 J. Bergqvist1,2*
J. Bergqvist1,2* F. Reite3
F. Reite3 F. Edin4L. Schiöler5M. Börjesson6,7S. Steinsvåg8
F. Edin4L. Schiöler5M. Börjesson6,7S. Steinsvåg8 S. Pettersson4†
S. Pettersson4† J. Hellgren9,10†
J. Hellgren9,10†- 1Department of Respiratory Medicine and Allergology, Sahlgrenska University Hospital, Gothenburg, Sweden
- 2Centre for Sleep and Wake Disorders, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 3Department Of Otolaryngology, Head and Neck Surgery, Sørlandet Hospital, Kristiansand, Norway
- 4Centre for Health and Performance, Department of Food and Nutrition, and Sport Science, University of Gothenburg, Gothenburg, Sweden
- 5Occupational and Environmental Medicine, School of Public Health and Community Medicine, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 6Department of Molecular and Clinical Medicine, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 7Center for lifestyle Intervention, Department of MGAÖ, Östra Hospital, Gothenburg, Sweden
- 8Department Of Otolaryngology, Head and Neck Surgery, Sørlandet Hospital and Haukeland University Hospital, University of Bergen, Bergen, Norway
- 9Department of Otorhinolaryngology, Head & Neck Surgery, Sahlgrenska University Hospital, Region Västra Götaland, Gothenburg, Sweden
- 10Department of Otorhinolaryngology, Institute of Clinical Sciences, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
Introduction: Nasal breathing is preferable for persons at rest and remains partially active during oronasal breathing in exercise. However, its potential contribution to performance–particularly in cases with a decongested nose–remains understudied in well-trained athletes. This study investigates whether nasal airflow during oronasal breathing influences performance in well-trained, endurance athletes. Specifically, we examine whether nasal decongestion during oronasal breathing enhances ventilatory efficiency and, thereby, improves time-to-exhaustion (TTE), maximal oxygen uptake (
Methods: Twelve male, well-trained cyclists/triathlon athletes (mean
Results: There were no significant differences between the three breathing modes (p > 0.05) in terms of the cardiopulmonary or performance parameters, including the rate of perceived exertion, respiratory frequency, mean minute ventilation,
Conclusion: Oral-only breathing is associated with a non-significant shorter TTE than oronasal breathing with or without nasal decongestion, although it results in significantly lower mean capillary blood lactate levels following maximal aerobic exercise. These findings suggest that a single, low-resistance oral breathing route reduces lactate accumulation under maximal effort, whereas oronasal breathing–particularly in the presence of nasal decongestion–may be more beneficial for sustaining endurance.
1 Introduction
Nasal breathing is the preferred breathing route in most humans during sleep and at rest, even though approximately two-thirds of the total airway resistance occurs in the anterior part of the nose (Haight and Cole, 1983). As ventilatory demand increases during exercise, the nasal breathing capacity is eventually exceeded, prompting a transition to oronasal breathing. Nevertheless, continued nasal breathing during exercise has been proposed to enhance performance (Walker et al., 2016), which could include improvements in maximal oxygen uptake (
While some mechanisms have been proposed, the empirical findings have been inconsistent. LaComb et al. compared nasal and oral breathing during graded exercise and found that while oral breathing produced larger respiratory and metabolic volumes, it did not necessarily improve ventilatory efficiency (LaComb et al., 2017). Meir et al. reported no significant differences in performance, perceived exertion, blood lactate, or ventilatory parameters in rugby players who were performing repeated, high-intensity shuttle runs with or without nasal occlusion (Meir et al., 2014). Similarly, Recinto and coworkers observed no significant differences in power output or performance between subjects with nasal and oral-only breathing in a Wingate anaerobic cycling test (Recinto et al., 2017).
A systematic review and meta-analysis concluded that external nasal stents did not significantly improve
While most of these studies included relevant physiologic measures, such as
2 Methodology
2.1 Study participants
Thirteen well-trained, male cyclists and triathletes in the age range of 19–48 years were recruited in the Gothenburg region of Sweden via contacts. One participant who completed only one of the three experimental trials before withdrawing due to a common cold was excluded from the final analysis. Thus, 12 participants aged (mean ± SD) 30.6 ± 8.7 years (height, 181.9 ± 5.4 cm; body weight, 75.8 ± 4.3 kg; percent fat mass, 14.4 ± 3.6; and
2.2 Study overview
As illustrated in Figure 1, participants attended five separate visits to the exercise laboratory at the Center for Health and Performance (CHP), Department of Food and Nutrition and Sport Science (IKI), University of Gothenburg (GU). These visits comprised two characterization sessions and three experimental trials.
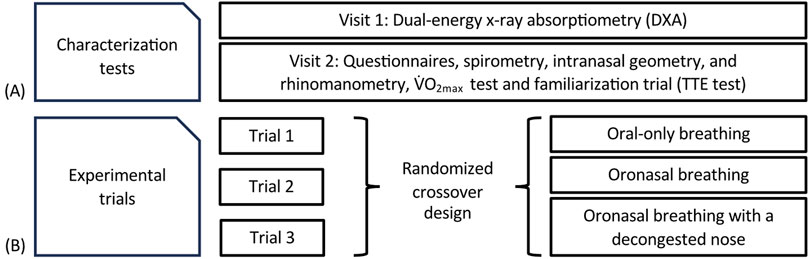
Figure 1. Flowchart of the study design and schematic of (A) the characterization tests; and (B) the experimental exercise trials. TTE; Time to exhaustion.
The study employed a novel design to evaluate nasal dynamics during oronasal breathing in endurance exercise. This was achieved by combining standardized cardiopulmonary exercise testing (CPET) with systematic nasal examinations across a range of exercise intensities, from low intensity up to
(i) oral-only breathing (with the nose occluded using a nose clip);
(ii) oronasal breathing; and
(iii) oronasal breathing following nasal decongestion.
The minimum washout period between trials was 4 days, with a mean duration of 23 ± 14 days between the first and third experimental session. To ensure adherence to the assigned breathing routes, all participants wore a standard V2 face mask (Hans Rudolph Inc., United States). In the oral-only condition, nasal airflow was mechanically occluded using a nose clip positioned beneath the mask to prevent nasal breathing. In the oronasal condition, no such restriction was applied. Investigators continuously monitored participants throughout each test to verify breathing route adherence. Although the mask itself does not restrict nasal airflow, the combination of the nose clip in the oral-only condition and continuous visual monitoring minimized the risk of unintentional deviation. In the nasal decongestion trial, participants were administered oxymetazoline 0.5 mg/mL (Otrivin®; Haleon Denmark ApS, Copenhagen, Denmark), with two sprays in each nostril 10 min before exercise onset to reduce congestion of the nasal mucosa.
Variables related to CPET measurements collected during the experimental trials included: oxygen consumption (
Participants were instructed to refrain from alcohol and vigorous physical activity during the 24 h preceding each visit. Upon arrival at the CHP, height and nude body mass (BM) were measured (seca 764; seca GmbH, Hamburg, Germany), and hydration status was assessed via urine specific gravity (USG), with values ≤ 1.025 (Atago Co. Ltd., Tokyo, Japan) considered as indicative of euhydration. All exercise tests were performed on a cadence-independent cycle ergometer (LC7TT; Monark AB, Vansbro, Sweden) under standardized environmental conditions (ambient pressure, 759 ± 10 mmHg; temperature, 20.5°C ± 0.5°C; relative humidity, 31.7% ± 3.0%) (Vaisala PTU300; Vaisala Oyj, Vantaa, Finland). Gas exchange parameters (
2.3 Characterization tests
At the first characterization visit (Figure 1), body composition was assessed following an overnight fast using dual-energy x-ray absorptiometry (DXA; GE Medical Systems, Madison, WI, United States). The accompanying enCore software (ver. 16.10) was used to calculate automatically the whole-body fat mass and fat-free mass. To standardize the pre-assessment conditions, participants were instructed to consume 500 mL of water upon waking and to use a low-intensity mode of transportation (e.g., walking or cycling with minimal effort) to the CHP laboratory.
At the second characterization visit, a multi-step nasal examination was performed prior to the experimental trials. First, the participants completed a nose-related questionnaire to assess potential nasal obstruction. Subsequently, an ENT specialist conducted an anterior rhinoscopic examination to identify any significant anatomical abnormalities, such as septal deviation, nasal polyps or signs of nasal inflammation.
The
2.4 Experimental trials
The experimental trial protocol is illustrated in Figure 2. Each test consisted of five 6-min submaximal, steady-state exercise stages followed by a sixth stage–an incremental maximal performance test to exhaustion.
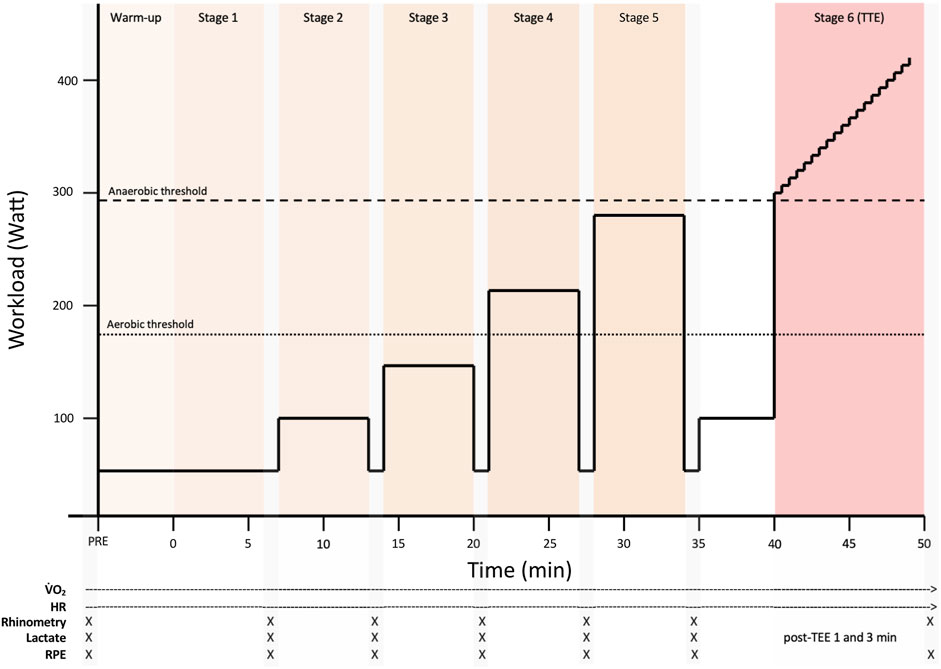
Figure 2. An overview of the experimental trial protocol. Each trial consisted of five 6-min submaximal, steady-state exercise stages followed by a sixth stage–an incremental maximal performance test to exhaustion. HR = Heart rate, RPE = Rating of perceived exertion, TTE = Time to exhaustion.
The protocol was designed to span a physiologically relevant range from low to near-maximal intensities, covering workloads below, at, and above the first (LT1) and second (LT2) lactate thresholds, in accordance with established submaximal testing guidelines (Binder et al., 2008; Faude et al., 2009). After a warm-up at 50 W (50 rpm), stages 1 and 2 were set at 50 W and 100 W, both at 50 rpm, to provide low-intensity steady-state conditions for baseline respiratory and metabolic assessment. These stages also allowed all participants to perform identical absolute workloads, facilitating comparisons at matched submaximal levels. Given their low intensity, they fall within the range where a shift from nasal to oral breathing may occur (Niinimaa et al., 1980).
Stages 3–5 were performed at 40%, 58%, and 75% of each participant’s Wmax (149 ± 18 W, 216 ± 26 W, and 280 ± 34 W) at 80 rpm, approximating LT1 and LT2 in trained endurance athletes while reflecting typical performance cadence. Following a 1-min recovery at 50 W and a 5-min re-warm-up at 40% Wmax, the final stage began at 80% Wmax with a 1 W/6 s ramp at 90 rpm, consistent with validated protocols for inducing exhaustion while minimizing pacing effects (Bentley et al., 2007). CPET-related variables were measured continuously throughout each stage using a metabolic cart. For stages 1–5, gas exchange parameters, including
Nasal airway measurements were conducted immediately following each stage (Stages 1–6). Intranasal geometry was assessed using acoustic rhinometry, and nasal airflow resistance (NAR) was evaluated using anterior active rhinomanometry (A1 Acoustic Rhinometer and NR6 Rhinomanometer; GM Instruments, Irvine, Scotland). These assessments were also performed before trial. Rhinomanometry was conducted with a pressure probe inserted into one nostril and sealed with a foam plug. A transparent face mask covered the nose and mouth, measuring the airflow in the open nostril during nasal-only breathing with the mouth closed. The procedure was then repeated on the contralateral side. Data from three automatically approved breaths per side were used for the analysis. Acoustic rhinometry was performed with a nosepiece fitted to the nostril to prevent leakage. Each side was measured five times while the participant held their breath with a slightly open mouth.
During the final performance stage, gas exchange variables and heart rate values were averaged over the final minute of effort. The RPE was recorded immediately upon termination, and lactate was measured at 1 and 3 min post-exercise. Spirometry was conducted before each test using a nose clip (Spiro-SP TrueFlow, Spirare; Diagnostica AS, Oslo, Norway).
3 Statistical analyses
Descriptive statistics are presented as mean and standard deviations. Cohen’s d (d) was calculated as a standardized measure of effect size for pairwise comparisons. Data were analyzed with mixed models to account for the repeated measurements, with random effects for subject and breathing mode. For stage (of the incremental exercise test), we modeled the dependence among residuals (R-side effects) with a first-order autoregressive covariance structure, i.e., AR (1), in some cases with a heterogenous variance, i.e., ARH (1). We considered different types of covariance matrices (variance components, compound symmetry, unstructured, compound symmetry with separate parameters across levels) and selected the ones with the lowest Akaike information criterion where convergence was attained. All analyses were performed using SAS version 9.4 TS1M7 (SAS Institute, Cary, North Carolina, United States). A two-sided p-value <0.05 was considered statistically significant.
4 Results
The results of the three experimental trials, including performance-related variables, are shown in Table 1, and their associated effect size estimates (Cohen’s d) are detailed in Table 2. The values of Wmax during the time-to-exhaustion test did not differ significantly (p > 0.05) between the breathing modes. The time to exhaustion was 2.8% shorter with oral-only breathing compared to oronasal breathing (d = −0.19), and 4.2% shorter compared to oronasal breathing with nasal decongestion (d = −0.28); however, these differences were not statistically significant (p > 0.05). No significant differences were observed between the three breathing modes for RPE, RF,
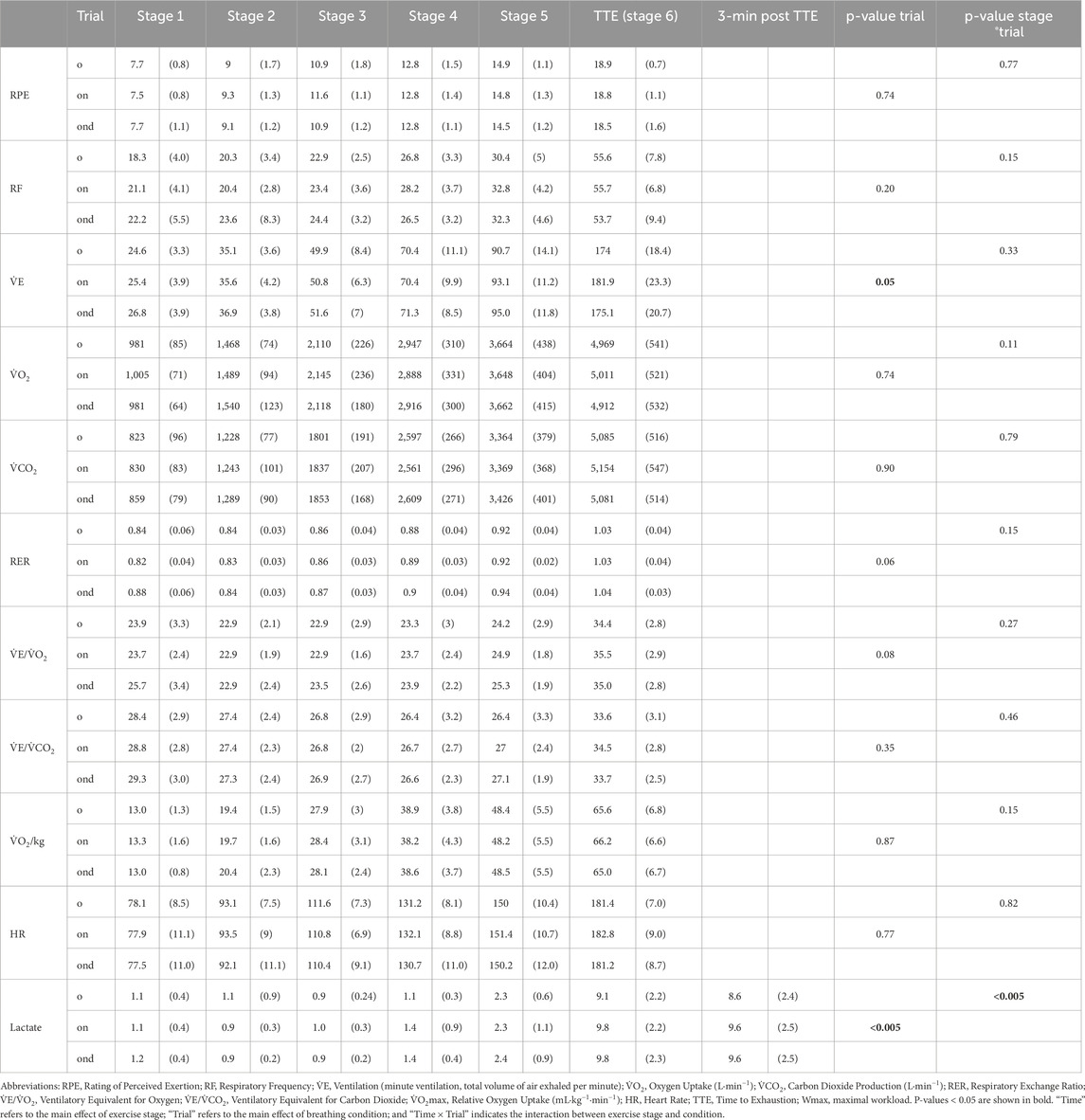
Table 1. Cardiopulmonary, perceptual, metabolic, and performance responses across six incremental exercise stages and at 3 min post–time to exhaustion (TTE) in well-trained endurance athletes (N = 12), assessed under three experimental conditions: oral-only breathing (o), oronasal breathing (on), and oronasal breathing with a decongested nose (ond). Data are presented as mean (SD).
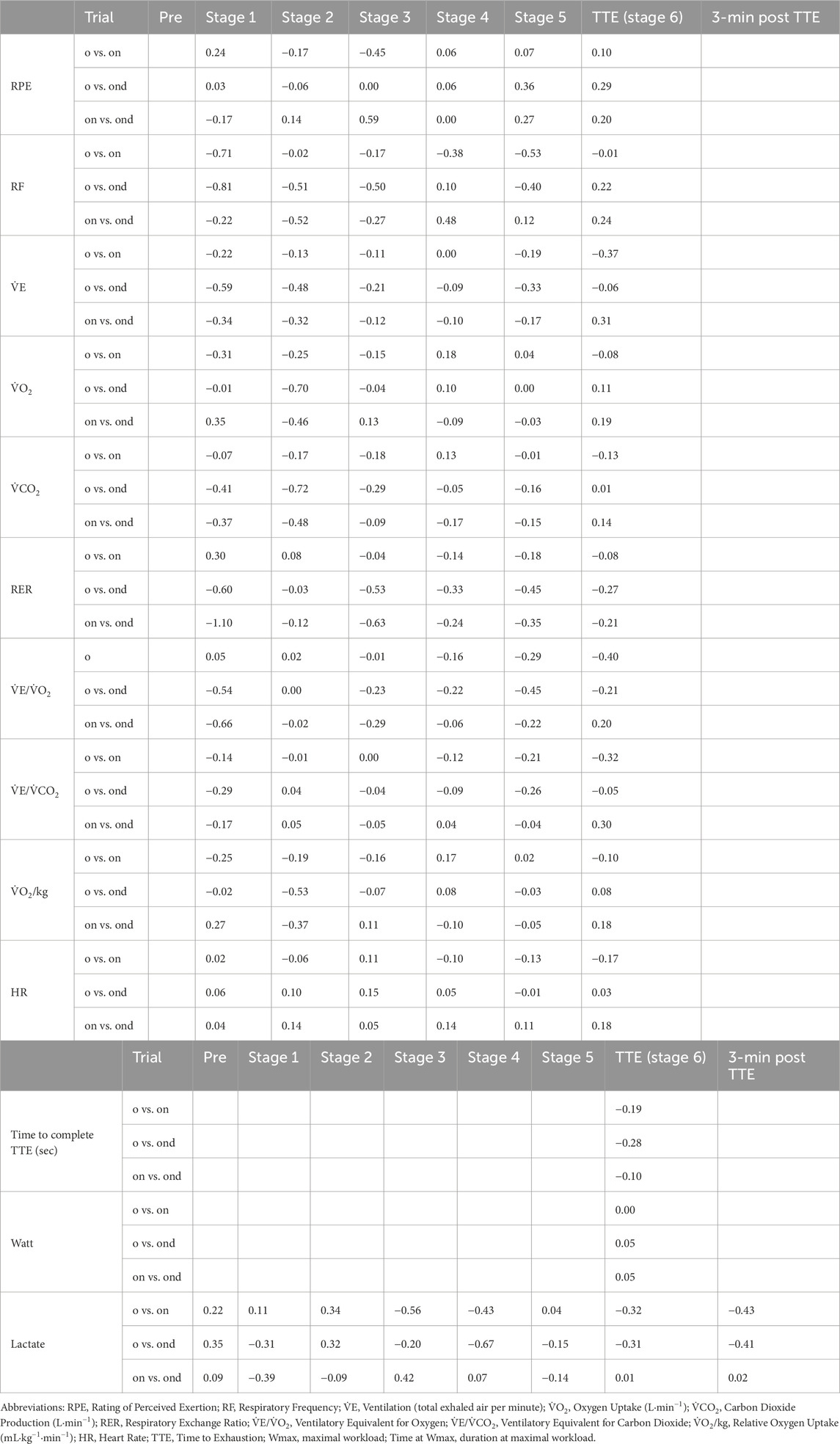
Table 2. Effect size estimates (Cohen’s d) for cardiopulmonary, perceptual, metabolic, and performance responses across six incremental exercise stages and at 3 min post time to exhaustion (TTE) in 12 well-trained endurance athletes (N = 12) under three experimental conditions: oral-only breathing (o), oronasal breathing (on), and oronasal breathing with a decongested nose (ond).
The results for the mean NAR, mean nasal airflow, mean minimal cross-sectional area (MCA), and mean nasal volume are listed in Table 3 and Figure 3. There were no significant differences (p > 0.05) in the nasal function measures between the three breathing modes.
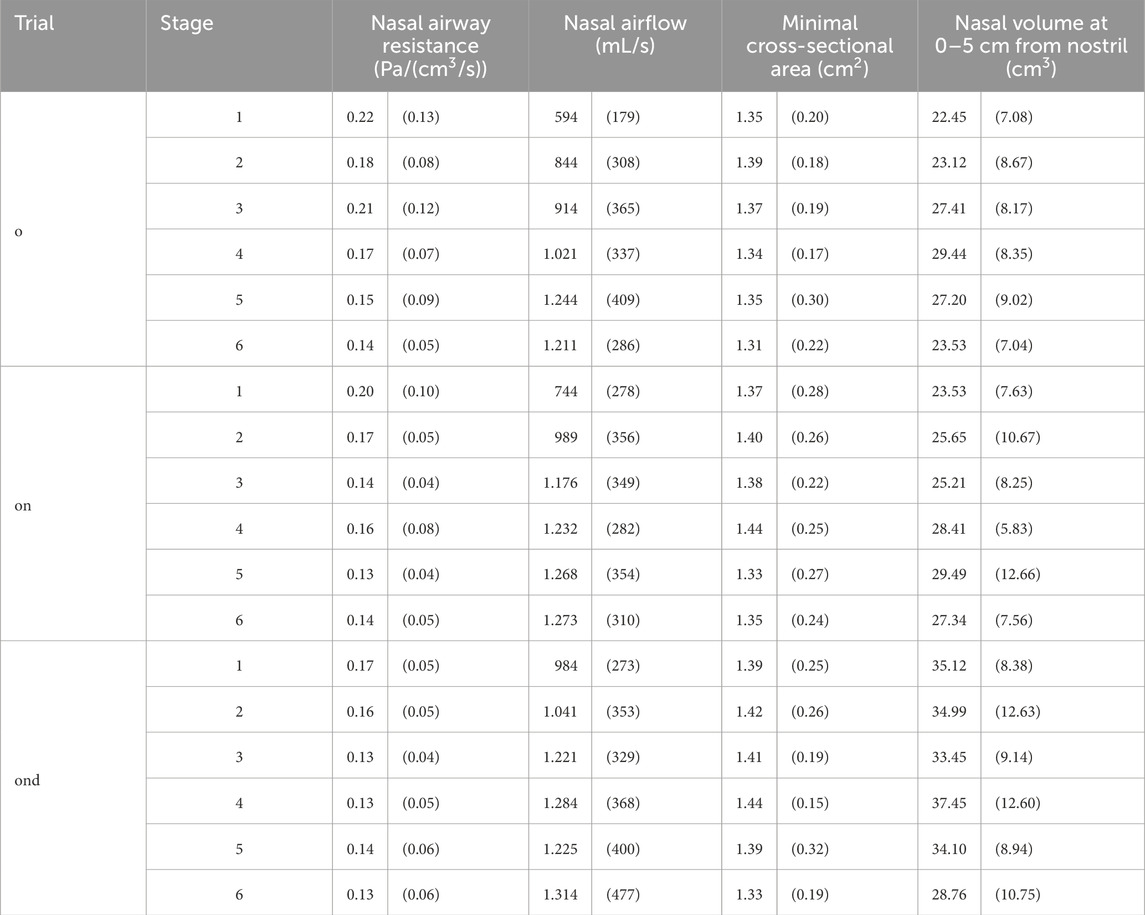
Table 3. Mean nasal airway resistance and mean nasal airflow, mean minimal cross-sectional area and mean nasal volume at 0–5 cm from the nostril at the 6 stages during: oral-only breathing (o), oronasal breathing (on) and oronasal breathing with a decongested nose (ond). Data are presented as mean (SD).
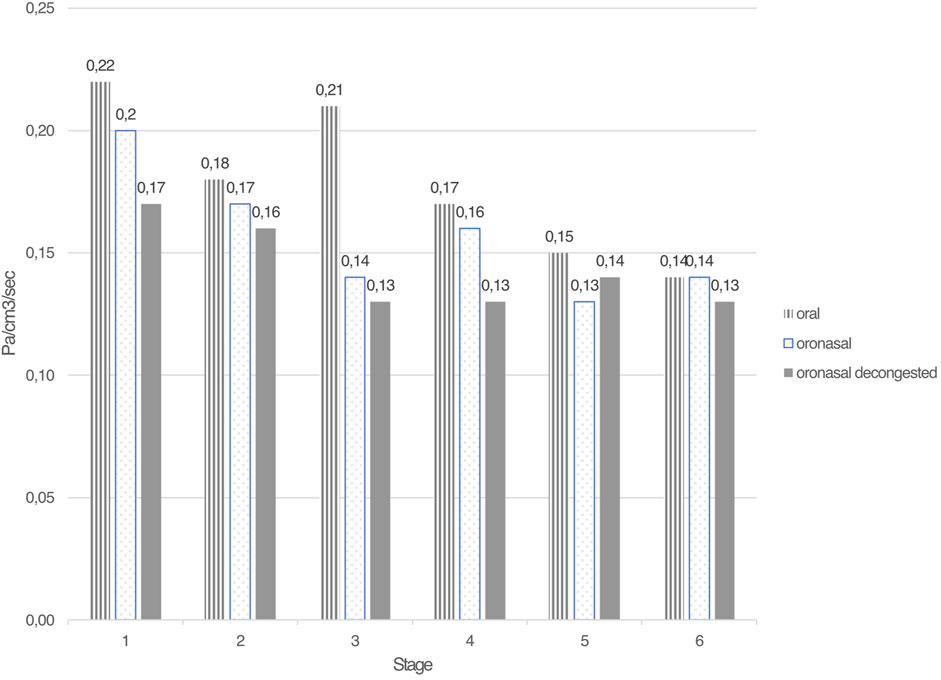
Figure 3. Mean nasal airway resistance (in Pa/cm3/sec) for the 6 test stages during oral-only, oronasal and oronasal decongested breathing.
5 Discussion
This randomized, controlled, cross-over trial investigated the effects of oral-only (mouth) breathing versus oronasal breathing–with and without nasal decongestion–during a graded maximal exercise test. The outcomes included performance (power output and TTE), pulmonary gas exchange variables, blood lactate concentrations, HR values, and perceived exertion levels in well-trained, male endurance athletes. No significant differences were observed between the three breathing conditions during the incremental (submaximal) stages. However, performance during the final stage, i.e., the maximal test to exhaustion, was notably, albeit not significantly, lower during the oral-only condition compared to oronasal breathing, with or without nasal decongestion. In contrast, the mean capillary blood lactate concentrations were significantly lower with oral-only breathing compared to the oronasal breathing conditions. All participants reported a low subjective sensation of nasal obstruction on the VAS scale at baseline, exhibited normal spirometry before each test, and their levels of nasal airway resistance were reduced by more than 50% between the start and end of the three experimental tests, as expected (Table 3) (Forsyth et al., 1983).
Although
Although not statistically significant, the 2.8% and 4.2% longer times to exhaustion observed during oronasal breathing, without and with nasal decongestion, respectively, compared to oral-only breathing, suggest a subtle performance benefit that is potentially meaningful in competitive settings where marginal gains are critical. The corresponding effect sizes (Cohen’s d = 0.19 and 0.28) were small, with the latter nearing the threshold for a moderate effect. Based on Cohen’s established guidelines (d ≈ 0.2 = small, 0.5 = moderate, 0.8 = large), such effects may still have practical relevance for elite athletes, for whom small improvements can influence the outcomes (Cohen, 1988). Further research is warranted to explore the ergogenic potentials of nasal decongestion strategies across different exercise modes, intensities, and durations.
In addition to
5.1 Strengths and limitations
A key strength of the present study is the inclusion of capillary blood lactate level as an objective marker of exercise intensity, complementing other physiologic and ventilatory parameters. The use of time to exhaustion and power output as performance outcomes, alongside HR, ventilatory equivalents, and perceived exertion, provide a comprehensive physiologic profile. A limitation of this study is the absence of arterial oxygen pressure (PaO2) or peripheral oxygen saturation (SpO2) measurements during exercise. Consequently, it is not possible to determine whether participants experienced exercise-induced hypoxemia (EIH), commonly defined as a ≥10 mmHg drop in PaO2 and a ≥5% reduction in arterial oxygen saturation (SaO2) during intense exercise compared to resting values (Dempsey et al., 1984). Given the high aerobic capacity of the participants, EIH cannot be ruled out as a potential factor influencing oxygen delivery and performance. Another notable strength is the relatively homogeneous group of participants, in that all the subjects were well-trained male cyclists, highly experienced in their sport and familiar with cycle ergometry testing. This reduced the inter-individual variability related to sex, fitness level, sport-specific adaptations, and testing familiarity, which are factors that could have influenced the results in previous studies. Although participants were uniformly well-trained and familiar with ergometer cycling, including both cyclists and triathletes may have introduced minor sport-specific differences (e.g., ventilatory mechanics; (Bentley et al., 2002)). However, the within-subject crossover design minimizes the impact of such variation on comparisons between breathing conditions. The present study also stands out for its detailed and repeated measurements of nasal airway function using both rhinomanometry and acoustic rhinometry, not only at rest but also during each incremental stage and post-exhaustion. This offers novel insights into the dynamic behavior of the nasal airflow during exercise. In line with earlier studies (Forsyth et al., 1983; Syabbalo et al., 1985), our findings confirm that there is a progressive reduction in nasal airway resistance during physical activity. There were no statistically significant differences in nasal resistance between the breathing modes, although a more-rapid reduction in resistance was observed under the decongested condition.
One limitation is that the experimental exercise trial used in this study has not been previously validated. However, the protocol was specifically designed to enable reliable and valid integration of cardiopulmonary exercise testing with repeated nasal airway assessments. Submaximal workloads were strategically selected to span a physiologic range that spanned from below to above the aerobic and anaerobic thresholds, while still ensuring steady-state conditions (Binder et al., 2008), making it appropriate for the dual purposes of this investigation. In addition to protocol validation, methodological constraints related to breathing route verification should also be acknowledged. A limitation is the inability to objectively verify precise breathing routes, particularly during oronasal trials. Although visual monitoring was used and nasal airflow was blocked in the oral-only condition, brief or subtle deviations may have gone undetected. While physical restrictions have been applied in low-intensity settings (Rappelt et al., 2023), real-time nasal airflow monitoring during high-intensity exercise remains technically and practically challenging.
6 Conclusion
This randomized, controlled cross-over trial shows that the time to exhaustion is 2.8% and 4.2% longer during oronasal breathing and decongested oronasal breathing, respectively, as compared with oral-only breathing. Although these differences did not reach statistical significance, effect size estimates (Cohen’s d = 0.19–0.28) suggest a small to potentially meaningful physiological impact. Oral-only breathing was associated with lower post-exercise blood lactate concentrations; however, this could reflect, at least partly, the shorter exercise duration, implying that reduced metabolic strain may result from less total work performed rather than from the breathing route itself.
Nevertheless, the consistent association between exclusive oral breathing and lower lactate suggests that breathing route may still influence lactate accumulation, warranting further investigation. Taken together, these findings imply that minimizing nasal airway resistance supports endurance performance, while exclusive oral breathing may alter metabolic responses. Future studies should explore nasal airflow dynamics and decongestion strategies across different exercise modalities and athlete populations.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Swedish Ethical Review Authority (Dnr. 2020-03808). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JB: Methodology, Supervision, Formal Analysis, Visualization, Conceptualization, Data curation, Software, Writing – original draft, Project administration, Writing – review and editing, Investigation. FR: Writing – original draft, Data curation, Software, Conceptualization, Writing – review and editing. FE: Investigation, Conceptualization, Funding acquisition, Formal Analysis, Writing – review and editing, Project administration, Resources, Data curation, Visualization, Methodology, Writing – original draft, Software. LS: Software, Writing – review and editing, Writing – original draft, Formal Analysis, Visualization, Methodology, Data curation, Validation, Conceptualization. MB: Supervision, Methodology, Formal Analysis, Project administration, Writing – review and editing, Writing – original draft, Conceptualization, Funding acquisition. SS: Methodology, Writing – review and editing, Supervision, Conceptualization, Writing – original draft. SP: Resources, Visualization, Project administration, Conceptualization, Writing – review and editing, Data curation, Validation, Funding acquisition, Software, Methodology, Writing – original draft, Formal Analysis, Supervision, Investigation. JH: Visualization, Data curation, Supervision, Project administration, Writing – review and editing, Validation, Formal Analysis, Methodology, Writing – original draft, Conceptualization, Investigation, Software, Resources, Funding acquisition.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Open access funding provided by the University of Gothenburg. The Swedish Research Council for Health, Working Life and Welfare, the ALF Agreement relating to the research and education of doctors (state funding), the Gothenburg Medical Society.
Acknowledgments
We thank Louise Hafsten, research nurse at the Department of ORL, Head and Neck Surgery, Sahlgrenska University Hospital, Gothenburg and Dr. Louise Hellgren, Lund University for their contributions to this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bartoloni B., Mannelli M., Gamberi T., Fiaschi T. (2024). The multiple roles of lactate in the skeletal muscle. Cells 13 (14), 1177. doi:10.3390/cells13141177
Bassett D. R., Howley E. T. (2000). Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med. Sci. Sports Exerc 32 (1), 70–84. doi:10.1097/00005768-200001000-00012
Benninger M. S., Sarpa J. R., Ansari T., Ward J. (1992). Nasal patency, aerobic capacity, and athletic performance. Otolaryngol. Head. Neck Surg. 107 (1), 101–104. doi:10.1177/019459989210700116
Bentley D. J., Millet G. P., Vleck V. E., McNaughton L. R. (2002). Specific aspects of contemporary triathlon: implications for physiological analysis and performance. Sports Med. 32 (6), 345–359. doi:10.2165/00007256-200232060-00001
Bentley D. J., Newell J., Bishop D. (2007). Incremental exercise test design and analysis: implications for performance diagnostics in endurance athletes. Sports Med. 37 (7), 575–586. doi:10.2165/00007256-200737070-00002
Binder R. K., Wonisch M., Corra U., Cohen-Solal A., Vanhees L., Saner H., et al. (2008). Methodological approach to the first and second lactate threshold in incremental cardiopulmonary exercise testing. Eur. J. Cardiovasc Prev. Rehabil. 15 (6), 726–734. doi:10.1097/HJR.0b013e328304fed4
Borg G. (1970). Physical training. 3. Perceived exertion in physical work. Lakartidningen 67 (40), 4548–4557.
Cohen J. (1988). Statistical power analysis for the behavioral sciences. New York, NY: Routledge. 2nd ed.
Dempsey J. A., Hanson P. G., Henderson K. S. (1984). Exercise-induced arterial hypoxaemia in healthy human subjects at sea level. J. Physiol. 355, 161–175. doi:10.1113/jphysiol.1984.sp015412
Dempsey J. A., Romer L., Rodman J., Miller J., Smith C. (2006). Consequences of exercise-induced respiratory muscle work. Respir. Physiol. Neurobiol. 151 (2-3), 242–250. doi:10.1016/j.resp.2005.12.015
Dinardi R. R., Ferreira C. H. S., Silveira G. S., de Araujo Silva V. E., da Cunha Ibiapina C., de Andrade C. R. (2021). Does the external nasal dilator strip help in sports activity? A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 278 (5), 1307–1320. doi:10.1007/s00405-020-06202-5
Faude O., Kindermann W., Meyer T. (2009). Lactate threshold concepts: how valid are they? Sports Med. 39 (6), 469–490. doi:10.2165/00007256-200939060-00003
Forsyth R. D., Cole P., Shephard R. J. (1983). Exercise and nasal patency. J. Appl. Physiol. Respir. Environ. Exerc Physiol. 55 (3), 860–865. doi:10.1152/jappl.1983.55.3.860
Haight J. S., Cole P. (1983). The site and function of the nasal valve. Laryngoscope 93 (1), 49–55. doi:10.1288/00005537-198301000-00009
Harms C. A., Babcock M. A., McClaran S. R., Pegelow D. F., Nickele G. A., Nelson W. B., et al. (1997). Respiratory muscle work compromises leg blood flow during maximal exercise. J. Appl. Physiol. 82 (5), 1573–1583. doi:10.1152/jappl.1997.82.5.1573
LaComb C., Lee S.-P., Young J., Navalta J. (2017). Oral versus nasal breathing during moderate to high intensity submaximal aerobic exercise. Int. J. Kinesiol. Sports Sci. 5, 8. doi:10.7575//aiac.ijkss.v.5n.1p.8
Lundberg J. O. (2008). Nitric oxide and the paranasal sinuses. Anat. Rec. Hob. 291 (11), 1479–1484. doi:10.1002/ar.20782
Lundberg J. O., Settergren G., Gelinder S., Lundberg J. M., Alving K., Weitzberg E. (1996). Inhalation of nasally derived nitric oxide modulates pulmonary function in humans. Acta Physiol. Scand. 158 (4), 343–347. doi:10.1046/j.1365-201X.1996.557321000.x
Meir R., Zhao G. G., Zhou S., Beavers R., Davie A. (2014). The acute effect of mouth only breathing on time to completion, heart rate, rate of perceived exertion, blood lactate, and ventilatory measures during a high-intensity shuttle run sequence. J. Strength Cond. Res. 28 (4), 950–957. doi:10.1519/JSC.0000000000000246
Niinimaa V., Cole P., Mintz S., Shephard R. J. (1980). The switching point from nasal to oronasal breathing. Respir. Physiol. 42 (1), 61–71. doi:10.1016/0034-5687(80)90104-8
Niinimaa V., Cole P., Mintz S., Shephard R. J. (1981). Oronasal distribution of respiratory airflow. Respir. Physiol. 43 (1), 69–75. doi:10.1016/0034-5687(81)90089-x
Nishimura M. (2015). High-flow nasal cannula oxygen therapy in adults. J. Intensive Care 3 (1), 15. doi:10.1186/s40560-015-0084-5
Pettersson S., Ahnoff M., Edin F., Lingstrom P., Simark Mattsson C., Andersson-Hall U. (2020). A hydrogel drink with high fructose content generates higher exogenous carbohydrate oxidation and lower dental biofilm pH compared to two other, commercially available, carbohydrate sports drinks. Front. Nutr. 7, 88. doi:10.3389/fnut.2020.00088
Rappelt L., Held S., Wiedenmann T., Deutsch J. P., Hochstrate J., Wicker P., et al. (2023). Restricted nasal-only breathing during self-selected low intensity training does not affect training intensity distribution. Front. Physiol. 14, 1134778. doi:10.3389/fphys.2023.1134778
Recinto C., Efthemeou T., Boffelli P. T., Navalta J. W. (2017). Effects of nasal or oral breathing on anaerobic power output and metabolic responses. Int. J. Exerc Sci. 10 (4), 506–514. doi:10.70252/EHDR7442
Seiler S. (2010). What is best practice for training intensity and duration distribution in endurance athletes? Int. J. Sports Physiol. Perform. 5 (3), 276–291. doi:10.1123/ijspp.5.3.276
Sheel A. W., Derchak P. A., Morgan B. J., Pegelow D. F., Jacques A. J., Dempsey J. A. (2001). Fatiguing inspiratory muscle work causes reflex reduction in resting leg blood flow in humans. J. Physiol. 537 (Pt 1), 277–289. doi:10.1111/j.1469-7793.2001.0277k.x
Syabbalo N. C., Bundgaard A., Widdicombe J. G. (1985). Effects of exercise on nasal airflow resistance in healthy subjects and in patients with asthma and rhinitis. Bull. Eur. Physiopathol. Respir. 21 (6), 507–513.
Keywords: VO2max, lactate, nasal breathing, rhinomanometry, athlete
Citation: Bergqvist J, Reite F, Edin F, Schiöler L, Börjesson M, Steinsvåg S, Pettersson S and Hellgren J (2025) Effects of oral, oronasal, and oronasal breathing with a decongested nose during incremental maximal exercise testing of well-trained endurance athletes: a randomized cross-over study. Front. Physiol. 16:1654725. doi: 10.3389/fphys.2025.1654725
Received: 26 June 2025; Accepted: 26 August 2025;
Published: 24 September 2025.
Edited by:
Sabah Hussain, McGill University, CanadaReviewed by:
Seyed Houtan Shahidi, İstanbul Gedik University, TürkiyeGökhan Metin, Istanbul University, Türkiye
Copyright © 2025 Bergqvist, Reite, Edin, Schiöler, Börjesson, Steinsvåg, Pettersson and Hellgren. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: J. Bergqvist, am9lbC5iZXJncXZpc3RAZ3Uuc2U=
†These authors share senior authorship