 Francesca Salamanna
Francesca Salamanna Francesca Veronesi
Francesca Veronesi Lucia Martini1
Lucia Martini1 Milena Fini
Milena Fini- 1IRCCS Istituto Ortopedico Rizzoli, Complex Structure of Surgical Sciences and Technologies, Bologna, Italy
- 2IRCCS Istituto Ortopedico Rizzoli, Scientific Direction, Bologna, Italy
Whilst the entire world is battling the second wave of COVID-19, a substantial proportion of patients who have suffered from the condition in the past months are reporting symptoms that last for months after recovery, i. e., long-term COVID-19 symptoms. We aimed to assess the current evidence on the long-term symptoms in COVID-19 patients. We did a systematic review on PubMed, Web of Science, EMBASE, and Google Scholar from database inception to February 15, 2021, for studies on long-term COVID-19 symptoms. We included all type of papers that reported at least one long-term COVID-19 symptom. We screened studies using a standardized data collection form and pooled data from published studies. Cohort cross-sectional, case-report, cases-series, case-control studies, and review were graded using specific quality assessment tools. Of 11,361 publications found following our initial search we assessed 218 full-text articles, of which 145 met all selection criteria. We found that 20.70% of reports on long-term COVID-19 symptoms were on abnormal lung functions, 24.13% on neurologic complaints and olfactory dysfunctions, and 55.17% on specific widespread symptoms, mainly chronic fatigue, and pain. Despite the relatively high heterogeneity of the reviewed studies, our findings highlighted that a noteworthy proportion of patients who have suffered from SARS-CoV-2 infection present a “post-COVID syndrome.” The multifaceted understanding of all aspects of the COVID-19 pandemic, including these long-term symptoms, will allow us to respond to all the global health challenges, thus paving the way to a stronger public health.
Introduction
As of March 2021, about 117 million people worldwide have been diagnosed with COVID-19, with more than 2.6 million deaths (1). COVID-19 is caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a heterogeneous virus that manifests itself with a wide spectrum of symptoms, from asymptomatic to life-threatening and fatal disease (2–7). Interstitial pneumonia is one of the most common features of SARS-CoV-2 and can be complicated by acute respiratory distress syndrome (ARDS), a disease related with high mortality, particularly in elderly people with multiple comorbidities (2, 3). As the pandemic of COVID-19 continues, numerous additional symptoms, such as fever, dry cough, shortness of breath, fatigue, myalgias, nausea/vomiting or diarrhea, headache, weakness, rhinorrhea, anosmia/ageusia, and many laboratory abnormalities, i.e., lymphopenia and elevated inflammatory markers (e.g., erythrocyte sedimentation rate, C-reactive protein, ferritin, tumor necrosis factor-α, IL-1, and IL-6) have been reported (2, 3). Other critical and severe complications of COVID-19 can include impaired function of the heart, brain, lung, liver, kidney, and coagulation system (4–7).
Most of the infected patients completely recovered after COVID-19 infection. However, a substantial proportion of patients who have been infected with SARS-CoV-2 continue to have symptoms long past the time that they recovered from the initial phases of COVID-19 disease. Clinicians worldwide called these long-term effects of COVID-19 “Long-Haul COVID-19” or “Long-term COVID-19” (8–11). In detail, “long-term COVID-19” defines those individuals who have had SARS-CoV-2 infection but do not recover completely over a period of a few weeks (commonly 2–3 weeks) (8–11). Based on the COVID-19 Symptom Study, a study carried-out on more than 4 million people in the US, UK, and Sweden, in which people enter their ongoing symptoms on a smartphone app, around 10% of patients who have tested positive for SARS-CoV-2 virus remain unwell beyond 3 weeks, and a smaller proportion for months (8). Thus, it is becoming clear, that some people who had a SARS-CoV-2 infection, even those described as “mild,” continue to suffer from persisting or cyclical symptoms. However, because COVID-19 is a novel disease, to date, there is not yet consensus on the definition of post-COVID-19 symptoms. Since long-term symptoms and complications have been described for other highly homologous human coronaviruses, i.e., Middle East Respiratory Syndrome (MERS) and Severe Acute Respiratory Syndrome (SARS), to date, it is unknown whether lessons from MERS and SARS are applicable to COVID-19 and the critical question is: “Do persistent symptoms at the post-viral stage of the disease constitute a post-COVID-19 syndrome (long-term COVID-19) and what are the main persistent symptoms in patients that might cause such a syndrome?” (12–14). The obvious answer is in research, but to date we do not know what to tell patients when they are asking about the course and prognosis of their ongoing complaints and potential long-term symptoms. Finding a concrete answer to these questions would also provide more information on the COVID-19 disease and enable comprehensive and targeted care to be given to survivors through the development of preventive and effective treatments. Although we are aware that it is too early to completely answer these questions, we believe that some general predictions are now possible, and would help to implement the right public health measures in particular after the pandemic has subsided. Thus, to give a complete overview on the persistent symptoms at the post-viral stage of COVID-19, we carried out a systematic review of the current data considering all types of papers evaluating individual persistent symptoms in mild, moderate, and severe/critical COVID-19 patients. Realizing the long-term sequelae of COVID-19 is imperative for understanding the complete history of disease, truly predicting the growing effect of the disease beyond hospitalization and mortality and defining whether inpatient or post-discharge-specific rehabilitation should be evaluated.
Methods
Eligibility Criteria
The PICO model was used to formulate the questions for this study: (1) studies that considered patients with long-term COVID-19 symptoms (Population), (2) studies where the primary aim was to evaluate long-term COVID-19 symptoms in mild, moderate, severe, and critical patients that have a follow-up of at least 14 days (Interventions), (3) studies with or without a control group (Comparisons), (4) studies that reported the long-term COVID-19 symptoms (Outcomes). Studies conducted up to February 15, 2021 were included in this review if they met the PICO criteria.
Search Strategies
Our systematic review involved a search conducted on February 15, 2021. We performed the review according to PRISMA statement (15). The search was carried out on PubMed, Web of Science, EMBASE, and Google Scholar databases to identify all type of papers on the long-term symptoms of COVID-19. The search was conducted combining the terms COVID-19, persistent symptoms, long-term symptoms, chronic symptoms, enduring symptoms, permanent symptoms. The combination of free-vocabulary and/or MeSH terms for the identification of studies in PubMed, Web of Science, EMBASE, and Google Scholar were reported in Table 1. Reference lists of relevant articles were searched for other potentially appropriate publications.

Table 1. Cohort (perspective and retrospective), cross-sectional, case-report, cases-series and case-control studies on long-term lungs symptoms, long-term neurological and olfactory symptoms, and widespread long-term symptoms.
Inclusion and Exclusion Criteria
Papers of any design evaluating individual persistent symptoms in mild, moderate, severe, and critical COVID-19 patients that have a follow-up of at least 14 days were included in this review.
Exclusion criteria included: unpublished reports, unspecified date/location of the study or suspicion of duplicate reporting, coronavirus strains other than COVID-19, unreported long-term COVID-19 symptoms, and studies that only hypothesize post-COVID-19 sequelae.
Study Selection and Data Extraction
Possible relevant articles were screened using the title and abstract by one reviewer (FS) and articles that did not meet the inclusion criteria were excluded. After screening the title and abstract, articles were submitted to a public reference manager (Mendeley v.1.17.9) to eliminate duplicates. Subsequently, the remaining full-text articles were examined by two reviewers (FS and FV). Any disagreement was resolved through discussion until a consensus was reached, or with the involvement of a third reviewer (MF).
The following items were extracted from each cohort study, cross-sectional, case-report, cases-series, case-control studies, if available: author, study type, study country, and period, patient characteristics (numbers, gender, age), COVID-19 severity (mild, moderate, severe, and critical), hospitalization, ICU admission, baseline COVID-19 symptoms, method of evaluating long-term COVID-19 symptoms, follow-up, and long-term COVID-19 symptoms.
Risk of Bias Assessment
Two reviewers (FS and FV) independently assessed the methodological quality of cohort, cross-sectional, case-reports, case-control, case-series studies, and reviews. Disagreements regarding the methodological quality of the studies were discussed between the two reviewers. If consensus was not reached, a third reviewer (MF) arbitrated. Cohort and Cross-Sectional Studies were assessed by Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies from the National Heart, Lung, and Blood Institute (NIH) (16). Case-control studies were assessed by the quality assessment criteria of The Quality Assessment Tool for Case-Control Studies from NIH (16). The methodological quality of case-series and case-reports were assessed by the quality assessment tool proposed by Murad et al. (17). Finally, reviews were assessed by the Quality Assessment Tool for Systematic Reviews and Meta-Analyses from NIH (16). No bias evaluation was performed for letters, commentary, editorial, news articles, survey, practice, communications, and medical hypothesis.
Results
Study Selection and Characteristics
The initial literature search retrieved 11,361 studies. Of those, 3,132 studies were identified using PubMed, 2,776 using Web of Science, 2,073 using EMBASE and 3,380 using Google Scholar. After screening the title and abstract 315 articles were run through Mendeley to eliminate duplicate articles. The resulting 218 full-text articles were then reviewed to establish whether the publication met the inclusion criteria and 139 were considered eligible. From the reference lists of the selected articles 6 additional publications were found. Of the 145 articles eligible for this review 47 were cohort studies (22 retrospective and 25 prospective), 11 cross-sectional, 2 case-control, 3 case-series, 14 case-reports, 10 review, 16 letters to Editor (of which 6 reported a cohort study, 1 reported a cross-sectional study, 1 reported a case-report, and 3 reported surveys), 3 commentary, 2 reply to commentary, 1 correspondence, 6 editorial, 18 survey (social media, interview, phone application), 1 opinion, 1 brief communication that reported a retrospective cohort study, 1 clinical update and 1 view point, 1 practice, 6 news articles, and 1 medical hypothesis. Search strategy and study inclusion and exclusion criteria are detailed in Figure 1.
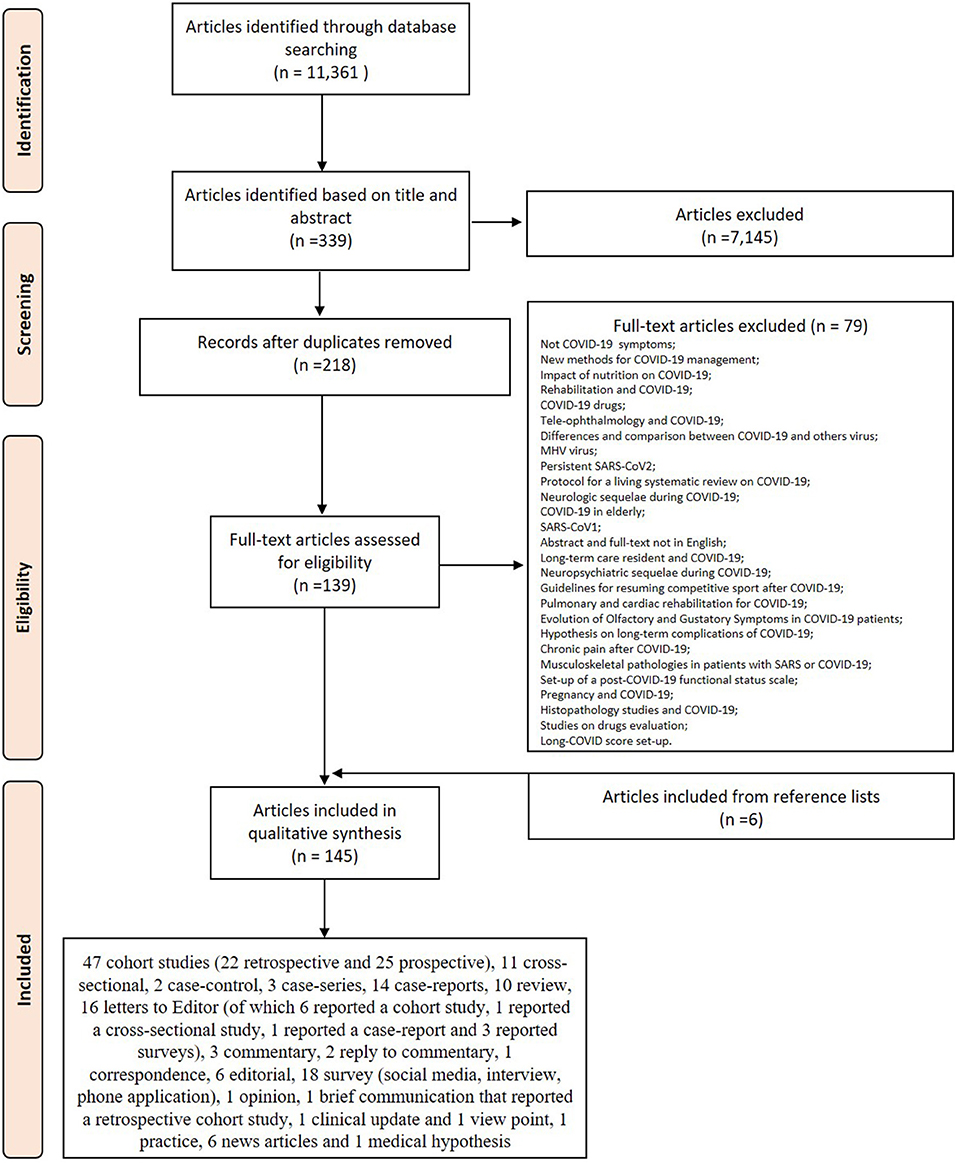
Figure 1. PRISMA flowchart for the study selection.
Risk of Bias Assessment
Of the 145 articles eligible for the review, we found 54 cohort studies (28 prospective, 26 retrospective), six of which were published as letters and one as brief communication, and 12 cross-sectional studies, one of which was published as letters. Using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (16), we rated three prospective studies, one ambidirectional cohort study and two cross-sectional studies at a “good” quality rating and 60 studies at a “fair” quality rating (Supplementary Material 1). For the 60 cohort and cross-sectional studies at a “fair” quality rating, the principal missing quality assessment criteria were sample size justification, blinded assessors to the exposure of participants, and missing data on key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s). Concerning the two case-control studies found, one was at a “good” quality rating and it did not specify only if outcome assessors did not know whether participants were exposed/unexposed, while the other was at a “fair” quality rating (Supplementary Material 1). For the case-control at “fair” quality rating, data on sample size justification, random selection of cases and controls, measures of exposure/risk across all study participants and on blinded assessors of exposure/risk were not reported. The methodological quality of the three case-series and of the 15 case-reports, one of which was published as letters, assessed by the tool proposed by Murad et al. (17), showed that 17/18 studies were at a “good” quality rating (Supplementary Material 1). For the two case-reports rated at a “fair” quality rating, the missing quality assessments criteria were the not adequately ascertained outcome, the lack of alternative causes that may explain the observation, and the absence of sufficient and specific details to describe the case. The quality assessment of reviews showed that 1/10 reviews was at a “good” quality rating while all the others were at a “poor” quality rating (Supplementary Material 1). The “poor” quality rating was because none of them include a comprehensive search of potentially relevant articles and did not use explicit criteria in the selection of articles. The research designs and study characteristics were not appraised, data were not synthesized, and results were not interpreted using a predefined systematic approach.
Long-Term Symptoms of COVID-19
Of the 145 eligible papers, 30 were on persistent lung symptoms (20.70%), 35 were on persistent neurological and olfactory dysfunctions (24.13%), and 80 were on widespread persistent symptoms (55.17%) (Table 1). Table 1 was split-up based on long-term lung symptoms, long-term neurological and olfactory symptoms, and widespread long-term symptoms.
Persistent Lung Symptoms and Dysfunctions
While SARS-CoV-2 was detected in many organ systems, the lungs seem to be the main organs affected by the virus (105–107). Abnormal lung functions and structural changes were reported up to 6 months after hospitalization in mild-to-critical COVID-19 patients (25, 27, 28, 32, 34, 36, 39, 41), also with diffuse alveolar damage, desquamation of alveolar epithelial type II cells, fibrine exudation, hyaline membranes, scattered interstitial inflammation, monocytes, and macrophages (23, 24, 34). Several authors reported that these persistent lung symptoms and dysfunctions correlated with prior COVID-19 severity (19, 20, 24, 25, 27, 36, 38, 41). In this context, Han et al. in a prospective study evaluating 114 severe COVID-19 patients showed lung fibrotic-like changes in 35% patients up to 6 months after infection (24). Differently, Latronico et al. showed that since residual abnormal chest-X ray findings were detected in about 70% of critically ill COVID-19 patients at 3 months, very few of them (~12%) had persisting respiratory symptoms at 6 months (27). An anecdotal
study by Zhu et al. also reported long-term abnormal airway function for up to 11 months in a severe COVID-19 patient (44). However, because is a single case, this research does not provide conclusive evidence. A small cohort of critically ill COVID-19 patients also showed alteration in the diffusing capacity of the lung for carbon monoxide (DLCO) for up to 3 months (20, 27, 38, 40). Persistent DLCO impairment was also detected in non-critical COVID-19 patients that also presented shortness of breath and dyspnea up to 4 months after infection (18, 22, 33, 43). Unlike the above cited studies which analyzed exclusively critically ill patients and two case-reports that analyzed solely mild COVID-19 patients (30, 42) all other studies analyzed heterogeneous cohorts of patients, i.e., from mild to severe. Lower lung functions were detected in 246 mild-to-severe SARS-CoV-2 convalescents patients with few comorbidities up to 2 months after infection (37). Widespread lung damages in mild-to-severe COVID-19 patients were further confirmed by numerous papers and by an Editorial where it was underlined that “months after infection with SARS-CoV-2, some people are still battling lung damage” (108–110), with more than one-third of them that having pulmonary tissue death and visible scars up to 6 months after symptoms onset (18, 21, 26, 35, 109, 110). In a news feature article it was reported that these lung damages lessened with time, 88% of patients had visible damage up to 6 weeks after infection, but 2 months after symptom onset this number had fallen to 56% (109). By examining retrospectively a cohort of 158 mild-to-severe COVID-19 patients, it was shown that these persistent pulmonary damages were also associated with a persistent elevation of IL-6 up to 2 months after infection (29). At the same follow-up, Chun et al., evaluating 61 prevalently non-critical COVID-19 patients, highlighted also higher levels of Lipocalin 2, suggesting that COVID-19 patients may have an ongoing neutrophil activation that could be amenable to targeted therapy (19). Sonnweber et al., evaluating a cohort of 109 patients with mild-to-critical COVID-19, showed that severe lung pathologies were also significantly associated with persisting hyperferritinemia that was present in ~38% of patients (35). Other authors evaluated the lung abnormalities by CT scans at different stages of SARS-CoV-2 infection (21, 26). Ding et al., analyzing retrospectively a cohort of 112 COVID-19 patients at different stages of the disease, showed that the frequency of crazy-paving pattern, consolidation, and linear opacities peaked at 10–14 days (62.7%), 15–21 days (75.0%), and at 22–28 days (83.1%) and decreased thereafter (21). However, at more than 28 days of follow-up 98.1% of CT scans still showed abnormalities. Similarly, Hu et al., evaluating 46 patients with mild-to-severe COVID-19 who had an isolated pulmonary lesion on the first positive CT, highlighted the presence of reticular patterns from the 14 days after symptoms onset in 45% of patients. At 22–31 days, the lesions were completely absorbed only in 28.57% (26). Mo et al. also noted pulmonary anomalies in a cohort of 110 discharged COVID-19 cases, 24 mild cases, 67 cases of pneumonia and 19 cases of severe pneumonia (31). The duration from onset of disease to pulmonary function test was 20 ± 6 days in mild cases, 29 ± 8 days in pneumonia cases and 34 ± 7 days in cases with severe pneumonia (110). Anomalies were noted in DLCO (47.2%), total lung capacity (25.0%), forced expiratory volume in 1 s (FEV1) (13.6%), forced vital capacity (FVC) (9.1%), FEV1/FVC (4.5%), and small airway function (7.3%) (31).
Persistent Neurological Symptoms and Olfactory Dysfunctions
Despite SARS-CoV-2 primarily affecting lungs, numerous data supported the neuro-invading potential of SARS-CoV-2 and, according to the first-hand evidence by Mao et al., ~36.4% of COVID-19 patients presented neurological symptoms (5, 111). Additionally, conditions such as hypoxia, encephalitis, and stroke, all present in severe COVID-19 patients, can produce both long-term neurological symptoms and permanent neurocognitive impairment (52, 58, 112, 113). In fact, a case-series by Negrini et al. associated the long-term neurological symptoms and general cognitive decay to the length of stay in the ICU (58). Despite the long-term neurological symptoms and the general cognitive decay being associated to severe/critical COVID-19 patients, in this review we did not find any studies based solely on critically/severely ill patients. On the other hand, we found a retrospective study and several case reports on mild COVID-19 patients (51, 53, 54, 65). Gallus et al., evaluating retrospectively 48 mild COVID-19 patients, underlined that 8.3% patients reported hearing loss, 4.2% tinnitus, 8.3% dizziness, 2% spinning vertigo, 2% dynamic imbalance, and 6.3% static imbalance at about 1 month of follow-up (51). Several anecdotal reports in mild COVID-19 patients also detected persistent deficits in memory and psychotic symptoms during up to 5 months of follow-up (53, 54, 65). In addition to these studies, all the others found in this review analyzed heterogenic populations of patients with COVID-19, from mild to severe. In this context, a recent editorial and a systematic review provided a detailed overview into the spectrum of mental disorders that can occur during the intermediate and long-term phases of COVID-19 in mild-to-critical patients (114, 115). The most frequent neurological long-term symptoms in these patients were myalgia, arthralgia, sleeping troubles, and headache (46, 50, 61, 116). Additionally, a general cognitive decay, i.e., deficit in attention and calculation, short-term memory, constructional apraxia, and written language, was also observed during up to 6 months of follow-up (61). At 2 months of follow-up 58.7% of 179 mild-to-severe COVID-19 patients presented a moderate neurocognitive decline while 39.1% of patients also showed psychiatric morbidity (56). At a longer follow-up of 6 months, Pilotto et al., analyzing retrospectively 165 moderate-to-severe COVID-19 patients, showed that these long-term symptoms persisted in about 37% of patients (61). Also, symptoms consistent with orthostatic hypoperfusion syndrome and painful small fiber neuropathy were reported at short (3 weeks) and long (up to 3 months) follow-ups in two case-reports and in a small case-series (48, 59, 63). In a “Long-Haul COVID” communication, Nath et al., summarizing symptoms reported after mild-to-severe COVID-19, also highlighted persistent symptoms that overlapped with those patients with myalgic encephalomyelitis/chronic fatigue syndrome (117). In addition to the long-term neurological symptoms Lu et al. prospectively examined the presence of brain micro-structural changes in 60 mild-to-critical COVID-19 patients reporting presence of alterations in 50% of recovered patients after 3 months (55). Anecdotal evidence also showed the presence of long-term impairment of the brain structures in two COVID-19 patients highlighting hypometabolism of the olfactory/rectus gyrus in both patients (52).
Since SARS-CoV-2 can affect neuronal cells by both direct and indirect mechanisms, this can lead to various neurological manifestations also including anosmia and hypogeusia. Anosmia and hypogeusia are present both in mild/moderate cases and in severe cases of COVID-19 (45, 47, 49, 57, 60, 62, 64, 66–68, 118–122). As long-term COVID-19 symptoms, anosmia, and hypogeusia were evaluated in severe COVID-19 patients only in one protective study (67). The study evaluated 138 COVID-19 patients at 2 months of follow-up showing that 5.8% of patients had moderate to severe olfactory dysfunction, while 4.3% had a significant taste disorder (67). A greater number of studies evaluated olfactory and gustatory disfunctions in mild COVID-19 patients (45, 47, 49, 64, 66, 68, 118). Using a retrospective questionnaire Fjaeldstad evaluated olfactory and gustatory loss in 109 mild COVID-19 patients (49). At ~1 month after symptoms onset since the chemosensory loss, participants reported relatively low recovery and improvement rates. For participants with olfactory loss, only 44% were fully recovered, whereas 28% had not yet experienced any improvement of symptoms (49). After gustatory loss, 50% had fully recovered, whereas 20% had not yet experienced any improvement. At a longer follow-up of 2 months after symptoms onset, Otte et al. evaluating through a questionnaire 91 mild COVID-19 patients for olfactory function, showed that 45.1% of patients were hyposmic while 53.8% showed an olfactory performance within the normal range (118). In the same way, at 2 months of follow-up, Boscolo-Rizzo et al. evaluated prospectively 183 mildly symptomatic COVID-19 patients showing that 18.6% presented altered sense of smell or taste (45). Interestingly, Ugurlu et al. in a cohort of mild COVID-19 patients showed persistent olfactory dysfunction in 14.3% of patients up to 3 months after symptoms onset (66). At the same follow-up, a long-term anosmia was also reported in a case-report of a 40-year-old woman with a mild COVID-19 diagnosis (64). Differently, other studies analyzing mild and asymptomatic COVID-19 patients for smell and taste disturbance reported resolution of anosmia up to 1 month after diagnosis (47, 60). Comparable results were also reported at the same follow-up by Konstantinidis et al. evaluating mild/moderate COVID-19 patients (119). Finally, Paolo et al., analyzing 75 mild-to moderate COVID-19 patients through a questionnaire reported olfactory and dysgeusia recovery within an average of 17 days, also finding a significantly decrease in viral load (120).
Finally, other studies evaluating heterogenous populations of mild-to-severe COVID-19 patients further confirmed persistent loss of smell up to 6 months after symptom onset (57, 61, 62, 64, 121, 122). Moein et al. in a prospective study on 82 mild-to-severe COVID-19 patients showed smell loss in ~37% of patients at 2 months of follow-up (57). At the same follow-up, a prospective study on 138 patients and a retrospective study on 90 mild-to-severe patients showed persistent hyposmia in 5–8% of patients (57, 67). Lastly, Pilotto et al., by examining retrospectively 165 patients detected the presence of hyposmia in ~15% of patients at up to 6 months of follow-up (61).
Widespread Persistent Symptoms
Numerous research groups reported widespread persisting symptoms in COVID-19 patients for up to 6 months after SARS-CoV-2 infection (70, 75, 123–142). They also described practice on the management of post-acute COVID-19 and performed comprehensive analyses of health-related quality of life (70, 75, 123). Furthermore, numerous editorials, reviews, news articles, clinical updates, narrative interviews, and focus groups have been published to explore what it is like to live with long-term COVID-19, also trying to emphasize the putative pathophysiology, risk factors, and treatments (124–142). Two cohort studies on severe/critical COVID-19 patients reported persistent physiological impairment and decrease in quality of life in more than half of the patients at up to 6 months of follow up (77, 100). Taboada et al. showed that at 6 months of follow-up only 16% of patients were completely free of persistent symptoms (100). However, in a Multistate Health Care Systems Network, Tenforde et al. reported that among 270 interviews conducted on COVID-19 patients, also among persons with milder outpatient illness, 14–21 days after symptoms onset, the 35% of patients had not returned to their usual state of health (143). In this context, Pellaud et al., examining the outcomes of 196 consecutively mild-moderate COVID-19 patients, 1 month after onset of symptoms, showed that among the 60% of patients that returned home, 63% reported persistent symptoms (90). Two months after symptom onset, evaluating 150 mild/moderate COVID-19 patients, Carvalho-Schneider et al. showed that about 66% of patients presented at least one symptom (74). Similarly, evaluating the long-term COVID-19 symptoms in 233 mild COVID-19 patients Cirulli et al. highlighted that ~24% of patients had at least one symptom also after 3 months (76). These results were also confirmed by an online survey of doctors conducted by the British Medical Association (144). They reported that of 3,729 doctors who answered a question about patients' persistent symptoms after COVID-19, a third said that they had seen or treated patients with long-term COVID-19 symptoms (144). Davido et al. also reported that since mid-May they evaluated an average of 30 individuals per week for whom COVID-19 symptoms have not completely subsided, essentially young women (sex ratio 4:1) around 40 years old with no relevant medical history (145–147). Additionally, it was reported that female sex (mean age 47.22) is also a risk factor for poor health-related quality of life in Chinese COVID-19 patients (75). Also, Sudre et al. analyzing 4,182 incident cases of non-severe COVID-19 who logged their symptoms prospectively in the COVID-19 Symptom Study App showed that women aged 50–60 were at greatest risk of developing “long-COVID” (148). Patients described symptoms in every part of the body which were sometimes severe or fluctuating (149, 150). Paul Garner, a professor at Liverpool School of Tropical Medicine and Co-ordinating Editor of the Cochrane Infectious Diseases Group, wrote on the 95th day after symptoms onset in the British Medical Journal Opinion (151). He said “I am unable to be out of bed for more than three hours at a stretch…I have ringing in the ears, intermittent brain fog, palpitations, and dramatic mood swings” (151). Other people also described similar complaints in the same journal (152–154). The science journalist Linda Geddes also discussed data from the Irish Centre for Vascular Biology in Dublin that reported COVID-19 patients being discharged from hospital, only to return several weeks later not only with widespread symptoms but also with deep vein thrombosis or blood clots on the lungs (155).
The main widespread reported long-term symptoms in COVID-19 patients were chronic fatigue, dyspnea, shortness of breath, chest pains, headache, loss of smell/taste, muscle, and joint pain, followed by depression, anxiety, insomnia, and itchy body, heart palpitations, tachycardia, anorexia, tingling fingertips, and brain fog (69, 70, 72, 77, 84, 85, 87, 91, 97, 98, 101, 103, 123, 138, 145–147, 150, 156–159). However, it was reported that the number of widespread long-term symptoms were higher for COVID-19 patients who were initially more ill (77, 100). D'Cruz et al. and Taboada et al., analyzing prospectively two cohorts of 119 and 91 severe/critical COVID-19 patients, respectively, showed the presence of dyspnoea on exertion (57%), asthaenia (37%), myalgia (37%), and arthralgia (29%) up to 2 months after symptoms onset and a general decrease in quality of life (mobility, usual activities, self-care, pain/discomfort, anxiety/depression) in 67% of patients at up to 6 months of follow-up (77, 100). However, these widespread long-term symptoms were not only present in severe COVID-19 patients, but also in patients who had mild and moderate disease (72, 76, 80, 94, 98, 146, 159). Carvalho-Schneider et al., in a prospective study on 150 mild/moderate COVID-19 patients at 2 months of follow-up, highlighted dyspnea and asthenia, respectively, in 30 and 40% of patients (74, 98). Similar results were also obtained in a cross-sectional study on 451 mild COVID-19 patients (98). In addition to these symptoms in a prospective study by Cirulli et al. symptoms such as difficulty concentrating, fatigue, memory loss, confusion, headache, heart palpitations, chest pain, pain with deep breaths, dizziness, and tachycardia were detected at 3 months of follow up (76). Fatigue, dyspnea, and heart dysfunctions in mild COVID-19 patients were also reported in several case-reports (69, 72, 80) at up to 8 months of follow-up. In addition, a case-report on three women also reported telogen effluvium, temporary hair shedding, as a long-term COVID-19 symptom 3 months after getting the infection (94). Several studies analyzing all together mild-to-severe COVID-19 patients also confirmed these long-term widespread symptoms (73, 78–81, 83, 88, 89, 92, 93, 95, 99, 102–104, 160–162). In a large cohort of 355 mild-to-severe COVID-19 patients Mahmud et al. detected that about 46% of patients developed long-term symptoms at 1 month of follow-up and that post-COVID features were significantly higher among the female gender with fatigue as the main long-term symptom (88). Similarly, persistent fatigue was also reported in about 12% of patients by examining a cohort of 1,002 mild-to-severe COVID-19 patients (95). At a longer follow-up, Rosales-Castillo et al. and Townsend et al. confirmed persistence of fatigue as the main long-term symptom in a cohort of mild-to-severe COVID-19 patients (93, 102). Banda et al., analyzing 150 tweets from moderate-to-severe COVID-19 patients, reported that the 10 most commonly long-term symptoms after COVID-19 were chronic fatigue (62%), dyspnea (19%), tachycardia/palpitations (13%), chest pain (13%), sleep disorders (10%), cough (9%), headache (7%), and joint pain, fever, and unspecified pain by 6% each (160). This analysis also matches clinician-collected data reported by an Italian study (73). The study followed 143 hospitalized mild-to-severe patients who were discharged from the hospital after COVID-19 and that had two negative test results for SARS-CoV-2 (73). At an average of 2 months after initial onset of symptoms, “only 12.6% were completely free of any COVID-19-related symptom, while 32% had 1 or 2 symptoms and 55% had 3 or more” (73). Also, in this case the most common symptoms were chronic fatigue (53.1%), dyspnea (43.4%), joint pain (27.3%), and chest pain (21.7%) (73). Authors also observed that individuals who had an initial symptom of dyspnea were more likely to develop long-term symptoms (73). These results were also confirmed by a case-control study that examined 141 mild-to-moderate COVID-19 patients and 78 controls at 2 months of follow-up (79). At the same follow-up a retrospective study on 206 mild-to-moderate COVID-19 patients also detected chronic pain in ~40% of the patients (78). A particular cross-sectional study on 46 mild-to-severe COVID-19 patients also described an extremely low outlier ratio of total protein, albumin, and globulin at 2 months of follow-up, underlying a persistent abnormal liver function (104). At the same follow-up lymphopenia, elevated D-dimer, and C reactive protein were also detected and associated to persistent fatigue, dyspnea, and anosmia (87, 103). Fatigue and dyspnea were also the two most prevalent persistent symptoms 3 months after a SARS-CoV-2 infection in hospitalized and non-hospitalized patients (83, 92, 103, 161). Furthermore, at the same follow-up, Raman et al. also reported abnormalities in heart (26%), liver (10%), and kidneys (29%) (92). Dyspnea (42%), associated with chronic fatigue (55%), loss of memory (34%), concentration and sleep disorders (28 and 30.8%, respectively), was likewise reported in 120 COVID-19 patients (relatively non-severe) analyzed by questionnaire, 100 days after initial symptoms onset (162). In was also shown that these long-term symptoms persisted for up to 6 months, with fatigue or muscle weakness and sleep difficulties as the most common symptoms (81, 99). At 6 months, by examining 9,989 mild-to-severe COVID-19 patients, persistent neuropsychiatric, pulmonary, metabolic, and coagulopathic phenotypes were also reported (89).
Recent data reported several of these widespread long-term symptoms, i.e., fatigue, dyspnea, chest pains, muscle and joint pain, headache, insomnia, and palpitations, also in children and adolescent up to 6–8 months of follow-up (71, 86, 96). At 6 months of follow-up high blood pressure levels and persistence of a prehypertension were also detected in ~13% of mild COVID-19 children (82). Examining a larger cohort of children, it was also described that ~53–70% of these patients had at least one symptom 100 days or more after COVID-19 diagnosis (71, 82, 96, 163). Given these emerging data, recently, Hertting et al. in an editorial on Acta Paediatrica underlined the need to have more research and studies on the long-term effects of COVID-19 in children and adolescents (164).
Discussion
Although we are aware that there are no long-term data on large numbers of COVID-19 patients with persistent symptoms and with comparison groups, and that an analysis in a field as engaging as COVID-19 can never be updated, this review allowed us to outline that a noteworthy number of patients present long-lasting sequelae, up to 6 months, in the post-COVID time. These long-term symptoms are not only present in severe COVID-19, but also in mild and moderate patients. In addition, recent preliminary data also underlined the presence of long-term COVID-19 symptoms on children and adolescents. Some clinical studies and survey questionnaires also highlighted a potential high-risk factor for long-term COVID-19 in the female gender; women's risk of developing long-term COVID-19 seems to be double that of men among patients aged between 40 and 50. After the age of 60 the risk level of long-term COVID between male and female should become similar. This pattern appears to be like that of autoimmune diseases that are more common in female through menopause to become similar between male and female after age 60 (165). Thus, it is possible that these gender differences, as well as other aspects of the disease, may be due to a different immune system response during and after COVID-19. However, currently, it is not yet clear whether this data reflects the population of people with long-term COVID-19 and which is the full spectrum of the duration and severity of long-term symptoms in these patients.
What emerges from this review is that the most common reported symptoms after COVID-19 are abnormal lung functions prevalently with persistent dyspnea, general neurological decay, smell and taste disturbances, and chronic fatigue. Other common symptoms include joint pain and chest pain. These symptoms may linger or recur for weeks or months following initial recovery. In detail, for patients with mild-to-moderate COVID-19 the more common long-term symptoms are chronic fatigue, anosmia/ageusia, dyspnea, but also difficulty in concentration, memory loss, and confusion. These symptoms seem to be present in a higher percentage of patients who were initially more ill. In critical-to-severe COVID-19 patients' supplementary long-term symptoms are lung fibrotic-like changes up to 6 months after infection and a high reduction in diffusing capacity of the lung for DLCO that frequently required oxygen uses also after hospital discharge. Likewise, the general cognitive decay, despite also being present in mild-to-moderate COVID-19 patients, also appears to be more closely related to critical-to-severe forms of COVID-19. Considering the whole overview of widespread long-term symptoms reported in this review the one undeniably most prevalent in mild-to-critical COVID-19 patients is chronic fatigue. This is in line with past research that highlighted high levels of post-infectious fatigue for survivors of epidemics such as SARS and Ebolavirus (166, 167). Moreover, fatigue has been related with infections, such as mononucleosis, that occur outside of an epidemic or pandemic scale (167). Currently, it is not clear why chronic fatigue and the other long-term complications persist in some COVID-19 patients. However, most researchers and clinicians agree that the long-term COVID-19 symptoms are associated with the coronavirus' ability to trigger a massive inflammatory response. Thus, it will be mandatory to analyze cytokine networks in patients who recover from COVID-19 to evaluate whether the “cytokine storm” present during the disease persists and contributes to these long-term complications.
The main strength of this study is that it highlights multiple long-term symptoms which may hinder return to pre-COVID-19 infection functional status. However, despite this finding a weakness of our review was that while some studies included in this review focused on a single population of infected COVID-19 patients, i.e., mild/moderate and severe/critical, numerous studies included heterogeneous populations, from mild to critical, not taking into account disease severity as well as preexisting co-morbidities, treatment regimens, mean ages, gender, and other aspects. This bias can lead to alterations in the data evaluation and analysis, which potentially affect the results. Data from prospective designs, developed by evaluating homogeneous populations of COVID-19 patients able to consider their characteristics prior to and during infection, might provide new and detailed information into predisposing factors that lead to long-term COVID-19 symptoms. Another bias that should be considered is that despite the fact that in some studies the long-term COVID-19 sequelae were evaluated through clinical visits and/or specific instrumental analyzes, many others have used self-administered questionnaires and scores, telephone/online interview, and phone applications. This is because, to date, assessing the patient in the hospital is difficult due to the entry restrictions into the COVID-19 departments. On the other hand, checking and evaluating them at home presents almost insurmountable logistical problems during an emergency health situation like the one we are facing. However, this type of self-assessment highlights bias in the detection of symptoms as patients may have psychological and emotional involvement due to the disease itself.
At this stage, a detailed analysis and understanding of all the aspects associated with long-term COVID-19 are mandatory to mitigate against the potential persistent symptoms identified in the current review. Future studies should assess: (1) the full range of disorders associated with COVID-19 and their long-term manifestations; (2) the underlying associations between viral spread, associated pro-inflammatory changes, and long-term disease pathogenesis; (3) the duration and extent of long-term symptoms in relation to the resolution of the disease; (4) the association between disease severity and long-term dysfunctions; (5) the effect of specific antiviral therapies and/or interventions on long-term symptoms; (6) why symptoms persist or recur; and (7) the potential late effects of COVID-19 on children/adolescents. Another important point that should be assessed is SARS-CoV-2 levels (detection, load) in patients and how this relates to long-term symptoms. To date, it is not clear whether the initial viral load, per se, may meaningfully impact long-term symptoms, particularly in mild-to-moderate COVID-19 patients. Information relating to SARS-CoV-2 detection and viral load at different time points of infection will help the clinical interpretation of long-term symptoms of COVID-19. Similarly, there is a need for further studies to provide robust data on the association between viral shedding and long-term COVID-19. Despite has reports that the median duration of viral shedding goes from 12-to-20 days, there is evidence that ongoing viral shedding in SARS-CoV-2 may be prolonged in the feces compared to respiratory secretions (168–170). The persistent fragments of viral genes, though not infectious, may still be triggering a violent immune overreaction that could explain the symptoms persistence in COVID-19-free patients. Alternatively, even if the virus is cleared, the immune system could continue to be overactive or perturbed, analogous to the long-term debilitation after glandular fever (165). A greater understanding of these last points could improve the knowledge not only of the causes of long-term symptoms but also on the immune system involvement and on transmission risk.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author Contributions
FS and MF designed the review. FS and FV performed the literature search and collected and assembled the data. FS, FV, and MF analyzed the obtained articles. FS, FV, ML, and MF wrote the paper. MF, LM, and ML revised the manuscript critically. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by IRCCS Istituto Ortopedico Rizzoli (Ricerca Corrente).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.653516/full#supplementary-material
References
1. COVID-19 Dashboard by the Center for Systems Science Engineering (CSSE) at Johns Hopkins University (JHU). Available online at: https://coronavirus.jhu.edu/map.html (accessed December 17, 2020).
2. Mao R, Qiu Y, He JS, Tan JY, Li XH, Liang J, et al. Manifestations and prognosis of gastrointestinal and liver involvement in patients with COVID-19: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. (2020) 5:667–78. doi: 10.1016/S2468-1253(20)30126-6
3. Levi M, Thachil J, Iba T, Levy JH. Coagulation abnormalities and thrombosis in patients with COVID-19. Lancet Haematol. (2020) 7:438–40. doi: 10.1016/S2352-3026(20)30145-9
4. Long B, Brady WJ, Koyfman A, Gottlieb M. Cardiovascular complications in COVID-19. Am J Emerg Med. (2020) 38:1504–7. doi: 10.1016/j.ajem.2020.04.048
5. Mao L, Jin H, Wang M, Hu Y, Chen S, He Q, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. (2020) 77:1–9. doi: 10.1001/jamaneurol.2020.1127
6. Middeldorp S, Coppens M, van Haaps TF, Foppen M, Vlaar AP, Müller MCA, et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost. (2020) 18:1995–2002. doi: 10.1111/jth.14888
7. Chen YT, Shao SC, Hsu CK, Wu IW, Hung MJ, Chen YC. Incidence of acute kidney injury in COVID-19 infection: a systematic review and meta-analysis. Crit Care. (2020) 24:346. doi: 10.1186/s13054-020-03009-y
8. COVID Symptom Study. How Long Does COVID-19 Last? Available online at: https://covid19.joinzoe.com/post/covid-long-term?fbclid=IwAR1RxIcmmdL-EFjh_aI- (accessed December 17, 2020).
9. Correia AO, Feitosa PWG, Moreira JLS, Nogueira SÁR, Fonseca RB, Nobre MEP. Neurological manifestations of COVID-19 and other coronaviruses: a systematic review. Neurol Psychiatry Brain Res. (2020) 37:27–32. doi: 10.1016/j.npbr.2020.05.008
10. NICE. Covid-19 Rapid Guideline: Managing the Long-Term Effects of Covid-19. Available online at: https://www.nice.org.uk/guidance/ng188/chapter/4-Planning-care (accessed February 15, 2021).
11. Hui DS, Joynt GM, Wong KT, Gomersall CD, Li TS, Antonio G, et al. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. (2005) 60:401–9. doi: 10.1136/thx.2004.030205
12. Hui DS, Wong KT, Ko FW, Tam LS, Chan DP, Woo J, et al. The 1-year impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and quality of life in a cohort of survivors. Chest. (2005) 128:2247–61. doi: 10.1378/chest.128.4.2247
13. Ngai JC, Ko FW, Ng SS, To KW, Tong M, Hui DS. The long-term impact of severe acute respiratory syndrome on pulmonary function, exercise capacity and health status. Respirology. (2010) 15:543–50. doi: 10.1111/j.1440-1843.2010.01720.x
14. Park WB, Jun KI, Kim G, Choi JP, Rhee JY, Cheon S, et al. Correlation between pneumonia severity and pulmonary complications in Middle East respiratory syndrome. J Korean Med Sci. (2018) 33:169. doi: 10.3346/jkms.2018.33.e169
15. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009). 6:1000097. doi: 10.1371/journal.pmed.1000097
16. Study Quality Assessment Tools. Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed December 17, 2020).
17. Murad MH, Sultan S, Haffar S, Bazerbachi F. Methodological quality and synthesis of case series and case reports. BMJ Evid Based Med. (2018) 23:60–3. doi: 10.1136/bmjebm-2017-110853
18. Bellan M, Soddu D, Balbo PE, Baricich A, Zeppegno P, Avanzi GC, et al. Respiratory and psychophysical sequelae among patients with COVID-19 four months after hospital discharge. JAMA Netw Open. (2021) 4:e2036142. doi: 10.1001/jamanetworkopen.2020.36142
19. Chun HJ, Coutavas E, Pine A, Lee AI, Yu V, Shallow M, et al. Immuno-fibrotic drivers of impaired lung function in post-COVID-19 syndrome. medRxiv [Preprint]. (2021). doi: 10.1101/2021.01.31.21250870
20. Daher A, Balfanz P, Cornelissen C, Müller A, Bergs I, Marx N, et al. Follow up of patients with severe coronavirus disease 2019 (COVID-19): pulmonary and extrapulmonary disease sequelae. Respir Med. (2020). 174:106197. doi: 10.1016/j.rmed.2020.106197
21. Ding X, Xu J, Zhou J, Long Q. Chest CT findings of COVID-19 pneumonia by duration of symptoms. Eur J Radiol. (2020) 127:109009. doi: 10.1016/j.ejrad.2020.109009
22. Frija-Masson J, Debray MP, Gilbert M, Lescure FX, Travert F, Borie R, et al. Functional characteristics of patients with SARS-CoV-2 pneumonia at 30 days post-infection. Eur Respir J. (2020) 56:2001754. doi: 10.1183/13993003.01754-2020
23. Hall J, Myall K, Lam JL, Mason T, Mukherjee B, West A, et al. Identifying patients at risk of post-discharge complications related to COVID-19 infection. Thorax. (2021). doi: 10.1136/thoraxjnl-2020-215861. [Epub ahead of print].
24. Han X, Fan Y, Alwalid O, Li N, Jia X, Yuan M, et al. Six-month follow-up chest CT findings after severe COVID-19 pneumonia. Radiology. (2021) 299:203153. doi: 10.1148/radiol.2021203153
25. Heiss R, Grodzki DM, Horger W, Uder M, Nagel AM, Bickelhaupt S. High-performance low field MRI enables visualization of persistent pulmonary damage after COVID-19. Magn Reson Imaging. (2020) 76:49–51. doi: 10.1016/j.mri.2020.11.004
26. Hu Q, Guan H, Sun Z, Huang L, Chen C, Ai T, et al. Early CT features and temporal lung changes in COVID-19 pneumonia in Wuhan, China. Eur J Radiol. (2020) 128:109017. doi: 10.1016/j.ejrad.2020.109017
27. Latronico N, Peli E, Rodella F, Novelli MP, Rasulo FA, Piva S, et al. Six-Month Outcome in Survivors of COVID-19 Associated Acute Respiratory Distress Syndrome. SSRN. Available online at: https://ssrn.com/abstract=3756865 (accessed March, 2021).
28. Liang L, Yang B, Jiang N, Fu W, He X, Zhou Y, et al. Three-month follow-up study of survivors of coronavirus disease 2019 after discharge. J Korean Med Sci. (2019) 35:e418. doi: 10.3346/jkms.2020.35.e418
29. Liao B, Liu Z, Tang L, Li L, Gan Q, Shi H, et al. Longitudinal clinical and radiographic evaluation reveals interleukin-6 as an indicator of persistent pulmonary injury in COVID-19. Int J Med Sci. (2021) 18:29–41. doi: 10.7150/ijms.49728
30. Manckoundia P, Franon E. Is persistent thick copious mucus a long-term symptom of COVID-19? Eur J Case Rep Intern Med. (2020) 7:002145. doi: 10.12890/2020_002145
31. Mo X, Jian W, Su Z, Chen M, Peng H, Peng P, et al. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J. (2020) 55:2001217. doi: 10.1183/13993003.01217-2020
32. Moreno-Pérez O, Merino E, Leon-Ramirez JM, Andres M, Ramos JM, Arenas-Jiménez J, et al. Post-acute COVID-19 syndrome. Incidence and risk factors: a Mediterranean cohort study. J Infect. (2021) 82:378–83. doi: 10.1016/j.jinf.2021.01.004
33. Ramakrishnan A, Zreloff J, Moore MA, Bergquist SH, Cellai M, Higdon J, et al. Prolonged symptoms after COVID-19 infection in outpatients. Open Forum Infect Dis. (2021) 8:ofab060. doi: 10.1093/ofid/ofab060
34. Shah AS, Wong AW, Hague CJ, Murphy DT, Johnston JC, Ryerson CJ, et al. A prospective study of 12-week respiratory outcomes in COVID-19-related hospitalisations. Thorax. (2020) 3. doi: 10.1136/thoraxjnl-2020-216308
35. Sonnweber T, Boehm A, Sahanic S, Pizzini A, Aichner M, Sonnweber B, et al. Persisting alterations of iron homeostasis in COVID-19 are associated with non-resolving lung pathologies and poor patients' performance: a prospective observational cohort study. Respir Res. (2020) 21:276. doi: 10.1186/s12931-020-01546-2
36. Tabatabaei SMH, Rajebi H, Moghaddas F, Ghasemiadl M, Talari H. Chest CT in COVID-19 pneumonia: what are the findings in mid-term follow-up? Emerg Radiol. (2020) 27:711–719. doi: 10.1007/s10140-020-01869-z
37. Trinkmann F, Müller M, Reif A, Kahn N, Kreuter M, Trudzinski F, et al. Residual symptoms and lower lung function in patients recovering from SARS-CoV-2 infection. Eur Respir J. (2021). 57:2003002. doi: 10.1183/13993003.03002-2020
38. Truffaut L, Demey L, Bruyneel AV, Roman A, Alard S, De Vos N, et al. Post-discharge critical COVID-19 lung function related to severity of radiologic lung involvement at admission. Respir Res. (2021) 22:29. doi: 10.1186/s12931-021-01625-y
39. van den Borst B, Peters JB, Brink M, Schoon Y, Bleeker-Rovers CP, Schers H, et al. Comprehensive health assessment three months after recovery from acute COVID-19. Clin Infect Dis. (2020) 21:ciaa1750. doi: 10.1093/cid/ciaa1750
40. van Gassel RJJ, Bels JLM, Raafs A, van Bussel BCT, van de Poll MCG, Simons SO, et al. High prevalence of pulmonary sequelae at 3 months after hospital discharge in mechanically ventilated survivors of COVID-19. Am J Respir Crit Care Med. (2021) 203:371–4. doi: 10.1164/rccm.202010-3823LE
41. Weerahandi H, Hochman KA, Simon E, Blaum C, Chodosh J, Duan E, et al. Post-discharge health status and symptoms in patients with severe COVID-19. J Gen Intern Med. (2021) 36:738–45. doi: 10.1007/s11606-020-06338-4
42. Yao XH, He ZC, Li TY, Zhang HR, Wang Y, Mou H, et al. Pathological evidence for residual SARS-CoV-2 in pulmonary tissues of a ready-for-discharge patient. Cell Res. (2020) 30:541–3. doi: 10.1038/s41422-020-0318-5
43. Zhao YM, Shang YM, Song WB, Li QQ, Xie H, Xu QF, et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine. (2020) 25:100463. doi: 10.1016/j.eclinm.2020.100463
44. Zhu M, Chen D, Zhu Y, Xiong X, Ding Y, Guo F, et al. Long-term sero-positivity for IgG, sequelae of respiratory symptoms, and abundance of malformed sperms in a patient recovered from severe COVID-19. Eur J Clin Microbiol Infect Dis. (2021). doi: 10.1007/s10096-021-04178-6. [Epub ahead of print].
45. Boscolo-Rizzo P, Polesel J, Spinato G, Menegaldo A, Fabbris C, Calvanese L, et al. Predominance of an altered sense of smell or taste among long-lasting symptoms in patients with mildly symptomatic COVID-19. Rhinology. (2020) 58:524–5. doi: 10.4193/Rhin20.263
46. Caronna E, Ballvé A, Llauradó A, Gallardo VJ, Ariton DM, Lallana S, et al. Headache: a striking prodromal and persistent symptom, predictive of COVID-19 clinical evolution. Cephalalgia. (2020) 40:1410–21 doi: 10.1177/0333102420965157
47. D'Ascanio L, Pandolfini M, Cingolani C, Latini G, Gradoni P, Capalbo M, et al. Olfactory dysfunction in COVID-19 patients: prevalence and prognosis for recovering sense of smell. Otolaryngol Head Neck Surg. (2020) 164:82–6. doi: 10.1177/0194599820943530
48. Dani M, Dirksen A, Taraborrelli P, Torocastro M, Panagopoulos D, Sutton R, et al. Autonomic dysfunction in 'long COVID': rationale, physiology and management strategies. Clin Med. (2020) 21:e63–7. doi: 10.7861/clinmed.2020-0896
49. Fjaeldstad AW. Prolonged complaints of chemosensory loss after COVID-19. Dan Med J. (2020) 67:A05200340
50. Galal I, Hussein AAR, Amin MT, Saad MM, Zayan HEE, Abdelsayed MZ, et al. Determinants of persistent post COVID-19 symptoms: value of a novel COVID-19 symptoms score. Egypt J Bronchol. (2021) 15:10. doi: 10.1101/2020.11.11.20230052
51. Gallus R, Melis A, Rizzo D, Piras A, De Luca LM, Tramaloni P, et al. Audiovestibular symptoms and sequelae in COVID-19 patients. J Vestib Res. (2021). doi: 10.3233/VES-201505. [Epub ahead of print].
52. Guedj E, Million M, Dudouet P, Tissot-Dupont H, Bregeon F, Cammilleri S, et al. (18)F-FDG brain PET hypometabolism in post-SARS-CoV-2 infection: substrate for persistent/delayed disorders? Eur J Nucl Med Mol Imaging. (2020). 30:1–4. doi: 10.21203/rs.3.rs-40021/v1
53. Hellmuth J, Barnett TA, Asken BM, Kelly JD, Torres L, Stephens ML, et al. Persistent COVID-19-associated neurocognitive symptoms in non-hospitalized patients. J Neurovirol. (2021) 2:1–5. doi: 10.1007/s13365-021-00954-4
54. Lim ST, Janaway B, Costello H, Trip A, Price G. Persistent psychotic symptoms following COVID-19 infection. BJPsych Open. (2020) 6:105. doi: 10.1192/bjo.2020.76
55. Lu Y, Li X, Geng D, Wu PY, Huang CC, Jia T, et al. Cerebral micro-structural changes in COVID-19 patients - an MRI-based 3-month follow-up study. EClinicalMedicine. (2020) 25:100484. doi: 10.1016/j.eclinm.2020.100484
56. Méndez R, Balanzá-Martínez V, Luperdi SC, Estrada I, Latorre A, González-Jiménez P, et al. Short-term neuropsychiatric outcomes and quality of life in COVID-19 survivors. J Intern Med. (2021). doi: 10.1111/joim.13262. [Epub ahead of print].
57. Moein ST, Hashemian SM, Tabarsi P, Doty RL. Prevalence and reversibility of smell dysfunction measured psychophysically in a cohort of COVID-19 patients. Int Forum Allergy Rhinol. (2020) 10:1127–35. doi: 10.1002/alr.22680
58. Negrini F, Ferrario I, Mazziotti D, Berchicci M, Bonazzi M, de Sire A, et al. Neuropsychological features of severe hospitalized coronavirus disease 2019 Patients at clinical stability and clues for postacute rehabilitation. Arch Phys Med Rehabil. (2020) 102:155–8. doi: 10.1016/j.apmr.2020.09.376
59. Novak P. Post COVID-19 syndrome associated with orthostatic cerebral hypoperfusion syndrome, small fiber neuropathy and benefit of immunotherapy: a case report. eNeurologicalSci. (2020) 21:100276. doi: 10.1016/j.ensci.2020.100276
60. Panda S, Mohamed A, Sikka K, Kanodia A, Sakthivel P, Thakar A, et al. Otolaryngologic manifestation and long-term outcome in mild COVID-19: experience from a Tertiary Care Centre in India. Indian J Otolaryngol Head Neck Surg. (2020) 14:1–6. doi: 10.1007/s12070-020-02217-w
61. Pilotto A, Cristillo V, Cotti Piccinelli S, Zoppi N, Bonzi G, Sattin D, et al. COVID-19 severity impacts on long-term neurological manifestation after hospitalisation. medRxiv [Preprint]. (2020). doi: 10.1101/2020.12.27.20248903
62. Printza A, Katotomichelakis M, Metallidis S, Panagopoulos P, Sarafidou A, Petrakis V, et al. The clinical course of smell and taste loss in COVID-19 hospitalized patients. Hippokratia. (2020) 24:66–71.
63. Raahimi MM, Kane A, Moore CE, Alareed AW. Late onset of Guillain-Barré syndrome following SARS-CoV-2 infection: part of 'long COVID-19 syndrome'? BMJ Case Rep. (2021) 14:e240178. doi: 10.1136/bcr-2020-240178
64. Sampaio Rocha-Filho PA, Voss L. Persistent headache and persistent anosmia associated with COVID-19. Headache. (2020) 60:1797–9. doi: 10.1111/head.13941
65. Clouden TA. Persistent hallucinations in a 46-year-old woman after COVID-19 infection: a case report. Cureus. (2020) 12:e11993. doi: 10.7759/cureus.11993
66. Ugurlu BN, Akdogan O, Yilmaz YA, Yapar D, Aktar Ugurlu G, Yerlikaya HS, et al. Quantitative evaluation and progress of olfactory dysfunction in COVID-19. Eur Arch Otorhinolaryngol. (2021). doi: 10.1007/s00405-020-06516-4. [Epub ahead of print].
67. Vaira LA, Hopkins C, Petrocelli M, Lechien JR, Chiesa-Estomba CM, Salzano G, et al. Smell and taste recovery in coronavirus disease 2019 patients: a 60-day objective and prospective study. J Laryngol Otol. (2020) 134:703–9. doi: 10.1017/S0022215120001826
68. Yan CH, Prajapati DP, Ritter ML, DeConde AS. Persistent smell loss following undetectable SARS-CoV-2. Otolaryngol Head Neck Surg. (2020) 163:923–5. doi: 10.1177/0194599820934769
69. Abdallah H, Porterfield F, Fajgenbaum D. Symptomatic relapse and long-term sequelae of COVID-19 in a previously healthy 30-year-old man. BMJ Case Rep. (2020) 13:e239825. doi: 10.1136/bcr-2020-239825
70. Arnold DT, Hamilton FW, Milne A. Patient outcomes after hospitalisation with COVID-19 and implications for follow-up: results from a prospective UK cohort. Thorax. (2020). doi: 10.1101/2020.08.12.20173526. [Epub ahead of print].
71. Buonsenso D, Munblit D, De Rose C, Sinatti D, Ricchiuto A, Carfi A, et al. Preliminary evidence on long COVID in children. medRxiv [Preprint]. (2021). doi: 10.1101/2021.01.23.21250375
72. Buselli R, Corsi M, Necciari G, Pistolesi P, Baldanzi S, Chiumiento M, et al. Sudden and persistent dysphonia within the framework of COVID-19: The case report of a nurse. Brain Behav Immun Health. (2020) 9:100160. doi: 10.1016/j.bbih.2020.100160
73. Carfì A, Bernabei R, Landi F. Gemelli against COVID-19 post-acute care study group. JAMA. (2020) 324:603–5. doi: 10.1001/jama.2020.12603
74. Carvalho-Schneider C, Laurent E, Lemaignen A, Beaufils E, Bourbao-Tournois C, Laribi S, et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin Microbiol Infect. (2020) 27:258–63. doi: 10.1016/j.cmi.2020.09.052
75. Chen KY, Li T, Gong FH, Zhang JS, Li XK. Predictors of health-related quality of life and influencing factors for COVID-19 patients, a follow-up at one month. Front Psychiatry. (2020) 11:668. doi: 10.3389/fpsyt.2020.00668
76. Cirulli E, Schiabor Barrett KM, Riffle S, Bolze A, Neveux I, Dabe S, et al. Long-term COVID-19 symptoms in a large unselected population. medRxiv [Preprint]. (2020). doi: 10.1101/2020.10.07.20208702
77. D'Cruz RF, Waller MD, Perrin F, Periselneris J, Norton S, Smith LJ, et al. Chest radiography is a poor predictor of respiratory symptoms and functional impairment in survivors of severe COVID-19 pneumonia. ERJ Open Res. (2021) 7:00655–2020. doi: 10.1183/23120541.00655-2020
78. Erçalik T, Ayyildiz A, Gencer-Atalay K, Akgün C, Özdemir HM, Kuran B. Pain symptoms in COVID-19. Am J Phys Med Rehabil. (2021). doi: 10.1097/PHM.0000000000001699. [Epub ahead of print].
79. Galván-Tejada CE, Herrera-García CF, Godina-González S, Villagrana-Bañuelos KE, Amaro JDL, Herrera-García K, et al. Persistence of COVID-19 symptoms after recovery in Mexican population. Int J Environ Res Public Health. (2020) 17:9367. doi: 10.3390/ijerph17249367
80. Hosseini Z, Ghodsi S, Hejazi SF. Persistent complete heart block in a patient with COVID-19 infection: a case report. SN Compr Clin Med. (2021) 6:1–4. doi: 10.1007/s42399-020-00712-3
81. Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. (2021). 397:220–32. doi: 10.1016/S0140-6736(20)32656-8
82. Soldi S, Mallardo S, Marcellino A, Bloise S, Dilillo A, Iorfida D, et al. The comprehensive clinic, laboratory, and instrumental evaluation of children with COVID-19: a 6-months prospective study. J Med Virol. (2021) 93:3122–32. doi: 10.1002/jmv.26871
83. Iqbal A, Iqbal K, Arshad Ali S, Azim D, Farid E, Baig MD, Bin Arif T, Raza M. The COVID-19 sequelae: a cross-sectional evaluation of post-recovery symptoms and the need for rehabilitation of COVID-19 survivors. Cureus. (2021) 13:e13080. doi: 10.7759/cureus.13080
84. Jacobs LG, Gourna Paleoudis E, Lesky-Di Bari D, Nyirenda T, Friedman T, Gupta A, et al. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS ONE. (2020) 15:e0243882. doi: 10.1371/journal.pone.0243882
85. Khalaf M, Bazeed SE, Abdel-Gawad M, Abu-Elfatth A, Abdelhamed W, Zaghloul M, et al. Prevalence and Predictors of Persistent Symptoms after Clearance of SARS-CoV-2 Infection: A Report from Egypt. Available online at: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=3727954 (accessed December 3, 2020).
86. Ludvigsson JF. Case report and systematic review suggest that children may experience similar long-term effects to adults after clinical COVID-19. Acta Paediatr. (2020) 110:914–21. doi: 10.1111/apa.15673
87. Mandal S, Barnett J, Brill SE, Brown JS, Denneny EK, Hare SS, et al. ‘Long-COVID’: a cross-sectional study of persisting symptoms, biomarker and imaging abnormalities following hospitalisation for COVID-19. Thorax. (2020). doi: 10.1136/thoraxjnl-2020-215818. [Epub ahead of print].
88. Mahmud R, Rahman M, Rassel MA, Monayem FB, Sayeed SJB. Post COVID syndrome among symptomatic COVID-19 patients: a prospective study in a Tertiary Care Center in Bangladesh. SSRN. (2021). doi: 10.2139/ssrn.3759687. [Epub ahead of print].
89. Martin JT, Akama-Garren E, Puranik A, Liukasemsarn S, Venkatakrishnan AJ, O'Horo JC, et al. Augmented curation of clinical notes of COVID-19 and influenza patients reveals that long-term neuropsychiatric and coagulopathic symptoms are more associated with COVID-19. medRxiv [Preprint]. (2021). doi: 10.1101/2021.01.03.20248997
90. Pellaud C, Grandmaison G, Pham Huu Thien HP, Baumberger M, Carrel G, Ksouri H, et al. Characteristics, comorbidities, 30-day outcome and in-hospital mortality of patients hospitalised with COVID-19 in a Swiss area - a retrospective cohort study. Swiss Med Wkly. (2020) 150:w20314. doi: 10.4414/smw.2020.20314
91. Petersen MS, Kristiansen MF, Hanusson KD, Danielsen ME, Á Steig B, Gaini S, Strøm M, et al. Long COVID in the Faroe Islands - a longitudinal study among non-hospitalized patients. Clin Infect Dis. (2020). doi: 10.1093/cid/ciaa1792. [Epub ahead of print].
92. Raman B, Cassar MP, Tunnicliffe EM, Filippini N, Griffanti L, Alfaro-Almagro F, et al. Medium-term effects of SARS-CoV-2 infection on multiple vital organs, exercise capacity, cognition, quality of life and mental health, post-hospital discharge. EClinicalMedicine. (2021) 31:100683. doi: 10.1016/j.eclinm.2020.100683
93. Rosales-Castillo A, García de Los Ríos C, Mediavilla García JD. Persistent symptoms after acute COVID-19 infection: importance of follow-up. Med Clin. (2021) 156:35–36. doi: 10.1016/j.medcle.2020.08.003
94. Saeed W, Hussain I, Altaf F. Telogen effluvium: long term Covid-19 symptom. J Pakistan Assoc Dermatol. (2020) 30:700–3.
95. Islam MS, Ferdous MZ, Islam US, Mosaddek ASM, Potenza MN, Pardhan S. Treatment, persistent symptoms, and depression in people infected with COVID-19 in Bangladesh. Int J Environ Res Public Health. (2021) 18:1453. doi: 10.3390/ijerph18041453
96. Smane L, Stars I, Pucuka Z, Roge I, Pavare J. Persistent clinical features in paediatric patients after SARS-CoV-2 virological recovery: a retrospective population-based cohort study from a single centre in Latvia. BMJ Paediatr Open. (2020). 4:e000905. doi: 10.1136/bmjpo-2020-000905
97. Sofian M, Velayati AA, Banifazl M, Fotouhi F, Sadat Larijani M, Afzali N, et al. SARS-CoV-2, a virus with many faces: a series of cases with prolonged persistence of COVID-19 symptoms. Wien Med Wochenschr. (2020) 171:3–6. doi: 10.1007/s10354-020-00793-8
98. Stavem K, Ghanima W, Olsen MK, Gilboe HM, Einvik G. Persistent symptoms 1.5-6 months after COVID-19 in non-hospitalised subjects: a population-based cohort study. Thorax. (2020). doi: 10.1136/thoraxjnl-2020-216377. [Epub ahead of print].
99. Sykes DL, Holdsworth L, Jawad N, Gunasekera P, Morice AH, Crooks MG. Post-COVID-19 symptom burden: what is long-COVID and how should we manage it? Lung. (2021) 11:1–7. doi: 10.1007/s00408-021-00423-z
100. Taboada M, Moreno E, Cariñena A, Rey T, Pita-Romero R, Leal S, et al. Quality of life, functional status, and persistent symptoms after intensive care of COVID-19 patients. Br J Anaesth. (2021) 126:e110–3. doi: 10.1016/j.bja.2020.12.007
101. Townsend L, Dyer AH, Jones K, Dunne J, Mooney A, Gaffney F, et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE. (2020) 15:e0240784. doi: 10.1371/journal.pone.0240784
102. Townsend L, Dowds J, O'Brien K, Sheill G, Dyer AH, O'Kelly B, et al. Persistent poor health post-COVID-19 is not associated with respiratory complications or initial disease severity. Ann Am Thorac Soc. (2021). doi: 10.1513/AnnalsATS.202009-1175OC. [Epub ahead of print].
103. Varghese J, Sandmann S, Vollenberg R, Ochs K, Schrempf I, Froemmel C, et al. Follow Up of COVID-19 Features in Recovered Adults without Comorbidities- Persistent Symptoms and Lab-Abnormalities. Res Square [Preprint]. doi: 10.21203/rs.3.rs-116030/v1
104. An YW, Song S, Li WX, Chen YX, Hu XP, Zhao J, et al. Liver function recovery of COVID-19 patients after discharge, a follow-up study. Int J Med Sci. (2021) 18:176–86. doi: 10.7150/ijms.50691
105. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. (2020). 382:1708-1720. doi: 10.1056/NEJMoa2002032
106. Yang X, Yu Y, Xu J, Shu H, Xia J, Liu H, et al. Clinical course and outcomes of critically ill patients with SARS1456 CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. (2020) 8:475–81. doi: 10.1016/S2213-2600(20)30079-5
107. Xu Z, Shi L, Wang Y, Zhang J, Huang L, Zhang C, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. (2020) 8:420–2. doi: 10.1016/S2213-2600(20)30076-X
108. Fraser E. Long term respiratory complications of covid-19. BMJ. (2020) 370:m3001. doi: 10.1136/bmj.m3001
109. Marshall M. The lasting misery of coronavirus long-haulers. Nature. (2020) 585:339–341. doi: 10.1038/d41586-020-02598-6
110. Shaw B, Daskareh M, Gholamrezanezhad A. The lingering manifestations of COVID-19 during and after convalescence: update on long-term pulmonary consequences of coronavirus disease 2019 (COVID-19). Radiol Med. (2020) 1:1–7. doi: 10.1007/s11547-020-01295-8
111. Ahmad I, Rathore FA. Neurological manifestations and complications of COVID-19: A literature review. J Clin Neurosci. (2020) 77:8–12. doi: 10.1016/j.jocn.2020.05.017
112. Bougakov D, Podell K, Goldberg E. Multiple neuroinvasive pathways in COVID-19. Mol Neurobiol. (2020) 29:1–12. doi: 10.1007/s12035-020-02152-5
113. Candan SA, Elibol N, Abdullahi A. Consideration of prevention and management of long-term consequences of post-acute respiratory distress syndrome in patients with COVID-19. Physiother Theory Pract. (2020) 36:663–8. doi: 10.1080/09593985.2020.1766181
114. Wijeratne T, Gillard Crewther S, Sales C, Karimi L. COVID-19 pathophysiology predicts that ischemic stroke occurrence is an expectation, not an exception-a systematic review. Front Neurol. (2021) 11:607221. doi: 10.3389/fneur.2020.607221
115. Fischer PR, Renemane R. Mental disorders following COVID-19 infection: a systematic review of acute and long-term psychiatric manifestations and associated brain changes. Proc. Latvian Acad. Sci., Section B. (2020) 74:347–57. doi: 10.2478/prolas-2020-0053
116. Hundreds of ‘Long Haulers’ Present with Neurologic Complaints at Post-COVID-19 Clinics. Available online at: https://journals.lww.com/neurotodayonline/Fulltext/2020/11050/Hundreds_of__Long_Haulers__Present_with_Neurologic.3.aspx (accessed November 5, 2020).
118. Otte MS, Eckel HNC, Poluschkin L, Klussmann JP, Luers JC. Olfactory dysfunction in patients after recovering from COVID-19. Acta Otolaryngol. (2020) 140:1032–5. doi: 10.1080/00016489.2020.1811999
119. Konstantinidis I, Delides A, Tsakiropoulou E, Maragoudakis P, Sapounas S, Tsiodras S. Short-term follow-up of self-isolated COVID-19 patients with smell and taste dysfunction in Greece: two phenotypes of recovery. ORL J Otorhinolaryngol Relat Spec. (2020) 82:295–303. doi: 10.1159/000511436
120. Paolo G. Does COVID-19 cause permanent damage to olfactory and gustatory function? Med Hypotheses. (2020) 143:110086. doi: 10.1016/j.mehy.2020.110086
121. Hopkins C, Burges Watson DL, Kelly C, Leary V, Smith BC. Managing long covid: don't overlook olfactory dysfunction. BMJ. (2020) 370:m3736. doi: 10.1136/bmj.m3736
122. Hopkins C, Surda P, Vaira LA, Lechien JR, Safarian M, Saussez S, et al. Six month follow-up of self-reported loss of smell during the COVID-19 pandemic. Rhinology. (2021) 59:26–31. doi: 10.4193/Rhin20.544
123. Greenhalgh T, Knight M, A'Court C, Buxton M, Husain L. Management of post-acute covid-19 in primary care. BMJ. (2020) 370:m3026. doi: 10.1136/bmj.m3026
124. Kamal M, Abo Omirah M, Hussein A, Saeed H. Assessment and characterisation of post-COVID-19 manifestations. Int J Clin Pract. (2020). doi: 10.1111/ijcp.13746. [Epub ahead of print].
125. Amenta EM, Spallone A, Rodriguez-Barradas MC, El Sahly HM, Atmar RL, Kulkarni PA. Postacute COVID-19: an overview and approach to classification. Open Forum Infect Dis. (2020) 7:ofaa509. doi: 10.1093/ofid/ofaa509
126. Del Rio C, Collins LF, Malani P. Long-term health consequences of COVID-19. JAMA. (2020) 324:1723–24. doi: 10.1001/jama.2020.19719
127. Hayes JP. Considering the long-term respiratory effects of Covid-19. Occup Med. (2021) Jan 22:kqaa224. doi: 10.1093/occmed/kqaa224
128. Higgins V, Sohaei D, Diamandis EP, Prassas I. COVID-19: from an acute to chronic disease? Potential long-term health consequences. Crit Rev Clin Lab Sci. (2020). doi: 10.1080/10408363.2020.1860895. [Epub ahead of print].
129. Iacobucci G. Long covid: damage to multiple organs presents in young, low risk patients. BMJ. (2020) 371:m4470. doi: 10.1136/bmj.m4470
130. Ladds E, Rushforth A, Wieringa S, Taylor S, Rayner C, Husain L, et al. Developing services for long COVID: lessons from a study of wounded healers. Clin Med. (2021) 21:59–65. doi: 10.7861/clinmed.2020-0962
131. Leth S, Gunst JD, Mathiasen VD, Hansen KS, Søgaard OS, Østergaard L, Jensen-Fangel S, et al. Persistent symptoms in hospitalized patients recovering from COVID-19 in Denmark. Open Forum Infectious Diseases. (2021) ofab042. doi: 10.1093/ofid/ofab042
132. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. medRxiv [Preprint]. (2021). doi: 10.21203/rs.3.rs-266574/v1
134. Mendelson M, Nel J, Blumberg L, Madhi SA, Dryden M, Stevens W, et al. Long-COVID: an evolving problem with an extensive impact. S Afr Med J. (2020) 111:10–12. doi: 10.7196/SAMJ.2020.v111i11.15433
135. Nikhra V. Living with ‘Long COVID-19’: the long-term complications and sequelae. Int J Clin Virol. (2021) 5:011–7.
136. Norton A, Olliaro P, Sigfrid L, Carson G, Hastie C, Kaushic C, et al. Long COVID: tackling a multifaceted condition requires a multidisciplinary approach. Lancet Infect Dis. (2021). doi: 10.1016/S1473-3099(21)00043-8. [Epub ahead of print].
137. Outhoff K. Sick and tired of COVID-19: long haulers and post viral (fatigue) syndromes. SAGP. (2020) 1:132–4. doi: 10.36303/SAGP.2020.1.4.0041
138. Pearmain L, Avram C, Yioe V, Webb P, Margaritopoulos GA, Rivera-Ortega P, et al. P168 patient symptoms following discharge from hospital after COVID-19 pneumonia. Thorax. (2021). doi: 10.1136/thorax-2020-BTSabstracts.313. [Epub ahead of print].
139. Saigal A, Naidu SB, Shah AJ, Brill SE, Jarvis H, Goldring JG, et al. S54 ‘long-COVID’: the need for multi-disciplinary working. Thorax. (2021) 76(Suppl. 1) A33–4. doi: 10.1136/thorax-2020-BTSabstracts.59
140. Simani L, Ramezani M, Darazam IA, Sagharichi M, Aalipour MA, Ghorbani F, et al. Prevalence and correlates of chronic fatigue syndrome and post-traumatic stress disorder after the outbreak of the COVID-19. J Neurovirol. (2021) 27:154–9. doi: 10.1007/s13365-021-00949-1
141. Yong SJ. Long-haul COVID-19: putative pathophysiology, risk factors, and treatments. Preprints. (2020) 2020120242. doi: 10.20944/preprints202012.0242.v1
142. Zapatero DC, Hanquet G, Van Den Heede K. Epidemiology of Long Covid: A Pragmatic Review of the Literature. Available online at: https://kce.fgov.be/sites/default/files/atoms/files/2020-04HSR_LongCOVID_COVID%20Contributions_01022021.pdf (accessed March, 2021).
143. Tenforde MW, Kim SS, Lindsell CJ, Billig Rose E, Shapiro NI, Files DC, et al. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a Multistate Health Care Systems Network - United States, March-June 2020. MMWR Morb Mortal Wkly Rep. (2020). 69:993–8. doi: 10.15585/mmwr.mm6930e1
144. Rimmer A. Covid-19: Impact of long-term symptoms will be profound, warns BMA. BMJ. (2020) 370:m3218. doi: 10.1136/bmj.m3218
145. Davido B, Seang S, Tubiana R, de Truchis P. Post-COVID-19 chronic symptoms: a postinfectious entity? Clin Microbiol Infect. (2020) 26:1448–1449. doi: 10.1016/j.cmi.2020.07.028
146. Davido B, Seang S, Barizien N, Tubiana R, de Truchis P. 'Post-COVID-19 chronic symptoms' - Author's reply. Clin Microbiol Infect. (2020) 27:495–6. doi: 10.1016/j.cmi.2020.09.001
147. Miglis MG, Goodman BP, Chémali KR, Stiles L. Re: 'Post-COVID-19 chronic symptoms' by Davido et al. Clin Microbiol Infect. (2020). 27:494. doi: 10.1016/j.cmi.2020.08.028
148. Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, et al. Attributes and predictors of long-COVID: analysis of COVID cases and their symptoms collected by the Covid Symptoms Study App. medRxiv [Preprint]. (2020). doi: 10.1101/2020.10.19.20214494
149. Ladds E, Rushforth A, Wieringa S, Taylor S, Rayner C, Husain L, et al. Persistent symptoms after Covid-19: qualitative study of 114 “long Covid” patients and draft quality criteria for services. medRxiv [Preprint]. (2020). doi: 10.1101/2020.10.13.20211854
150. Yelin D, Wirtheim E, Vetter P, Kalil AC, Bruchfeld J, Runold M, et al. Long-term consequences of COVID-19: research needs. Lancet Infect Dis. (2020) 20:1115–7. doi: 10.1016/S1473-3099(20)30701-5
151. Garner P. Covid-19 at 14 Weeks—Phantom Speed Cameras, Unknown Limits, and Harsh Penalties. Available online at: https://blogs.bmj.com/bmj/2020/06/23/paul-garner-covid-19-at-14-weeks-phantom-speed-cameras-unknown-limits-and-harsh-penalties/ (accessed November 25, 2020).
152. Rayner C, Lokugamage AU, Molokhia M. COVID-19: Prolonged and Relapsing Course of Illness Has Implications for Returning Workers. Available online at: https://blogs.bmj.com/bmj/2020/06/23/covid-19-prolonged-and-relapsing-course-of-illness-has-implications-for-returning-workers/ (accessed November 25, 2020).
153. Alwan NA, Attree E, Blair JM, Bogaert D, Bowen MA, Boyle J, et al. From doctors as patients: a manifesto for tackling persisting symptoms of covid-19. BMJ. (2020) 370:m3565. doi: 10.1136/bmj.m3565
154. Kingstone T, Taylor AK, O'Donnell CA, Atherton H, Blane DN, Chew-Graham CA. Finding the 'right' GP: a qualitative study of the experiences of people with long-COVID. BJGP Open. (2020) 4:bjgpopen20X101143. doi: 10.3399/bjgpopen20X101143
155. Geddes L. The enduring grip of covid-19. New Sci. (2020) 246:34–8. doi: 10.1016/S0262-4079(20)31141-6
156. Williams FMK, Muirhead N, Pariante C. Covid-19 and chronic fatigue. BMJ. (2020) 370:m2922. doi: 10.1136/bmj.m2922
157. Nehme M, Braillard O, Alcoba G, Aebischer Perone S, Courvoisier D, Chappuis F, et al. COVID-19 symptoms: longitudinal evolution and persistence in outpatient settings. Ann Intern Med. (2020) 8:M20–5926. doi: 10.7326/M20-5926
158. Zuin M, Rigatelli G, Zuliani G, Roncon L. Fatigue as long-term consequence of ARDS in COVID-19 patients. Anaesth Crit Care Pain Med. (2020) 26:100787. doi: 10.1016/j.accpm.2020.10.016
159. Bliddal S, Banasik K, Pedersen OB, Nissen I, Cantwell L, Schwinn M, et al. Acute and persistent symptoms in non-hospitalized PCR-confirmed COVID-19 patients. medRxiv [Preprint]. (2021). doi: 10.1101/2021.01.22.21249945
160. Banda JM, Singh GV, Alser O, Prieto-Alhambra D. Long-term patient-reported symptoms of COVID-19: an analysis of social media data. medRxiv [Preprint]. (2020). doi: 10.1101/2020.07.29.20164418
161. Goërtz YMJ, Van Herck M, Delbressine JM, Vaes AW, Meys R, Machado FVC, et al. Persistent symptoms 3 months after a SARS-CoV-2 infection: the post-COVID-19 syndrome? ERJ Open Res. (2020) 6:00542-2020. doi: 10.1183/23120541.00542-2020
162. Garrigues E, Janvier P, Kherabi Y, Le Bot A, Hamon A, Gouze H, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. (2020) 81:e4–e6. doi: 10.1016/j.jinf.2020.08.029
163. Ludvigsson JF. Reporting suspicions of long COVID in children is justified during this global emergency. Acta Paediatr. (2021). doi: 10.1111/apa.15762
164. Hertting O. More research is needed on the long-term effects of COVID-19 on children and adolescents. Acta Paediatr. (2021) 110:744–5. doi: 10.1111/apa.15731
165. British Society for Immunology. Long-Term Immunological Health Consequences of COVID-19. Available online at: https://www.immunology.org/sites/default/files/BSI_Briefing_Note_August_2020_FINAL.pdf (accessed August 13, 2020).
166. Moldofsky H, Patcai J. Chronic widespread musculoskeletal pain, fatigue, depression and disordered sleep in chronic post-SARS syndrome; a case-controlled study. BMC Neurol. (2011) 11:37. doi: 10.1186/1471-2377-11-37
167. Wilson HW, Amo-Addae M, Kenu E, Ilesanmi OS, Ameme DK, Sackey SO. Post-ebola syndrome among Ebola virus disease survivors in Montserrado County, Liberia (2016). Biomed Res Int. (2018) 2018:1909410. doi: 10.1155/2018/1909410
168. Zheng S, Fan J, Yu F, Feng B, Lou B, Zou Q. Viral load dynamics and disease severity in patients infected with SARS-CoV-2 in Zhejiang province, China, January-March 2020: retrospective cohort study. BMJ. (2020) 369:m1443. doi: 10.1136/bmj.m1443
169. Widders A, Broom A, Broomc J. SARS-CoV-2: the viral shedding vs. infectivity dilemma. Infect Dis Health. (2020) 25:210–5. doi: 10.1016/j.idh.2020.05.002
Keywords: COVID-19, long-term symptoms, persistent symptoms, long-term sequalae, virus
Citation: Salamanna F, Veronesi F, Martini L, Landini MP and Fini M (2021) Post-COVID-19 Syndrome: The Persistent Symptoms at the Post-viral Stage of the Disease. A Systematic Review of the Current Data. Front. Med. 8:653516. doi: 10.3389/fmed.2021.653516
Received: 15 January 2021; Accepted: 10 March 2021;
Published: 04 May 2021.
Edited by:
Susan Christina Welburn, University of Edinburgh, United KingdomReviewed by:
Daniel Bereczki, Semmelweis University, HungaryRaimund Helbok, Innsbruck Medical University, Austria
Mark Graham, King's College London, United Kingdom
Copyright © 2021 Salamanna, Veronesi, Martini, Landini and Fini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesca Veronesi, ZnJhbmNlc2NhLnZlcm9uZXNpQGlvci5pdA==