 Habib Benzian*†
Habib Benzian*† Richard Niederman†
Richard Niederman†- WHO Collaborating Center Quality Improvement & Evidence-Based Dentistry, Department Epidemiology & Health Promotion, College of Dentistry, New York University, New York, NY, United States
Dental services are significantly impacted by the COVID-19 pandemic. Almost all dental procedures carry a high infection risk for providers and patients due to the spread of aerosols. As a consequence, public health agencies and professional associations have issued guidelines for enhanced infection control and personal protection equipment and have also limited care to urgent or emergency services. However, there is no dental service concept for pandemic disaster preparedness or response that might be applied. Moreover, pathways to dental care provision in a post-pandemic future with persisting risks are needed. We propose Safer Aerosol-Free Emergent Dentistry (SAFER Dentistry) as one approach to dental services during and emerging from the pandemic. The concept's starting point is the identification of the most common patient needs. The next step is to replace common treatments addressing the most frequent needs with alternative interventions involving a lower infection risk because they do not generate aerosols. SAFER Dentistry is innovative, avoids risk, and responds to the requirements of a pandemic and post-pandemic emergency where the risk of airborne disease transmission remains high. SAFER Dentistry thereby ensures continuity of dental services while protecting providers and patients from infectious pathogens. Moreover, SAFER Dentistry allows dental service providers to remain operational and generate income even under pandemic conditions. Potential implementation and policy options for SAFER Dentistry include universal availability without co-payments by patients and a uniform bundled payment scheme for providers to simplify budgeting, reimbursement, and administration during a pandemic. Adaptations and adjustments of the concept are possible and encouraged as long as the principle of avoiding aerosol-generating procedures is maintained.
SARS-CoV-2 Disrupts Health Care and Dentistry Worldwide
In a crisis, be aware of the danger, but recognize the opportunity. John F. Kennedy.
Healthcare services are adapting to the COVID-19 pandemic, yet oral health care and dentistry are particularly affected due to the proximity to the patient and the generation of aerosols through common treatment procedures. The SARS-CoV-2 virus seriously disrupts routine dental procedures around the world. The reports, analyses, and recommendations emerging alongside first-hand experience from dental settings in China are alarming (1, 2). The risks of infection for oral health personnel as well as cross-infection between patients and anyone in a dental care setting are high.
The toll of the COVID-19 pandemic on health systems and availability of dental care has been unprecedented. At the height of the pandemic in the U.S., about 80% of practices offered only limited emergency services, and 17% did not see patients at all (3). This impacts heavily on service availability and patient access to essential services. At the same time, such service limitations result in significant economic losses for the entire dental sector, leading to layoffs of dental teams and growing unemployment. In addition, the prospect of re-starting services remains bleak and uncertain and will be so for months to come (4). Little is known so far about the impact on dental services in low- and middle-income countries, though recommendations for service limitations to emergency care and increased precautions were issued in many countries (5).
The Infection Risk From Aerosols in Dentistry
Dental teams are generally used to high standards of infection control and personal protection measures owing to the fact that dental personnel are among the most at risk for any kind of infection transmitted via contaminated aerosols and saliva, bodily fluids, blood, or tissue particles (6, 7).
Current evidence suggests three main pathways for virus transmission in dental settings: (1) direct transmission through inhalation of cough, sneeze, or droplets containing the virus; (2) transmission via eye, nasal, or oral mucous membranes; and (3) contact transmission through contaminated surfaces (2). All these transmission pathways are facilitated and possibly amplified by aerosols that are generated by most dental procedures (7, 8).
In reaction to the COVID-19 pandemic, international and U.S. federal public health agencies, as well as dental professional associations, have issued specific guidance for the control of SARS-CoV-2 in dental practice (5, 9–13).
These recommendations focus on three main areas where adaptation to the pandemic context is required to break potential transmission chains: patient management and teledentistry to prevent sick or possibly infected patients from coming to the practice, enhanced infection-control measures that include strict protocols for personal protective equipment (PPE), and limitation of dental care to urgent and emergency procedures. Some authorities demand that for patients with COVID-19 symptoms, emergency oral health care should be performed in a negative-pressure operatory with maximum PPE to reduce infectious health hazards (14, 15). Countries like the UK have therefore established special dental care centers to ensure appropriate protection (16).
In the U.S., the Occupational Safety and Health Administration (OSHA) considers work environments where aerosols may occur to be of high or very high infection risk for COVID-19 (14). In a specific update for dentistry, the OSHA requires telephone triage, office engineering controls that include air circulation and patient isolation, universal precautions for airborne pathogens, the use of PPE appropriate for the pandemic, limiting care to urgent and emergency procedures that do not generate aerosols, and environmental cleaning post-care. The recommendation for airborne infection isolation rooms (AIIR) with negative pressure is in line with the U.S. Centers for Disease Control and Prevention's (CDC) existing guidance (17).
Such measures beyond the standard dental infection-control procedures are challenging due to limited or costly supplies of PPE, and they would require significant infrastructure investments. Many of the requirements are unrealistic to achieve even in sophisticated university dental college settings, at least in the short term. For many dental care contexts, such as mobile dental services for schools, remote communities, nursing homes, prisons, homeless shelters, or refugee camps, as well as dental services in low-resource settings where the shortage of supplies is a constant challenge, such enhanced protective measures are near impossible.
The risks from infectious aerosols are central to all recommended alterations of current dental practice, yet uncertainties and open questions related to transmission details remain and oblige dental practitioners to assume they are operating under the highest possible infection risk and to act accordingly with appropriate precautions (18).
Dentistry as we know it is seriously disrupted and may not be able to return to the clinical routines of a pre-COVID-19 time. At this point of the pandemic, dentistry needs a concept for continued dental services that avoids procedures generating infectious aerosols while being able to address the most frequent patient oral health needs.
Safer Aerosol-free Emergent (SAFER) Dentistry
With aerosol-generating procedures being at the core of the current challenge for dental services, interventions that avoid aerosol generation should be the interventions of choice. Such procedures exist and may replace possibly hazardous “standard” therapies in an emergency context with airborne pathogens such as SARS-CoV-2. We propose the concept of Safer Aerosol-Free Emergent Dentistry (SAFER Dentistry). SAFER Dentistry builds on a prioritization of the most common patient needs, and systematically selects bundles of effective, evidence-based, and value-based care that do not require aerosol-generating procedures.
Focusing on emergency and urgent dental services, SAFER Dentistry addresses common care scenarios with a set of bundled interventions. Table 1 details the treatment options with significantly lower risk of generating aerosols, including scientific references for the respective non-aerosol options. They comprise the following.
1. Examination/diagnosis via in-person teledentistry: when performed in person, this includes antiseptic mouthrinse and visual and/or tactile inspection without intraoral radiography for diagnosis.
2. Acute pain, swelling, or infection: depending on the diagnosis, pulp devitalization/temporary filling (pulpitis), antibiotic therapy (acute inflammation), and/or local anesthesia and tooth extraction.
3. Toothache due to caries without pulpal involvement: silver-diamine-fluoride application (SDF), glass-ionomer sealants/Atraumatic Restorative Treatment (ART), fluoride varnish/gel, and/or toothbrushing with high fluoride-containing toothpaste (HFT, 5,000 ppm fluoride).
4. Acute periodontitis: hand scaling and metronidazole/amoxicillin combination for 1 week.
5. Denture repair/reline, lost crown or orthodontic bracket, or orthodontic wire: denture repair with soft re-line, crown and bracket re-cementation, and wire adjustment, repair, or removal as well as removal of stiches from previous surgery.
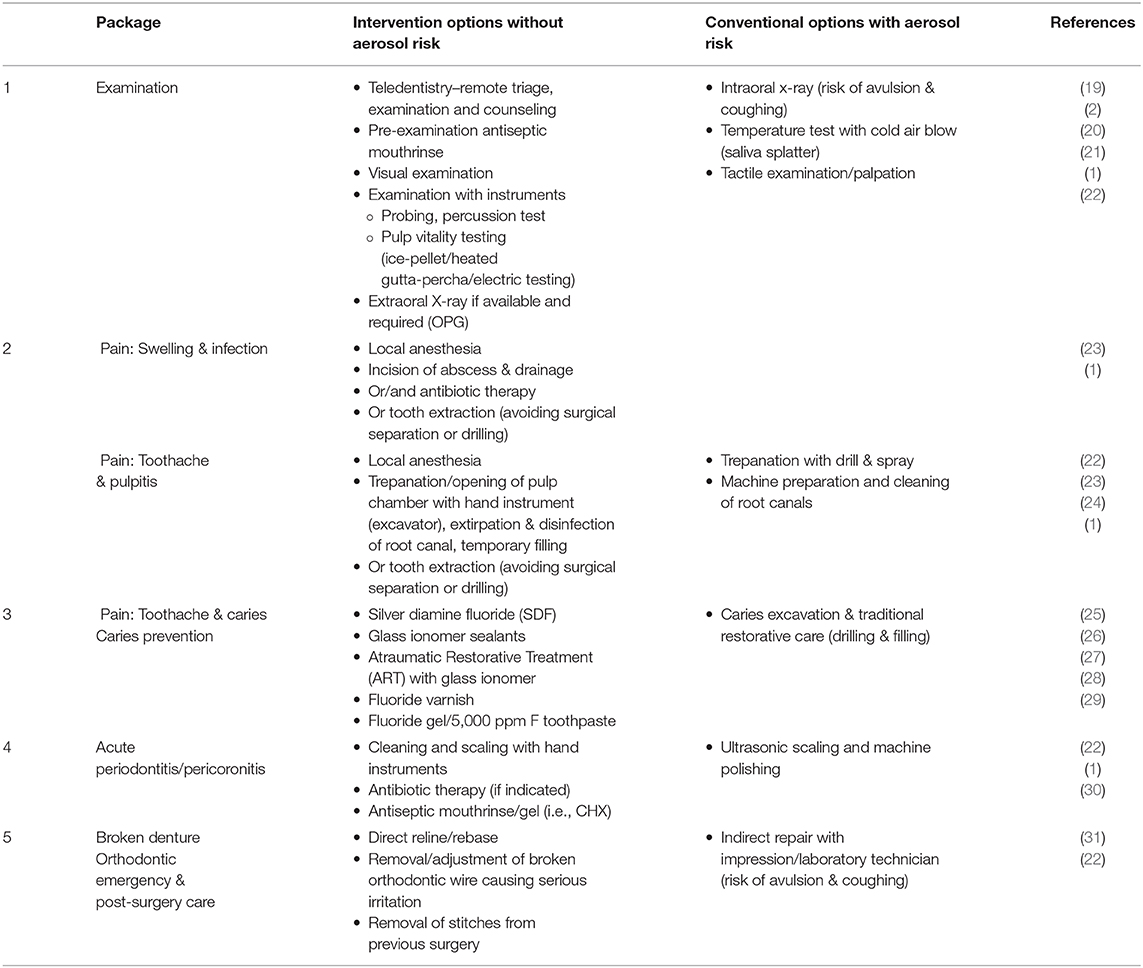
Table 1. SAFER Dentistry Packages and intervention options.
The interventions of SAFER Dentistry are effective and realistic, even for resource-poor settings. Individually, they have been used for decades and have been promoted widely (30). The systematic bundling and prioritization, however, is new and innovative and responds to a pandemic and post-pandemic context where the risk of disease transmission remains high or might be intermittently increasing or decreasing. This approach ensures that dental services can continue during a pandemic by providing oral health care for the most frequent patient needs, while protecting providers and patients from pathogens. Dental teams will require little to no additional training to perform the interventions of SAFER Dentistry, since none of the procedures are new or unknown.
There is no clinical dental care situation without any infectious risk. The alternative interventions suggested are not completely risk-free, but carry a significantly lower and more manageable risk. We therefore use the acronym SAFER Dentistry in analogy to the HIV pandemic's response concept of Safer Sex, which also significantly reduces the risk of transmission of HIV and other sexually transmitted diseases (32).
Healthy System Options for Implementing SAFER Dentistry
Pandemics are a constant challenge to public health and reveal with relentless clarity the shortcomings of health systems in terms of capacity, coverage, quality, and financing. The same applies to inequalities and differential impact of the pandemic on different population groups. Oral health status and access to dental care has long been recognized as a prime example for such challenges (33). With millions of people unemployed due to the COVID-19 pandemic, many are losing their health insurance benefits at a time when most needed. There is growing recognition that basic health (and oral health) services are a public good that should be universally available for everyone, irrespective of their employment status (34). SAFER Dentistry, covering the most frequent oral health needs, is one starting point for a basic oral health benefit package. Further adaptations and evolving implementation may also include aerosol-free cavity prevention (dental sealants and the like) and other preventive measures to reduce the need for dental care as pandemics continue to emerge. In order to ensure maximum population coverage, we propose that SAFER Dentistry be universally available with no co-payments. Initial economic modeling for children shows that SAFER Dentistry is cost-saving and cost-effective compared to conventional aerosol-generating interventions (35).
Providers could be reimbursed through a single, uniform payment for any combination of examination and additional procedure, thereby simplifying documentation, billing, and reimbursement, which is of particular importance in an emergency context. Such an approach would work for health systems relying on a fee-for-service approach as well as for capitation-based systems. However, the details of the required changes in guidelines, service directives or other adaptations need to be determined nationally/locally depending on existing conditions, resources, local guidelines, and political support. Aspects of teledentistry should be included in the benefit package since they will become a more frequent practice and specific reimbursement positions are often not yet in place (19).
As the pandemic and related limitations of clinical practice endure, more and more patients will have to use emergency hospital services for relief of their dental problems. In the US, even without a pandemic, every 15 s a patient visits a hospital emergency service for dental care due to millions lacking dental insurance coverage (36). Universally available SAFER Dentistry would reduce such hospital visits for common dental ailments and unburden hospital personnel, infrastructure, and resources; it would instead offer an opportunity for dental service providers to remain operational and generate income. At the same time, SAFER Dentistry allows providers to offer a safe and hygienic service environment as a key component to regaining patient trust in the period of pandemic recovery.
Conclusions
The early experiences in dentistry from China during this COVID-19 pandemic are instructive and telling: They implemented rapid and bold actions to contain the pandemic, including limited emergency dental services in a tertiary care center with maximum precautions (1). The UK and other countries also established specialized emergency care centers for dentistry (37, 38). Yet, the level of infrastructure and service provisions possible in such centers are not realistic for general dental practices or oral health training programs in the U.S. or globally.
SAFER Dentistry, together with general measures to mitigate risk in dental settings, is an adaptation to a pandemic emergency and a pandemic recovery process by avoiding hazardous infectious aerosols. It is also a first step toward oral health care that does not require complex technology, as envisaged in the landmark Lancet Series on Oral Health (39). If continued and institutionalized as a universally available benefit and coverage feature, substantial gains in oral health status and significant reductions in oral health care expenditure could be achieved in the long run.
The dangers of the crisis are clear. Continuation of dentistry as usual during the COVID-19 pandemic will result in incalculable risks for patients and providers. For U.S. governmental agencies and professional organizations, oral healthcare training institutions, clinicians, and patients not willing to accept a complete shutdown of oral healthcare, including deterioration of health and well-being, there is no alternative to SAFER Dentistry.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Meng L, Hua F, Bian Z. Coronavirus Disease 2019 (COVID-19): emerging and future challenges for dental and oral medicine. J Dent Res. (2020) 99:481–7. doi: 10.1177/0022034520914246
2. Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. (2020) 12:9. doi: 10.1038/s41368-020-0075-9
3. Health Policy Institute (HPI) American Dental Association (ADA). COVID-19: Economic Impact on Dental Practices (week of April 20 results). Available online at: https://bit.ly/2z9tLcY (accessed May 25, 2020).
4. Nasseh K, Vujicic M. Modeling the Impact of COVID-19 on U.S. Dental Spending. Chicago: Health Policy Institute/American Dental Association (2020).
5. COVID-19 Dental Services Evidence Review (CoDER) Working Group. Recommendations for the Re-Opening of Dental Services: A Rapid Review of International Sources (Version 1.3). Available at: https://oralhealth.cochrane.org/sites/oralhealth.cochrane.org/files/public/uploads/covid19_dental_reopening_rapid_review_07052020.pdf (accessed May 13, 2020)
7. Harrel SK, Molinari J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc. (2004) 135:429–37. doi: 10.14219/jada.archive.2004.0207
8. Ge Z-y, Yang L-m, Xia J-j, Fu X-h, Zhang Y-z. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J Zhejiang Univ Sci B. (2020) 21:361–8. doi: 10.1631/jzus.B2010010
9. Centers for Disease Control and Prevention (CDC). Guidance for Dental Settings: Interim Infection Prevention and Control Guidance for Dental Settings During the COVID-19 Response. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html (accessed May 19, 2020).
10. Indian Dental Association. COVID-19 Advisory. Available online at: https://www.ida.org.in/pdf/20200317_Advisory_on_Corona.pdf (accessed March 17, 2020).
11. Lazzerini M, Putoto G. COVID-19 in Italy: momentous decisions and many uncertainties. Lancet Glob Health. (2020) 8:e641–2. doi: 10.1016/S2214-109X(20)30110-8
12. Ordre National des Chirugiens-Dentistes [French National Dental Council]. Recommandations d'experts pour la prise ne charge des patients en cabinet dentaire de ville au stade 3 de l'epidemie de COVID-19 [Expert recommendations for patient care in urban dental clinics during phase 3 of the COVID-19 epidemic. Available online at: https://lescdf.fr/sites/default/files/inline-files/Recommandations%20COVID%2019%20v1%2024%20mars%202020_0.pdf (accessed March 24, 2020).
14. Occupational Safety and Health Administration (OSHA) Department of Labor. Guidance on Preparing Workplaces for COVID-19 (OSHA 3990-02 2020). Available online at: www.osha.gov/Publications/OSHA3990.pdf (accessed May 25, 2020).
15. Ather A, Patel B, Ruparel N, Diogenes A, Heargreaves K. Coronavirus Disease 19 (COVID-19): implications for clincial dental care. J Endod. (2020) 46:584–95. doi: 10.1016/j.joen.2020.03.008
16. Carter E, Currie C, Asuni A, Goldsmith R, Toon G, Horridge C, et al. The first 6 weeks: setting up a UK urgent dental care centre during the COVID-19 pandemic. Br Dent J. (2020) 228:842–8. doi: 10.1038/s41415-020-1708-2
17. Cleveland JL, Robison VA, Panlilio AL. Tuberculosis epidemiology, diagnosis and infection control recommendations for dental settings: an update on the Centers for Disease Control and Prevention guidelines. J Am Dent Assoc. (2009) 140:1092–9. doi: 10.14219/jada.archive.2009.0335
18. Beltrán-Aguilar E, Benzian H, Niederman R. Rational perspectives on risk and certainty for dentistry during the COVID-19 pandemic. Am J Infect Control. (2020). doi: 10.1590/SciELOPreprints.537
19. Alabdullah JH, Daniel SJ. A systematic review on the validity of teledentistry. Telemed e-Health. (2018) 24:639–48. doi: 10.1089/tmj.2017.0132
20. Chen E, Abbott PV. Dental pulp testing: a review. Int J Dent. (2009) 2009:365785. doi: 10.1155/2009/365785
21. Bartoloni J, Basquill L. Infection control and dental radiography. Infection Control Pract. (2003) 2:1–8.
22. Alharbi A, Alharbi S, Alqaidi S. Guidelines for dental care provision during the COVID-19 pandemic. Saudi Dental J. (2020) 32:181–6. doi: 10.1016/j.sdentj.2020.04.001
23. Dave M, Seoudi N, Coulthard P. The oral surgery response to urgent dental care for patients during the COVID-19 pandemic. Lancet. (2020) 395:1257. doi: 10.1016/S0140-6736(20)30806-0
24. Yu J, Zhang T, Zhao D, Haapasalo M, Shen Y. Characteristics of endodontic emergencies during COVID-19 outbreak in Wuhan. J Endodontics. (2020).
25. Seifo N, Robertson M, MacLean J, Blain K, Grosse S, Milne R, et al. The use of silver diamine fluoride (SDF) in dental practice. British Dental J. (2020) 228:75–81. doi: 10.1038/s41415-020-1203-9
26. Marinho VC, Worthington HV, Walsh T, Chong LY. Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. (2015) 6:CD002280. doi: 10.1002/14651858.CD002280.pub2
27. Frencken JE. Atraumatic restorative treatment and minimal intervention dentistry. Br Dent J. (2017) 223:183–9. doi: 10.1038/sj.bdj.2017.664
28. Slayton RL, Urquhart O, Araujo MWB, Fontana M, Guzmán-Armstrong S, Nascimento MM, et al. Evidence-based clinical practice guideline on nonrestorative treatments for carious lesions: a report from the American Dental Association. J Am Dent Assoc. (2018) 149:837–49.e19. doi: 10.1016/j.adaj.2018.07.002
29. Douglas GV, Ramsdale MP, Vinall-Collier K, Csikar JI. Using high fluoride concentration products in public policy: a rapid review of current guidelines for high fluoride concentration products. Caries Res. (2016) 50(Suppl. 1):50–60. doi: 10.1159/000443409
30. Niederman R, Feres M, Ogunbodede E. Chapter 10: Dentistry. In: Debas H, Donkor P, Gawande A, J amison D, Kruk M, Mock C, Washington DC: World Bank (2015). p. 173–195. doi: 10.1596/978-1-4648-0346-8_ch10
31. Felton D, Cooper L, Duqum I, Minsley G, Guckes A, Haug S, et al. Evidence-based guidelines for the care and maintenance of complete dentures: a publication of the American College of Prosthodontists. J Prosthodontics. (2011) 20:S1–S12. doi: 10.1111/j.1532-849X.2010.00683.x
32. Merson MH, O'Malley J, Serwadda D, Apisuk C. The history and challenge of HIV prevention. Lancet. (2008) 372:475–88. doi: 10.1016/S0140-6736(08)60884-3
33. Peres MA, Daly B, Guarnizo-Herreno C, Benzian H, Watt R. Oral diseases: a global public health challenge - Author's Reply. Lancet. (2020) 395:186–7. doi: 10.1016/S0140-6736(19)32997-6
34. Chakrabarti M. COVID-19: Make Health Systems a Global Public Good (27 April 2020); OECD Development Matters (Blog). Available at: https://oecd-development-matters.org/2020/04/29/covid-19-make-health-systems-a-global-public-good/ (accessed April 27, 2020).
35. Huang SS, Ruff RR, Niederman R. An economic evaluation of a comprehensive school-based caries prevention program. JDR Clin Trans Res. (2019) 4:378–87. doi: 10.1177/2380084419837587
36. Health Policy Institute (HPI) American Dental Association (ADA). Emergency Departments Visits for Dental Conditions - A Snapshot. (2020). Available online at: https://www.ada.org/media/ADA/Science%20and%20Research/HPI/Files/HPIgraphic_0420_1.pdf?la=en (accessed May 25, 2020).
37. NHS England, NHS Improvement. COVID-19 Guidance and Standard Operating Procedure. Urgent Dental Care Systems in the Context of the Coronavirus. Available at: https://bit.ly/3b4BAhw (accessed April 15, 2020).
38. Bundeszahnärztekammer [German Federal Dental Council]. Position zur Ausbreitung von Sars-CoV-2/COVID 19. Risikomanagement in Zahnarztpraxen [Position on the Sars-CoV-2/COVID 19 epidemic. Risk management in dental clinics]. available at https://www.bzaek.de/fileadmin/PDFs/b/2020_Position_Sars-CoV-2.pdf (accessed March 27, 2020).
Keywords: COVID-19, infection control, pandemic preparedness and response, infectious dental aerosols, airborne transmission of diseases, dental care, emergency dental service
Citation: Benzian H and Niederman R (2020) A Dental Response to the COVID-19 Pandemic—Safer Aerosol-Free Emergent (SAFER) Dentistry. Front. Med. 7:520. doi: 10.3389/fmed.2020.00520
Received: 09 May 2020; Accepted: 27 July 2020;
Published: 12 August 2020.
Edited by:
Nicola Petrosillo, Istituto Nazionale per le Malattie Infettive Lazzaro Spallanzani (IRCCS), ItalyReviewed by:
Lin Chen, Jinhua Central Hospital, ChinaFang Hua, School of Stomatology, Wuhan University, China
Copyright © 2020 Benzian and Niederman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Habib Benzian, aGFiaWIuYmVuemlhbkBueXUuZWR1
†These authors have contributed equally to this work