology of injuries in professional football: a systematic review and meta-analysis. Br. J. Sports. Med. 54 (12), 711–718. doi:10.1136/bjsports-2018-099577
Losciale J. M., Zdeb R. M., Ledbetter L., Reiman M. P., Sell T. C. (2019). The association between passing return-to-sport criteria and second anterior cruciate ligament injury risk: a systematic review with meta-analysis. J. Orthop. Sports Phys. Ther. 49 (2), 43–54. doi:10.2519/JOSPT.2019.8190
Merrigan J. J., Stone J. D., Thompson A. G., Guy Hornsby W., Hagen J. A. (2020). Monitoring neuromuscular performance in military personnel. Int. J. Environ. Res. Public Health 17 (23), 9147–26. doi:10.3390/IJERPH17239147
Nagai T., Schilaty N. D., Laskowski E. R., Hewett T. E. (2020). Hop tests can result in higher limb symmetry index values than isokinetic strength and leg press tests in patients following ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 28 (3), 816–822. doi:10.1007/s00167-019-05513-3
Negahban H., Mazaheri M., Kingma I., van Dieën J. H. (2014). A systematic review of postural control during single-leg stance in patients with untreated anterior cruciate ligament injury. Knee Surg. Sports Traumatology, Arthrosc. 22 (7), 1491–1504. doi:10.1007/S00167-013-2501-4
Nichols Z. W., O’Brien D., White S. G. (2021). Is resistance training intensity adequately prescribed to meet the demands of returning to sport following anterior cruciate ligament repair? A systematic review. BMJ Open Sport. 7 (3), e001144. doi:10.1136/BMJSEM-2021-001144
Nyland J., Mattocks A., Kibbe S., Kalloub A., Greene J., Caborn D. (2016). Anterior cruciate ligament reconstruction, rehabilitation, and return to play: 2015 update. Open Access J. Sports Med. 7, 21–32. doi:10.2147/OAJSM.S72332
Ohji S., Aizawa J., Hirohata K., Ohmi T., Mitomo S., Jinno T., et al. (2021). Characteristics of landing impact in athletes who have not returned to sports at the pre-injury competition level after anterior cruciate ligament reconstruction. Asia-Pacific J. Sports Med. Arthrosc. Rehabilitation Technol. 25, 47–52. doi:10.1016/J.ASMART.2021.05.001
Øiestad B. E., Holm I., Risberg M. A. (2018). Return to pivoting sport after ACL reconstruction: association with osteoarthritis and knee function at the 15-year follow-up. Br. J. Sports Med. 52 (18), 1199–1204. doi:10.1136/bjsports-2017-097718
Oliveira M., Júnior P. L., Imoto A. M., Santos T., Borges J. H. S., Nunes P., et al. (2022). Unilateral versus bilateral resistance exercise in postoperative rehabilitation after ACL reconstruction with bone-patellar tendon-bone graft: a randomized controlled trial. Orthop. J. Sports Med. 10 (4), 23259671221088830. doi:10.1177/23259671221088830
Ramirez-Campillo R., Alvarez C., García-Pinillos F., Sanchez-Sanchez J., Yanci J., Castillo D., et al. (2018). Optimal reactive strength index: is it an accurate variable to optimize plyometric training effects on measures of physical fitness in young soccer players? J. Strength Cond. Res. 32 (4), 885–893. doi:10.1519/JSC.0000000000002467
Raya-González J., Nakamura F. Y., Castillo D., Yanci J., Fanchini M. (2019). Determining the relationship between internal load markers and noncontact injuries in young elite soccer players. Int. J. Sports Physiology Perform. 14 (4), 421–425. doi:10.1123/ijspp.2018-0466
Raya-González J., Pulido J. J., Beato M., Ponce-Bordón J. C., López del Campo R., Resta R., et al. (2022). Analysis of the effect of injuries on match performance variables in professional soccer players: a retrospective, experimental longitudinal design. Sports Med. - Open 8 (1), 31. doi:10.1186/s40798-022-00427-w
Read P. J., Davies W. T., Bishop C., McAuliffe S., Wilson M. G., Turner A. N. (2023). Residual deficits in reactive strength after anterior cruciate ligament reconstruction in soccer players. J. Athl. Train. 58 (5), 423–429. doi:10.4085/0169-20
Rekik R. N., Tabben M., Eirale C., Landreau P., Bouras R., Wilson M. G., et al. (2018). ACL injury incidence, severity and patterns in professional Male soccer players in a Middle Eastern league. BMJ Open Sport Exerc. Med. 4 (1), e000461. doi:10.1136/BMJSEM-2018-000461
Requejo-Herrero P., Pineda-Galan C., Medina-Porqueres I. (2023). Anterior cruciate ligament ruptures in Spanish soccer first division: an epidemiological retrospective study. Knee 41, 48–57. doi:10.1016/J.KNEE.2022.11.014
Waldén M., Hägglund M., Magnusson H., Ekstrand J. (2016). ACL injuries in men’s professional football: a 15-year prospective study on time trends and return-to-play rates reveals only 65% of players still play at the top level 3 years after ACL rupture. Br. J. Sports Med. 50 (12), 744–750. doi:10.1136/BJSPORTS-2015-095952
Webster K. A., Gribble P. A. (2010). Time to stabilization of anterior cruciate ligament-reconstructed versus healthy knees in national collegiate athletic association division I female athletes. J. Athl. Train. 45 (6), 580–585. doi:10.4085/1062-6050-45.6.580
Zahalka F., Maly T., Ford K., Sugimoto D., Mala L., Hank M., et al. (2021). Vertical jump performance: relevance for competition success in elite soccer. Med. and Sci. Sports and Exerc. 53 (8S), 48. doi:10.1249/01.MSS.0000759644.82994.50
Zsidai B., Piussi R., Thomeé R., Sundemo D., Musahl V., Samuelsson K., et al. (2023). Generalised joint hypermobility leads to increased odds of sustaining a second ACL injury within 12 months of return to sport after ACL reconstruction. Br. J. Sports Med. 57 (15), 972–978. doi:10.1136/BJSPORTS-2022-106183
Keywords: anterior cruciate ligament, football, neuromuscular training, return to play, recovery
Citation: Jiménez-Rubio S, García-Calvo T, Martínez-Aranda LM and Raya-González J (2025) A specific reconditioning training program implemented 12 months after ACL surgery improves lower-limb jump variables in amateur soccer players. Front. Physiol. 16:1630156. doi: 10.3389/fphys.2025.1630156
Received: 16 May 2025; Accepted: 23 July 2025;
Published: 05 August 2025.
Edited by:
Hassane Zouhal, University of Rennes 2 – Upper Brittany, FranceReviewed by:
Ariadna Hernaiz-Sánchez, European University of Madrid, SpainGuido Belli, University of eCampus, Italy
Copyright © 2025 Jiménez-Rubio, García-Calvo, Martínez-Aranda and Raya-González. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Manuel Martínez-Aranda, bG1tYXJhcmFAdXBvLmVz