 Immaculate M. Langmia1
Immaculate M. Langmia1 Katja S. Just1
Katja S. Just1 Sabrina Yamoune1
Sabrina Yamoune1 Jürgen Brockmöller2
Jürgen Brockmöller2 Collen Masimirembwa3
Collen Masimirembwa3 Julia C. Stingl1*
Julia C. Stingl1*- 1Institute of Clinical Pharmacology, University Hospital of Rheinisch-Westfälische Technische Hochschule Aachen, Aachen, Germany
- 2Department of Clinical Pharmacology, University Medical Center Göttingen, Georg-August University, Göttingen, Germany
- 3African Institute of Biomedical Science and Technology (AiBST), Harare, Zimbabwe
Adverse drug reactions (ADRs) are one of the major causes of morbidity and mortality worldwide. It is well-known that individual genetic make-up is one of the causative factors of ADRs. Approximately 14 million single nucleotide polymorphisms (SNPs) are distributed throughout the entire human genome and every patient has a distinct genetic make-up which influences their response to drug therapy. Cytochrome P450 2B6 (CYP2B6) is involved in the metabolism of antiretroviral, antimalarial, anticancer, and antidepressant drugs. These drug classes are commonly in use worldwide and face specific population variability in side effects and dosing. Parts of this variability may be caused by single nucleotide polymorphisms (SNPs) in the CYP2B6 gene that are associated with altered protein expression and catalytic function. Population variability in the CYP2B6 gene leads to changes in drug metabolism which may result in adverse drug reactions or therapeutic failure. So far more than 30 non-synonymous variants in CYP2B6 gene have been reported. The occurrence of these variants show intra and interpopulation variability, thus affecting drug efficacy at individual and population level. Differences in disease conditions and affordability of drug therapy further explain why some individuals or populations are more exposed to CYP2B6 pharmacogenomics associated ADRs than others. Variabilities in drug efficacy associated with the pharmacogenomics of CYP2B6 have been reported in various populations. The aim of this review is to highlight reports from various ethnicities that emphasize on the relationship between CYP2B6 pharmacogenomics variability and the occurrence of adverse drug reactions. In vitro and in vivo studies evaluating the catalytic activity of CYP2B6 variants using various substrates will also be discussed. While implementation of pharmacogenomic testing for personalized drug therapy has made big progress, less data on pharmacogenetics of drug safety has been gained in terms of CYP2B6 substrates. Therefore, reviewing the existing evidence on population variability in CYP2B6 and ADR risk profiles suggests that, in addition to other factors, the knowledge on pharmacogenomics of CYP2B6 in patient treatment may be useful for the development of personalized medicine with regards to genotype-based prescription.
Introduction
Adverse drug reactions (ADRs) are globally one of the major causes of morbidity and mortality (Giardina et al., 2018; Patel and Patel, 2018). According to the World Health Organization (WHO), ADR is a noxious and unintended response to a medication (Agency, 2017). ADRs can range from mild to severe causing ~6.5% of all visits to the emergency department and longer duration of hospitalization (Giardina et al., 2018; Patel and Patel, 2018; Schurig et al., 2018). Drug clearance may vary up to 10-fold between two individuals of the same weight taking the same drug dosage (Stingl et al., 2013). This variation can be influenced by pathophysiological, physiological, or environmental factors. However, genetic polymorphisms in drug transporters, drug targets and most importantly drug metabolizing enzymes have been emphasized over the years as one of the major factors causing variability in drug response (Weinshilboum, 2003; Evans and Relling, 2004).
The cytochrome P450 (CYPs) enzymes are involved in phase I drug metabolism. Variability in patient exposure and response to various medication have been associated to genetic variants in genes that code for CYP enzymes (Lynch and Price, 2007; Zanger and Schwab, 2013). The human genome harbors 18 CYP families divided into 41 subfamilies encoding 57 genes. Specifically, CYP1, CYP2, and CYP3 families catalyze the biotransformation of many xenobiotic agents. CYP2B6 is the only gene in the human CYP2B subfamily encoding a functional enzyme (Nebert et al., 2013).
The CYP2B6 gene which consists of nine exons is located on chromosome 19 at position 19q13.2. It is highly expressed in the liver, and to a certain extent in the extrahepatic tissues such as brain, kidney, digestive tract and the lungs (Lonsdale et al., 2013). CYP2B6 is a polymorphic cytochrome P450 enzyme with many single nucleotide polymorphisms (SNPs) encoding thirty-eight variants. These variants are referred as star alleles on the Pharmacogene Variation website with designated clinical function as normal, decrease, increase, no or uncertain function (Thorn et al., 2010). Compared to other well-studied phase I enzymes such as CYP2D6, CYP2C19 and CYP2C9, CYP2B6 at first had been thought to play a minor role in human drug metabolism (Desta et al., 2021). However, with the increase in techniques to evaluate its regulation, relative hepatic expression and function, it became evident that CYP2B6 constitutes up to 10% of the functional CYP enzymes in the liver. It is involved in the metabolism of 10–12% of all drugs commercially available in the market (Hanna et al., 2000; Rendic, 2002) and accounts for the metabolism of 4% of top 200 drugs in the market (Zanger et al., 2008). Specifically, it is fully or partially involved in the catalytic biotransformation of at least 90 drugs. Table 1 shows selected drug substrates which are metabolism by CYP2B6.

Table 1. Drug substrates known for metabolism by the CYP2B6 enzyme.
Interestingly, variability in the expression and function of the CYP2B6 enzyme alters the metabolism of these substrates leading to altered pharmacokinetics and therapeutic efficacy. Abnormal drug efficacy associated with patient CYP2B6 genotype has been reported in various populations (Sarfo et al., 2014; Kharasch and Greenblatt, 2019; Chaivichacharn et al., 2020). The scope of this review is to report the evidence on ADRs of CYP2B6 substrates and elucidate possible functional mechanisms of the influence of CYP2B6 polymorphisms on enzyme function and ADRs. Population disparity in the use of CYP2B6 substrates and consequent exposure to substrate-related ADRs are discussed. Serious ADRs due to high-risk pharmacogenetic variants might be avoided by the use of preemptive genotyping (Dolgin, 2011; Bielinski et al., 2014; Kim et al., 2017; Bank et al., 2019) and the use of pharmacogenetic testing has greatly improved the lives of many patients (Lonsdale et al., 2013; Drozda et al., 2018). The knowledge on pharmacogenomics of CYP2B6 in patient treatment may be useful for the development of personalized medicine with regards to genotype-based prescriptions.
Factors That Influence CYP2B6 Expression and Function
A significant interindividual variability in the mRNA expression, protein levels and activity of CYP2B6 has been reported in human liver microsomes (Ekins et al., 1998; Lang et al., 2001; Hesse et al., 2004). This variability is caused by the following factors; transcriptional regulation involving inhibition or induction of CYP2B6 expression via the constitutive androstane receptor (CAR) and/or pregnane X receptor (PXR) (Wang et al., 2003a), inductive expression via glucocorticoid receptor (GR) (Lee et al., 2003; Wang et al., 2003b), inhibition of CYP2B6 by cytokines through CAR and PXR (Aitken and Morgan, 2007; Liptrott et al., 2009), induction of CYP2B6 by estrogen via the estrogen responsive element (ERE) (Faucette et al., 2004; Lo et al., 2010) and most importantly genetic polymorphism in the CYP2B6 gene itself (Lang et al., 2001). Developmental regulation (age), gender and disease condition are other confounders of CYP2B6 differential expression and function (Pearce et al., 2016). It is estimated that genetic polymorphisms and/or gene regulation are the major factors that impact variability in CYP2B6 expression and function.
Substrates of CYP2B6
Previous investigations revealed diversity in the structure among CYP2B6 substrates (Lewis and Lake, 1997). They also confer differences in the site of metabolism (Lewis and Lake, 1997). Typically substrates of CYP2B6 are hydrophobic small molecules, neutral or weak bases, very lipophilic with one or two hydrogen-bond acceptors (Ekins et al., 2008). Table 1 indicates that CYP2B6 catalyzes demethylation, hydroxylation and oxidation reactions to form active or inactive metabolites (Hidestrand et al., 2001; Xie et al., 2003; Ekins et al., 2008; Zhang et al., 2017). Substrates of CYP2B6 are found in ~23 different therapeutic classes (Table 1). It is predicted that CYP2B6 is the major catalytic enzyme in the biotransformation of important drugs commonly used worldwide. In combination with other cytochromes, CYP2B6 also plays a minor role in the metabolism of other xenobiotics. Notably, common metabolism of drugs is mediated by CYP2B6, CYP2C19, and CYP3A4 in terms of metabolism of clinically relevant therapeutics (Table 1). The CYP2B6 enzyme confers stereoselectivity, showing higher KM for certain enantiomers such as S-efavirenz, S-mephenytoin, S-fluoxetine, S-ifosfamide, S-methadone, S-ketamine, S-bupropion (Coles and Kharasch, 2008; Ekins et al., 2008; Rakhmanina and van den Anker, 2010). CYP2B6 variants are substrate specific in their metabolic function. Thus, evaluating the impact of each enzyme variant on the metabolism of a specific substrate is of clinical importance (Ariyoshi et al., 2011). For example, recombinant CYP2B6*6 showed a decreased metabolism for both efavirenz and cyclophosphamide, while CYP2B6*4 showed increased metabolic activity toward efavirenz but less efficient metabolic activity toward cyclophosphamide (Ariyoshi et al., 2011).
CYP2B6 Allele Variability Across Populations
Wide variability in CYP2B6 allelic frequencies is reported across populations. There exists intra and interethnic variability in the frequency of CYP2B6*6 and CYP2B6*18 variants. For example, at global level, the minor allele frequency of the CYP2B6*6 ranged from 0.33 to 0.5 in African Americans and Africans, 0.10–0.21 in Asians, 0.14–0.27 in Caucasians and 0.62 in Papua New Guineans (Zanger and Schwab, 2013; Rajman et al., 2017). Furthermore, allele frequency at the global level may not represent intraethnic differences within a specific population (Table 2). Though the CYP2B6*6 allele is more frequent in Africans and people of African descent, large intraethnic variability within these populations is observed (Rajman et al., 2017). For instance, the frequency of CYP2B6*6 in the Nigerian Yoruba population was reported to be 42%, Kenya Kikuyu 34% and Tswana of Bostwana 22% (Table 2). Also, the frequency of CYP2B6*9 (G516T) which forms part of the CYP2B6*6 variants was reported to be 55% in the Congolese, 20% in South African Xhosa and 37% in the Cameroonian population (Table 2). CYP2B6*4 is more frequent in the African, American, and Asian compared to the European population (Table 2). Meanwhile CYP2B6*2 is more frequent in the European and African compare to the Asian population (Table 2). This differences are associated with CYP2B6 functional variability and the occurrence of substrate specific ADR.
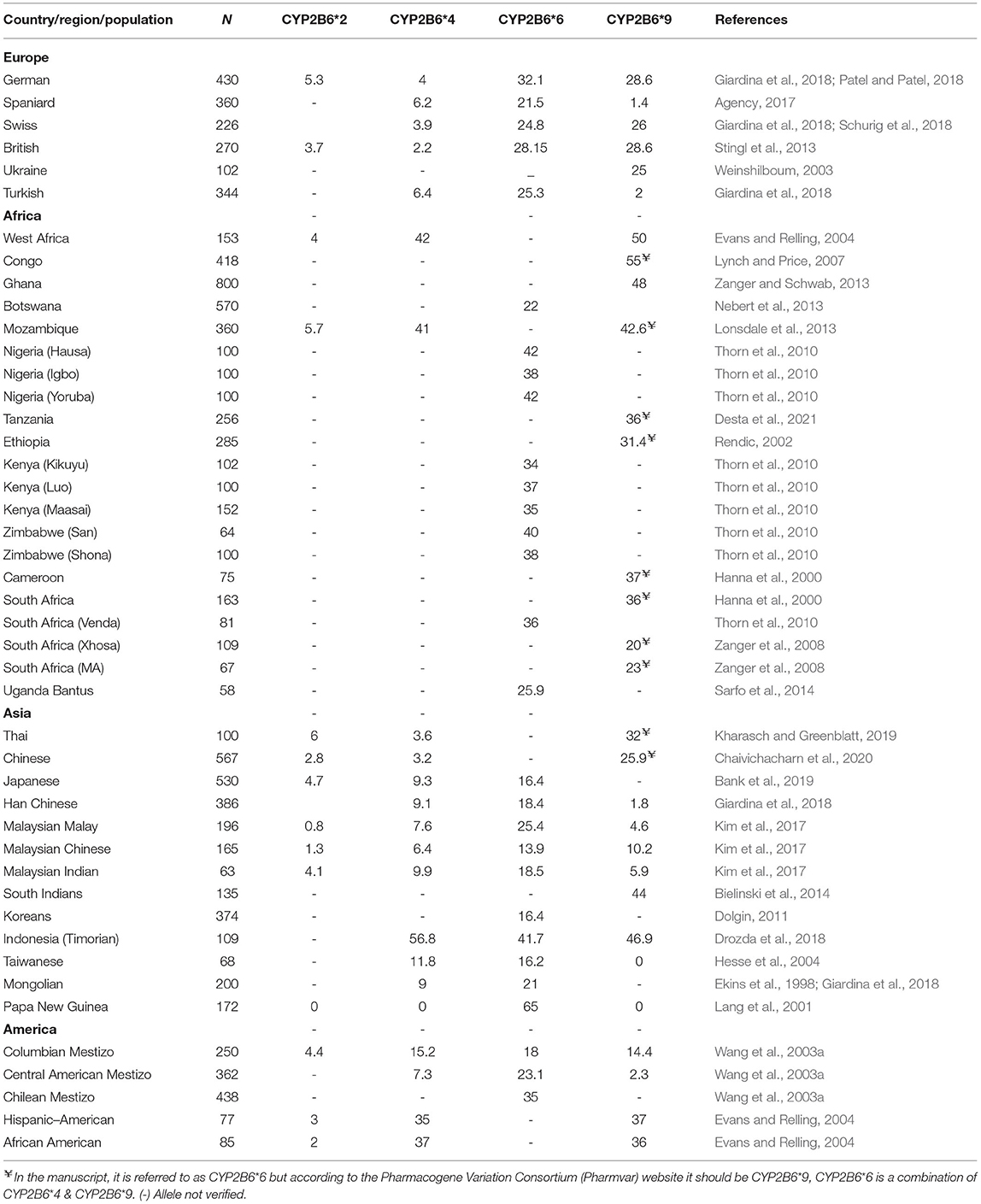
Table 2. Selected studies revealing variability in allele frequency of CYP2B6 alleles in different ethnicities.
Population Disparity in the Use of CYP2B6 Substrates and Consequent Exposure to Substrate-Specific Adverse Drug Reaction (ADR)
Efavirenz and Nevirapine
Efavirenz (EFV) is classified as an effective non-nucleoside reverse transcriptase inhibitor used in the treatment of HIV infection1,2. As part of the highly active antiretroviral therapy, EFV is used in combination with other nucleoside reverse transcriptase inhibitors (NRTIs)1, 2. EFV, which is presented in the form of 600 mg once daily or in a reduced dose of 400 mg oral tablets, is metabolized mainly by hepatic CYP2B6. EFV therapy is limited due to its narrow therapeutic window, thus, there exist a small difference between therapeutic and toxic doses. ADRs which are linked to the use of EFV includes increased risk of neurotoxicity, neuropsychiatric disorders, sleep disorders, high cholesterol level and drug induced liver disease (Cohen et al., 2009; Yimer et al., 2011; Aminkeng et al., 2014; Sarfo et al., 2014; Dhoro et al., 2015).
CYP2B6 genotype is a strong predictor of high systemic exposure to EFV in HIV infected patients. Table 3 presents studies on associations between CYP2B6 genotype and the occurrence of CYP2B6 substrate related ADRs in various ethnicities. According to reports across ethnicities, patients harboring the CYP2B6*6 (516G>T, 785A>G) and the CYP2B6*18 (983T>C) variants experience reduced metabolism of EFV and increased exposure to the drug (Table 3). Patients with the homozygote 516TT and/or 785GG genotype as well as those with the 983CC genotype (poor metabolizers) experience significant increase in EFV plasma concentration and reduced clearance (Table 3). High exposure to EFV increases the risk of ADRs in these patients (Gounden et al., 2010; Mukonzo et al., 2013; Sarfo et al., 2014). Amongst all CYP2B6 substrates, EFV is the most studied drug with diverse forms of ADRs reported from various ethnicities. EFV is among top drugs causing ADRs in HIV patients in Africa, some part of Eastern Europe, and Asia (Manosuthi et al., 2013; Birbal et al., 2016; Rajman et al., 2017).
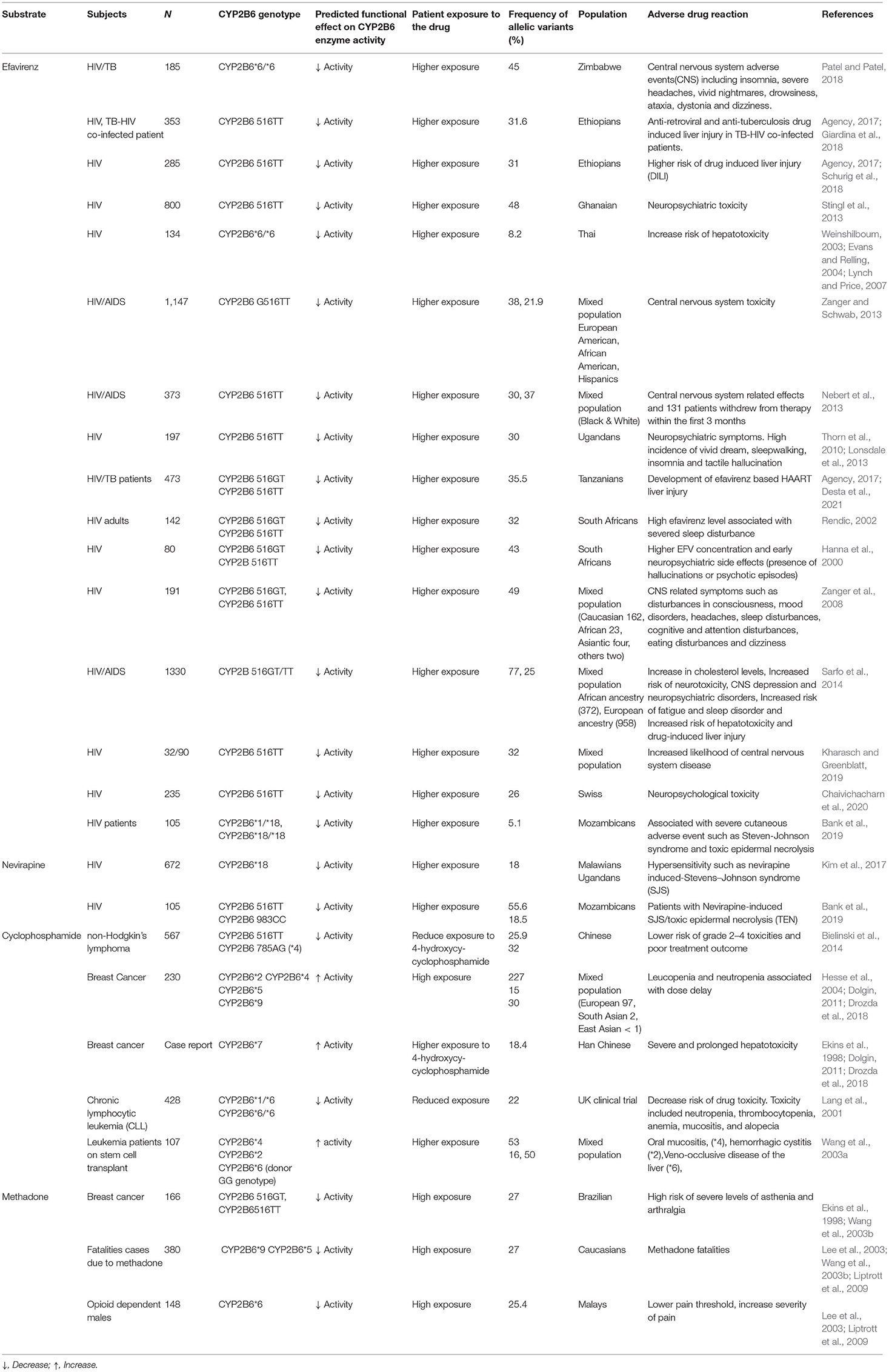
Table 3. CYP2B6 polymorphisms and adverse drug reactions reported amongst patients in various ethnicities.
Nevirapine (NVP) based antiretroviral therapy is also used as a first line regimen for HIV infection. Its usage is limited due to side effects including hepatotoxicity, fever, Steven-Johnson syndrome and toxic epidermal necrolysis (Ciccacci et al., 2013; Aminkeng et al., 2014). In addition to other factors such as weight and gender, CYP2B6 genotype influences patient response to NVP (Srivastava et al., 2010; Rajman et al., 2017; Yoon et al., 2020). These variants, CYP2B6 516G>T and 983T>C (CYP2B6*18) also impact patient exposure to NVP as reported by few studies from different ethnicities (Uttayamakul et al., 2010; Calcagno et al., 2012; Vardhanabhuti et al., 2013; Mhandire et al., 2015; Giacomelli et al., 2018). A reduced metabolic activity of the CYP2B6 enzyme leading to increased exposure of the patient and subsequent ADRs are observed (Yoon et al., 2020) (Table 3). NVP induced hypersensitivity reactions in HIV patients (Ciccacci et al., 2010; Carr et al., 2014). The variant allele of CYP2B6*18 and CYP2B6*4 were associated with the occurrence of Stevens-Johnson syndrome (SJS) among HIV patients (Ciccacci et al., 2013; Carr et al., 2014). Studies suggest dose reduction in patients harboring CYP2B6 poor metabolizer variants (Schipani et al., 2011; Morales-Pérez, 2021).
Interestingly, the use of EFV and NVP for HIV treatment is variable among populations. Highly active antiretroviral therapy (HAART) that includes EFV or NVP is mostly used in low and middle income countries (LMICs) including countries in Africa, Asia and some part of Eastern Europe (Gokengin et al., 2018; Ndashimye and Arts, 2019). Some studies have examined the reasons for such disparity in the use of EFV. It was observed that countries with higher income had greater access to novel drugs and new drug classes as first-line treatment than countries with low income (Gokengin et al., 2018; Ndashimye and Arts, 2019). Although most HAART regimens are given free to patients in all countries, the high level of donor dependency in LMICs might be a major obstacle to accessibility to new, expensive, more quality and less toxic drugs (Gokengin et al., 2018). The high cost of new first-line drugs with better tolerability and lower toxicity influences the choice of treatment regimen, with high income countries (HICs) choosing regimens that include new drugs compared to LMICs who depend on cheaper regimens (Gokengin et al., 2018). We observe an association between countries depending on cheaper drugs (EFV) and a high frequency of CYP2B6*6 which enhances the risk of EFV related ADRs in these populations (Africans, Papua New Guineans and African Americans with low income/incomplete insurance coverage). Intraethnic variability of CYP2B6 alleles within the African population, further indicates differences in the risk profiles of occurrence of CYP2B6*6 and CYP2B6*9-EFV-related ADRs between these African countries. This genomic diversity of African populations has been observed for many genes (Rajman et al., 2017) and highlights the potential error in generalizing the likely response to medicines of populations on the African continent (Ampadu et al., 2016). HIV infected individuals in LMICs are more likely to suffer from EFV-related ADRs than those in HICs.
Even though many LMICs have transited from the use of EFV and NVP to the use of the HIV-1 integrase inhibitor dolutegravir (DTG) which is assumed to be less expensive and less toxic (Vitoria et al., 2018), DTG has its own limitations as confirmed by the U.S. Food and Drug Administration (FDA). DGT may be unsuitable for patients with hepatitis B and C infection due to elevated levels of hepatic enzyme (Vitoria et al., 2018). Risk of hypersensitivity reactions and development of renal failure may be observed (Vitoria et al., 2018). New-onset or worsening hepatic or renal toxicity with longer cumulative exposure is a potential risk (Vitoria et al., 2018). In pregnancy, there are concerns that the baby may be harmed, thus women are recommended to take effective birth control while on the drug (Vitoria et al., 2018; Zash et al., 2019; Alhassan et al., 2020). Weight gain was observed in patients treated with DTG compared to EFV in clinical trials performed in sub-Saharan Africa and studies in Europe and North America. Therefore, long term use of DTG is still under concern (Kouanfack et al., 2019; Bourgi et al., 2020; Sax et al., 2020). A recent communication in December 2020 by Siedner et al. found that patients with drug resistant mutation in the reverse transcriptase are unlikely to benefit from the HIV integrase inhibitor DTG (Siedner et al., 2020). That implies EFV and NVP might still be in use for specific group of patients (Vitoria et al., 2018).
The occurrence of other diseases, including hepatitis and liver disease, are more common among HIV patients in LMICs (Labarga et al., 2007; Su et al., 2018). Unfortunately, much care is not given to HIV patients who have comorbid conditions, thus increasing the risk of ADRs amongst these patients (Labarga et al., 2007; Wu et al., 2017; Su et al., 2018). For example, patients with liver disease and hepatitis may experience enhanced hepatotoxicity due to EFV (Agbaji et al., 2013; Wu et al., 2017; Nampala et al., 2018; Su et al., 2018). Certain preexisting conditions, such as mild psychiatric disorder, may be exacerbated by EFV. Patients in LMICs may be vulnerable to ADRs not just because of the choice of regimen or their CYP2B6 genotype, but also because of comorbidity conditions. As such individualized prescriptions taking into account the pharmacogenetic profile, patient vulnerability caused by comorbid disease, and the toxicity profile of the drug will help to reduce ADR amongst these group of individuals in any part of the world.
Cyclophosphamide
Cyclophosphamide (CP) is an anticancer agent that is widely used in the treatment of pediatric and adult malignancies. CP is also known as an antirheumatic and anti-inflammatory drug (Brummaier et al., 2013; Sevko et al., 2013). CP is a prodrug that requires enzymatic bioactivation to produce its therapeutic function (Raccor et al., 2012). The formation of 4-hydroxycyclophosphamide (4-OHCP) is catalyzed by CYP2B6, CYP2C9, CYP2C19, CYP3A4 and CYP3A5. CYP2B6 and CYP2C19 confer the highest metabolic activity for the bioactivation of CP (Roy et al., 1999; Griskevicius et al., 2003; Raccor et al., 2012).
There is a significant variation in the plasma levels of CP ranging from 1.0 to 12.6 L/h (Batey et al., 2002; de Jonge et al., 2005). According to in vitro studies, it is clear that genetic polymorphisms in CYP2B6 gene and interindividual differences in the CYP2B6 enzymatic activity are associated with variability in CP efficacy (Roy et al., 1999; Xie et al., 2003; Hofmann et al., 2008). Very limited clinical studies have evaluated the impact of CYP2B6 variants on patient exposure to CP, instead, many studies have investigated the influence of patient genotype on therapeutic outcome or treatment efficacy of CP. However, Shu et al., showed a significant association between CYP2B6 genotype and exposure to 4-OHCP amongst 567 patients with non-Hodgkin lymphoma (Table 3). Reduced expression and catalytic activity of CYP2B6 protein was found among homozygous and heterozygous carriers of CYP2B6*6, *29, and *30 (Table 3). Patients with the 785G allele (*6) showed the worst treatment response (Shu et al., 2017). In breast cancer patients, a higher incidence of dose delay due to toxicity was observed among carriers of the CPY2B6 *2 and *5 (Bray et al., 2010). Furthermore, CYP2B6*2, *4, *8, and *9 alleles where associated with worse treatment outcome (Bray et al., 2010). In another study, an association was observed between CYP2B6*6 allele and inferior treatment response in patients with chronic lymphocytic leukemia. Patients harboring at least one CYP2B6*6 allele were less likely to achieve complete response to CP and fludarabine combination therapy due to impaired cytoreduction (Johnson et al., 2013).
Decreased risk of drug toxicity (neutropenia, thrombocytopenia, anemia, mucositis and alopecia) was observed in carriers of CYP2B6 *1/*6 and CYP2B6*6/*6 genotypes (Table 3). Considering the fact that CYP2B6*6 is a decreased function allele, these patients seem to experience less toxicity and impaired cytoreduction due to the inability of the variant enzyme with reduced activity to convert CP to the active anticancer metabolite which is also responsible for toxicity. A significant association was observed between CYP2B6 785A>G (*4) and shorter progression free survival (Falk et al., 2012) in patients with multiple myeloma. Patients with the 785GG genotype had the worse outcome compared to patients with the wild type allele. In another study involving lymphoma patients who were placed on high dose CP prior to hematopoietic stem cell transplant, patients with the CYP2B6*1/*5 genotype had a higher 2 years relapse and decrease overall survival than patients with the wild type genotype (Bachanova et al., 2015). Though the CYP2B6*5 variant is designated as normal function, in vitro studies of CP revealed reduced conversion of CP in human liver microsomes and recombinant expressed CYP2B6*5 variants confer 50% decrease in the formation of 4-OHCP compared to the wild type enzyme (Helsby et al., 2010; Raccor et al., 2012). Most recently, CP related toxicity was associated with CYP2B6 variants in patients with leukemia after HLA-identical hematopoietic stem cell transplantation (Rocha et al., 2009). Donor CYP2B6*6 was associated with Veno-occlusive disease of the liver meanwhile recipient CYP2B6*2 and *4 were associated with hemorrhagic cystitis and oral mucositis correspondingly (Rocha et al., 2009). High risk of severe levels of asthenia and arthralgia was observed amongst breast cancer women with CYP2B6 516GT and 516TT genotype placed on FAC-D combination therapy (Paula et al., 2020). Some studies also evaluated the role of CYP2C19 variants alongside with CYP2B6 in the efficacy and toxicity of cyclophosphamide. Even though few studies could not find any association between CYP2B6 or CYP2C19 and treatment outcome and/or toxicity of CP, differences in the study design, ethnicity, physiological or disease condition as well as power of the studies might have a role in the experimental outcome. However, it appears that these two pharmacogenes (CYP2B6 & CYP2C19) play a significant role in the bioactivation and efficacy of CP.
Variability in CYP2B6 polymorphisms between populations indicates that cancer patients in various ethnicities will respond variably to CP therapy. For example, CYP2B6*9 and CYP2B6*2 variants which are associated with toxicity and worse treatment outcome were not detected among 172 individuals from Papua New Guinea (Mehlotra et al., 2006; Bray et al., 2010), thus, cancer patients in this region are less likely to experience CYP2B6 pharmacogenetic associated-CP toxicity. Meanwhile, in Mozambique and Germany, patients are more likely to experience toxicity and worse treatment outcome due to the frequency of CYP2B6*9 (42.6 and 28.6%) in these populations (Tables 2, 3). Furthermore, reduced CP toxicity and impaired cytoreduction are likely to occur in populations with high frequency of CYP2B6*6 (Tables 2, 3).
According to research, the number of cancer survivals vary between and within countries. These differences are partly due to limited access to high quality and effective treatment in some part of the world (Newton et al., 2010; Eniu et al., 2019). CP is included in the WHO list of essential medicine (Bazargani et al., 2015). However, the majority of cancer patients living in LMICs have limited access to essential medicine and sometimes imported medication are either counterfeits or of poor quality (Fernandez et al., 2011; Ruff et al., 2016). Cancer care is not included in most resource limited settings due to high cost, as such, patients have to pay for cancer treatment out of their pocket (Eniu et al., 2019). In Asia, the number of death in a year ranged from 12% in Malaysia to 45% in Myanmar amongst cancer patients and those with low income were at risk of adverse outcomes even at early disease stages (ACTION Study Group, 2017). Important barriers to availability and affordability of anticancer drugs include lack of governmental reimbursement, allocation of healthcare budgets, generic and biosimilar products as well as the right to patent (Renner et al., 2013; Eniu et al., 2019). Therefore, patients in these regions are likely to experience drug resistance, treatment failure and more ADRs than those in HICs (Newton et al., 2010).
Additionally, increase number of adverse outcome is expected to occur in Africa, Asia and some parts of Europe, where other diseases such as HIV, tuberculosis and hepatitis are found amongst cancer patients who are self-sponsored without any health care coverage and reduced compliance to medication due to lack of funds and timely treatment (ACTION Study Group, 2017; Eniu et al., 2019). Therefore, in addition to other confounders, increased accessibility to essential medicine, availability of health care coverage, special care for patients with comorbidity and genotyping of patients may improve therapy.
Bupropion
Bupropion, generally used as an antidepressant, was later recommended as a non-nicotine treatment for smoking cessation. It is approved for treatment of nicotine dependence in patients with tobacco use disorder (Jorenby et al., 1999; Schnoll and Lerman, 2006). It acts by increasing dopaminergic and noradrenergic transmission via the blockage of neurotransmitter reuptake at the synapse thereby antagonizing the effects of nicotine acetylcholine receptor leading to nicotine withdrawal (Paterson et al., 2007). Also, bupropion is prescribed alone or in combination with other antidepressants for treatment of major depressive disorder and seasonal affective disorder. It is used as an adjunctive medication to reverse antidepressant-associated sexual dysfunction and to improve the efficacy of other antidepressants in partial or non-responders (Fava et al., 2005). Both bupropion and the active metabolite S-hydroxybupropion are responsible for the antidepressant and smoking cessation effect of bupropion (Zhu et al., 2012; Laib et al., 2014).
In vitro studies revealed variability in the rate of metabolism of S-bupropion by various CYP2B6 variants (Wang et al., 2020). Studies from different ethnicities show that the CYP2B6 allelic variants *4, *6, and *18 are associated with altered bupropion metabolism (Kirchheiner et al., 2003; Zhu et al., 2012; Benowitz et al., 2013). Depending on the patient's genotype, they can experience either increased or decreased exposure to the active metabolite hydroyxbupropion compared to wild type (Kirchheiner et al., 2003; Benowitz et al., 2013). Reportedly, patients harboring at least one reduced function allele had reduced exposure to the active metabolite and a lower clearance of the parent drug (Kirchheiner et al., 2003). Meanwhile, those with at least one increased function allele have increased exposure to hydroxyl active metabolites and a higher clearance of the parent drug (Kirchheiner et al., 2003).
Some studies have linked patient genotype to the efficacy of bupropion as a smoking cessation agent. In a smoking cessation trial involving 326 Europeans, a significant rate of abstinence was observed among patients with the CYP2B6*1/*6 and CYP2B6*6/*6 genotype (Lee et al., 2007). The CYP2B6*4 variant allele was associated with lower success rate in bupropion therapy. Specifically, patients with the AA genotype (wild type) succeeded in ceasing smoking compared to those with the variant genotype 785AG and 785GG (Tomaz et al., 2015). The increase function alleles might have led to higher clearance of the drug as well as reduced efficacy. In another clinical trial, bupropion drug gene interaction indicated that individuals with at least one T allele of CYP2B6*5 (1459CT, TT) and DRD2-Taq1 A2/A2 genotype had higher odds of abstinence (David et al., 2007). There are some differences in experimental outcome, for example, in a clinical trial involving 540 African American light smokers, a direct association between CYP2B6 genotype and smoking cessation was not observed, according to the authors, poor adherence amongst the participants might have led to the observed results. Most studies did not assess the impact of CYP2B6 polymorphisms on the antidepressant effect of bupropion. Instead, many focused on the CYP2B6 pharmacogenetics of bupropion in smoking cessation (Pharmgkb, 2000; Clark et al., 2012).
Compared to HICs, mental health in LMICs is still limited with low number of clinical trials and extremely low number of patients receiving treatment (Sankoh et al., 2018; Chibanda et al., 2020). Individuals with serious mental health problems in Nigeria cannot have access to health care due to the limited number of resources and mental health staff (Chibanda et al., 2020). Approximately, 300 psychiatric doctors serve a population of about 200 million people. Currently, these issues are being addressed by the Nigerian government via the forthcoming Mental Health and substance abuse bill (Brathwaite et al., 2020; Ugochukwu et al., 2020). Another study involving 683 prescriptions and case records of patients who were placed on antidepressants showed that tricyclic antidepressants were the most prescribed drugs (61.3%), followed by selective serotonin re-uptake inhibitors (38.7%) in Nigeria (Oyinlade, 2017). Amitriptyline hydrochloride, fluoxetine, clomipramine, escitalopram, and imipramine hydrochloride are the antidepressants found on the WHO list of essential medicine for Nigeria (WHO, 2017)3. In Zimbabwe, a research made in 2017 indicated that psychiatrists sometimes experience shortage of drugs which results in relapse among patients (Kidia et al., 2017). The antidepressants available were old generation drugs with many side effects (Kidia et al., 2017). According to one of the psychiatrists, more attention is being given to people with HIV than those with mental health, furthermore mental health policies were never implemented because of inadequate funding (Kidia et al., 2017). The African Mental Health Research Initiative group aims to create awareness and strengthen the mental health sector via research and capacity building in Sub-Saharan Africa (Chibanda et al., 2020; Langhaug et al., 2020).
The Global Health Observatory (GHO) data indicates the availability of bupropion in various countries (GHO/WHO, 2007). In some countries bupropion is available in the pharmacy with prescription. In others, it is found in general stores without prescription (Langhaug et al., 2020). Meanwhile, for some countries, data for the use of bupropion is not available. For example, GHO data shows that in Germany, France, Australia, Canada, United States of America, Congo, and India bupropion is available in pharmacies with prescription, whereas in Nigeria, it is found in general stores without prescription, in Malaysia, Ukraine, Zimbabwe, and Cameroon, GHO 2012 data shows that bupropion was present in pharmacy with prescription. In Hungary, Algeria, Tanzania, Mali, no data was available from 2007 to 2018 (GHO/WHO, 2007). Compared to HICs, the shortage of medication faced in LMIC is likely to increase relapse and the use of old drugs with more side effects can aggravate ADRs among patients.
Though bupropion is cost effective and widely used in most countries, its application as a smoking cessation agent is still very limited in some LMICs. The MPOWER tobacco control measures put in place by the World Health Organization (WHO) in 2005 have greatly helped many countries to discourage the use of tobacco and to help users quit tobacco addiction4. MPOWER measure is a tobacco free initiative established by WHO for defeating the global tobacco epidemic via Monitoring tobacco use, Protecting people from tobacco use, Offering help to quit, Warning about dangers of tobacco, Enforcing bans on advertising and sponsorship and Raising taxes on tobacco in all parts of the world (Batini et al., 2019). According to a recent report by Batini et al., the application of the MPOWER measures vary across continents and countries with a marked discrepancy observed between LMICs, and HICs, where cost, governmental buy in and resources influence implementation of the various measures (Batini et al., 2019). Using the African continent as an example, authors report that pharmacotherapy for smoking cessation is scarce in Nigeria with few pharmacies offering nicotine replacement therapy. In Zimbabwe, there are currently no smoking cessation services in the public sector except for private sectors, which is offered at very high cost (NRT 130USD/week, varenicline 250USD/month). In Tanzania, nicotine replacement therapy is available and smoking cessation therapy has been introduced into the methadone clinic in Dar es Salaam (Batini et al., 2019). However, the use of non-nicotine therapy such as bupropion is still lacking in these countries.
Depression seems to coexist with many diseases that are common in both high and LMICs. In Sub Saharan Africa, depression is common among HIV patients and people with disability (Mayston et al., 2020). In India, high prevalence of depressive episodes were found among diabetic patients (Kanwar et al., 2019). In a comparison between Ethiopian and German cancer patients, depression and anxiety were found in both groups, but a little higher among uneducated Ethiopian patients (Wondie et al., 2020). Considering the fact that some HIV and cancer patients in LMICs are not able to afford treatment, depression might be high among these group of patients. It is well-established that CYP2B6 genotype is a significant contributor to variability in hydroxybupropion and bupropion levels, influencing the efficacy of bupropion therapy in smoking cessation patients. Knowledge on CYP2B6 genotype in consideration with other factors might give a clue on patients who are likely to benefit from therapy. Constant supply of bupropion could help to reduce relapse among patients in most LMICs. Treatments of other comorbidities that are risk factors of depression have the potential to improve therapy and reduce the number of depressive patients worldwide. There is need to create awareness in the area of mental health via research and innovation, including capacity building, training more mental health staff and psychiatric doctors in LMICs.
Ketamine
Ketamine is a World Health Organization Essential Medicine widely used for perioperative, acute and chronic pain, and sedation. It is used either solely or in combination with opioids for the management of acute post-operative and chronic refractory pain (Laskowski et al., 2011). Its use in the management of status epilepticus, bipolar disorder, suicidal behavior, major depressive disorder and treatment resistant depression has been demonstrated (Yeh et al., 2011; Synowiec et al., 2013; Pizzi et al., 2017; Borsato et al., 2020). Ketamine acts as a non-competitive antagonist of the N-Methyl-D-aspartic acid receptor blocking its action, thereby preventing the development and chronification of pain (Noppers et al., 2010). CYP2B6 is among other enzymes (CYP2C9, CYP3A4) involved in the hepatic N-demethylation of ketamine to norketamine (Yanagihara et al., 2001; Hijazi and Boulieu, 2002; Portmann et al., 2010; Desta et al., 2012; Palacharla et al., 2018). Although ketamine has a large therapeutic window, its use is limited due to low efficacy and huge interindividaul variability in treatment response including ADRs that require cessation of therapy (Kvarnström et al., 2004; Noppers et al., 2010; Laskowski et al., 2011; Hardy et al., 2012; Perez-Ruixo et al., 2020). Ketamine has been associated with increased blood pressure, alteration of speech, muscular discoordination, euphoria, hallucination, loss of consciousness, seizure, nausea, out of body experience, hypothermia, traffic accident or drowning and irrational behavior (Iyalomhe and Iyalomhe, 2014; Lonnée et al., 2018; Gajewski et al., 2020).
Variability in the expression and catalytic activity of CYP2B6 variant enzymes results in differences in the hepatic clearance of ketamine (Wang et al., 2018). Individual differences in hepatic blood flow leading to differences in patient clearance of the drug has also been implicated (Yanagihara et al., 2001). The presence of the CYP2B6*6 allele led to a decrease in the intrinsic clearance of ketamine of up to 89% in human liver microsomes and 55% in cDNA-expressed CYP2B6 protein in vitro (Yanagihara et al., 2001). The CYP2B6*1/*1 (wildtype) genotype confers a 6-fold higher clearance of both enantiomers of ketamine compared to the CYP2B6*6/*6 genotype (Li et al., 2013). In a study involving patients with chronic opioid-refractory pain, the plasma clearance of ketamine was lower in patients with CYP2B6*6/*6 and CYP2B6*1/*6 genotype compared to patients with CYP2B6*1/*1 genotype (Li et al., 2015). Although there were no direct associations between the genotype of the patients and the occurrence of ADRs, drowsiness and hallucination were more often observed in patients with lower clearance than those with higher clearance. The authors hypostatized that higher plasma concentrations due to reduced clearance may have predisposed patients to ketamine ADRs. In vitro studies further demonstrate that CYP2B6 variants confer variability in the metabolism of ketamine. S-ketamine metabolism ranged from CYP2B6*1 (wildtype) > CYP2B6*4 > CYP2B6*26, CYP2B6*19, CYP2B6*17, CYP2B6*6 > CYP2B6*5, CYP2B6*7 > CYP2B6*9, respectively (Wang et al., 2018). This indicates that patients harboring different CYP2B6 variants will respond differently to the drug (Borsato et al., 2020). Genetic variations in CYP2B6 and other CYPs including CYP3A4 might result in different plasma concentration of ketamine and its metabolites. Therefore, knowing the genotype of the patient prior to prescription could help to address individual needs and reduce ADRs.
There is a huge difference in availability and application of anesthesia between high and LMICs as reviewed by Dolman et al. Factors influencing these differences include limited physician anesthesiologists and nurse anesthetists, insufficient anesthesia equipment and infrastructure, patient comorbidities and late presentations (LeBrun et al., 2014; Dohlman, 2017). In LMICs, ketamine is the only anesthetic drug in many hospitals as compared to HICs, where it is used as an adjunct in combination with other anesthetics (Dohlman, 2017). LMICs are lacking in the provision and training for safe anesthesia practice. In a cross-sectional survey made in Zimbabwe involving 42 hospitals, the number of specialist physician anesthetics were limited (Lonnée et al., 2018). Further, 19% of the nurse anesthetists have had no formal training (Lonnée et al., 2018). In Nigeria, intravenous ketamine is used as general anesthesia in parts of the country where anesthesiologist's services are scarce. However, few patients experience adverse effects including high blood pressure, priapism, emergent delirium, tachycardia, disorientation and confusion (Iyalomhe and Iyalomhe, 2014). In a recent survey conducted in Tanzania, Malawi and Zambia, ketamine was widely used in many of the hospitals to compensate for shortages of other forms of anesthesia. Anesthesia care in these countries were performed by non-physician anesthetists, some of whom had no formal training. Shortage of staff, interrupted access to electricity and water for some facilities and lack of functional anesthesia machines were reported (Gajewski et al., 2020). Though ketamine is considered safe, its application by untrained personal might lead to abnormal doses and contribute to adverse effects in these populations.
Methadone
Methadone is a synthetic opioid utilized for the treatment of chronic, acute and neuropathic pain. It is also used as an analgesic to treat pain in cancer patients and as a maintenance therapy for opiate addiction (Chou et al., 2009; Parsons et al., 2010; Kharasch, 2011). In opioid use disorder, methadone reduces the painful symptoms of opiate withdrawal and relieves drug craving by acting on the opioid receptor in the brain. Methadone is administered as a racemate consisting of the S-and R-enantiomers (Crettol et al., 2005; Ansermot et al., 2010). Methadone is metabolized in the liver via N-demethylation performed by various cytochromes including CYP3A4 and CYP2B6. CYP2B6 confers enantioselectivity for the S-enantiomer (Yang et al., 2016), further, the influence of CYP2B6 variants on the S-enantiomer has been reported (Kharasch and Crafford, 2019).
In vitro studies demonstrate differential metabolism and clearance of methadone by CYP2B6 variants ranging from CYP2B6*4 ≥ CYP2B6*1 > CYP2B6*5 > CYP2B6*9 ≥ CYP2B6*6 (Gadel et al., 2015). CYP2B6 genotype influences the plasma levels of both enantiomers (Victorri-Vigneau et al., 2019). Also, decreased clearance and high plasma concentration of methadone enantiomers was observed in patients with CYP2B6*1/*6 and CYP2B6*6/*6 compared to controls (Eap et al., 2007; Kharasch et al., 2015; Kringen et al., 2017; Talal et al., 2020). In a study involving 125 methadone fatality cases, the frequency of CYP2B6*9 was high in the methadone group compared to the control groups. High plasma levels of methadone were observed in individuals with the CYP2B6*5 homozygous genotype compared to the wild type and heterozygous genotype (Ahmad et al., 2017). Studies also show that CYP2B6 genotype influences the severity of neonatal abstinence syndrome (Mactier et al., 2017) in infants of methadone-maintained opioid-dependent mothers. Infants who needed treatment were more likely to carry the wild type genotype for CYP2B6*6 allele (516GG, 785AA) (Mactier et al., 2017). Studies involving Malay opioid dependent males revealed association between CYP2B6*6 and increased severity of pain (Zahari et al., 2016). The presence of concomitant diseases such as HCV infection influence methadone therapy. Reportedly, HCV patients often require higher doses of methadone. Most studies have reported the inability of patients, harboring the CYP2B6*6 allele to metabolize and clear the drug (Crettol et al., 2005; Hung et al., 2011; Bart et al., 2014; Csajka et al., 2016). Thus, patients are likely to experience unwanted effects of the drug. Therefore, dose reduction in this group of patients may yield methadone safety. Meanwhile, others have shown that the CYP2B6*4 allele results in increased metabolism of the drug, thus patients might require increased dose. Patient genotyping for CYP2B6 variants may be of importance when considering dose requirement in methadone maintenance treatment most especially among HCV and HIV patients.
Even though methadone maintenance therapy is effective and affordable, it is still unavailable in many LMICs where it is highly needed. High prevalence of HIV, hepatitis C virus (HCV) and tuberculosis is reported among people with drug use disorder (Wu and Clark, 2013; Larney et al., 2017). As reported in 2018, out of 179 countries with evidence of drug use disorder, opioid substitution therapy (OST) was available in only 86 countries (Avert, 2016; International HR, 2019). OST is a replacement therapy whereby prescribed medications such as methadone and buprenorphine are given to opioid dependent patients, which enables them to reduce or cease from injecting drugs. OST is not found in Nigeria and Zimbabwe despite the presence of drug addicts and HIV patients. However, the Nigerian government has initiated guidelines on the use of methadone for treatment of drug rehabilitation (International HR, 2018). OST is available in South Africa and on a smaller scale in Tanzania, Uganda, Senegal, and is highly expanding in Zanzibar and Kenya (International HR, 2019). In Asia, OST is present in most countries with the highest number in China and the least in Cambodia (International HR, 2019). In Eastern Europe and Central Asia, OST is applied in many countries but coverage is limited. In Western Europe and North American countries, OST is vastly available. However, in Germany opiate substitution treatment is variable between people in prison and those living outside of prison. According to a report by Stöver et al., the application of OST in German prisons depends on the federal state, the prison and prison doctors (Stöver et al., 2019). Existing barriers to accessing OST in both high and LMICs include criminalization and financial barrier, for example, OST is forbidden in Russia and Uzbekistan. Though OST is free in Australia, most people still buy it at a minimum cost of AU35 per week. If people with opiate addiction are not treated, the prevalence of HIV will continue to rise in LMICs. There is a need for more countries to provide OST with good coverage so as to reduce HIV, hepatitis C and mortality among drug users. There is need for the government to provide funds for the health care in some LMICs.
Artemisinin
Artemisinin-based combination therapy (ACT) is the basis of treatment and considered first-line for the majority of malaria infection cases (WHO, 2015). ACT, presently approved for treatment of uncomplicated Plasmodium falciparum malaria in many malaria-endemic countries, are substrates of CYP enzymes (Svensson and Ashton, 1999). Combining artemisinin agents, which are fast acting with a short half-life with partner drugs that have long half-life enables optimization of parasite killing and greatly protects against reinfection (White et al., 2014). Patient's response to antimalarial treatment can be influenced by factors such as quality of the antimalarial agent, the natural immune system of the host, parasite resistance, concomitant diseases and the pharmacokinetics of the malaria drug (Travassos and Laufer, 2009). Most studies on the efficacy of antimalarial agents have focused more on understanding the resistant mechanism of the parasite by investigating the parasites multi drug resistant genes (Travassos and Laufer, 2009). However, studies have shown interindividual variations in the concentration of artimisinin, dihydroartemisinin, artesunate, and their anti-malarial effect among malaria infected individuals. Underdosing seems to enhance parasite resistance to the therapeutic agents. Due to the lack of efficacy, optimization of antimalarial treatment is the main factor considered toward global eradication of the diseases (WHO, 2015).
Among many other factors, host genetics, especially polymorphisms in CYP enzymes involved in the metabolism of the drugs, may be one of the confounders, causing variability in ACT drugs levels and treatment failure. In vitro studies show that artemisinin metabolism in human liver microsomes is mediated primarily by CYP2B6 with a contribution of CYP3A4 in individuals with low expression of CYP2B6 (Svensson and Ashton, 1999). So far, a report from Tanzania indicated their concern about metabolism of ACT and high prevalence of CYP2B6 G516T and other CYP polymorphisms in the population. The prevalence of CYP2B6 G516T in the Tanzanian population was 36% (Marwa et al., 2014). Authors did not evaluate the direct impact of these polymorphisms on treatment outcome or safety of the drugs (Marwa et al., 2014). Another study in the malaria-endemic population of Timor Leste indicated that the prevalence of CYP2B6*4, *9, and *6 might impact the metabolism and efficacy of artemisinin and its derivatives among the Timorians (Hananta et al., 2018). Another study amongst Nigerian HIV-malaria infected subjects explored the impact of CYP2B6 516GT polymorphism on NVR and artemether-lumefantrine drug-drug interaction. The authors showed that decreased exposure to artemether and desbutyl-lumefantrine caused by NVR was further enhanced by patients with CYP2B6 516GG genotype (ultrarapid metabolizers) (Abdullahi et al., 2020). Again, the CYP2B6 516TT genotype (poor metabolizers) also influenced increased exposure to dihydroartemisinin and lumefantrine caused by NVR (Abdullahi et al., 2020). According to the authors, the inductive effect of NRV on CYP2B6 and CYP3A4 enzymes, both of which are involved in the metabolism of these antimalarial drugs, might have caused this variability (Abdullahi et al., 2020). An Iranian study also indicated high prevalence of CYP2B6*2, *4, *5, *6, and *7 alleles among the Iranian Baluchi, which may affect patient response to artemisinin and derivatives (Zakeri et al., 2014).
Limited effort has been employed to determine genetic polymorphisms in CYP enzymes, which may lead to therapeutic failure in patients who are extensive metabolizers or cause toxicity and resistance in patients who are slow metabolizers (Gil, 2013). ACT is an effective treatment for resistant malaria, knowledge on polymorphisms influencing their efficacy may help to improve malaria therapy. The fight against over the counter drugs will help to reduce relapse among patients and improve the lives of people in the rural population.
The quality of malaria care offered in many malaria pandemic LMICs is still very poor, presumption diagnosis is common whereby treatment is provided to patients without any malaria test inspite of the WHO recommendation of “test and treat” (Macarayan et al., 2020). Over the counter poor quality malaria drugs, some of which have no active ingredients, are offered especially by smaller vendors (Bassat et al., 2016; Walker et al., 2018). In Uganda, compared to the urban population, the rural populations spent more money and experienced 97.9% of deaths due to poor quality antimalarial drugs.
Discussion and Future Perspective
CYP2B6 Pharmacogenetics and Drug Response
This article provides evidence on CYP2B6 functional variability in drug metabolism and exposure across populations. The impact of CPY2B6 variant on patient response to various substrates is evident in most ethnicities involved in this study. Depending on CYP2B6 genotype, patients may be vulnerable to ADRs ranging from mild to severe due to increased exposure to active oral drugs, or otherwise experience therapeutic failure due to reduced exposure to active metabolite in the case of prodrugs. Poor metabolizers are likely to experience more ADRs (active compounds) or treatment failure (prodrugs) than intermediate or normal metabolizers. According to literature, CYP2B6*6, which is a haplotype of two variants, CYP2B6*4 and CYP2B6*9, is the most studied allele (Li et al., 2012; Desta et al., 2021). Due to the increasing knowledge on the role of CYP2B6 enzyme in drug metabolism, there is the need to evaluate other CYP2B6 variants on substrate metabolism in various populations or ethnicity. According to the information gathered, some studies considered the G516T (*4) variant as CYP2B6*6 allele, to maintain a common style of variant nomenclature in articles. Researchers can make use of the publicly available pharmacogene variation (PharmVar) website, which clearly defines each haplotype or alleles (Desta et al., 2021). CYP2B6 loss of function alleles (poor metabolizer genotypes), which lead to an increase in individual active drug exposure and toxicity are frequent in some populations leading to high risk of ADRs in these populations.
In order to achieve the Joint United Nations Programme on HIV/AIDS (UNAIDS) 90-90-90 target and complete eradication of AIDS by 2030, pharmacogenetics testing for CYP2B6 to assist EFV therapy in patients who are unlikely to benefit from dolutegravir is of urgent need (Masimirembwa et al., 2016; Mukonzo et al., 2016). The Clinical Pharmacogenetics Implementation Consortium guideline for CYP2B6 and EFV-containing antiretroviral therapy might serve as a basis for implementation of CYP2B6 pharmacogenetic testing for EVF therapy (Desta et al., 2019). This may help to reduce ADRs and increase patient compliance with subsequent reduction in drug resistance due to lack of patient compliance. At the moment, many pharmacogenomics related ADRs are noticed only after the drugs have been administered to the patients. Population specific pharmacogenomics approaches at the level of drug development can be used to address differences in susceptibility to ADRs between populations. The inclusion of pharmacogenomics in clinical trials could give a clue on populations that are likely to benefit or suffer from adverse effects. This could guide dose adjustments for some populations. Previous clinical trials included individuals from African descent to represent the African population, while it is clear that the African continent demonstrates high genetic diversity. Likewise, Asian Americans or Asian Europeans cannot represent the Asian population. Therefore, the inclusion of a diverse population in clinical trials is inevitable. Interestingly, intrapopulation as well as inter-individual variability in CYP2B6 alleles further complicates the efficacy of many of its substrates. This could potentially be improved by the application of patient genotyping prior to prescription in clinical practice. Thus, a robust and more personalized therapy could be provided to the patients.
Availability and Accessibility of Medication
According to our findings, HAART combination therapy that includes EFV or NVP is mostly used in LMICs despite the high frequency of CYP2B6 loss of function alleles in these populations. Thus, pharmacovigilance is urgently needed in these populations for the detection and subsequent prevention of ADRs. Contrary to LMICs, in HICs more potent, less toxic and novel antiretroviral drugs are used quite often. Higher donor dependency and cost of medication has been highlighted as barriers to the accessibility of quality and less toxic drugs in LMICs. Donor funding has saved many lives in LMICs for the past decades. The help from richer countries is provided in the form of finance or medication via Government officials or private agencies in health sectors. With the growing population in LMICs, it is evident that donor funding can no longer benefit every individual. Therefore, in this era, donors should focus more on human capacity building and establishment of infrastructures that will help LMICs become independent or self-sponsored (Pillai et al., 2018). For example, antiretroviral drugs are manufactured and sold at a cheaper rate in India compared to African countries, where drugs are mostly imported at a very high cost (Dickson, 2001). The African pharmaceutical industry, for example, could be expanded and strengthened. This could help to remove financial barriers to medicines as well as to improve access to more potent, expensive, less toxic medication. The public health sector needs to fully support organizations such as the African Pharmacogenomics Consortium (APC), which seeks to address the issue of drug safety, financial problems in the health care sector, disease burden, research training and implementation of pharmacogenomics in Africa (Dandara et al., 2019). There is a need for creating awareness, funding and provision of medication in countries where mental health has been neglected. For example, a significant reduction of heroin use and improvement of mental health was observed among participants who were retained for methadone therapy for 6 months in South Africa (Scheibe et al., 2020).
Health Polices and Patent
There is a need for amendments of foreign and government policies, that limit the growth of health care. According to Tomlinson et al., amending the patent law could improve affordability and accessibility of medicines in South Africa (Tomlinson et al., 2019). The government in LMICs needs to develop strategies to raise internal funds to support health care rather than solely depending on foreign aid. There is a need for allocation of healthcare budgets in both public and private sectors. Additionally, accountability and better amendment of funds in healthcare can help to improve health care services.
Comorbidities
People with two or more diseases need special attention and health care coverage, for example, people with HCV and HIV coinfection. The treatment of HIV might worsen HCV infection in such individuals. Thus, increasing health coverage and accessibility to diagnosis and counseling by trained medical staffs can help patients to receive the right therapy and avoid drug-drug interactions due to concomitant use of HIV and HCV drugs.
Conclusion
In conclusion, there is a high level of CYP2B6 genetic variability between and within ethnicities. In addition to other confounders that can affect the pharmacokinetics and pharmacodynamics properties of a drug, CYP2B6 genotyping could be considered in regards to all CYP2B6 substrates prescriptions in populations with expected high variability and drugs with narrow therapeutic window.
Author Contributions
JS developed the presented idea, supervised the manuscript progress and data analysis, and published own data on CYP2B6 pharmacogenetics. SY, KJ, JB, and CM contributed to the manuscript content, data analysis, and literature search. IL did the systematic review of the literature, evaluated, analyzed the impact of the CYP2B6 alleles on drug safety in a global view, and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Funding
This project has received funding from the European Union's Horizon 2020 research and innovation program under Grant Agreement No. 668353.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Footnotes
1. ^Drugbank. Available online at: https://go.drugbank.com/drugs/DB00625.
2. ^FDA. Available online at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2019/210649Orig1s000TOC.cfm.
3. ^WHO. Available online at: https://digicollections.net/medicinedocs/#/d/s19018en.2010.
4. ^WHO. Tobacco Free Initiative. Available online at: https://www.who.int/tobacco/mpower/en/.
References
Abdullahi, S. T., Soyinka, J. O., Olagunju, A., Bolarinwa, R. A., Olarewaju, O. J., Bakare-Odunola, M. T., et al. (2020). Differential Impact Of Nevirapine On Artemether-Lumefantrine Pharmacokinetics In Individuals Stratified by CYP2B6 c.516G>T genotypes. Antimicrob. Agents Chemother. 64:e00947–19. doi: 10.1128/AAC.00947-19
ACTION Study Group (2017). Policy and priorities for national cancer control planning in low- and middle-income countries: lessons from the Association of Southeast Asian Nations (ASEAN) Costs in Oncology prospective cohort study. Eur. J. Cancer. 74, 26–37. doi: 10.1016/j.ejca.2016.12.014
Agbaji, O., Thio, C. L., Meloni, S., Graham, C., Muazu, M., Nimzing, L., et al. (2013). Impact of hepatitis C virus on HIV response to antiretroviral therapy in Nigeria. J. Acquir. Immune. Defic. Syndr. 62, 204–207. doi: 10.1097/QAI.0b013e31827ce536
Agency, E. M. (2017). Available online at: https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-good-pharmacovigilance-practices-annex-i-definitions-rev-4_en.pdf (accessed October 13, 2017).
Ahmad, T., Sabet, S., Primerano, D. A., Richards-Waugh, L. L., and Rankin, G. O. (2017). Tell-Tale SNPs: the role of CYP2B6 in methadone fatalities. J. Anal. Toxicol. 41, 325–333. doi: 10.1093/jat/bkw135
Aitken, A. E., and Morgan, E. T. (2007). Gene-specific effects of inflammatory cytokines on cytochrome P450 2C, 2B6 and 3A4 mRNA levels in human hepatocytes. Drug Metab. Dispos. 35, 1687–1693. doi: 10.1124/dmd.107.015511
Alhassan, Y., Twimukye, A., Malaba, T., Orrell, C., Myer, L., Waitt, C., et al. (2020). Community acceptability of dolutegravir-based HIV treatment in women: a qualitative study in South Africa and Uganda. BMC Public Health 20:1883. doi: 10.1186/s12889-020-09991-w
Aminkeng, F., Ross, C. J., Rassekh, S. R., Brunham, L. R., Sistonen, J., Dube, M. P., et al. (2014). Higher frequency of genetic variants conferring increased risk for ADRs for commonly used drugs treating cancer, AIDS and tuberculosis in persons of African descent. Pharmacogenomics J. 14, 160–170. doi: 10.1038/tpj.2013.13
Ampadu, H. H., Hoekman, J., de Bruin, M. L., Pal, S. N., Olsson, S., Sartori, D., et al. (2016). Adverse drug reaction reporting in africa and a comparison of individual case safety report characteristics between africa and the rest of the world: analyses of spontaneous reports in VigiBase®. Drug Saf. 39, 335–345. doi: 10.1007/s40264-015-0387-4
Ansermot, N., Albayrak, O., Schläpfer, J., Crettol, S., Croquette-Krokar, M., Bourquin, M., et al. (2010). Substitution of (R,S)-methadone by (R)-methadone: Impact on QTc interval. Arch. Intern. Med. 170, 529–536. doi: 10.1001/archinternmed.2010.26
Ariyoshi, N., Ohara, M., Kaneko, M., Afuso, S., Kumamoto, T., Nakamura, H., et al. (2011). Q172H replacement overcomes effects on the metabolism of cyclophosphamide and efavirenz caused by CYP2B6 variant with Arg262. Drug Metab. Dispos. 39, 2045–2048. doi: 10.1124/dmd.111.039586
Avert (2016). Opioid Substitution Therapy (OST) for HIV Prevention. Available online at: https://www.avert.org/professionals/hiv-programming/prevention/opioid-substitution-therapy (accessed February 15, 2019).
Bachanova, V., Shanley, R., Malik, F., Chauhan, L., Lamba, V., Weisdorf, D. J., et al. (2015). Cytochrome P450 2B6*5 increases relapse after cyclophosphamide-containing conditioning and autologous transplantation for lymphoma. Biol. Blood Marrow Transplant 21, 944–948. doi: 10.1016/j.bbmt.2015.02.001
Bank, P. C. D., Swen, J. J., and Guchelaar, H. J. (2019). Estimated nationwide impact of implementing a preemptive pharmacogenetic panel approach to guide drug prescribing in primary care in The Netherlands. BMC Med. 17:110. doi: 10.1186/s12916-019-1342-5
Bart, G., Lenz, S., Straka, R. J., and Brundage, R. C. (2014). Ethnic and genetic factors in methadone pharmacokinetics: a population pharmacokinetic study. Drug Alcohol Depend. 145, 185–193. doi: 10.1016/j.drugalcdep.2014.10.014
Bassat, Q., Tanner, M., Guerin, P. J., Stricker, K., and Hamed, K. (2016). Combating poor-quality anti-malarial medicines: a call to action. Malar. J. 15:302. doi: 10.1186/s12936-016-1357-8
Batey, M. A., Wright, J. G., Azzabi, A., Newell, D. R., Lind, M. J., Calvert, A. H., et al. (2002). Population pharmacokinetics of adjuvant cyclophosphamide, methotrexate and 5-fluorouracil (CMF). Eur. J. Cancer 38, 1081–1089. doi: 10.1016/S0959-8049(02)00024-2
Batini, C. A. T., Ameer, S., Kolonzo, G., Ozoh, U., and van Zyl Smit, R. (2019). Smoking cessation on the African continent: challenges and opportunities. Afr. J. Thor. Crit. Care Med. 25, 46–48. doi: 10.7196/SARJ.2019.v25i2.015
Bazargani, Y. T., de Boer, A., Schellens, J. H. M., Leufkens, H. G. M., and Mantel-Teeuwisse, A. K. (2015). Essential medicines for breast cancer in low and middle income countries. BMC Cancer 15:591. doi: 10.1186/s12885-015-1583-4
Benowitz, N. L., Zhu, A. Z., Tyndale, R. F., Dempsey, D., and Jacob, P. III. (2013). Influence of CYP2B6 genetic variants on plasma and urine concentrations of bupropion and metabolites at steady state. Pharmacogenet. Genomics. 23, 135–141. doi: 10.1097/FPC.0b013e32835d9ab0
Bielinski, S. J., Olson, J. E., Pathak, J., Weinshilboum, R. M., Wang, L., Lyke, K. J., et al. (2014). Preemptive genotyping for personalized medicine: design of the right drug, right dose, right time-using genomic data to individualize treatment protocol. Mayo Clin. Proc. 89, 25–33. doi: 10.1016/j.mayocp.2013.10.021
Birbal, S., Dheda, M., Ojewole, E., and Oosthuizen, F. (2016). Adverse drug reactions associated with antiretroviral therapy in South Africa. Afr. J. AIDS Res. 15, 243–248. doi: 10.2989/16085906.2016.1191519
Borsato, G. S., Siegel, J. L., Rose, M. Q., Ojard, M., Feyissa, A. M., Quinones-Hinojosa, A., et al. (2020). Ketamine in seizure management and future pharmacogenomic considerations. Pharmacogenomics J. 20, 351–354. doi: 10.1038/s41397-019-0120-2
Bourgi, K., Rebeiro, P. F., Turner, M., Castilho, J. L., Hulgan, T., Raffanti, S. P., et al. (2020). Greater weight gain in treatment-naive persons starting dolutegravir-based antiretroviral therapy. Clin. Infect. Dis. 70, 1267–1274. doi: 10.1093/cid/ciz407
Brathwaite, R., Rocha, T. B.-M., Kieling, C., Kohrt, B. A., Mondelli, V., Adewuya, A. O., et al. (2020). Predicting the risk of future depression among school-attending adolescents in Nigeria using a model developed in Brazil. Psychiatry Res. 294:113511. doi: 10.1016/j.psychres.2020.113511
Bray, J., Sludden, J., Griffin, M. J., Cole, M., Verrill, M., Jamieson, D., et al. (2010). Influence of pharmacogenetics on response and toxicity in breast cancer patients treated with doxorubicin and cyclophosphamide. Br. J. Cancer 102, 1003–1009. doi: 10.1038/sj.bjc.6605587
Brummaier, T., Pohanka, E., Studnicka-Benke, A., and Pieringer, H. (2013). Using cyclophosphamide in inflammatory rheumatic diseases. Eur. J. Intern. Med. 24, 590–596. doi: 10.1016/j.ejim.2013.02.008
Calcagno, A., D'Avolio, A., Simiele, M., Cusato, J., Rostagno, R., Libanore, V., et al. (2012). Influence of CYP2B6 and ABCB1 SNPs on nevirapine plasma concentrations in Burundese HIV-positive patients using dried sample spot devices. Br. J. Clin. Pharmacol. 74, 134–140. doi: 10.1111/j.1365-2125.2012.04163.x
Carr, D. F., Chaponda, M., Cornejo Castro, E. M., Jorgensen, A. L., Khoo, S., Van Oosterhout, J. J., et al. (2014). CYP2B6 c.983T>C polymorphism is associated with nevirapine hypersensitivity in Malawian and Ugandan HIV populations. J. Antimicrob. Chemother. 69, 3329–3334. doi: 10.1093/jac/dku315
Chaivichacharn, P., Avihingsanon, A., Manosuthi, W., Ubolyam, S., Tongkobpetch, S., Shotelersuk, V., et al. (2020). Dosage optimization of efavirenz based on a population pharmacokinetic-pharmacogenetic model of HIV-infected patients in Thailand. Clin. Ther. 42, 1234–1245. doi: 10.1016/j.clinthera.2020.04.013
Chibanda, D., Abas, M., Musesengwa, R., Merritt, C., Sorsdahl, K., Mangezi, W., et al. (2020). Mental health research capacity building in sub-Saharan Africa: the African mental health research initiative. Glob. Ment. Health (Camb) 7:e8. doi: 10.1017/gmh.2019.32
Chou, R., Fanciullo, G. J., Fine, P. G., Adler, J. A., Ballantyne, J. C., Davies, P., et al. (2009). Clinical guidelines for the use of chronic opioid therapy in chronic noncancer pain. J. Pain 10, 113–130. doi: 10.1016/j.jpain.2008.10.008
Ciccacci, C., Borgiani, P., Ceffa, S., Sirianni, E., Marazzi, M. C., Altan, A. M., et al. (2010). Nevirapine-induced hepatotoxicity and pharmacogenetics: a retrospective study in a population from Mozambique. Pharmacogenomics 11, 23–31. doi: 10.2217/pgs.09.142
Ciccacci, C., Di Fusco, D., Marazzi, M. C., Zimba, I., Erba, F., Novelli, G., et al. (2013). Association between CYP2B6 polymorphisms and Nevirapine-induced SJS/TEN: a pharmacogenetics study. Eur. J. Clin. Pharmacol. 69, 1909–1916. doi: 10.1007/s00228-013-1549-x
Clark, S. L., Adkins, D. E., Aberg, K., Hettema, J. M., McClay, J. L., Souza, R. P., et al. (2012). Pharmacogenomic study of side-effects for antidepressant treatment options in STAR*D. Psychol. Med. 42, 1151–1162. doi: 10.1017/S003329171100239X
Cohen, K., Grant, A., Dandara, C., McIlleron, H., Pemba, L., Fielding, K., et al. (2009). Effect of rifampicin-based antitubercular therapy and the cytochrome P450 2B6 516G>T polymorphism on efavirenz concentrations in adults in South Africa. Antivir. Ther. 14, 687–695.
Coles, R., and Kharasch, E. D. (2008). Stereoselective metabolism of bupropion by cytochrome P4502B6 (CYP2B6) and human liver microsomes. Pharm. Res. 25, 1405–1411. doi: 10.1007/s11095-008-9535-1
Crettol, S., Déglon, J. J., Besson, J., Croquette-Krokkar, M., Gothuey, I., Hämmig, R., et al. (2005). Methadone enantiomer plasma levels, CYP2B6, CYP2C19, and CYP2C9 genotypes, and response to treatment. Clin. Pharmacol. Ther. 78, 593–604. doi: 10.1016/j.clpt.2005.08.011
Csajka, C., Crettol, S., Guidi, M., and Eap, C. B. (2016). Population genetic-based pharmacokinetic modeling of methadone and its relationship with the QTc interval in opioid-dependent patients. Clin. Pharmacokinet 55, 1521–1533. doi: 10.1007/s40262-016-0415-2
Dandara, C., Masimirembwa, C., Haffani, Y. Z., Ogutu, B., Mabuka, J., Aklillu, E., et al. (2019). African pharmacogenomics consortium: consolidating pharmacogenomics knowledge, capacity development and translation in Africa: Consolidating pharmacogenomics knowledge, capacity development and translation in Africa. AAS Open Res. 2:19. doi: 10.12688/aasopenres.12965.1
David, S. P., Brown, R. A., Papandonatos, G. D., Kahler, C. W., Lloyd-Richardson, E. E., Munafò, M. R., et al. (2007). Pharmacogenetic clinical trial of sustained-release bupropion for smoking cessation. Nicotine Tob Res. 9, 821–833. doi: 10.1080/14622200701382033
de Jonge, M. E., Huitema, A. D., Rodenhuis, S., and Beijnen, J. H. (2005). Clinical pharmacokinetics of cyclophosphamide. Clin. Pharmacokinet 44, 1135–1164. doi: 10.2165/00003088-200544110-00003
Desta, Z., El-Boraie, A., Gong, L., Somogyi, A. A., Lauschke, V. M., Dandara, C., et al. (2021). PharmVar GeneFocus: CYP2B6. Clin. Pharmacol. Ther. 110, 82–97. doi: 10.1002/cpt.2166
Desta, Z., Gammal, R. S., Gong, L., Whirl-Carrillo, M., Gaur, A. H., Sukasem, C., et al. (2019). Clinical pharmacogenetics implementation consortium (CPIC) guideline for CYP2B6 and efavirenz-containing antiretroviral therapy. Clin. Pharm. Therap. 106, 726–733. doi: 10.1002/cpt.1477
Desta, Z., Moaddel, R., Ogburn, E. T., Xu, C., Ramamoorthy, A., Venkata, S. L., et al. (2012). Stereoselective and regiospecific hydroxylation of ketamine and norketamine. Xenobiotica 42, 1076–1087. doi: 10.3109/00498254.2012.685777
Dhoro, M., Zvada, S., Ngara, B., Nhachi, C., Kadzirange, G., Chonzi, P., et al. (2015). CYP2B6*6, CYP2B6*18, Body weight and sex are predictors of efavirenz pharmacokinetics and treatment response: population pharmacokinetic modeling in an HIV/AIDS and TB cohort in Zimbabwe. BMC Pharm. Toxicol 16:4. doi: 10.1186/s40360-015-0004-2
Dickson, D. (2001). Indian company offers cheap anti-AIDS drugs. Nature 409:751. doi: 10.1038/35057474
Dohlman, L. E. (2017). Providing anesthesia in resource-limited settings. Curr. Opin. Anesthes. 30:477. doi: 10.1097/ACO.0000000000000477
Dolgin, E. (2011). Preemptive genotyping trialed to prevent adverse drug reactions. Nat. Med. 17:1323. doi: 10.1038/nm1111-1323
Drozda, K., Pacanowski, M. A., Grimstein, C., and Zineh, I. (2018). Pharmacogenetic labeling of FDA-approved drugs: a regulatory retrospective. JACC Basic Transl. Sci. 3, 545–549. doi: 10.1016/j.jacbts.2018.06.001
Eap, C. B., Crettol, S., Rougier, J. S., Schläpfer, J., Sintra Grilo, L., Déglon, J. J., et al. (2007). Stereoselective block of hERG channel by (S)-methadone and QT interval prolongation in CYP2B6 slow metabolizers. Clin. Pharmacol. Ther. 81, 719–728. doi: 10.1038/sj.clpt.6100120
Ekins, S., Iyer, M., Krasowski, M. D., and Kharasch, E. D. (2008). Molecular characterization of CYP2B6 substrates. Curr. Drug Metab. 9, 363–373. doi: 10.2174/138920008784746346
Ekins, S., Vandenbranden, M., Ring, B. J., Gillespie, J. S., Yang, T. J., Gelboin, H. V., et al. (1998). Further characterization of the expression in liver and catalytic activity of CYP2B6. J. Pharmacol. Exp. Ther. 286, 1253–1259.
Eniu, A., Cherny, N. I., Bertram, M., Thongprasert, S., Douillard, J.-Y., Bricalli, G., et al. (2019). Cancer medicines in Asia and Asia-Pacific: what is available, and is it effective enough? ESMO Open 4:e000483. doi: 10.1136/esmoopen-2018-000483
Evans, W. E., and Relling, M. V. (2004). Moving towards individualized medicine with pharmacogenomics. Nature 429, 464–468. doi: 10.1038/nature02626
Falk, M. K., Thunell, L., Nahi, H., and Gréen, H. (2012). Association of CYP2B6 genotype with survival and progression free survival in cyclophosphamide treated multiple myeloma. J. Cancer Ther. 3, 20–7. doi: 10.4236/jct.2012.31003
Faucette, S. R., Wang, H., Hamilton, G. A., Jolley, S. L., Gilbert, D., Lindley, C., et al. (2004). Regulation of CYP2B6 in primary human hepatocytes by prototypical inducers. Drug Metab. Dispos. 32, 348–358. doi: 10.1124/dmd.32.3.348
Fava, M., Rush, A. J., Thase, M. E., Clayton, A., Stahl, S. M., Pradko, J. F., et al. (2005). 15 years of clinical experience with bupropion HCl: from bupropion to bupropion SR to bupropion XL. Prim Care Companion J. Clin. Psychiatry 7, 106–113. doi: 10.4088/PCC.v07n0305
Fernandez, F. M., Hostetler, D., Powell, K., Kaur, H., Green, M. D., Mildenhall, D. C., et al. (2011). Poor quality drugs: grand challenges in high throughput detection, countrywide sampling, and forensics in developing countries. Analyst 136, 3073–82. doi: 10.1039/C0AN00627K
Gadel, S., Friedel, C., and Kharasch, E. D. (2015). Differences in methadone metabolism by CYP2B6 variants. Drug Metab. Dispos. 43, 994–1001. doi: 10.1124/dmd.115.064352
Gajewski, J., Pittalis, C., Lavy, C., Borgstein, E., Bijlmakers, L., Mwapasa, G., et al. (2020). Anesthesia capacity of district-level hospitals in malawi, tanzania, and zambia: a mixed-methods study. Anesth. Analg. 130, 845–853. doi: 10.1213/ANE.0000000000004363
GHO/WHO (2007). Available online at: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/gho-tobacco-offerhelp-medication-bupropion-place-available-2018 (accessed May 28, 2020).
Giacomelli, A., Rusconi, S., Falvella, F. S., Oreni, M. L., Cattaneo, D., Cozzi, V., et al. (2018). Clinical and genetic determinants of nevirapine plasma trough concentration. SAGE Open Med. 6:2050312118780861. doi: 10.1177/2050312118780861
Giardina, C., Cutroneo, P. M., Mocciaro, E., Russo, G. T., Mandraffino, G., Basile, G., et al. (2018). Adverse drug reactions in hospitalized patients: results of the FORWARD (Facilitation of Reporting in Hospital Ward) Study. Front. Pharm. 9:350. doi: 10.3389/fphar.2018.00350
Gil, J. P. (2013). Malaria pharmacogenomics: return to the future. Pharmacogenomics 14, 707–710. doi: 10.2217/pgs.13.41
Gokengin, D., Oprea, C., Begovac, J., Horban, A., Zeka, A. N., Sedlacek, D., et al. (2018). HIV care in Central and Eastern Europe: how close are we to the target? Int. J. Infect. Dis. 70, 121–130. doi: 10.1016/j.ijid.2018.03.007
Gounden, V., van Niekerk, C., Snyman, T., and George, J. A. (2010). Presence of the CYP2B6 516G> T polymorphism, increased plasma Efavirenz concentrations and early neuropsychiatric side effects in South African HIV-infected patients. AIDS Res. Ther. 7:32. doi: 10.1186/1742-6405-7-32
Griskevicius, L., Yasar, U., Sandberg, M., Hidestrand, M., Eliasson, E., Tybring, G., et al. (2003). Bioactivation of cyclophosphamide: the role of polymorphic CYP2C enzymes. Eur. J. Clin. Pharmacol. 59, 103–109. doi: 10.1007/s00228-003-0590-6
Hananta, L., Astuti, I., Sadewa, A. H., Alice, J., Hutagalung, J., and Mustofa. (2018). The prevalence of CYP2B6 gene polymorphisms in malaria-endemic Population of Timor in East Nusa Tenggara Indonesia. Osong Public Health Res. Perspect. 9, 192–196. doi: 10.24171/j.phrp.2018.9.4.08
Hanna, I. H., Reed, J. R., Guengerich, F. P., and Hollenberg, P. F. (2000). Expression of human cytochrome P450 2B6 in Escherichia coli: characterization of catalytic activity and expression levels in human liver. Arch. Biochem. Biophys. 376, 206–216. doi: 10.1006/abbi.2000.1708
Hardy, J., Quinn, S., Fazekas, B., Plummer, J., Eckermann, S., Agar, M., et al. (2012). Randomized, double-blind, placebo-controlled study to assess the efficacy and toxicity of subcutaneous ketamine in the management of cancer pain. J. Clin. Oncol. 30, 3611–3617. doi: 10.1200/JCO.2012.42.1081
Helsby, N. A., Hui, C. Y., Goldthorpe, M. A., Coller, J. K., Soh, M. C., Gow, P. J., et al. (2010). The combined impact of CYP2C19 and CYP2B6 pharmacogenetics on cyclophosphamide bioactivation. Br. J. Clin. Pharmacol. 70, 844–853. doi: 10.1111/j.1365-2125.2010.03789.x
Hesse, L. M., He, P., Krishnaswamy, S., Hao, Q., Hogan, K., von Moltke, L. L., et al. (2004). Pharmacogenetic determinants of interindividual variability in bupropion hydroxylation by cytochrome P450 2B6 in human liver microsomes. Pharmacogenetics 14, 225–238. doi: 10.1097/00008571-200404000-00002
Hidestrand, M., Oscarson, M., Salonen, J. S., Nyman, L., Pelkonen, O., Turpeinen, M., et al. (2001). CYP2B6 and CYP2C19 as the major enzymes responsible for the metabolism of selegiline, a drug used in the treatment of Parkinson's disease, as revealed from experiments with recombinant enzymes. Drug Metab. Dispos. 29, 1480–1484.
Hijazi, Y., and Boulieu, R. (2002). Contribution of CYP3A4, CYP2B6, and CYP2C9 isoforms to N-demethylation of ketamine in human liver microsomes. Drug Metab. Dispos. 30, 853–858. doi: 10.1124/dmd.30.7.853
Hofmann, M. H., Blievernicht, J. K., Klein, K., Saussele, T., Schaeffeler, E., Schwab, M., et al. (2008). Aberrant splicing caused by single nucleotide polymorphism c.516G>T [Q172H], a marker of CYP2B6*6, is responsible for decreased expression and activity of CYP2B6 in liver. J. Pharmacol. Exp. Ther. 325, 284–292. doi: 10.1124/jpet.107.133306
Hung, C. C., Chiou, M. H., Huang, B. H., Hsieh, Y. W., Hsieh, T. J., Huang, C. L., et al. (2011). Impact of genetic polymorphisms in ABCB1, CYP2B6, OPRM1, ANKK1 and DRD2 genes on methadone therapy in Han Chinese patients. Pharmacogenomics 12, 1525–1533. doi: 10.2217/pgs.11.96
International HR (2018). Global State of Harm Reduction. Available online at: https://www.hri.global/global-state-harm-reduction-2018
International HR (2019). Global State of Harm Reduction: 2019 Updates. Available online at: https://www.hri.global/global-state-of-harm-reduction-2019
Iyalomhe, G., and Iyalomhe, S. (2014). Intravenous ketamine anaesthesia: a 20-year experience in a sub-urban hospital in nigeria. Int. J. Med. Appl. Sci. 3:2014.
Johnson, G. G., Lin, K., Cox, T. F., Oates, M., Sibson, D. R., Eccles, R., et al. (2013). CYP2B6*6 is an independent determinant of inferior response to fludarabine plus cyclophosphamide in chronic lymphocytic leukemia. Blood 122, 4253–4258. doi: 10.1182/blood-2013-07-516666
Jorenby, D. E., Leischow, S. J., Nides, M. A., Rennard, S. I., Johnston, J. A., Hughes, A. R., et al. (1999). A controlled trial of sustained-release bupropion, a nicotine patch, or both for smoking cessation. N. Engl. J. Med. 340, 685–691. doi: 10.1056/NEJM199903043400903
Kanwar, N. S. R., Sharma, D. D., Ramesh, M. K., and Mokta, J. K. (2019). Prevalence of psychiatric comorbidity among patients of type 2 diabetes mellitus in a hilly state of North India. Ind. J. Endocr. Metab. 602:23. doi: 10.4103/ijem.IJEM_521_19
Kharasch, E. D. (2011). Intraoperative methadone: rediscovery, reappraisal, and reinvigoration? Anesth. Analg. 112, 13–16. doi: 10.1213/ANE.0b013e3181fec9a3
Kharasch, E. D., and Crafford, A. (2019). Common polymorphisms of CYP2B6 influence stereoselective bupropion disposition. Clin. Pharmacol. Ther. 105, 142–152. doi: 10.1002/cpt.1116
Kharasch, E. D., and Greenblatt, D. J. (2019). Methadone disposition: implementing lessons learned. J. Clin. Pharm. 59, 1044–1048. doi: 10.1002/jcph.1427
Kharasch, E. D., Regina, K. J., Blood, J., and Friedel, C. (2015). Methadone pharmacogenetics: CYP2B6 polymorphisms determine plasma concentrations, clearance, and metabolism. Anesthesiology 123, 1142–1153. doi: 10.1097/ALN.0000000000000867
Kidia, K., Machando, D., Mangezi, W., Hendler, R., Crooks, M., Abas, M., et al. (2017). Mental health in Zimbabwe: a health systems analysis. Lancet Psychiatry 4, 876–886. doi: 10.1016/S2215-0366(17)30128-1
Kim, G. J., Lee, S. Y., Park, J. H., Ryu, B. Y., and Kim, J. H. (2017). Role of preemptive genotyping in preventing serious adverse drug events in South Korean patients. Drug Saf 40, 65–80. doi: 10.1007/s40264-016-0454-5
Kirchheiner, J., Klein, C., Meineke, I., Sasse, J., Zanger, U. M., Mürdter, T. E., et al. (2003). Bupropion and 4-OH-bupropion pharmacokinetics in relation to genetic polymorphisms in CYP2B6. Pharmacogenetics 13, 619–626. doi: 10.1097/00008571-200310000-00005
Kouanfack, C., Mpoudi-Etame, M., Omgba Bassega, P., Eymard-Duvernay, S., Leroy, S., Boyer, S., et al. (2019). Dolutegravir-based or low-dose efavirenz-based regimen for the treatment of HIV-1. N. Engl. J. Med. 381, 816–826. doi: 10.1056/NEJMoa1904340
Kringen, M. K., Chalabianloo, F., Bernard, J. P., Bramness, J. G., Molden, E., and Høiseth, G. (2017). Combined effect of CYP2B6 genotype and other candidate genes on a steady-state serum concentration of methadone in opioid maintenance treatment. Ther. Drug Monit. 39, 550–555. doi: 10.1097/FTD.0000000000000437
Kvarnström, A., Karlsten, R., Quiding, H., and Gordh, T. (2004). The analgesic effect of intravenous ketamine and lidocaine on pain after spinal cord injury. Acta Anaesthesiol. Scand. 48, 498–506. doi: 10.1111/j.1399-6576.2003.00330.x
Labarga, P., Soriano, V., Vispo, M. E., Pinilla, J., Martin-Carbonero, L., Castellares, C., et al. (2007). Hepatotoxicity of antiretroviral drugs is reduced after successful treatment of chronic hepatitis C in HIV-infected patients. J. Infect. Dis. 196, 670–676. doi: 10.1086/520092
Laib, A. K., Brünen, S., Pfeifer, P., Vincent, P., and Hiemke, C. (2014). Serum concentrations of hydroxybupropion for dose optimization of depressed patients treated with bupropion. Ther. Drug Monit. 36, 473–479. doi: 10.1097/FTD.0000000000000042
Lang, T., Klein, K., Fischer, J., Nüssler, A. K., Neuhaus, P., Hofmann, U., et al. (2001). Extensive genetic polymorphism in the human CYP2B6 gene with impact on expression and function in human liver. Pharmacogenetics 11, 399–415. doi: 10.1097/00008571-200107000-00004
Langhaug, L. F., Jack, H., Hanlon, C., Holzer, S., Sorsdahl, K., Mutedzi, B., et al. (2020). “We need more big trees as well as the grass roots”: going beyond research capacity building to develop sustainable careers in mental health research in African countries. Int. J. Ment. Health Syst. 14:66. doi: 10.1186/s13033-020-00388-1
Larney, S., Peacock, A., Leung, J., Colledge, S., Hickman, M., Vickerman, P., et al. (2017). Global, regional, and country-level coverage of interventions to prevent and manage HIV and hepatitis C among people who inject drugs: a systematic review. Lancet Glob. Health 5:e1208–e20. doi: 10.1016/S2214-109X(17)30373-X
Laskowski, K., Stirling, A., McKay, W. P., and Lim, H. J. (2011). A systematic review of intravenous ketamine for postoperative analgesia. Can. J. Anaesth. 58, 911–923. doi: 10.1007/s12630-011-9560-0
LeBrun, D. G., Chackungal, S., Chao, T. E., Knowlton, L. M., Linden, A. F., Notrica, M. R., et al. (2014). Prioritizing essential surgery and safe anesthesia for the Post-2015 Development Agenda: operative capacities of 78 district hospitals in 7 low- and middle-income countries. Surgery 155, 365–373. doi: 10.1016/j.surg.2013.10.008
Lee, A. M., Jepson, C., Hoffmann, E., Epstein, L., Hawk, L. W., Lerman, C., et al. (2007). CYP2B6 genotype alters abstinence rates in a bupropion smoking cessation trial. Biol. Psychiatry 62, 635–641. doi: 10.1016/j.biopsych.2006.10.005
Lee, W., Tirona, R. G., and Kim, R. B. (2003). Localization of the distal enhancer elements conferring synergistic activation of the human CYP2B6 gene by the constitutive androstane receptor and hepatocyte nuclear factor 4α. Clin. Pharm. Therap. 73:P60–P. doi: 10.1016/S0009-9236(03)90580-7
Lewis, D. F., and Lake, B. G. (1997). Molecular modelling of mammalian CYP2B isoforms and their interaction with substrates, inhibitors and redox partners. Xenobiotica 27, 443–478. doi: 10.1080/004982597240433
Li, J., Menard, V., Benish, R. L., Jurevic, R. J., Guillemette, C., Stoneking, M., et al. (2012). Worldwide variation in human drug-metabolism enzyme genes CYP2B6 and UGT2B7: implications for HIV/AIDS treatment. Pharmacogenomics 13, 555–570. doi: 10.2217/pgs.11.160
Li, Y., Coller, J. K., Hutchinson, M. R., Klein, K., Zanger, U. M., Stanley, N. J., et al. (2013). The CYP2B6*6 allele significantly alters the N-demethylation of ketamine enantiomers in vitro. Drug Metab. Dispos. 41, 1264–1272. doi: 10.1124/dmd.113.051631
Li, Y., Jackson, K. A., Slon, B., Hardy, J. R., Franco, M., William, L., et al. (2015). CYP2B6*6 allele and age substantially reduce steady-state ketamine clearance in chronic pain patients: impact on adverse effects. Br. J. Clin. Pharmacol. 80, 276–284. doi: 10.1111/bcp.12614
Liptrott, N. J., Penny, M., Bray, P. G., Sathish, J., Khoo, S. H., Back, D. J., et al. (2009). The impact of cytokines on the expression of drug transporters, cytochrome P450 enzymes and chemokine receptors in human PBMC. Br. J. Pharmacol. 156, 497–508. doi: 10.1111/j.1476-5381.2008.00050.x
Lo, R., Burgoon, L., Macpherson, L., Ahmed, S., and Matthews, J. (2010). Estrogen receptor-dependent regulation of CYP2B6 in human breast cancer cells. Biochim. Biophys. Acta 1799, 469–479. doi: 10.1016/j.bbagrm.2010.01.005
Lonnée, H. A., Madzimbamuto, F., Erlandsen, O. R. M., Vassenden, A., Chikumba, E., Dimba, R., et al. (2018). Anesthesia for cesarean delivery: a cross-sectional survey of provincial, district, and mission hospitals in Zimbabwe. Anesth. Analg. 126, 2056–2064. doi: 10.1213/ANE.0000000000002733
Lonsdale, J., Thomas, J., Salvatore, M., Phillips, R., Lo, E., Shad, S., et al. (2013). The genotype-tissue expression (GTEx) project. Nat. Gen. 45, 580–585. doi: 10.1038/ng.2653
Lynch, T., and Price, A. (2007). The effect of cytochrome P450 metabolism on drug response, interactions, and adverse effects. Am. Fam. Physic. 76, 391–396.
Macarayan, E., Papanicolas, I., and Jha, A. (2020). The quality of malaria care in 25 low-income and middle-income countries. BMJ Glob Health 5:e002023. doi: 10.1136/bmjgh-2019-002023
Mactier, H., McLaughlin, P., Gillis, C., and Osselton, M. D. (2017). Variations in infant CYP2B6 genotype associated with the need for pharmacological treatment for neonatal abstinence syndrome in infants of methadone-maintained opioid-dependent mothers. Am. J. Perinatol. 34, 918–921. doi: 10.1055/s-0037-1600917
Manosuthi, W., Sukasem, C., Lueangniyomkul, A., Mankatitham, W., Thongyen, S., Nilkamhang, S., et al. (2013). Impact of pharmacogenetic markers of CYP2B6, clinical factors, and drug-drug interaction on efavirenz concentrations in HIV/tuberculosis-coinfected patients. Antimicrob. Agents Chemother. 57, 1019–1024. doi: 10.1128/AAC.02023-12
Marwa, K. J., Schmidt, T., Sjögren, M., Minzi, O. M. S., Kamugisha, E., and Swedberg, G. (2014). Cytochrome P450 single nucleotide polymorphisms in an indigenous Tanzanian population: a concern about the metabolism of artemisinin-based combinations. Malar. J. 13:420. doi: 10.1186/1475-2875-13-420
Masimirembwa, C., Dandara, C., and Leutscher, P. D. (2016). Rolling out efavirenz for HIV precision medicine in Africa: are we ready for pharmacovigilance and tackling neuropsychiatric adverse effects? Omics 20, 575–580. doi: 10.1089/omi.2016.0120
Mayston, R., Frissa, S., Tekola, B., Hanlon, C., Prince, M., and Fekadu, A. (2020). Explanatory models of depression in sub-Saharan Africa: synthesis of qualitative evidence. Soc. Sci. Med. 246:112760. doi: 10.1016/j.socscimed.2019.112760
Mehlotra, R. K., Ziats, M. N., Bockarie, M. J., and Zimmerman, P. A. (2006). Prevalence of CYP2B6 alleles in malaria-endemic populations of West Africa and Papua New Guinea. Eur. J. Clin. Pharmacol. 62, 267–275. doi: 10.1007/s00228-005-0092-9
Mhandire, D., Lacerda, M., Castel, S., Mhandire, K., Zhou, D., Swart, M., et al. (2015). Effects of CYP2B6 and CYP1A2 genetic variation on nevirapine plasma concentration and pharmacodynamics as measured by CD4 cell count in Zimbabwean HIV-infected patients. Omics 19, 553–562. doi: 10.1089/omi.2015.0104
Morales-Pérez, M. (2021). Adverse reactions to antiretrovirals in cuban patients living with HIV/AIDS. Medicc Rev 23:21. doi: 10.37757/MR2021.V23.N2.7
Mukonzo, J. K., Bisaso, R. K., Ogwal-Okeng, J., Gustafsson, L. L., Owen, J. S., and Aklillu, E. (2016). CYP2B6 genotype-based efavirenz dose recommendations during rifampicin-based antituberculosis cotreatment for a sub-Saharan Africa population. Pharmacogenomics 17, 603–613. doi: 10.2217/pgs.16.7
Mukonzo, J. K., Okwera, A., Nakasujja, N., Luzze, H., Sebuwufu, D., Ogwal-Okeng, J., et al. (2013). Influence of efavirenz pharmacokinetics and pharmacogenetics on neuropsychological disorders in Ugandan HIV-positive patients with or without tuberculosis: a prospective cohort study. BMC Infect. Dis 13:261. doi: 10.1186/1471-2334-13-261
Nampala, H., Luboobi, L. S., Mugisha, J. Y. T., Obua, C., and Jablonska-Sabuka, M. (2018). Modelling hepatotoxicity and antiretroviral therapeutic effect in HIV/HBV coinfection. Math. Biosci. 302, 67–79. doi: 10.1016/j.mbs.2018.05.012
Ndashimye, E., and Arts, E. J. (2019). The urgent need for more potent antiretroviral therapy in low-income countries to achieve UNAIDS 90-90-90 and complete eradication of AIDS by (2030). Infect. Dis. Poverty 8:63. doi: 10.1186/s40249-019-0573-1
Nebert, D. W., Wikvall, K., and Miller, W. L. (2013). Human cytochromes P450 in health and disease. Philos. Trans. R Soc. Lond. B Biol. Sci. 368:20120431. doi: 10.1098/rstb.2012.0431
Newton, P. N., Green, M. D., and Fernández, F. M. (2010). Impact of poor-quality medicines in the 'developing' world. Trends Pharmacol. Sci. 31, 99–101. doi: 10.1016/j.tips.2009.11.005
Noppers, I., Niesters, M., Aarts, L., Smith, T., Sarton, E., and Dahan, A. (2010). Ketamine for the treatment of chronic non-cancer pain. Expert. Opin. Pharmacother. 11, 2417–2429. doi: 10.1517/14656566.2010.515978
Oyinlade, A. (2017). Kehinde ENA, Isaac Abah. Drug utilization patterns of antidepressants in Federal Neuro-Psychiatric Hospital Lagos, Nigeria. J. Hosp. Administ. 6:99. doi: 10.5430/jha.v6n5p12
Palacharla, R. C., Nirogi, R., Uthukam, V., Manoharan, A., Ponnamaneni, R. K., and Kalaikadhiban, I. (2018). Quantitative in vitro phenotyping and prediction of drug interaction potential of CYP2B6 substrates as victims. Xenobiotica 48, 663–675. doi: 10.1080/00498254.2017.1354267
Parsons, H. A., de la Cruz, M., El Osta, B., Li, Z., Calderon, B., Palmer, J. L., et al. (2010). Methadone initiation and rotation in the outpatient setting for patients with cancer pain. Cancer 116, 520–528. doi: 10.1002/cncr.24754
Patel, T. K., and Patel, P. B. (2018). Mortality among patients due to adverse drug reactions that lead to hospitalization: a meta-analysis. Eur. J. Clin. Pharmacol. 74, 819–832. doi: 10.1007/s00228-018-2441-5
Paterson, N. E., Balfour, D. J., and Markou, A. (2007). Chronic bupropion attenuated the anhedonic component of nicotine withdrawal in rats via inhibition of dopamine reuptake in the nucleus accumbens shell. Eur. J. Neurosci. 25, 3099–3108. doi: 10.1111/j.1460-9568.2007.05546.x
Paula, D. P., do Brasil Costa, V. I., Jorge, R. V., and Nobre, F. F. (2020). Impact of protocol change on individual factors related to course of adverse reactions to chemotherapy for breast cancer. Suppor. Care Cancer 28, 395–403. doi: 10.1007/s00520-019-04841-x
Pearce, R. E., Gaedigk, R., Twist, G. P., Dai, H., Riffel, A. K., Leeder, J. S., et al. (2016). Developmental expression of CYP2B6: a comprehensive analysis of mRNA expression, protein content and bupropion hydroxylase activity and the impact of genetic variation. Drug Metab. Dispos. 44, 948–958. doi: 10.1124/dmd.115.067546
Perez-Ruixo, C., Rossenu, S., Zannikos, P., Nandy, P., Singh, J., Drevets, W. C., et al. (2020). Population pharmacokinetics of esketamine nasal spray and its metabolite noresketamine in healthy subjects and patients with treatment-resistant depression. Clin. Pharmacok. 60, 501–516. doi: 10.1007/s40262-020-00953-4
Pharmgkb (2000). Available online at: https://www.pharmgkb.org/chemical/PA448687/clinicalAnnotation
Pillai, G., Chibale, K., Constable, E. C., Keller, A. N., Gutierrez, M. M., Mirza, F., et al. (2018). The Next Generation Scientist program: capacity-building for future scientific leaders in low- and middle-income countries. BMC Med. Educ. 18:233. doi: 10.1186/s12909-018-1331-y
Pizzi, M. A., Kamireddi, P., Tatum, W. O., Shih, J. J., Jackson, D. A., and Freeman, W. D. (2017). Transition from intravenous to enteral ketamine for treatment of nonconvulsive status epilepticus. J. Intensive Care 5:54. doi: 10.1186/s40560-017-0248-6
Portmann, S., Kwan, H. Y., Theurillat, R., Schmitz, A., Mevissen, M., and Thormann, W. (2010). Enantioselective capillary electrophoresis for identification and characterization of human cytochrome P450 enzymes which metabolize ketamine and norketamine in vitro. J. Chromatogr. A 1217, 7942–7948. doi: 10.1016/j.chroma.2010.06.028
Raccor, B. S., Claessens, A. J., Dinh, J. C., Park, J. R., Hawkins, D. S., Thomas, S. S., et al. (2012). Potential contribution of cytochrome P450 2B6 to hepatic 4-hydroxycyclophosphamide formation in vitro and in vivo. Drug Metab. Dispos. 40, 54–63. doi: 10.1124/dmd.111.039347
Rajman, I., Knapp, L., Morgan, T., and Masimirembwa, C. (2017). African genetic diversity: implications for cytochrome p450-mediated drug metabolism and drug development. EBioMedicine 17, 67–74. doi: 10.1016/j.ebiom.2017.02.017
Rakhmanina, N. Y., and van den Anker, J. N. (2010). Efavirenz in the therapy of HIV infection. Expert Opin. Drug Metab. Toxicol. 6, 95–103. doi: 10.1517/17425250903483207
Rendic, S. (2002). Summary of information on human CYP enzymes: human P450 metabolism data. Drug Metab. Rev. 34, 83–448. doi: 10.1081/DMR-120001392
Renner, L., Nkansah, F. A., and Dodoo, A. N. (2013). The role of generic medicines and biosimilars in oncology in low-income countries. Ann. Oncol. 24(Suppl. 5):v29–32. doi: 10.1093/annonc/mdt326
Rocha, V., Porcher, R., Fernandes, J. F., Filion, A., Bittencourt, H., Silva, W. Jr., et al. (2009). Association of drug metabolism gene polymorphisms with toxicities, graft-versus-host disease and survival after HLA-identical sibling hematopoietic stem cell transplantation for patients with leukemia. Leukemia 23, 545–556. doi: 10.1038/leu.2008.323
Roy, P., Yu, L. J., Crespi, C. L., and Waxman, D. J. (1999). Development of a substrate-activity based approach to identify the major human liver P-450 catalysts of cyclophosphamide and ifosfamide activation based on cDNA-expressed activities and liver microsomal P-450 profiles. Drug Metab. Dispos. 27, 655–666.
Ruff, P., Al-Sukhun, S., Blanchard, C., and Shulman, L. N. (2016). Access to cancer therapeutics in low- and middle-income countries. Am. Soc. Clin. Oncol. Educ. Book 2016, 58–65. doi: 10.1200/EDBK_155975
Sankoh, O., Sevalie, S., and Weston, M. (2018). Mental health in Africa. Lancet Global Health 6, e954–e5. doi: 10.1016/S2214-109X(18)30303-6
Sarfo, F. S., Zhang, Y., Egan, D., Tetteh, L. A., Phillips, R., Bedu-Addo, G., et al. (2014). Pharmacogenetic associations with plasma efavirenz concentrations and clinical correlates in a retrospective cohort of Ghanaian HIV-infected patients. J. Antimicrob. Chemother. 69, 491–499. doi: 10.1093/jac/dkt372
Sax, P. E., Erlandson, K. M., Lake, J. E., McComsey, G. A., Orkin, C., Esser, S., et al. (2020). Weight gain following initiation of antiretroviral therapy: risk factors in randomized comparative clinical trials. Clin. Infect. Dis. 71, 1379–1389. doi: 10.1093/cid/ciz999
Scheibe, A., Shelly, S., Gerardy, T., von Homeyer, Z., Schneider, A., Padayachee, K., et al. (2020). Six-month retention and changes in quality of life and substance use from a low-threshold methadone maintenance therapy programme in Durban, South Africa. Addict. Sci. Clin. Practice 15:13. doi: 10.1186/s13722-020-00186-7
Schipani, A., Wyen, C., Mahungu, T., Hendra, H., Egan, D., Siccardi, M., et al. (2011). Integration of population pharmacokinetics and pharmacogenetics: an aid to optimal nevirapine dose selection in HIV-infected individuals. J. Antimicrob. Chemoth. 66, 1332–1339. doi: 10.1093/jac/dkr087
Schnoll, R. A., and Lerman, C. (2006). Current and emerging pharmacotherapies for treating tobacco dependence. Expert. Opin. Emerg. Drugs 11, 429–444. doi: 10.1517/14728214.11.3.429
Schurig, A. M., Böhme, M., Just, K. S., Scholl, C., Dormann, H., Plank-Kiegele, B., et al. (2018). Adverse Drug Reactions (ADR) and emergencies. Dtsch. Arztebl. Int. 115, 251–258. doi: 10.3238/arztebl.2018.0251
Sevko, A., Sade-Feldman, M., Kanterman, J., Michels, T., Falk, C. S., Umansky, L., et al. (2013). Cyclophosphamide promotes chronic inflammation-dependent immunosuppression and prevents antitumor response in melanoma. J. Invest. Dermatol. 133, 1610–1619. doi: 10.1038/jid.2012.444
Shu, W., Chen, L., Hu, X., Zhang, M., Chen, W., Ma, L., et al. (2017). Cytochrome P450 genetic variations can predict mRNA expression, cyclophosphamide 4-hydroxylation, and treatment outcomes in chinese patients with non-hodgkin's lymphoma. J. Clin. Pharmacol. 57, 886–898. doi: 10.1002/jcph.878
Siedner, M. J., Moorhouse, M. A., Simmons, B., de Oliveira, T., Lessells, R., Giandhari, J., et al. (2020). Reduced efficacy of HIV-1 integrase inhibitors in patients with drug resistance mutations in reverse transcriptase. Nat. Commun. 11:5922. doi: 10.1038/s41467-020-19801-x
Srivastava, A., Lian, L.-Y., Maggs, J. L., Chaponda, M., Pirmohamed, M., Williams, D. P., et al. (2010). Quantifying the metabolic activation of nevirapine in patients by integrated applications of NMR and mass spectrometries. Drug Metab. Dispos. 38, 122–132. doi: 10.1124/dmd.109.028688
Stingl, J. C., Brockmöller, J., and Viviani, R. (2013). Genetic variability of drug-metabolizing enzymes: the dual impact on psychiatric therapy and regulation of brain function. Mol. Psychiatry 18, 273–287. doi: 10.1038/mp.2012.42
Stöver, H., Jamin, D., Michels, I. I., Knorr, B., Keppler, K., and Deimel, D. (2019). Opioid substitution therapy for people living in German prisons—inequality compared with civic sector. Harm. Reduct. J. 16:72. doi: 10.1186/s12954-019-0340-4
Su, S., Fairley, C. K., Sasadeusz, J., He, J., Wei, X., Zeng, H., et al. (2018). HBV, HCV, and HBV/HCV co-infection among HIV-positive patients in Hunan province, China: Regimen selection, hepatotoxicity, and antiretroviral therapy outcome. J. Med. Virol. 90, 518–525. doi: 10.1002/jmv.24988
Svensson, U. S., and Ashton, M. (1999). Identification of the human cytochrome P450 enzymes involved in the in vitro metabolism of artemisinin. Br. J. Clin. Pharmacol. 48, 528–535. doi: 10.1046/j.1365-2125.1999.00044.x
Synowiec, A. S., Singh, D. S., Yenugadhati, V., Valeriano, J. P., Schramke, C. J., and Kelly, K. M. (2013). Ketamine use in the treatment of refractory status epilepticus. Epilepsy Res. 105, 183–188. doi: 10.1016/j.eplepsyres.2013.01.007
Talal, A. H., Ding, Y., Venuto, C. S., Chakan, L. M., McLeod, A., Dharia, A., et al. (2020). Toward precision prescribing for methadone: Determinants of methadone deposition. PLoS ONE. 15:e0231467. doi: 10.1371/journal.pone.0231467
Thorn, C. F., Lamba, J. K., Lamba, V., Klein, T. E., and Altman, R. B. (2010). PharmGKB summary: very important pharmacogene information for CYP2B6. Pharmacog. Genomics 20, 520–523. doi: 10.1097/FPC.0b013e32833947c2
Tomaz, P. R., Santos, J. R., Issa, J. S., Abe, T. O., Gaya, P. V., Krieger, J. E., et al. (2015). CYP2B6 rs2279343 polymorphism is associated with smoking cessation success in bupropion therapy. Eur. J. Clin. Pharmacol. 71, 1067–1073. doi: 10.1007/s00228-015-1896-x
Tomlinson, C., Waterhouse, C., Hu, Y. Q., Meyer, S., and Moyo, H. (2019). How patent law reform can improve affordability and accessibility of medicines in South Africa: Four medicine case studies. South Afr. Med. J. 109:14001. doi: 10.7196/SAMJ.2019.v109i6.14001
Travassos, M. A., and Laufer, M. K. (2009). Resistance to antimalarial drugs: molecular, pharmacologic, and clinical considerations. Pediatric Res. 65, 64–70. doi: 10.1203/PDR.0b013e3181a0977e
Ugochukwu, O., Mbaezue, N., Lawal, S. A., Azubogu, C., Sheikh, T. L., and Vallières, F. (2020). The time is now: reforming Nigeria's outdated mental health laws. Lancet Global Health 8, e989–e90. doi: 10.1016/S2214-109X(20)30302-8
Uttayamakul, S., Likanonsakul, S., Manosuthi, W., Wichukchinda, N., Kalambaheti, T., Nakayama, E. E., et al. (2010). Effects of CYP2B6 G516T polymorphisms on plasma efavirenz and nevirapine levels when co-administered with rifampicin in HIV/TB co-infected Thai adults. AIDS Res. Ther. 7:8. doi: 10.1186/1742-6405-7-8
Vardhanabhuti, S., Acosta, E. P., Ribaudo, H. J., Severe, P., Lalloo, U., Kumarasamy, N., et al. (2013). Clinical and genetic determinants of plasma nevirapine exposure following an intrapartum dose to prevent mother-to-child HIV transmission. J. Infect. Dis. 208, 662–671. doi: 10.1093/infdis/jit223
Victorri-Vigneau, C., Verstuyft, C., Bouquié, R, Laforgue, E.-J., Hardouin, J.-B., Leboucher, J., et al. (2019). Relevance of CYP2B6 and CYP2D6 genotypes to methadone pharmacokinetics and response in the OPAL study. Br. J. Clin. Pharm. 85, 1538–1543. doi: 10.1111/bcp.13936
Vitoria, M., Hill, A., Ford, N., Doherty, M., Clayden, P., Venter, F., et al. (2018). The transition to dolutegravir and other new antiretrovirals in low-income and middle-income countries: what are the issues? Aids 32, 1551–1561. doi: 10.1097/QAD.0000000000001845
Walker, E. J., Peterson, G. M., Grech, J., Paragalli, E., and Thomas, J. (2018). Are we doing enough to prevent poor-quality antimalarial medicines in the developing world? BMC Public Health 18:630. doi: 10.1186/s12889-018-5521-7
Wang, H., Faucette, S., Sueyoshi, T., Moore, R., Ferguson, S., Negishi, M., et al. (2003b). A novel distal enhancer module regulated by pregnane X receptor/constitutive androstane receptor is essential for the maximal induction of CYP2B6 gene expression. J. Biol. Chem. 278, 14146–14152. doi: 10.1074/jbc.M212482200
Wang, H., Faucette, S. R., Gilbert, D., Jolley, S. L., Sueyoshi, T., Negishi, M., et al. (2003a). Glucocorticoid receptor enhancement of pregnane X receptor-mediated CYP2B6 regulation in primary human hepatocytes. Drug Metab. Dispos. 31, 620–630. doi: 10.1124/dmd.31.5.620
Wang, P. F., Neiner, A., and Kharasch, E. D. (2018). Stereoselective ketamine metabolism by genetic variants of cytochrome P450 CYP2B6 and cytochrome P450 oxidoreductase. Anesthesiology 129, 756–768. doi: 10.1097/ALN.0000000000002371
Wang, P. F., Neiner, A., and Kharasch, E. D. (2020). Stereoselective bupropion hydroxylation by cytochrome P450 CYP2B6 and cytochrome P450 oxidoreductase genetic variants. Drug Metab. Dispos. 48, 438–445. doi: 10.1124/dmd.119.090407
Weinshilboum, R. (2003). Inheritance and drug response. N. Engl. J. Med. 348, 529–537. doi: 10.1056/NEJMra020021
White, N. J., Pukrittayakamee, S., Hien, T. T., Faiz, M. A., Mokuolu, O. A., and Dondorp, A. M. (2014). Malaria. Lancet 383, 723–735. doi: 10.1016/S0140-6736(13)60024-0
WHO (2015). Guidelines for the Treatment of Malaria - Third edition. 3rd edn. World Health Orgnaization, Regional Office for Africa, 316.
WHO (2017). Available online at: https://digicollections.net/medicinedocs/#d/s23533en (accessed July, 2017).
Wondie, Y., Mehnert, A., and Hinz, A. (2020). The hospital anxiety and depression scale (HADS) applied to Ethiopian cancer patients. PLoS ONE 15:e0243357. doi: 10.1371/journal.pone.0243357
Wu, P. Y., Cheng, C. Y., Liu, C. E., Lee, Y. C., Yang, C. J., Tsai, M. S., et al. (2017). Multicenter study of skin rashes and hepatotoxicity in antiretroviral-naïve HIV-positive patients receiving non-nucleoside reverse-transcriptase inhibitor plus nucleoside reverse-transcriptase inhibitors in Taiwan. PLoS ONE 12:e0171596. doi: 10.1371/journal.pone.0171596
Wu, Z., and Clark, N. (2013). Scaling up opioid dependence treatment in low- and middle-income settings. Bull. World Health Organ 91:82–A. doi: 10.2471/BLT.12.110783
Xie, H. J., Yasar, U., Lundgren, S., Griskevicius, L., Terelius, Y., Hassan, M., et al. (2003). Role of polymorphic human CYP2B6 in cyclophosphamide bioactivation. Pharmacogenomics J. 3, 53–61. doi: 10.1038/sj.tpj.6500157
Yanagihara, Y., Kariya, S., Ohtani, M., Uchino, K., Aoyama, T., Yamamura, Y., et al. (2001). Involvement of CYP2B6 in n-demethylation of ketamine in human liver microsomes. Drug Metab. Dispos. 29, 887–890.
Yang, H. C., Chu, S. K., Huang, C. L., Kuo, H. W., Wang, S. C., Liu, S. W., et al. (2016). Genome-wide pharmacogenomic study on methadone maintenance treatment identifies SNP rs17180299 and multiple haplotypes on CYP2B6, SPON1, and GSG1L associated with plasma concentrations of methadone R- and S-enantiomers in heroin-dependent patients. PLoS Genet 12:e1005910. doi: 10.1371/journal.pgen.1005910
Yeh, P. S., Shen, H. N., and Chen, T. Y. (2011). Oral ketamine controlled refractory nonconvulsive status epilepticus in an elderly patient. Seizure 20, 723–726. doi: 10.1016/j.seizure.2011.06.001
Yimer, G., Ueda, N., Habtewold, A., Amogne, W., Suda, A., Riedel, K.-D., et al. (2011). Pharmacogenetic & pharmacokinetic biomarker for efavirenz based ARV and rifampicin based anti-TB drug induced liver injury in TB-HIV infected patients. PLoS ONE 6:e27810. doi: 10.1371/journal.pone.0027810
Yoon, H. Y., Cho, Y. A., Yee, J., and Gwak, H. S. (2020). Effects of CYP2B6 polymorphisms on plasma nevirapine concentrations: a systematic review and meta-analysis. Sci. Rep. 10:17390. doi: 10.1038/s41598-020-74506-x
Zahari, Z., Lee, C. S., Ibrahim, M. A., Musa, N., Mohd Yasin, M. A., Lee, Y. Y., et al. (2016). Relationship between CYP2B6*6 and cold pressor pain sensitivity in opioid dependent patients on methadone maintenance therapy (MMT). Drug Alcohol Depend 165, 143–150. doi: 10.1016/j.drugalcdep.2016.05.028
Zakeri, S., Amiri, N., Pirahmadi, S., and Dinparast Djadid, N. (2014). Genetic variability of CYP2B6 polymorphisms in southeast Iranian population: implications for malaria and HIV/AIDS treatment. Arch. Iran Med. 17, 685–691.
Zanger, U. M., and Schwab, M. (2013). Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharm. Therap. 138, 103–141. doi: 10.1016/j.pharmthera.2012.12.007
Zanger, U. M., Turpeinen, M., Klein, K., and Schwab, M. (2008). Functional pharmacogenetics/genomics of human cytochromes P450 involved in drug biotransformation. Anal. Bioanal. Chem. 392, 1093–1108. doi: 10.1007/s00216-008-2291-6
Zash, R., Holmes, L., Diseko, M., Jacobson, D. L., Brummel, S., Mayondi, G., et al. (2019). Neural-tube defects and antiretroviral treatment regimens in botswana. N. Engl. J. Med. 381, 827–840. doi: 10.1056/NEJMoa1905230
Zhang, Y. J., Li, M. P., Tang, J., and Chen, X. P. (2017). Pharmacokinetic and pharmacodynamic responses to clopidogrel: evidences and perspectives. Int. J. Environ. Res. Public Health 14:301. doi: 10.3390/ijerph14030301
Keywords: drug metabolism, adverse drug reaction, cytochrome P450 2B6, genetic polymorphism, drug safety, pharmacogenetics, pharmacogenomics, personalized medicine
Citation: Langmia IM, Just KS, Yamoune S, Brockmöller J, Masimirembwa C and Stingl JC (2021) CYP2B6 Functional Variability in Drug Metabolism and Exposure Across Populations—Implication for Drug Safety, Dosing, and Individualized Therapy. Front. Genet. 12:692234. doi: 10.3389/fgene.2021.692234
Received: 07 April 2021; Accepted: 14 June 2021;
Published: 12 July 2021.
Edited by:
Jasmine Luzum, University of Michigan, United StatesReviewed by:
Alessandra Campos-Staffico, University of Michigan, United StatesJai Narendra Patel, Levine Cancer Institute, United States
Copyright © 2021 Langmia, Just, Yamoune, Brockmöller, Masimirembwa and Stingl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia C. Stingl, anN0aW5nbEB1a2FhY2hlbi5kZQ==