 Louisa Barré
Louisa Barré Narinée Hovhannisyan
Narinée Hovhannisyan Caroline Bodet-Milin
Caroline Bodet-Milin Françoise Kraeber-Bodéré
Françoise Kraeber-Bodéré Gandhi Damaj3
Gandhi Damaj3- 1LDM-TEP Group, UMR6030 Imagerie et Stratégies Thérapeutiques des Pathologies Cérébrales et Tumorales, Caen, France
- 2Service de Médecine Nucléaire, Centre Hospitalier Universitaire de Nantes, Nantes, France
- 3Department of Hematology, University Hospital Center of Caen, Caen, France
With the emergence of PET/CT using 18F-FDG, molecular imaging has become the reference for lymphoma lesion detection, tumor staging, and response assessment. According to the response in some lymphoma subtypes it has also been utilized for prognostication of disease. Although 18F-FDG has proved useful in the management of patients with lymphoma, the specificity of 18F-FDG uptake has been critically questioned, and is not without flaws. Its dependence on glucose metabolism, which may indiscriminately increase in benign conditions, can affect the 18F-FDG uptake in tumors and may explain the causes of false-positive imaging data. Considering these drawbacks, 18F-fludarabine, an adenine nucleoside analog, was developed as a novel PET imaging probe. An efficient and fully automated radiosynthesis has been implemented and, subsequently preclinical studies in xenograft murine models of hematological maligancies (follicular lymphoma, CNS lymphoma, multiple myeloma) were conducted with this novel PET probe in parallel with 18F-FDG. The results demonstrated several crucial points: tumor-specific targeting, weaker uptake in inflammatory processes, stronger correlation between quantitative values extracted from [18]F-fludarabine and histology when compared to 18F-FDG-PET, robustness during immunotherapy with rituximab, divergent responses between CNS lymphoma and glioblastoma (GBM). All these favorable findings permitted to establish a “first in man” study where 10 patients were enrolled. In DLBCL patients, increased uptake was observed in sites considered abnormal by CT and [18F]FDG; in two patients discrepancies were observed in comparison with 18F-FDG. In CLL patients, the uptake coincided with sites expected to be involved and displayed a significant uptake in hematopoietic bone marrow. No uptake was observed, whatever the disease group, in the cardiac muscle and brain. Moreover, its mean effective dose was below the effective dose reported for 18F-FDG. These preclinical and clinical findings revealed a marked specificity of 18F-fludarabine for lymphoma tissues. Furthermore, it might well be a robust tool for correctly quantifying the disease, in the presence of confounding inflammatory processes, thus avoiding false-positive results, and an innovative approach for imaging hematological malignancies.
Introduction
Cancer diagnosis has significantly been improved over the past decades, due to novel imaging agents that enable earlier detection. The challenge of an imaging technique is to demonstrate with accuracy the morphology and functional status of a tumor tissue. Historically, the staging and restaging of lymphoma have been established using CT. The higher accuracy of PET/CT using 18F-FDG in baseline lymphoma staging compared with traditional anatomical imaging techniques such as CT or MRI has profoundly changed the management of patients. This investigation appears as the most efficient in the initial assessment and appreciation of the therapeutic response. In addition, this approach affords important information in terms of prognosis and can lead to an optimization of the therapeutic strategy. Although PET/CT is a non-invasive imaging technique, which constitutes one of its major advantages, the findings using 18F-FDG may be misinterpreted to differentiate uptake within a site of cancer from uptake in a site of inflammation or infection. In fact, false-positives occur because 18F-FDG is taken up in any process associated with increased glycolysis such as inflammation, infection, or granulomatous disease. On the other hand, it is to highlight that normal physiological uptake of 18F-FDG into the brain, heart, digestive tract will mask the lesion, and hence downgrade the disease falsely. A consensus exists to consider 18F-FDG-PET more valuable in Hodgkin's disease and early-stage aggressive non-Hodgkin's lymphoma (NHL) and less useful in indolent NHL which represent 40% of all non-Hodgkin lymphoma subtypes (1–3).
Based on the characteristics of 18F-FDG-PET, novel imaging probe must be developed to fulfill the need of a more specific radiopharmaceutical for a better tumor delineation and a more precise evaluation of the response to therapy. To improve the diagnostic accuracy, in particular in lymphoma with a fluctuating 18F-FDG avidity, 18F-fludarabine was introduced as a novel PET probe. Though, 18F-fludarabine appears to be an appealing tool in evaluation of suspicious finding on 18F-FDG PET both before or after treatment (4).
Our approach was based on the therapeutic activity of fludarabine, alone or in combination with other active drugs, in the clinical treatment of lymphoid malignancies and more particularly in the treatment of lymphoma that have a low proliferative index. Fludarabine is transported into the cells and phosphorylated intracellularly into its triphosphate form, by the deoxycytidine kinase, the principal active compound. One of the characteristics of this drug is its cellular accumulation, which is cell-cycle-independent (5). This nucleoside analog which has a fluorine atom is resistant to deamination resulting in a therapeutic activity. To elaborate a probe for PET imaging, the fluorine atom was replaced by a fluorine-18. The manufacturing process, which includes efficiency of radiolabeling, purification, and stability of the final product, automation, was subject to various quality control tests prior to 18F-fludarabine implementation for in vivo studies (6).
Radiosynthesis of 18F-Fludarabine
The most reliable radiosynthesis of 18F-fludarabine involved a simple two-step procedure. The strategy reported for the radiolabeling was based on a nucleophilic substitution of a nitro group at the two-position on the purine ring to act as a leaving group. The protected nitro precursor, described as a 2-nitro-pentabenzoyl adenosine derivative, was involved in a classical fluorination reaction using K18F/K222 followed by an intermediate purification on a Sep-Pak silica.
To generate 18F-fludarabine, hydrolysis of benzoyl groups using a mixture of methanol/aqueous ammonia was applied before a final HPLC purification. The robustness of the described process (radiochemical yield 48 ± 3%, specific activity 310 ± 72 GBq/μmol, radiochemical purity up to 99%) allowed us to initiate several preclinical studies and a first-in-man clinical trial (6).
Preclinical Studies
In preliminary studies biodistribution or pharmacokinetic properties, metabolism, and dosimetry were established on control animals which are important prerequisites, before testing 18F-fludarabine on animal models of hematological malignancies.
18F-Fludarabine in Control Animals
The accumulated activity of 18F-fludarabine, over 1 h period and after i.v. injection (5–12 MBq), was preferentially in the spleen and the kidneys which, respectively, confirmed the selectivity for lymphoid organ, and demonstrated its renal excretion (7). Moreover, our in vivo findings indicated no degradation of the probe 60 min post injection, which is an ideal characteristic for an imaging agent. To estimate the maximum dosage of 18F-fludarabine that could be safely administrated to patients, radiation dose was calculated in major organs; the results revealed that the urinary bladder wall, considered as a limiting organ, received the highest dose. Nevertheless, the effective dose obtained by extrapolation of animal data to humans, was consistent (7.3 mSv) with the previously reported values of 18F-FDG (3.8–10.7 mSv) (8).
18F-Fludarabine in a Xenograft Model of Human Follicular Lymphoma
Follicular lymphoma is the most common subtype of indolent lymphoma. This lymphoma is FDG-avid and PET/CT using 18F-FDG is the current standard tool in its management in humans (9). To determine the potential of 18F-fludarabine and to acquire comparative preclinical data with 18F-FDG, biodistribution was carried out in parallel on a SCID xenografted tumor model. A marked difference in their behavior was observed which was in favor of 18F-fludarabine: in the tumor, its accumulation increased rapidly to reach a plateau within 20 min and its specific binding led to high-contrast images by comparison with 18F-FDG (Figure 1A). The clear positive correlation (p < 0.001) between the tracer uptake in the tumor and the density of lymphoid cells (determined by histological analysis) highlighted, the sensitivity of 18F-fludarabine. It was also important to demonstrate that the treatment with the anti-CD20 antibody rituximab did not have any negative influence on the tumor-targeting ability and, we hypothesized that 18F-fludarabine could be able to detect residual disease under treatment (10).
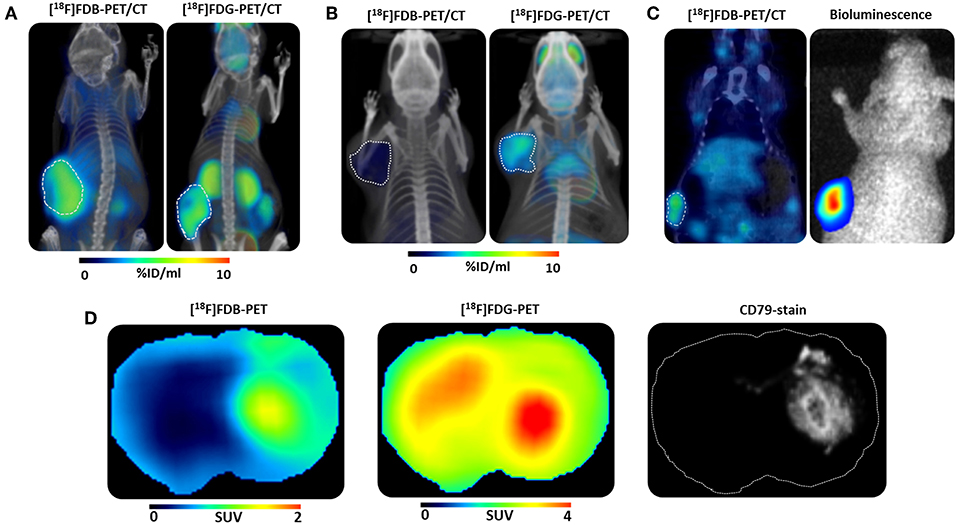
Figure 1. Preclinical studies. 3D illustration of μPET/CT fused scans with [18F]Fludarabine ([18F]FDB) and [18F]Fluorodeoxyglucose ([18F]FDG) in (A) mice bearing human follicular lymphoma xenograft, reproduced from Hovhannisyan et al. (10), no permission required (B) inflammation-bearing mouse, reproduced from Hovhannisyan et al. Copyright 2016 American Chemical Society (11), permission obtained (C) μPET/CT scan with [18F]FDB and corresponding bioluminescence image of a mouse bearing human multiple myeloma xenograft, reproduced from Hovhannisyan et al. (12), no permission required (D) Representative co-registered μPET scans and corresponding immunohistochemistry image of a mouse bearing human CNS lymphoma xenograft, reproduced from Hovhannisyan et al. (13), no permission required.
18F-Fludarabine in a Murine Model of Inflammation
The major drawback of 18F-FDG is its uptake in inflammatory tissue providing false-positives which could lead to a misinterpretation and perhaps an overtreatment of the patient. For this purpose, our reflex was to test 18F-fludarabine and compare to 18F-FDG in a previously described murine model of inflammation (14). The PET image analysis revealed that the uptake of this novel radiopharmaceutical in the inflamed tissue is negligible compared to 18F-FDG (Figure 1B). These results enhance the potential of 18F-fludarabine as a more specific probe (11).
18F-Fludarabine in Brain Tumors (CNS Lymphoma vs. Glioblastoma)
Primary central nervous system lymphoma (PCNSL) account for 5% of primary brain tumors and are predominantly diffuse large B cell lymphoma (90% of cases). MRI is the reference imaging for the diagnosis and monitoring (15). The evaluation of the therapeutic response, based on MRI, is perfectible. This imaging modality can miss atypical forms not enhanced by gadolinium and the significance of contrast enhancement occurring under or after treatment is sometimes ambiguous (16). 18F-FDG is established as the reference imaging in systemic lymphomas, but its applications in PSNCL are restricted by the limited specificity of cerebral fixations, and high uptake in healthy brain tissue (17). Taken into account the limitations of 18F-FDG, we demonstrated in a human CNS lymphoma model the pertinence to use 18F-fludarabine to detect brain lesions and we established its superiority over18F-FDG in differentiating brain tumors (13).
In the CNS lymphoma model, which closely mimics disseminated lesions, a marked retention was observed with 18F-fludarabine in accordance with histological findings (CD79 staining) representative of cells lymphoma (p < 0.001). 18F-Fludarabine exhibited tumor to background ratio (TBR) 2 to 3-fold higher than 18F-FDG, this made delineation of the tumor more precise. 18F-FDG, on the other hand, is poor in accurate delineation of the lesion due to its normal physiological brain uptake and poor specificity (Figure 1D). Considering high-grade glioma (GBM) and CNS lymphoma differentiation, the diagnostic accuracy is uncertain due to a similar imaging appearance on MRI or the previously described limitations of 18F-FDG. The scenario to use 18F-fludarabine is relevant taking into consideration that this probe has a rapid clearance from glioblastoma and this feature can help to discriminate between both brain tumors.
18F-Fludarabine in Multiple Myeloma (MM)
Multiple myeloma (MM) is a clonal plasma cells that accounts for 15% of all hematological malignancies. 18F-FDG is an accepted imaging technique to assess and monitor myeloma therapy. Despite the fact that 18F-FDG is reasonably sensitive and specific for bone disease, the detection of diffuse infiltration of plasma-cells in bone marrow, and lytic lesions in the skull is underestimated (1, 19). Based on our previous results in the animal models, 18F-fludarabine was then considered in a xenograft MM murine model. The tumor growth was followed by bioluminescence (BLI), after injection of a luciferase reporter MM cell line and characterized by immunohistochemistry (IHC, CD 138 staining) (Figure 1C). To compare with 18F-FDG, the metabolically active tumor was defined for both radiotracers (12). Although the 18F-FDG uptake was superior, the quantitative data extracted from IHC or BLI are in better agreement with the 18F-fludarabine uptake. These findings enforce the hypothesis that this radiopharmaceutical could be more suitable to detect MM disease.
Clinical Study
The reported preclinical studies revealed the real potential of 18F-fludarabine to detect hematological malignancies and have resulted in the design of a clinical research protocol. This novel PET probe has been evaluated in human to better identify pathological from physiological or inflammatory uptake at initial staging of the disease and, in the future to enhance PET performance for therapeutic evaluation. Ten untreated patients with either B-cell chronic lymphocytic leukemia (B-CLL, n = 5) or diffuse large B-cell lymphoma (DLBCL, n = 5) were included in the study (18). CLL imaging with 18F-FDG-PET is not recommended, except in the case of suspected disease transformation (Richter syndrome), in contrast to DLBCL disease where it is being included as part of clinical practice. Nevertheless, despite an excellent sensitivity, the analysis of some areas remains difficult due to the lack of 18F-FDG specificity (bone marrow or spleen for example). Despite new criteria (20), the interpretation of 18F-FDG-PET positivity after therapy remains difficult, partly due to tumor-, and/or treatment-associated inflammation leading to false positives (4).
The design of the pilot clinical trial was to acquire six successive partial body scans for 250 min (0–10, 15–25, 30–50, 90–100, 180–190, 240–250 min) after i.v. injection of 18F-fludarabine (4 MBq/kg) in both groups. In all patients, any side effects were observed to the radiopharmaceutical injection. The average activity received by the patients was 305 ± 76 MBq with a 18F-fludarabine mass of 0.23 ± 0.14 μg. The results with conventional modalities CT and [18F]FDG-PET (for DLBCL) were investigated. The imaging session was performed 60–80 min after injection of 335 ± 77MBq of 18F-FDG. In DLBCL patients, increased uptake of 18F-fludarabine was observed in sites deemed suspicious by CT and/or 18F-FDG. At 50 min, SUVs were significantly higher in involved lesions (SUVmax = 7.1) in comparison with histologically normal bone marrow (SUVmax = 2.3) or ascending aorta considered as reference (SUVmax = 1.4). In this group, aged 57–73 years, divergence was observed in two patients. In one patient a positivity with 18F-FDG was detected and not with 18F-fludarabine in bilateral hilar foci. These foci persisted at subsequent evaluation with 18F-FDG and were considered as false positives (Figures 2B–D). Indeed this patient was free from relapse more than 2 years after the end of treatment. In the second patient, unilateral testicular lymphomatous infiltration was not observed with 18F-fludarabine and could be attributed to the role of the testis barrier (21). In CLL patients, aged 51–70 years, 18F-fludarabine revealed all involved lymph nodes, with also a marked accumulation in the spleen and bone marrow involvement. At 50 min, SUVmax was 1.5 on the mediastinal vascular noise (taken as reference) against 6.05 in the affected lymph nodes, 7.7 for the spleen, and 4.4 in bone marrow, indicating a very good tumor/tissue contrast (Figure 2A). In both groups, no physiological uptake was noted in heart and brain.
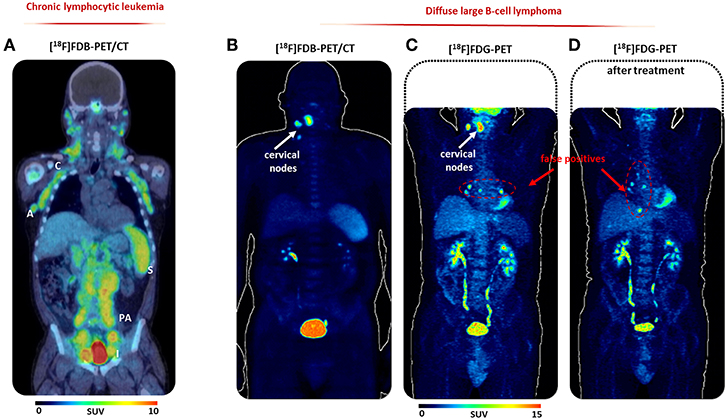
Figure 2. First-in-man study. (A) [18F]FDB-PET/CT (30–50 min scan period) of a representative CLL patient; (B) [18F]FDB-PET (30–50 min scan period), (C) [18F]FDG-PET (60–80 min), and (D) post-treatment (60–80 min) of a representative DLBCL patient, reproduced from Chantepie et al. (18), no permission required. A, axillary nodes; C, cervical nodes; I, iliac nodes; PA, paraaortic nodes; S, spleen.
Conclusion
This recent study as a “proof of concept” in human paved the way to several underway national clinical trials including a larger cohort of patients to define the role and prognostic impact of 18F-fludarabine-PET/CT in the management of hematological malignancies. An exploratory, multicenter prospective clinical trial to evaluate the interest of PET images using 18F-fludarabine for initial staging and therapeutic evaluation in three subtypes of newly diagnosed lymphomas (DLBCL, Hodgkin lymphoma, and follicular lymphoma) is ongoing.
Author Contributions
LB prepared a first draft of the manuscript. NH, CB-M, FK-B, and GD critically reviewed the manuscript. All authors conceived the idea of this review article and approved the final version.
Funding
All this research was supported by a grant from Commissariat à l'Energie Atomique et aux Energies Alternatives (CEA), the French National Agency for Research (ANR-11 LABEX-0018-01) and the Region Basse-Normandie.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors gratefully acknowledge the team Laboratoire de Développements Méthodologiques en TEP.
References
1. Valls L, Badve C, Avril S, Herrmann K, Faulhaber P, O'Donnell J, et al. FDG-PET imaging in hematological malignancies. Blood Rev. (2016) 30:317–31. doi: 10.1016/j.blre.2016.02.003
2. Ayers EC, Fardin S, Gholami S, Alavi A, Mato AR. Personalized management approaches in lymphoma: utility of fluorodeoxyglucose-PET imaging. PET Clin. (2016) 11:209–18. doi: 10.1016/j.cpet.2016.02.001
3. Alobthani G, Romanov V, Isohashi K, Matsunaga K, Watabe T, Kato H, et al. Value of 18F-FDG PET/CT in discrimination between indolent and aggressive non-Hodgkin's lymphoma: a study of 328 patients. Hell J Nucl Med. (2018) 21:7–14. doi: 10.1967/s002449910701
4. Barrington SF, Friedman K. PET/MRI in lymphoma. In: Iagaru A, Hope T, Veit-Haibach P, editors. PET/MRI in Oncology. Cham: Springer (2018). p. 373–400.
5. Grégoire V, Van NT, Stephens LC, Brock WA, Milas L, Plunkett W, et al. The role of fludarabine-induced apoptosis and cell cycle synchronization in enhanced murine tumor radiation response in vivo. Cancer Res. (1994) 54:6201–9.
6. Guillouet S, Patin D, Tirel O, Delamare J, Gourand F, Deloye JB, et al. Fully automated radiosynthesis of 2-[18F]fludarabine for PET imaging of low-grade lymphoma. Mol Imaging Biol. (2014) 16:28–35. doi: 10.1007/s11307-013-0657-4
7. Dhilly M, Guillouet S, Patin D, Fillsoye F, Abbas A, Gourand F, et al. 2-[18F]Fludarabine, a novel positron emission tomography (PET) tracer for imaging lymphoma: a micro-PET study in murine models. Mol Imaging Biol. (2014) 16:118–26. doi: 10.1007/s11307-013-0659-2
8. Deloar HM, Fujiwara T, Shidahara M, Nakamura T, Watabe H, Narita Y, et al. Estimation of absorbed dose for 2-[F-18]fluoro-2-deoxy-D-glucose using whole-body positron emission tomography and magnetic resonance imaging. Eur J Nucl Med. (1998) 25:565–74. doi: 10.1007/s002590050257
9. Wirth A, Foo M, Seymour JF, Macmanus MP, Hicks RJ. Impact of [18f]fluorodeoxyglucose positron emission tomography on staging and management of early-stage follicular non-Hodgkin lymphoma. Int J Radiat Oncol Biol Phys. (2008) 71:213–9. doi: 10.1016/j.ijrobp.2007.09.051
10. Hovhannisyan N, Guillouet S, Fillesoye F, Dhilly M, Patin D, Galateau F, et al. Evaluation of the specificity of [18F]fludarabine PET/CT in a xenograft model of follicular lymphoma: comparison with [18F]FDG and impact of rituximab therapy. EJNMMI Res. (2015) 5:23. doi: 10.1186/s13550-015-0101-7
11. Hovhannisyan N, Dhilly M, Guillouet S, Leporier M, Barré L. Comparative analysis between [18F]Fludarabine-PET and [18F]FDG-PET in a murine model of iInflammation. Mol Pharm. (2016) 13:2136–9. doi: 10.1021/acs.molpharmaceut.6b00050
12. Hovhannisyan N, Dhilly M, Fidalgo M, Fillesoye F, Guillouet S, Sola B, et al. [18F]Fludarabine-PET in a murine model of multiple myeloma. PLoS ONE. (2017) 12:e0177125. doi: 10.1371/journal.pone.0177125
13. Hovhannisyan N, Fillesoye F, Guillouet S, Ibazizene M, Toutain J, Gourand F, et al. [18 F]Fludarabine-PET as a promising tool for differentiating CNS lymphoma and glioblastoma: comparative analysis with [18F]FDG in human xenograft models. Theranostics. (2018) 8:4563–73. doi: 10.7150/thno.26754
14. Yamada S, Kubota K, Kubota R, Ido T, Tamahashi N. High accumulation of fluorine-18-fluorodeoxyglucose in turpentine-induced inflammatory tissue. J Nucl Med. (1995) 36:1301–6.
15. Hoang-Xuan K, Bessell E, Bromberg J, Hottinger AF, Preusser M, Rudà R, et al. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. Lancet Oncol. (2015) 16:e322–32. doi: 10.1016/S1470-2045(15)00076-5
16. Valles FE, Perez-Valles CL, Regalado S, Barajas RF, Rubenstein JL, Cha S. Combined diffusion and perfusion MR imaging as biomarkers of prognosis in immunocompetent patients with primary central nervous system lymphoma. Am J Neuroradiol. (2013) 34:35–40. doi: 10.3174/ajnr.A3165
17. Kawai N, Miyake K, Okada M, Yamamoto Y, Nishiyama Y, Tamiya T. Usefulness and limitation of FDG-PET in the diagnosis of primary central nervous system lymphoma. No Shinkei Geka. (2013) 41:117–26. doi: 10.11477/mf.1436101928
18. Chantepie S, Hovhannisyan N, Guillouet S, Pelage J-P, Ibazizene M, Bodet-Milin C, et al. 18F-Fludarabine-PET for lymphoma imaging: first-in-man study in DLBCL and CLL patients. J Nucl Med. (2018) 59:1380–5. doi: 10.2967/jnumed.117.206920
19. Cavo M, Terpos E, Nanni C, Moreau P, Lentzsch S, Zweegman S. Role of 18F-FDG PET/CT in the diagnosis and management of multiple myeloma and other plasma cell disorders: a consensus statement by the International Myeloma Working Group. Lancet Oncol. (2017) 18:e206–17. doi: 10.1016/S1470-2045(17)30189-4
20. Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E, et al. Andrew lister recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-hodgkin lymphoma: the Lugano classification. J Clin Oncol. (2014) 32:3059–67. doi: 10.1200/JCO.2013.54.8800
Keywords: 18F-fludarabine, lymphoma, PET—positron emission tomography, imaging, diagnosis
Citation: Barré L, Hovhannisyan N, Bodet-Milin C, Kraeber-Bodéré F and Damaj G (2019) [18F]-Fludarabine for Hematological Malignancies. Front. Med. 6:77. doi: 10.3389/fmed.2019.00077
Received: 07 February 2019; Accepted: 29 March 2019;
Published: 17 April 2019.
Edited by:
Anil Kumar Mishra, Institute of Nuclear Medicine & Allied Sciences (DRDO), IndiaReviewed by:
George K. Loudos, Technological Educational Institute of Athens, GreeceSerge Goldman, Free University of Brussels, Belgium
Baljinder Singh, Post Graduate Institute of Medical Education and Research (PGIMER), India
Copyright © 2019 Barré, Hovhannisyan, Bodet-Milin, Kraeber-Bodéré and Damaj. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Louisa Barré, YmFycmVAY3ljZXJvbi5mcg==