 Maria Freytsis1*
Maria Freytsis1* Iain Barclay2
Iain Barclay2 Swapna Krishnakumar Radha3
Swapna Krishnakumar Radha3 Adam Czajka4
Adam Czajka4 Geoffery H. Siwo3,5Ian Taylor2,3
Geoffery H. Siwo3,5Ian Taylor2,3 Sherri Bucher5,6*
Sherri Bucher5,6*- 1NeoInnovate Collaborative Consortium, New York, NY, United States
- 2School of Computer Science and Informatics, Cardiff University, Cardiff, United Kingdom
- 3Center for Research Computing, University of Notre Dame, Notre Dame, IN, Unitde States
- 4Department of Computer Science and Engineering, University of Notre Dame, Notre Dame, IN, United States
- 5Eck Institute for Global Health, University of Notre Dame, Notre Dame, IN, United States
- 6Indiana University School of Medicine, Department of Pediatrics, NeoInnovate Collaborative Consortium, Indianapolis, IN, United States
Birth registration is a critical element of newborn care. Increasing the coverage of birth registration is an essential part of the strategy to improve newborn survival globally, and is central to achieving greater health, social, and economic equity as defined under the United Nations Sustainable Development Goals. Parts of Eastern and Southern Africa have some of the lowest birth registration rates in the world. Mobile technologies have been used successfully with mothers and health workers in Africa to increase coverage of essential newborn care, including birth registration. However, mounting concerns about data ownership and data protection in the digital age are driving the search for scalable, user-centered, privacy protecting identity solutions. There is increasing interest in understanding if a self-sovereign identity (SSI) approach can help lower the barriers to birth registration by empowering families with a smartphone based process while providing high levels of data privacy and security in populations where birth registration rates are low. The process of birth registration and the barriers experienced by stakeholders are highly contextual. There is currently a gap in the literature with regard to modeling birth registration using SSI technology. This paper describes the development of a smartphone-based prototype system that allows interaction between families and health workers to carry out the initial steps of birth registration and linkage of mothers-baby pairs in an urban Kenyan setting using verifiable credentials, decentralized identifiers, and the emerging standards for their implementation in identity systems. The goal of the project was to develop a high fidelity prototype that could be used to obtain end-user feedback related to the feasibility and acceptability of an SSI approach in a particular Kenyan healthcare context. This paper will focus on how this technology was adapted for the specific context and implications for future research.
1 Introduction
The Sustainable Development Goals agenda (UN General Assembly, 2015), launched by the United Nations in 2015, spurred renewed focus on the high rates of neonatal mortality and low rates of birth registration in low and middle-income countries (LMICs). Neonatal mortality is a key indicator of the overall well-being of a society, and birth registration is central to ensuring not only newborn health, but continued well-being and access to essential rights and services throughout the lifespan (Solberg, 2015). Low rates of birth registration, the lack of a reliable system for vital statistics reporting and tracking of mother-baby pairs contribute to the problem of excess neonatal mortality by preventing health care systems from effectively delivering crucial evidence-based interventions (Hereward et al., 2019).
An estimated 2.5 million babies globally die during their first month of life, known as the neonatal period, and approximately 47% of all the deaths of children under 5 years old occurred in the neonatal period (Hug et al., 2019). Birth registration is almost universal in most high income countries where the vast majority of births take place in facilities. But in LMICs, where many births take place in the home, about 1 in 4 children under age five are not registered. Of the children who are registered, an estimated 237 million children under age five globally do not have proof of registration in the form of a birth certificate (Selim, 2019). Some of the highest rates of neonatal mortality and lowest rates of birth registration can be found in parts of Sub-Saharan Africa. SDG targets 16.9 and 17.9 set forth the goals of providing legal identity for all, including birth registration, by 2030, and supporting countries to establish robust civil registration systems (Hereward et al., 2019). The agenda calls for development of innovative technologies to help reach these targets, however, experts are calling for caution that new technologies do not increase the potential for human rights abuses or further disenfranchize marginalized populations. A lack of adequate data governance infrastructure across nations threatens the ability of identity technologies to protect the personal identifying data of both children and guardians (Privacy International, 2018; World Bank, 2018; Hug et al., 2019; Schoemaker et al., 2019).
Continued growth in mobile device and telecommunication service penetration, as well as a decreasing gender gap in digital literacy and device ownership in Sub-Saharan Africa has led to a proliferation of mobile-phone based programs targeting maternal and newborn health (GSM Association, 2013; Sahay et al., 2013; Kurth et al., 2015; Sondaal et al., 2016; Rowntree and Shanahan, 2020). In 2019 Kenya reported 51% penetration of unique mobile subscribers which was up from 29.9% in 2009. The penetration of mobile internet use in 2019 was 25.8% (GSM Association, 2020). For the last 10 years, the NeoInnovate Collaborative Consortium (NCC), a multidisciplinary group of academic collaborators from multiple universities, has been developing and studying technologies to reduce preventable newborn mortality in Sub-Saharan Africa, with a particular focus on Kenya. Employing a user-centered design approach with end-users in the Moi Teaching and Referral Hospital system, the NCC built and deployed its foundational technology called mobile Helping Babies Survive (mHBS). mHBS is a suite of mobile phone-based applications for training, clinical decision support, and data collection, developed to support health workers in the scale-up of Helping Babies Survive programs. The applications were built on the open source DHIS2 platform, which is also the national health data reporting system in Kenya (Manya et al., 2012). mHBS was developed for Android smart phones using an iterative process with multiple rounds of user testing (Bucher et al., 2020). Integration of birth registration and mother/baby linkage with mHBS/DHIS2 has been an area of interest to the collaborative as it could allow for tracking of mother/baby pairs to provide invaluable data on essential newborn care delivered and newborn health outcomes (Aluvaala and English, 2020).
In 2018, the Kenyan Ministry of ICT solicited stakeholder presentations addressing opportunities for use of blockchain technology in Kenya1. In response to this solicitation, NCC developed a vision for a birth registration and newborn health technology incorporating blockchain and self-sovereign identity (SSI) principles, as a proof of concept project called NeoLinkID. SSI describes the ability of an individual to have ownership of their personal data and to control who has access to that data, without the need for centralized infrastructure, or any control or authorization by any third party (Allen, 2016). Acknowledging that blockchain-based technologies were gaining increasing attention in a landscape of poor global data governance infrastructure, the project was envisioned as an opportunity to understand how the SSI approach can offer additional data protection from within the context of the centralized birth registration process in Kenya and the challenges involved in integrating the SSI layer into the existing system.
A partnership with the Evernym ID for Good accelerator2, and support of Google Summer of Code3, enabled NCC to rapidly develop a prototype that will allow end-user feedback on the feasibility and acceptability of this technology approach with both health workers and families in a facility-based birth registration use case in Kenya. While the majority of unregistered Kenyan births take place in the community, the technology platform’s heavy reliance on connected environments made it clear that development for community settings would not be possible at the outset. However, developing this technology would allow for study of other possible benefits of this approach, such as facilitating privacy preserving digital linkage with the national birth certificate acquisition process, contribution of aggregate newborn health data to vital statistics and public health via DHIS2 integration, and linkage of mother-baby pairs for health tracking via a mobile personal health record for newborns held by guardians. A different research team within NCC is currently working to develop a solution to work in environments with limited internet connectivity.
2 Kenyan Context: Birth Registration and Digital Innovation
Currently, the neonatal mortality rate (NMR) in Kenya is 21/1,000 (UNICEF4); the SDG NMR target, by 2030, is 12/1,000. Despite significant changes in the health system over the past few years, including devolution to the County level (Barker et al., 2014), and elimination of user fees for facility-based births, rates of maternal and perinatal mortality have remained stagnant (Kunkel et al., 2019; Gitobu et al., 2018). The current birth registration rate in Kenya is 67%, with rural areas having 61% coverage, and urban areas at 79%5. However, rates as low as 20% and as high as 90% have been documented across regions (Gelb et al., 2016). In one study published in 2014 about half of the participating Kenyan children had birth certificates, with participants in urban areas more likely to have birth certificates than in rural locations (Apland et al., 2014).
In Kenya, as in many other LMICs, birth registration is a process by which “informants” who include health workers in facilities (primarily midwives), and assistant village chiefs/elders in the communities, acting on behalf of the Civil Registration Department (CRD), interact with “guardians” (primarily mothers and fathers) in order to provide documentation of birth for both the guardians and for the health and civil registration systems (Figure 1). Informants verify the parents’ identities via legal identity documents and document birth details and other background information as required by Form B16. Informants are legally authorized and obligated to do this in relation to their role as health care providers and assistant village chiefs/elders. The issuance of a birth notification document, which is the top portion of Form B1, by the informant to the guardian is the first step in birth registration. The remaining part of the form is sent to the local office of the CRD which allows for the birth to be counted in vital statistics. When parents take the next step of applying for the birth certificate at the local CRD office, they are required to present the birth notification document, which will be matched with the lower portion of the form submitted by the informant (Apland et al., 2014; MEASURE Evaluation, 2014).
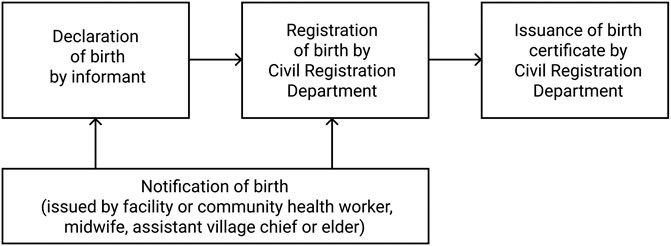
FIGURE 1. Kenyan birth registration process.
Without a birth certificate, Kenyan parents may not be able to access services, ranging from health insurance to education, which would ensure a thriving childhood. The birth certificate is helpful but not required to obtain the current form of national ID (Apland et al., 2014). However, lacking a birth certificate can be a profound threat to children during periods of conflict or forced migration, and a life-long barrier to accessing essential services such as voting, obtaining a passport, opening a bank account, and mobile phone ownership which enables access to a growing range of essential digital services (Apland et al., 2014; Selim, 2019).
The barriers to birth registration are complex. Although there are common themes across countries and geographic areas, these barriers are also highly contextual. Over the last 20 years there have been multiple initiatives aimed at strengthening the Kenyan civil registration system including research and targeted interventions aimed at specifically understanding and ameliorating the barriers to birth registration. (Apland et al., 2014; MEASURE Evaluation, 2014; Gelb et al., 2016). Barriers fall into several categories including:
1. Lack of awareness regarding the importance of birth registration and obtaining a birth certificate.
2. Physical and situational difficulties contribute to the inability to complete the multi-step process. This may include traveling long distances to the registration authority and fear of penalties for late registration, which in Kenya can include not only monetary fees but prison time. Additionally, language barriers or illiteracy, or parents not having the personal identity documents required for registration, such as in the case of refugees or stateless groups, can also be contributing factors. There are also cultural beliefs within some groups that are not aligned with registering newborn births.
3. Discriminatory laws and practices which prohibit certain groups of people from accessing birth registration based on race, ethnicity, religion, gender, or other characteristics. This can include officials requiring bribes to process applications.
4. Inadequate staff and infrastructure to perform birth registration efficiently, as well as negative attitudes of some registration workers (Apland et al., 2014; Gelb et al., 2016; UNHCR, 2017; Kenya Human Rights Commission, 2019).
Research in Kenya has also found a lack of motivation by parents to register their children in advance of any particular need and local officials not placing a high priority on incentivizing registration (Gelb et al., 2016). A 2014 study found Kenyan parents reported high awareness and low practical barriers and concluded that parents are making a deliberate informed choice not to pursue birth registration, weighing the cost and benefit. Suggestions of the researchers included increasing the use of information and communication technology to impact parental decision-making (Pelowski et al., 2015). Other interventions have focused on mass education campaigns, targeted education and incentivization of community based birth registration including linking opportunity for registration with other essential services such as immunization and school enrollment, and introduction of mobile technology to support the birth registration process (World Health Organization, 2013; Apland et al., 2014).
Kenya has an extremely active, innovative, and engaged digital health landscape representing an enabling environment for new technology. Known as the “silicon savannah” (Schoemaker et al., 2019), Kenya has led the world in regards to technological innovations related to mobile banking (e.g., mPESA7), crowdsourced, decentralized monitoring and reporting (Ushahidi), and development of vibrant innovation ecosystems (iHub8). Mobile phone-base health interventions have also proliferated over the last decade with many focusing on maternal and child health. However, evidence shows that many of these interventions have not been evaluated and few have scaled beyond pilot projects. Additionally, few projects had been implemented in marginalized areas with more health care needs (Njoroge et al., 2017).
The Kenyan context also presents myriad challenges for implementing identity technology including a high proportion of vulnerable and marginalized populations such as refugees and other groups of stateless persons, a fragmented identity ecosystem, increasing reliance on digital services with a private sector directly connected to the state, and a government with opaque operations, dense bureaucracy, and a history of corruption. At the same time, e-Government services are growing, and the entire health reporting system has been cloud-based since 2010. The current national debate about a new form of biometric national ID has brought issues of data protection to the forefront. The policy landscape related to data protection is evolving with significant advocacy efforts from community service organizations and numerous failed attempts at passing data protection legislation, culminating in the current Data Protection Act, introduced in 2019, making its way through the lawmaking process (India, 2013; Gelb et al., 2016; Kenya Human Rights Commission, 2019; Schoemaker et al., 2019).
3 Use Case: Technology Design and Development
3.1 Self-Sovereign Identity Background
SSI is built upon well established cryptography techniques (Preneel, 1994) where a securely held private key is used to sign documents, while a complimentary public key can be used to verify the signature and that the document has not been tampered with. Researchers have developed mechanisms (Sporny et al., 2019) for organisations and individuals to issue signed credentials to other parties, where each is identified by a unique decentralized identifier (DID). In this way, any party attesting something about another party can declare and sign their claim, using their DID and cryptographic protocols. The signed document is known as a Verifiable Credential (VC), and is held by the subject of the credential, or in the case of a child, by a guardian. At a later date, when the holder of a VC needs to enter into a transaction, a service provider can request proof of their status or entitlements. The holder of the credential can generate a Verifiable Presentation containing assertions from the VC document, to provide cryptographically verifiable proof of the claims being made. A level of privacy is provided by the principle of Selective Disclosure, which allows VC holders to provide presentations containing only selected elements of credentials, so that they retain control over the data shared in any individual transaction. These data models and protocols are implemented in software toolkits, which can be used by third party developers to add SSI capabilities to their solutions. The Sovrin network provides the foundation for many of the toolkits, including the Evernym platform adopted here, and uses the public-permissioned Hyperledger Indy blockchain ledger to keep a permanent and immutable record of the DIDs of public agencies, along with credential schemas. No personal information is written to the blockchain (Kondova and Erbguth, 2020).
3.2 Modeling Birth Registration Processes as an SSI System
Prototype design and development was preceded by a research phase including a literature review and interviews with Kenyan facility-based midwives to understand the current birth registration process. A set of personas representing the two groups of end users–guardians (parents, primarily mothers) and informants (facility-based health workers, primarily midwives), were developed. A high level use case description based on these personas was conceived and then evolved into user stories describing the workflows for the two applications. Assumptions regarding the selected context and users include consistent mobile device access with the possibility of shared devices, English language literacy, technology literacy with Android smartphones, reliable connectivity, and adequate mobile data. Interactions between informants and guardians were considered to take place at the facility where the birth occurred prior to the mother/baby dyad’s discharge home. The prototype represented the process of creating a digital “copy” of the birth registration process alongside the current paper-based process. Personas for the roles of informant and guardian in the community-based birth registration process were also developed to illustrate the challenges of extending this technology approach to those populations who may have lower language literacy, less proficiency with smartphones, unreliable connectivity, and less consistent device and data access.
Designing systems to use decentralized SSI protocols involves developing an understanding of the participants of the system in the real world, their differing goals, and the interactions and dependencies that they have on each other to fulfill those goals. In previous work (Barclay et al., 2020) the authors introduced an application of the iStar (Yu, 2011) conceptual modeling framework as a method of describing the actors and their interactions in an SSI system, in the context of the birth registration process. In order to meet their goal of “Get Birth Certificate”, a newborn’s guardian needs to receive a copy of the birth notification document (BND), which is issued to them by the informant. The prototype required that the informant issues the BND on provision of a suitable proof of the guardian’s identity. In a deployed system, this type of requirement would be a government policy decision, and the technology would be adapted to meet the needs.
3.3 Architecture
The NeoLinkID prototype adopts three participant roles–CRD, as the credential issuing authority (and represented by the research team in the prototype design); the informant, or health worker; and the guardian, as the recipient and holder of the credential. In interactions, the informant is considered to be a representative of the CRD, which manifests in the architecture as the informant requesting the CRD to issue credentials. Credentials developed for the prototype include a credential to record that the informant has checked the guardian’s identity, the BND and a linking credential which creates mother-baby linkage, as detailed in Table 1.

TABLE 1. Credentials developed for Prototype.
Issues related to the SSI concept of “guardianship”9 were not addressed in credential development, but rather, the Link Credential was built to provide a mechanism to study context for the development of a local guardianship framework. Verification of credentials was not addressed in the first iteration but the design process allowed for considerations of various verification scenarios.
In the prototype system, the informant is issued with a mobile web application which accesses a server operated for the CRD. The server integrates with the core SSI platform, which provides verifiable credential structures, and populates and issues credentials. The informant’s web application provides forms to collect information about guardians and newborns, and then requests the CRD server to sign and issue credentials to the guardian. An Android smartphone application was developed to receive and hold credentials for the guardian. No direct connection is established between the informant’s web application and the guardian’s application. The informant’s application provides data to the server to populate and request credentials to be sent to the guardian’s application. An informant will meet with many guardians during the course of the day. To issue credentials to the correct guardian, the informant application creates a connection between the server and the guardian they are currently meeting by presenting a QR code to be scanned by the guardian. When the appointment finishes the informant ends the session, and the connection is removed. The informant’s application displays forms that are populated with the guardian and used to generate and issue credentials. The server sends credentials directly to the guardian’s mobile application, where they are stored for later use. Figure 2 shows the handshaking and credential issuing process flows and the interactions between the three participants. Screenshots of the applications developed for the informant and the guardian are shown in Figure 3.
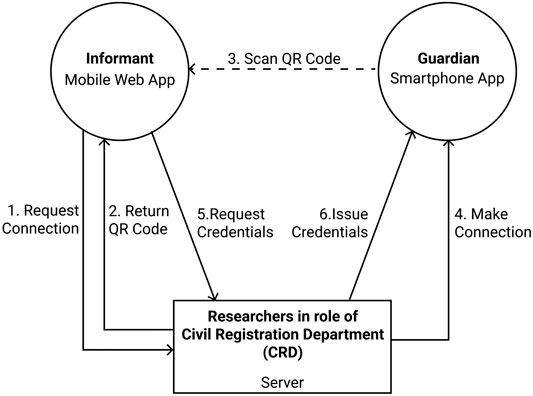
FIGURE 2. Interaction flows between the participants in the system.
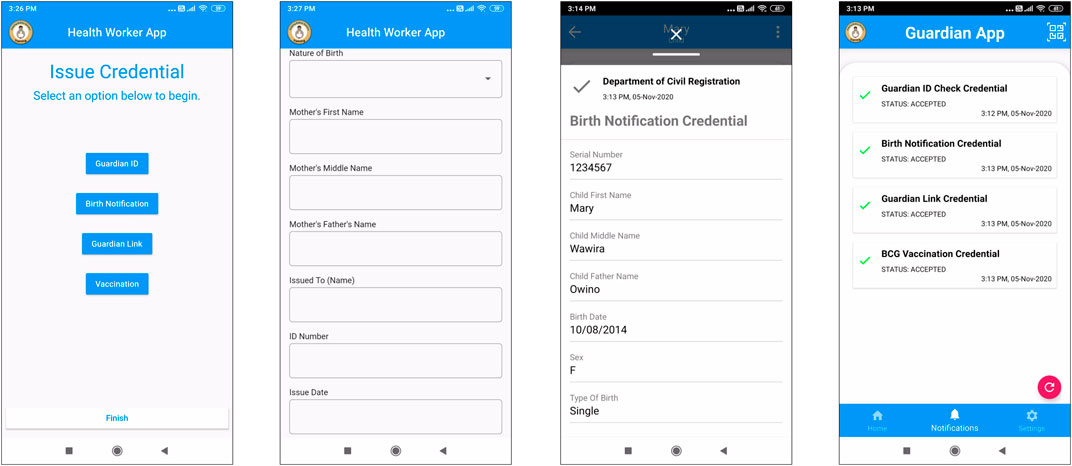
FIGURE 3. Mobile applications for informants and guardians.
4 Discussion
The goal of the project was to develop a prototype modeling the first steps of birth registration using SSI concepts that would allow the team to obtain user feedback from health workers and parents related to the feasibility and acceptability of an SSI-based technology approach for facility-based birth in Kenya.
Building on the Evernym SSI platform lowered the barrier to delivering an initial prototype capable of demonstrating a complete interaction between the issuer and holder of credentials. The project team also de-risked delivery, by adding a simulation mode to the prototype, which used representations of transitions between the applications to present pre-loaded credentials to the user of the guardian application. Ultimately, this has proven to be useful, as the COVID-19 pandemic resulted in an unexpected delay for the planned participatory design and user feedback activities in Kenya. The simulation mode in the applications will enable researchers to introduce the application and its operations to facility staff remotely, prior to any future facility-based user trials being conducted. The use of simulations for the SSI interactions was not considered prior to the project inception, but will be considered in future work, as this technique has been found to provide an efficient way of demonstrating concepts and interactions. The development process which has been utilized also allows for understanding of technology issues that, in turn, can guide future research, as described below.
4.1 SSI Within the Kenyan Healthcare Context
The prototype was developed as a standalone system, which enabled the team to focus on the SSI architecture and technology. Any practical future deployment will require integration into existing healthcare and civil registration technology systems for successful adoption, as shown in Figure 4, with a need for integration between the credentialing system and existing DHIS2 framework utilized by the Ministry of Health, as well as digital CRD systems. In this scenario, a mobile application would be used by informants to collect information about newborns from parents and guardians, which would be integrated into the centralized DHIS2 system. A digital copy of the BND would be issued to guardians, to maintain on their smartphone. The guardian would be able to use this digital copy of the BND when they needed to provide proof for any reason. A claimed benefit of holding the digital copy in a self-sovereign identity-based system would be that the guardian has control over access to their data, and can share it as needed. Selective disclosure means that the guardian would, theoretically, have control over which parts of the digital document were shared with third parties. The decentralized architecture of the SSI system implies that presented credentials, when used in a SSI ecosystem, could be verified without the CRD having knowledge of the circumstances. This proposed architecture, however, does not eliminate the need for central databases held by government agencies, which can pose risks to human rights given lack of data protection frameworks (Dixon, 2017); however, it may provide greater privacy at the point of transactions.
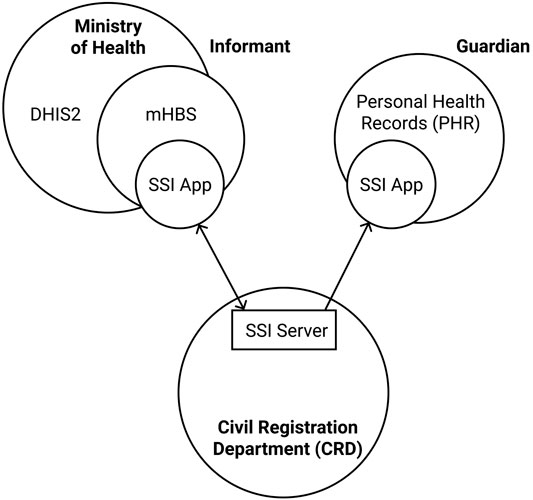
FIGURE 4. The prototype in context as part of a larger infrastructure.
The current prototype has two applications, one for the informant and one for the guardian, as shown in Figure 3. In a future deployment, the informant’s application would need to be integrated with the existing mHBS application suite, which is already in use and familiar to the health worker community. User studies undertaken with the prototype system will help to identify the most effective point of integration with the mHBS app, such that it could be most efficiently adopted into the health worker’s workflow.
The guardian’s application was developed for use by parents and other guardians, and uses the guardian’s own smartphone to receive and store credentials issued by the informant. This reduces the cost of deployment of the NeoLinkID prototype, but places a burden onto users to provide the necessary equipment, and to be comfortable installing the software onto their own devices. It is clear that this approach will not be applicable for those areas of Kenya that currently have lowest birth registration rates, however, it is possible that this approach could improve birth registration rates among smartphone owners who are a large and rapidly growing segment of the population (Rowntree and Shanahan, 2020). Typically in an SSI deployment this application is based upon the metaphor of a “wallet,” and uses concepts of credentials and proofs. The NeoLinkID use case presents an opportunity to provide an application more suited to its target audience, and to research language and metaphors that could be readily adopted by that community. The future vision for this application is a personal health record design modeled on the paper Mother and Child Health Booklet currently used in Kenya. The World Health Organization (WHO) recommends the use of home-based records, as a complement to facility-based records, for the care of pregnant women, mothers, newborns, and children (World Health Organization, 2018). Adopting an SSI-based solution as part of nascent personal health records systems10,11 has the potential to provide data security and privacy to parents and guardians, such that they are able to hold a cryptographically secured copy of their health data which can be used without involvement of a centralized authority.
4.2 Identity Verification and Authentication
In the NeoLinkID prototype, informants are required to check the identity of a guardian against existing identification, e.g., a photographic identity card. This identity source is referenced by its unique identifier in the “Identity Checked” credential, so that it can form a link between the credential and its holder, and can be used to provide proof that the credential is being legitimately presented. A credential is also issued to verify the birth of the newborn, based on the witness account of the informant. A further credential links the guardian and the newborn, and contains identifiers from both the guardian’s identity credential and the newborn’s credential, to form an inextricable connection between the two.
Authentication processes are needed to ensure that a verified identity is subsequently presented by the authorized person, i.e., that the presented identity matches the person. In a credential-based system, the verifying party needs to have assurance that credentials are being presented by the correct party. The prototype highlighted particular concerns about providing identity assurance where a phone is shared by multiple users. Any practical system would need to ensure that an application storing credentials is protected from unauthorized use with login protection, so it can only be accessed by the user of the phone that the “wallet” app belongs to, and provide assurance that the presenter of the credential is the authorized party.
For mother and baby pairs, authentication would be necessary to show that both the mother and the baby being presented match personal identifiers in their credentials. An architecture can be designed to include a biometric identifier within a credential, and used to authenticate the presenter of the credential (Hardman et al., 2019). This could be developed in a decentralized manner, without requiring a national or centralized biometric service, with the biometric template being used solely to verify the presenter of the credential. Formally, verification should be matched to identified assurance levels, as defined by national and/or international standards, though this may be complicated in some countries. The biometric mode must be carefully chosen with consideration for its specificity in newborns. The use of biometrics for newborns has not been widely studied and is a high priority research topic for this use case. The authors are exploring the possibility of applying iris recognition methods adapted to newborn eyes, due to demonstrated long-term stability of iris patterns. A slight drop in similarity between iris images as a function of time between enrollment and verification has been demonstrated by various research groups (Baker et al., 2009; Czajka, 2013). The impact of these observed time-related fluctuations on commercial iris recognition systems has been found, however, less important than other factors contributing to potential degradation of recognition reliability, as demonstrated by NIST in their IREX VI report (Grother et al., 2013). The research to fully understand iris aging is ongoing.
4.3 Interoperability and Open Source
Robust interoperability and open source development are critical elements of scalable health technology for LMICs12. It is an ongoing requirement for the SSI community at large which has led to development of open standards by W3C and non-profit organizations such as the Decentralized Identity Foundation and the Hyperledger Foundation, who are collectively bringing interoperability to the top of their agenda13. As well as open standards, open source implementations of these protocols are also becoming increasingly available14. Future NeoLinkID work will prioritize open standards, open source development, and interoperability of credentials as criteria for platform selection. Since mHBS and NeoLinkID are being incubated under the open source community of LibreHealth, there is an additional opportunity to leverage the expertize of the DHIS2 and OpenMRS developer communities to explore integration of SSI-based birth registration with both of these health IT platforms which have been adopted at the national level in Kenya.
5 Conclusion
The NeoLinkID project has successfully developed an SSI-based prototype modeling the first steps of birth registration based on the Kenyan process, using a personal health record approach to store information about newborns and their guardians. This development phase has provided some initial insights into the possibilities for improving data privacy, security, and portability, as well as the possible limitations of a decentralized approach to birth registration. The next phase of this work will be a feasibility, acceptability, and user design study, conducted virtually with Kenyan nurse-midwives. This paper represents an initial body of contextual knowledge for SSI-based birth registration in Kenya. SSI protocols continue to evolve and platforms and implementations are immature, presenting challenges for technology adoption outside of research and proof-of-concept deployments. Areas of high priority for research include authentication and verification, particularly integration of newborn biometrics, as well as integration with DHIS2 and the local framework for guardianship.
Increasing access to birth registration is a critical part of improving the survival and health of Kenyan newborns (Målqvist et al., 2008). Creating user-centered systems for birth registration that prioritize data protection and selective data sharing could mitigate some of the inherent risks and barriers of the birth registration process for segments of the Kenyan population. The experience of adapting SSI technology for this use case has illuminated multiple challenges that warrant further research for applying SSI to birth registration in Kenya and other LMIC settings. Effective solutions will require detailed understanding of the specific local context. Systems interoperability will be critical in order to derive benefits of this technology for increasing both birth registration rates and birth certificate acquisition, as well as the quality of data available for public health and vital statistics (Labrique et al., 2018; Wang and De Filippi, 2020). Research on SSI for birth registration should target the diverse local stakeholders whose collaboration will be essential for deployment success, including registration, justice, health, statistics, and civil society, as well as a broad representation of parent, family, and community stakeholders (AbouZahr et al., 2015). Investment in SSI-based birth registration solutions for LMICs should prioritize research to understand the unique needs and perspectives of all stakeholder groups, particularly those who are vulnerable to discrimination or exclusion based on their demographic, health, or political status.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
In-kind support for prototype development was provided by The Evernym ID for Good Accelerator. Funding for engineering was provided by Google Summer of Code to LibreHealth (May–August 2020). LibreHealth provided generous in-kind hosting for the GSoC efforts. GS was supported in part by an IBM Faculty Award.
Conflict of Interest
This work was made possible, in part, by in-kind support from the for-profit company, Evernym, whose tools and engineering support were used in the development of the prototype described in the article. IT is CTO and IB Research Director at SIMBA Chain, Inc., a blockchain technology company.
Acknowledgments
We are grateful to the team at LibreHealth for incubating this project on their open source community platform and to Prajwal Belagavi for his dedicated development work through the Google Summer of Code program. Robby O’Connor, provided highly engaged and expert guidance for our team’s successful participation as NeoLinkID GSoC mentors. Dan Barclay developed the mobile web application for informants. We are also grateful for the technical support provided by the Evernym team throughout the participation in the accelerator. This work would not be possible without the bi-directional partnership that we are privileged to share with collaborators at Moi University, Alupe University College, and Moi Teaching and Referral Hospital, in Kenya. We are also grateful to the Helping Babies Survive Master Trainer Corps in Kenya, which, over the years, has provided invaluable feedback for concepts and technologies developed by the NeoInnovate Collaborative Consortium, including NeoLinkID.
Footnotes
1https://ict.go.ke/taskforce-on-distributed-ledgers-and-artificial-intelligence-presentation-schedule
2https://www.evernym.com/identityforgood/
3https://summerofcode.withgoogle.com
4https://data.unicef.org/country/ken/
5https://data.worldbank.org/indicator/SP.REG.BRTH.ZS?end=2014&locations=KE&start=2003&view=chart
6http://forms.co.ke/forms/41_Birth_Acknowledgement-of-Birth-Notification-For-Parents_Form-B1.pdf
7https://techcrunch.com/2015/07/23/the-rise-of-silicon-savannah-and-africas-tech-movement/
8https://www.dw.com/en/finding-digital-solutions-to-local-problems-kenyas-innovation-scene-is-no-one-hit-wonder/a-47119339-0
9https://sovrin.org/library/guardianship-white-paper/
10https://news.vumc.org/2017/11/16/teams-mobile-app-helping-healthcare-workers-in-africa/
12https://id4d.worldbank.org/principles
13https://identity.foundation/interop/
14https://github.com/decentralized-identity
References
AbouZahr, C., De Savigny, D., Mikkelsen, L., Setel, P. W., Lozano, R., Nichols, E., et al. (2015). Civil registration and vital statistics: progress in the data revolution for counting and accountability. Lancet 386, 1373–1385. doi:10.1016/S0140-6736(15)60173-8
Allen, C. (2016). The path to self-sovereign identity. Available at: http://www.lifewithalacrity.com/2016/04/the-path-to-self-soverereign-identity.html (Accessed April 24, 2016).
Aluvaala, J., and English, M. (2020). Implementing change for facility-based peripartum care in low-income and middle-income countries. Lancet Global Health 8, e980–e981. doi:10.1016/S2214-109X(20)30306-5
Apland, K., Blitz, B. K., Calabia, D., Fielder, M., Hamilton, C., Indika, N., et al. (2014). Technical Report. Birth registration and children’s rights: a complex story. Available at: https://eprints.mdx.ac.uk/id/eprint/17346 (Accessed August 04, 2015).
Baker, S. E., Bowyer, K. W., and Flynn, P. J. (2009). “Empirical evidence for correct iris match score degradation with increased time-lapse between gallery and probe matches,” in International conference on biometrics, Alghero, Italy, June 2–5, 2009 (Berlin, Heidelberg: Springer), 1170–1179.
Barclay, I., Freytsis, M., Bucher, S., Radha, S., Preece, A., and Taylor, I. (2020). Towards a modelling framework for self-sovereign identity systems. Preprint repository name [Preprint]. Available at: arXiv:2009.04327 (Accessed September 9, 2020).
Barker, C., Mulaki, A., Mwai, D., and Dutta, A. (2014). Devolution of healthcare in Kenya assessing county health system readiness in Kenya: a review of selected health inputs. Facilities. 16, 18. doi:10.13140/RG.2.2.36622.87363
Bucher, S. L., Cardellichio, P., Muinga, N., Patterson, J. K., Thukral, A., Deorari, A. K., et al. (2020). Digital health innovations, tools, and resources to support helping babies survive programs. Pediatrics 146, S165–S182. doi:10.1542/peds.2020-016915I
Czajka, A. (2013). Template ageing in iris recognition. BioSignals 1, 70–78. doi:10.5220/0004245800700078
Dixon, P. (2017). A failure to “do no harm”–India’s aadhaar biometric id program and its inability to protect privacy in relation to measures in Europe and the us. Health Technol 7, 539–567. doi:10.1007/s12553-017-0202-6
Gelb, A. H., Anandan, V., and Cannata, A. (2016). “Identification for development (ID4D) country diagnostic: Kenya,” in Technical report. Washington, DC: The World Bank, 1–82.
Gitobu, C., Gichangi, P., and Mwanda, W. (2018). The effect of Kenya’s free maternal health care policy on the utilization of health facility delivery services and maternal and neonatal mortality in public health facilities. BMC Pregnancy Childbirth 18, 77. doi:10.1186/s12884-018-1708-2
Grother, P. J., Matey, J. R., Tabassi, E., Quinn, G. W., and Chumakov, M. (2013). Tech. rep. IREX VI-Temporal stability of iris recognition accuracy. Available at: https://nvlpubs.nist.gov/nistpubs/ir/2013/NIST.IR.7948.pdf (Accessed July 11, 2013).
GSM Association (2013). Mobile birth registration in sub-saharan africa a case study of orange Senegal and Uganda telecom solutions. Available at: https://www.gsma.com/identity/resources/mobile-birth-registration-in-sub-saharan-africa-a-case-study-of-orange-senegal-and-uganda-telecom-solutions (Accessed July 2, 2013).
GSM Association (2020). Mobile taxation in Kenya: accelerating digital development. Available at: https://www.gsma.com/publicpolicy/resources/mobile-taxation-in-kenya-accelerating-digital-development (Accessed March 23, 2020).
Hardman, D., Harchandani, L., Othman, A., and Callahan, J. (2019). Using biometrics to fight credential fraud. IEEE Commun. Stand. Mag. 3, 39–45. doi:10.1109/mcomstd.001.1900033
Hereward, M., Williams, C., Petrowski, N., and Cappa, C. (2019). Universal birth registration by 2030: progress and challenges. Lancet 394, 2211–2212. doi:10.1016/s0140-6736(19)33101-0
Hug, L., Alexander, M., You, D., Alkema, L., and For Child, U. I.-A. G. (2019). National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Global Health 7, e710–e720. doi:10.1016/S2214-109X(19)30163-9
India, H. (2013). Technical Report. Systematic review of eCRVS and mCRVS interventions in low and middle income countries. Available at: https://www.who.int/publications/i/item/systematic-review-of-ecrvs-and-mcrvsinterventions-in-low-and-middle-income-countries (Accessed October 19, 2013).
Kenya Human Rights Commission (2019). Report of the digital identification document (id) and citizenship consultative meeting. Available at: https://www.khrc.or.ke/mobile-publications/equality-and-anti-discrimination/198-report-of-digital-identification-citizenship-workshop-naivasha/file.html (Accessed January 18, 2019).
Kondova, G., and Erbguth, J. (2020). “Self-sovereign identity on public blockchains and the gdpr,” in Proceedings of the 35th annual ACM symposium on applied computing, Brno, Czech Republic, March–April 30–3, 2020 (New York, USA: SAC) 342–345.
Kunkel, M., Marete, I., Cheng, E. R., Bucher, S., Liechty, E., Esamai, F., et al. (2019). “Place of delivery and perinatal mortality in Kenya,” in Seminars in perinatology. Editor E. D. Mary (New York, NY: Elsevier), 43, 252–259.
Kurth, A., Inwani, I., Agot, K., Macharia, P., and Buttolph, J. (2015). mHEALTH compendium volume 5. Available at: http://www.africanstrategies4health.org/uploads/1/3/5/3/13538666/mhealthvol5_final_15jun15_webv.pdf (Accessed November 20, 2016).
Labrique, A. B., Wadhwani, C., Williams, K. A., Lamptey, P., Hesp, C., Luk, R., et al. (2018). Best practices in scaling digital health in low and middle income countries. Glob. Health 14, 103. doi:10.1186/s12992-018-0424-z
Målqvist, M., Eriksson, L., Nga, N. T., Fagerland, L. I., Hoa, D. P., Wallin, L., et al. (2008). Unreported births and deaths, a severe obstacle for improved neonatal survival in low-income countries; a population based study. BMC Int. Health Human Rights 8, 4. doi:10.1186/1472-698x-8-4
Manya, A., Braa, J., Øverland, L., Titlestad, O., Mumo, J., and Nzioka, C. (2012). “National roll out of district health information software (dhis 2) in Kenya, 2011–central server and cloud based infrastructure,” in IST-Africa 2012 conference proceedings, Dares, Salaam, May 9–11, 2012 (Dublin, Ireland: International Information Management Corporation), 1–9.
MEASURE Evaluation (2014). Technical Report 14–110. County civil registration and vital statistics stakeholder forums: strengthening civil registration systems at the county level. Available at: https://www.measureevaluation.org/resources/publications/ (Accessed October, 2014).
Njoroge, M., Zurovac, D., Ogara, E. A., Chuma, J., and Kirigia, D. (2017). Assessing the feasibility of ehealth and mhealth: a systematic review and analysis of initiatives implemented in Kenya. BMC Res. Notes 10, 1–11. doi:10.1186/s13104-017-2416-0
Pelowski, M., Wamai, R. G., Wangombe, J., Nyakundi, H., Oduwo, G. O., Ngugi, B. K., et al. (2015). Why don’t you register your child? a study of attitudes and factors affecting birth registration in Kenya, and policy suggestions. J. Dev. Stud. 51, 881–904. doi:10.1080/00220388.2015.1010156
Privacy International (2018). The sustainable development goals, identity, and privacy: does their implementation risk human rights? Available at: https://privacyinternational.org/long-read/2237/sustainable-development-goals-identity-and-privacy-does-their-implementation-risk (Accessed August 29, 2018).
Rowntree, O., and Shanahan, M. (2020). The mobile gender gap report 2020. Available at: https://www.gsma.com/mobilefordevelopment/wp-content/uploads/2020/05/GSMA-The-Mobile-Gender-Gap-Report-2020.pdf (Accessed March 5, 2020).
Sahay, S., Nielsen, P., and Saebo, J. (2013). Systematic review of eCRVS and mCRVS interventions in low and middle income countries. Available at: https://webcache.googleusercontent.com/ (Accessed October 19, 2013).
Schoemaker, E., Kirk, T., and Rutenberg, I. (2019). Caribou digital, Kenya’s identity ecosystem. Farnham, Surrey: Caribou Digital Publishing, 1–60.
Selim, L. (2019). What is birth registration and why does it matter? Available at: https://www.unicef.org/stories/what-birth-registration-and-why-does-it-matter (Accessed December 10, 2019).
Solberg, E. (2015). From mdgs to sdgs the political value of common global goals. Harv. Int. Rev. 37, 58. doi:10.4045/tidsskr.14.1445
Sondaal, S. F. V., Browne, J. L., Amoakoh-Coleman, M., Borgstein, A., Miltenburg, A. S., Verwijs, M., et al. (2016). Assessing the effect of mhealth interventions in improving maternal and neonatal care in low-and middle-income countries: a systematic review. PloS One 11, e0154664. doi:10.1371/journal.pone.0154664
Sporny, M., Noble, G., Longley, D., Burnett, D. C., and Zundel, B. (2019). Verifiable credentials data model. Available at: https://www.w3.org/TR/vc-data-model/ (Accessed March 1, 2019).
UN General Assembly (2015). Transforming our world: the 2030 Agenda for sustainable development (UN). Available at: https://sdgs.un.org/2030agenda (Accessed November 25–27, 2015).
UNHCR (2017). Ensuring birth registration for the prevention of statelessness. Available at: https://www.refworld.org/pdfid/5a0ac8f94.pdf (Accessed November 02, 2017).
Wang, F., and De Filippi, P. (2020). Self-sovereign identity in a globalized world: credentials-based identity systems as a driver for economic inclusion. Front Blockchain 2, 28. doi:10.3389/fbloc.2019.00028
World Bank (2018). Principles on identification for sustainable development : toward the digital age. Available at: https://id4d.worldbank.org/principles (Accessed March 15, 2017).
World Health Organization (2013). Move it: report on monitoring of vital events using information technology. Available at: https://www.who.int/publications-detail-redirect/move-it-report-on-monitoring-of-vital-events-using-information-technology (Accessed October 20, 2013).
World Health Organization (2018). WHO recommendations on home-based records for maternal, newborn and child health. Available at: https://www.who.int/publications/i/item/9789241550352 (Accessed January 1, 2018).
Keywords: self-sovereign identity, decentralized identifiers (DIDs), blockchain, birth registration, newborn health, mobile phones, Kenya
Citation: Freytsis M, Barclay I, Radha SK, Czajka A, Siwo GH, Taylor I and Bucher S (2021) Development of a Mobile, Self-Sovereign Identity Approach for Facility Birth Registration in Kenya. Front. Blockchain 4:631341. doi: 10.3389/fbloc.2021.631341
Received: 19 November 2020; Accepted: 08 January 2021;
Published: 15 February 2021.
Edited by:
Kaliya Young, Merritt College, United StatesReviewed by:
Ilene Speizer, University of North Carolina at Chapel Hill, United StatesPaula Braitstein, University of Toronto, Canada
Copyright © 2021 Freytsis, Barclay, Radha, Czajka, Siwo, Taylor and Bucher. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Freytsis, bWhlYWx0aG1pZHdpZmVAZ21haWwuY29t; Sherri Bucher, c2hidWNoZXJAaXUuZWR1