 Soraya Puglisi
Soraya Puglisi Francesco Ferraù
Francesco Ferraù Marta Ragonese
Marta Ragonese Federica Spagnolo
Federica Spagnolo Salvatore Cannavò
Salvatore Cannavò- 1Endocrine Unit, University Hospital G. Martino, Messina, Italy
- 2Internal Medicine, Department of Clinical and Biological Sciences, University of Turin, Turin, Italy
- 3Department of Human Pathology of Adulthood and Childhood, University of Messina, Messina, Italy
Acromegaly is a disease due to chronic GH excess and a consequent rise in IGF-1 levels. This rare endocrine condition is associated with metabolic alterations such as hyperglycaemia, dyslipidaemia, and systemic arterial hypertension, which, in addition to GH excess-related cardiovascular changes, play critical roles in increasing cardiovascular risk and mortality rates. Biochemical control of acromegaly, achieved by means of surgical, and/or medical treatment, positively impacts on cardiovascular risk factors and metabolic alterations, reducing overall patient mortality. However, treatment modalities of acromegaly and disease control differently impact on glucose homeostasis and lipid changes, and consequently on cardiometabolic risk. In this regard, pasireotide was shown to significantly influence glucose metabolism. This review summarizes the cardiometabolic consequences of acromegaly and its treatment, focusing on available data around the effects of medical therapy with pasireotide on factors that influence cardiometabolic risk.
Cardiovascular and Metabolic Complications in Acromegaly: an Overview
Acromegaly is a rare disease, resulting from excessive GH production and a consequent rise of IGF-1 levels. This condition is associated with increased morbidity and mortality when compared with an age-matched general population, mainly owing to higher cardiovascular risk and a worse metabolic profile (1, 2). In fact, cardiovascular disease seems to contribute toward death in 23–50% of cases (depending on patient age, or years in which the studies were conducted) (3). It is known that increased levels of GH/IGF-1 have a sodium-retaining effect, causing an increase in extracellular volume which contributes to hypertension (4), as well as determining morpho-functional heart alterations such as hypertrophy, diastolic dysfunction, up to systolic dysfunction in the end-stage (5).
Hypertension affects 33.6% of patients with acromegaly, ranging from 11 to 54.7% in different series (6), and represents an independent predictor of mortality (7). A positive correlation between disease duration and the prevalence of hypertension (8) has been demonstrated, similar to what is observed about other cardiac complications in acromegaly patients, including valvulopathy (found, at diagnosis, in ~75% of patients), and arrhythmias (occurring ~90% of patients with active disease) (3). Conversely, conflicting data has been reported regarding the prevalence of atherosclerosis in acromegaly, since some authors reported increased incidence of carotid intima-media thickness (9), while others did not confirm this finding (10). Similarly, one study failed to demonstrate an increased risk for coronary artery disease (11), while we found, by means of an integrated assessment of the Framingham score with the Agatston coronary artery calcium score, a risk of coronary atherosclerosis in 40% of acromegaly patients, and evidence of coronary calcifications in about half of them (12). Moreover, a subsequent study of our group demonstrated reduced life expectancy in acromegaly patients with a high Framingham score, and an increased risk of lethal ischemic cardiovascular (CV) events associated with an elevated Agatston score (13).
In this context, the role of lipid abnormalities in acromegaly is crucial. It is known that GH/IGF-I hypersecretion provides anabolic and lipolytic effects, while the most common lipid profile alterations are hypertriglyceridemia (occurring in 33–40% of patients with acromegaly, which is three times higher than in the general population) and low levels of HDL cholesterol (39–47% of cases), whereas the prevalence of hypercholesterolemia is similar to that of the general population (3). On the other hand, circulating levels of Lp-a, Apo A-I, and Apo E, which are involved in the transport of triglycerides, cholesterol, and small dense LDL particles, and promote the development of vascular damage and atherosclerosis, were found to be elevated in acromegaly patients (3).
In addition, a notable contribution to the unfavorable cardiovascular profile of acromegaly patients is provided by glucose metabolism impairment. GH/IGF-1 hypersecretion affects insulin sensitivity, promotes gluconeogenesis, reduces glucose uptake in fat tissue and muscles, and impairs the function of β pancreatic cells (14). Consequently, the prevalence of glucose metabolism abnormalities in acromegaly exceeds that of the general population, varying significantly between studies mainly due to the heterogeneity of diagnostic criteria. The frequency of diabetes mellitus (DM) ranges from 16 to 56%; impaired glucose tolerance (IGT) from 6 to 45%; and impaired fasting glucose (IFG) from 7 to 22% (3). In patients with acromegaly, DM occurs at a younger age than in the general population (15, 16), and is associated with a worse prognosis (16, 17). It is worthy of note that the development of glucose metabolism abnormalities is associated with disease duration and severity, but they often occur in the earliest phases of acromegaly (14). In some studies, DM has been found to correlate positively with hypertension and to be a predictor of disease activity, mortality, and of a low probability of achieving disease control (7, 15, 16).
Finally, acromegaly is associated with sleep apnea (occurring in 45–80% of cases, according to a different series) (18), which is known to be predisposing to hypertension and arrhythmias, as well as affect metabolic profiles, and therefore contribute to increased cardiovascular mortality.
Effects of Biochemical Control of Acromegaly on Cardiometabolic Complications
In acromegaly, transsphenoidal surgical removal of the pituitary adenoma remains the treatment of choice in most cases, but medical therapy has been playing an increasing role in recent decades (19). First-line medical therapy consists of somatostatin analogs (SSA), including octreotide and lanreotide, with proven efficacy for around 50% of patients in terms of GH control and IGF-1 normalization (20). Nevertheless, encouraging data about the efficacy of pasireotide, a new multireceptor-targeted SSA, has been provided (21). Moreover, a significant figure (60–90%) of patients treated with the GH-receptor antagonist pegvisomant (PEG) achieve IGF-1 normalization (22–25). Further treatment options to help obtain disease control are cabergoline and radiotherapy (19).
The benefits of acromegaly control have been demonstrated at multiple levels. First of all, achieving biochemical control seems to positively impact on mortality risk. In 2004, Holdaway et al. reported a mortality rate reduced to near that of the general population among acromegaly patients who obtain normalization of serum IGF-1 and reduction of GH values <1 μg/L (7). The same study also showed that the last GH (or, in substitution, the last IGF-1) value was an independent predictor of survival in multivariate analysis. These findings were confirmed by meta-analysis, which reported a Standard Mortality Rate (SMR) close to that of the general population in biochemically controlled acromegaly patients (random serum GH <2.5 μg/L, or normalization of IGF-1 levels at the last follow-up) (26). Accordingly, a retrospective single-center study confirmed that SMR was higher in acromegaly patients when GH was >2.5 ng/ml at last visit, showing that overall mortality can be reduced by using a multimodal approach and carefully managing comorbidities (27). More recently, Postma et al. showed that SMR was not increased in adequately controlled acromegaly patients (28). Taking into account that one of the most important causes of death in acromegaly patients is CV events (7, 15, 29), it is reasonable to suppose an effect of acromegaly control on CV diseases. This hypothesis has been indirectly confirmed by Jayasena et al. (30), who demonstrated an association between ischemic heart disease and a high GH burden (calculated for each patient by multiplying the number of years of disease duration by the mean level of GH recorded during the entire follow-up), and between cerebrovascular disease/cardiomyopathy and a higher mean IGF-1 burden (calculated similarly to the GH burden, using the mean IGF-1 index). Similarly, Varadhan et al. (31) reported significantly higher cumulative GH exposure in acromegaly patients who died and in those who developed hypertension, diabetes, or CV events during follow-up. In contrast to these findings, a retrospective study, including 200 acromegaly patients (11.8% of whom reported CV events during follow-up), only identified age and smoking as predictors of CV events in multivariate analysis, although a lack of control of acromegaly was the strongest determinant of diabetes (32).
The effects of attaining control over GH and IGF-1 excess have been demonstrated by acromegalic cardiomyopathy. An improvement of the left ventricular mass index has been reported in patients treated with surgery (9, 33), SSA (33–35), and PEG (36). The effects of biochemical control of acromegaly on hypertension are more controversial, being heterogeneous across studies. Some authors reported a higher rate of hypertension in uncontrolled acromegaly than in patients with controlled disease (37, 38), while other researches resized the relevance of the normalization of hormonal parameters on hypertension (32, 39).
Moreover, blood pressure profile also seems to be influenced by abnormalities of glucose metabolism (40), thus adding a further incentive to control metabolic comorbidities. In this context, there are consistent data about the improvement of glycemic alterations after surgery (34, 41). A recent study, assessing 151 newly diagnosed acromegaly patients with an oral glucose tolerance test (OGTT) before and 3–12 months after surgery, showed an improvement of glucose tolerance in 87.3% patients with IGT, and in 66.7% of those with DM (41). Conversely, medical therapies exert different effects on glucose metabolism. Although octreotide and lanreotide reduce pancreatic insulin secretion, the negative impact on glucose homeostasis seems to be counterbalanced by the improvement of insulin resistance (14). However, the debate is still open, and several trials have been carried out to clarify this issue (Table 1). In the last decade, two meta-analyses led to different conclusions (Table 1) (42, 49). Mazziotti et al. (42), evaluating 31 retrospective and prospective studies performed from 1987 to 2008, concluded that conventional doses of octreotide and lanreotide do not significantly increase fasting plasma glucose (FPG) or serum glycosylated hemoglobin (HbA1c), while possibly negatively impacting on response to OGTT. Conversely, Cozzolino et al. (49) analyzed 47 prospective studies performed from 1993 to 2017 and showed an increase of HbA1c and glucose levels after OGTT, reporting a significant increase of FPG only if SSA were used as second-line treatment.
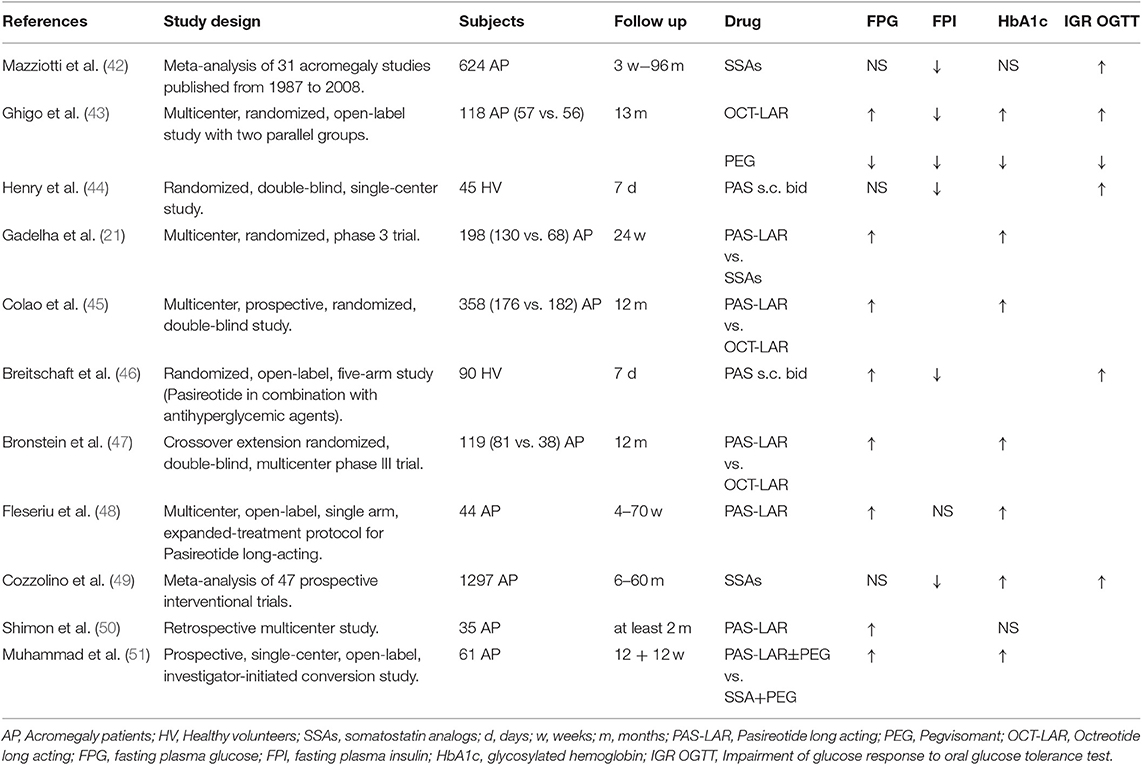
Table 1. Effects of first- and second-generation SSAs on glucose metabolism.
The effect of PEG on glycemic alterations is more defined, showing improvement of insulin sensitivity, FPG, and HbA1c in IGT and DM, although it is debated whether these changes are due to biochemical control (without inhibition of insulin secretion by SSA) or specific drug effects (43, 52, 53).
Biochemical control of acromegaly also impacts on lipid alterations. A retrospective study showed an improvement of hypertriglyceridemia and HDL cholesterol levels after normalization of IGF-1/GH levels achieved with either surgery or medical therapy, although this did not occur in all patients with controlled disease (54). More recently, 42 patients with untreated active acromegaly were prospectively studied, evaluating changes in metabolic profile after surgery and comparing those who achieved remission with those who did not. Total and LDL cholesterol levels did not change after surgery for either controlled or uncontrolled patients. Conversely, in the remission group, HDL levels rose while triglycerides levels fell, whereas in patients with persistent active acromegaly there was no change (55). A 48-week treatment with lanreotide autogel (120 mg/4 weeks) has been reported to significantly decrease triglycerides and increase HDL cholesterol levels in non-diabetic acromegaly patients, without significant changes to total as well as LDL cholesterol levels (56).
Finally, medical therapy of acromegaly improves sleep apnea, although frequently irreversible alterations of the craniofacial anatomy and the upper respiratory tract hamper a total remission (18). The beneficial effects of SSA are due to the reduction in swelling of the upper airway soft tissue, and particularly of tongue volume (57). Grunstein et al. (58) reported a 40% decrease in total apnea time, with an improvement in indices of oxygen desaturation and sleep quality after 6 months of octreotide. However, the authors showed no correlation between the decrease in total apnea time and the reduction of GH levels. Similarly, Annamalai et al. (59) demonstrated an improvement of the apnea/hypopnea index score in 61% of patients treated for 24 weeks with lanreotide autogel, but without any correlation to changes of GH and IGF-1. Therefore, medical treatment with SSA reduces the severity of sleep apnea, which can persist despite normalization of GH levels or significantly improve, even in cases of partial biochemical remission.
The Cardiometabolic Risk Among Acromegaly Patients Treated With Pasireotide
Treatment modalities of acromegaly and disease control impact differently on glucose homeostasis and lipid changes, and consequently on cardiometabolic risk. In the class of SSA, pasireotide (PAS) was shown to significantly influence glucose metabolism (60). PAS is a multi-receptor targeted SSA with higher binding affinity for somatostatin receptor (SSTR) 1, 3, and 5 and lower for SSTR2 than octreotide and lanreotide (61).
Clinical studies demonstrated that, compared to OCT-LAR, PAS long acting release (PAS-LAR) treatment was more effective in achieving biochemical control in acromegaly patients, and was able to provide greater biochemical control in patients inadequately controlled by OCT-LAR or lanreotide autogel (21, 45, 47, 62). Clinical trials demonstrated the efficacy but also the safety of treatment with PAS, although hyperglycaemia-related adverse events were common (63). Indeed, Colao et al. showed that hyperglycaemia occurred in the 28.7% of patients treated with PAS-LAR and in the 8.3% of those treated by OCT-LAR (45). Moreover, antidiabetic medication was needed in 44.4% of patients treated with PAS-LAR, and in 26.1% of those treated with OCT-LAR (45). In the PAOLA study, at 24-week evaluation, 21 and 26% of 198 patients treated with PAS-LAR 40 mg/ or 60 mg/28 days, respectively, developed diabetes mellitus (21). In a 12-month crossover extension of the PAOLA study, patients with inadequate biochemical control at the end of core study were switched to PAS-LAR or OCT-LAR. In the PAS-LAR treated group, 13.6% discontinued the treatment because of hyperglycaemia-related adverse events, while no one discontinued OCT-LAR because of glucose metabolism alterations (47). Results from the ACCESS study documented hyperglycaemia-related adverse events in 45.5% of acromegaly patients receiving PAS-LAR 40 mg/28 days, with type 2 diabetes mellitus occurring in 13.6% of cases. Mean HbA1c and fasting plasma glucose levels significantly increased, respectively, from 5.9% and 100.4 mg/dl at baseline to 6.8% and 135.9 mg/dl after 3 months of treatment (48). Recently, in a “real life” retrospective multicentre study, PAS-LAR was shown to be effective in 54% of acromegaly patients resistant to OCT-LAR or lanreotide autogel, and treated with PAS-LAR, while 63% experienced glucose metabolism alterations, leading to initiation or intensification of antidiabetic treatment in 77.3% of them (50).
In the PAPE study, 61 patients with controlled acromegaly under SSA or PEG were switched to PAS-LAR with or without PEG. After 24 weeks of treatment, PAS-LAR was well-tolerated, but the 88.5% of adverse events were hyperglycaemia-related (65.6% were grade 1 and 2, while 23.0% were grade 3 and 4; all related to PAS-LAR). Moreover, the number of diabetic patients doubled, increasing from 32.8% at baseline to 68.9% at the end of the study. After 24 weeks, 44% of patients started an antidiabetic treatment while almost 25% had to change to a glucose-lowering drug, most of them treated with a combination of metformin and DPP4 inhibitor (51). In the PAPE extension study, frequency of diabetes mellitus increased from 68% at 24 weeks to 77% at 48 weeks, while 9 patients had to discontinue PAS-LAR because of severe hyperglycaemia. In this study, moreover, PAS-induced hyperglycaemia was inversely correlated with baseline insulin secretion. In this regard, in clinical trials, the risk of developing hyperglycaemia was higher in patients who were defined diabetic or prediabetic at baseline (51). In the PAOLA study, 31 and 26% of the patients receiving PAS-LAR 40 mg/ and 60 mg/28 days, respectively, were treated with antidiabetic medication at study entry, while 25% in each group initiated antidiabetic drugs during the study. Patients who received antidiabetic medications during PAS-LAR treatment had higher baseline mean FPG and HbA1c levels than patients who did not require treatment for diabetes. In detail, among patients with baseline FPG >100 mg/dL, 52 and 71% of those receiving PAS-LAR 40 or 60 mg respectively, developed hyperglycaemia during treatment (21). Overall these findings would suggest that baseline glucose status is a potential predictive factor for the development of hyperglycaemia during PAS-LAR treatment. Therefore, before starting PAS treatment, patients should undergo a glucose metabolism evaluation, and in case of glycaemic abnormalities, antidiabetic medication should be optimized before starting PAS therapy.
Response to PAS-LAR treatment does not seem to influence glucose homeostasis alterations, since the effect on HbA1c was similar for responders and non-responders in the PAOLA study (21). Interestingly, in the same study, PAS-associated elevations in glucose levels generally plateaued after ~2–3 months of treatment, as already reported. The hyperglycaemic effect of PAS can be explained by its binding affinity to SSTR. Indeed, glucagon is produced by cells expressing SSTR2, while insulin is produced by cells that also express SSTR5. Due to the high binding affinity to SSTR5, PAS suppresses insulin secretion, while it does not induce an effective inhibition on glucagon secretion. Furthermore, PAS appears to reduce glucagon-like peptide 1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) levels, while leaving insulin sensitivity unaffected (44). Vildagliptin and liraglutide were the most effective drugs in minimizing PAS-related glucose alterations in healthy volunteers, confirming the existence of an anomalous incretin response (46).
However, available data on PAS treatment overall suggests a generally reversible hyperglycaemic effect which requires active monitoring and is manageable with an appropriate therapeutic strategy involving available antidiabetics agents. On the other hand, the adverse metabolic effects of PAS can impact negatively on the cost-effectiveness of this treatment when compared with PEG, considering the costs related to the management of hyperglycemia-related adverse events (64).
The effect of PAS on lipid profiles has been investigated by Chen et al. who studied pharmacokinetics and safety of PAS in 45 healthy Chinese male subjects (65), showing that PAS reduced serum cholesterol and triglyceride levels in a dose-dependent manner.
In this regard, it is worth of mentioning that lipid profile influences the visceral adiposity index (VAI) that is a marker of visceral fat dysfunction, indirectly reflecting cardiometabolic risk. In acromegaly, VAI seems to be strongly related to insulin resistance, adipose tissue dysfunction, and cardiometabolic risk, especially in post-menopausal women (66). Interestingly, some authors demonstrated that 1 year of PAS treatment had a positive effect on cardiometabolic risk in 16 patients with Cushing's disease (CD), despite the increase of diabetes mellitus prevalence (67). Indeed, PAS treatment improved anthropometric parameters, reduced the prevalence of dyslipidaemia, ameliorated the lipid profile, and significantly reduced VAI and adipose tissue dysfunction in CD patients (67). However, studies of acromegaly patients which address the impact of PAS treatment on lipid changes and adipose tissue dysfunction as factors influencing cardiometabolic risk, regardless the effects on glucose homeostasis, are needed.
In conclusion, acromegaly is associated with metabolic alterations, such as hyperglycaemia, dyslipidaemia, and systemic arterial hypertension, which in addition to cardiovascular changes play a critical role in increasing cardiovascular risk and mortality rate. Surgical or medical control of acromegaly, with SSA or pegvisomant, positively influences cardiovascular risk factors, metabolic alterations, and related mortality. Pasireotide-related beneficial effects in terms of biochemical and clinical disease control can be burdened by its diabetogenic effect, but can be adequately counteracted by a proper pharmacological strategy, while—in this context—studies on other cardiometabolic outcomes are still needed.
Author Contributions
SP, FF, MR, and FS reviewed the literature. SP, FF, and MR wrote the manuscript. SC revised the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Colao A, Ferone D, Marzullo P, Lombardi G. Systemic complications of acromegaly, epidemiology, pathogenesis, and management. Endocr Rev. (2004) 25:102–52. doi: 10.1210/er.2002-0022
2. Berg C, Petersenn S, Lahner H, Herrmann BL, Buchfelder M, Droste M, et al. Investigators, Cardiovascular risk factors in patients with uncontrolled and long-term acromegaly, comparison with matched data from the general population and the effect of disease control. J Clin Endocrinol Metab. (2010) 95:3648–56. doi: 10.1210/jc.2009-2570
3. Pivonello R, Auriemma RS, Grasso LF, Pivonello C, Simeoli C, Patalano R, et al. Complications of acromegaly, cardiovascular, respiratory and metabolic comorbidities. Pituitary. (2017) 20:46–62. doi: 10.1007/s11102-017-0797-7
4. Kamenicky P, Blanchard A, Frank M, Salenave S, Letierce A, Azizi M, et al. Body fluid expansion in acromegaly is related to enhanced epithelial sodium channel (ENaC) activity. J Clin Endocrinol Metab. (2011) 96:2127–35. doi: 10.1210/jc.2011-0078
5. Mosca S, Paolillo S, Colao A, Bossone E, Cittadini A, Iudice FL, et al. Cardiovascular involvement in patients affected by acromegaly, an appraisal. Int J Cardiol. (2013) 167:1712–8. doi: 10.1016/j.ijcard.2012.11.109
6. Puglisi S, Terzolo M. Hypertension and acromegaly. Endocrinol Metab Clin North Am. (2019) 48:779–93. doi: 10.1016/j.ecl.2019.08.008
7. Holdaway IM, Rajasoorya RC, Gamble GD. Factors influencing mortality in acromegaly. J Clin Endocrinol Metab. (2004) 89:667–74. doi: 10.1210/jc.2003-031199
8. Colao A, Pivonello R, Grasso L F, Auriemma R S, Galdiero M, Savastano S, et al. Determinants of cardiac disease in newly diagnosed patients with acromegaly, results of a 10 year survey study. Eur J Endocrinol. (2011) 165:713–21. doi: 10.1530/EJE-11-0408
9. Colao A, Spiezia S, Cerbone G, Pivonello R, Marzullo P, Ferone D, et al. Increased arterial intima-media thickness by B-M mode echodoppler ultrasonography in acromegaly. Clin Endocrinol. (2001) 54:515–24. doi: 10.1046/j.1365-2265.2001.01256.x
10. Paisley AN, Banerjee M, Rezai M, Schofield RE, Balakrishnannair S, Herbert A, et al. Changes in arterial stiffness but not carotid intimal thickness in acromegaly. J Clin Endocrinol Metab. (2011) 96:1486–92. doi: 10.1210/jc.2010-2225
11. Akutsu H, Kreutzer J, Wasmeier G, Ropers D, Rost C, Möhlig M, et al. Acromegaly per se does not increase the risk for coronary artery disease. Eur J Endocrinol. (2010) 162:879–86. doi: 10.1530/EJE-09-0945
12. Cannavo S, Almoto B, Cavalli G, Squadrito S, Romanello G, Vigo MT, et al. Acromegaly and coronary disease, an integrated evaluation of conventional coronary risk factors and coronary calcifications detected by computed tomography. J Clin Endocrinol Metab. (2006) 91:3766–72. doi: 10.1210/jc.2005-2857
13. Ragonese M, Alibrandi A, Di Bella G, Salamone I, Puglisi S, Cotta OR, et al. Cardiovascular events in acromegaly, distinct role of Agatston and Framingham score in the 5-year prediction. Endocrine. (2014) 47:206–12. doi: 10.1007/s12020-013-0115-8
14. Ferraù F, Albani A, Ciresi A, Giordano C, Cannavò S. Diabetes secondary to acromegaly, physiopathology, clinical features and effects of treatment. Front Endocrinol. (2018) 9:358. doi: 10.3389/fendo.2018.00358
15. Arosio M, Reimondo G, Malchiodi E, Berchialla P, Borraccino A, De Marinis L, et al. Acromegaly, predictors of morbidity and mortality in acromegaly, an Italian survey. Eur J Endocrinol. (2012) 167:189–98. doi: 10.1530/EJE-12-0084
16. Fieffe S, Morange I, Petrossians P, Chanson P, Rohmer V, Cortet C, et al. Diabetes in acromegaly, prevalence, risk factors, and evolution, data from the French acromegaly registry. Eur J Endocrinol. (2011) 164:877–84. doi: 10.1530/EJE-10-1050
17. Wen-Ko C, Szu-Tah C, Feng-Hsuan L, Chen-Nen C, Ming-Hsu W, Jen-Der L. The impact of diabetes mellitus on the survival of patients with acromegaly. Endokrynol Pol. (2016) 67:501–6. doi: 10.5603/EP.a2016.0031
18. Davì MV, Giustina A. Sleep apnea in acromegaly, a review on prevalence, pathogenetic aspects and treatment. Expert Rev Endocrinol Metab. (2012) 7:55–62. doi: 10.1586/eem.11.82
19. Katznelson L, Laws ER, Melmed S, Molitch ME, Murad MH, Utz A, et al. Acromegaly, an endocrine society clinical practice guideline. J Clin Endocrinol Metab. (2014) 99:3933–51. doi: 10.1210/jc.2014-2700
20. Carmichael JD, Bonert VS, Nuño M, Ly D, Melmed S. Acromegaly clinical trial methodology impact on reported biochemical efficacy rates of somatostatin receptor ligand treatments, a meta-analysis. J Clin Endocrinol Metab. (2014) 99:1825–33. doi: 10.1210/jc.2013-3757
21. Gadelha MR, Bronstein MD, Brue T, Coculescu M, Fleseriu M, Guitelman M, et al. Pasireotide versus continued treatment with octreotide or lanreotide in patients with inadequately controlled acromegaly (PAOLA), a randomised, phase 3 trial. Lancet Diabetes Endocrinol. (2014) 2:875–84. doi: 10.1016/S2213-8587(14)70169-X
22. Trainer PJ, Drake WM, Katznelson L, Freda PU, Herman-Bonert V, van der Lely AJ, et al. Treatment of acromegaly with the growth hormone-receptor antagonist pegvisomant. N Engl J Med. (2000) 342:1171–7. doi: 10.1056/NEJM200004203421604
23. van der Lely J, Hutson RK, Trainer PJ, Besser GM, Barkan AL, Katznelson L, et al. Long-term treatment of acromegaly with pegvisomant, a growth hormone receptor antagonist. Lancet. (2001) 358:1754–9. doi: 10.1016/S0140-6736(01)06844-1
24. Ragonese M, Grottoli S, Maffei P, Alibrandi A, Ambrosio MR, Arnaldi G, et al. How to improve effectiveness of pegvisomant treatment in acromegalic patients. J Endocrinol Invest. (2018) 41:575–81. doi: 10.1007/s40618-017-0773-0
25. Grottoli S, Maffei P, Bogazzi F, Cannavò S, Colao A, Ghigo E, et al. ACROSTUDY, the Italian experience. Endocrine. (2015) 48:334–41. doi: 10.1007/s12020-014-0393-9
26. Holdaway IM, Bolland MJ, Gamble GD. A meta-analysis of the effect of lowering serum levels of GH and IGF-I on mortality in acromegaly. Eur J Endocrinol. (2008) 159:89–95. doi: 10.1530/EJE-08-0267
27. Mercado M, Gonzalez B, Vargas G, Ramirez C, de los Monteros AL, Sosa E, et al. Successful mortality reduction and control of comorbidities in patients with acromegaly followed at a highly specialized multidisciplinary clinic. J Clin Endocrinol Metab. (2014) 99:4438–46. doi: 10.1210/jc.2014-2670
28. Postma MR, Wolters TLC, van den Berg G, van Herwaarden AE, Muller Kobold AC, Sluiter WJ, et al. Postoperative use of somatostatin analogs and mortality in patients with acromegaly. Eur J Endocrinol. (2019) 180:1–9. doi: 10.1530/EJE-18-0166
29. Ritvonen E, Löyttyniemi E, Jaatinen P, Ebeling T, Moilanen L, Nuutila P, et al. Mortality in acromegaly, a 20-year follow-up study. Endocr Relat Cancer. (2016) 23:469–80. doi: 10.1530/ERC-16-0106
30. Jayasena CN, Comninos AN, Clarke H, Donaldson M, Meeran K, Dhillo WS. The effects of long-term growth hormone and insulin-like growth factor-1 exposure on the development of cardiovascular, cerebrovascular and metabolic co-morbidities in treated patients with acromegaly. Clin Endocrinol. (2011) 75:220–5. doi: 10.1111/j.1365-2265.2011.04019.x
31. Varadhan L, Reulen RC, Brown M, Clayton RN. The role of cumulative growth hormone exposure in determining mortality and morbidity in acromegaly, a single centre study. Pituitary. (2016) 19:251–61. doi: 10.1007/s11102-015-0700-3
32. Sardella C, Cappellani D, Urbani C, Manetti L, Marconcini G, Tomisti L, et al. Disease activity and lifestyle influence comorbidities and cardiovascular events in patients with acromegaly. Eur J Endocrinol. (2016) 175:443–53. doi: 10.1530/EJE-16-0562
33. De Marinis L, Bianchi A, Mazziotti G, Mettimano M, Milardi D, Fusco A, et al. The long-term cardiovascular outcome of different GH-lowering treatments in acromegaly. Pituitary. (2008) 11:13–20. doi: 10.1007/s11102-007-0062-6
34. Colao A, Pivonello R, Galderisi M, Cappabianca P, Auriemma RS, Galdiero M, et al. Impact of treating acromegaly first with surgery or somatostatin analogs on cardiomyopathy. J Clin Endocrinol Metab. (2008) 93:2639–46. doi: 10.1210/jc.2008-0299
35. Colao A, Auriemma RS, Galdiero M, Lombardi G, Pivonello R. Effects of initial therapy for five years with somatostatin analogs for acromegaly on growth hormone and insulin-like growth factor-I levels, tumor shrinkage, and cardiovascular disease, a prospective study. J Clin Endocrinol Metab. (2009) 94:3746–56. doi: 10.1210/jc.2009-0941
36. Kuhn E, Maione L, Bouchachi A, Rozière M, Salenave S, Brailly-Tabard S, et al. Long-term effects of pegvisomant on comorbidities in patients with acromegaly, a retrospective single-center study. Eur J Endocrinol. (2015) 173:693–702. doi: 10.1530/EJE-15-0500
37. Carmichael JD, Broder MS, Cherepanov D, Chang E, Mamelak A, Said Q, et al. Long-term treatment outcomes of acromegaly patients presenting biochemically-uncontrolled at a tertiary pituitary center. BMC Endocr Disord. (2017) 17:49. doi: 10.1186/s12902-017-0199-x
38. Colao A, Terzolo M, Bondanelli M, Galderisi M, Vitale G, Reimondo G, et al. GH and IGF-I excess control contributes to blood pressure control, results of an observational, retrospective, multicentre study in 105 hypertensive acromegalic patients on hypertensive treatment. Clin Endocrinol. (2008) 69:613–20. doi: 10.1111/j.1365-2265.2008.03258.x
39. González B, Vargas G, de Los Monteros ALE, Mendoza V, Mercado M. Persistence of diabetes and hypertension after multimodal treatment of acromegaly. J Clin Endocrinol Metab. (2018) 103:2369–75. doi: 10.1210/jc.2018-00325
40. Jaffrain-Rea ML, Moroni C, Baldelli R, Battista C, Maffei P, Terzolo M, et al. Relationship between blood pressure and glucose tolerance in acromegaly. Clin Endocrinol. (2001) 54:189–95. doi: 10.1046/j.1365-2265.2001.01206.x
41. He W, Yan L, Wang M, Li Q, He M, Ma Z, et al. Surgical outcomes and predictors of glucose metabolism alterations for growth hormone-secreting pituitary adenomas, a hospital-based study of 151 cases. Endocrine. (2019) 63:27–35. doi: 10.1007/s12020-018-1745-7
42. Mazziotti G, Floriani I, Bonadonna S, Torri V, Chanson P, Giustina A. Effects of somatostatin analogs on glucose homeostasis, a metaanalysis of acromegaly studies. J Clin Endocrinol Metab. (2009) 94:1500–8. doi: 10.1210/jc.2008-2332
43. Ghigo E, Biller BM, Colao A, Kourides IA, Rajicic N, Hutson RK, et al. Comparison of pegvisomant and long-acting octreotide in patients with acromegaly naïve to radiation and medical therapy. J Endocrinol Invest. (2009) 32:924–33. doi: 10.1007/BF03345774
44. Henry RR, Ciaraldi TP, Armstrong D, Burke P, Ligueros-Saylan M, Mudaliar S. Hyperglycemia associated with pasireotide, results from a mechanistic study in healthy volunteers. J Clin Endocrinol Metab. (2013) 98:3446–53. doi: 10.1210/jc.2013-1771
45. Colao A, Bronstein M D, Freda P, Gu F, Shen CC, Gadelha M, et al. Pasireotide versus octreotide in acromegaly, a head-to-head superiority study. J Clin Endocrinol Metab. (2014) 99:791–9. doi: 10.1210/jc.2013-2480
46. Breitschaft A, Hu K, Hermosillo Resendiz K, Darstein C, Golor G. Management of hyperglycemia associated with pasireotide (SOM230), healthy volunteer study. Diabetes Res Clin Pract. (2014) 103:458–65. doi: 10.1016/j.diabres.2013.12.011
47. Bronstein M D, Fleseriu M, Neggers S, Colao A, Sheppard M, Gu F, et al. Switching patients with acromegaly from octreotide to pasireotide improves biochemical control, crossover extension to a randomized, double-blind, Phase III study. BMC Endocr Disord. (2016) 16:16. doi: 10.1186/s12902-016-0096-8
48. Fleseriu M, Rusch E, Geer EB, Investigators AS. Safety and tolerability of pasireotide long-acting release in acromegaly-results from the acromegaly, open-label, multicenter, safety monitoring program for treating patients who have a need to receive medical therapy (ACCESS) study. Endocrine. (2017) 55:247–55. doi: 10.1007/s12020-016-1182-4
49. Cozzolino A, Feola T, Simonelli I, Puliani G, Pozza C, Giannetta E, et al. Somatostatin analogs and glucose metabolism in acromegaly, a meta-analysis of prospective interventional studies. J Clin Endocrinol Metab. (2018) 103:2189–2099. doi: 10.1210/jc.2017-02566
50. Shimon I, Adnan Z, Gorshtein A, Baraf L, Saba Khazen N, Gershinsky M, et al. Efficacy and safety of long-acting pasireotide in patients with somatostatin-resistant acromegaly, a multicenter study. Endocrine. (2018) 62:448–55. doi: 10.1007/s12020-018-1690-5
51. Muhammad A, van der Lely AJ, Delhanty PJD, Dallenga AHG, Haitsma IK, Janssen J, et al. Efficacy and safety of switching to pasireotide in patients with acromegaly controlled with pegvisomant and first-generation somatostatin analogues (PAPE Study). J Clin Endocrinol Metab. (2018) 103:586–95. doi: 10.1210/jc.2017-02017
52. Lindberg-Larsen R, Møller N, Schmitz O, Nielsen S, Andersen M, Orskov H, Jørgensen JO. The impact of pegvisomant treatment on substrate metabolism and insulin sensitivity in patients with acromegaly. J Clin Endocrinol Metab. (2007) 92:1724–8. doi: 10.1210/jc.2006-2276
53. Rose DR, Clemmons DR. Growth hormone receptor antagonist improves insulin resistance in acromegaly. Growth Horm IGF Res. (2002) 12:418–24. doi: 10.1016/S1096-6374(02)00083-7
54. Giordano C, Ciresi A, Amato MC, Pivonello R, Auriemma RS, Grasso LF, et al. Clinical and metabolic effects of first-line treatment with somatostatin analogues or surgery in acromegaly, a retrospective and comparative study. Pituitary. (2012) 15:539–51. doi: 10.1007/s11102-011-0365-5
55. Reyes-Vidal C, Fernandez JC, Bruce JN, Crisman C, Conwell IM, Kostadinov J, et al. Prospective study of surgical treatment of acromegaly, effects on ghrelin, weight, adiposity, and markers of CV risk. J Clin Endocrinol Metab. (2014) 99:4124–32. doi: 10.1210/jc.2014-2259
56. Caron PJ, Petersenn S, Houchard A, Sert C, Bevan JS, Group PS. Glucose and lipid levels with lanreotide autogel 120 mg in treatment-naïve patients with acromegaly, data from the PRIMARYS study. Clin Endocrinol. (2017) 86:541–51. doi: 10.1111/cen.13285
57. Herrmann BL, Wessendorf TE, Ajaj W, Kahlke S, Teschler H, Mann K. Effects of octreotide on sleep apnoea and tongue volume (magnetic resonance imaging) in patients with acromegaly. Eur J Endocrinol. (2004) 151:309–15. doi: 10.1530/eje.0.1510309
58. Grunstein RR, Ho KK, Sullivan CE. Effect of octreotide, a somatostatin analog, on sleep apnea in patients with acromegaly. Ann Intern Med. (1994) 121:478–83. doi: 10.7326/0003-4819-121-7-199410010-00002
59. Annamalai AK, Webb A, Kandasamy N, Elkhawad M, Moir S, Khan F, et al. A comprehensive study of clinical, biochemical, radiological, vascular, cardiac, and sleep parameters in an unselected cohort of patients with acromegaly undergoing presurgical somatostatin receptor ligand therapy. J Clin Endocrinol Metab. (2013) 98:1040–50. doi: 10.1210/jc.2012-3072
60. Colao A, Grasso LFS, Giustina A, Melmed S, Chanson P, Pereira AM, et al. Acromegaly. Nat Rev Dis Primers. (2019) 5:20. doi: 10.1038/s41572-019-0071-6
61. Gatto F, Arvigo M, Amaru J, Campana C, Cocchiara F, Graziani G, et al. Cell specific interaction of pasireotide, review of preclinical studies in somatotroph and corticotroph pituitary cells. Pituitary. (2019) 22:89–99. doi: 10.1007/s11102-018-0926-y
62. Sheppard M, Bronstein MD, Freda P, Serri O, De Marinis L, Naves L, et al. Pasireotide LAR maintains inhibition of GH and IGF-1 in patients with acromegaly for up to 25 months, results from the blinded extension phase of a randomized, double-blind, multicenter, Phase III study. Pituitary. (2015) 18:385–94. doi: 10.1007/s11102-014-0585-6
63. Silverstein JM. Hyperglycemia induced by pasireotide in patients with Cushing's disease or acromegaly. Pituitary. (2016) 19:536–43. doi: 10.1007/s11102-016-0734-1
64. Peral C, Cordido F, Gimeno-Ballester V, Mir N, Sanchez-Cenizo L, Rubio-Rodriguez D, et al. Cost-effectiveness analysis of second-line pharmacological treatment of acromegaly in Spain. Expert Rev Pharmacoecon Outcomes Res. (2019) 6:1–10. doi: 10.1080/14737167.2019.1610396
65. Chen X, Shen G, Jiang J, Liu H, Hu K, Darstein C, et al. Pharmacokinetics and safety of subcutaneous pasireotide and intramuscular pasireotide long-acting release in Chinese male healthy volunteers, a phase I, single-center, open-label, randomized study. Clin Ther. (2014) 36:1196–210. doi: 10.1016/j.clinthera.2014.06.006
66. Ciresi A, Amato MC, Pivonello R, Nazzari E, Grasso LF, Minuto F, et al. The metabolic profile in active acromegaly is gender-specific. J Clin Endocrinol Metab. (2013) 98:E51–9. doi: 10.1210/jc.2012-2896
Keywords: pasireotide, acromegaly, GH-secreting pituitary tumor, acromegaly treatment, cardiometabolic risk
Citation: Puglisi S, Ferraù F, Ragonese M, Spagnolo F and Cannavò S (2020) Cardiometabolic Risk in Acromegaly: A Review With a Focus on Pasireotide. Front. Endocrinol. 11:28. doi: 10.3389/fendo.2020.00028
Received: 15 September 2019; Accepted: 14 January 2020;
Published: 06 February 2020.
Edited by:
Marek Bolanowski, Wroclaw Medical University, PolandReviewed by:
Roberto Salvatori, Johns Hopkins University, United StatesLuiz Eduardo Armondi Wildemberg, Instituto Estadual do Cérebro Paulo Niemeyer, Brazil
Copyright © 2020 Puglisi, Ferraù, Ragonese, Spagnolo and Cannavò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesco Ferraù, francesco.ferrau1@gmail.com; fferrau@unime.it