 Juan David Ruiz-Zapata1
Juan David Ruiz-Zapata1 Luis Mauricio Figueroa-Gutiérrez1Jaime Alberto Mesa-Franco1
Luis Mauricio Figueroa-Gutiérrez1Jaime Alberto Mesa-Franco1 Paula Andrea Moreno-Gutierrez2*
Paula Andrea Moreno-Gutierrez2*- 1Faculty of Health Sciences, Universidad Tecnológica de Pereira, Pereira, Colombia
- 2Grupo de Investigación en Biomedicina, Fundación Universitaria Autónoma de las Américas, Pereira, Colombia
Myasis is the infestation by fly larvae (Diptera) in live vertebrates including humans. Myasis has been reported most commonly in tropical and subtropical areas around the world with poor sanitation and presence of cattle. Neonatal umbilical myiasis is an important cause of death in bovines and produces major economic losses in the livestock industry. However, its presentation in humans is rare, with a few cases reported worldwide. Moreover, umbilical myasis can be life-treating due to the risk of larvae migration to deeper tissues of the abdomen, omphalitis, and sepsis. We describe the case of a 7-day-old infant admitted to the hospital due to umbilical cord myiasis. In total, 55 larvae were removed from the wound and identified as Cochliomyia hominivorax. The patient recovered satisfactorily after treatment with ivermectin and amoxicillin. A literature search was performed in Pubmed, Medline, Lilacs and Google Scholar, with 64 cases of myasis by C. hominivorax being reviewed. Oral cavity, wounds, scalp and natural orifices are the main affected anatomical areas. Risk factors include the extremes of age, male sex, poor hygiene, alcohol and drug use, cancer, and mental disability. Programs for human myiasis prevention and surveillance are needed in neotropical areas where living conditions make it difficult to implement control strategies.
Introduction
Myiasis is infestation by fly larvae (Diptera) in live vertebrates, including humans. Fly larvae feed on wound tissue of their host, causing a disease whose severity may depend on the larva species and anatomical sites affected (1, 2). It is widespread in neotropical areas around the world, causing economic and public health problems in low-income populations. Human infection is facilitated by poor hygienic conditions and close contact with wild or domestic animals (2, 3). Umbilical cord myiasis is a common type of wound myiasis in animals but it has been described only rarely in humans (2). We present the first report of neonatal umbilical myiasis in Colombia and review the most relevant aspects of this disease. Recent case reports of myiasis by C. hominivorax are reviewed in the discussion.
Case Report
The research procedures for this case were carried out in accordance with the recommendations of the guidelines of the Helsinki Committee. Written informed consent was obtained from the mother of the newborn for pictures and publication of this case.
A 7-day-old female neonate was taken to a primary health facility in June 2017 because something was coming out of her umbilicus. The patient was born full-term at the local hospital by vaginal delivery from a 17-year-old mother. At birth, the newborn had respiratory depression and mild perinatal asphyxia but without further complications. The umbilical cord was cut following standard care measures for in-hospital delivery. The patient lived on a farm with a cowshed next to the house in the rural area of the municipality of La Virginia (04°54′1.617″ N, 75°52′47.445″ W), in the state of Risaralda, located in the coffee region of Colombia. The mother practiced exclusive breastfeeding and used a fabric girdle, which is traditionally used in Colombia for protection of the umbilical stump during the first days of life.
The neonate was transferred to a tertiary care hospital. On admission, she was visibly irritated and jaundiced. On physical exam, weight was 3,300 g and vital signs (temperature, heart rate, respiratory rate, blood pressure, and blood oxygen levels) were normal. Umbilical stump inspection revealed numerous live larvae (Supplementary Figure 1) and foul-smelling serohaematic secretion. The rest of the examination was normal. Initial blood count showed 20,140 leukocytes/μl (52% neutrophils, 3% eosinophils, 4% lymphocytes, and 5% monocytes). Total serum bilirubin was 18.0 mg/dl (cutoff point to consider phototherapy: 20.5 mg/dl) (4). Wound and blood cultures on admission and 48 h later were negative.
Initial treatment included covering the umbilical stump with gauze soaked in ivermectin and nitrofurazone, followed by a single oral dose of ivermectin (0.15 mg/kg). To prevent late-onset sepsis, intravenous ampicillin (200 mg/kg/day) and gentamicin (4 mg/kg/day) were administered. On the second day, 39 live larvae were removed from the umbilical stump under aseptic conditions using a surgical clamp. One live and 15 dead larvae were extracted on the third day. A follow-up abdominal ultrasonography was normal and the patient was discharged 7 days after admission.
After extraction, seven larvae were preserved in a solution containing 80% alcohol. The specimens were sent to an entomologist and examined using a microscope with 10× magnification. Third instar larvae of C. hominivorax were identified by their smooth appearance with prominent spine bands and one body process in the last segments (Supplementary Figure 2). Pigmented dorsal tracheal trunks were present in two to three of the last segments. The posterior spiracular plates contained three oval-shaped slips pointing to the peritreme (5).
Discussion
Umbilical myiasis is a rare type of wound myiasis in humans, but the occurrence of cases in widely distributed areas shows that this may be a latent risk in all neotropic zones were myiasis has been reported (2). A handful of case reports of umbilical myiasis have been made, mainly in India (3, 6–13). One case was reported in the United States (14) and another in Argentina (15), the latter associated with C. hominivorax. The largest case collection of umbilical myiasis was carried out in Nigeria, where active detection in a region of the Niger Delta resulted in 55 cases of omphalitis (16). Other anatomical sites of myiasis in human neonates include the nostrils (17), ear (18), skin (19), and genitals (20).
The warm and moist environment of the umbilical stump attracts the female flies to lay their eggs on it (11). In our case, the use of an umbilical girdle could have retained moisture around the stump and delayed the separation, creating ideal conditions for larvae growth and also hiding the disease. Umbilical girdles were used traditionally to secure the navel of newborns (21) and remain a common practice in Colombia that goes against current recommendations to keep the stump uncovered to help dry out the base. The girdle also facilitates omphalitis, which in turn increases the size of the wound and creates a proper environment for egg hatching (11). Traditional methods for stump care, such as application of cow dung or herb leaves on the umbilicus of neonates, have been described in previous reports as sources of cross-contamination (16, 22).
Clinical signs of umbilical myiasis are hardly recognized by the caregiver. The disease is usually detected once the larvae are visible or clinical signs of omphalitis appear (11). Imaging and biopsy are rarely necessary for diagnosis but may be useful in umbilical myiasis to determine the extent of the infestation and any organ involvement. Leukocytosis along with neutrophilia and eosinophilia are common clinical findings (2). Hyperbilirubinaemia that resolved after larvae extraction was reported in one case of cutaneous myiasis by Drosophila in a newborn (23), but not in prior cases of neonatal umbilical myiasis.
Neonatal myiasis has been consistently attributed to conditions related to low socioeconomic status, such as poor hygiene, contact with farm animals, home delivery using unsterilized instruments and the use of traditional methods to take care of the stump (8, 9, 11, 24). Nonetheless, wound myiasis can also be an indicator of neglect or self-neglect (24). Thus, social counseling should be considered in these cases and newborn care must be reinforced. Adequate wound care, keeping the umbilicus covered with clean dressings and adequate hygienic habits in general should all be included in the recommendations given to the mother or caretaker before discharge (2, 14, 15).
The New World screwworm (C. hominivorax), is the most common species causing myiasis in Central and South America. The incidence of human myiasis by this species has been declining progressively since 1958 due to the implementation of programmes using the sterile insect technique (SIT) that have led to the eradication of C. hominivorax in Curacao, North and Central America and North Africa (25). Sixty-five case reports of human disease have been published from 2000 up to 30 September 2019 according to a literature search performed in Pubmed, Medline, Google Scholar and Lilacs (Table 1). Sixty of the cases (92%) occurred in South America, mainly in Brazil (n = 31, 48%) and Argentina (n = 7, 11%). There was one case report in India, but the species could have been mistakenly identified. Common anatomical sites of infection were the oral cavity, chronic or traumatic wounds, scalp and natural orifices (ear, nose, vagina). Risk factors for infection include the extreme ages, male gender, rural residency, poor hygienic conditions, cancer, alcohol and drug use, malnutrition, mental impairment, prolonged mouth opening, and prosthetic material. Myiasis in the scalp was facilitated by pediculosis or seborrheic dermatitis.
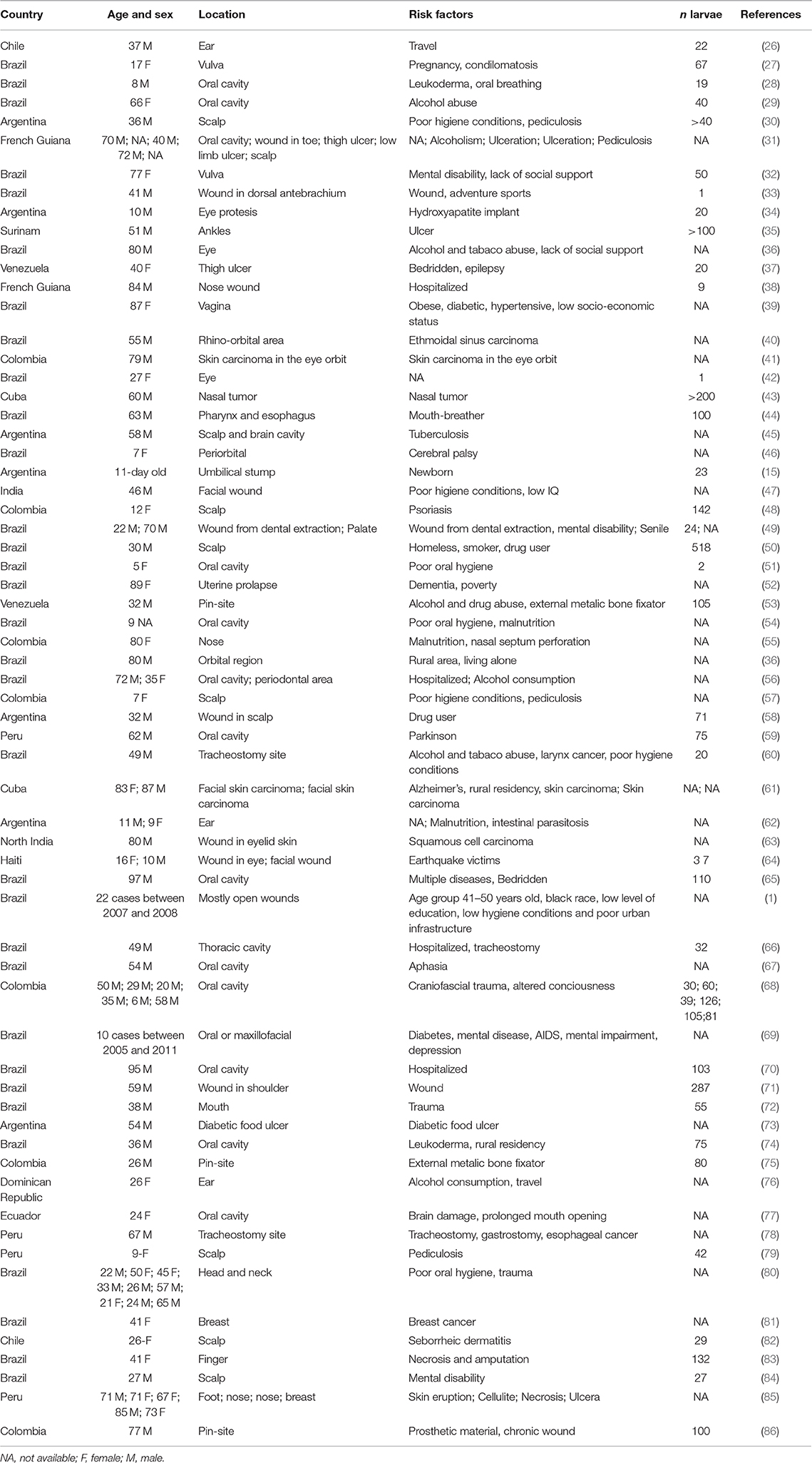
Table 1. Cases of myiasis by Cochliomyia hominivorax published since 2000 in Pubmed, Medline, Google Scholar, and Lilacs.
In Colombia, the geographic distribution and economic burden of C. hominivorax, as well as the epidemiology of myiasis in both animals and humans, is unknown but this species is recognized as in important cause of livestock loss (87). Human myiasis by this species has been reported in the states of Antioquia (88, 89), Atlantico (57), Cundinamarca (41), and Boyaca (90), however notification of cases is not mandatory. Research is needed on the biology, epidemiology and population dynamics of this species in order to assess the political, geographic and economic viability of the implementation of programs for insect control in the country (87). Thus, nationwide protocols and surveillance systems are urgently needed to control this ongoing threat to animal and human health.
During its larvae stage, C. hominivorax is an obligate parasite of warm-blooded animals, including humans. Once the female is gravid, it deposits an average of 200 eggs in open wounds or natural orifices (1). Egg hatching occurs in approximately 12 h and then it takes 5–7 days for larvae to reach the third instar of maturity inside bovine wounds. This means that the patient possibly was infected in the first 2 days of life. Larvae penetrate deeply into wounds, tearing tissue and making tunnels with their mouths to find a warm and moist place. Then, they hook and cause an extensive destruction of tissue known as traumatic myiasis, which provokes wound swelling that may facilitate bacterial infection (91). Umbilical myiasis is particularly dangerous because it might induce fistulation, penetration of deep layers of the abdomen wall and secondary sepsis associated with omphalitis (2, 92), although none of these were found in our patient.
As in our case, treatment of myiasis is based on the removal of all visible larvae, cleaning of the wound and debridement of remaining necrotic tissue. Irrigation is helpful if the lesions have holes and/or cavities. Local application of ivermectin paralyzes the parasite and kills the larvae, facilitating the extraction and relieving pain (31). Turpentine or ether is used to suffocate the larvae, but this practice is not recommended as it could lead to complications such as anaphylaxis and sepsis (22). Surgical treatment is required when larvae are dead, decomposing or laying in deep tissues (8). Topical anthelmintic medication, bactericides, tetanus toxoid vaccine and systemic antibiotics should also be considered to prevent secondary sepsis. In many reports, the use of systemic ivermectin showed positive results, but further studies are needed to consider this a standard therapy (2, 7, 8).
Correct identification by a trained entomologist is helpful to understand the infestation mechanism, to plan treatment and to consider preventive actions. For etiological diagnosis, the larvae should be immersed in hot water for 30 s to retain length and morphology and then preserved in a 70–90% ethanol solution or isopropyl alcohol. The regions where the patient has been, the climatic conditions and the endemic species are also important for accurate identification (2). The peak period of infestation by C. hominivorax has been reported to be between June and August, in humid and warm locations (5), such as the city where the patient lived.
Livestock is an important economic source in neotropical regions where poverty and inadequate health conditions make it difficult to implement control and eradication programs. Therefore, myiasis will continue to be a sanitary problem in many countries of America, Africa and Asia. Furthermore, global warming and internationalization are likely to influence the migration of screwworm and other myiasis-causing species into new geographic areas that were previously unaffected by this problem. Naïve livestock host are more susceptible to insect replication, increasing the likelihood of outbreaks (93). Groups of individuals at high risk of myiasis should be targeted in prevention programs for C. hominivorax infection in areas were insect eradication programs are not available.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin. A written informed consent was obtained from the mother of the newborn for pictures and publication of this case.
Author Contributions
LF-G and JM-F contributed to the diagnosis and treatment of the patient. They also obtained informed consent and gathered clinical data. JR-Z and PM-G reviewed the literature and wrote the manuscript. All the authors discussed and analyzed the case.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2019.00292/full#supplementary-material
References
1. Batista-da-Silva JA, Moya-Borja GE, Queiroz MM. Factors of susceptibility of human myiasis caused by the new world screw-worm, Cochliomyia hominivorax in Sao Goncalo, Rio de Janeiro, Brazil. J Insect Sci. (2011) 11:14. doi: 10.1673/031.011.0114
3. Mondal M. Umbilical myiasis with sepsis in a neonate. Asian J Med Sci. (2014) 5:106–7. doi: 10.3126/ajms.v5i4.10004
4. Rennie J, Burman-Roy S, Murphy MS. Neonatal jaundice: summary of NICE guidance. BMJ. (2010) 340:c2409. doi: 10.1136/bmj.c2409
5. The World Organisation for Animal Health (OIE). Chapter 3.1.13: New World screwworm (Cochliomyia hominivorax) and Old World screwworm (Chrysomya bezziana). In: Manual of Diagnostic Tests and Vaccines for Terrestrial Animals 2019. Paris (2019).
6. Ghosh T, Nayek K, Ghosh N, Ghosh MK. Umbilical myiasis in newborn. Indian Pediatr. (2011) 48:321–3.
7. Patra S, Purkait R, Basu R, Konar MC, Sarkar D. Umbilical myiasis associated with Staphylococcus aureus sepsis in a neonate. J Clin Neonatol. (2012) 1:42–3. doi: 10.4103/2249-4847.92229
8. Ambey R, Singh A. Umbilical myiasis in a healthy newborn. Paediatr Int Child Health. (2012) 32:56–7. doi: 10.1179/1465328111Y.0000000043
9. Kumar V, Gupta S. Umbilical myiasis in a neonate. Paediatr Int Child Health. (2012) 32:58–9. doi: 10.1179/1465328111Y.0000000022
10. Dey P, Bhattacharya T, Pal S, Das S, Pal S. Umbilical myiasis in a newborn: a case report. JCMS Nepal. (2013) 8:42–5. doi: 10.3126/jcmsn.v8i4.8700
11. Kumar M, Thakur KC, Chib R, Gupta G. Neonatal umbilical myiasis. J Clin Neonatol. (2017) 6:121. doi: 10.4103/jcn.JCN_122_16
12. Kotha R, Pandala P, Singh H, Reddy BS, Reddy ST, Rathod M, et al. Neonatal umbilical myiasis. Int J Contemp Pediatr. (2019) 6:1. doi: 10.18203/2349-3291.ijcp20190004
13. Jauhari S, Nautiyal S. Umblical myiasis in a newborn: a case report. Int J Commun Med Public Health. (2017) 4:872–4. doi: 10.18203/2394-6040.ijcmph20170776
14. Puvabanditsin S, Malik I, Weidner LM, Jadhav S, Sanderman J, Mehta R. Neonatal umbilical cord myiasis in New Jersey. J Perinatol. (2014) 34:718–9. doi: 10.1038/jp.2014.69
15. Duro E, Mariluis JC, Mulieri PR. Umbilical myiasis in a human newborn. J Perinatol. (2007) 27:250–1. doi: 10.1038/sj.jp.7211654
16. Ogbalu O, Eze C, Manuelrb B. A new trend of Omphalitis complicated with myiasis in neonates of the Niger Delta, Nigeria. Epidemiology. (2016) 6:231. doi: 10.4172/2161-1165.1000231
17. Martínez-Rojano H, Noguez JC, Huerta H. Nosocomial myiasis caused by Lucilia sericata (Diptera: Calliphoridae) and neonatal myiasis by Sarcophaga spp. (Diptera: Sarcophagidae) in Mexico. Case Rep Infect Dis. (2018) 2018:5067569. doi: 10.1155/2018/5067569
18. Singh A, Singh Z. Incidence of myiasis among humans—a review. Parasitol Res. (2015) 114:3183–99. doi: 10.1007/s00436-015-4620-y
19. Dedeke IOF, Agbo DD, Soile BH, Alao SO, Evwibovwe E, Akinseinde JA. Neonatal cutaneous myiasis: a mistaken identity for impetigo. Open J Pediat. (2019) 9:133–8. doi: 10.4236/ojped.2019.92014
20. Ogbalu OK, Achufusi TG, Orlu EE, Bawo DS, Adibe CH, Kumbe L, et al. Human myiasis in neonates and children of the Niger Delta Wetlands and South-East Nigeria. J Cosmet Dermatol Sci Appl. (2011) 1:171–6. doi: 10.4236/jcdsa.2011.14026
22. Burgess I. Umbilical myiasis. Paediatr Int Child Health. (2012) 32:1–2. doi: 10.1179/204690512X13296079158208
23. Clark J, Weeks W, Tatton J. Drosophila myiasis mimicking sepsis in a newborn. West J Med. (1982) 136:443–4.
24. Hall MJR, Wall RL, Stevens JR. Traumatic myiasis: a neglected disease in a changing world. Annu Rev Entomol. (2016) 61:159–76. doi: 10.1146/annurev-ento-010715-023655
25. Skoda S, Chen H, Chaudhurry M, Sagel A, Phillips P. Artificial diets used in mass production of the New World screwworm, Cochliomyia hominivorax. J Appl Entomol. (2014) 138:708–14. doi: 10.1111/jen.12112
26. Neira OP, Muñoz SN, Cantero CD. Miasis auricular por Cochliomyia hominivorax (Diptera: Calliphoridae) (Coquerel, 1858). Revista Médica de Chile. (2002) 130:907–9. doi: 10.4067/S0034-98872002000800011
27. Passos MRL, Varella RQ, Tavares RR, Barreto NA, Santos CC, Pinheiro V, et al. Vulvar myiasis during pregnancy. Infect Dis Obstet Gynecol. (2002) 10:153–8. doi: 10.1155/S1064744902000157
28. Chicarelli M, Daniel AN, Santoro MA, Teodoro U. Miíase humana bucal por Cochliomyia hominivorax (Coquerel, 1858) em Nova Esperança, estado do Paraná, Brasil. Revista da Faculda de de Odontologia-UPF. (2002) 7. doi: 10.5335/rfo.v7i2.1217
29. Gomez RS, Perdigão PF, Pimenta FJGS, Rios Leite AC, Tanos de Lacerda JC, Custódio Neto AL. Oral myiasis by screwworm Cochliomyia hominivorax. Br J Oral Maxillofac Surg. (2003) 41:115–6. doi: 10.1016/S0266-4356(02)00302-9
30. Visciarelli EC, García SH, Salomón C, Jofré C, Costamagna SR. Un caso de miasis humana por Cochliomyia hominivorax (Díptera: Calliphoridae) asociado a pediculosis en Mendoza, Argentina. Parasitología Latinonot. (2003) 58:166–8. doi: 10.4067/S0717-77122003000300014
31. Clyti E, Couppie P, Cazanave C, Fouque F, Sainte-Marie D, Pradinaud R. Traitement des myiases dues à Cochliomyia hominivorax par application locale d'ivermectine. Bull Soc Pathol Exot. (2003) 96:410–1.
32. Martinez CAR, Romani G, Prioli D. Miíase vulvar: relato de caso. RBGO. (2003) 25. doi: 10.1590/S0100-72032003000400011
33. Seppänen M, Virolainen-Julkunen A, Kakko I, Vilkamaa P, Meri S. Myiasis during adventure sports race. Emerg Infect Dis. (2004) 10:137–9. doi: 10.3201/eid1001.020825
34. Devoto MH, Zaffaroni MC. Orbital myiasis in a patient with a chronically exposed hydroxyapatite implant. Ophthalmic Plast Reconstr Surg. (2004) 20:395–6. doi: 10.1097/01.IOP.0000139526.01850.D1
35. Zupan-Kajcovski B, Simonian H, Keller JJ, Faber WR. [Cutaneous myiasis caused by a double infestation with larvae of Dermatobia hominis and Cochliomyia hominivorax]. Ned Tijdschr Geneeskund. (2004) 148:2086–9.
36. Pierre-filho PDTP, Minguini N, Pierre LM, Pierre AM. Use of ivermectin in the treatment of orbital myiasis caused by Cochliomyia hominivorax. Scand J Infect Dis. (2004) 36:503–5. doi: 10.1080/00365540410020136
37. Moissantde Román E, García ME, Quijada J, Simoes D, Marcial T. Miasis cutánea humana. Un caso clínico. Kasmera. (2004) 32:12–5.
38. Couppié P, Roussel M, Rabarison P, Sockeel M-J, Sainte-Marie D, Marty C, et al. Nosocomial nasal myiasis owing to Cochliomyia hominivorax: a case in French Guiana. Int J Dermatol. (2005) 44:302–3. doi: 10.1111/j.1365-4632.2004.02547.x
39. da Silva BB, Borges US, Pimentel ICC. Human vaginal myiasis caused by Cochliomyia hominivorax. Int J Gynecol Obstet. (2005) 89:152–3. doi: 10.1016/j.ijgo.2004.12.046
40. Costa D, Pierre-Filho PdTP, Medina FMC, Mota R, Carrera C. Use of oral ivermectin in a patient with destructive rhino-orbital myiasis. Eye. (2005) 19:1018–20. doi: 10.1038/sj.eye.6701713
41. Osorio J, Moncada L, Molano A, Valderrama S, Gualtero S, Franco-Paredes C. Role of ivermectin in the treatment of severe orbital myiasis due to Cochliomyia hominivorax. Clin Infect Dis. (2006) 43:e57–9. doi: 10.1086/507038
42. Saraiva VdS, Amaro MH, Belfort R Jr, Burnier MN Jr. A case of anterior internal ophthalmomyiasis: case report. Arquivos Brasileiros de Oftalmologia. (2006) 69:741–3. doi: 10.1590/S0004-27492006000500023
43. Rodríguez Diego JG, Córdova Ramos G, Arozarena R. First notification of the cattle screw worm (Cochliomyia hominivorax) in a human case in Cuba. Revista de Salud Animal. (2007) 29:193.
44. Pasternak J, Joo SH, Ganc AJ, Junior MdSD, Morsh RD, Pinto TH. A case of throat Cochliomyia hominovorax infestation. Einstein. (2007) 5:170–2.
45. Oliva A, Ramos NL, Bosio L. Fatal scalp myiasis: autopsy finding of Cochliomyia hominivorax (Diptera: Calliphoridae) in the brain cavity. Can Soc Forensic Sci J. (2007) 40:183.
46. Takahagi RU, Gonçalves FP, Madeira NG, Schellini SA. Oftalmomiíase externa causada por Cochliomyia hominivorax. Revista Brasileira de Oftalmologia. (2007) 66:58–62.
47. Baskaran M, Jagan Kumar B, Geeverghese A. Cutaneous myiasis of face. J Oral Maxillofac Pathol. (2007) 11:70–2. doi: 10.4103/0973-029X.37386
48. Mariwalla K, Langhan M, Welch KA, Kaplan DH. Cutaneous myiasis associated with scalp psoriasis. J Am Acad Dermatol. (2007) 57:S51–2. doi: 10.1016/j.jaad.2006.10.022
49. Gealh WC, Ferreira GM, Farah GJ, Teodoro U, Camarini ET. Treatment of oral myiasis caused by Cochliomyia hominivorax: two cases treated with ivermectin. Br J Oral Maxillofac Surg. (2009) 47:23–6. doi: 10.1016/j.bjoms.2008.04.009
50. Ferraz AC, Nunes RV, Gadelha BQ, Nascimento BP, Meirelles P, Coelho VM, et al. Raro caso de miíase por Cochliomyia hominivorax (Diptera: Calliphoridae) e Dermatobia hominis (Diptera: Oestridae) em paciente humano. Arquivos de Ciências da Saúde da UNIPAR. (2008) 15:142–4.
51. de Souza Barbosa T, Salvitti Sa Rocha RA, Guirado CG, Rocha FJ, student G, Duarte Gavião MB. Oral infection by Diptera larvae in children: a case report. Int J Dermatol. (2008) 47:696–9. doi: 10.1111/j.1365-4632.2008.03725.x
52. Lopes-Costa PV, dos Santos AR, Pereira-Filho JD, da Silva BB. Myiasis in the uterine cavity of an elderly woman with a complete uterine prolapse. Trans Royal Soc Trop Med Hyg. (2008) 102:1058–60. doi: 10.1016/j.trstmh.2008.04.004
53. Paris LA, Viscarret M, Uban C, Vargas J, AJ R-M. Pin-site myiasis: a rare complication of a treated open fracture of tibia. Surg Infect. (2008) 9:403–6. doi: 10.1089/sur.2007.045
54. de Araújo RJG, Corrêa AM, Santos WRA, Júnior MTM. Advanced stage of oral myiasis in children: a clinical case report. Quintessence Int. (2008) 39:39–43.
55. González C, Salamanca JC, Olano V, Pérez CE. Miasis cavitaria. Reporte de un caso. Rev Med. (2008) 16:95–8.
56. Lima Júnior SM, Asprino L, Prado ÂP, Moreira RWF, de Moraes M. Oral myiasis caused by Cochliomyia hominivorax treated nonsurgically with nitrofurazone: report of 2 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. (2010) 109:e70–3. doi: 10.1016/j.tripleo.2009.11.014
57. de la Ossa N, Castro LE, Visbal L, Santos AM, Díaz E, Romero-Vivas CM. Cutaneous myiasis by Cochliomyia hominivorax (Coquerel)(Diptera Calliphoridae) in Hospital Universidad del Norte, Soledad, Atlántico. Biomédica. (2009) 29:12–7. doi: 10.7705/biomedica.v29i1.36
58. Trombetta L, Oliva A, Galache V, Bava J, Troncoso A. Cutaneous myiasis due to Cochliomyia hominivorax in a drug user. J Infect Dev Ctries. (2009) 3:873–6. doi: 10.3855/jidc.170
59. Espinoza A, Quiñones-Silva J, Garay O. Miasis en cavidad oral por Cochliomyia Hominivorax: reporte de un caso. Revista Peruana de Medicina Experimental y Salud Publica. (2009) 26:573–6.
60. de Carvalho DC, Camargo RPM, Menegali TT, Gehlen D, Klaus MZB. Relato de caso: infestação da cânula de traqueostomia por miíase. Arquivos Catarinenses de Medicina. (2009) 38:96–9.
61. Delys Fernández DRE, Borges García DT, Valdés Borroto DAC, Rivas de Armas DRA. Miiasis facial por gusano barrenador del ganado asociado a un carcinoma. Presentación de dos Pacientes. (2011) 2011.
62. Menghi C, Gatta C, Oliva A. Otomiasis por Cochliomyia hominivorax en dos niños del conurbano bonaerense, Argentina. Revista Argentina de Microbiología. (2010) 42:176–8.
63. Khurana S, Biswal M, Bhatti H, Pandav S, Gupta A, Chatterjee S, et al. Ophthalmomyiasis: three cases from North India. Indian J Med Microbiol. (2010) 28:257–61. doi: 10.4103/0255-0857.66490
64. Lindsay R, Stancil J, Ray JM. Myiasis of facial wounds by Cochliomyia hominivorax sustained in a natural disaster in Haiti. Otolaryngol Head Neck Surg. (2010) 143:595–6. doi: 10.1016/j.otohns.2010.04.273
65. Ribeiro MC, De Oliveira Pepato A, De Matos FP, Sverzut CE, Abrahão AAC, Trivellato AE. Oral myiasis in an elderly patient. Gerodontology. (2012) 29:e1136–9. doi: 10.1111/j.1741-2358.2010.00432.x
66. Batista-da-Silva JA, Borja GEM, Queiroz MMC. Patient with tracheostomy parasitized in hospital by larvae of the screwworm, Cochliomyia hominivorax. J Insect Sci. (2011) 11:163. doi: 10.1673/031.011.16301
67. Vale DS, Cavalieri I, Araujo MM, Santos MBP, dos Santos Canellas JV, Espínola LVP, et al. Myiasis in palate by Cochliomyia hominivorax. J Craniofac Surg. (2011) 22:e57–9. doi: 10.1097/SCS.0b013e318231e1f3
68. Duque FL, Ardila CM. Oral myiasis caused by the screwworm Cochliomyia hominivorax treated with subcutaneous ivermectin and creolin: report of six cases after trauma. Dental Traumatology. (2011) 27:404–7. doi: 10.1111/j.1600-9657.2011.01004.x
69. Antunes AA, de Santana Santos T, Avelar RL, Neto ECM, Macedo Neres B, Laureano Filho JR. Oral and maxillofacial myiasis: a case series and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. (2011) 112:e81–5. doi: 10.1016/j.tripleo.2011.05.026
70. Thyssen PJ, Nassu MP, Costella AMU, Costella ML. Record of oral myiasis by Cochliomyia hominivorax (Diptera: Calliphoridae): case evidencing negligence in the treatment of incapable. Parasitol Res. (2012) 111:957–9. doi: 10.1007/s00436-012-2856-3
71. Batista-da-Silva JA, Borja G, Queiroz M. A severe case of cutaneous myiasis in São Gonçalo, Brazil, and a simple technique to extract New World screw-worm Cochliomyia hominivorax (Coquerel) (Diptera: Calliphoridae). Neotropical entomol. (2012) 41:341–2. doi: 10.1007/s13744-012-0038-8
72. Costa FS, Bellotti A, Farah GJ, Camarini ET. Treatment of myiasis resulting from complex facial trauma. Revista de Cirurgia e Traumatologia Buco-Maxilo-Facial. (2012) 12:25–30.
73. Olea MS, Centeno N, Aybar CAV, Ortega ES, Galante GB, Olea L, et al. First report of myiasis caused by Cochliomyia hominivorax (Diptera: Calliphoridae) in a diabetic foot ulcer patient in Argentina. Korean J Parasitol. (2014) 52:89–92. doi: 10.3347/kjp.2014.52.1.89
74. Novo-Neto JP, Santos FdSAd, Pontes AEF, Ribeiro FS, Scannavino FLF, Martins AT. Oral myiasis caused by Cochliomyia hominivorax in a disabled person. Case Rep Pathol. (2015) 2015:904658. doi: 10.1155/2015/904658
75. Africano FJ, Faccini-Martinez AA, Perez CE, Espinal A, Bravo JS, Morales C. Pin-site myiasis caused by screwworm fly, Colombia. Emerg Infect Dis. (2015) 21:905–6. doi: 10.3201/eid2105.141680
76. LaCourse SM, Martinez RM, Spach DH, Fang FC. Pain and bloody ear discharge in a returning traveler. Am J Trop Med Hyg. (2015) 92:599–600. doi: 10.4269/ajtmh.14-0617
77. Reinoso-Quezada S, Alemán-Iñiguez JM. Rara miasis maxilar por Cochliomyia hominivorax: reporte de caso, actualidad y entomología. Revista Española de Cirugía Oral y Maxilofacial. (2016) 38:111–6. doi: 10.1016/j.maxilo.2014.04.005
78. Failoc-Rojas VE, Silva-Díaz H. Review of cases and a patient report of myiasis with tracheostomy, peru. Emerg Infect Dis. (2016) 22:563–5. doi: 10.3201/eid2203.151631
79. Calderón-Castrat X, Idrogo-Bustamante JL, Peceros-Escalante J, Ballona R. Wound myiasis caused by Cochliomyia hominivorax: the role of entodermoscopy. Int J Dermatol. (2017) 56:330–2. doi: 10.1111/ijd.13432
80. de Arruda JAA, de Oliveira Silva LV, Silva PUJ, de Figueiredo EL, Callou G, Mesquita RA, et al. Head and neck myiasis: a case series and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. (2017) 124:e249–56. doi: 10.1016/j.oooo.2017.06.120
81. Rodrigues FT, Klemig LR, Cardozo MRP, Alves PC, Aguiar VM, Lessa CS. Myiasis associated with an invasive ductal carcinoma of the left breast: case study. Revista do Instituto de Medicina Tropical de São Paulo. (2017) 59:e35. doi: 10.1590/s1678-9946201759035
82. Calderon HP, Rojas EC, Apt BW, Castillo OD. [Cutaneous myiasis due to Cochliomyia hominivorax associated with seborrheic dermatitis]. Rev Med Chil. (2017) 145:250–4. doi: 10.4067/S0034-98872017000200013
83. Durão C, Barros A, Campos P. A rare case of digital myiasis. J Infect Public Health. (2017) 10:886–7. doi: 10.1016/j.jiph.2016.11.002
84. Vianna Gontijo JR, Vasques Bittencourt F. Wound myiasis: the role of entodermoscopy. Anais Brasileiros de Dermatologia. (2018) 93:746–8. doi: 10.1590/abd1806-4841.20188043
85. Failoc-Rojas VE, Molina-Ayasta C, Salazar-Zuloeta J, Samamé A, Silva-Díaz H. Case report: Myiasis due to Cochliomyia hominivorax and Dermatobia hominis: clinical and pathological differences between two species in Northern Peru. Am J Trop Med Hyg. (2018) 98:150–3. doi: 10.4269/ajtmh.16-0437
86. Villamil-Gómez WE, Cardona-Ospina JA, Prado-Ojeda JS, Hernández-Prado H, Figueroa M, Causil-Morales PN, et al. Pin-Site myiasis caused by screwworm fly in nonhealed wound, Colombia. Emerg Infect Dis. (2019) 25:379–80. doi: 10.3201/eid2502.181053
87. Forero E, Cortés J, Villamil L. The problem of screwworm, Cochliomyia hominivorax (Coquerel, 1858), in Colombia. Rev MVZ Córdoba. (2008) 13:1400–14.
88. Pape T, Wolff M, Amat E. Los califóridos, éstridos, rinofóridos y sarcofágidos (Diptera: Calliphoridae, Oestridae, Rhinophoridae, Sarcophagidae) de Colombia. Biota Colomb. (2004) 5:201–8.
89. Maxwell M, Subia J, Abrego J, Garabed R, Xiao N, Toribio R. Temporal and spatial analysis of the new world screwworm (Cochliomyia hominivorax) in Darien and Embera, Panama (2001–2011). Transb Emerg Dis. (2017) 64:899–905. doi: 10.1111/tbed.12457
90. Forero-Becerra G, Cortés-Vecino J, Villamil-Jiménez L. Associated risk factors to myiasis by Cochliomyia hominivorax on cattle farms in Puerto Boyacá (Colombia). Rev Científica Fac de Cienc Vet Univ del Zulia. (2009) 19:460–5.
91. Adams TS, Reinecke JP. The reproductive physiology of the screwworm, Cochliomyia hominivorax (Diptera: Calliphoridae). I. oogenesis. J Med Entomol. (1979) 15:472–83. doi: 10.1093/jmedent/15.5-6.472
92. Thomas DB, Mangan RL. Oviposition and wound-visiting behavior of the screwworm fly, Cochliomyia hominivorax (Diptera: Calliphoridae). Ann Entomol Soc Am. (1989) 82:526–34. doi: 10.1093/aesa/82.4.526
Keywords: screwworm infection, newborn, umbilicus, myiasis, ivermectin, Colombia
Citation: Ruiz-Zapata JD, Figueroa-Gutiérrez LM, Mesa-Franco JA and Moreno-Gutierrez PA (2020) Umbilical Myiasis by Cochliomyia hominivorax in an Infant in Colombia. Front. Med. 6:292. doi: 10.3389/fmed.2019.00292
Received: 22 July 2019; Accepted: 28 November 2019;
Published: 22 January 2020.
Edited by:
Matthew H. Collins, Emory University, United StatesReviewed by:
Mario Santoro, Stazione Zoologica Anton Dohrn, ItalyAna Afonso, University of São Paulo, Brazil
Copyright © 2020 Ruiz-Zapata, Figueroa-Gutiérrez, Mesa-Franco and Moreno-Gutierrez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Paula Andrea Moreno-Gutierrez, cGF1bGEubW9yZW5vQHVhbS5lZHUuY28=