 Alberto Pilotto
Alberto Pilotto Daniele Sancarlo2
Daniele Sancarlo2 Julia Daragjati
Julia Daragjati Francesco Panza
Francesco Panza- 1Geriatrics Unit, Azienda ULSS 16 Padova, Hospital S. Antonio, Padova, Italy
- 2Geriatric Unit, Laboratory of Gerontology and Geriatrics, Department of Medical Sciences, IRCCS “Casa Sollievo della Sofferenza”, San Giovanni Rotondo, Foggia, Italy
- 3Neurodegenerative Disease Unit, Department of Basic Medicine, Neuroscience, and Sense Organs, University of Bari Aldo Moro, Bari, Italy
A complex decision path with a careful evaluation of the risk–benefit ratio is mandatory for drug treatment in advanced age. Enrollment biases in randomized clinical trials (RCTs) cause an under-representation of older individuals. In high-risk frail older subjects, the lack of RCTs makes clinical decision-making particularly difficult. Frail individuals are markedly susceptible to adverse drug reactions, and frailty may result in reduced treatment efficacy. Life expectancy should be included in clinical decision-making paths to better assess the benefits and risks of different drug treatments in advanced age. We performed a scoping review of principal hospital- and community-based prognostic indices in older age. Mortality prognostic tools could help clinical decision-making in diagnostics and therapeutics, tailoring appropriate intervention for older patients. The effectiveness of drug treatments may be significantly different in older patients with different risk of mortality. Clinicians need to consider the prognostic information obtained through well-validated, accurate, and calibrated predictive tools to identify those patients who may benefit from drug treatments given with the aim of increasing survival.
Evidence-Based Medicine in Older Age
Drug treatment in advanced age is achieved through a complex decision path requiring a careful evaluation of the risk–benefit ratio. Age-related changes in response to drugs can arise from pharmacokinetic and pharmacodynamic differences. However, age itself is not the only factor that could affect pharmacokinetic and pharmacodynamic responses to drugs in older people. Although guidelines pertaining to the inclusion of older participants in randomized clinical trials (RCTs) have existed for more than two decades (1), different studies and systematic reviews suggested ongoing enrollment biases with under-representation of older individuals especially in clinical trials of cardiovascular diseases (2–4) and cancer (5, 6). In fact, older adults remain underrepresented in clinical trials of patients hospitalized with an acute coronary syndrome (2) or in ongoing RCTs regarding heart failure (3), while a very recent systematic review found that no RCTs of statin or any other hypocholesterolemic medication included persons older than 82 years at baseline (4). On the same vein, from 2007 to June 2010, 24 drugs were approved for the treatment of cancer, and, on average, only 33% of patients included in the registration trials were aged 65 years or older (6), down from the 36% reported from 1992 to 2002 (5).
Conducting RCTs with older adults can be challenging for various reasons including an increased prevalence of multiple comorbidities and polypharmacy. It is well known that due to these factors, the line between benefit and harm caused by drug treatments is really thin in older subjects and not easily evaluable in routine clinical practice. Indeed, numerous clinical trials excluded patients with comorbidities such as kidney failure, hypertension, and diabetes, all of which increase in prevalence with advancing age. Moreover, even in the absence of specific age- or disease-based exclusion criteria, older subjects suffering from multiple comorbidities, with polypharmacy, physical disability, functional and cognitive impairments, malnutrition, a low familiar and social care network, or a reduced life expectancy are usually excluded from RCTs (7). While the exclusion of older subjects from RCTs is often understandable from the standpoint of completing a study safely and efficiently, the results of studies that include a very narrow, highly selected subset of subjects and exclude most of the older high-risk patients may be less generalizable to patients cared outside of the context of clinical trials. This situation may lead to uncertainty and confusion in clinical decision-making of the older people.
Beyond clinical decision-making for drug treatment in older age, prognostic information can be very useful to make a decision before high-risk interventions such as major surgery (8), particularly to prevent institutionalization, a second fracture in institutionalized patients, and decrease mortality after a hip fracture (9). In fact, the decision to proceed with surgery in the frail older adult requires careful deliberation to determine whether surgical management is preferable to alternative approaches (8). Older patients considering surgery should undergo a Comprehensive Geriatric Assessment (CGA)-based preoperative assessment, including an evaluation of comorbidities and functional, cognitive, and nutritional conditions (8). A number of tools are available to facilitate individualized preoperative risk assessment such as the American Society of Anesthesiologists (ASA) grade (10) or more comprehensive systems including the Physiological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM) (11) and its modifications (the Portsmouth or P-POSSUM), the Simplified Acute Physiology Score II (SAPS II) (12), and the Acute Physiology and Chronic Health Evaluation II (APACHE II) score (13). However, there are no geriatric-specific tools and no single instrument incorporates every important geriatric variable (8). A recent narrative review found that multidomain phenotype frailty was associated with increased risk for operative mortality (8). Therefore, for example, the Waterlow score, a tool used to stratify the risk of pressure sores and a marker of frailty has been recently compared with the ASA and the P-POSSUM to predict post-operative mortality and morbidity risk in older surgical patients obtaining good discrimination and accuracy (14). In the present article, we performed a scoping review of principal hospital- and community-based prognostic indices in older age, with a focus on drug treatment.
Clinical Decisions in Older Adults: The Role of Frailty and Prognosis
The lack of RCTs in older subjects makes clinical decisions particularly difficult and not always appropriated, as they are based mostly on indirect data obtained from adult or younger subjects with characteristics really dissimilar from the majority of older subjects. Therefore, there is an urgent need to implement the scientific evidence in clinical practice permitting to drive more appropriately clinical decisions in older subjects, especially frail subjects with higher mortality risk. In fact, the concept of frailty, as a marker of reduced physiologic reserve, may have direct relevance to clinical care, and clearly identifies a population at greater risk of adverse health outcomes, including institutionalization, hospitalization, and death (15).
Recent epidemiological data suggested that frailty is common among critically ill patients and represents a prognostic determinant of survival and health resource utilization (16). Indeed, frail individuals are particularly susceptible to adverse drug reactions (ADRs) (17, 18), and frailty may also result in reduced treatment efficacy (19). For example, treating hypertension in healthy, robust patients older than 80 years resulted in reduced mortality and cardiovascular disease end points, but the benefits were not seen if the older patients were frail (19). The recognition of frail older subjects therefore may enable improved prognostication and shared decision-making and identify vulnerable subgroups with specific needs who might benefit from follow-up and personalized interventions. Indeed, in order to better assess the benefits and risks of different drug treatments and thus provide an health care service as close as possible to the real needs of the patients, avoiding over or underutilization of therapeutic interventions, recent guidelines recommend including life expectancy in clinical decision-making paths (20). The ultimate aim is the identification of subjects who will really benefit from a specific therapeutic intervention avoiding futile diagnostic testing (over-diagnosis) as well as surgical/invasive procedures, which do not add value and may cause harm (overtreatment o mistreatment). This action, in addition, will allow the avoidance of time- and cost-consuming medical interventions in older subjects not receiving any advantage or in fact likely displaying a higher risk of ADRs (20).
Clinical prediction rules (CPRs) (also called clinical decision rules, prediction models, prognostic tools, and risk scores) are tools designed to assist clinical decision-making. CPRs generally provide an estimate of the risk of disease, disease outcome, or the benefit of a diagnostic or therapeutic action. Recently, great attention has been paid to the proper identification of mortality prognostic tools that could help clinical decision-making in diagnostics and therapeutics to tailor appropriate intervention for the patient (21). While several risk prediction models have often been developed and validated in different populations and for different outcomes, the prognostic performance of the most popular and widely used risk models in terms of discrimination, calibration, generalizability, and reclassification is largely unknown (22). This is particularly important in advanced age due to the frequent presence of multiple comorbidities and functional deficits directly and/or indirectly affecting life expectancy.
Multidimensional Assessment and Prognosis
There is a large and increasing body of evidence indicating that the prognosis of older patients is strongly related to the presence of concomitant diseases and to the degree of physical, cognitive, biological, and social impairment (23). The CGA, capable to effectively exploring these multiple domains of health, is indeed the multidimensional and multidisciplinary tool of choice to determine the prognosis of the functionally compromised and frail older subject (24). Initially, the “first generation” instruments for the CGA had specific targets, and were applied to specific older populations with the aim to identify and stratify the risk in predetermined clinical settings, such as older patients with depression, cognitive impairment, or physical disability. More recently, new multidimensional instruments have been introduced, creating global scores including several items that permitted to explore several different aspects of different pathologies and reassuming them in a single, standardized, and simple numerical score, assessing the global impairment of the subject that expressed the risk of health negative outcomes such as institutionalization, hospitalization, or death. Examples of these cumulative CGA-based indices are the Frailty Index-CGA (FI-CGA) (25) and the Multidimensional Prognostic Index (MPI) (26, 27) that could be useful in identifying high-risk older subjects. In particular, the FI-CGA was a 10-domain multidimensional instrument useful to assess mild, moderate, and severe frailty (25), while the 8-domain MPI was developed and validated to predict low, moderate, and severe risk of all-cause mortality (26, 27). These tools are mainly based on a list of risk factors that are mentioned to be of great importance to the concept of frailty (28), including the physical dimension (nutritional status, physical activity, mobility, strength, and energy), the psychological dimension (cognition and mood), and the social dimension (lack of social contacts and social support). These frailty/prognostic instruments are multidimensional in nature, and mostly based on a standardized CGA. A recent systematic review evaluated the clinimetric properties of 20 frailty instruments, i.e., the accuracy including discrimination and calibration, generalizability, feasibility in clinical practice, potential bias, and the possibility to be used as outcome measures (29). Unfortunately, the overall results of the assessment by using these frailty instruments suggested that they are mainly developed and validated as risk assessment tools, and not as possible outcome measures and none of these indices has been validated as predictive tool in clinical decision-making of older people (29).
The Prognostic Indices in Older Age
Hospital-Based Setting
A recent large systematic review identified, from a total number of over 21,000 titles examined, a small number of prognostic indices for mortality that meet the requirements of accuracy and calibration required to be used in a clinical setting involving hospitalized older patients (eight indices), living in nursing homes (two indices), and living in their own homes (six indices) (30). Among the eight indices selected in the hospital-based setting, only four tools estimated 1-year mortality on admission: (1) the CARING index based on four pre-specified predictors (31); (2) the Burden of Illness Score for Elderly Persons based on functional and laboratory data added to diagnoses from administrative data (32); (3) the Hospitalized Elder Longitudinal Project (HELP) survival model (33), a nomogram developed in medicine and intensive care units patients older than 80 years based on clinical information including the APACHE III scale, which requires arterial blood gas measurement; and (4) the MPI (26, 27). The MPI was the only one CGA-based predictive tool to be included in this list. None of the examined indices had accuracy excellent, i.e., a c-statistic value ≥0.9; moreover, for the CARING index, no c-statistic was reported for the external validation (31), and the Burden of Illness Score for Elderly Persons model was well calibrated at the extremes, but was less accurate in middle risk groups (32).
Among these indices used in hospital-based setting, the MPI, originally developed and validated in two independent cohorts of older patients hospitalized for acute illnesses or exacerbations of chronic diseases (26), has been identified as a tool well-calibrated (<10% of variation between the estimated and the observed mortality rates), with a good discrimination as well as with an accuracy that is maintained both at 1 month [C-index 0.76, 95% confidence intervals (CI) = 0.73–0.79] (27) and 1 year (C-index 0.75, 95% CI = 0.71–0.80) of follow-up (26) (Table 1). Among the totality of non-disease-specific prognostic indices described in this systematic review (30), the MPI was the only tool based on information obtained from a CGA exploring comprehensively health conditions (multiple comorbidities, medications, risk of pressure sores), functional (basal and instrumental activities of daily living) cognitive, and nutritional aspects as well as co-habitation status using standardized rating scales extensively validated and widely used in the aged population. The multidimensional approach as a key criterion in defining the clinical outcome in older subjects was also confirmed by studies showing the higher prognostic mortality value of MPI compared to the value displayed by the individual parameters used to build the MPI.
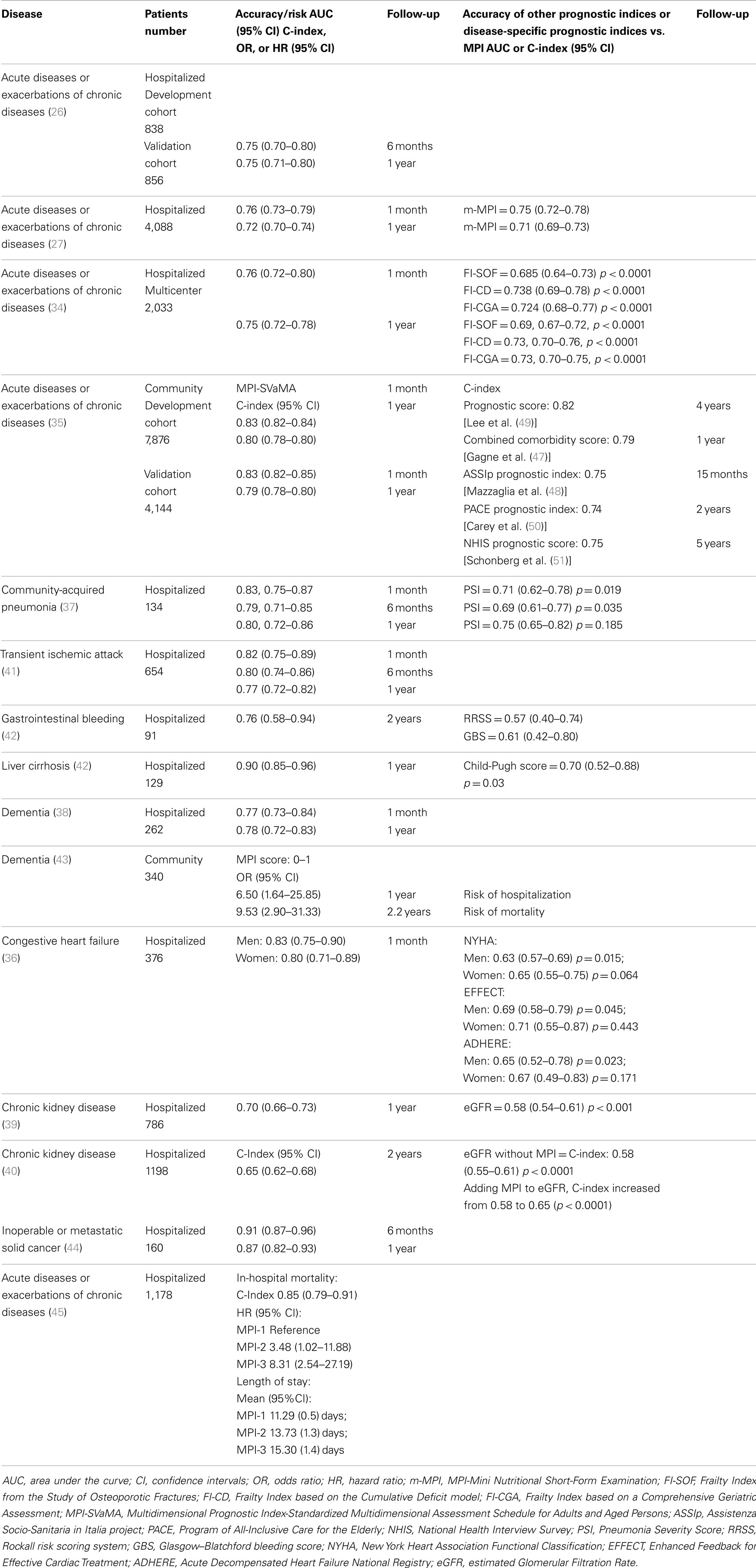
Table 1. Clinical studies of development and validation of the Multidimensional Prognostic Index (MPI) and predictive values against different disease-specific prognostic indices.
The MPI has been validated in over 12,000 older hospitalized patients suffering from major diseases leading to death in older subjects including gastrointestinal bleeding (42), liver cirrhosis (42), community-acquired pneumonia (37), dementia (38), congestive heart failure (36), chronic kidney disease (39, 40), transient ischemic attack (41), and cancer (44), showing also a greater predictive power for all-cause mortality than disease-specific indices for most of these conditions (36, 37, 42) (Table 1). In addition, a prospective multicenter study involving over 2,000 hospitalized older patients recruited in 20 Geriatric Units has shown that MPI was a significantly more accurate predictor of short- and long-term all-cause mortality than other three frailty indices commonly used in clinical practice (34), including the FI-CGA (25) (Table 1). Also, very recently, in a prospective study of 1,178 older patients admitted to 20 Geriatrics units, MPI score assessed at hospital admission was an independent predictor of in-hospital mortality and the length of hospital stay (45) (Table 1). Finally, the MPI in older hospitalized patients has been significantly associated to other outcomes including re-hospitalization rates and discharge destination (homes vs. nursing homes) (46), substantially improving the usefulness of this tool for resource planning purposes.
Community-Based Setting
Several prognostic instruments that estimated mortality risk from 1 to 5 years have been described and validated in community-dwelling older populations. Most of these tool are based only on comorbidity score (47), while other instruments are self-reported questionnaires that evaluated functional status, age, and gender (48–50), and also the presence of multiple comorbidities (51). In community-dwelling cohorts, other indicators, more related to the pre-disability concept of frailty and to physical performance, have demonstrated a very powerful prediction of mortality, i.e., gait speed (52). Very recently, a version of the MPI, based on information collected through the Standardized Multidimensional Assessment Schedule for Adults and Aged Persons (SVaMA) has been developed and validated in two large and independent cohorts of community-dwelling older subjects (35). This MPI-SVaMA showed a very good prognostic accuracy to predict 1-month (survival C-index of 0.83) and 1-year mortality (survival C-index of 0.79) with an excellent calibration. Compared to other prognostic indices, the MPI-SVaMA differs in some crucial points: (1) the MPI-SVaMA was the only prognostic tool completely based on a CGA; (2) all data were collected directly by a multidisciplinary team, including doctors, a social worker, and a nurse; (3) no participant was excluded on the basis of incapacity of self-report; and (4) the clinical and functional scores used to calculate the prognostic index have been specifically developed and validated in older subjects. Indeed, although considering the intrinsic limitation of an indirect comparison among different prognostic instruments, the MPI-SVaMA demonstrated comparable (47, 49) or higher (48, 50, 51) discrimination as determined by the survival C-index values (Table 1). Very recently, findings from the Treviso Dementia (TREDEM) Study demonstrated that the MPI was effective also in assessing the risk of all-cause mortality and hospitalization in 340 outpatients evaluated in a tertiary care center for cognitive impairment (43) (Table 1).
Notably, the MPI showed to be an outcome measure sensitive to the antidepressant treatment in late-life major depressive disorder (MDD), suggesting an impact of selective serotonin reuptake inhibitors also on measures linked to multidimensional impairment and all-cause mortality, with a clear improvement of the MPI linked to the antidepressant treatment in older outpatients with late-life MDD (53). Furthermore, in a very recent pilot study, the integrated treatment of rivastigmine transdermal patch (RTP) plus cognitive stimulation in Alzheimer’s disease (AD) patients for 6 months improved significantly cognition, depressive and neuropsychiatric symptoms, functional status, and mortality risk assessed with the MPI in comparison with a group of AD patients receiving only RTP, confirming the possible role of this multidimensional CGA-based index as an outcome measures also in dementia (54). Therefore, the MPI score was sensitive to variations of the subject health over time in outpatients (53, 54) and hospital-based setting (45), strongly supporting the concept that considering multidimensional aggregate information could be the basis of interventions in older age.
Prognosis and Risk–Benefit Evaluation of Drug Treatment in Older Age
Despite a great number of prognostic indices for mortality has been developed and validated, there is currently no evidence that their routine use may improve patient outcomes. Indeed, previous studies reported that the combined approach including life expectancies obtained from life tables with clinical and functional judgments by physicians can facilitate clinical decision-making in older persons (55, 56). With full access to prognostic information derived from accurate and validated predictive tools, physicians will be better equipped to make clinical decisions that are aligned with their patients’ needs in terms of safety and efficacy. For example, the decision to treat with anticoagulants older frail patients with atrial fibrillation (AF) is particularly difficult due to the high risk of serious side effects and low compliance of this treatment. Indeed, data on subjects with AF have shown that older patients with different risk of mortality are generally treated differently from each other (57). A recent retrospective observational study on almost 1300 community-dwelling frail patients aged 65 years and older with a previous hospitalization for AF, confirmed that higher MPI-SVaMA scores were associated with lower rates of warfarin treatment and higher mortality. However, a significant association between anticoagulant treatment and increased survival at 3 years of follow-up was found to be independent from age and multidimensional impairment. In fact, the analyses for heterogeneity suggested that the effect of warfarin treatment was not different among the three MPI-SVaMA groups (58).
Similarly, the clinical decision-making for the administration of statins to older patients with cardio- and cerebrovascular disease is under debate (4), with little evidence to support or refute benefit, particularly in frail older patients with comorbidity and high mortality risk. Recently, a retrospective observational study in patients aged 65 years and older with or without statin treatment, demonstrated that higher mortality risk, assessed by the MPI-SVaMA score, was associated with lower rates of statin prescription. Nonetheless, statin use was significantly associated with reduced 3-year mortality in all MPI-SVaMA-risk classes, suggesting that increased survival associated with statins in frail older patients with cardio- and cerebrovascular disease was independent of age and mortality risk (59).
Future Research in the Field
Age distribution of patients should be representative in studies presented for marketing authorization, and collection of data from all possible sources might also be required to consolidate knowledge regarding higher-risk subpopulations. While evidence from RCTs is used to determine the efficacy of a treatment or intervention under ideal conditions, studies of observational designs are used to measure the effectiveness of an intervention in non-experimental, “real world” scenarios. Indeed, a very recent Cochrane review assessing the impact of study design on the effect measures estimated suggested that there was little evidence for significant effect estimate differences between observational studies and RCTs, regardless of specific observational study design, heterogeneity, or inclusion of studies of pharmacological interventions (60). Therefore, preliminary data from observational studies on anticoagulant and statin treatment suggested that it is time to develop clinical trials designed specifically for frail older adults (58, 59), until today not included in RCTs as a result of comorbidity or functional status. These trials might be tailored to include novel dosing schemes, alternative end points such as the impact of therapy on quality of life, cognitive or physical function, and multidimensional assessment tools to assess functional independence, family support, and also insurance coverage in older individuals (61). Unfortunately, at present, although non-disease-specific prognostic indices for older adults hold the promise of improving the targeting of interventions in advanced age, there is insufficient evidence to recommend the widespread use of prognostic indices in clinical practice (30). Large prospective trials that randomize clinicians to using these tools or not, demonstrating their impact on prognostic estimates, clinical decision-making, and patient outcomes have not been performed. Future studies are needed to independently test the accuracy of these prognostic tools in heterogeneous populations and their ability to improve clinical outcomes before their widespread use can be recommended. In conclusion, the risk of mortality may influence the effectiveness of a specific treatment in older patients. Clinicians need to consider the prognostic information obtained through well validated, accurate, and calibrated predictive tools to identify those patients who may benefit from drug treatments given with the aim of increasing survival.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Center for the Study of Drugs Likely to be Used in the Elderly. Guideline for the Study of Drugs Likely to be used in the Elderly. Washington, DC: US Department of Health and Human Services (1989).
2. Dodd KS, Saczynski JS, Zhao Y, Goldberg RJ, Gurwitz JH. Exclusion of older adults and women from recent trials of acute coronary syndromes. J Am Geriatr Soc (2011) 59(3):506–11. doi: 10.1111/j.1532-5415.2010.03305.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
3. Cherubini A, Oristrell J, Pla X, Ruggiero C, Ferretti R, Diestre G, et al. The persistent exclusion of older patients from ongoing clinical trials regarding heart failure. Arch Intern Med (2011) 171(6):550–6. doi:10.1001/archinternmed.2011.31
4. Strandberg TE, Kolehmainen L, Vuorio A. Evaluation and treatment of older patients with hypercholesterolemia: a clinical review. JAMA (2014) 312(11):1136–44. doi:10.1001/jama.2014.10924
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
5. Talarico L, Chen G, Pazdur R. Enrollment of elderly patients in clinical trials for cancer drug registration: a 7-year experience by the US Food and Drug Administration. J Clin Oncol (2004) 22(22):4626–31. doi:10.1200/JCO.2004.02.175
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
6. Scher KS, Hurria A. Under-representation of older adults in cancer registration trials: known problem, little progress. J Clin Oncol (2012) 30(17):2036–8. doi:10.1200/JCO.2012.41.6727
7. Crome P, Lally F, Cherubini A, Oristrell J, Beswick AD, Clarfield AM, et al. Exclusion of older people from clinical trials: professional views from nine European countries participating in the PREDICT study. Drugs Aging (2011) 28(8):667–77. doi:10.2165/11591990-000000000-00000
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
8. Oresanya LB, Lyons WL, Finlayson E. Preoperative assessment of the older patient: a narrative review. JAMA (2014) 311(20):2110–20. doi:10.1001/jama.2014.4573
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
9. Martinez-Reig M, Ahmad L, Duque G. The orthogeriatrics model of care: systematic review of predictors of institutionalization and mortality in post-hip fracture patients and evidence for interventions. J Am Med Dir Assoc (2012) 13(9):770–7. doi:10.1016/j.jamda.2012.07.011
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
10. Mak PH, Campbell RC, Irwin MG. The ASA physical status classification: interobserver consistency. Anaesth Intensive Care (2002) 30(5):633–40.
11. Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg (1991) 78(3):355–60. doi:10.1002/bjs.1800780327
12. Le Gall JR, Lemeshow S, Saulnier F. A new simplified acute physiology score (SAPS II) based on a European/North American multicenter study. JAMA (1993) 270(24):2957–63. doi:10.1001/jama.270.24.2957
13. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med (1985) 13(10):818–29. doi:10.1097/00003246-198510000-00009
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
14. Thorn CC, Smith M, Aziz O, Holme TC. The Waterlow score for risk assessment in surgical patients. Ann R Coll Surg Engl (2013) 95(1):52–6. doi:10.1308/003588413X13511609954770
15. Bagshaw SM, McDermid RC. The role of frailty in outcomes from critical illness. Curr Opin Crit Care (2013) 19(5):496–503. doi:10.1097/MCC.0b013e328364d570
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
16. Bagshaw SM, Stelfox HT, McDermid RC, Rolfson DB, Tsuyuki RT, Baig N, et al. Association between frailty and short- and long-term outcomes among critically ill patients: a multicentre prospective cohort study. CMAJ (2014) 186(2):E95–102. doi:10.1503/cmaj.130639
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
17. Mangoni AA. Predicting and detecting adverse drug reactions in old age: challenges and opportunities. Expert Opin Drug Metab Toxicol (2012) 8(5):527–30. doi:10.1517/17425255.2012.665874
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
18. Dalleur O, Spinewine A, Henrard S, Losseau C, Speybroeck N, Boland B. Inappropriate prescribing and related hospital admissions in frail older persons according to the STOPP and START criteria. Drugs Aging (2012) 29(10):829–37. doi:10.1007/s40266-012-0016-1
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
19. Muller M, Smulders YM, de Leeuw PW, Stehouwer CD. Treatment of hypertension in the oldest old: a critical role for frailty? Hypertension (2014) 63(3):433–41. doi:10.1161/HYPERTENSIONAHA.113.00911
20. Gill TM. The central role of prognosis in clinical decision making. JAMA (2012) 307(2):199–200. doi:10.1001/jama.2011.1992
21. Siontis GC, Tzoulaki I, Ioannidis JP. Predicting death: an empirical evaluation of predictive tools for mortality. Arch Intern Med (2011) 171(19):1721–6. doi:10.1001/archinternmed.2011.334
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
22. Siontis GC, Tzoulaki I, Siontis KC, Ioannidis JP. Comparisons of established risk prediction models for cardiovascular disease: systematic review. BMJ (2012) 344:e3318. doi:10.1136/bmj.e3318
23. Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories of disability in the last year of life. N Engl J Med (2010) 362(13):1173–80. doi:10.1056/NEJMoa0909087
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
24. Clegg A, Young J, Iliffe S, Olde Rikkert M, Rockwood K. Frailty in elderly people. Lancet (2013) 381(9868):752–62. doi:10.1016/S0140-6736(12)62167-9
25. Jones DM, Song X, Rockwood K. Operationalizing a frailty index from a standardized comprehensive geriatric assessment. J Am Geriatr Soc (2004) 52(11):1929–33. doi:10.1111/j.1532-5415.2004.52521.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
26. Pilotto A, Ferrucci L, Franceschi M, D’Ambrosio LP, Scarcelli C, Cascavilla L, et al. Development and validation of a multidimensional prognostic index for one-year mortality from comprehensive geriatric assessment in hospitalized older patients. Rejuvenation Res (2008) 11(1):151–61. doi:10.1089/rej.2007.0569
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
27. Sancarlo D, D’Onofrio G, Franceschi M, Scarcelli C, Niro V, Addante F, et al. Validation of a modified multidimensional prognostic index (m-MPI) including the mini nutritional assessment short-form (MNA-SF) for the prediction of one-year mortality in hospitalized elderly patients. J Nutr Health Aging (2011) 15(3):169–73. doi:10.1007/s12603-010-0293-5
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
28. Rodríguez-Mañas L, Féart C, Mann G, Viña J, Chatterji S, Chodzko-Zajko W, et al. Searching for an operational definition of frailty: a Delphi method based consensus statement: the frailty operative definition-consensus conference project. J Gerontol A Biol Sci Med Sci (2013) 68(1):62–7. doi:10.1093/gerona/gls119
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
29. De Vries NM, Staal JB, van Ravensberg CD, Hobbelen JS, Olde-Rikkert MGM, Nijhuis-van der Sanden MWG. Outcome instruments to measure frailty: a systematic review. Ageing Res Rev (2011) 10(1):104–14. doi:10.1016/j.arr.2010.09.001
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
30. Yourman LC, Lee SJ, Schonberg MA, Widera EW, Smith AK. Prognostic indices for older adults: a systematic review. JAMA (2012) 307(2):182–92. doi:10.1001/jama.2011.1966
31. Fischer SM, Gozansky WS, Sauaia A, Min SJ, Kutner JS, Kramer A. A practical tool to identify patients who may benefit from a palliative approach: the CARING criteria. J Pain Symptom Manage (2006) 31(4):285–92. doi:10.1016/j.jpainsymman.2005.08.012
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
32. Inouye SK, Bogardus ST Jr, Vitagliano G, Desai MM, Williams CS, Grady JN, et al. Burden of illness score for elderly persons: risk adjustment incorporating the cumulative impact of diseases, physiologic abnormalities, and functional impairments. Med Care (2003) 41(1):70–83. doi:10.1097/00005650-200301000-00010
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
33. Teno JM, Harrell FE Jr, Knaus W, Phillips RS, Wu AW, Connors A Jr, et al. Prediction of survival for older hospitalized patients: the HELP survival model. Hospitalized elderly longitudinal project. J Am Geriatr Soc (2000) 48(5 Suppl):S16–24.
34. Pilotto A, Rengo F, Marchionni N, Sancarlo D, Fontana A, Panza F, et al. Comparing the prognostic accuracy for all-cause mortality of the frailty instruments: a multicentre 1-year follow-up in hospitalized older patients. PLoS One (2012) 7(1):e29090. doi:10.1371/journal.pone.0029090
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
35. Pilotto A, Gallina P, Fontana A, Sancarlo D, Bazzano S, Copetti M, et al. Development and validation of a multidimensional prognostic index for mortality based on a standardized multidimensional assessment schedule (MPI-SVaMA) in community-dwelling older subjects. J Am Med Dir Assoc (2013) 14(4):287–92. doi:10.1016/j.jamda.2013.01.005
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
36. Pilotto A, Addante F, Franceschi M, Leandro G, Rengo G, D’Ambrosio P, et al. A multidimensional prognostic index (MPI) based on a comprehensive geriatric assessment predict short-term mortality in older patients with heart failure. Circ Heart Fail (2010) 3(1):14–20. doi:10.1161/CIRCHEARTFAILURE.109.865022
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
37. Pilotto A, Addante F, Ferrucci L, Leandro G, D’Onofrio G, Corritore M, et al. The multidimensional prognostic index predicts short- and long-term mortality in hospitalized geriatric patients with pneumonia. J Gerontol A Biol Sci Med Sci (2009) 64(8):880–7. doi:10.1093/gerona/glp031
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
38. Pilotto A, Sancarlo D, Panza F, Paris F, D’Onofrio G, Cascavilla L, et al. The multidimensional prognostic index (MPI) based on a comprehensive geriatric assessment predicts short- and long-term mortality in hospitalized older patients with dementia. J Alzheimers Dis (2009) 18(1):191–9. doi:10.3233/JAD-2009-1139
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
39. Pilotto A, Sancarlo D, Franceschi M, Aucella F, D’Ambrosio P, Scarcelli C, et al. A multidimensional approach to the geriatric patient with chronic kidney disease. J Nephrol (2010) 23(Suppl 15):S5–10.
40. Pilotto A, Sancarlo D, Aucella F, Fontana A, Addante F, Copetti M, et al. Addition of the multidimensional prognostic index to the estimated glomerular filtration rate improves prediction of long-term all-cause mortality in older patients with chronic kidney disease. Rejuvenation Res (2012) 15(1):82–8. doi:10.1089/rej.2011.1210
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
41. Sancarlo D, Pilotto A, Panza F, Copetti M, Longo MG, D’Ambrosio P, et al. A multidimensional prognostic index (MPI) based on a comprehensive geriatric assessment predicts short- and long-term all-cause mortality in older hospitalized patients with transient ischemic attack. J Neurol (2012) 259(4):670–8. doi:10.1007/s00415-011-6241-4
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
42. Pilotto A, Addante F, D’Onofrio G, Sancarlo D, Ferrucci L. The comprehensive geriatric assessment and the multidimensional approach. A new look at the older patient with gastroenterological disorders. Best Pract Res Clin Gastroenterol (2009) 23(6):829–37. doi:10.1016/j.bpg.2009.10.001
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
43. Gallucci M, Battistella G, Bergamelli C, Spagnolo P, Mazzuco S, Carlini A, et al. Multidimensional prognostic index in a cognitive impairment outpatient setting: mortality and hospitalizations. The Treviso Dementia (TREDEM) study. J Alzheimers Dis (2014) 42(4):1461–8. doi:10.3233/JAD-140516
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
44. Giantin V, Valentini E, Iasevoli M, Falci C, Siviero P, De Luca E, et al. Does the multidimensional prognostic index (MPI), based on a comprehensive geriatric assessment (CGA), predict mortality in cancer patients? Results of a prospective observational trial. J Geriatr Oncol (2013) 4(3):208–17. doi:10.1016/j.jgo.2013.04.008
45. Volpato S, Bazzano S, Fontana A, Ferrucci L, Pilotto A, On Behalf of the MPI-TriVeneto Study Group. Multidimensional prognostic index predicts mortality and length of stay during hospitalization in the older patients: a multicenter prospective study. J Gerontol A Biol Sci Med Sci (2014). doi:10.1093/gerona/glu167
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
46. Manganaro D, De Colle P, Sceusa R, Biolo G, Toigo G. Prognostic value of the multidimensional prognostic index on long-term mortality, discharge planning and hospital re-admission in elderly acutely ill patients. Giorn Gerontol (2012) 60(6):366.
47. Gagne JJ, Glynn RJ, Avorn J, Schneeweiss S. A combined comorbidity score predicted mortality in elderly patients better than existing scores. J Clin Epidemiol (2011) 64(7):749–59. doi:10.1016/j.jclinepi.2010.10.004
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
48. Mazzaglia G, Roti L, Corsini G, Colombini A, Maciocco G, Marchionni N, et al. Screening of older community-dwelling people at risk for death and hospitalization: the assistenza socio-sanitaria in Italia project. J Am Geriatr Soc (2007) 55(12):1955–60. doi:10.1111/j.1532-5415.2007.01446.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
49. Lee SJ, Lindquist K, Segal MR, Covinsky KE. Development and validation of a prognostic index for 4-year mortality in older adults. JAMA (2006) 295(7):801–8. doi:10.1001/jama.295.7.801
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
50. Carey EC, Covinsky KE, Lui LY, Eng C, Sands LP, Walter LC. Prediction of mortality in community-living frail elderly people with long-term care needs. J Am Geriatr Soc (2008) 56(1):68–75. doi:10.1111/j.1532-5415.2007.01496.x
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
51. Schonberg MA, Davis RB, McCarthy EP, Marcantonio ER. Index to predict 5-year mortality of community-dwelling adults aged 65 and older using data from the National Health Interview Survey. J Gen Intern Med (2009) 24(10):1115–22. doi:10.1007/s11606-009-1073-y
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
52. Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, et al. Gait speed and survival in older adults. JAMA (2011) 305(1):50–8. doi:10.1001/jama.2010.1923
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
53. Pilotto A, D’Onofrio G, Panza F, Copetti M, Cascavilla L, Paris F, et al. Treatment of late-life major depressive disorder with selective serotonin reuptake inhibitors improves the multidimensional prognostic index. J Clin Psychopharmacol (2012) 32(5):726–9. doi:10.1097/JCP.0b013e31826866bd
54. D’Onofrio G, Sancarlo D, Addante F, Ciccone F, Cascavilla L, Paris F, et al. A pilot randomized controlled trial evaluating an integrated treatment of rivastigmine transdermal patch and cognitive stimulation in patients with Alzheimer’s disease. Int J Geriatr Psychiatry (2014). doi:10.1002/gps.4247
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
55. Walter LC, Covinsky KE. Cancer screening in elderly patients: a framework for individualized decision making. JAMA (2001) 285(21):2750–6. doi:10.1001/jama.285.21.2750
56. Reuben DB. Medical care for the final years of life: “when you’re 83, it’s not going to be 20 years”. JAMA (2009) 302(24):2686–94. doi:10.1001/jama.2009.1871
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
57. Scowcroft AC, Lee S, Mant J. Thromboprophylaxis of elderly patients with AF in the UK: an analysis using the general practice research database (GPRD) 2000-2009. Heart (2013) 99(2):127–32. doi:10.1136/heartjnl-2012-302843
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
58. Pilotto A, Sancarlo D, Fontana A, Paroni G, Copetti M, Gallina P, et al. Usefulness of the multidimensional prognostic index (MPI) in evaluating the efficacy of warfarin treatment in older patients with atrial fibrillation. Eur Geriatr Med (2012) 3(Suppl 1):S5. doi:10.1016/j.eurger.2012.07.031
59. Pilotto A, Pellegrini F, Maggi S, Cruz-Jentoft AJ, Paccalin M, Polidori MC, et al. Statin treatment reduces all-cause mortality in older patients with cardio- or cerebrovascular disease regardless of their mortality risk. Results of the EU-funded MPI_AGE Project. Eur Geriatr Med (2014) 5(Suppl 1):S112. doi:10.1016/S1878-7649(14)70270-0
60. Anglemyer A, Horvath HT, Bero L. Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials. Cochrane Database Syst Rev (2014) 4:MR000034. doi:10.1002/14651858.MR000034.pub2
Pubmed Abstract | Pubmed Full Text | CrossRef Full Text | Google Scholar
Keywords: older age, frailty, clinical decision-making, multidimensional prognostic index, comprehensive geriatric assessment
Citation: Pilotto A, Sancarlo D, Daragjati J and Panza F (2015) Perspective: the challenge of clinical decision-making for drug treatment in older people. The role of multidimensional assessment and prognosis. Front. Med. 1:61. doi: 10.3389/fmed.2014.00061
Received: 21 November 2014; Accepted: 24 December 2014;
Published online: 14 January 2015.
Edited by:
Graziano Onder, Università Cattolica del Sacro Cuore, ItalyReviewed by:
Marco Inzitari, Parc Sanitari Pere Virgili, SpainDing-Cheng (Derrick) Chan, National Taiwan University Hospital, Taiwan
Copyright: © 2015 Pilotto, Sancarlo, Daragjati and Panza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alberto Pilotto, Geriatrics Unit, Azienda ULSS 16 Padova, S Antonio Hospital, Via Facciolati 71, Padova, I-35127, Italy e-mail:YWxiZXJ0by5waWxvdHRvQHNhbml0YS5wYWRvdmEuaXQ=