 Silvana Júnia Roriz1
Silvana Júnia Roriz1 Thiago Almeida Pereira1,2*
Thiago Almeida Pereira1,2* Guilherme Vaz de Melo Trindade1,3Júlia Fonseca de Morais Caporali1,4
Guilherme Vaz de Melo Trindade1,3Júlia Fonseca de Morais Caporali1,4 José Roberto Lambertucci1,4
José Roberto Lambertucci1,4- 1Graduate Program in Infectious Diseases and Tropical Medicine, School of Medicine, Federal University of Minas Gerais, Belo Horizonte, Brazil
- 2Institute for Stem Cell Biology and Regenerative Medicine, Stanford University School of Medicine, Stanford, CA, United States
- 3Physiology, School of Medicine, National University of Ireland, Galway, Galway, Ireland
- 4Department of Internal Medicine, School of Medicine, Federal University of Minas Gerais, Belo Horizonte, Brazil
Schistosomiasis is a major public health problem in tropical areas of the world. Health-related quality of life (HRQOL) measurement is being widely used to evaluate the impact of a disease or treatment in several aspects of daily life. However, few studies evaluated the impact of severe forms of schistosomiasis on HRQOL of affected individuals and compared them to healthy controls with a similar socio-demographic background. Our aims were to evaluate the HRQOL in patients with hepatosplenic schistosomiasis (HS) and schistosomal myeloradiculopathy (SMR) and healthy volunteers (HV) and determine if clinical complications of the disease are associated with HRQOL scores. We interviewed and evaluated the HRQOL in 49 patients with HS, 22 patients with SMR, and 26 HV from an outpatient clinic of the Federal University of Minas Gerais University Hospital using the WHOQOL-BREF questionnaire. SMR and HS patients had a significantly lower overall quality of life score when comparing with the HV control group (p = 0.003 and p = 0.005, respectively). Multivariate ordinal regression model adjusted for sex, age, and educational level indicated that HS and SMR patients have three and five times more chances of having a lower quality of life than healthy volunteers (Odds Ratio 3.13 and 5.04, respectively). There was no association between complications of HS disease and quality of life scores. In contrast, worse quality of life was observed in SMR patients that presented back or leg pain, leg paresthesia, and bladder dysfunction. In conclusion, HS and SMR significantly impact the overall quality of life of the affected individuals, reinforcing the importance of efforts to control and eradicate this debilitating disease and suggesting that multidisciplinary clinical management of schistosomiasis patients would be more appropriate and could potentially improve patient's quality of life.
Introduction
Schistosomiasis continues to be a significant health threat in tropical areas of the world, affecting over 250 million people (1). In Brazil, the country harboring most cases in the Americas, it is estimated that 1.6–6 million people are infected with Schistosoma mansoni, and over 25 million individuals are at risk of infection (2–5).
Infected individuals have various clinical manifestations that generally cluster into three distinct forms of the disease: acute, hepatointestinal, and hepatosplenic schistosomiasis (6, 7). Ectopic forms of the disease can occur, and schistosomal myeloradiculopathy is the most severe and disabling ectopic manifestation of schistosomiasis (6–9).
The acute phase is rarely symptomatic in infected individuals from endemic areas due to early childhood infection and exposure to schistosome antigens and anti-schistosome antibodies in-utero and breast milk (6, 10). In contrast, individuals from non-endemic areas that become infected with S. mansoni usually develop a symptomatic acute form of schistosomiasis, characterized by a systemic hypersensitivity reaction against the migrating schistosomula and mature eggs (6, 10). The majority of chronically infected individuals develop hepatointestinal schistosomiasis (90–96%), a mild form of the disease consisted of granulomatous hepatic and intestinal inflammation, absent or discrete hepatosplenomegaly, and minimal liver periportal fibrosis without portal hypertension (7, 11). The severe form of the disease, named hepatosplenic schistosomiasis, is observed in a small percentage of infected individuals (4–10%) and is characterized by hepatosplenomegaly, severe liver periportal fibrosis, portal hypertension, and thrombocytopenia (7, 11). Schistosomal myeloradiculopathy is the most common manifestation of neuroschistosomiasis associated with S. mansoni infection (8, 9). This ectopic form of the disease can be observed in patients with acute or hepatointestinal schistosomiasis but is rarely observed in hepatosplenic patients (8, 9). Patients with schistosomal myeloradiculopathy frequently present lumbar and lower limb pain, paraparesis, paresthesia, and bladder dysfunction (urinary retention and other urological complications such as hydronephrosis, bladder calculi and recurrent urinary tract infections) (8, 9). The lesions are caused by a granulomatous inflammation induced by the eggs trapped in the central nervous system (8, 9).
Health-related quality of life (HRQOL) measurement is being widely used to evaluate the impact of a disease or treatment in several aspects of daily life (12, 13). Assessment of HRQOL, together with morbidity and mortality measurements, is crucial to determine the disease's burden in the community, evaluate interventions and standard health care policies, and identify areas that require further improvement (12–16). Generic HRQOL, such as WHOQOL-BREF or EQ-5D-3L, has been validated in different languages, cultural settings, and different diseases, including schistosomiasis (12–25).
Hepatosplenic schistosomiasis and schistosomal myeloradiculopathy are considered the most severe manifestations of S. mansoni infection (7–9). However, few studies evaluated the impact of severe forms of schistosomiasis on HRQOL of affected individuals and compared to healthy controls with a similar socio-demographic background (15, 17–19, 22, 26).
In Brazil, a recent study investigated the quality of life and quality-adjusted life years in chronic schistosomiasis patients and observed a similar reduction of HRQOL in hepatointestinal and hepatosplenic patients (22). Although some studies evaluate HRQOL in hepatointestinal patients with different intensity of infection, or hepatosplenic patients with different degrees of morbidity, no study evaluated schistosomal myeloradiculopathy's impact on HRQOL (15, 17–19, 22, 26). Therefore, our aims were to evaluate the HRQOL in healthy volunteers and patients with hepatosplenic schistosomiasis and schistosomal myeloradiculopathy and determine if the disease's clinical manifestations are associated with HRQOL scores.
Materials and Methods
Study Design and Ethical Considerations
This was a descriptive, observational cross-sectional study approved by the Federal University of Minas Gerais Research Ethics Committee (Protocol 692545/2014) and fully conducted according to the guidelines in the Declaration of Helsinki from the World Medical Association (27). All patients and healthy volunteers agreed to participate and provided informed consent to be included in this study. Interviews were conducted in a private room to ensure the patient's privacy.
Study Population and Inclusion Criteria
We recruited patients with hepatosplenic schistosomiasis mansoni (HS) and with schistosomal Myeloradiculopathy (SMR) previously diagnosed and currently receiving medical care at Orestes Diniz Infectious and Parasitic Diseases Treatment Center, an outpatient clinic of the Federal University of Minas Gerais University Hospital (Belo Horizonte, Brazil). The caregivers accompanying patients to their clinic appointment served as non-infected controls and were included in the healthy volunteer group (HV). The sample size was calculated based on a pilot study conducted with 10 volunteers from each group (HS, SMR and HV) that indicated a minimum sample size 21 of participants for each study group, considering a 95% two-sided confidence level and 80% power. Adult individuals (18–65 years old) of both genders that fit the inclusion criteria for each group were invited to participate in the study. The following exclusion criteria were applied: individuals diagnosed with other infectious diseases, other liver diseases, other forms of myeloradiculopathy, and noticeable memory loss. HS group consisted of 49 adult patients, of both genders, with a previous hepatosplenic schistosomiasis diagnosis based on parasitological stool test (PST), rectal biopsy, liver biopsy serological tests and ultrasonography of the abdomen and upper digestive endoscopy. For the SMR group, 22 adult patients, of both genders, with a previous diagnosis of SMR based on PST, history of contact with S. mansoni contaminated freshwater, serological tests, examination of cerebrospinal fluid, clinical evidence of spinal cord injury confirmed by magnetic resonance of the lumbar spine and differential diagnosis to exclude other causes of myelitis (spinal cord trauma, tumor, vitamin B12 deficiency, antiphospholipid syndrome, diabetic or autoimmune vasculitis, HIV, HTLV, HCV, HSV, HBV, syphilis, tuberculosis, neurocysticercosis, medullary abscess, syringomyelia, herniated lumbar disc, polyradiculoneuritis, demyelinating diseases, radiotherapy) (8, 28), were included. The HV group consisted of 26 adults of both genders, that were the caregivers of patients undergoing treatment at the clinic and were apparently healthy, negative for S. mansoni infection, and without a previous diagnosis of schistosomiasis.
Assessment of Health-Related Quality of Life
All participants were interviewed on the day of their routine appointment at the outpatient clinic and answered a clinical-socio-demographic questionnaire and the WHOQOL-BREF questionnaire, the shortened version of the World Health Organization Quality of Life questionnaire (WHOQOL-100) (12). The WHOQOL-BREF contains 26 questions, with two questions referring to the overall quality of life and the remaining questions related to physical, psychological, social and environmental domains (12). The Portuguese language version of WHOQOL-BREF has been validated and is widely used in Brazil as an appropriate tool to measure HRQOL in clinical settings (29–33).
Statistical Analysis
The data collected was stored in a computerized database using Excel software (Microsoft Office 2013) and analyzed using the Statistical Package for Social Sciences software (SPSS), version 20.0 (SPSS, IBM Company, Chicago, IL). Significance was accepted at the 0.05 level. Frequency distribution tables were constructed, and central tendency and variability measures were calculated for the total sample and for each study group. Kolmogorov-Smirnov normality was used to determine if the variables have a Gaussian distribution. Categorical variables were compared using Pearson's chi-square or exact Fisher test, and the numerical variables using the Kruskal-Wallis test. For multiple comparisons among groups, Mann-Whitey test with Bonferroni correction was used. The proportional odds logistic regression model was used to estimate the odds ratio with 95% confidence intervals.
Results
The socio-demographic data of the study population are depicted in Table 1. All groups were similar regarding relationship status, race/skin color, household income, and BMI. However, the study groups differed when evaluating the variables sex, age, educational levels, and occupation. Males were predominant in the hepatosplenic schistosomiasis and schistosomal myeloradiculopathy groups, while females were the majority among the healthy volunteers. Although similar age distribution was observed in SMR and healthy volunteers, HS patients were, on average, about 7 years older. Healthy volunteers presented higher education levels (secondary and tertiary) than schistosomiasis patients. However, a higher frequency of college level educated individuals was observed in the SMR group. A higher frequency of individuals currently on sick leave were observed in the SMR group, and in SMR and HS groups, there were more retired and unemployed individuals than the HV group.
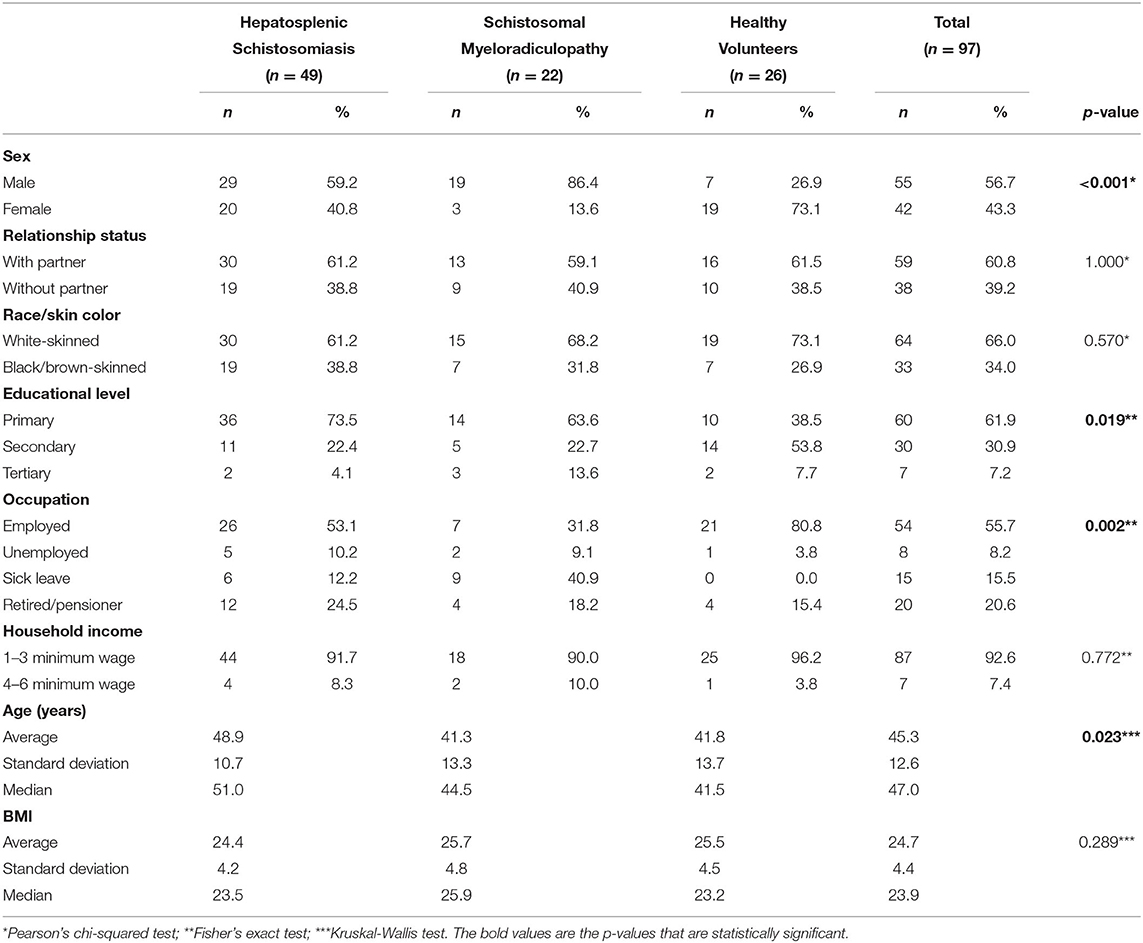
Table 1. Socio-demographic data of schistosomiasis patients and healthy volunteers included in this study.
The WHOQOL-BREF questionnaire analysis demonstrated that schistosomiasis patients had worse perceived health-related quality of life when taking into account the overall quality of life score (Table 2, p = 0.007). There were no statistical differences among groups when the physical, environmental, social, and psychological domains of WHOQOL-BREF were evaluated. Multiple comparison analysis demonstrated that SMR or HS had a significantly lower overall quality of life score when comparing with the HV group (p = 0.003 and p = 0.005, respectively). Although SMR had a lower overall quality of life score when compared to HS, this difference was not statistically significant (p = 0.363). Further analysis using the multivariate ordinal regression model and adjusting for sex, age, and educational level indicate that HS and SMR patients have three and five times more chances of having a lower quality of life than healthy volunteers (Table 3; Odds Ratio 3.13 and 5.04, respectively). Our model showed good agreement according to the deviance and parallel lines test (Table 3).
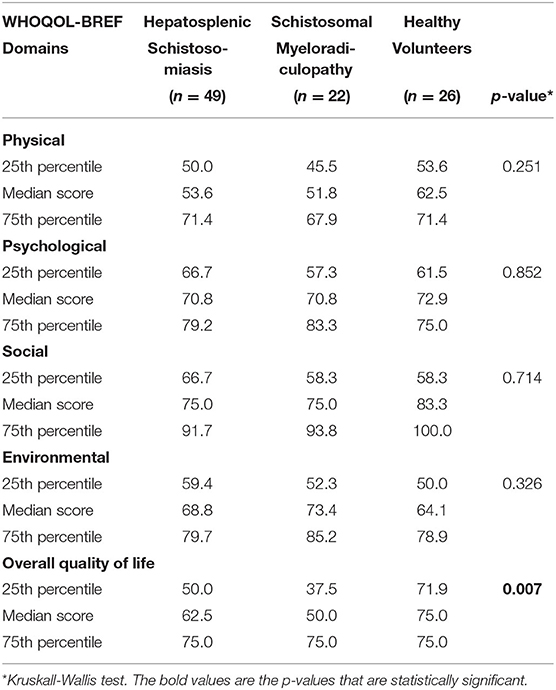
Table 2. Analysis of perceived quality of life in schistosomiasis patients and non-infected volunteers based on the short form of the World Health Organization Quality of Life questionnaire (WHOQOL-BREF).
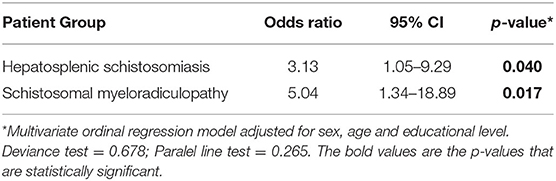
Table 3. Multivariate ordinal regression model for overall quality of life based on the short form of the World Health Organization Quality of Life questionnaire (WHOQOL-BREF) in patients with schistosomiasis compared to non-infected volunteers.
Finally we examined if complications of HS or SMR were associated with worse quality of life scores. For HS patients, there was no association between complications of the disease and quality of life scores (Table 4). In contrast, worse quality of life was observed in SMR patients that presented with back or leg pain, leg paresthesia, and bladder dysfunction (Table 5).
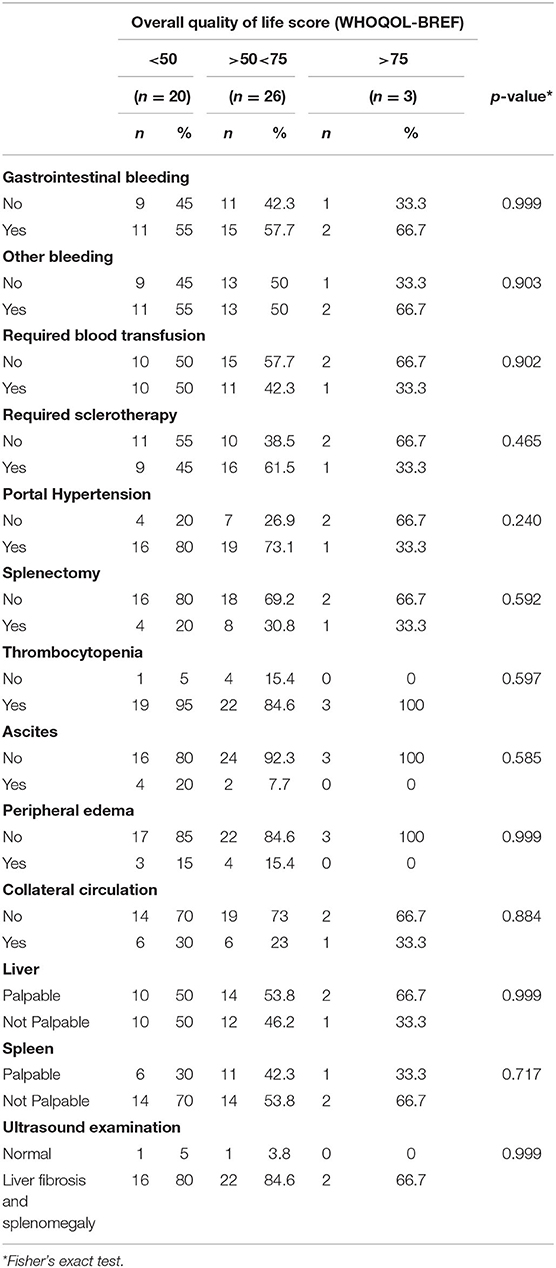
Table 4. Analysis of overall quality of life score and clinical complications of hepatosplenic schistosomiasis.
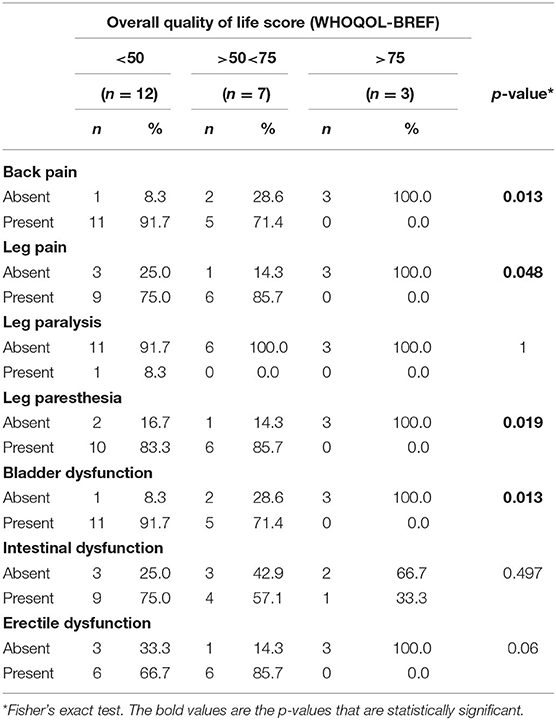
Table 5. Analysis of overall quality of life score and clinical complications of schistosomal myeloradiculopathy.
Discussion
Assessment of HRQOL in schistosomiasis patients is commonly used to evaluate therapeutic interventions and mass drug administration strategies in endemic areas (16, 19, 21, 23–25). However, studies that determine the burden of severe forms of schistosomiasis on patients' quality of life are scarce and rarely include an appropriate control group with similar socio-demographic background for comparison (15, 17, 18, 22, 26).
In the present study, we evaluated the HRQOL in healthy volunteers and patients with hepatosplenic schistosomiasis and schistosomal myeloradiculopathy. Although there was no significant difference among the groups on the scores in the four domains of the WHOQOL-BREF questionnaire, patients with schistosomiasis had a significantly lower overall quality of life score than healthy volunteers. SMR patients had lower scores of overall quality of life than HS, but this difference was not statistically significant. In addition, patients with HS had three times more chances to have lower scores of overall quality of life, while patients with SMR had five times more chances to present worse quality of life than healthy adults with similar socio-demographic backgrounds. To the best of our knowledge, our study is the first that addressed HRQOL in patients with SMR and compared the scores with HS patients and non-infected individuals.
Kamel et al. (26) evaluated S. mansoni and S. haematobium infection's impact on the quality of life and productivity in workers of a textile factory in Egypt. The authors used the WHOQOL-BREF questionnaire and demonstrated that infected individuals had lower scores in the physical, social, and environmental domains than non-infected workers (26). Furthermore, they observed a significant correlation between the severity of schistosomiasis and lower quality of life and productivity scores (26).
Furst et al. (18) investigated the self-reported quality of life using the WHOQOL-BREF questionnaire in adults with schistosomiasis, soil-transmitted helminthiasis, or non-infected volunteers in Côte d'Ivoire. Although the sample size of patients with schistosomiasis was small (187 participants, 2.1% infected with S. mansoni and 2.1% with S. haematobium), they observed that infection with S. mansoni reduced the overall quality of life of individuals by 16 points when compared to non-infected individuals, thus reinforcing that schistosomiasis have a significant impact on the quality of life of individuals (18). In our patient cohort, we observed that the median of the scores for overall quality of life in patients with HS and SMR patients were, respectively, 12.5 and 25 points lower than the scores for healthy volunteers.
In China, studies that used the EQ-5D plus questionnaire indicated that chronically infected patients with S. japonicum also had low quality of life scores and heavy disability weights that are associated with age, impaired work capacity, depression, anxiety, ascites, and active hepatitis B infection (15, 17). In our study, we did not find an association of lower quality of life scores and HS complications, but in SMR patients, lower scores were significantly associated with the presence of back or leg pain, leg paresthesia, and bladder dysfunction.
In Brazil, Barbosa and Pereira da Costa (34, 35) evaluated the impact of different forms of chronic schistosomiasis in the productivity of sugarcane cane cutters. Both studies were conducted prior to the standardization of HRQOL generic questionnaires and evaluated only the disease impact on the physical domain, and measured the productivity based on the salary received and tons of sugarcane collected by individuals from each group in one harvest (34, 35). The authors demonstrated that workers with hepatosplenic schistosomiasis had significantly lower productivity than workers with hepatointestinal form of the disease, indicating that hepatosplenic schistosomiasis negatively impacted the ability to work for those individuals (34, 35). We observed that HS patients had lower scores in the physical, social, and environmental domains than healthy volunteers, but this difference was not statistically different.
Nascimento et al. (22) conducted the first study of HRQOL in schistosomiasis patients in Brazil. HRQOL was investigated using the EQ-5D-3L questionnaire in 147 patients (56 hepatointestinal and 91 hepatosplenic). Although the authors did not include a non-infected control group, the study demonstrated that schistosomiasis is associated with lower scores in the pain/discomfort and anxiety/depression dimensions (22). Female patients and the presence of comorbidities were associated with worse quality of life, while there was no significant difference in the quality of life scores between hepatointestinal and hepatosplenic patients (22). In our study, none of the socio-demographic variables, including gender and the presence of comorbidities, were associated with poor quality of life. Only the variable “S. mansoni infection” was associated with lower scores of overall HRQOL.
This study indicated that HS and SMR patients had a higher chance of having a worse quality of life. However, our results should be taken with caution. The non-infected control group consisted of caregivers accompanying patients receiving medical care at our outpatient clinic. Although we observed significant differences among patients and non-infected controls, healthy volunteers also reported low scores of HRQOL. Cruz et al. (36) previously demonstrated that in Brazil lower quality of life is frequently observed in females, individuals from lower economic class, and individuals with lower education levels (36). The scores reported by Cruz et al. (36) for the physical, psychological, social and environmental domains of the WHOQOL-BREF questionnaire for healthy individuals from lower economic class (class D, household income = 2–4 minimum wage) were similar to our HV group (36). It has been reported that caregivers are subjected to psychological distress and have increased stress hormone levels and lower HRQOL than the general population (37). The HS, SMR, and healthy volunteer groups were fairly homogeneous regarding socio-demographic variables but differed in gender, age, educational levels, and occupation. We cautiously evaluated if the difference in the distribution of those variables influenced our results and adjusted the model to account for this caveat. Even though the groups were not as homogeneous as desirable, we were able to compare the groups and proceed with our analysis. Subsequent studies should avoid, if possible, discrepancies regarding the socio-demographic variables.
Some of the differences observed in the socio-demographic variables among the different groups are due to the inherent characteristics of the disease forms or related to the participants' professional occupation. HS patients are usually older than patients with other forms of schistosomiasis because severe liver fibrosis and portal hypertension take a long time to develop, and it usually requires multiple infections (7, 11). Symptomatic SMR is more frequently observed in males partly due to work-related exposure to S. mansoni in rural areas (8, 9). The HV group consisted of the caregivers accompanying patients to their visit to our outpatient clinic and were usually the patients' wives or daughters. SMR and HS are associated with high morbidity and are often incapacitating conditions; therefore, retirement, sick leave, and unemployment were more frequent among those groups. Unfortunately, we did not have access to patients with other clinical forms of schistosomiasis such as hepatointestinal schistosomiasis and symptomatic acute schistosomiasis. Future studies that include other forms of the disease and appropriately matched controls will be required to determine schistosomiasis' impact on HRQOL.
In conclusion, our results indicate that HS and SMR significantly impact the overall quality of life of the affected individuals, reinforcing the importance of efforts to control and eradicate this debilitating disease and suggesting that multidisciplinary clinical management of schistosomiasis patients would be more appropriate and could potentially improve patient's quality of life.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Federal University of Minas Gerais Research Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SR, TP, and JL designed the study, supervised patient recruitment, performed statistical analysis and wrote the manuscript. SR, GV, and JC recruited patients, performed the analytical tests, collected the data. All authors critically revised the manuscript and approved the final submission.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. McManus DP, Dunne DW, Sacko M, Utzinger J, Vennervald BJ, Zhou XN. Schistosomiasis. Nat Rev Dis Primers. (2018) 4:13. doi: 10.1038/s41572-018-0013-8
2. Katz N, Peixoto SV. Critical analysis of the estimated number of Schistosomiasis mansoni carriers in Brazil. Rev Soc Bras Med Trop. (2000) 33:303–8. doi: 10.1590/S0037-86822000000300009
3. Scholte RG, Gosoniu L, Malone JB, Chammartin F, Utzinger J, Vounatsou P. Predictive risk mapping of schistosomiasis in Brazil using Bayesian geostatistical models. Acta Trop. (2014) 132:57–63. doi: 10.1016/j.actatropica.2013.12.007
4. Oliveira WJ, Magalhaes FDC, Elias AMS, de Castro VN, Favero V, Lindholz CG, et al. Evaluation of diagnostic methods for the detection of intestinal schistosomiasis in endemic areas with low parasite loads: Saline gradient, Helmintex, Kato-Katz and rapid urine test. PLoS Negl Trop Dis. (2018) 12:e0006232. doi: 10.1371/journal.pntd.0006232
5. Silva-Moraes V, Shollenberger LM, Siqueira LMV, Castro-Borges W, Harn DA, Grenfell R, et al. Diagnosis of Schistosoma mansoni infections: what are the choices in Brazilian low-endemic areas? Mem Inst Oswaldo Cruz. (2019) 114:e180478. doi: 10.1590/0074-02760180478
6. Lambertucci JR. Acute schistosomiasis mansoni: revisited and reconsidered. Mem Inst Oswaldo Cruz. (2010) 105:422–35. doi: 10.1590/S0074-02762010000400012
7. Lambertucci JR. Revisiting the concept of hepatosplenic schistosomiasis and its challenges using traditional and new tools. Rev Soc Bras Med Trop. (2014) 47:130–6. doi: 10.1590/0037-8682-0186-2013
8. Lambertucci JR, Silva LC, do Amaral RS. Guidelines for the diagnosis and treatment of schistosomal myeloradiculopathy. Rev Soc Bras Med Trop. (2007) 40:574–81. doi: 10.1590/S0037-86822007000500016
9. Vale TC, de Sousa-Pereira SR, Ribas JG, Lambertucci JR. Neuroschistosomiasis mansoni: literature review and guidelines. Neurologist. (2012) 18:333–42. doi: 10.1097/NRL.0b013e3182704d1e
10. Caldas IR, Campi-Azevedo AC, Oliveira LF, Silveira AM, Oliveira RC, Gazzinelli G. Human schistosomiasis mansoni: immune responses during acute and chronic phases of the infection. Acta Trop. (2008) 108:109–17. doi: 10.1016/j.actatropica.2008.05.027
11. Andrade ZA. Schistosomiasis and liver fibrosis. Parasite Immunol. (2009) 31:656–63. doi: 10.1111/j.1365-3024.2009.01157.x
12. WHO. Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol Med. (1998) 28:551–8. doi: 10.1017/S0033291798006667
13. King CH. Health metrics for helminth infections. Acta Trop. (2015) 141:150–60. doi: 10.1016/j.actatropica.2013.12.001
14. King CH, Dangerfield-Cha M. The unacknowledged impact of chronic schistosomiasis. Chronic Illn. (2008) 4:65–79. doi: 10.1177/1742395307084407
15. Jia TW, Utzinger J, Deng Y, Yang K, Li YY, Zhu JH, et al. Quantifying quality of life and disability of patients with advanced schistosomiasis japonica. PLoS Negl Trop Dis. (2011) 5:e966. doi: 10.1371/journal.pntd.0000966
16. King CH, Binder S, Shen Y, Whalen CC, Campbell CH, Wiegand RE, et al. SCORE studies on the impact of drug treatment on morbidity due to Schistosoma mansoni and Schistosoma haematobium infection. Am J Trop Med Hyg. (2020) 103:30–5. doi: 10.4269/ajtmh.19-0830
17. Jia TW, Zhou XN, Wang XH, Utzinger J, Steinmann P, Wu XH. Assessment of the age-specific disability weight of chronic schistosomiasis japonica. Bull World Health Organ. (2007) 85:458–65. doi: 10.2471/BLT.06.033035
18. Furst T, Silue KD, Ouattara M, N'Goran DN, Adiossan LG, N'Guessan Y, et al. Schistosomiasis, soil-transmitted helminthiasis, and sociodemographic factors influence quality of life of adults in Cote d'Ivoire. PLoS Negl Trop Dis. (2012) 6:e1855. doi: 10.1371/journal.pntd.0001855
19. Won KY, Abudho B, Blackstock AJ, Montgomery SP, Kennedy ED, Person B, et al. Assessment of quality of life as a tool for measuring morbidity due to Schistosoma mansoni infection and the impact of treatment. Am J Trop Med Hyg. (2014) 90:322–8. doi: 10.4269/ajtmh.13-0361
20. Song L, Wu X, Ren J, Gao Z, Xu Y, Xie H, et al. Assessment of the effect of treatment and assistance program on advanced patients with schistosomiasis japonica in China from 2009 to 2014. Parasitol Res. (2016) 115:4267–73. doi: 10.1007/s00436-016-5207-y
21. Shen Y, King CH, Binder S, Zhang F, Whalen CC, Evan Secor W, et al. Protocol and baseline data for a multi-year cohort study of the effects of different mass drug treatment approaches on functional morbidities from schistosomiasis in four African countries. BMC Infect Dis. (2017) 17:652. doi: 10.1186/s12879-017-2738-5
22. Nascimento GL, Domingues ALC, Ximenes RAA, Itria A, Cruz LN, Oliveira MRF. Quality of life and quality-adjusted life years of chronic schistosomiasis mansoni patients in Brazil in 2015. Trans R Soc Trop Med Hyg. (2018) 112:238–44. doi: 10.1093/trstmh/try038
23. Shen Y, Wiegand RE, Olsen A, King CH, Kittur N, Binder S, et al. Five-year impact of different multi-year mass drug administration strategies on childhood Schistosoma mansoni-associated morbidity: a combined analysis from the Schistosomiasis consortium for operational research and evaluation cohort studies in the Lake Victoria regions of Kenya and Tanzania. Am J Trop Med Hyg. (2019) 101:1336–44. doi: 10.4269/ajtmh.19-0273
24. Abudho BO, Guyah B, Ondigo BN, Ndombi EM, Ireri E, Carter JM, et al. Evaluation of morbidity in Schistosoma mansoni-positive primary and secondary school children after four years of mass drug administration of praziquantel in western Kenya. Infect Dis Poverty. (2020) 9:67. doi: 10.1186/s40249-020-00690-7
25. Olsen A, Kinung'hi S, Kaatano G, Magnussen P. Changes in morbidity, physical fitness, and perceived quality of life among schoolchildren following four years of different mass drug administration strategies against Schistosoma mansoni infection in Mwanza Region, Northwestern Tanzania. Am J Trop Med Hyg. (2020) 102:100–5. doi: 10.4269/ajtmh.19-0428
26. Kamel MI, Ghafar YA, Foda N, Khashab S. Impact of type and stage of schistosomiasis on quality of life and productivity of infected workers. J Egypt Soc Parasitol. (2001) 31:153–67.
27. World Medical Association. World medical association declaration of helsinki ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
28. Caporali JF, Utsch Goncalves D, Labanca L, Dornas de Oliveira L, Vaz de Melo Trindade G, de Almeida Pereira T, et al. Vestibular Evoked Myogenic Potential (VEMP) Triggered by Galvanic Vestibular Stimulation (GVS): a promising tool to assess spinal cord function in schistosomal myeloradiculopathy. PLoS Negl Trop Dis. (2016) 10:e0004672. doi: 10.1371/journal.pntd.0004672
29. Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref. Rev Saude Publica. (2000) 34:178–83. doi: 10.1590/S0034-89102000000200012
30. Hofelmann DA, Gonzalez-Chica DA, Peres KG, Boing AF, Peres MA. Chronic diseases and socioeconomic inequalities in quality of life among Brazilian adults: findings from a population-based study in Southern Brazil. Eur J Public Health. (2018) 28:603–10. doi: 10.1093/eurpub/ckx224
31. Fumis RRL, Ferraz AB, de Castro I, Barros de Oliveira HS, Moock M, Junior JMV. Mental health and quality of life outcomes in family members of patients with chronic critical illness admitted to the intensive care units of two Brazilian hospitals serving the extremes of the socioeconomic spectrum. PLoS ONE. (2019) 14:e0221218. doi: 10.1371/journal.pone.0221218
32. Gayoso MV, Domingues FS, Franca Junior MC, Felgoise SH, Oliveira ASB, de Barros GAM. Cross-cultural adaptation and validation for the Brazilian population of the instrument Amyotrophic Lateral Sclerosis-Specific Quality of Life-Short Form (ALSSQOL-SF). Qual Life Res. (2020) 29:805–13. doi: 10.1007/s11136-019-02342-2
33. Quintino ND, Sabino EC, da Silva JLP, Ribeiro ALP, Ferreira AM, Davi GL, et al. Factors associated with quality of life in patients with Chagas disease: SaMi-Trop project. PLoS Negl Trop Dis. (2020) 14:e0008144. doi: 10.1371/journal.pntd.0008144
34. Barbosa FS, Pereira Da Costa DP. Incapacitating effects of schistosomiasis mansoni on the productivity of sugar-cane cutters in northeastern Brazil. Am J Epidemiol. (1981) 114:102–11. doi: 10.1093/oxfordjournals.aje.a113156
35. Pereira da Costa DP, Simoes Barbosa F. Effect of schistosomiasis on the productivity of sugar cane cutters during the sugar harvest at the Catende Mill, Pernambuco. Mem Inst Oswaldo Cruz. (1982) 77:425–9. doi: 10.1590/S0074-02761982000400009
36. Cruz LN, Polanczyk CA, Camey SA, Hoffmann JF, Fleck MP. Quality of life in Brazil: normative values for the WHOQOL-bref in a southern general population sample. Qual Life Res. (2011) 20:1123–9. doi: 10.1007/s11136-011-9845-3
Keywords: hepatosplenic schistosomiasis, schistosomal myeloradiculopathy, schistosomiasis mansoni, quality of life, WHOQOL-BREF
Citation: Roriz SJ, Pereira TA, Vaz de Melo Trindade G, Caporali JFM and Lambertucci JR (2021) Quality of Life Assessment Among Patients Living With Hepatosplenic Schistosomiasis and Schistosomal Myeloradiculopathy. Front. Med. 8:629484. doi: 10.3389/fmed.2021.629484
Received: 14 November 2020; Accepted: 10 May 2021;
Published: 01 June 2021.
Edited by:
Ana Afonso, University of São Paulo, BrazilReviewed by:
Angèle Viola, UMR7339 Centre de Résonance Magnétique Biologique et Médicale (CRMBM), FranceRoberto De Cleva, University of São Paulo, Brazil
Edford Sinkala, University of Zambia, Zambia
Samar Nagah El-Beshbishi, Mansoura University, Egypt
Copyright © 2021 Roriz, Pereira, Vaz de Melo Trindade, Caporali and Lambertucci. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Thiago Almeida Pereira, dGhpYWdvYXBAc3RhbmZvcmQuZWR1