 Sára Imola Csuka
Sára Imola Csuka Barbara Horvát
Barbara Horvát Georgina Csordás
Georgina Csordás Csilla Lakatos4,†
Csilla Lakatos4,† Tamás Martos
Tamás Martos- 1Institute of Psychology, University of Szeged, Szeged, Hungary
- 2Schools of PhD Studies, Semmelweis University, Budapest, Hungary
- 3Department of Developmental and Educational Psychology, Eszterházy Károly Catholic University, Eger, Hungary
- 4Faculty of Health Sciences, University of Miskolc, Miskolc, Hungary
- 5Faculty of Psychotherapy Science, Sigmund Freud Private University, Vienna, Paris
Introduction: A growing number of health technology solutions are designed for people with diabetes to ease disease self-management. However, according to some studies, technology can also bring dissatisfaction. According to the Motivation, Engagement, and Thriving in User Experience model, the use of technology is only beneficial if it is linked to the experience of autonomy. The study aimed to investigate the associations between health technology use and technology adoption motivation and associated health behavior of people with type 1 and type 2 diabetes.
Methods: A cross-sectional questionnaire study was conducted on a sample of 315 patients with diabetes. The Technology Adoption Propensity Questionnaire was applied to assess general attitudes toward technology, the Autonomy and Competence in Technology Adoption Questionnaire for underlying motives of technology use, and the Summary of Diabetes Self-Care Activities tool for health behavior.
Results: The results showed that technology use was predicted by proficiency (but not optimism) and lower levels of vulnerability and dependence. In addition, technology use predicted health behavior (diet and physical exercise) frequency. After refining the results further, among technology users, only autonomous motivation of technology use predicted health behavior, while controlled motivation had a slightly negative predictive effect on following the diet.
Discussion: Particular attention should be paid to person-based health-related technology interventions for enhancing proficiency and reducing feelings of vulnerability and dependence on technologies. Ultimately, it is not the adoption of a technology per se, but the autonomous motivation for adoption that is associated with more favorable health behavior.
1 Introduction
The number of people living with chronic diseases is increasing. According to the WHO (1), diabetes is projected to become the seventh leading cause of death by 2030. In 2014, approximately 15% of the adult population in Hungary was found to have some kind of metabolic disorder related to diabetes, and 65% were considered overweight or obese, which are the risk factors for type 2 diabetes (2). There may also be gender differences in health behavior. The results of studies showed inconsistent findings regarding diet adherence, with some studies showing no gender differences (3, 4) while other studies found that men were more successful in weight control, which also included following the diet (5). Another study also showed that men benefited more from weight loss diabetes prevention interventions in which dietary changes and increased physical activity were important components; however, women had greater autonomous motivation (6).
The healthcare sector is now rich in opportunities to provide its users with a partnership in their treatment (7–9). The number of smartphones used worldwide has almost doubled from 3.668 to 6.378 million since 2016 (10). In Europe, 79% of the population owns a smartphone (11) and, in Hungary, 89% of the population used a smartphone in 2019 (12). Mobile applications for people with diabetes are some of the most widely used medical condition support applications (13). However, there are little data on the subjective experiences of patients using health technologies and their relationship with health behavior.
According to some studies, technology-supported disease management can be beneficial (14, 15), while other studies argued that the same technology undermines personal autonomy (e.g., giving commands or using external reinforcement strategies) (16, 17). For proper technology adoption support, it is important to investigate general technological attitudes and underlying motives of technology adaptation (18, 19).
1.1 New technologies in diabetes self-management
An important element of self-management for patients with diabetes is the integration of health behaviors (specifically diet and exercise) into their daily lives because proper disease management, with the active involvement of the patient, is one of the most important elements for preventing complications (20, 21). To achieve a physically and mentally favorable state, diabetes self-management education and support, medical nutrition therapy, routine physical activity, smoking cessation (when needed), and psychosocial care are recommended (22). Previous studies on technology use show that disease management mainly focused on mobile phone applications, which were found to be effective in facilitating lifestyle changes, particularly in people with type 2 diabetes (23, 24).
Despite the rapid emergence of new technologies, consumers' receptiveness varies. The Technology Adoption Propensity (TAP) construct was created by Ratchford and Barnhart (19) to capture attitudes toward technology in general. The model suggests that technological optimism and proficiency can facilitate the use of technology, whereas vulnerability and technological dependence can inhibit use. It allows the testing of a wide range of technologies, therefore, we have applied it to digital health technologies used by people with diabetes, which to our knowledge has not been investigated before.
1.2 Technology use and self-determination
The self-determination theory [SDT (25)] is a motivational theory that defines autonomy as the freedom of choice and the experience of self-endorsed activities (26). The opposite of autonomy is external control, when the activity is performed for extrinsic social (e.g., following medical instructions to meet the doctors’ expectations without personal involvement) or material (e.g., to look good) reasons. The Motivation, Engagement, and Thriving in User Experience (METUX) model defined by Peters et al. (18) is based on the self-determination theory and focuses on the wellbeing-enhancing element of technology, going beyond the experience of purely positive emotions (27). Up to now, few studies have examined the underlying motives (autonomous or controlled) of health technology adoption (28). According to a qualitative study among people living with diabetes, patients actively use strategies in their everyday lives to maintain autonomy and experience self-directedness in the course of disease management (29). Another study showed that the same digital health technology can be autonomy-supportive for some, while it can frustrate the autonomy of others (30). Similarly, Owens and Cribb (17) concluded that wearable devices can support personal autonomy in achieving better health, while at the same time, these can amplify health anxiety. In the case of diabetes applications, satisfaction declines in inverse proportion to the number of available features (13) and diabetes support technologies sometimes lack professional design (31). Consequently, it is crucial to take subjective experiences and the motivational aspects of technology use into account.
1.3 Overview of the current study
The concept of autonomously motivated technology usage is a crucial part of maintaining global health (30, 32). This study aimed to investigate the predictors of current health technology use (smartphone applications or wearable and portable devices), technology adoption motivation, and associated health behavior of individuals diagnosed with type 1 and type 2 diabetes in Hungary. Among the health behaviors, the central focus of our study was a healthy diet in general (i.e., following a healthy eating plan according to the person's perception) and physical activity. Both healthy diet and physical activity are self-management activities considered beneficial in all disease conditions (33), including type 1 and type 2 diabetes (34). Otherwise, the focus of the research was not on diabetes-related technologies and these are non-pharmacological treatment options (33). It is important to note that we focused on the patients’ subjective experiences in general, including their technology-related attitudes and motivations for technology use. Therefore, we worked with broad device categories and did not differentiate between specific types and characteristics.
First, we aimed to identify the sociodemographic (e.g. gender, age, and level of education) and disease-specific (e.g., diabetes type and duration) characteristics (hereafter referred to as personal characteristics) that predict technology usage. We then examined whether the usage of health technologies predicted health behavior. Furthermore, to gain a deeper understanding of the background factors of technology adoption, we applied the METUX model (18) to examine the motivation for adopting (autonomous vs. controlled adoption) a technology.
The study had three main questions:
(1) Which personal characteristics predict more frequent health technology usage by patients with diabetes when taking TAP and personal characteristics into account?
(2) Does health technology use predict the health behavior of patients with diabetes (weekly frequency of diet and exercise) when controlled for personal variables?
(3) Does the quality of motivation for technology use predict more adaptive health behavior of patients with diabetes (weekly frequency of diet and exercise) among users of health technology?
The following hypotheses were posed based on the theory and literature presented. Weekly frequencies of diet and exercise refer to the number of days in the previous week that the person did physical activity and followed their diet.
H1: A higher level of technological optimism and proficiency is associated with more frequent technology use after controlling for the effect of personal (i.e., sociodemographic and disease-specific) characteristics.
H2: A higher level of technological dependence and vulnerability is associated with less frequent technology use after controlling for the effect of personal (i.e., sociodemographic and disease-specific) characteristics.
H3: The use of health technology is associated with a higher weekly frequency of diet and exercise after controlling for personal (i.e., sociodemographic and disease-specific) characteristics.
H4: Autonomously motivated technology adoption is associated with a higher weekly frequency of diet and exercise after controlling for personal (i.e., sociodemographic and disease-specific) characteristics.
H5: Externally motivated technology adoption is associated with a lower weekly frequency of diet and exercise after controlling for personal (i.e., sociodemographic and disease-specific) characteristics.
2 Materials and methods
2.1 Participants and procedure
The study was part of a joint research project between Semmelweis University and the University of Szeged. Participants were recruited via the mailing lists of diabetes organizations and online diabetes groups. The inclusion criteria for the study were having type 1 or type 2 diabetes, not being under psychiatric treatment, and being over 18 years of age. The study was conducted using an online data collection platform (LimeSurvey) and the research was conducted in compliance with ethical rules and authorized by the Scientific and Research Ethics Committee of the Medical Research Council (authorization number: IV/2517-2020/EKU). Before participation, subjects were provided with detailed information about the study and voluntarily agreed to participate. They were able to respond anonymously and could withdraw from the study at any time.
2.2 Measurements
Beyond questions on general demographic and disease-specific data (e.g., diabetes type, duration), for health technology use, we applied the following measures.
Technology adoption: To categorize technology users and non-users and understand the types of health technologies used by participants, the participants had to indicate the digital technology or application that they used most often to maintain their health or to prevent deterioration of their health status (predefined examples given in brackets practically defined these two broad categories). The response options were (a) smartphone applications (e.g., Google Fit, Fitbit, MyFitnessPal, and Drink Water), (b) wearable and portable devices for monitoring body functions (e.g., smartwatch, smart bracelet, and smart blood glucose meter), and (c) “other device” (with the option of adding responses in their own words). For the sake of clarity, the “other” category was not included in the analysis when a digital but not clearly online tool was mentioned; however, in most cases, the response matched one of the previous categories and it was reclassified (e.g., Samsung Health was reclassified as a mobile app). We are aware that the broad category of health technology users has a high degree of heterogeneity. Thus, we followed the general definition of wearable devices “… as digital self-tracking devices designed to improve the health, fitness and well-being of their users by collecting, analyzing and displaying biomedical data” (17).
Two self-regulation scales (i.e., autonomous and controlled adoption motivation) in the Autonomy and Competence in Technology Adoption scale [ACTA (18)] were used to measure the quality of motivation behind technology adaptation. Participants were instructed to fill out the questionnaire regarding the previously indicated health technology (1 = not at all true, 5 = very true). The autonomous motivation scale contained two subscales: intrinsic (e.g. “It is going to be fun to use.”) and identified motivation (e.g. “I believe it could improve my life.”). Controlled motivation consisted of the introjected (e.g. “It will look good to others if I use it.”) and the external regulation (e.g. “I feel pressured to use it.”) subscales. The respondents who indicated that they did not use any health-related technology skipped the ACTA and were automatically led to the next scale.
The Technology Adoption Propensity Questionnaire [TAP (19, 35)] was used to measure general attitudes toward technologies (1 = the weakest agreement, 7 = the strongest agreement). The questionnaire consisted of four scales, which were optimism (e.g., “Technology gives me more control over my daily life”), proficiency (e.g., “I enjoy figuring out how to use new technologies”), vulnerability (e.g., “I think high-tech companies convince us that we need things that we don't really need”), and dependence (e.g., “Technology controls my life more than I control technology”). According to the Hungarian validation study of the questionnaire (35), an aggregated subscale of vulnerability and dependence was applied.
The Summary of Diabetes Self-Care Activities measure [SDSCA (36)] was used to measure diabetes management activities. The questionnaire includes items about general diet (r = 0.55) and physical activity. The diet-related subscale consisted of two items asking whether the respondent followed a healthy eating plan in the previous week and followed their eating plan (1 = 0 days/week, 8 = 7 days/week) for an average number of days per week during the previous month. The physical activity variable used in the analyses was completed with an additional physical activity frequency variable to enhance the internal consistency of the variable [“In the last week, how many days did you do at least 30 min of physical activity? (Total duration of continuous physical activity, including walking),” Cronbach α = 0.77].
2.3 Statistical analyses
Statistical analyses were performed using the IBM SPSS Statistics version 28 software package. The statistical procedures used were preceded by a check of the conditions of applicability in all cases. After a descriptive characterization of our sample, comparisons (independent sample t-test for continuous variables, χ2 test for binary variables, and Kolmogorov–Smirnov Z test for ordinal variables) were first made at the bivariate level between the groups of non-users and users of health technology according to personal characteristics.
To test our hypotheses, multivariate procedures were used. In the first part, binary logistic regression analysis was conducted to examine predictors of actual use of health technology. In the second part, two sets of hierarchical regression analyses were conducted. In the first set, we used two regression models to examine whether technology use predicts diet adherence and physical activity. In the second set, we included only those who used health technology and examined whether the type of technology-use-motivation predicted healthy behavior.
3 Results
Data from 315 participants were analyzed (nmen: 93, nwomen: 221, missing = 1). The mean age was 54.9 years (SD = 16.48, range = 19–87). Approximately one-third of the participants had a university, college, or higher degree (34.6%, n = 109), 13% (n = 41) had vocational qualifications, 30.2% (n = 95) had a high school diploma, and 22.2% (n = 70) graduated from primary school or vocational school. More than half of the respondents (53.9%, n = 166) reported a medium level of self-rated health, 37% (n = 114) rated their health status as good or very good, and only 9.1% (n = 28) of them rated their health status as poor or very poor (missing = 7). Of the 315 respondents, 100 reported having type 1 diabetes, and 181 reported having type 2 diabetes (missing = 35). The 297 respondents had diabetes for an average of 15.17 years (SD = 11.35, range = 1–58). Regarding the proportion of technology use, 56.2% (n = 177) of the respondents used health technology, with 53.1% (n = 94) of them using smartphone apps and 46.9% (n = 83) using wearable and portable body function monitoring devices. We followed the research questions in the analytic process and present the results in accordance.
3.1 Question 1
General differences were examined between non-user patients (43.8%, n = 138) and health technology users (56.2%, n = 177).
First, we compared patients with diabetes who used health technology to those who did not use any technology in terms of general sociodemographic and disease-related variables, health behavior (dieting and physical activity), and general willingness to adopt a technology. Table 1 summarizes the results of the independent-samples t-tests, the χ2 tests, and the Kolmogorov–Smirnov Z tests. The results show that, on average, technology users were younger [t (df = 306.68) = 5.29, p < 0.001], had higher educational attainment (Kolmogorov–Smirnov Z test = 1.79, p < 0.01), and the patients with type 1 diabetes were more likely to be technology users relative to the patients with type 2 diabetes [χ2 (df = 1) = 10.35, p < 0.01]. Regarding health behavior, technology users were more likely to follow a healthy diet [t (df = 283) = −2.04, p < 0.05] and exercise more frequently [t (df = 283) = −3.00, p < 0.01], and consequently had better overall self-rated health status (Kolmogorov–Smirnov Z test = 1.74, p < 0.01). Their attitudes were more optimistic toward technology in general [t (df = 302) = −5.78, p < 0.001] and rated themselves more proficient with technology [t (df = 252.73) = −7.67, p < 0.001].
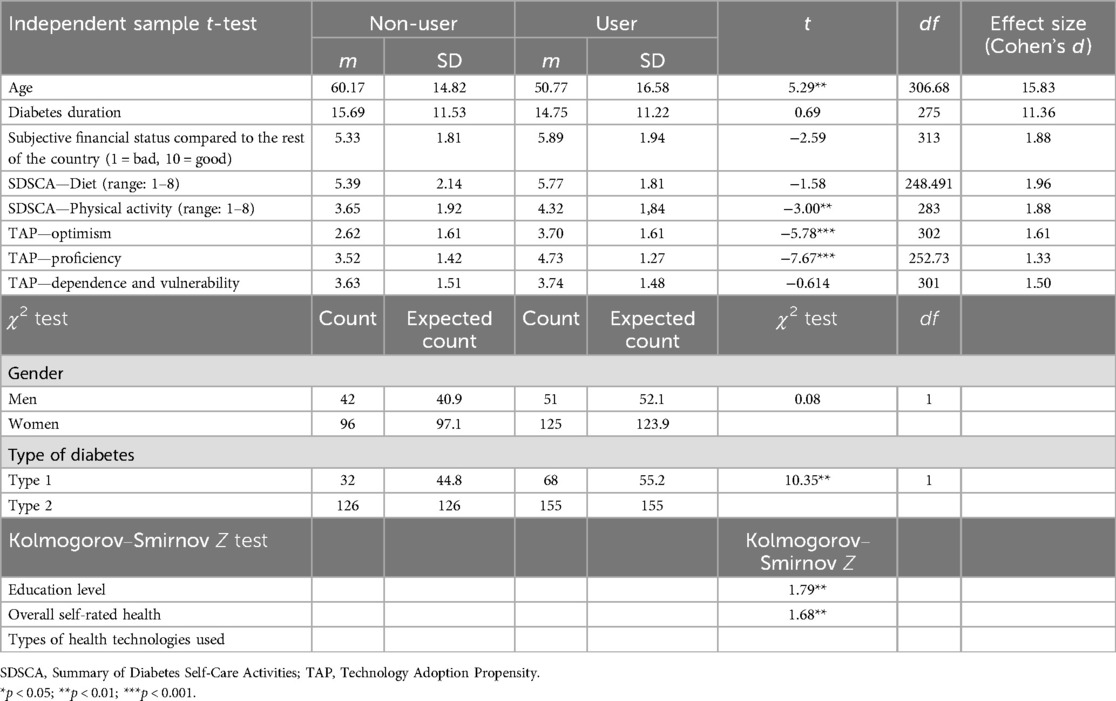
Table 1. Differences between health technology users and non-users in the studied variables.
The binary logistic regression analysis was used to examine which personal characteristics and general attitudes toward technology predicted the actual technology use (Table 2). Age [ExpB (df = 1) = 0.977, p < 0.05] and feelings of dependence and vulnerability inversely predicted health technology adoption [ExpB (df = 1) = 0.723, p < 0.01], while proficiency [ExpB (df = 1) = 2.161, p < 0.001] and having a vocational qualification [ExpB (df = 1) = 3.324, p < 0.05] positively predicted health technology adoption.
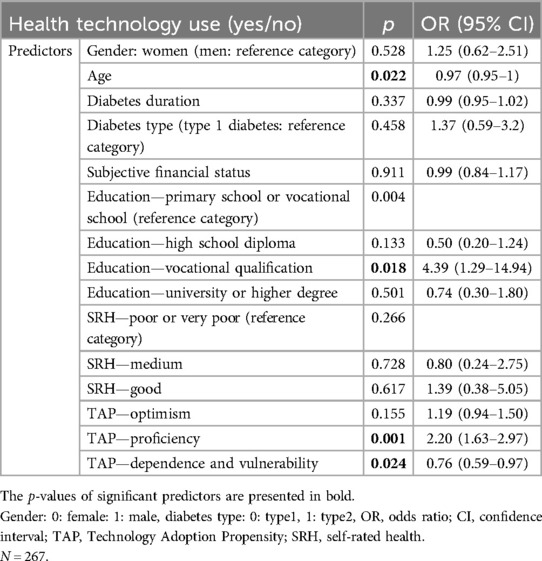
Table 2. Binary logistic regression of predictors of technology adoption (personal characteristics and technology adoption propensity).
3.2 Question 2
The hierarchical regression analysis was used to examine whether health technology use predicted health behavior after controlling for the effect of personal characteristics (Table 3).
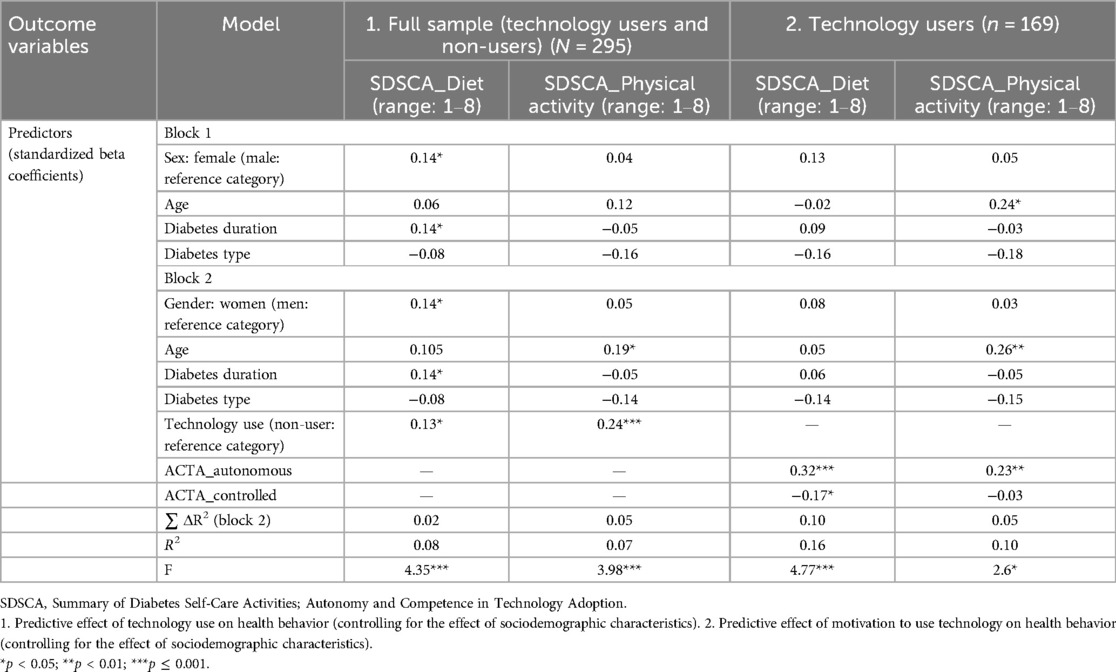
Table 3. Hierarchical regression analysis.
Both weekly healthy diet adherence (β = 0.13, p < 0.05) and exercise frequency (β = 0.24, p < 0.01) were significantly predicted by technology adoption. In addition, following a diet was predicted by gender (β = 0.14, p < 0.05, as women are more likely to follow a diet) and the duration of diagnosis (β = 0.14, p < 0.05, those living with diabetes for a longer period of time, regardless of the type of diabetes, are more likely to follow the diet). Beyond technology use, age (β = 0.19, p < 0.05, older individuals exercise more frequently) also predicted exercise frequency.
3.3 Question 3
Two additional hierarchical regression analyses were conducted only including individuals who used health technology (smartphone application or a wearable and portable device) (Table 3). We examined whether the quality of motivation underlying technology adoption predicts healthy behavior while controlling for other variables (personal characteristics). The results showed that following a diet was predicted by autonomous (β = 0.32, p < 0.001) and controlled (β = −0.17, p < 0.05) motivations for technology use, while personal characteristics did not have significant predictive power. The frequency of physical activity was also predicted by autonomously motivated technology adoption (β = 0.23, p < 0.01). However, controlled motivation and personal characteristics had no predictive power.
4 Discussion
This research aimed to investigate the complex associations between the use of health technology and health behavior in people living with type 1 and type 2 diabetes. We did not study the technology itself but rather the subjective attitudes of patients with diabetes toward these technologies and the underlying motivation for usage by applying the METUX model (18).
4.1 Personal characteristics and technology adoption
Our first research question was which personal characteristics predict health technology adoption of patients with diabetes. According to the results, the use of health technology was predicted by the following attitudes toward technology: high proficiency and low sense of dependence and vulnerability. In contrast, optimism which is a facilitating factor according to the TAP model (19) had no significant exploratory power. It is conceivable that merely a positive perception of technology is not enough to induce one to use such a technology. As reported by a recent study on the adoption of self-service technologies, proficiency had the strongest effect on actual use (37).
Our results confirmed that older people with diabetes are less likely to use technology to maintain their health. As previous studies showed, older age groups are less likely to adapt well to technology (38, 39). The increasing prevalence and multimorbidity of type 2 diabetes in the elderly underline the importance of supporting them in technology use (40).
The subjective financial status of respondents did not predict technology adoption. Previous studies showed that individuals with lower levels of income and with lower education are less likely to use technologies (38, 39). However, our sample collection probably did not reach the most disadvantaged groups, and considering the rise in smartphone usage in Europe in recent years (11), it appears that these technologies are less of a luxury. According to a recent study conducted in Hungary, almost 70% of homeless people owned a mobile phone and they used it for health purposes (41). Consequently, the actual use of mobile phones is less limited by lack of availability.
Actual health technology use was not predicted by diabetes characteristics (type and duration of diabetes). Consequently, diabetes type itself may not determine the adoption of health technology, which shows that these findings are widely applicable. However, the findings of recent reviews have shown that mobile phone diabetes applications are well established and applicable for type 2 diabetes, while these were not or less effective in people with type 1 diabetes (23, 24). In contrast, according to Adu et al. (42), a mobile phone intervention to support self-management was useful for both diabetes types. Further investigation is needed to determine the special requirements of each diabetes type.
4.2 Technology use and healthy behavior
Our second research question was about factors predicting healthy behavior (i.e., healthy diet and exercise) in people with diabetes. Health technology use was a significant predictor of the frequency of healthy behavior. Hence, those who use technology seem to be more likely to be able to use it effectively in disease management. Previous studies have suggested that health technologies can be effective facilitators of disease management (9, 23) by providing feedback and enabling self-monitoring, social networking, and regular reminders (14, 15, 43).
Some other factors besides technology use were also positively associated with healthy behavior. Those living with diabetes for longer periods were more likely to follow a diet, which suggests more established healthy behavior, and that they may be further in the process of adaptation to diabetes (44). Being a woman also predicted adherence to a healthy diet. This may be a cultural specificity as in Hungary there are higher rates of overweight men than women (40.1% of men relative to 29.2% of women) (1). This is also relevant because the rate of obesity in those with type 1 diabetes is comparable to that in the normal population (45, 46). These gender differences in health behavior require further investigation.
The frequency of physical activity was predicted by older age. It is conceivable that older people may be more likely to engage in regular physical activity, as a previous study has suggested they can devote more time to diabetes self-management and with greater regularity (4). It can be concluded that any intervention to promote health technology use should take these individual characteristics into account.
4.3 Technology use motivation and health behavior
We found that among individuals with diabetes who use health technology, internalization of the technology adoption predicted healthy behavior. This can reconcile contradictions between technology use and wellbeing (16, 17). While the autonomous motivation for technology use predicted both diet adherence and exercise frequency, the controlled motivation was independent of or showed negative associations with healthy behavior. From a theoretical perspective, our results provide support for the METUX model (18) among people with diabetes.
4.4 Limitations and future research
Our study contains some limitations. It was cross-sectional and correlational, and thus, we could not explore cause and effect relationships. For example, it is possible that a greater sense of proficiency eases the adoption of new technology, but inversely, technology adoption can also strengthen competence. A more detailed study of the antecedents of adoption processes should be conducted.
Although technology is becoming part of our everyday lives, the online data collection method may bias our findings. Nevertheless, internet users are fairly heterogeneous in terms of internet usage characteristics (47) and it is conceivable that those who use the internet are generally more competent and open to technology.
A further limitation is that we asked about health technologies (smartphone applications or wearable and portable devices) in general. Although the focus of our study was general healthy behavior and technological attitudes, this may blur potential differences between specific experiences with different technologies. However, health technology use was not predicted by the type of diabetes in previous studies (23, 24), while those with different diabetes subtypes can benefit differently from mobile phone apps promoting healthy lifestyles. It would be reasonable to investigate technologies used specifically for diabetes self-management and examine whether there are some special differences in health technology use between diabetes types. In addition, beyond diet and exercise, which are more preventive in nature, some other disease management activities (e.g., blood glucose self-monitoring) should be considered.
The motivation to use technology was examined using the METUX model (18); however, the adoption of technology is only one sphere of experience with technology. It would be worthwhile broadening the focus and examining user experiences according to what extent the technology interface or the behavior is autonomy-supportive (16, 30). In addition, targeted testing of specific health technologies through randomized control trials (48) will be needed in the future.
5 Conclusions
The results indicate that if the motivation to adopt a health technology is only externally motivating, it may not have positive consequences on health (30). Depending on patients' motivation, technology can deepen their dependence on external instructions, but can also serve as a way of experiencing autonomy. Motivational design should be applied to create technology interfaces that enhance autonomy and competence, fostering a sense of control and confidence in users. Particular attention should be paid to person-based health-related technology interventions for enhancing proficiency and reducing feelings of vulnerability and dependence (15, 28). It is suggested that practitioners should not only demonstrate the technology itself but also support the user's autonomy in using it when introducing a new health technology.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Scientific and Research Ethics Committee of the Medical Research Council, Hungary. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
SC: Conceptualization, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. BH: Methodology, Writing – original draft, Writing – review & editing. GC: Writing – original draft, Writing – review & editing, Investigation. CL: Writing – original draft, Writing – review & editing, Investigation. TM: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The research was partly supported by the NKFIH project no. K 138372, which has been implemented with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed under the K_21 funding scheme and partly by the Digital Society Competence Centre of the Humanities and Social Sciences Cluster of the Centre of Excellence for Interdisciplinary Research, Development and Innovation of the University of Szeged, where the authors are members of the “Well-being and Health in the Digital Age” research group. Manuscript preparation (writing and language editing) was also funded through Semmelweis University (Grant No. EFOP-3.6.3-VEKOP-16-2017-00009).
Acknowledgments
We would like to sincerely thank all the participants in this study for their valuable contributions. Their insights have been essential in advancing our understanding of the topic.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
SDT, self-determination theory; METUX, Motivation, Engagement, and Thriving in User Experience; TAP, Technology Adoption Propensity.
References
1. Global Obesity Observatory. Prevalence of Adult Overweight & Obesity (%). London: World Obesity Federation (2022). Available online at: https://data.worldobesity.org/tables/prevalence-of-adult-overweight-obesity-2/
2. Leong KS, Wilding JP. Obesity and diabetes. Best Pract Res Clin Endocrinol Metab. (1999) 13(2):221–37. doi: 10.1053/beem.1999.0017
3. Mirahmadizadeh A, Khorshidsavar H, Seif M, Sharifi MH. Adherence to medication, diet and physical activity and the associated factors amongst patients with type 2 diabetes. Diabetes Ther. (2020) 11(2):479–94. doi: 10.1007/s13300-019-00750-8
4. Xie Z, Liu K, Or C, Chen J, Yan M, Wang H. An examination of the socio-demographic correlates of patient adherence to self-management behaviors and the mediating roles of health attitudes and self-efficacy among patients with coexisting type 2 diabetes and hypertension. BMC Public Health. (2020) 20(1):1227. doi: 10.1186/s12889-020-09274-4
5. Koponen AM, Simonsen N, Suominen S. Success in increasing physical activity (PA) among patients with type 2 diabetes: a self-determination theory perspective. Health Psychol Behav Med. (2018) 6(1):104–19. doi: 10.1080/21642850.2018.1462707
6. Trief PM, Cibula D, Delahanty LM, Weinstock RS. Self-determination theory and weight loss in a diabetes prevention program translation trial. J Behav Med. (2017) 40(3):483–93. doi: 10.1007/s10865-016-9816-9
7. Mesko B. Digital health technologies and well-being in the future. IT Prof. (2020) 22(1):20–3. doi: 10.1109/MITP.2019.2963121
8. Meskó B, Drobni Z, Bényei É, Gergely B, Győrffy Z. Digital health is a cultural transformation of traditional healthcare. mHealth. (2017) 3:38–38. doi: 10.21037/mhealth.2017.08.07
9. Moller AC, Merchant G, Conroy DE, West R, Hekler E, Kugler KC, et al. Applying and advancing behavior change theories and techniques in the context of a digital health revolution: proposals for more effectively realizing untapped potential. J Behav Med. (2017) 40(1):85–98. doi: 10.1007/s10865-016-9818-7
10. Statista. Statista (Number of Smartphone Subscriptions Worldwide from 2016 to 2021, with Forecasts from 2022 to 2027). Hamburg: Statista (2022). Available online at: https://www.statista.com/statistics/330695/number-of-smartphone-users-worldwide/ (Accessed June 23, 2022) (Accessed November 21, 2020).
11. GSMA. The Mobile Economy Europe 2022. London: GSMA (2022). Available online at: https://www.gsma.com/mobileeconomy/wp-content/uploads/2022/10/051022-Mobile-Economy-Europe-2022.pdf (Accessed January 16, 2023).
12. eNET. 5,3 Millió Okostelefon-használó Hazánkban=5.3 Million Smartphone Users in our Conuntry. Budapest: eNET (2019). Available online at: https://enet.hu/53-millio-okostelefon-hasznalo-hazankban/
13. Hood M, Wilson R, Corsica J, Bradley L, Chirinos D, Vivo A. What do we know about mobile applications for diabetes self-management? A review of reviews. J Behav Med. (2016) 39(6):981–94. doi: 10.1007/s10865-016-9765-3
14. Wang Y, Xue H, Huang Y, Huang L, Zhang D. A systematic review of application and effectiveness of mHealth interventions for obesity and diabetes treatment and self-management. Adv Nutr Int Rev J. (2017) 8(3):449–62. doi: 10.3945/an.116.014100
15. Wulfovich S, Fiordelli M, Rivas H, Concepcion W, Wac K. “I must try harder”: design implications for mobile apps and wearables contributing to self-efficacy of patients with chronic conditions. Front Psychol. (2019) 10:2388. doi: 10.3389/fpsyg.2019.02388
16. Calvo RA, Peters D, Vold K, Ryan RM. Supporting human autonomy in AI systems: a framework for ethical enquiry. In: Burr C, Floridi L, editors. Ethics of Digital Well-Being. Cham: Springer International Publishing (2020) 140. p. 31–54. Philosophical Studies Series. doi: 10.1007/978-3-030-50585-1_2 (Accessed July 29, 2022).
17. Owens J, Cribb A. ‘My Fitbit thinks I can do better!’ do health promoting wearable technologies support personal autonomy? Philos Technol. (2019) 32(1):23–38. doi: 10.1007/s13347-017-0266-2
18. Peters D, Calvo RA, Ryan RM. Designing for motivation, engagement and wellbeing in digital experience. Front Psychol. (2018) 9:797. doi: 10.3389/fpsyg.2018.00797
19. Ratchford M, Barnhart M. Development and validation of the technology adoption propensity (TAP) index. J Bus Res. (2012) 65(8):1209–15. doi: 10.1016/j.jbusres.2011.07.001
20. Beck J, Greenwood DA, Blanton L, Bollinger ST, Butcher MK, Condon JE, et al. National standards for diabetes self-management education and support. Diabetes Spectr. (2017) 30(4):301–14. doi: 10.2337/ds17-0067
21. Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. (2013) 12(1):14. doi: 10.1186/2251-6581-12-14
22. The American Diabetes Association (ADA). Index. Diabetes Care. (2022) 45(Supplement_1):S259–64. doi: 10.2337/dc22-in01
23. Wu X, Guo X, Zhang Z. The efficacy of mobile phone apps for lifestyle modification in diabetes: systematic review and meta-analysis. JMIR MHealth UHealth. (2019) 7(1):e12297. doi: 10.2196/12297
24. Wu Y, Yao X, Vespasiani G, Nicolucci A, Dong Y, Kwong J, et al. Mobile app-based interventions to support diabetes self-management: a systematic review of randomized controlled trials to identify functions associated with glycemic efficacy. JMIR MHealth UHealth. (2017) 5(3):e35. doi: 10.2196/mhealth.6522
25. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. (2000) 55(1):68–78. doi: 10.1037/0003-066X.55.1.68
26. Ryan RM, Deci EL. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York, NY: Guilford Press (2017). Available online at: https://www.google.com/books/edition/Self_Determination_Theory/th5rDwAAQBAJ?hl=en&gbpv=1&dq=inauthor:%22Richard+M.+Ryan%22 (Accessed August 1, 2022).
27. Peters D, Ahmadpour N, Calvo RA. Tools for wellbeing-supportive design: features, characteristics, and prototypes. Multimodal Technol Interact. (2020) 4(3):40. doi: 10.3390/mti4030040
28. Yardley L, Morrison L, Bradbury K, Muller I. The person-based approach to intervention development: application to digital health-related behavior change interventions. J Med Internet Res. (2015) 17(1):e30. doi: 10.2196/jmir.4055
29. Sallay V, Klinovszky A, Csuka SI, Buzás N, Papp-Zipernovszky O. Striving for autonomy in everyday diabetes self-management—qualitative exploration via grounded theory approach. BMJ Open. (2021) 11(12):e058885. doi: 10.1136/bmjopen-2021-058885
30. Wannheden C, Stenfors T, Stenling A, von Thiele Schwarz U. Satisfied or frustrated? A qualitative analysis of need satisfying and need frustrating experiences of engaging with digital health technology in chronic care. Front Public Health. (2021) 8:623773. doi: 10.3389/fpubh.2020.623773
31. Hoppe CD, Cade JE, Carter M. An evaluation of diabetes targeted apps for android smartphone in relation to behaviour change techniques. J Hum Nutr Diet. (2017) 30(3):326–38. doi: 10.1111/jhn.12424
32. Burr C, Taddeo M, Floridi L. The ethics of digital well-being: a thematic review. Sci Eng Ethics. (2020) 26(4):2313–43. doi: 10.1007/s11948-020-00175-8
33. Evert AB, Riddell MC. Lifestyle intervention. Med Clin North Am. (2015) 99(1):69–85. doi: 10.1016/j.mcna.2014.09.001
34. Garvey WT, Arathuzik G. Lifestyle therapy for diabetes Mellitus. In: Mechanick JI, Kushner RF, editors. Lifestyle Medicine. Cham: Springer International Publishing (2016). p. 221–43. doi: 10.1007/978-3-319-24687-1_22 (Accessed January 18, 2023).
35. Martos T, Kapornaky M, Csuka S, Sallay V. A technológiai megoldásokkal kapcsolatos attitűdök mérése: a TRI és a TAP magyar változatának pszichometriai jellemzői. Alkalm Pszichol. (2019) 19(1):97–117. doi: 10.17627/ALKPSZICH.2019.1.97
36. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. (2000) 23(7):943–50. doi: 10.2337/diacare.23.7.943
37. Ratchford M, Ratchford BT. A cross-category analysis of dispositional drivers of technology adoption. J Bus Res. (2021) 127:300–11. doi: 10.1016/j.jbusres.2021.01.037
38. Lustria MLA, Smith SA, Hinnant CC. Exploring digital divides: an examination of eHealth technology use in health information seeking, communication and personal health information management in the USA. Health Informatics J. (2011) 17(3):224–43. doi: 10.1177/1460458211414843
39. Magotra I, Sharma J, Sharma SK. Technology adoption propensity of the banking customers in India: an insight. Int J Manag Account Econ. (2015) 2(2):111–24.
40. Bellary S, Kyrou I, Brown JE, Bailey CJ. Type 2 diabetes mellitus in older adults: clinical considerations and management. Nat Rev Endocrinol. (2021) 17(9):534–48. doi: 10.1038/s41574-021-00512-2
41. Radó N, Girasek E, Békási S, Győrffy Z. Digital technology access and health-related internet use among people experiencing homelessness in Hungary: quantitative survey. J Med Internet Res. (2022) 24(10):e38729. doi: 10.2196/38729
42. Adu MD, Malabu UH, Malau-Aduli AE, Drovandi A, Malau-Aduli BS. User retention and engagement with a mobile app intervention to support self-management in Australians with type 1 or type 2 diabetes (my care hub): mixed methods study. JMIR MHealth UHealth. (2020) 8(6):e17802. doi: 10.2196/17802
43. Lewinski AA, Anderson RA, Vorderstrasse AA, Fisher EB, Pan W, Johnson CM. Type 2 diabetes education and support in a virtual environment: a secondary analysis of synchronously exchanged social interaction and support. J Med Internet Res. (2018) 20(2):e61. doi: 10.2196/jmir.9390
44. Sebire SJ, Toumpakari Z, Turner KM, Cooper AR, Page AS, Malpass A, et al. “I’ve made this my lifestyle now”: a prospective qualitative study of motivation for lifestyle change among people with newly diagnosed type two diabetes mellitus. BMC Public Health. (2018) 18:204. doi: 10.1186/s12889-018-5114-5
45. Wallace AS, Chang AR, Shin JI, Reider J, Echouffo-Tcheugui JB, Grams ME, et al. Obesity and chronic kidney disease in US adults with type 1 and type 2 diabetes mellitus. J Clin Endocrinol Metab. (2022) 107(5):1247–56. doi: 10.1210/clinem/dgab927
46. Polsky S, Ellis SL. Obesity, insulin resistance, and type 1 diabetes mellitus. Curr Opin Endocrinol Diabetes Obes. (2015) 22(4):277–82. doi: 10.1097/MED.0000000000000170
47. Zajac I. Internet usage and openness to internet-delivered health information among Australian adults aged over 50 years. Australas Med J. (2012) 5(5):262–7. doi: 10.4066/AMJ.2012.1065
Keywords: patients with diabetes, health technology, self-determination theory, METUX model, technology adoption
Citation: Csuka SI, Horvát B, Csordás G, Lakatos C and Martos T (2025) Technology use and health behavior among patients with diabetes: do underlying motives for technology adoption matter? Front. Digit. Health 7:1455261. doi: 10.3389/fdgth.2025.1455261
Received: 26 June 2024; Accepted: 17 March 2025;
Published: 15 April 2025.
Edited by:
Edith Eva Holloway, Australian Centre for Behavioural Research in Diabetes (ACBRD), AustraliaReviewed by:
Richard M. Ryan, Australian Catholic University, AustraliaLubna Daraz, University of Montreal, Canada
Copyright: © 2025 Csuka, Horvát, Csordás, Lakatos and Martos. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sára Imola Csuka, Y3N1a2Euc2FyYUBzenRlLmh1
†ORCID:
Sára Imola Csuka
orcid.org/0000-0001-6337-2723
Barbara Horvát
orcid.org/0000-0002-2518-2096
Georgina Csordás
orcid.org/0000-0002-9225-6251
Csilla Lakatos
orcid.org/0000-0002-9566-4496
Tamás Martos
orcid.org/0000-0001-5946-1299