 Babette L. R. Reijs1*
Babette L. R. Reijs1* Charlotte E. Teunissen2
Charlotte E. Teunissen2 Nikolai Goncharenko3
Nikolai Goncharenko3 Fay Betsou3
Fay Betsou3 Kaj Blennow4
Kaj Blennow4 Inês Baldeiras5
Inês Baldeiras5 Frederic Brosseron6
Frederic Brosseron6 Enrica Cavedo7
Enrica Cavedo7 Tormod Fladby8,9
Tormod Fladby8,9 Lutz Froelich10
Lutz Froelich10 Tomasz Gabryelewicz11
Tomasz Gabryelewicz11 Hakan Gurvit12
Hakan Gurvit12 Elisabeth Kapaki13
Elisabeth Kapaki13 Peter Koson14,15
Peter Koson14,15 Luka Kulic16
Luka Kulic16 Sylvain Lehmann17
Sylvain Lehmann17 Piotr Lewczuk18,19
Piotr Lewczuk18,19 Alberto Lleó20,21
Alberto Lleó20,21 Walter Maetzler22,23Alexandre de Mendonça24
Walter Maetzler22,23Alexandre de Mendonça24 Anne-Marie Miller25José L. Molinuevo26
Anne-Marie Miller25José L. Molinuevo26 Brit Mollenhauer27,28
Brit Mollenhauer27,28 Lucilla Parnetti29
Lucilla Parnetti29 Uros Rot30
Uros Rot30 Anja Schneider31
Anja Schneider31 Anja Hviid Simonsen32
Anja Hviid Simonsen32 Fabrizio Tagliavini33
Fabrizio Tagliavini33 Magda Tsolaki34
Magda Tsolaki34 Marcel M. Verbeek35,36
Marcel M. Verbeek35,36 Frans R. J. Verhey1Marzena Zboch37
Frans R. J. Verhey1Marzena Zboch37 Bengt Winblad38
Bengt Winblad38 Philip Scheltens39
Philip Scheltens39 Henrik Zetterberg40,41
Henrik Zetterberg40,41 Pieter Jelle Visser1,39*
Pieter Jelle Visser1,39*
- 1Department of Psychiatry and Neuropsychology, School for Mental Health and Neuroscience, Alzheimer Center Limburg, Maastricht University Medical Center, Maastricht, Netherlands
- 2Neurochemistry Laboratory and Biobank, Department of Clinical Chemistry, VU University Medical Center, Amsterdam, Netherlands
- 3Integrated Biobank of Luxembourg, Luxembourg, Luxembourg
- 4Clinical Neurochemistry Laboratory, Department of Neuroscience and Physiology, Sahlgrenska University Hospital, The Sahlgrenska Academy at University of Gothenburg, Mölndal, Sweden
- 5Center for Neuroscience and Cell Biology, Institute for Biomedical Imaging and Life Sciences, Faculty of Medicine, University of Coimbra, Coimbra, Portugal
- 6German Center for Neurodegenerative Diseases (DZNE) e.V. Clinical Neuroscience and Biomarkers, Bonn, Germany
- 7Laboratory of Alzheimer’s Neuroimaging and Epidemiology, IRCCS Fatebenefratelli, Brescia, Italy
- 8Department of Neurology, Akershus University Hospital, Lørenskog, Norway
- 9Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 10Department of Geriatric Psychiatry, Central Institute of Mental Health, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
- 11Department of Neurodegenerative Disorders, Mossakowski Medical Research Centre, Polish Academy of Sciences, Warsaw, Poland
- 12Behavioural Neurology and Movement Disorders Unit, Department of Neurology, Istanbul Faculty of Medicine, Istanbul University, Istanbul, Turkey
- 13Neurochemistry Unit, Division of Cognitive and Movement Disorders, 1st Department of Neurology, National and Kapodistrian University of Athens, Athens, Greece
- 14Department of Neurology, Slovak Medical University, University Hospital Bratislava, Bratislava, Slovakia
- 15Institute of Neuroimmunology, Slovak Academy of Sciences, Bratislava, Slovakia
- 16Division of Psychiatry Research, University of Zurich, Schlieren, Switzerland
- 17Laboratoire de Biochimie Protéomique Clinique, INSERM U1183, Institut de Médecine Régénérative et Biothérapies, CHRU de Montpellier, Université de Montpellier, Montpellier, France
- 18Department of Psychiatry and Psychotherapy, Universitätsklinikum Erlangen and Friedrich-Alexander Universität Erlangen-Nürnberg, Erlangen, Germany
- 19Department of Neurodegeneration Diagnostics, Medical University of Bialystok, Bialystok, Poland
- 20Memory Unit, Department of Neurology, Hospital de la Santa Creu i Sant Pau-Biomedical Research Institute Sant Pau, Barcelona, Spain
- 21Centro de Investigación Biomédica en Red de Enfermedades Neurodegenerativas (CIBERNED), Madrid, Spain
- 22Department of Neurodegeneration, Hertie Institute for Clinical Brain Research, University of Tübingen, Tübingen, Germany
- 23German Center for Neurodegenerative Diseases (DZNE), University of Tübingen, Tübingen, Germany
- 24Faculty of Medicine, University of Lisbon, Lisbon, Portugal
- 25Medical Gerontology, School of Medicine, Trinity College Dublin, Dublin, Ireland
- 26ICN Hospital Clinic i Universitari, Institut d’Investigacions Biomèdiques August Pi i Sunyer, Barcelona, Spain
- 27Paracelsus-Elena-Klinik, Kassel, Germany
- 28Department of Neurosurgery and Institute of Neuropathology, University Medical Center Göttingen, Göttingen, Germany
- 29Section of Neurology, Centre for Memory Disturbances, University of Perugia, Perugia, Italy
- 30Laboratory for CSF Diagnostics, Department of Neurology, University Medical Centre, Ljubljana, Slovenia
- 31Department of Psychiatry and Psychotherapy, University Medical Center Göttingen and Translational Dementia Research Group, German Center for Neurodegenerative Diseases (DZNE), Göttingen, Germany
- 32Danish Dementia Research Centre, Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark
- 33Unit of Neuropathology, Department of Diagnostics and Technology, IRCCS Foundation “Carlo Besta” Neurological Institute, Milan, Italy
- 343rd Department of Neurology, Aristotle University of Thessaloniki, Thessaloniki, Greece
- 35Department of Neurology, Radboud Alzheimer Centre, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Centre, Nijmegen, Netherlands
- 36Department of Laboratory Medicine, Radboud Alzheimer Centre, Donders Institute for Brain, Cognition and Behaviour, Radboud University Medical Centre, Nijmegen, Netherlands
- 37Research-Scientific-Didactic Centre of Dementia-Related Diseases, Wrocław Medical University, Scinawa, Poland
- 38Division of Neurogeriatrics, Center for Alzheimer Research, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Huddinge, Sweden
- 39Department of Neurology, Alzheimer Center, VU University Medical Center, Amsterdam, Netherlands
- 40Department of Psychiatry and Neurochemistry, Institute of Neuroscience and Physiology, The Sahlgrenska Academy at the University of Gothenburg, Mölndal, Sweden
- 41UCL Institute of Neurology, London, UK
Biobanks are important resources for biomarker discovery and assay development. Biomarkers for Alzheimer’s and Parkinson’s disease (BIOMARKAPD) is a European multicenter study, funded by the EU Joint Programme-Neurodegenerative Disease Research, which aims to improve the clinical use of body fluid markers for the diagnosis and prognosis of Alzheimer’s disease (AD) and Parkinson’s disease (PD). The objective was to standardize the assessment of existing assays and to validate novel fluid biomarkers for AD and PD. To support the validation of novel biomarkers and assays, a central and a virtual biobank for body fluids and associated data from subjects with neurodegenerative diseases have been established. In the central biobank, cerebrospinal fluid (CSF) and blood samples were collected according to the BIOMARKAPD standardized pre-analytical procedures and stored at Integrated BioBank of Luxembourg. The virtual biobank provides an overview of available CSF, plasma, serum, and DNA samples at each site. Currently, at the central biobank of BIOMARKAPD samples are available from over 400 subjects with normal cognition, mild cognitive impairment (MCI), AD, frontotemporal dementia (FTD), vascular dementia, multiple system atrophy, progressive supranuclear palsy, PD, PD with dementia, and dementia with Lewy bodies. The virtual biobank contains information on over 8,600 subjects with varying diagnoses from 21 local biobanks. A website has been launched to enable sample requests from the central biobank and virtual biobank.
Introduction
There is an urgent need for biomarkers facilitating diagnosis of Alzheimer’s disease (AD) and Parkinson’s disease (PD) at an early stage in the disease course before the onset of clinical symptoms and to predict disease progression. For AD, the 42 amino acid form of β-amyloid (Aβ42) reflecting Aβ deposition in plaques, total tau (T-tau) reflecting the intensity of neuroaxonal degeneration, and phosphorylated tau (P-tau) reflecting the amount of brain tangle pathology are promising cerebrospinal fluid (CSF) biomarkers for early detection (1), but they do not cover all the neurodegenerative processes involved. For PD and dementia with Lewy bodies (DLB), no diagnostic or prognostic CSF or blood biomarkers exist, except for α-synuclein in CSF (2). The use of Aβ42, tau proteins, and α-synuclein for the diagnosis and prognosis of AD and PD is challenged by the high intra- and inter-center variability in biomarker concentration measurements (3–5). The variability in measurements is likely caused by differences in pre-analytical and analytical protocols for sample collection, sample handling, and local assay handling (3, 6–10), as well as by inconsistencies in kit production with batch-to-batch and even within-plate variation (11, 12).
Biomarkers for Alzheimer’s and Parkinson’s Disease (BIOMARKAPD) was a European multicenter study, funded by EU Joint Programme-Neurodegenerative Disease Research (JPND), designed to standardize the assessment of existing assays and to validate novel fluid biomarkers for AD and PD. To support these objectives, BIOMARKAPD has established a central biobank and a virtual biobank for neurodegenerative diseases. Samples for the central biobank have been collected and handled according to standardized operating procedures (13). The virtual biobank provides an overview of the local sample stock at each site. In this article, we will give an overview of clinical data, availability of samples, and the methods for sample collection and processing. Finally, we will explain the procedures for requesting samples.
Materials and Methods
Central Biobank
Study Population
Inclusion criteria for subjects in the central biobank of BIOMARKAPD were a diagnosis of normal cognition, mild cognitive impairment (MCI), AD, PD, dementia with Lewy bodies (DLB), frontotemporal dementia (FTD), vascular dementia (VaD), progressive supranuclear palsy (PSP), multiple system atrophy (MSA), or another type of dementia. Subjects were required to be at least 55 years old (in the MCI group) or at least 40 years old (in all other diagnostic groups). Subjects with normal cognition were clinically evaluated and were required to score above the 10th percentile on the age and education corrected mini-mental state examination (MMSE) (14). MCI was defined as referral to a memory clinic because of cognitive complaints in the absence of dementia. MCI subtypes could be defined post hoc based on neuropsychological test performance or CDR score. Subjects with PD were clinically diagnosed according to the UKPDBB criteria (15) or Gelb criteria (16). Subjects with dementia had a minimum score of 18 on the MMSE and were clinically diagnosed according to the NINCDS-ADRDA criteria for probable or possible AD (17), Neary criteria for FTD (18), NINDS-AIREN criteria for VaD (19), and McKeith criteria for DLB (20). Exclusion criteria for all subjects were contra-indications for lumbar puncture and other obvious causes of cognitive impairment such as strokes, severe depression, or endocrine disorders.
Clinical Data
The central biobank collected information on age, gender, education, clinical history [e.g., diagnosis, medication use, a selection of co-morbid disorders (cardiovascular, cerebrovascular, neurological, endocrine, somatic, and psychiatric disorders)], smoking habits and alcohol intake, physical examination [i.e., blood pressure, height, weight, and body mass index (BMI)], general cognition (CDR and MMSE), neuropsychological test performance for the domains of memory, fluency, visuospatial construction, attention, and executive functioning (expressed as raw scores and as z-scores according to local norms corrected for age, gender, and education), procedures for sample collection and processing, and the availability of imaging data (e.g., MRI, PET). Clinical data were collected within a timeframe of 6 months around blood/CSF collection.
Standardized Operating Procedures
Samples for the central biobank were collected according to defined biobanking pre-analytical standard operating procedures (SOPs) of the BIOMARKAPD project. For CSF collection, processing, and storage, we adhered to the BIOMARKAPD SOP published by del Campo et al. (13). For plasma and serum samples, we adhered to the biobanking guidelines published by Teunissen et al. (21). In addition, we recommended a 60 min minimum clotting time for blood for serum samples in accordance with the instructions of the tube manufacturer. For blood for DNA samples, we recommended storage at maximal −20°C consistent with the guidelines by Teunissen et al. (22). Centers were asked to report deviations from the SOP.
Sample Collection, Processing, and Storage
Tubes for sample collection and storage were distributed by Integrated BioBank of Luxembourg (IBBL). Blood samples were collected in the following polypropylene tubes: 10 mL EDTA [Becton, Dickinson and Company (BD), ref. 367525] for plasma, 4 mL EDTA (BD, ref. 368861) for whole blood, and 10 mL clot activator tubes (CAT) (BD, ref. 367896) for serum. CSF was collected in 10 mL polypropylene tubes (Sarstedt, ref. 62.610.018). Blood samples for DNA were not centrifuged and stored at maximal −20°C. All other samples were centrifuged at room temperature at 2,000 × g (min 1,800 × g, max 2,200 × g) and stored at −80°C. A maximum of 2 h was allowed between collection and freezing. A more detailed description of the SOP used for the collection of samples for the central biobank can be found elsewhere (13). For every subject 2 mL CSF, 2 mL serum, and 2 mL plasma were stored in 0.5 aliquots (in 0.5 mL Matrix 2D Thermo tubes) and 4 mL blood was stored for DNA isolation. Primary specimens and samples derivatives were coded with a three-letter center code and a subject number. Samples were at first stored locally, and then shipped on dry ice to IBBL for long-term storage. DNA extraction was performed at the IBBL. Samples and associated data were processed and stored at IBBL in compliance with ISO 9001:2008, NF S96-900: 2011, and ISO 17025:2005 standards and the ISBER Best Practices.
Virtual Biobank
The virtual biobank provides an estimation of the number of samples, and clinical (i.e., age, gender, education, CDR scores, MMSE scores, Parkinson scales, neuropsychological test results, information on medication use, and co-morbid disorders) and other biomarker data (i.e., MRI data, amyloid PET, dopamine SPECT) available at each center of subjects with normal cognition, MCI, AD, PD, PD with dementia, DLB, FTD, VaD, PSP, MSA, and other types of dementia. Retrospectively collected samples had been collected according to the center’s own SOPs. Centers that changed to the standardized BIOMARKAPD SOP during the project reported the transition date. All samples remained stored on site.
Ethics
Centers received approval from their local Ethical Committee and all subjects provided informed consent. All human research was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Central Biobank
Sample collection for the central biobank was performed in the period October 2013–December 2015. A total of 14 European centers have contributed samples and data to the central biobank. Currently, the central biobank database contains clinical information on 419 subjects, of which 49 had normal cognition, 117 MCI, 164 AD, 24 FTD, 3 VaD, 11 DLB, 25 PD, 5 PD with dementia, 3 PSP, 1 MSA, and 18 other types of dementia (i.e., either unknown or mixed pathology). From almost all subjects CSF samples (n = 410), plasma samples (n = 413 subjects), serum samples (n = 414), and DNA samples (n = 414) are available at the central biobank. At the local sites, MRI imaging data are available from 299 subjects, SPECT from 6 subjects, amyloid PET from 14 subjects, and FDG-PET from 28 subjects. Table 1 lists demographic information, neuropsychological tests results, and available imaging data according to diagnostic group. At least 1 neuropsychological test result was available from 307 subjects. The deviations reported from the SOP are shown in Table 2. The most common deviation (82%) was the use of a different needle than the 25G atraumatic needle. For most lumbar punctures, this needle was unavailable (n = 239), it was impossible to collect CSF with this needle (n = 19) or the neurologist preferred a traumatic needle (n = 79). None of the samples had more than the maximum of two freeze and thaw cycles, while 12% of the CSF samples, 1% of the plasma samples, and 13% of the serum samples underwent one freeze and thaw cycle. If the deviation related to needle use and number of freeze and thaw cycles was not taken into account, adherence to the BIOMARKAPD SOP was 91% for CSF collection and centrifugation, 96% for plasma collection and centrifugation, 93% for serum collection and centrifugation, and 100% for DNA collection and processing.
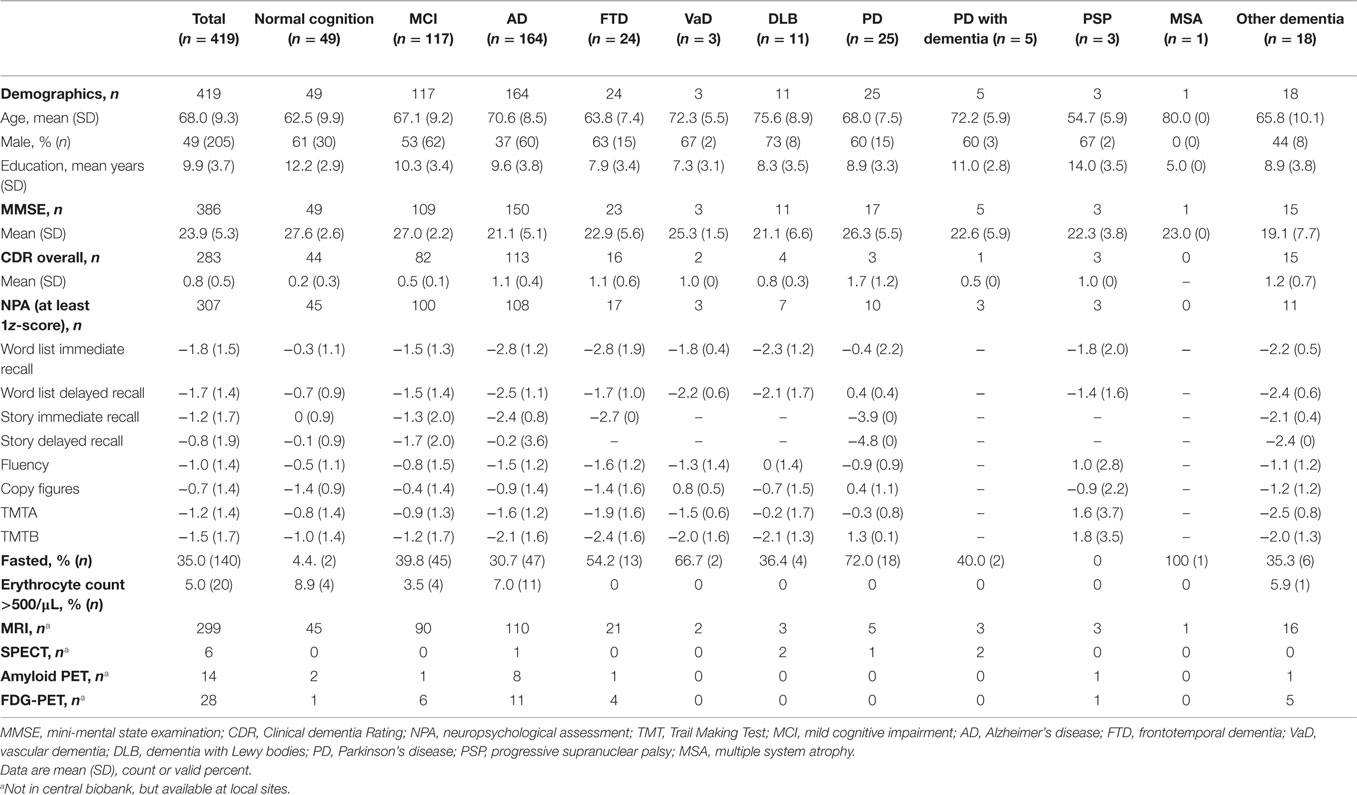
Table 1. Central biobank subject characteristics, z-scores on neuropsychological tests, and biomarker data available according to diagnostic group.
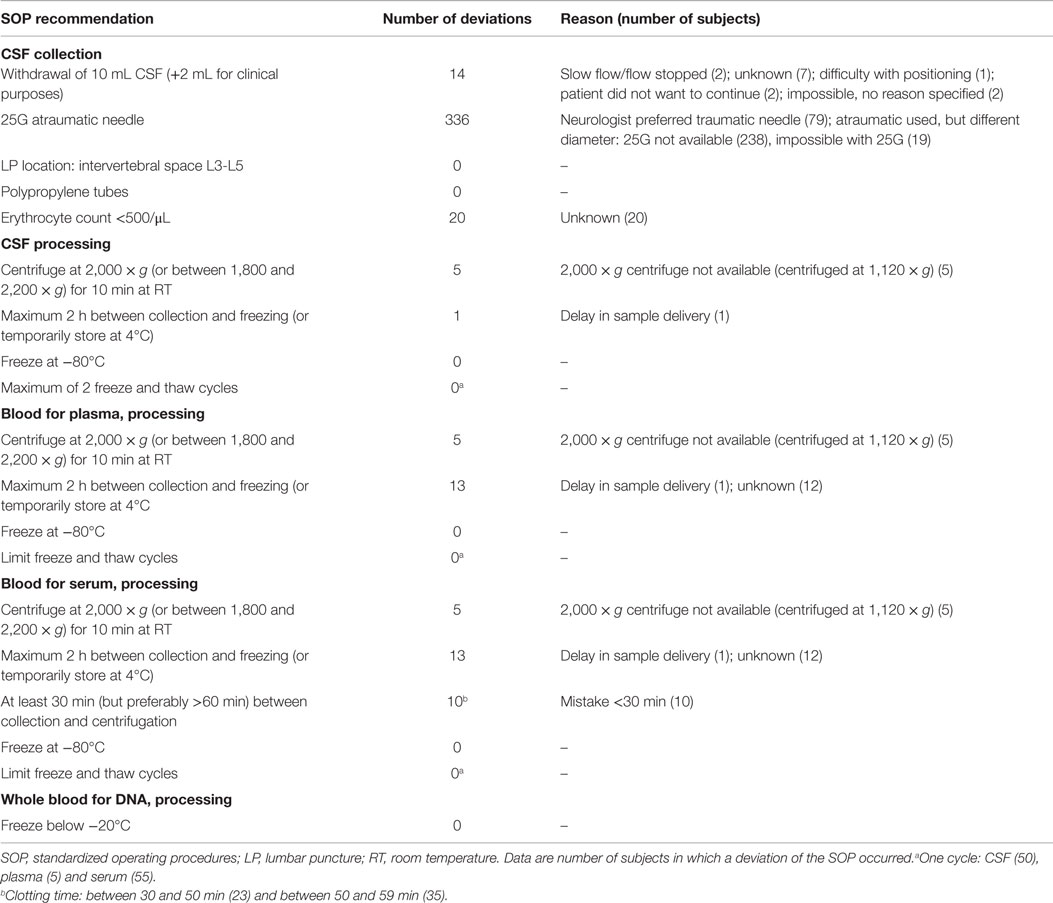
Table 2. Deviations from the SOP reported for samples in the central biobank.
Virtual Biobank
Currently, 21 centers have contributed data to the virtual biobank of BIOMARKAPD. The virtual biobank contains information on CSF samples from 7,550 subjects, EDTA plasma samples from 8,676 subjects, and serum samples from 8,141 subjects. So far, 11 centers have reported that they followed, or changed to, the BIOMARKAPD SOP for sample collection and processing. Table 3 lists the number of subjects per diagnostic group with CSF, EDTA plasma, and serum samples available.
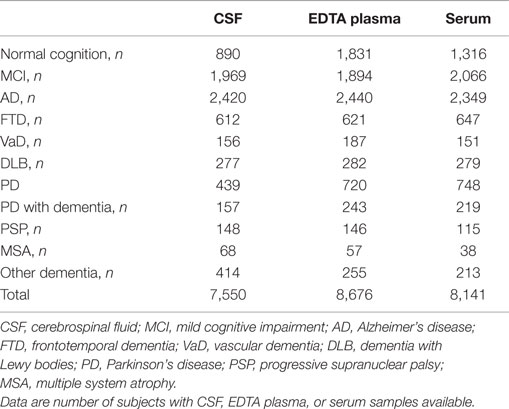
Table 3. Number of subjects in virtual biobank with CSF, EDTA plasma, and serum samples available according to diagnostic group.
Discussion
As part of BIOMARKAPD, a large central and virtual biobank with body fluids were established from over 9,000 subjects with neurodegenerative disorders. The central biobank contains samples from more than 400 subjects of which nearly 40% have AD. Adherence to the BIOMARKAPD SOP was high (>91%) for the collection and processing of CSF, plasma, and serum and blood samples. The virtual biobank contains CSF samples from over 7,500 subjects, plasma samples from over 8,600 subjects, and serum samples from over 8,100 subjects. Samples for the virtual biobank have been collected according to varying local SOPs. However, so far more than half of the centers have reported adopting the BIOMARKAPD SOP in the course of the project.
Requesting Samples from the Central or Virtual Biobank
Researchers in the field of neurodegenerative disorders interested in requesting samples from the central biobank or from the virtual biobank of BIOMARKAPD are invited to consult the following website: http://jpnd.arone.com/. Requests should meet the objectives of BIOMARKAPD project, i.e., to standardize the assessment of existing assays and to validate novel fluid biomarkers for AD and PD. Sample requests will be evaluated by the Analysis Advisory Board (AAB). Approval from the AAB will depend on scientific quality, whether the sample request meets the objectives of BIOMARKAPD, and sample availability. Furthermore, the sample request must meet the following three criteria. First, the researcher must demonstrate that the analysis complies with local medical ethical standards, for example, by showing regulatory approval of a medical ethical committee (MEC), institutional review board (IRB), or equivalent. Second, technical characteristics of assays such as linearity, recovery, specificity, imprecision, sensitivity, and lot-to-lot variability have already been established and of sufficient performance. Third, prior to the request, the diagnostic or prognostic value of the assay should have been already demonstrated in at least 20 controls and 20 diseased subjects. For the central biobank, fees will apply to cover the costs for sample and data collection, processing, and sample storage. Before shipment a material transfer agreement (MTA) needs to be signed.
For the virtual biobank, individual centers can decide on a case-to-case basis whether or not they would like to provide samples and which conditions will apply. When requesting samples from the virtual biobank, contact details will be provided of centers that are interested in meeting the sample request. Centers may use the MTA from the central biobank for the shipment of samples. Detailed information on the methodology of sample preparation and handling, and available clinical information should be requested directly from the center.
Conclusion
The central and virtual biobanks of BIOMARKAPD provide access to a large repository of CSF and blood samples for researchers in the field of neurodegenerative disorders, enabling progress in the clinical use of biomarkers for the diagnosis and prognosis of neurodegenerative disorders.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work is part of the BIOMARKAPD project within the EU Joint Programme for Neurodegenerative Diseases Research (JPND). This project is supported through the following funding organizations under the aegis of JPND – www.jpnd.eu
Funding organizations.
| Country | Funding organization |
| Belgium | IWT |
| Canada | Fonds de la Recherche en Santé du Québec FRSQ |
| Denmark | Danish Strategic Research Council |
| Finland | The Academy of Finland AoF |
| France | French National Research Agency |
| Germany | German Bundesministerium für Bildung und Forschung (BMBF); LF received funding by BMBF/DLR (01ED1203J), PL received funding by BMBF (01ED1203D) |
| Greece | Ministry of Education, Life Long Learning and Religious Affairs, General Secretariat for Research and Technology |
| Ireland | Health Research Board |
| Italy | Ministero della Salute |
| Luxembourg | Fonds National de la Recherche, Luxembourg |
| The Netherlands | ZonMW- The Netherlands Organisation for Health Research and Development grant number 629000002 |
| Norway | The Research Council of Norway |
| Poland | National Centre for Research and Development |
| Portugal | Fundação para a Ciência e a Tecnologia (FCT) |
| Slovakia | Ministry of Education, Science, Research and Sports of the Slovak Republic |
| Slovenia | Javna agencija za raziskovalno dejavnost Republike Slovenije |
| Spain | Instituto de Salud Carlos III (ISCII) |
| Sweden | Swedish Research Council (SRC) |
| Switzerland | Swiss National Science Foundation (SNSF) |
| Turkey | Türkiye Bilimsel ve Teknolojik Aras˛tırma Kurumu |
| United Kingdom | Medical Research Council |
We thank EU JPND and all national funding organizations involved for the BIOMARKAPD funding, and we thank IBBL for their various contributions in kind to the project, in particular for the provision of the IT infrastructure for the central and virtual biobanks, and for continuing storage of samples after the project.
Supplementary Material
The Supplementary Material for this article can be found online at http://journal.frontiersin.org/article/10.3389/fneur.2015.00216
References
1. Blennow K, Hampel H, Weiner M, Zetterberg H. Cerebrospinal fluid and plasma biomarkers in Alzheimer disease. Nat Rev Neurol (2010) 6(3):131–44. doi: 10.1038/nrneurol.2010.4
2. Mollenhauer B, Locascio JJ, Schulz-Schaeffer W, Sixel-Doring F, Trenkwalder C, Schlossmacher MG. alpha-Synuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: a cohort study. Lancet Neurol (2011) 10(3):230–40. doi:10.1016/S1474-4422(11)70014-X
3. Mattsson N, Andreasson U, Persson S, Arai H, Batish SD, Bernardini S, et al. The Alzheimer’s association external quality control program for cerebrospinal fluid biomarkers. Alzheimers Dement (2011) 7(4):386–395e386. doi:10.1016/j.jalz.2011.05.2243
4. Mollenhauer B, El-Agnaf OM, Marcus K, Trenkwalder C, Schlossmacher MG. Quantification of alpha-synuclein in cerebrospinal fluid as a biomarker candidate: review of the literature and considerations for future studies. Biomark Med (2010) 4(5):683–99. doi:10.2217/bmm.10.90
5. Verwey NA, van der Flier WM, Blennow K, Clark C, Sokolow S, De Deyn PP, et al. A worldwide multicentre comparison of assays for cerebrospinal fluid biomarkers in Alzheimer’s disease. Ann Clin Biochem (2009) 46(Pt 3):235–40. doi:10.1258/acb.2009.008232
6. Bibl M, Esselmann H, Otto M, Lewczuk P, Cepek L, Ruther E, et al. Cerebrospinal fluid amyloid beta peptide patterns in Alzheimer’s disease patients and nondemented controls depend on sample pretreatment: indication of carrier-mediated epitope masking of amyloid beta peptides. Electrophoresis (2004) 25(17):2912–8. doi:10.1002/elps.200305992
7. Bjerke M, Portelius E, Minthon L, Wallin A, Anckarsater H, Anckarsater R, et al. Confounding factors influencing amyloid Beta concentration in cerebrospinal fluid. Int J Alzheimers Dis (2010) 2010:11. doi:10.4061/2010/986310
8. Lewczuk P, Beck G, Esselmann H, Bruckmoser R, Zimmermann R, Fiszer M, et al. Effect of sample collection tubes on cerebrospinal fluid concentrations of tau proteins and amyloid beta peptides. Clin Chem (2006) 52(2):332–4. doi:10.1373/clinchem.2005.058776
9. Schoonenboom NS, Mulder C, Vanderstichele H, Pijnenburg YA, Van Kamp GJ, Scheltens P, et al. Differences and similarities between two frequently used assays for amyloid beta 42 in cerebrospinal fluid. Clin Chem (2005) 51(6):1057–60. doi:10.1373/clinchem.2005.048629
10. Teunissen CE, Verwey NA, Kester MI, van Uffelen K, Blankenstein MA. Standardization of assay procedures for analysis of the CSF biomarkers amyloid beta((1-42)), Tau, and phosphorylated Tau in Alzheimer’s disease: report of an international workshop. Int J Alzheimers Dis (2010) 2010:6. doi:10.4061/2010/635053
11. Mattsson N, Zegers I, Andreasson U, Bjerke M, Blankenstein MA, Bowser R, et al. Reference measurement procedures for Alzheimer’s disease cerebrospinal fluid biomarkers: definitions and approaches with focus on amyloid beta42. Biomark Med (2012) 6(4):409–17. doi:10.2217/bmm.12.39
12. Vos SJ, Visser PJ, Verhey F, Aalten P, Knol D, Ramakers I, et al. Variability of CSF Alzheimer’s disease biomarkers: implications for clinical practice. PLoS One (2014) 9(6):e100784. doi:10.1371/journal.pone.0100784
13. del Campo M, Mollenhauer B, Bertolotto A, Engelborghs S, Hampel H, Simonsen AH, et al. Recommendations to standardize preanalytical confounding factors in Alzheimer’s and Parkinson’s disease cerebrospinal fluid biomarkers: an update. Biomark Med (2012) 6(4):419–30. doi:10.2217/bmm.12.46
14. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res (1975) 12(3):189–98. doi:10.1016/0022-3956(75)90026-6
15. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry (1992) 55(3):181–4. doi:10.1136/jnnp.55.3.181
16. Gelb DJ, Oliver E, Gilman S. Diagnostic criteria for Parkinson disease. Arch Neurol (1999) 56(1):33–9. doi:10.1001/archneur.56.1.33
17. McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s disease. Neurology (1984) 34(7):939–44. doi:10.1212/WNL.34.7.939
18. Neary D, Snowden JS, Northen B, Goulding P. Dementia of frontal lobe type. J Neurol Neurosurg Psychiatry (1988) 51(3):353–61. doi:10.1136/jnnp.51.3.353
19. Roman GC, Tatemichi TK, Erkinjuntti T, Cummings JL, Masdeu JC, Garcia JH, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology (1993) 43(2):250–60. doi:10.1212/WNL.43.10.2160
20. McKeith IG, Galasko D, Kosaka K, Perry EK, Dickson DW, Hansen LA, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology (1996) 47(5):1113–24. doi:10.1212/WNL.47.5.1113
21. Teunissen CE, Tumani H, Engelborghs S, Mollenhauer B. Biobanking of CSF: international standardization to optimize biomarker development. Clin Biochem (2014) 47(4–5):288–92. doi:10.1016/j.clinbiochem.2013.12.024
Keywords: biobank, cerebrospinal fluid, dementia, Alzheimer’s disease, Parkinson’s disease, neurodegenerative disorders, body fluids
Citation: Reijs BLR, Teunissen CE, Goncharenko N, Betsou F, Blennow K, Baldeiras I, Brosseron F, Cavedo E, Fladby T, Froelich L, Gabryelewicz T, Gurvit H, Kapaki E, Koson P, Kulic L, Lehmann S, Lewczuk P, Lleó A, Maetzler W, de Mendonça A, Miller A-M, Molinuevo JL, Mollenhauer B, Parnetti L, Rot U, Schneider A, Simonsen AH, Tagliavini F, Tsolaki M, Verbeek MM, Verhey FRJ, Zboch M, Winblad B, Scheltens P, Zetterberg H and Visser PJ (2015) The central biobank and virtual biobank of BIOMARKAPD: a resource for studies on neurodegenerative diseases. Front. Neurol. 6:216. doi: 10.3389/fneur.2015.00216
Received: 22 June 2015; Accepted: 22 September 2015;
Published: 15 October 2015
Edited by:
Ritchie Williamson, University of Bradford, UKReviewed by:
Roland Brandt, University of Osnabrück, GermanyJason Eriksen, University of Houston, USA
Copyright: © 2015 Reijs, Teunissen, Goncharenko, Betsou, Blennow, Baldeiras, Brosseron, Cavedo, Fladby, Froelich, Gabryelewicz, Gurvit, Kapaki, Koson, Kulic, Lehmann, Lewczuk, Lleó, Maetzler, de Mendonça, Miller, Molinuevo, Mollenhauer, Parnetti, Rot, Schneider, Simonsen, Tagliavini, Tsolaki, Verbeek, Verhey, Zboch, Winblad, Scheltens, Zetterberg and Visser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Babette L. R. Reijs, babette.reijs@maastrichtuniversity.nl;
Pieter Jelle Visser, pj.visser@maastrichtuniversity.nl