 Johanna B. Folk1*
Johanna B. Folk1* Heman Gill1
Heman Gill1 Catalina Ordorica1
Catalina Ordorica1 Christopher A. Rodriguez1
Christopher A. Rodriguez1 Evan D. Holloway1
Evan D. Holloway1 Jocelyn Meza1,2
Jocelyn Meza1,2 Marina Tolou-Shams1
Marina Tolou-Shams1- 1Department of Psychiatry and Behavioral Sciences, University of California, San Francisco, San Francisco, CA, United States
- 2Department of Psychiatry and Biobehavioral Sciences, University of California, Los Angeles, Los Angeles, CA, United States
Family-based interventions delivered via telehealth are a promising mode for overcoming barriers to behavioral health treatment among youth in foster care and their families. There is a dearth of research, however, regarding effectiveness of these interventions for youth in foster care, who commonly exhibit complex behavioral health treatment needs. Clinical research in this area directly relates to equity in service access and quality for these youth and families, with numerous barriers and enabling factors to consider in order to improve engagement in clinical trials and bolster the evidence base. We present a framework to better understand the multi-systemic factors impacting youth and family engagement in clinical research on family-based telehealth interventions, drawing on relevant theory, including the bioecological model and ecodevelopmental theory. We also draw on our experiences conducting technology-based clinical research through the Family Telehealth Project, an evaluation of a brief family-based affect management intervention designed specifically for youth in foster care and their families, as a case example. Recommendations for promoting engagement in clinical research on family-based telehealth interventions with diverse youth in foster care and their families are provided.
Introduction
The Child Welfare System in the United States [sometimes referred to as the Family Regulation System (1)] is charged with investigating reports of abuse or neglect and intervening to protect children, as needed; interventions may include mandating family-based services and placing children into foster care. In 2020, 407,493 youth ages 0 to 20 years were removed from their family and placed into foster care (2). Indigenous and Black youth are at highest risk of foster care placement before age 18 (3); these inequities are driven by systemic factors (i.e., structural racism), not the commonly noted spurious “risk factor” of race (4). Youth in foster care commonly exhibit significant behavioral health treatment needs, including histories of complex trauma, mental health symptoms, and substance use. Family-based interventions are a gold-standard for youth in foster care, having demonstrated efficacy in improving mental health, substance use, educational, and delinquency outcomes (5, 6). However, geographical distance between youth in foster care and their families of origin can impede participation in family-based interventions, both in clinical practice and research trials (7, 8).
Telehealth is one promising mode for overcoming barriers (e.g., transportation) to accessing family-based treatment with youth in foster care (9, 10), however, further research regarding the effectiveness of family-based interventions delivered via telehealth is needed. Most research on telehealth service delivery has been with individual behavioral health interventions and less complex clinical presentations than commonly found among youth in foster care (11, 12). Youth in foster care are also disproportionately impacted by the digital divide, with restricted access to technology compared to their peers (13–15), which can be a barrier to participation in technology-based interventions and clinical research. As such, to maximize engagement (e.g., enrollment, retention) in clinical research on family-based telehealth interventions with youth in foster care and their families, it is crucial to attend to barriers and enabling factors specific to both system involvement and technology.
Toward this aim, we present a framework for conceptualizing factors impacting engagement in research evaluating family-based telehealth interventions while youth are in foster care (see Figure 1). The authors draw on the bioecological model (16) and ecodevelopmental theory (17), as well as experiences conducting technology-based clinical research with youth in foster care and their families through the Family Telehealth Project. We offer concrete suggestions for overcoming barriers and promoting enabling factors to engagement in order to advance the field of digital health equity research with underserved youth and families.
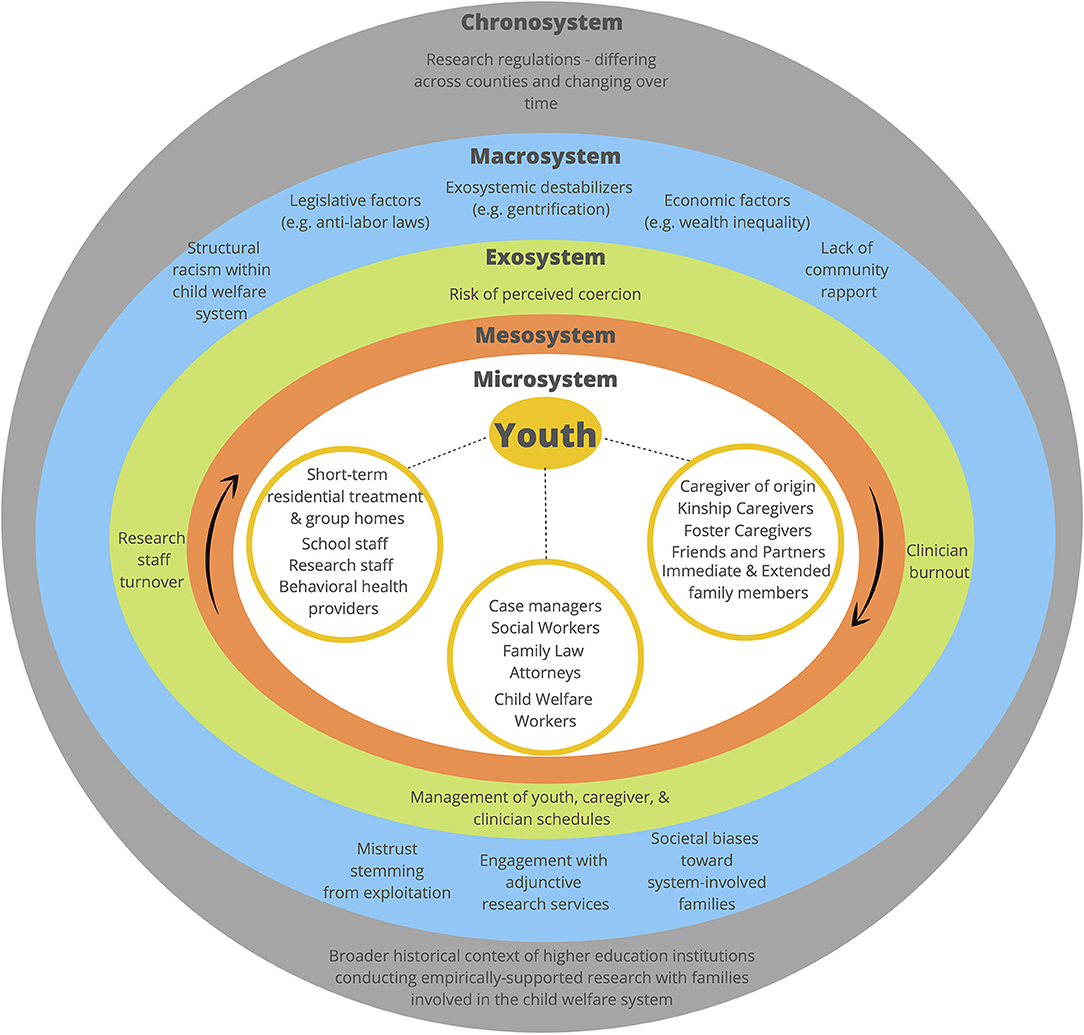
Figure 1. An ecodevelopmental framework for understanding and enhancing engagement in clinical research on family-based telehealth interventions.
An Ecodevelopmental Framework for Understanding and Enhancing Engagement in Clinical Research on Family-Based Telehealth Interventions
Ecodevelopmental Theory (17) extends Bronfenbrenner's bioecological model of human development (16) (i.e., micro-, meso-, exo-, macro-, and chrono-system influences on development and behavior) by accounting for the role of different contexts and developmental processes. Ecodevelopmental theory is particularly relevant to understanding engagement in clinical research on family-based interventions while youth are in foster care since such system involvement occurs during key developmental periods, from childbirth through adolescence. In addition to genetic and hormonal influences in utero from biological parents which directly influence early childhood development (e.g., attachment, temperament), the family microsystem has a fundamental influence on youth behavior due to prolonged and frequent interactions with family members. The family microsystem also reciprocally influences peer and romantic partner microsystems, institutional systems at the meso-system level (e.g., schools), and youth-family interactions reciprocally interact within proximal contexts (e.g., peer, community, cultural).
Factors affecting engagement (e.g., barriers and enabling factors) of youth in foster care and their families in clinical research should not be understood as uniform or static but rather as dynamic and contextual (see Figure 1). At the individual level, youth in foster care experience elevated behavioral health treatment needs, often due to sequelae of complex trauma. They also have complex micro-systems (i.e., direct interpersonal influences) consisting of not only family, friends, and partners, but also kinship or foster caregivers, child welfare workers, case managers, family law attorneys, school staff, and behavioral health clinicians, among others. The microsystem includes both physical and virtual (18) relationships; the physical microsystem consists of activities, social roles, and interpersonal relations in face-to-face (in-person) settings, whereas the virtual microsystem involves these same features on a digital platform. Individuals within the micro-system have the most direct and frequent contact with youth; researchers must therefore sustain collaborative relationships, build rapport, and maintain consistent communication with multiple persons to facilitate engagement in clinical intervention research for this specific population.
The meso-system involves interactive influences between various micro-systems (17) (e.g., parent/caregiver of origin and child welfare staff, family law attorneys and behavioral health clinicians, foster family and service delivery systems). To promote engagement at the meso-system level, researchers must assess the strength of existing relationships and encourage collaboration between individuals and systems that may not interact regularly or effectively with one another, such as child welfare workers and caregivers of origin (19).
Exo-systemic factors (i.e., indirect, interactive influences) (17) directly influence successful clinical research, including management of youth's, caregivers', and/or clinicians' schedules when coordinating family-based intervention sessions, clinician burnout, clinician and research staff turn-over, and research and legal regulatory requirements specific to this population. Specific to telehealth intervention trials, access to technology and privacy for participation in sessions and assessments may be impacted by youth's placement (e.g., youth in group homes may be sharing devices or have rules around unsupervised use of devices needed for session participation). Further, families face multiple pressures from the child welfare system to comply with mandated reunification plans, increasing the risk of coercion to participate in clinical intervention research. Families may perceive clinical intervention research participation to be required or believe participation will look favorable to the child welfare system. Although researchers have limited control/influence on exo-systemic factors and their effects on youth and families, researchers must be responsive to them to maximize youth and family engagement, particularly when it comes to perceived coercion to participate in research.
At the broader macro-systemic level, shifting societal factors that increase the likelihood of child welfare involvement should be considered to conduct prevention and intervention research more successfully. Researchers must be aware of, and responsive to, contributors to disproportionate system involvement of ethnoracial minoritized groups (3), including discrimination, structural oppression [e.g., increasingly expansive surveillance and net-widening (20), historical and ongoing effects of structural racism (4, 21)], as well as legislative and economic factors [e.g., family income, county-level poverty, and county-level income inequality (22, 23)] that contribute to child welfare system involvement, as they change over time. Macro-level factors affecting willingness to participate in clinical research may include a lack of trust toward the child welfare and affiliated healthcare systems (24–26) stemming from exploitative practices, systemic racism, and societal stereotypes and biases held toward marginalized youth impacted by the child welfare system and their families (27). Further, many youth are also dually involved in the juvenile delinquency and dependency court systems, which can result in “falling through the cracks” in timely access to needed care given challenges to information-sharing and cross-system collaboration (28); Black and Latinx youth in the child welfare system are at particularly high risk of entering the juvenile justice system (29). Specific to telehealth interventions, factors such as changes in access to technology (e.g., increasing internet access in rural areas) and wide-scale delivery of telehealth interventions which may influence their acceptability (e.g., during the COVID-19 pandemic with restrictions to in-person behavioral health services) may impact engagement in research (30). Understanding the effects of such macro-level factors can help researchers develop intervention content informed by various social, political, and cultural influences on a youth's development before and while they are enrolled in clinical research, which may facilitate engagement.
The chrono-level (i.e., temporal influences) accounts for changes that occur within and between systems at the micro-, meso-, exo- and macro-systemic levels over time (17). Interactions between multiple systems and their effects on youth and families impacted by the child welfare system are dynamic, especially those influenced by temporal changes within the family microsystem (e.g., socioeconomic mobility) and societal influences at the macro-systemic level (e.g., shifting political climate, funding priorities for services and research). Based on our own experiences, bureaucratic delays and evolving requirements when obtaining required approvals to conduct research with youth and families involved in the dependency and delinquency courts, historical contexts between research institutions and the specific populations they serve, and inequities within the higher educational system, all contribute to temporal changes impacting clinical research. Researchers must continuously identify and address gaps in the implementation of evidence-based practice, recognize how our institutions contribute to challenges engaging families impacted by the child welfare system into research and expand clinical intervention research to historically underrepresented populations.
The Family Telehealth Project
The authors draw on experiences conducting research through the Family Telehealth Project, which aims to improve behavioral health outcomes and reduce housing instability among youth in foster care (ages 12–18 years) through a family-based affect management intervention. Phase 1 involved the iterative adaptation of an empirically supported in-person family-based affect management intervention (31) for telehealth delivery and to meet the unique needs of adolescents impacted by the child welfare system and their caregivers of origin. The family-based affect management intervention being adapted was developed using the Social-Personal Framework (32), which recognizes adolescence is a period of significant emotional, cognitive, and physical changes. The Social-Personal Framework considers the interplay between individual, social, and environmental influences on adolescent risk, including individual factors, family context, and peer/partner influences. It has shown particular utility for understanding risk among adolescents in clinical settings and on probation (33, 34). The intervention includes an engagement session using motivational interviewing principles, four core modules, and a booster session (approximately 11 h of intervention time total). Core session content includes affect management, parental monitoring, and communication skills. Two clinicians work with each family to meet individually with the youth and the caregiver and then co-lead the family session. Family sessions allow for shared skill-building, practice, and discussion. Adaptation was conducted iteratively in collaboration with key stakeholders (youth, caregivers, child welfare supervisors, probation officers, judges, attorneys, school wellness staff) and through an open trial of the intervention. A caregiver-only version of the intervention is also available, covering the same core content and structure, when youth are unable to or not interested in participating. Phase 2 of the study involves an ongoing clinical trial to evaluate the effectiveness of the intervention.
Strategies for Improving Engagement of Youth in Foster Care and their Families in Clinical Research
Researchers must actively consider the dynamic, multiple levels of influence on youth in foster care and their families when conducting clinical research on family-based telehealth interventions. This includes exploration of structural vulnerabilities and social determinants of health for minoritized youth impacted by the child welfare system. Using a justice, equity, diversity and inclusion framework can enable real-word exploration of structural vulnerabilities for minoritized youth impacted by the child welfare system and facilitate the development of strategies on how to disrupt these vulnerabilities; such strategies include examination of social determinants of health and the integration of community based participatory research. We propose key recommendations addressing each system level, that we hope will disrupt these vulnerabilities (see Table 1). These proposed strategies are not exhaustive and focus on considerations unique to youth in foster care and their families; we do not include standard best practices for clinical research applicable to general populations, though these certainly still apply. We highlight select recommendations using the Family Telehealth Project as a case example.
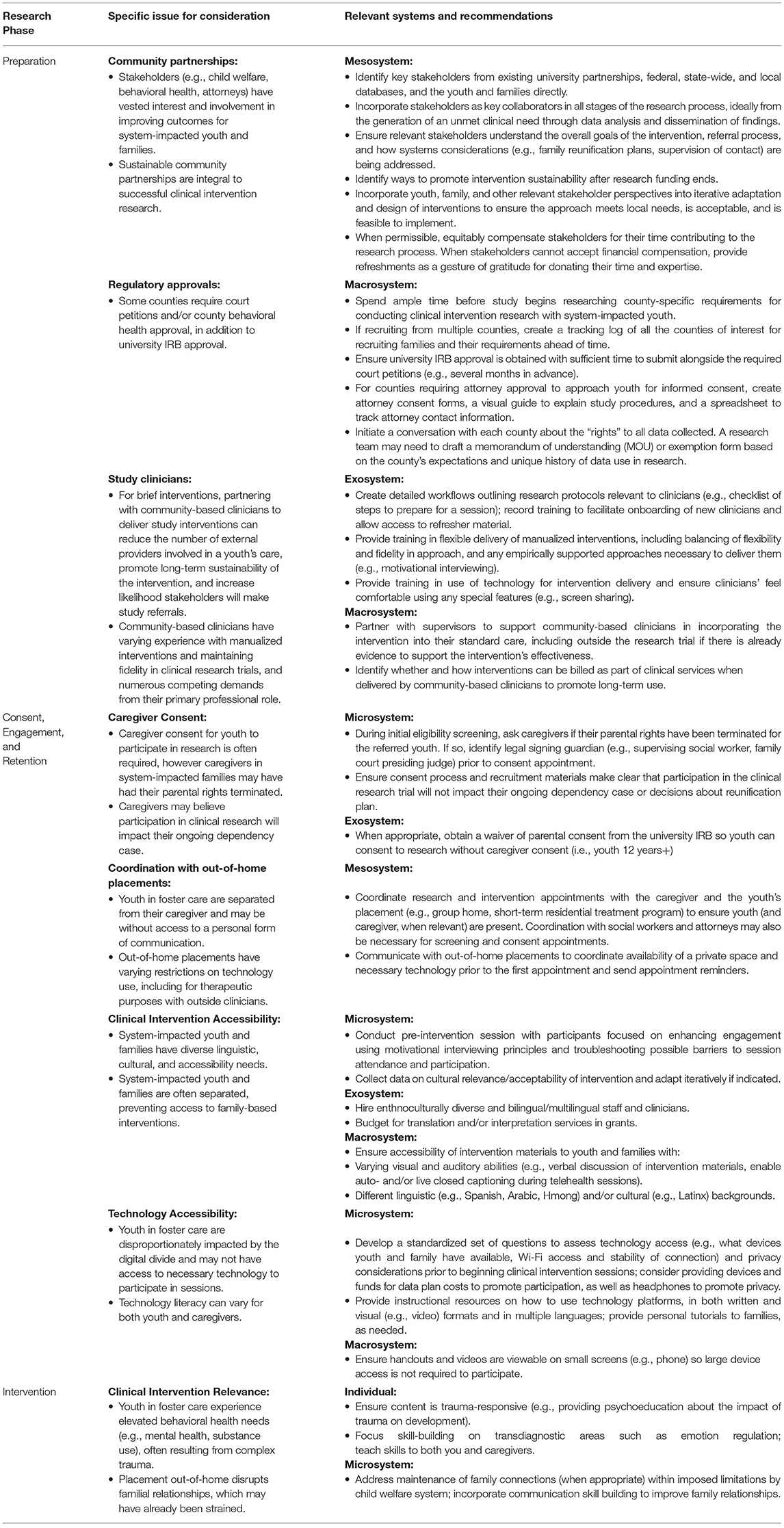
Table 1. Select recommendations for conducting clinical research on family-based telehealth interventions with youth in foster care and their families.
Interdisciplinary collaboration with key stakeholders working with youth and families impacted by the child welfare system is critical, starting from the preparation stage. In the Family Telehealth Project, we regularly consulted stakeholders from the child welfare, behavioral health, and legal (e.g., attorneys, family court judges) systems on research procedures (e.g., referral sources) and intervention content adaptation. Stakeholder input was gathered through formal data collection (i.e., focus groups) and informal meetings. For example, stakeholders reviewed all intervention session scripts in detail with the study team during monthly meetings in Phase 1 of the project. Stakeholders provided feedback on relevance of session content (e.g., maintain emphasis on substance use and sexual and reproductive health, addition of psychoeducational content on the impact of trauma and topics like dating violence) and suggested considerations for delivering content while youth are separated from their caregivers (e.g., how caregivers can engage in parental monitoring from a distance and within the context of supervised contact). Stakeholders also informed modification of activities to telehealth, noting considerations around length of sessions based on their experiences with youth over telehealth. Youth and caregivers also provided feedback on intervention content through qualitative interviews and session feedback forms during Phase 1; youth and caregivers provided invaluable insights into the utility of skills taught during sessions and overall acceptability of the intervention.
Regulatory approvals are complex when conducting research with system-impacted youth and families. In addition to approval by the institutional review board, many counties require court orders and county mental health approval to recruit youth and their caregivers into clinical intervention studies. In our experience, instructions for obtaining necessary approvals are often not clearly documented and it can require significant time and resources to determine requirements and navigate the approval process. In the Family Telehealth Project, we obtained approval to recruit for our clinical research study in five California counties; three required court orders, four required county mental health approval, and one had no formal requirements for research. We were unable to obtain approval in three additional counties due to lack of resources in the court to review and approve research proposals or requirements that the county own the data collected (rather than the researcher). Each county's approval process was unique and, in some cases, required research staff to draft court orders themselves, a skill not commonly required of research assistants in academic medicine. Each county also had unique requirements for conducting the research itself; for example, one required attorneys to provide consent prior to research staff contacting youth to explain the study and screen them for eligibility; unique attorney permission forms had to be created along with materials for attorneys to understand the research and permission process. This process was incredibly time and labor intensive. Researchers should therefore budget ample time before beginning a study researching county-specific requirements and obtaining necessary approvals. However, such system-level barriers require system-level solutions. Given the clear impact of clinical research on equity in services access and quality for youth in foster care and their families, counties should prioritize developing clear and standardized processes to support researchers dedicated to improving the health of system impacted youth and their families.
Accessibility of the intervention, both for clinicians to deliver and for youth and families to engage with, is multi-faceted. In the Family Telehealth Project, we trained clinicians at a community-based agency and a short-term residential treatment program to deliver the intervention in collaboration with study clinicians. We did so to promote continuity of care for youth already in a therapeutic relationship, ensure sustainability of the intervention after research funding ends, and build capacity among community clinicians in delivering manualized, skills-based interventions. Creation of detailed workflows and protocols related to session delivery, as well as providing training in flexible manualized intervention delivery and use of technology was critical. Community clinicians all had to complete human subjects training and be added to the institutional review board application. Clinician turnover was a major impediment; in one agency, all of the trained clinicians left their position within a year and 85% of those trained never had/referred an eligible client. Clinicians with potentially eligible clients should be carefully selected, and trainings held as close to enrollment of a potential participant as possible to ensure retention and application of knowledge. Further, training clinical supervisors in the intervention and recording training sessions for later review, can help ensure knowledge is retained within an agency even if individual clinicians leave.
For youth and caregivers, we had to account for technology factors (e.g., phone vs. computer use), varying visual and auditory abilities, and cultural and linguistic backgrounds, in delivery of the intervention. We found tailoring sessions for accessibility on a phone most useful, as many families did not have a larger screen device (e.g., computer, tablet) for participation. For example, handouts were designed for readability on a smaller phone screen. We did not provide devices or internet access to families in our study, though these are other ways to facilitate access to necessary materials for participation. For youth in group home placements, coordination with clinical staff on-site was instrumental to ensuring youth had device access and privacy to participate. Other accessibility accommodations included use of closed captioning and audio for all videos in the intervention, available in both English and Spanish; live closed captioning on videoconferencing and the chat could also be used during intervention sessions for participants with limited hearing abilities. We also hired multilingual/bilingual and ethnoculturally diverse staff to deliver the intervention and conduct research procedures with Spanish-speaking families; further, we are currently culturally adapting the intervention for Latinx families.
Discussion
The proposed framework and recommendations are intended to guide researchers committed to promoting equitable delivery of evidence-based behavioral healthcare for diverse youth in foster care and their families. Although the COVID-19 pandemic and restrictions to in-person behavioral health services highlighted the need for empirically supported interventions delivered via telehealth, behavioral healthcare via telehealth could reduce access barriers for families in non-pandemic times as well (e.g., overcoming challenges related to distance and transportation). Clinical research in this area is crucial as it directly relates to equity in services access and quality for youth in foster care and their families. It is crucial we identify ways to overcome barriers to delivery of empirically supported behavioral health treatment for youth in foster care and their families; failure to do so perpetuates service access inequities and engagement for racial/ethnic minoritized youth, who are disproportionately represented among youth in foster care (20, 35). Through cognizance of the multiple people, systems, and influences at play in a youth's life who is impacted by the child welfare system, we hope the collective research community can work to advance knowledge and implementation of empirically supported behavioral healthcare that is feasible, acceptable, and culturally relevant to reduce inequities for this highly marginalized group of youth and families.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author Contributions
All authors participated in the conceptualization of the proposed ecodevelopmental framework, writing, and editing process. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by a gift from the Visa Foundation (PI: MT-S) and a grant from the American Psychological Association (PIs: JF and MT-S). Authors also received salary support for this work from the National Institute on Drug Abuse (K23DA050798, K24DA046569, and T32DA007250) and the National Institute on Mental Health (T32MH018261).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank the members of the Juvenile Justice Behavioral Health team at the UCSF, the participants in the Family Telehealth Project, and our community stakeholder partners for their invaluable contributions to the clinical research.
References
1. Curry J, Cobbins A, Connie P, Delgado A, Gutierrez C, Ocegueda L, et al. San Francisco BIPOC Family Justice Summit: What Do BIPOC Families Need to Thrive in San Francisco? (2021). Available online at: https://bixbycenter.ucsf.edu/sites/bixbycenter.ucsf.edu/files/Family%20Justice%20Summit%20Report.pdf?utm_source=FJS+op-ed (accessed May 1, 2022).
2. Children's Bureau. The AFCARS Report (2020). Available online at: https://www.acf.hhs.gov/sites/default/files/documents/cb/afcarsreport28.pdf
3. Wildeman C, Emanuel N. Cumulative risks of foster care placement by age 18 for U.S. Children, 2000–2011. PLoS ONE. 9:e92785. doi: 10.1371/journal.pone.0092785
4. Stephens TN. Distinguishing racism, not race, as a risk factor for child welfare involvement: reclaiming the familial and cultural strengths in the lived experiences of child welfare-affected parents of color. Geneaology. (2021) 5:1–7. doi: 10.3390/genealogy5010011
5. Diamond G, Josephson A. Family-based treatment research: a 10-year update. J Am Acad Child Adolesc Psychiatry. (2005) 44:872–87. doi: 10.1097/01.chi.0000169010.96783.4e
6. Leve LD, Fisher PA, Chamberlain P. Multidimensional treatment foster care as a preventive intervention to promote resiliency among youth in the child welfare system. J Pers. (2009) 77:1869–902. doi: 10.1111/j.1467-6494.2009.00603.x
7. Schneiderman JU, Mcdaniel D, Xie B, Arnold JS. Child welfare caregivers : an evaluation of access to pediatric health care. Child Youth Serv Rev. (2010) 32:698–703.
8. Wrape ER, McGinn MM. Clinical and ethical considerations for delivering couple and family therapy via telehealth. J Marital Fam Ther. (2019) 45:296–308. doi: 10.1016/j.childyouth.2010.01.006
9. Loria H, McLeigh J, Wolfe K, Conner E, Smith V, Greeley CS, et al. Caring for children in foster and kinship care during a pandemic: lessons learned and recommendations. J Public Child Welf. (2021) 1–24. doi: 10.1080/15548732.2021.1965065
10. Defrain J. How Can Child Protection Agencies Use Telehealth to Increase Service Access for Children and Families? Strategy Brief: Strong Families. (2020). Available online at: https://www.casey.org/telehealth-strategy-brief/ (accessed January 05, 2022).
11. Backhaus A, Agha Z, Maglione ML, Repp A, Ross B, Zuest D, et al. Videoconferencing psychotherapy: a systematic review. Psychol Serv. (2012) 9:111–31. doi: 10.1037/a0027924
12. Richards D, Viganó N. Online counseling: a narrative and critical review of the literature. J Clin Psychol. (2013) 69:994–1011. doi: 10.1002/jclp.21974
13. Badillo-Urquiola K, Harpin S, Wisniewski P. Abandoned but not forgotten: Providing access while protecting foster youth from online risks. In: Proceedings of the 2017 Conference on Interaction Design and Children. Stanford, CA (2017). p. 17–26.
14. Badillo-Urquiola K, Page X, Wisniewski PJ. Risk vs. restriction: The tension between providing a sense of normalcy and keeping foster teens safe online. In: Proceedings of the 2019 CHI Conference on Human Factors in Computing Systems. (2019). p. 1–14. doi: 10.1145/3290605.3300497
15. Finn J, Kerman B, LeCornec J. Building skills–building futures: providing information technology to foster families. Fam Soc J Contemp Soc Serv. (2004) 85:165–76. doi: 10.1606/1044-3894.317
16. Bronfenbrenner U, Morris P. The ecology of the development process. In: Damon W, Lerner RM, editors. Handbook of Child Psychology. New York: Wiley (1998). p. 993–1028.
17. Szapocznik J, Coatsworth JD. An ecodevelopmental framework for organizing the influences on drug abuse: A developmental model of risk and protection. In: Glantz MD, Hartel CR, editors. Drug abuse: Origins & Interventions. American Psychological Association (1999), 331–66. doi: 10.1037/10341-014
18. Navarro JL, Tudge JRH. Technologizing bronfenbrenner: neo-ecological theory. Curr Psychol. (2022). doi: 10.1007/s12144-022-02738-3
19. Toros K, DiNitto DM, Tiko A. Family engagement in the child welfare system: a scoping review. Child Youth Serv Rev. (2018) 88:598–607. doi: 10.1016/j.childyouth.2018.03.011
20. Fong K. Neighborhood Inequality in the prevalence of reported and substantiated maltreatment. Child Abuse Negl. (2019) 90:13–21. doi: 10.1016/j.chiabu.2019.01.014
21. Hill RB. Institutional racism in child welfare. Race Soc. (2004) 7:17–33. doi: 10.1016/j.racsoc.2004.11.004
22. Eckenrode J, Smith EG, Mccarthy ME, Dineen M. Income inequality and child maltreatment in the United States. Pediatrics. (2014) 133:454–61. doi: 10.1542/peds.2013-1707
23. Lindsey D. Factors affecting the foster care placement decision: an analysis of national survey data. Am J Orthopsychiatry. (1991) 61:272–81. doi: 10.1037/h0085011
24. Hostetter M, Klein S. Understanding and Ameliorating Medical Mistrust Among Black Americans. Commonwealth Fund. (2021). p. 1–26. Available online at: https://www.commonwealthfund.org/publications/newsletter-article/2021/jan/medical-mistrust-among-black-americans (accessed May 1, 2022).
25. Jaiswal J. Whose responsibility is it to dismantle medical mistrust? Future directions for researchers and health care providers. Behav Med. (2019) 45:188–96. doi: 10.1080/08964289.2019.1630357
26. Scharf DP, Mathews KJ, Jackson P, Hofsuemmer J, Martin E, Edwards D. More than Tuskegee: Understanding mistrust about research participation. J Health Care Poor Underserved. (2010) 21:879–97. doi: 10.1353/hpu.0.0323
27. Najdowski CJ, Bernstein KM. Race, social class, and child abuse: Content and strength of medical professionals' stereotypes. Child Abus Negl. (2018) 86:217–22. doi: 10.1016/j.chiabu.2018.10.006
28. Hirsch RA, Dierkhising CB, Herz DC. Educational risk, recidivism, and service access among youth involved in both the child welfare and juvenile justice systems. Child Youth Serv Rev. (2018) 85:72–80. doi: 10.1016/j.childyouth.2017.12.001
29. Vidal S, Prince D, Connell CM, Caron CM, Kaufman JS, Tebes JK. Child abuse & neglect maltreatment, family environment, and social risk factors: determinants of the child welfare to juvenile justice transition among maltreated children and adolescents. Child Abuse Negl. (2017) 63:7–18. doi: 10.1016/j.chiabu.2016.11.013
30. Curfman A, McSwain SD, Chuo J, Yeager-McSwain B, Schinasi DA, Marcin J, et al. Pediatric telehealth in the COVID-19 pandemic era and beyond. Pediatrics. (2021) 148:e2020047795. doi: 10.1542/peds.2020-047795
31. Tolou-Shams M, Dauria E, Conrad SM, Kemp K, Johnson S, Brown LK. Outcomes of a family-based HIV prevention intervention for substance using juvenile offenders. J Subst Abuse Treat. (2017) 77:115–25. doi: 10.1016/j.jsat.2017.03.013
32. Donenberg GR, Pao M. Youths and HIV/AIDS: psychiatry's role in a changing epidemic. J Am Acad Child Adolesc Psychiatry. (2005) 44:728–47. doi: 10.1097/01.chi.0000166381.68392.02
33. Donenberg G, Emerson E, Kendall AD. HIV-risk reduction intervention for juvenile offenders on probation: The PHAT Life group randomized controlled trial. Heal Psychol. (2018) 37:364–74. doi: 10.1037/hea0000582
34. Brown LK, Hadley W, Donenberg GR, DiClemente RJ, Lescano C, Lang DM, et al. Project STYLE: a multisite RCT for HIV prevention among youths in mental health treatment. Psychiatr Serv. (2014) 65:338–44. doi: 10.1176/appi.ps.201300095
Keywords: child welfare, clinical trial, foster care, social environment (MeSH), telehealth, patient engagement
Citation: Folk JB, Gill H, Ordorica C, Rodriguez CA, Holloway ED, Meza J and Tolou-Shams M (2022) An Ecodevelopmental Framework for Engaging Diverse Youth in Foster Care and Their Families Into Technology-Based Family Intervention Research Trials. Front. Digit. Health 4:866139. doi: 10.3389/fdgth.2022.866139
Received: 30 January 2022; Accepted: 25 April 2022;
Published: 13 May 2022.
Edited by:
Terika McCall, Yale University, United StatesReviewed by:
Laura Roche, The University of Newcastle, AustraliaCopyright © 2022 Folk, Gill, Ordorica, Rodriguez, Holloway, Meza and Tolou-Shams. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johanna B. Folk, am9oYW5uYS5mb2xrQHVjc2YuZWR1