 Hanna Riekki1†
Hanna Riekki1† Linnea Aitokari1,2†
Linnea Aitokari1,2† Laura Kivelä1,2,3
Laura Kivelä1,2,3 Siiri Lahti1Pauliina Hiltunen4
Siiri Lahti1Pauliina Hiltunen4 Nina Vuorela1,4Heini Huhtala5Timo A. Lakka6,7,8
Nina Vuorela1,4Heini Huhtala5Timo A. Lakka6,7,8 Kalle Kurppa1,2,4,9*
Kalle Kurppa1,2,4,9*- 1Tampere Center for Child, Adolescent and Maternal Health Research, Tampere University, Tampere, Finland
- 2Celiac Disease Research Center, Tampere University, Tampere, Finland
- 3Children’s Hospital and Pediatric Research Center, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
- 4Department of Pediatrics, Tampere University Hospital, Tampere, Finland
- 5Faculty of Social Sciences, Tampere University, Tampere, Finland
- 6Institute of Biomedicine, School of Medicine, University of Eastern Finland, Kuopio, Finland
- 7Department of Clinical Physiology and Nuclear Medicine, Kuopio University Hospital, Kuopio, Finland
- 8Kuopio Research Institute of Exercise Medicine, Kuopio, Finland
- 9University Consortium of Seinäjoki, Seinäjoki, Finland
Introduction: Data on the prevalence of pediatric fatty liver disease remain limited, partly due to challenges in diagnosis. A novel concept of metabolic-associated fatty liver disease (MAFLD) makes it possible to establish the diagnosis in overweight children with sufficiently elevated alanine aminotransferase (ALT). We investigated the prevalence, risk factors, and metabolic co-morbidities of MAFLD in a large group of overweight children.
Methods: Data on 703 patients aged 2-16 years examined due to overweight in different levels of healthcare in 2002-2020 were collected retrospectively from patient records. MAFLD was here defined as ALT >2x reference (>44 U/l in girls and >50 U/l in boys) in overweight children according to recently updated definition. Patients with MAFLD and without it were compared, and subgroup analyses were conducted among boys and girls.
Results: Median age was 11.5 years, and 43% were girls. Altogether 11% were overweight, 42% obese and 47% severely obese. Abnormal glucose metabolism was present in 44%, dyslipidemia in 51%, hypertension in 48% and type 2 diabetes (T2D) in 2%. MAFLD prevalence varied between 14-20% in examined years without significant change (p=0.878). The pooled prevalence over the years was 15% (boys 18%, girls 11%; p=0.018), peaking in girls at early puberty and increasing in boys with age and puberty. Associated factors in boys were T2D (OR 7.55, 95% CI 1.23-46.2), postpubertal stage (5.39, 2.26-12.8), increased fasting insulin (3.20, 1.44-7.10), hypertriglyceridemia (2.97, 1.67-5.30), hyperglycemia (2.88, 1.64-5.07), decreased high-density lipoprotein (HDL) cholesterol (2.16, 1.18-3.99), older age (1.28, 1.15-1.42) and higher body-mass-index (1.01, 1.05-1.15), and in girls T2D (18.1, 3.16-103), hypertriglyceridemia (4.28, 1.99-9.21), and decreased HDL (4.06, 1.87-8.79).
Conclusion: Prevalence of MAFLD was 15%, with no statistically significant increase in the 2000s. The condition was associated in general with male gender, puberty stage and disturbances in glucose and lipid metabolism, and higher age and BMI in boys.
1 Introduction
Obesity-associated nonalcoholic fatty liver disease (NAFLD) is currently considered to be the most common chronic liver disease in children and adolescents (1–3). However, data on the actual prevalence remain scarce, primarily due to a lack of accurate or practical imaging tools and restricted applicability of liver biopsy in this age group (4). Determining the precise prevalence figures would enable better targeting of lifestyle interventions and limited healthcare resources (5). This issue is particularly important in pediatric patients, who often present with a rapidly progressing condition and may derive great benefit from early treatment (6, 7). Moreover, untreated NAFLD may be an independent risk factor for metabolic and cardiovascular comorbidities (7–10), although actual evidence is again scant.
The soaring prevalence of overweight in children and recognition of the importance of metabolic dysfunction as a contributory factor calls for more biologically meaningful and simplified diagnostics for NAFLD. The recently introduced concept of metabolic-associated fatty liver disease (MAFLD) defines the condition as increased liver adiposity together with the presence of metabolic abnormalities and/or obesity. It is a promising non-invasive diagnostic approach in children, as the presence liver steatosis can be identified based solely on laboratory evidence (11–13). Moreover, the co-existence of another hepatic condition is possible without exhaustive differential diagnostics necessary for the NALFD diagnosis (11, 14). MAFLD might thus offer a more unbiased means to study the prevalence and patient-related risk factors for fatty liver disease, and also to estimate a possible increase of the condition concurrently with overweight and obesity (11, 15).
We aimed to investigate the prevalence, risk factors, and metabolic co-morbidities of MAFLD in a large and well-defined group of overweight children and adolescents examined in different levels of healthcare.
2 Materials and methods
2.1 Patients and study design
The retrospective cross-sectional study was carried out at Tampere University and Tampere University Hospital. It comprised 1,000 consecutive patients aged 2-16 years who had received an obesity-related ICD 10 diagnosis code E65, E66.0-9 or R63.5 either at the primary care unit of the City of Tampere in 2006-2020 or at Tampere University Hospital in 2002-2020. Their comprehensive medical data was collected retrospectively from systematically maintained patient records. The clinical findings and laboratory data was collected at the time of the first obesity-related investigations in healthcare. Children and adolescents with insufficient data or lacking an alanine aminotransferase (ALT) value and those not deemed overweight after re-evaluation of the anthropometric measurements were excluded. Additionally, altogether 0.17% of the study children had a possibly hepatotoxic medication or a liver-affecting co-morbidity and were consequently excluded for simplicity, leaving 703 participants for the final analyses (Supplementary Figure 1).
The study design and collection of patient register data were approved by the City of Tampere Healthcare Services and by Tampere University Hospital according to the national ethical and data processing recommendations. None of the participants were contacted by the research group during the study. The Declaration of Helsinki was strictly followed in all stages.
2.2 Data collection and definitions
Age, sex, body mass index (BMI, body weight kg/body height m2), waist circumference and puberty stage, blood pressure, presence of acanthosis nigricans and relevant chronic diseases and medications, and use of possibly liver-affecting supplements, herbal products, alcohol, or illicit drugs were recorded at the time of the first obesity-related visit to healthcare.
Severity of overweight was categorized using BMI (kg/m2) and BMI Z-scores or weight-to-height percentages (WH%) as recommended by the International Obesity Task Force expert panel (16). Cutoff values for BMI Z-scores were >1.16 for overweight, >2.11 for obesity, and >2.76 for severe obesity in girls and >0.78, >1.70, and >2.36 in boys. These correspond to BMI values of >25 kg/m2, >30 kg/m2 and >35 kg/m2 at the age of ≥18 years (16, 17). The equivalent values for WH% were 10-20% for overweight, 20-40% for obesity, and >40% for severe obesity in those <7 years, and respectively 20-40%, 40-60%, and >60% in older participants (16, 17). Abnormal waist circumference was defined as >90th percentile for age and sex (18) and hypertension as systolic or diastolic blood pressure >95th percentile (19). Pubertal status was classified by a trained clinician based on Tanner staging as pre-pubertal (stage 1), pubertal (stages 2-4) and postpubertal (stage 5) (20, 21).
The following fasting plasma laboratory values were collected as available: ALT, glucose (reference value <5.6 mmol/l), insulin (prepubertal ≤15 mU/l, pubertal ≤30 mU/l and postpubertal ≤20 mU/l), HOMA-IR (<2.67 for prepubertal and <5.22 for pubertal boys and <2.22 for prepubertal and <3.82 for pubertal girls), total cholesterol (<5.18 mmol/l), high-density lipoprotein (HDL) cholesterol (≥1.04 mmol/l), low-density lipoprotein (LDL) cholesterol (<3.36 mmol/l) and triglycerides (<1.13 before and <1.47 mmol/l after the age of 10 years) (22, 23).
Impaired glucose metabolism was based on a two-hour plasma glucose of 7.8-11.0 mmol/l from a two-hour oral glucose tolerance test (OGTT) or impaired fasting glucose of 5.6-6.9 mmol/L, and type 2 diabetes on a fasting plasma glucose of >6.9 mmol/l or a two-hour plasma glucose of >11.0 mmol/l, as recommended by the American Diabetes Association (24). If OGTT was not available only a fasting glucose value was used.
ALT upper limit of normal (ULN) values of 22 U/l for girls and 25 U/l for boys was applied according to the National Health and Nutrition Examination Survey (NHANES) results and the North American Society of Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) guidelines (4, 25). In addition, an ALT cut-off of 80 U/l was tested separately due to a previously reported increased risk of advanced liver disease (4, 26). MALFD was defined as ALT twice ULN (>44 U/l for girls and >50 U/l for boys) in overweight or obese children (11).
2.3 Statistical analyses
Categorical variables are reported as numbers and percentages. Normality of continuous variables were tested with Q-Q Plot and with Kolmogorov-Smirnov and Shapiro-Wilk tests, and were found to be markedly skewed. Therefore, they were reported as medians with lower (Q1) and upper (Q3) quartiles or with ranges and tested with nonparametric tests. Children with and without MAFLD were compared by Mann-Whitney or Kruskal-Wallis test for continuous variables and by Chi-square or Fisher’s exact test for categorical variables in unadjusted comparisons. Due to the observed differences in age and sex between the two groups, the results were also adjusted by these variables by using binary logistic regression. The risk of having MAFLD according to the characteristics of participants were analyzed separately for boys and girls by using unadjusted logistic regression models and models adjusted for age. The results are reported as odds ratios (OR) with 95% confidence intervals (CI). The prevalence of MAFLD, increased ALT and obesity in children having their first healthcare visit in different timepoints was compared with Chi-square test. Statistical significance was defined as P value <0.05. All analyses were performed using SPSS version 25.0 (Armonk, NY: IBM Corp).
3 Results
The median age of the 703 children was 11.5 (range 2.2-16.7) years, 43.0% were girls and 91.0% had Finnish ethnicity. Altogether 10.8% were overweight, 89.2% obese and 46.8% severely obese, and 99.1% had central obesity (Supplementary Table). Moreover, 48.4% had hypertension, 29.2% fasting hypertriglyceridemia, 18.2% increased total cholesterol, 20.3% increased LDL cholesterol, 26.0% decreased HDL cholesterol, 81.4% increased HOMA-IR, 41.1% increased fasting insulin, and 35.6% impaired glucose metabolism. Altogether 27.6% had no metabolic abnormalities. Eleven (1.7%) participants fulfilled the criteria for T2D. None of the children or adolescents reported excessive use of supplements or herbal products. Two participants reported occasional alcohol use and in neither of these was the cumulative dose considered hepatotoxic. None were diagnosed with viral hepatitis.
Altogether 51.1% of the children and adolescents presented with increased ALT and 5.0% with ALT >80 U/l. The pooled prevalence of MAFLD over the years was 17.7% in boys, 11.3% in girls and 14.9% in both together. The prevalence increased linearly with age and pubertal stage in boys, whereas in girls it peaked at the age 10-12 years and during early puberty (Figure 1). There were no significant changes in the prevalence of obesity, increased ALT or MAFLD during the study period. Prevalence of obesity remained stable over time being 88.4% in 2005-7, 86.3% in 2008-10, 88.8% in 2011-13, 91.5% in 2014-16 and 89.3% in 2017-2020. The corresponding prevalences of increased ALT were 53.7%, 48.7%, 48.4%, 52.5% and 55.4%, respectively, and that of MAFLD 15.8%, 14.5%, 14.0%, 15.6% and 19.6%, respectively (Figure 2).
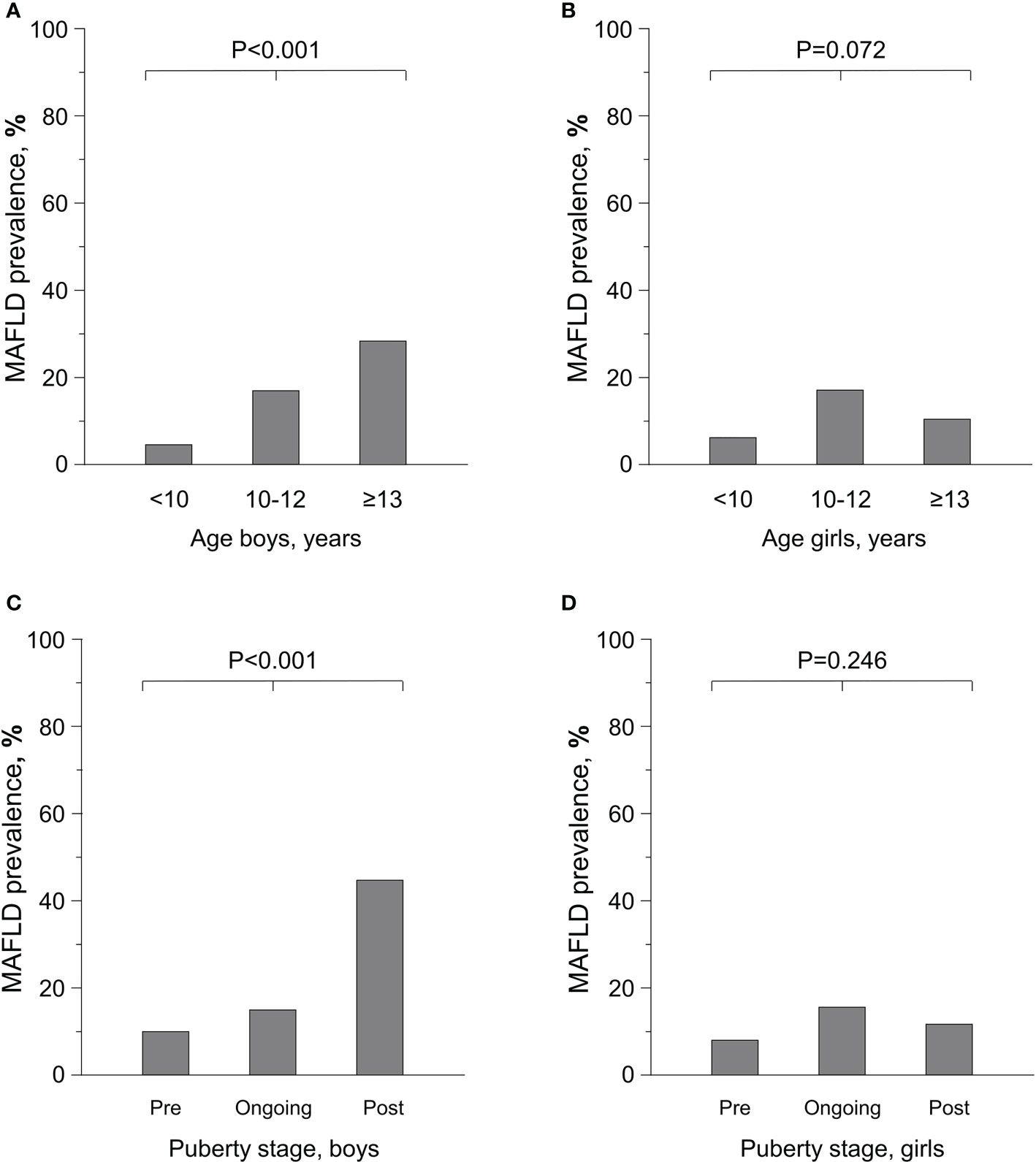
Figure 1 Prevalence of Metabolic-Associated Fatty Liver Disease (MAFLD) depending on age (A, B) and pubertal stage (C,D) in overweight and obese boys (N=401) and girls (N=302).
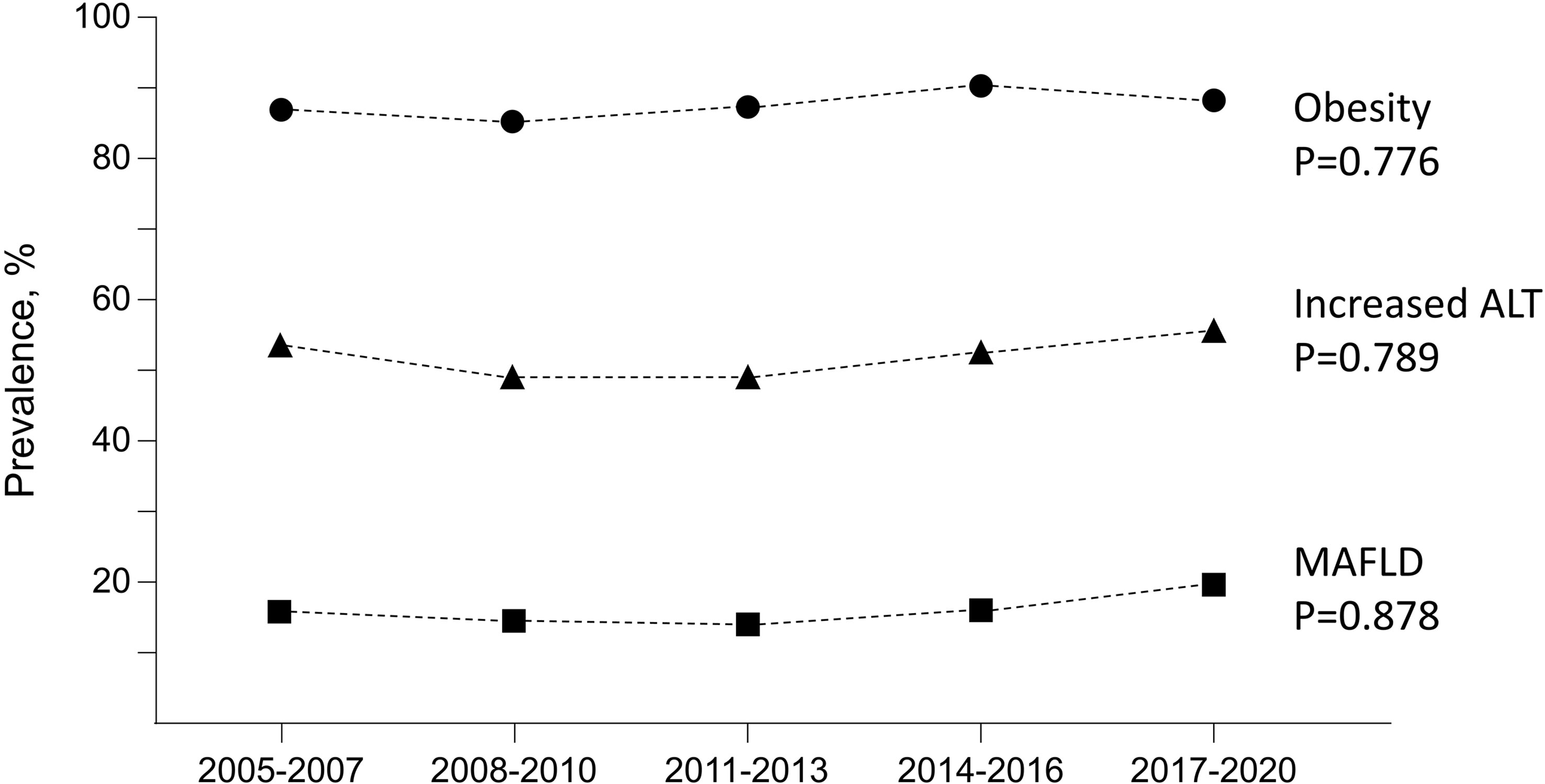
Figure 2 Changes over time in the prevalence of obesity, increased alanine aminotransferase (ALT, reference >22 U/l for girls and 25 U/l for boys) and Metabolic-Associated Fatty Liver Disease (MAFLD) in 659 overweight or obese children and adolescents. Changes in the sex distribution (p=0.771), median ages (p=0.292), median body mass index Z scores (p=0.132) or weight-to-height percentages (p=0.662) during the same period were not significant.
Children with MAFLD were older (median 12.8 vs. 11.3 years, p<0.001) and more likely boys (67.6% vs. 55.2%, p=0.018) and had higher median ALT values (68 U/l vs. 22 U/l, p<0.001) compared to those without MAFLD, while there was no difference in median BMI Z-scores (2.4 vs. 2.5, p=0.506) (Supplementary Table). In addition, they were more likely to have fasting hypertriglyceridemia, low HDL cholesterol, elevated insulin, impaired glucose metabolism, acanthosis nigricans, and T2D, whereas there was no significant difference in the prevalence of obesity or severe obesity, hypertension or other lipid parameters (Figure 3; Supplementary Table). Overall, children with MAFLD were more likely to have at least one significant cardiometabolic abnormality (hypertension, impaired glucose metabolism, insulin, HOMA-IR or triglycerides or decreased HDL) than did those without MAFLD (82.9% vs 70.6%, p=0.011). The risk of having MAFLD was highest in patients with multiple metabolic abnormalities (OR 1.58, 95% CI 1.34-1.85, p<0.001).
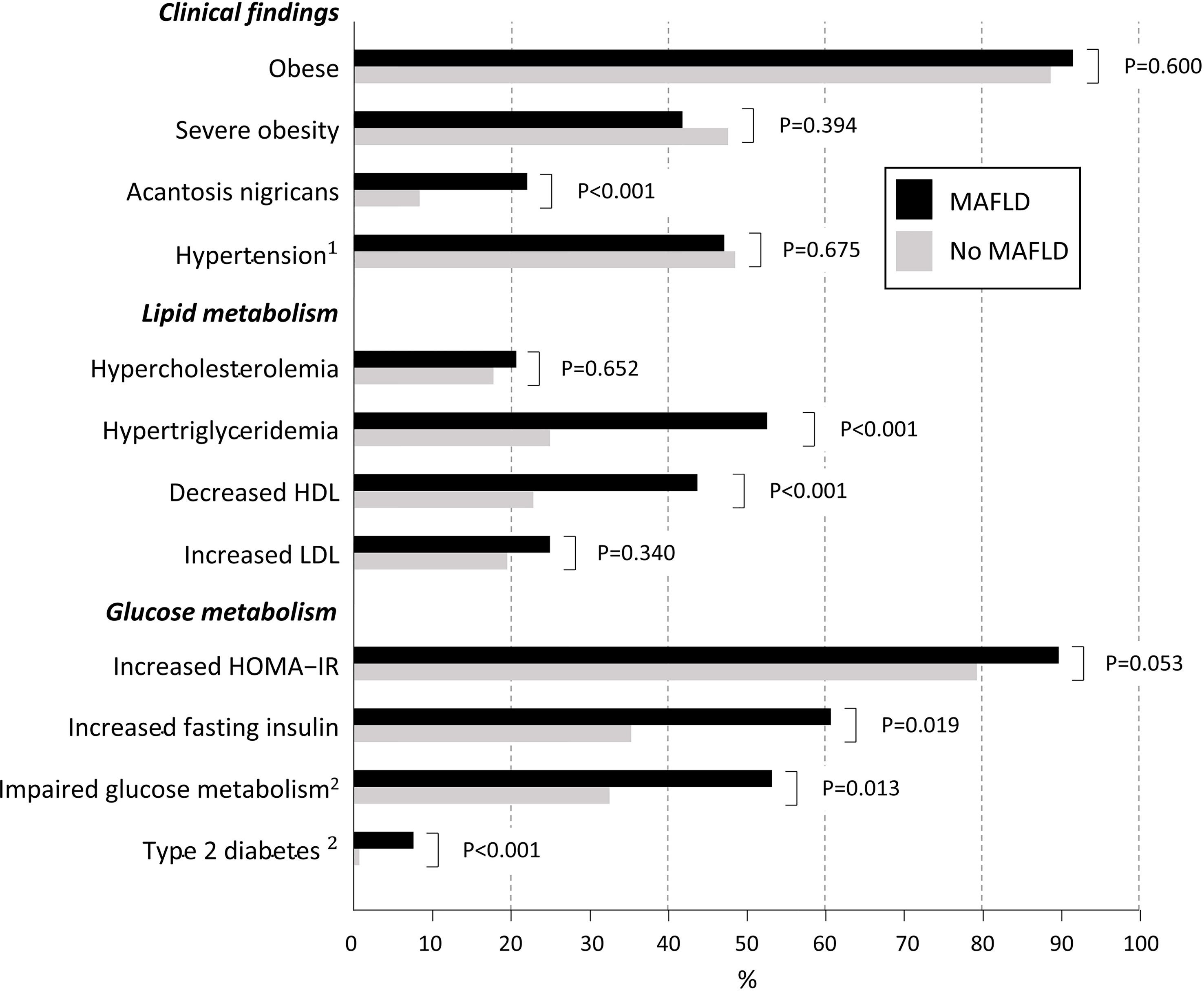
Figure 3 Characteristics of overweight children and adolescents with Metabolic-Associated Fatty Liver Disease (MALFD) (N=105) and without it (N=598). P-values are adjusted for age and sex based on the observed difference between MAFLD and non-MALFD groups in these variables. The following cut-offs for fasting laboratory values were used: total cholesterol ≥5.18 mmol/l; triglycerides ≥1.13 mmol/l (<10 years) and ≥1.47 mmol/l (≥10 years); HDL cholesterol <1.04 mmol/l; LDL cholesterol ≥3.36 mmol/l; HOMA-IR ≥2.67 for prepubertal and ≥5.22 for pubertal boys and ≥2.22 for prepubertal and ≥3.82 for pubertal girls; insulin prepubertal >15 mU/l, pubertal >30 mU/l and postpubertal >20 mU/l; glucose ≥5.6 mmol/l (22, 23). 1Blood pressure >95th percentile (19); 2Impaired glucose metabolism based on oral glucose tolerance test (OGTT) two-hour value 7.8-11.0 mmol/l or impaired fasting value 5.6-6.9 mmol/L; and type 2 diabetes on values >6.9 mmol/l or >11.0 mmol/l. If OGTT was not available only fasting glucose values were used (24). HDL, high-density lipoprotein cholesterol; HOMA-IR, Homeostatic Model Assessment of Insulin Resistance; LDL, low-density lipoprotein cholesterol.
Higher age and BMI, postpuberty, hypertriglyceridemia, decreased HDL cholesterol, hyperinsulinemia, impaired glucose metabolism, and T2D were significantly associated with MAFLD in boys in crude analysis, and hypertriglyceridemia, hyperinsulinemia and impaired glucose metabolism also after adjusting for age (Table 1). In girls, hypertriglyceridemia, decreased HDL cholesterol and T2D were associated with MAFLD both in crude analysis and after adjusting for age (Table 2).
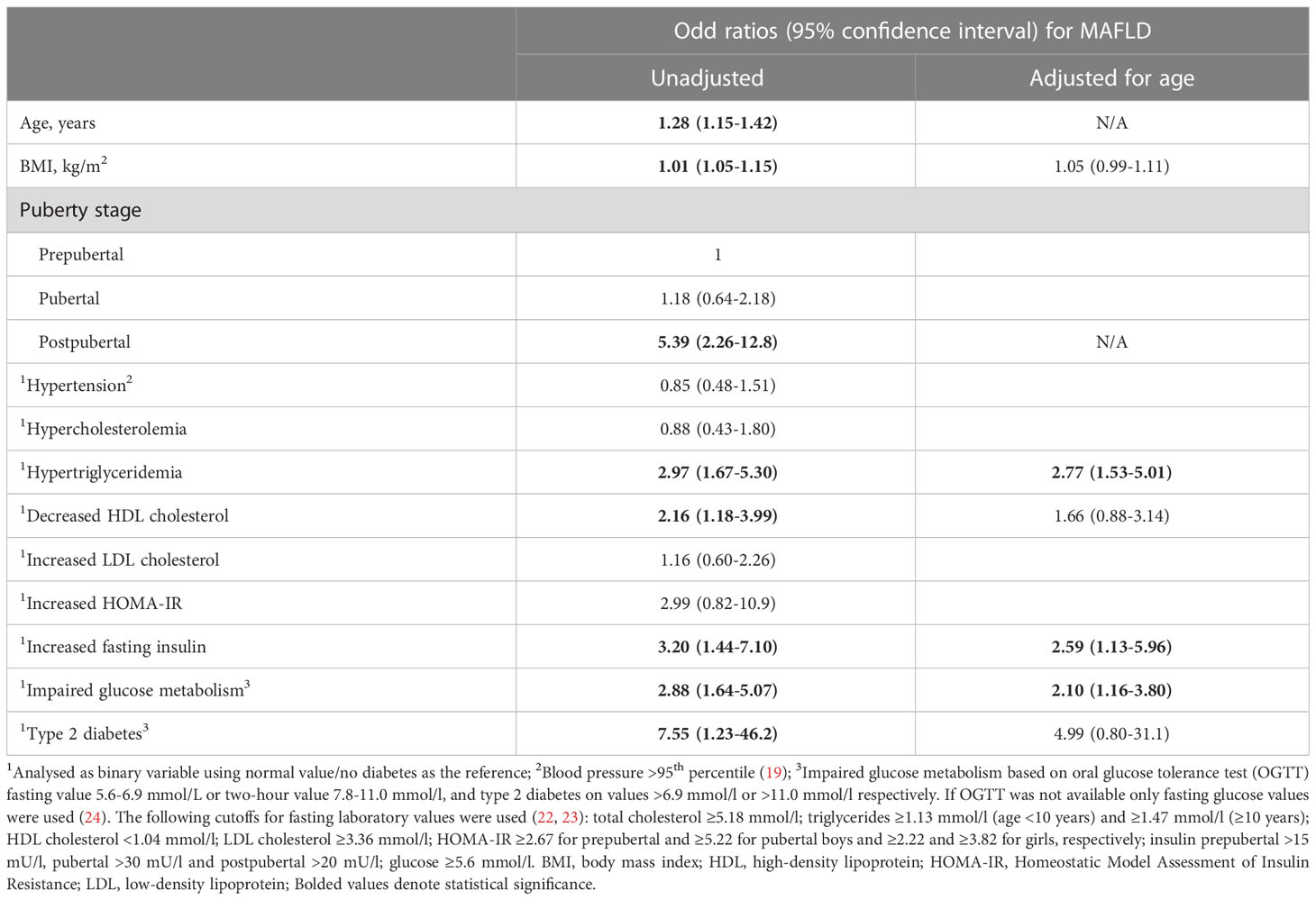
Table 1 Unadjusted and age adjusted analyses for related factors for metabolic-associated fatty liver disease (MAFLD) in 401 overweight or obese boys.
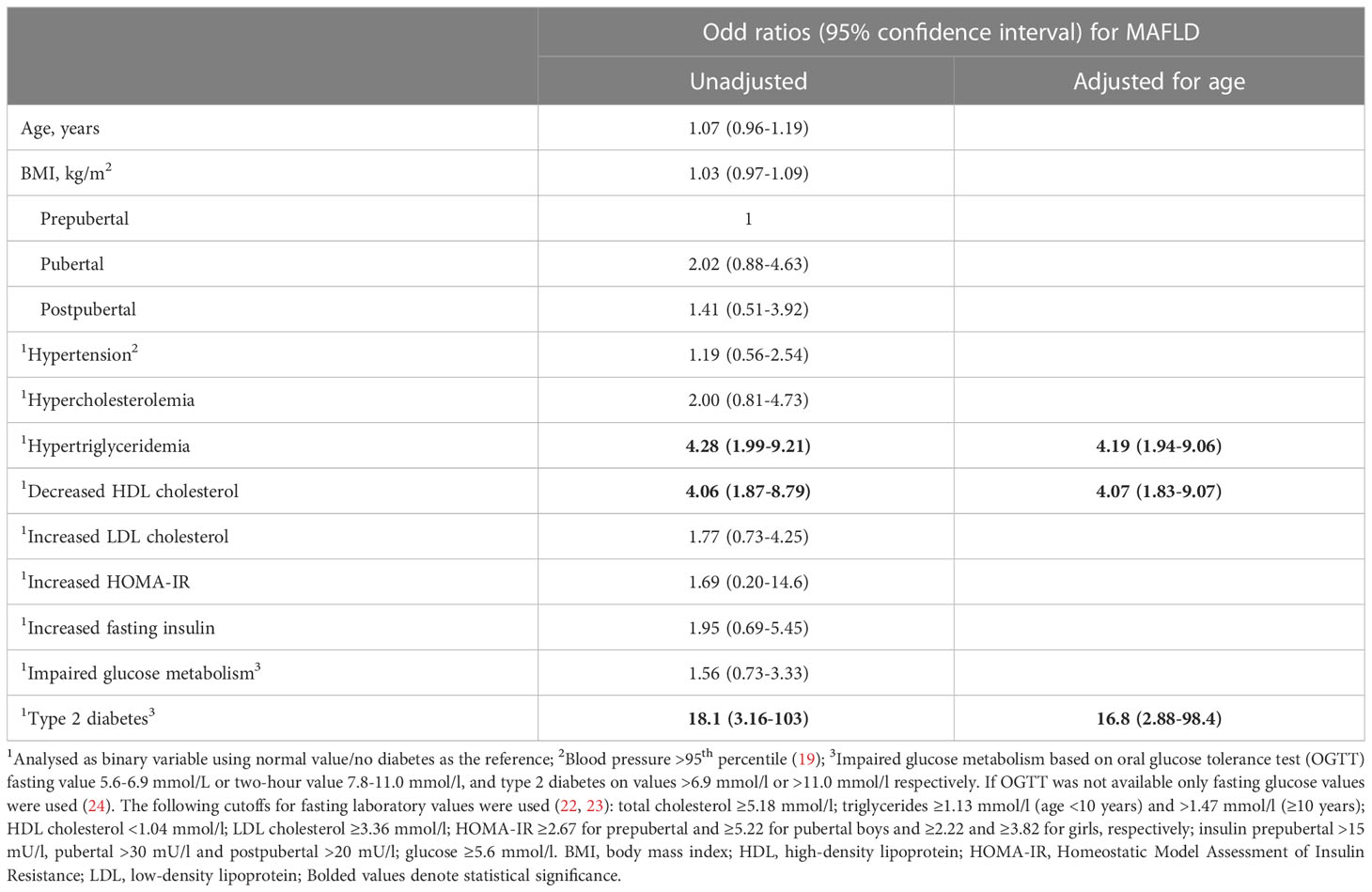
Table 2 Unadjusted and age adjusted analyses for related factors for metabolic-associated fatty liver disease (MAFLD) in 302 overweight or obese girls.
4 Discussion
4.1 Prevalence of MAFLD
MAFLD was present in 15% of the overweight Finnish children and, more specifically, in 18% of boys and 11% of girls. There are a limited number of comparable studies, but a meta-analysis by Cholongitas et al. (27) reported figures between 11.6% and 81.8% for NAFLD in children monitored in obesity clinics, the pooled prevalence being 32.5% in boys and 15.5% in girls. Only one included study used increased ALT as a diagnostic outcome (28), while the others used ultrasonography, magnetic resonance imaging (MRI), autopsy findings, transient elastography, and fatty liver index (27, 29). Another meta-analysis by Liu et al. reported overall prevalence of MAFLD to be 50.2% in overweight boys and 35.3% in girls with various diagnostic methods, but studies with ALT as an outcome were excluded (29). Additionally, a meta-analysis by Anderson et al. (15) observed a prevalences of increased ALT as a proxy for NAFLD varying between 6.2% and 27.6% in pediatric obesity clinics.
The varying prevalence of NAFLD could be partially due to differing use and performance of the diagnostic methods, as ultrasonography, for instance, has suboptimal accuracy (4, 27, 30) and MRI and liver biopsy are only performed on selected children (3, 4, 15, 31, 32). Although likewise imperfect as a diagnostic tool (33), ALT is a practical and unbiased option for measuring the prevalence of and temporal trends in MAFLD (4, 11, 25, 30, 32). A major challenge, however, is setting cutoffs for ALT (15). For example, we utilized the often-recommended ULNs that are based on data from 12-17-year-old US children with limited consideration for confounders (4, 11, 25). Moreover, it is unclear if these data are representative of other populations (34). The ALT cutoffs used in earlier reports have varied considerably and have rarely been sex-specific (15, 28). Moreover, the studies have often been small and involved heterogenous cohorts and diverse exclusion criteria for other conditions affecting the liver (15, 27, 28). Altogether, more standardized ALT thresholds based on sophisticated diagnostic outcomes (25, 32) and representative cohorts of both obese and non-obese children are called for. Of note, 5% of the children included in our study had ALT > 80 U/l, which has been associated with a significant risk of having advanced liver disease (26).
4.2 Patient-related associated factors
In line with earlier research (15, 29, 33–35), the risk of MAFLD was higher in boys than girls. Furthermore, the prevalence of MAFLD increased with age and puberty in boys, while in girls it already peaked in early puberty. These issues have not been studied with similar outcomes but, as an indirect comparison, Putri et al. (35) also found age – although significant in both genders – to be more strongly associated with increased ALT in boys. On contrary, Bussler et al. found ALT to increase at the onset of puberty in both genders and thereafter to decrease in girls (36). Furthermore, Koutny et al. (37) found no clear association between stage of puberty and ALT values. The peak observed in the prevalence of MAFLD at early puberty and the subsequent decrease in girls might be explained by hormonal changes, as female sex hormones have been associated to decreased liver adiposity in women (38). It must also be noted that fixed ALT cutoffs might not be optimal to all puberty stages (36). Additionally, although BMI continued to increase with age in both genders, on the individual level girls may be more prone to active dieting in adolescence e.g. due to peer pressure. Of note, although overweight is both a major risk factor at population level (39) and also a main criterion for MAFLD (11), we found it to be associated with MAFLD only in boys. Logical explanation could be the ceiling effect caused by the high proportion of severe obesity in the study group. Although the complex associations of sex, puberty, and BMI with MAFLD remain to be fully elucidated, present and past findings (40–42) indicate that these individual features may markedly affect the prevalence of MAFLD.
4.3 Associations of metabolic disturbances with MAFLD
Approximately half of the study population showed signs of abnormal glucose and lipid metabolism and hypertension. More specifically, T2D, hypertriglyceridemia, and low HDL cholesterol in both genders and hyperinsulinemia and impaired glucose metabolism in boys were associated with MAFLD. Furthermore, the presence of multiple metabolic abnormalities was also associated with MALFD. These results are in general consistent with those of earlier studies on pediatric NAFLD and MAFLD (8, 35, 37, 39). Together with the results of these studies, our observations show that the prevalences of metabolic disturbances are markedly higher than those reported, for example, among children and adolescents in a US population (43). These findings emphasize the metabolic etiology of MAFLD in the majority of cases and support the novel definition of the condition.
4.4 Temporal trends in prevalence
We observed no significant change in MAFLD prevalence during the 2000s. The meta-analyses by Anderson et al. and Liu et al. reported similar findings with NAFLD and MAFLD according to the publication years of the studies included (15, 29). However, Cholongitas et al. found the reported prevalences to be higher in 2012–2019 than in 2004–2011 (27). Additionally, a few population-based studies have reported an increase of NAFLD concurrently with obesity (44–46). We observed no change in obesity in overweight children and adolescents, while these data were not reported in other studies. It must, however, be kept in mind that this finding is applicable only to the Finnish population. Interestingly, the results of recent studies suggest that the risk of NAFLD may be increased irrespective of the severity of obesity that may be explained by early-life programming during pregnancy (47, 48), and further studies on this important issue are warranted.
4.5 Strengths and limitations
Our main strengths were the large and well-defined study population, availability of comprehensive medical data and consideration of possible confounders. Inclusion of patients seen in primary healthcare reduces the risk of selection bias compared to studies carried out in specialized centers. The retrospective design was a limitation, although this was counterbalanced by the systematic data collection with a pre-tested protocol and the use of unbiased ALT instead of imprecise disease codes (49). Additionally, exclusion of hepatic comorbidities was based on clinical decision-making and some cases may thus have remained unrecognized, although for example viral hepatitis is particularly rare among Finnish children (50). As regards generalizability, while the results may differ in other populations due to the role of individual and environmental factors in the etiology of MAFLD, the use of a simplified and systematic diagnostic outcome improves the comparability. Nevertheless, the fact that most of the participants were of Finnish origin inevitably reduces comparability to other ethnic groups.
4.6 Conclusions
To conclude, MAFLD was present in 18% of overweight Finnish boys and 11% of girls, with no significant change seen during the 2000s. The prevalence of MAFLD increased along with age, pubertal stage, and BMI in boys, while in girls it peaked in early puberty. The condition was also strongly associated with metabolic disturbances. The high prevalence of MALFD in overweight and obese children supports their systematic screening to enable early diagnosis. Furthermore, the here identified risk factors for MAFLD help to focus the limited healthcare resources for careful follow-up of high-risk individuals. Future prevalence studies should aim at better standardization of the possible confounders but, simultaneously, consider the effect of individual characteristics in the criteria used to define MAFLD.
Data availability statement
The datasets presented in this article are not publicly available due to privacy and ethical reasons. Requests to access the datasets should be directed to linnea.aarela@tuni.fi.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
HR: study design, data collection and analysis, drafting of the manuscript. LA: study design, data collection and analysis, drafting of the manuscript. LK: study design and critical revision of the manuscript. SL: data collection and critical revision of the manuscript. PH: study design and critical revision of the manuscript. NV: study design and critical revision of the manuscript. HH: study design, statistical analysis, and critical revision of the manuscript. TL: study design and critical revision of the manuscript. KK: study design, study supervision, and critical revision of the manuscript. No writing assistance was received. All authors contributed to the article and approved the submitted version.
Funding
The Orion Research Foundation, the Päivikki and Sakari Sohlberg Foundation, the Foundation for Pediatric Research, the Competitive State Research Financing of the Expert Area of Tampere University Hospital, the Maire Rossi Foundation, the Maud Kuistila Foundation, The Juho Vainio Foundation, the Mary and Georg Ehrnrooth Foundation, the Paulo Foundation, the Emil Aaltonen Foundation, the Finnish-Norwegian Medical Foundation, the Finnish Celiac Society and the Sigrid Jusélius Foundation. The funders had no role in study design, data collection and analysis, decision to publish, or in the preparation of the present manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fendo.2023.1090344/full#supplementary-material
References
1. Doycheva I, Watt KD, Rifai G, Abou Mrad R, Lopez R, Zein NN, et al. Increasing burden of chronic liver disease among adolescents and young adults in the USA: a silent epidemic. Dig Dis Sci (2017) 62(5):1373–80. doi: 10.1007/s10620-017-4492-3
2. Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C. Prevalence of fatty liver in children and adolescents. Pediatrics (2006) 118(4):1388–93. doi: 10.1542/peds.2006-1212
3. Flisiak-Jackiewicz M, Lebensztejn DM. Update on pathogenesis, diagnostics and therapy of nonalcoholic fatty liver disease in children. Clin Exp Hepatol (2019) 5(1):11–21. doi: 10.5114/ceh.2019.83152
4. Vos MB, Abrams SH, Barlow SE, Caprio S, Daniels SR, Kohli R, et al. NASPGHAN clinical practice guideline for the diagnosis and treatment of nonalcoholic fatty liver disease in hildren: recommendations from the expert committee on NAFLD (ECON) and the north American society of pediatric gastroenterology, hepatology and nutrition (NASPGHAN). J Pediatr Gastroenterol Nutr (2017) 64(2):319–34. doi: 10.1097/MPG.0000000000001482
5. Vajro P, Lenta S, Socha P, Dhawan A, McKiernan P, Baumann U, et al. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN hepatology committee. J Pediatr Gastroenterol Nutr (2012) 54(5):700–13. doi: 10.1097/MPG.0b013e318252a13f
6. Holterman A-XL, Guzman G, Fantuzzi G, Wang H, Aigner K, Browne A, et al. Nonalcoholic fatty liver disease in severely obese adolescent and adult patients. Obesity (2013) 21(3):591–7. doi: 10.1002/oby.20174
7. Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, Benson JT, Enders FB, Angulo P. The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut (2009) 58(11):1538–44. doi: 10.1136/gut.2008.171280
8. Schwimmer JB, Pardee PE, Lavine JE, Blumkin AK, Cook S. Cardiovascular risk factors and the metabolic syndrome in pediatric nonalcoholic fatty liver disease. Circulation (2008) 118(3):277–83. doi: 10.1161/CIRCULATIONAHA.107.739920
9. Kistler KD, Molleston J, Unalp A, Abrams SH, Behling C, Schwimmer JB. Symptoms and quality of life in obese children and adolescents with non-alcoholic fatty liver disease. Alimentary Pharmacol Ther (2010) 31(3):396–406. doi: 10.1111/j.1365-2036.2009.04181.x
10. Alkhouri N, Hanouneh IA, Zein NN, Lopez R, Kelly D, Eghtesad B, et al. Liver transplantation for nonalcoholic steatohepatitis in young patients. Transpl Int (2016) 29(4):418–24. doi: 10.1111/tri.12694
11. Eslam M, Alkhouri N, Vajro P, Baumann U, Weiss R, Socha P, et al. Defining paediatric metabolic (dysfunction)-associated fatty liver disease: an international expert consensus statement. Lancet Gastroenterol Hepatol (2021) 6(10):864–73. doi: 10.1016/S2468-1253(21)00183-7
12. Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol (2020) 73(1):202–9. doi: 10.1016/j.jhep.2020.03.039
13. Eslam M, Sanyal AJ, George J. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology (2020) 158(7):1999–2014. doi: 10.1053/j.gastro.2019.11.312
14. Cotter TG, Rinella M. Nonalcoholic fatty liver disease 2020: the state of the disease. Gastroenterology (2020) 158(7):1851–64. doi: 10.1053/j.gastro.2020.01.052
15. Anderson EL, Howe LD, Jones HE, Higgins JPT, Lawlor DA, Fraser A. The prevalence of non-alcoholic fatty liver disease in children and adolescents: a systematic review and meta-analysis. PloS One (2015) 10(10):e0140908. doi: 10.1371/journal.pone.0140908
16. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. Br Med J (2000) 320(7244):1240–3. doi: 10.1136/bmj.320.7244.1240
17. Saari A, Sankilampi U, Hannila M-L, Kiviniemi V, Kesseli K, Dunkel L. New Finnish growth references for children and adolescents aged 0 to 20 years: length/height-for-age, weight-for-length/height, and body mass index-for-age. Ann Med (2011) 43(3):235–48. doi: 10.3109/07853890.2010.515603
18. Xi B, Zong X, Kelishadi R, Litwin M, Hong YM, Poh BK, et al. International waist circumference percentile cutoffs for central obesity in children and adolescents aged 6 to 18 years. J Clin Endocrinol Metab (2020) 105(4):e1569–83. doi: 10.1210/clinem/dgz195
19. Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics (2017) 140(3):e20171904. doi: 10.1542/peds.2017-1904
20. Marshall WA, Tanner JM. Variations in the pattern of pubertal changes in boys. Arch Dis Child (1970) 45(239):13–23. doi: 10.1136/adc.45.239.13
21. Marshall WA, Tanner JM. Variations in pattern of pubertal changes in girls. Arch Dis Childh (1969) 44(235):291–303. doi: 10.1136/adc.44.235.291
22. De Jesus JM. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics (2011) 128(SUPP.5):213–56. doi: 10.1542/peds.2009-2107C
23. Kurtoglu S, Hatipoglu N, Maziciogu M, Kendirci M, Keskin M, Kondolot M. Insulin resistance in obese children and adolescents: HOMA-IR cut-off levels in the prepubertal and pubertal periods. J Clin Res Pediatr Endocrinol (2010) 2(3):100–6. doi: 10.4274/jcrpe.v2i3.100
24. American Diabetes association. classification and diagnosis of diabetes: standards of medical care in diabetes 2018. Diabetes Care (2018) 41(Suppl 1):S13–27. doi: 10.2337/dc18-S002
25. Schwimmer JB, Dunn W, Norman GJ, Pardee PE, Middleton MS, Kerkar N, et al. SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology (2010) 138(4):1357. doi: 10.1053/j.gastro.2009.12.052
26. Schwimmer JB, Newton KP, Awai HI, Choi LJ, Garcia MA, Ellis LL, et al. Paediatric gastroenterology evaluation of overweight and obese children referred from primary care for suspected non-alcoholic fatty liver disease. Aliment Pharmacol Ther (2013) 38(10):1267–77. doi: 10.1111/apt.12518
27. Cholongitas E, Pavlopoulou I, Papatheodoridi M, Markakis GE, Bouras E, Haidich AB, et al. Epidemiology of nonalcoholic fatty liver disease in Europe: a systematic review and meta-analysis. Ann Gastroenterol (2021) 34(3):404–14. doi: 10.20524/aog.2021.0604
28. Wiegand S, Keller K, Röbl M, Reinehr T, Widhalm K, Holl R. PEDIATRIC HIGHLIGHT obese boys at increased risk for nonalcoholic liver disease: evaluation of 16 390 overweight or obese children and adolescents. Int J Obes (2010) 34:1468–74. doi: 10.1038/ijo.2010.106
29. Liu J, Mu C, Li K, Luo H, Liu Y, Li Z. Estimating global prevalence of metabolic dysfunction-associated fatty liver disease in overweight or obese children and adolescents: systematic review and meta-analysis. Int J Public Health (2021) 6:1604371(66). doi: 10.3389/ijph.2021.1604371
30. Draijer LG, Feddouli S, Bohte AE, Slootweg OVB, Rijcken THP, Benninga MA, et al. Comparison of diagnostic accuracy of screening tests ALT and ultrasound for pediatric non-alcoholic fatty liver disease. Eur J Pediatr (2017) 178(6):863–70. doi: 10.1007/s00431-019-03362-3
31. Molleston JP, Schwimmer JB, Yates KP, Murray KF, Cummings OW, Lavine JE, et al. Histological abnormalities in children with nonalcoholic fatty liver disease and normal or mildly elevated alanine aminotransferase levels. J Pediatr (2014) 164(4):707–13. doi: 10.1016/j.jpeds.2013.10.071
32. Yu EL, Golshan S, Harlow KE, Angeles JE, Durelle J, Goyal NP, et al. Prevalence of nonalcoholic fatty liver disease in children with obesity. J Pediatr (2019) 207:64–70. doi: 10.1016/j.jpeds.2018.11.021
33. Park SH, Park YE, Lee J, Choi JH, Ny H, Park J, et al. The change in prevalence of suspected non-alcoholic fatty liver disease in Korean adolescents from 2001 to 2017. Paediatr Int Child Health (2020) 40(3):166–70. doi: 10.1080/20469047.2020.1747002
34. Schwimmer JB, McGreal N, Deutsch R, Finegold MJ, Lavine JE. Influence of gender, race, and ethnicity on suspected fatty liver in obese adolescents. Pediatrics (2005) 115(5):561–5. doi: 10.1542/peds.2004-1832
35. Putri RR, Casswall T, Hagman E. Prevalence of increased transaminases and its association with sex, age, and metabolic parameters in children and adolescents with obesity-a nationwide cross-sectional cohort study. BMC Pediatr (2021) 21(1):271. doi: 10.1186/s12887-021-02747-4
36. Bussler S, Vogel M, Pietzner D, Harms K, Buzek T, Penke M, et al. New pediatric percentiles of liver enzyme serum levels (alanine aminotransferase, aspartate aminotransferase, γ-glutamyltransferase): effects of age, sex, body mass index, and pubertal stage. Hepatology (2018) 68(4):1319–30. doi: 10.1002/hep.29542
37. Koutny F, Weghuber D, Bollow E, Greber-Platzer S, Hartmann K, Körner A, et al. Prevalence of prediabetes and type 2 diabetes in children with obesity and increased transaminases in European German-speaking countries. analysis of the APV initiative. Pediatr Obes (2020) 15(4):e12601. doi: 10.1111/ijpo.12601
38. Suzuki A, Abdelmalek MF. Nonalcoholic fatty liver disease in women. Womens Health (Lond) (2009) 5(2):191–203. doi: 10.2217/17455057.5.2.191
39. Putri RR, Casswall T, Hagman E. Risk and protective factors of non-alcoholic fatty liver disease in paediatric obesity: a nationwide nested case – control study. Clin Obes (2022) 12(2):e12502. doi: 10.1111/cob.12502
40. Clarck JM, Brancati FL, Diehl AM. Nonalcoholic fatty liver disease. Gastroenterology. (2022) 122(6):1649–57. doi: 10.2337/dc10-0856
41. Goran MI, Gower BA. Longitudinal study on pubertal insulin resistance. Diabetes (2001) 50(7-12):2444–50. doi: 10.2337/diabetes.50.11.2444
42. Suzuki A, Abdelmalek MF, Schwimmer JB, Lavine JE, Scheimann AO, Unalp-Arida A, et al. Association between puberty and features of nonalcoholic fatty liver disease. Clin Gastroenterol Hepatol (2012) 10(7):786–94. doi: 10.1016/j.cgh.2012.01.020
43. Johnson WD, Kroon JJM, Greenway FL, Bouchard C, Ryan D, Katzmarzyk PT. Prevalence of risk factors for metabolic syndrome in adolescents. Arch Pediatr Adolesc Med (2009) 163(4):371–7. doi: 10.1001/archpediatrics.2009.3
44. Welsh JA, Karpen S, Vos MB. Increasing prevalence of nonalcoholic fatty liver disease among united states adolescents, 1988-1994 to 2007-2010. J Pediatr (2013) 162(3):496–500. doi: 10.1016/j.jpeds.2012.08.043
45. Zhang X, Wu M, Liu Z, Yan H, Wu X, Shi T, et al. Increasing prevalence of NAFLD/NASH among children, adolescents and young adults from 1990 to 2017: a population-based observational study. BMJ Open (2021) 11:42843. doi: 10.1136/bmjopen-2020-042843
46. Kang Y, Park S, Kim S, Koh H. Normal serum alanine aminotransferase and non-alcoholic fatty liver disease among Korean adolescents: a cross-sectional study using data from KNHANES 2010-2015. BMC Pediatr (2018) 18(1):215. doi: 10.1186/s12887-018-1202-z
47. Abeysekera KW, Orr JG, Madley-Dowd P, Fernandes GS, Zuccolo L, Gordon FH, et al. Association of maternal pre-pregnancy BMI and breastfeeding with NAFLD in young adults: a parental negative control study. Lancet Reg Heal - Eur (2021) 10:100206. doi: 10.1016/j.lanepe.2021.100206
48. Bugianesi E, Bizzarri C, Rosso C, Mosca A, Panera N, Veraldi S, et al. Low birthweight increases the likelihood of severe steatosis in pediatric non-alcoholic fatty liver sisease. Am J Gastroenterol (2017) 112(8):1277–86. doi: 10.1038/ajg.2017.140
49. Hagström H, Adams LA, Allen AM, Byrne CD, Chang Y, Grønbaek H, et al. Administrative coding in electronic health care record-based research of NAFLD: an expert panel consensus statement. Hepatology (2021) 74(1):474–82. doi: 10.1002/hep.31726
Keywords: alanine aminotransferase, children, diabetes, dyslipidemia, glucose intolerance, MAFLD, NAFLD, obesity
Citation: Riekki H, Aitokari L, Kivelä L, Lahti S, Hiltunen P, Vuorela N, Huhtala H, Lakka TA and Kurppa K (2023) Prevalence and associated factors of metabolic-associated fatty liver disease in overweight Finnish children and adolescents. Front. Endocrinol. 14:1090344. doi: 10.3389/fendo.2023.1090344
Received: 05 November 2022; Accepted: 04 April 2023;
Published: 20 June 2023.
Edited by:
Rahul Kumar, Changi General Hospital, SingaporeReviewed by:
Hamza El Hadi, Leipzig Heart Center, GermanySara Karjoo, Johns Hopkins All Children’s Hospital, United States
Awat Feizi, Isfahan University of Medical Sciences, Iran
Copyright © 2023 Riekki, Aitokari, Kivelä, Lahti, Hiltunen, Vuorela, Huhtala, Lakka and Kurppa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kalle Kurppa, kalle.kurppa@tuni.fi
†These authors have contributed equally to this work and share first authorship