 Tiago Dias Domingues1,2
Tiago Dias Domingues1,2 Anna D. Grabowska3
Anna D. Grabowska3 Ji-Sook Lee4
Ji-Sook Lee4 Jose Ameijeiras-Alonso5
Jose Ameijeiras-Alonso5 Francisco Westermeier6,7
Francisco Westermeier6,7 Carmen Scheibenbogen8
Carmen Scheibenbogen8 Jacqueline M. Cliff4
Jacqueline M. Cliff4 Luis Nacul9,10
Luis Nacul9,10 Eliana M. Lacerda9
Eliana M. Lacerda9 Helena Mouriño1,11
Helena Mouriño1,11 Nuno Sepúlveda2,4,8*
Nuno Sepúlveda2,4,8*- 1Departamento de Estatística e Investigação Operacional, Faculdade de Ciências, Universidade de Lisboa, Lisboa, Portugal
- 2CEAUL–Centro de Estatística e Aplicações da Universidade de Lisboa, Lisboa, Portugal
- 3Department of Biophysics, Physiology, and Pathophysiology, Medical University of Warsaw, Warsaw, Poland
- 4Department of Infection Biology, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom
- 5Department of Statistics, Mathematical Analysis and Optimization, Universidade de Santiago de Compostela, Santiago de Compostela, Spain
- 6Institute of Biomedical Science, Department of Health Studies, FH Joanneum University of Applied Sciences, Graz, Austria
- 7Centro Integrativo de Biología y Química Aplicada (CIBQA), Universidad Bernardo O'Higgins, Santiago, Chile
- 8Institute of Medical Immunology, Charité–Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt Universität zu Berlin and Berlin Institute of Health, Berlin, Germany
- 9Department of Clinical Research, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom
- 10Complex Chronic Diseases Program, British Columbia Women's Hospital and Health Centre, Vancouver, BC, Canada
- 11CMAFcIO–Center of Mathematics, Fundamental Applications and Operations Research, Faculdade de Ciências, Universidade de Lisboa, Lisboa, Portugal
The evidence of an association between Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and chronic herpesviruses infections remains inconclusive. Two reasons for the lack of consistent evidence are the large heterogeneity of the patients' population with different disease triggers and the use of arbitrary cutoffs for defining seropositivity. In this work we re-analyzed previously published serological data related to 7 herpesvirus antigens. Patients with ME/CFS were subdivided into four subgroups related to the disease triggers: S0-42 patients who did not know their disease trigger; S1-43 patients who reported a non-infection trigger; S2-93 patients who reported an infection trigger, but that infection was not confirmed by a lab test; and S3-48 patients who reported an infection trigger and that infection was confirmed by a lab test. In accordance with a sensitivity analysis, the data were compared to those from 99 healthy controls allowing the seropositivity cutoffs to vary within a wide range of possible values. We found a negative association between S1 and seropositivity to Epstein-Barr virus (VCA and EBNA1 antigens) and Varicella-Zoster virus using specific seropositivity cutoff. However, this association was not significant when controlling for multiple testing. We also found that S3 had a lower seroprevalence to the human cytomegalovirus when compared to healthy controls for all cutoffs used for seropositivity and after adjusting for multiple testing using the Benjamini-Hochberg procedure. However, this association did not reach statistical significance when using Benjamini-Yekutieli procedure. In summary, herpesviruses serology could distinguish subgroups of ME/CFS patients according to their disease trigger, but this finding could be eventually affected by the problem of multiple testing.
Introduction
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a complex disease with unknown cause whose patients experience persistent fatigue that cannot be alleviated by rest and suffer from post-exertional malaise upon minimal physical and/or mental activity (1). Disease prevalence has been estimated around 0.4% after pooling data from different epidemiological studies (2). However, this estimate might be conservative (3, 4) due to poor societal recognition of the disease including amongst health professionals (5), the inexistence of an objective disease-specific biomarker for the corresponding diagnosis (6), a small number of well-designed epidemiological studies (7), and limited funding opportunities for more comprehensive and integrative research (8).
The etiology of ME/CFS and its pathogenesis remains a topic under intense debate with the proposal of many competing hypotheses (9–16). However, there is a general consensus that the disease could be initiated by a combination of genetic predisposing factors (17–20) and environmental triggers (e.g., exposure to toxins, chronic emotional and physical stress) (10, 21). In this regard, a large proportion of patients report an acute infection at the onset of their symptoms (22, 23). Herpesviruses such as the Epstein-Barr virus (EBV) and the human herpesvirus-6 (HHV6) were considered to be the main candidates for the causative agents of ME/CFS due to their high prevalence in adults and their reactivation observed in patients (11, 24, 25). To understand the role of these viruses on ME/CFS, many serological investigations were conducted with inconclusive or even contradicting findings (24). Possible reasons for this contrasting evidence could be related to disease misclassification and selection bias (26, 27), the necessity of dividing patients into different subtypes (28), the low number of patients recruited (6), or differences in the antigen and experimental assays used (29). An additional but often ignored reason is that serological studies are typically based on arbitrary cutoff values for identifying seropositive individuals or high antibody responders, as illustrated in two serological studies on herpesviruses (30, 31).
Recently, the analysis of serological data from the United Kingdom ME/CFS Biobank (UKMEB) did not find any association between ME/CFS and the presence of antibodies against chronic infections by different herpesviruses (32). In this work, we re-analyzed these data by dividing the ME/CFS patients into four subgroups related to non-infection vs. infection disease triggers. We also performed a sensitivity analysis of the association between ME/CFS and each herpesvirus as a function of the cutoff defining seropositivity.
Materials and Methods
Study Participants
All study participants are part of the UKMEB as described before (33). In summary, the data refer to a cohort of 226 patients with ME/CFS and 99 healthy controls (HC); note that the sample size of the healthy controls is in line with the ones used for this group by current serological studies on the role of herpesviruses on ME/CFS, as summarized elsewhere (24). At biobank enrollment, patients had to fill in a symptom's assessment questionnaire in which they were asked a specific question about whether they had an infection at the disease onset. This question had four categories of response, which we used to divide the patients into the following subgroups: subgroup S0– she/he did not know whether she/he had an infection at the disease onset (n = 42, 18.5%); subgroup S1– she/he did not have an infection at the disease onset (n = 43, 18.9%); subgroup S2– she/he had an infection at the disease onset, but this infection was not confirmed with a lab test (n = 93, 41.0%); subgroup S3– she/he had an infection at the disease onset and this infection was confirmed with a lab test (n = 48, 21.1%). In the participant questionnaire, patients were also asked to narrate the factors that could have triggered or contributed to the disease. Given that this was an open question, we only performed a brief description of the respective responses.
All individuals had age between 18 and 60 years old. Patients with ME/CFS were referred for a possible inclusion in the UKMEB by general practitioners working in the National Health System (NHS) of the United Kingdom. The respective diagnosis was confirmed using the 1994 Centers for Disease Control and Prevention (CDC) (34) or the 2003 Canadian Consensus Criteria (35) by the UKMEB dedicated clinical research team, according to their designed clinical protocol (36). Participants were excluded if they were taking any anti-viral drug or any medication that could alter their immune function in the three preceding months. Healthy controls were either family members or friends of the recruited patients with ME/CFS, or they were volunteers recruited by advertisement within Higher Education Institutions. Detailed information about exclusion and inclusion criteria of the UKMEB and additional information about recruitment and sample processing can be found elsewhere (36, 37).
Herpesviruses Serology
Serological data and the respective laboratory procedures were previously described in the original study (32). However, given that the main focus of this early study was cellular immunology, the description of herpesviruses serology was kept to a minimum. We have now provided some additional details.
The following commercial ELISA assays from Demeditec Diagnostics (Kiel, Germany) were used to quantify the plasma concentrations of IgG antibodies against the following viruses: the human cytomegalovirus (CMV; Prod. Ref. DECMV01), EBV-VCA antigen (Prod. Ref. DEEBVG0150), EBV-EBNA1 antigen (Prod. Ref. DE4246), herpes simplex virus-1 (HSV1; Prod. Ref. DEHSV1G0500), herpes simplex virus-2 (HSV2; Prod. Ref. DEHSV2G0540), Varicella-Zoster virus (VZV; Prof. Ref. DEVZVG0490). The commercial ELISA-VIDITEST from VIDIA (Vestec, Czech Republic) was used for the IgG quantification against HHV6 (Prod. Ref. ODZ-235).
Antibody quantification was expressed in arbitrary units per milliliter (U/ml). According to manufacturer's instructions, seropositivity was considered for all samples with concentration ≥ 12 U/ml for HSV1, HSV 2, VZV, CMV and EBV antigens. Likewise, individuals with antibody concentrations against HHV6 ≥ 12.5 U/ml were considered seropositive.
Statistical Analysis
To compare the age of the participants, the age of disease onset, and the disease duration of different study groups and/or subgroups of ME/CFS patients, we used the non-parametric Kruskal-Wallis test. To compare the gender distribution in the same subgroups, we applied the Pearson's χ2 test for testing independence in two-way contingency tables. For simplicity of the analysis, we only reported frequencies and the respective percentages of different disease triggers in the subgroups of ME/CFS that mentioned the occurrence of such triggers.
We previously performed thorough analyses of different cutoff values for seropositivity to each viral antigen (38, 39). These earlier analyses were based on the comparison and the selection of different scale mixtures of skew-normal distributions and four different criteria to define seropositivity. In accordance with a sensitivity analysis, instead of selecting a fixed cutoff, we here allowed this cutoff to vary between 10 U/ml and 100 U/ml with a lag of 1 U/ml. For each cutoff of a given antibody, we first estimated the unadjusted seropositivity odds ratio (OR) and the area under the Receiver Operating Characteristic curve (AUC) between each ME/CFS subgroup and the healthy controls using a logistic regression model in which seropositivity status of the individuals and a group indicator were the outcome and the covariate, respectively.
We then adjusted these ORs and AUCs using a similar logistic regression model but including age, gender, and a group indicator variable as the respective covariates. In both unadjusted and adjusted analyses, the effect of healthy controls was set as the reference of the group indicator variable. We calculated the p-values of the Wald's score test to assess the significance of different log-ORs of each subgroup of ME/CFS in relation to the group of healthy controls. The significance level of each executed test was set at 5%. In Supplementary File, one can find a detailed description of the likelihood function of the regression models used and how the ORs (or the log-ORs) are related to the parameters of these models.
To investigate the impact of multiple testing on the results, we adjusted the raw p-values of the Wald's score tests in order to ensure a false discovery rate of 5%. With this purpose, we used the Benjamini-Hochberg (BH) and Benjamini-Yekutieli (BY) procedures under the assumption of independent and positively correlated tests, respectively (40, 41). In this analysis, adjusted p < 0.05 were indicative of statistically significant associations.
Finally, we estimated the statistical power of the detected associations using a parametric Bootstrap approach (42). For each antibody, we used the following algorithm: (i) determine the optimal seropositivity cutoff by maximizing the likelihood ratio statistic as a function of this parameter when comparing the above logistic models with and without the group indicator covariate; (ii) generate the seropositivity data resulting from the optimal cutoff; (iii) estimate a logistic model including the group indicator as the only covariate (unadjusted analysis) or a logistic model including age, gender and group indicator variables as the respective covariates (adjusted analysis) using the seropositivity data obtained in (ii); simulate 1,000 data sets using the seropositive probability estimates obtained from models fitted in (iii); (iv) calculate the power of the association between seropositivity and each study group by the proportion of simulated data sets in which the association was deemed significant at the 5% significance level using the Wald's score test as described above.
The statistical analysis was conducted in the R software version 4.0.3. In particular, the estimation of the logistic regression models was done using the “glm” command and the analysis based on the AUC was conducted using the package “pROC” (43). In the multiple testing analysis, the raw p-values were adjusted by the BH and BY procedures using the package “MASS” (44). The corresponding scripts are available from the first or the corresponding author upon request.
Results
Basic Characterization of Study Participants
The four subgroups of ME/CFS had the same age distribution approximately (Kruskal-Wallis test, p = 0.30) with means of 44.6, 40.7, 43.3, and 40.9 years old for S0, S1, S2, and S3, respectively (Table 1). The respective mean ages of disease onset were 32.1, 30.2, 31.3, and 27.3 years old, while the mean disease durations were 12.7, 11.6, 12.1, and 13.5 years for the same subgroups. The differences in these variables were not statistically significant (p = 0.55 and 0.21, respectively). Similarly, the percentages of female patients ranged from 70.8% to 80.6%, but they were not statistically different (Pearson's χ2 test, p = 0.62).
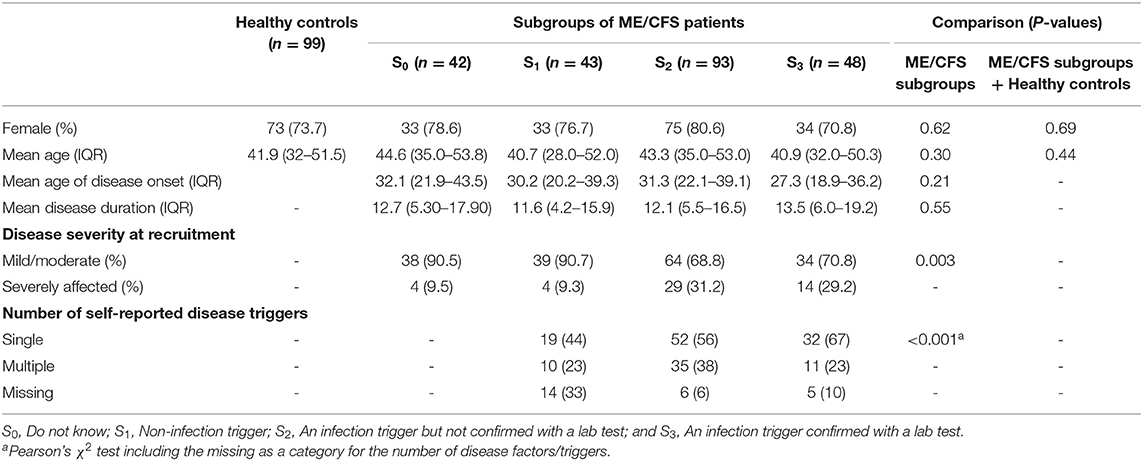
Table 1. Basic characteristics of study participants where patients with ME/CFS were split into four subgroups according to the responses about their disease triggers in the symptoms' assessment questionnaire.
Overall, the percentage of severely affected patients significantly differed among the subgroups (Pearson's χ2 test, p = 0.003). In particular, the percentage of these patients in S0 and S1 was approximately 9%. This value was in clear contrast with the 30% of severely affected patients belonging to S2 and S3, both groups related to infection triggers.
In terms of the number of narrated disease factors or triggers reported in the participant's questionnaire, the subgroup S1 had the lowest percentage of patients reporting a single factor or trigger for their disease (44%) when compared to infection-related subgroups S2 and S3 (56 and 67%, respectively; Table 1). The same subgroup was the one with the highest percentage of missing data to this question (33% for S1 vs. 6 and 10% for S2 and S3, respectively). Overall, the distribution of the number of reported disease factors or triggers was significantly different among subgroups S1, S2, and S3 (Pearson's χ2 test, p < 0.001) mostly due to differences in the amount of missing data.
These subgroups of ME/CFS patients were well matched for gender and age with respect to the healthy control group (Pearson's χ2 and Kruskal-Wallis tests, p = 0.69 and 0.44, respectively).
Disease Factors or Triggers Narrated by Different Subgroups of ME/CFS Patients
When the 184 patients belonging to the subgroups S1, S2, and S3 were asked to narrate the factors or triggers of their disease in the participant questionnaire, 103 (56%) and 56 (30%) of them reported single and multiple factors (or triggers), respectively. However, 25 patients (14%) did not mention any specific trigger or factor contributing to their disease. In total, there were 14 distinct categories of disease triggers narrated by the patients. These categories were consistent to the ones reported by previous epidemiological studies about possible triggers of ME/CFS (22, 23).
The following non-infection factors or triggers were mentioned by patients mostly belonging to the subgroup S1: stress subdivided into general anxiety (9%, n = 20), personal (8%, n = 18) or professional-related stress (5%, n = 11); accidents/injuries/surgeries (5%, n = 11); pregnancy, childbirth and other problems related to women's reproduction system (3%, n = 6), and other non-infection triggers (Table 2). The remaining factors were related to microbial infections and/or infectious diseases: upper respiratory tract infections – glandular fever (GF), tonsillitis, EBV infections, or throat infection (21%, n = 48); lower respiratory tract infections – chest infection or pneumonia (4%, n = 10); flu- or cold-like illnesses (11%, n = 26); gastrointestinal problems and related infections (4%; n = 9); and tropical infectious diseases – Dengue fever and schistosomiasis (1%, n = 3); and other viral or bacterial infection, and unspecified infections (22%, n = 51). Note that 6 patients from subgroup S1 mentioned an infection in the narrative question about the factors or triggers of their disease. However, the same patients also reported other possible non-infection triggers, such as trauma, bereavement, and stress. We speculate that these patients attributed a higher likelihood to these non-infection disease triggers when answering the related question in the symptoms' assessment questionnaire. Interestingly, patients belonging to the subgroup S3 reported the highest percentage of disease factors or triggers consistent with an EBV infection (46%, n = 22). Patients from subgroup S2 also self-reported a high frequency of EBV-related factors or triggers (27%, n = 25), but closely matched by a flu-like infection or illness (22%, n = 20).
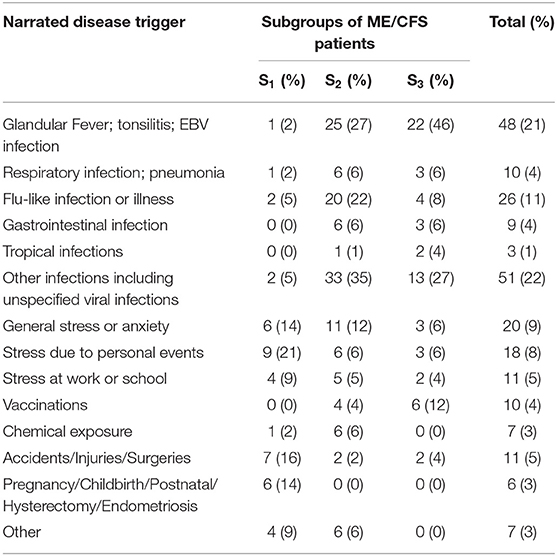
Table 2. Frequency and the respective percentage within brackets of specific disease factors or triggers narrated by patients from the subgroups S1 (n = 43), S2 (n = 93), and S3, (n = 48) in the participant's questionnaire.
Serological Data Analysis by Subgroup of ME/CFS Patients
We then compared the serological data of these ME/CFS subgroups of patients with the group of healthy controls (Figure 1). In this analysis, we intended to investigate the impact of cutoff on the resulting seropositivity OR and AUC between each subgroup of ME/CFS patients and the group of healthy controls.
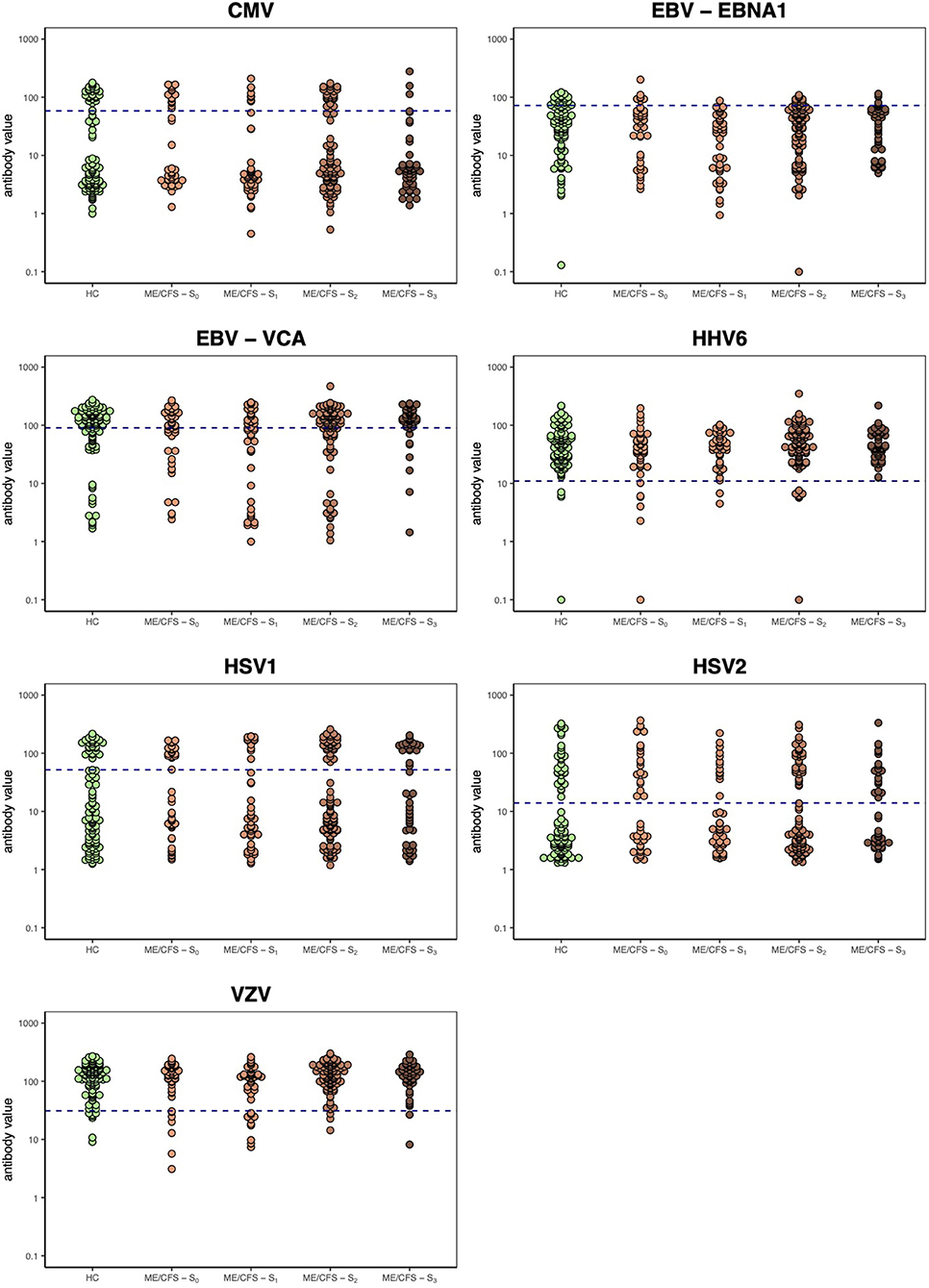
Figure 1. Herpesvirus serology data per study group including the four ME/CFS subgroups. Horizontal dashed lines represent the optimal seropositivity cutoff for the unadjusted analysis according to the maximization of likelihood ratio statistic for testing the significance of the group indicator covariate in the logistic models (see Supplementary Figure 1).
With respect to unadjusted analysis, the AUCs were in most cases estimated between 0.50 and 0.60 (Figure 2A). This finding suggested that serological data had limited predictive power to discriminate the seropositivity of subgroups of ME/CFS patients from that of healthy controls. The highest estimated AUC was approximately 0.75 for VZV when comparing the seropositivity of the subgroup S2 to healthy controls using cutoffs below 15 U/ml.
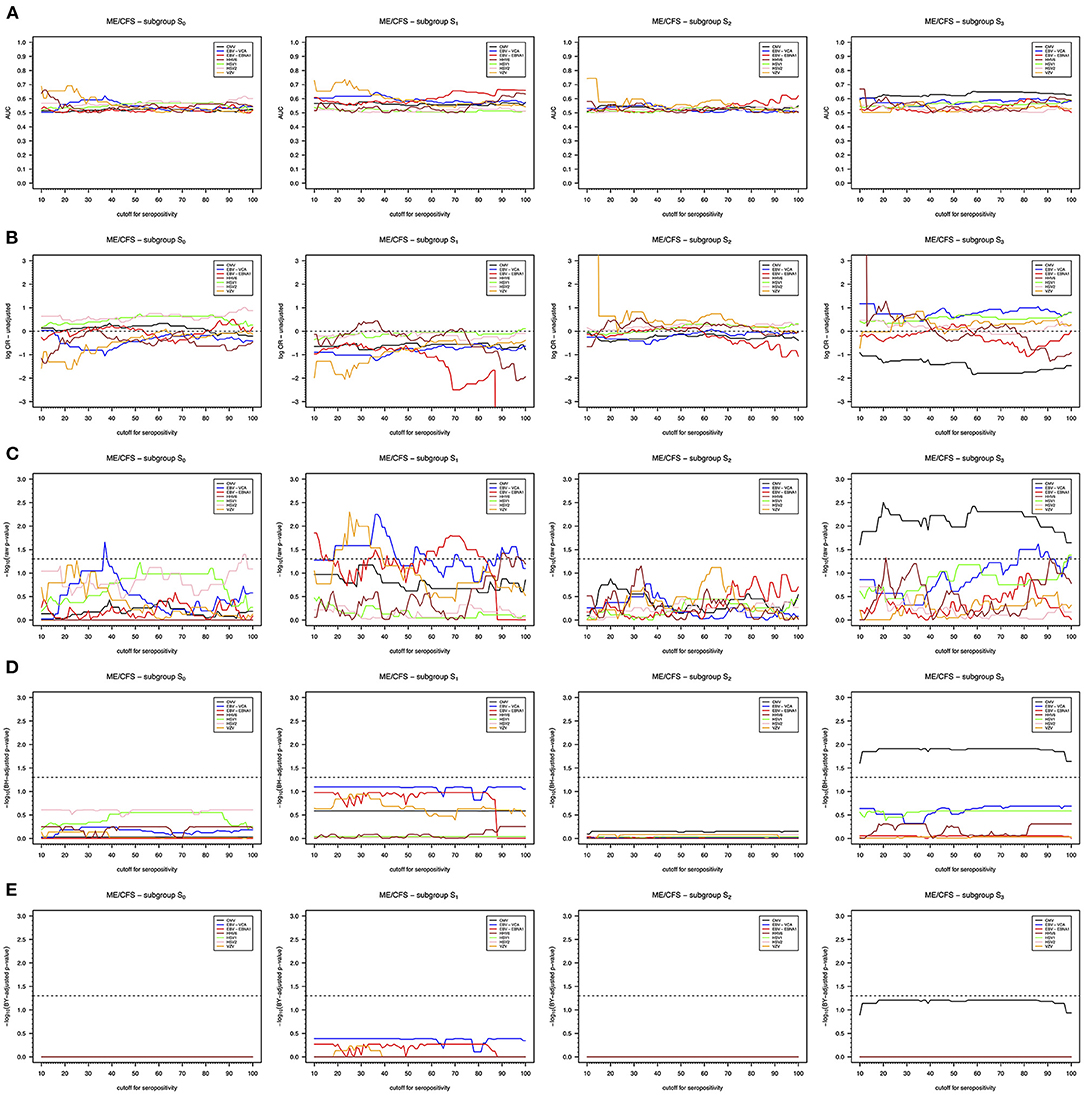
Figure 2. Unadjusted association analysis of seropositivity to different herpesvirus antigens as function of the cutoff defining seropositivity. (A) AUC of the probabilities of being seropositive estimated in each subgroup of ME/CFS patients when compared to the same probabilities estimated in the group of healthy controls. (B) Log-ORs of being seropositive in each subgroup of ME/CFS patients in relation to the group of healthy controls. (C) Raw p-values of Wald's score test for the significance of log-ORs. (D) The corresponding BH-adjusted p-values. (E) The corresponding BY-adjusted p-values. For convenience, raw and adjusted p-values were transformed as –log10(p-value). The dashed lines in the respective plots represent the threshold referring to the 5% significance level [i.e., –log10(0.05); C] or the 5% false discovery rate. (D,E) Cutoff values in which –log10(p-values) are above these thresholds provided evidence for significant associations.
According to the OR estimates, we could not find any significant association of subgroups S0 and S2 with herpesviruses serology (Figures 2B,C). The only exception was a putative association between the subgroup S0 and the antibodies against EBV-VCA using a cutoff of 37 U/ml. Interestingly, before correcting for multiple testing, we found significant negative associations (i.e., negative log-ORs) between the subgroup S1 and antibodies against EBV-VCA, EBV-EBNA1, and VZV depending on the cutoff used (Figures 2B,C). These negative associations suggested decreased seroprevalences to these herpesviruses in this subgroup when compared to the group of healthy controls. When controlling for multiple testing, these associations were not considered statistically significant using either BH or BY procedures (Figures 2D,E).
We also found a significant negative association between subgroup S3 and CMV seropositivity (Figures 2B,C), which suggested decreased antibody levels in this subgroup of patients in relation to group of healthy controls. The corresponding AUC was estimated around 0.65 for most of cutoffs (Figure 2A). This association was consistent across the range of cutoffs specified for the analysis and even after controlling for multiple testing using the BH procedure based on the assumption of independent tests (Figure 2D). However, the statistical significance of the association was lost after using the BY procedure based on the assumption of positively correlated tests (Figure 2E).
Similar findings were obtained when adjusting for possible confounding effects of age and gender (Supplementary Figures 2A–E). This agreement between unadjusted and adjusted analyses can be explained by a good matching between the different ME/CFS subgroups of patients and healthy controls in terms of age and gender (Table 1). However, the significance of adjusted ORs was slightly reduced due to these putative confounding factors (Supplementary Figure 2C).
Finally, we estimated the statistical power related to the identified associations using the optimal seropositivity cutoff for each herpesvirus antibody. For the unadjusted analysis, these optimal cutoffs varied from 11 U/ml to 90 U/ml (Supplementary Figure 1 and Supplementary Table 1). Similar optimal cutoffs were obtained for the analysis adjusting for age and gender (Supplementary Figure 3 and Supplementary Table 1) with the exception of EBV-EBNA1 for which the optimal cutoffs were 72 U/ml and 88 U/ml for the unadjusted and adjusted analyses, respectively. The maximum power (~90%) was obtained for the association between CMV seropositivity and ME/CFS subgroup S3 in either unadjusted or adjusted analyses (Supplementary Figure 4). A high power (~75%) was also obtained for the associations between VZV seropositivity and ME/CFS subgroup S1. The remaining associations between each study group and herpesvirus seropositivity had a power that did not exceed 60%. In conclusion, the manufacturer's seropositivity cutoffs were not the most adequate to maximize the chance of finding an association of ME/CFS subgroups with the herpesviruses serology and only three associations between the study groups and herpesviruses seropositivity had a high statistical power.
Discussion
In contrast with the original study where we could not find differences related to herpesviruses serology between healthy controls and ME/CFS patients divided according to their disease severity (32), our re-analysis of the same data identified two subgroups of ME/CFS patients (S1 and S3) in which such differences are now statistically significant. This new finding was only possible due to the stratification of patients according to a question related to the occurrence of an infection at disease onset together with a sensitivity analysis of the seropositivity cutoff used. Patients' stratification or subtyping was performed in line with past recommendations for ME/CFS research (28). Following this recommendation, we previously performed an immunological investigation based on a stratification of ME/CFS patients according to the severity of their symptoms (32). By using this stratification, we showed perturbations in the T-cell compartment, namely, in effector CD8+ T cells and in the mucosal-associated invariant T cells. In another study using similar stratification of the samples from the UKMEB, the levels of the cellular stress biomarker GDF15 were found to be increased in severely affected patients at different time points (45). We speculate that other immunological perturbations could be detected if our alternative stratification could have been used. This investigation will be carried out in the near future.
In line with our findings, evidence has been emerging that the occurrence of an acute infection at the onset of disease symptoms is indeed a key stratifying factor to detect genetic and immunological differences between subgroups of ME/CFS patients when compared to healthy controls (17, 46). However, the simplistic approach of dividing patients according to non-infection and infection triggers might not be sufficient to obtain relatively homogeneous subgroups of ME/CFS patients, which affects the statistical power to detect any disease-specific effects. Besides the limited choice of antibodies against different herpesvirus-related antigens, the large heterogeneity in infectious triggers seems a possible explanation for the lack of association between the subgroup S2 and herpesviruses seropositivity. Notwithstanding not having their infection trigger confirmed in the lab, patients from this subgroup reported the highest proportion of flu-like illnesses, which could have been caused by the influenza virus, the rhinovirus, or the respiratory syncytial virus (47). It is then conceivable that these patients exhibit different pathological mechanisms of ME/CFS according to the causative virus, some of which without any direct impact on the antibody responses against herpesviruses. To overcome these problems, we recommend the collection of infection-trigger data as detailed and accurate as possible.
Our most consistent association was obtained between CMV seropositivity and patients from the subgroup S3. These patients tended to be less seropositive to this herpesvirus when compared to healthy controls, irrespective of the seropositivity cutoff value used. Previously, different serological investigations did not provide conclusive evidence for the role of CMV on ME/CFS pathogenesis, as reviewed elsewhere (24). The lack of or the use of an inadequate stratification could also explain these past findings. In this regard, the unveiled association was obtained in a subgroup in which the accuracy of the reporting might be the highest, because the disease-triggering infections were supposedly confirmed in the lab. However, we cannot ignore the fact that this subgroup has a large fraction of patients whose disease trigger was related to an EBV infection, one of the most reported causative agents of ME/CFS. Therefore, it is possible that our finding resulted from a coincidence between a low-resolution patient's stratification and a random enrichment of a specific infection trigger in one of the subgroups.
A supposedly decreased seropositivity (or antibody levels) to CMV in an EBV-infection trigger could be explained by the hyperregulation hypothesis (11). According to this hypothesis, a possible pathological mechanism of ME/CFS is related to an expansion of regulatory CD4+ T cells (Tregs) driven by an autoimmune response against a viral antigen that mimics a self-antigen. This expansion of Tregs upon herpesvirus infection or reactivation locks the (adaptive) immune system in an active state of hyperregulation where different infections are more difficult to be cleared from the body. Frequent infections are in fact reported by patients with ME/CFS (33). The question is then how the expansion of Tregs could affect antibody responses against CMV. The so-called follicular Tregs might hold the answer to this question. These specialized Tregs are derived from Treg precursors with the ability to migrate to germinal center reactions (GCRs) to inhibit the respective antibody production and antibody maturation (48). In particular, experiments with animal models demonstrated that the amount of IgG antibodies against different foreign antigens is increased in immunized mice depleted of follicular Tregs (49, 50). In this line of thought, it is reasonable to assume that an increased proportion of Tregs in ME/CFS could be translated into an increased proportion of follicular Tregs. This increase could in turn decrease the antibody production derived from GCRs. We can then hypothesize that an EBV infection triggered an autoimmune response that disrupted the normal balance between Tregs and effector CD4+ T cells; a peptide of the viral EBNA6 was found to share a high sequence homology with the human lactoperoxidase and thyroid peroxidase (30). The disruption of this balance could lead to an increase of both natural and follicular Tregs. A possible consequence of this increase is a diminished antibody production against a posterior CMV infection or reactivation. Note that several peptides from CMV were also found as putative candidate for molecular mimicry with human proteins (51). Similar to the situation of immunosuppression, a reduction in the humoral immunity against CMV would render ME/CFS patients more susceptible to a possible reactivation of this virus (52). It is worth noting that the role of follicular Tregs was never investigated in ME/CFS patients.
Another interesting finding is the possible association between the subgroup S1 and EBV and VZV seropositivity. This subgroup refers to patients who reported non-infectious triggers, mostly related to stressful or stress-related events. It is also a group where ME/CFS was triggered in many women who had problems during and after pregnancy, had difficult childbirth or had disorders related to women's reproduction system. In line with this finding, stressful conditions and events such as the ones experienced by astronauts increase the chance of herpesvirus reactivation, specifically, EBV, VZV and CMV (53). Reactivation of latent herpesvirus infections could be explained by an increase in production of stress-related hormones together with an inflammatory cytokine signature that debilitates the immune system. This subgroup is then expected to have a higher prevalence of active herpesvirus infections than the remaining subgroups of ME/CFS patients and healthy controls. Given that this subgroup could represent <50% of the patients (22, 23), it is likely to have insufficient statistical power to detect any differences in herpesvirus reactivation rates between ME/CFS and healthy controls even in the case of a proper stratification of the patients' populations. This limitation is yet another reason that could explain the inconsistent findings on herpesvirus reactivation across many studies on ME/CFS.
We did not find any association between the subgroup S0 and herpesviruses seropositivity. This subgroup represented 18.5% of the patients' cohort, a value compatible with the percentages of patients that did not report any disease triggering event from past epidemiological studies [10%, (22); 24%, (54)]. The sample size of this subgroup was not very large and, therefore, we cannot rule out that our lack of associations could be simply due to insufficient statistical power to detect putative associations between this subgroup and herpesviruses seropositivity.
In our association analysis, we allowed the seropositivity cutoff to vary within a given range of possible values, similarly done in a recent study of molecular mimicry between Anoctamin 2 and EBNA1 in multiple sclerosis (55). This analytical approach seems reasonable given the difficulty to choose the best seropositivity cutoff among the different criteria and methods available, as illustrated in the earlier analyses of the same data (38, 39). This approach is also in line with several discussions about seropositivity estimation and the sensibility to use a fixed cutoff (56–59). However, varying the cutoffs defining seropositivity might increase the chance of false positives due to the multiple testing problem. We attempted to overcome this problem by controlling the false discovery rate, but the small sample size of each subgroup of ME/CFS did not allow to reach statistical significance of the detected associations when using the BY procedure based on the assumption of multiple positively correlated tests. On the other hand, our power calculations suggested a high probability of detecting some of the associations under the assumption that they were actually true. Therefore, the correct application of cutoff-varying approach should include a thorough assessment of a putative multiple testing problem together with a power calculation in order to assess the statistical consistency of the findings.
As final remarks, we should also note that cutoffs for detecting associations between herpesviruses and ME/CFS might vary from one lab to another and with the serological kits used. In addition, a high cutoff for the data might not define seropositivity per se, but rather a high antibody response whose detection could be the primary objective of the analysis (30, 31). The use of a high cutoff is also in accordance with a modeling approach where seropositivity might be subdivided into different levels (60–62). Therefore, our sensitivity-like approach seems to have the capacity to detect further serological associations beyond the ones based on the classical seroprevalence. Such a capacity could increase the chance of reaching scientific reproducibility. We then recommend the routine use of this approach in future serological investigations of ME/CFS.
Data Availability Statement
The raw data supporting the conclusions of this paper will be made available from Eliana M. Lacerda upon request.
Ethics Statement
The studies involving human participants were reviewed and approved by London School of Hygiene & Tropical Medicine (LSHTM) Ethics Committee (Ref. 6123) and the National Research Ethics Service (NRES) London-Bloomsbury Research Ethics Committee (REC ref. 11/10/1760, IRAS ID: 77765). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
NS conceived this research. HM and NS supervised this research. J-SL and JC generated the serology data. AG and EL compiled and curated the data related to ME/CFS triggers. EL and LN were responsible for data collection of the UKMEB. TD, AG, JA-A, and NS performed the data analysis. FW, CS, LN, and HM helped in data interpretation. TD, AG, and NS wrote the manuscript. All authors have revised, read, and approved the final version of the manuscript.
Funding
TD, HM, and NS were partially funded by the Fundação para a Ciência e a Tecnologia, Portugal (ref: UIDB/00006/2020 and UIDB/04561/2020). NS, EL, and CS were partially funded by ME Research UK (SCIO Charity Number SC036942) with the financial support of The Fred and Joan Davies Bequest. TD also received travel funding from the EUROMENE Cost Action (ref. CA15111) for a short scientific mission to the London School of Hygiene & Tropical Medicine in 2018. JA-A acknowledged the financial support of the Project MTM2016-76969-P from the Spanish State Research Agency (AEI) co-funded by the European Regional Development Fund (ERDF), the Competitive Reference Groups 2017-2020 (ED431C 2017/38) from the Xunta de Galicia through the ERDF. The UK ME/CFS Biobank was established with a joint grant from the charities ME Association (including continuing support), ME Research UK and Action for ME, as well as private donors. Research reported in this manuscript was supported by the National Institutes of Health (NIH) under award number 2R01AI103629. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2021.686736/full#supplementary-material
References
1. Rivera MC, Mastronardi C, Silva-Aldana CT, Arcos-Burgos M, Lidbury BA. Myalgic encephalomyelitis/chronic fatigue syndrome: a comprehensive review. Diagnostics. (2019) 9:91. doi: 10.3390/diagnostics9030091
2. Lim EJ, Ahn YC, Jang ES, Lee SW, Lee SH, Son CG. Systematic review and meta-analysis of the prevalence of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J Transl Med. (2020) 18:100. doi: 10.1186/s12967-020-02269-0
3. Hanson MR, Germain A. Letter to the editor of metabolites. Metabolites. (2020) 10:216. doi: 10.3390/metabo10050216
4. Valdez AR, Hancock EE, Adebayo S, Kiernicki DJ, Proskauer D, Attewell JR, et al. Estimating prevalence, demographics, and costs of ME/CFS using large scale medical claims data and machine learning. Front Pediatr. (2019) 6:412. doi: 10.3389/fped.2018.00412
5. Raine R, Carter S, Sensky T, Black N. General practitioners' perceptions of chronic fatigue syndrome and beliefs about its management, compared with irritable bowel syndrome: Qualitative study. Br Med J. (2004) 328:1354–6. doi: 10.1136/bmj.38078.503819.EE
6. Scheibenbogen C, Freitag H, Blanco J, Capelli E, Lacerda E, Authier J, et al. The European ME/CFS Biomarker Landscape project: An initiative of the European network EUROMENE. J Transl Med. (2017) 15:162. doi: 10.1186/s12967-017-1263-z
7. Estévez-López F, Mudie K, Wang-Steverding X, Bakken IJ, Ivanovs A, Castro-Marrero J, et al. Systematic Review of the Epidemiological Burden of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Across Europe: Current Evidence and EUROMENE Research Recommendations for Epidemiology. J Clin Med. (2020) 9:1557. doi: 10.3390/jcm9051557
8. Pheby DFH, Araja D, Berkis U, Brenna E, Cullinan J, de Korwin J-D, et al. The Development of a Consistent Europe-Wide Approach to Investigating the Economic Impact of Myalgic Encephalomyelitis (ME/CFS): A Report from the European Network on ME/CFS (EUROMENE). Healthcare. (2020) 8:88. doi: 10.3390/healthcare8020088
9. Sotzny F, Blanco J, Capelli E, Castro-Marrero J, Steiner S, Murovska M, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome–Evidence for an autoimmune disease. Autoimmun Rev. (2018) 17:601–9. doi: 10.1016/j.autrev.2018.01.009
10. Blomberg J, Gottfries CG, Elfaitouri A, Rizwan M, Rosén A. Infection elicited autoimmunity and Myalgic encephalomyelitis/chronic fatigue syndrome: An explanatory model. Front Immunol. (2018) 9:229. doi: 10.3389/fimmu.2018.00229
11. Sepúlveda N, Carneiro J, Lacerda E, Nacul L. Myalgic encephalomyelitis/chronic fatigue syndrome as a hyper-regulated immune system driven by an interplay between regulatory T cells and chronic human herpesvirus infections. Front Immunol. (2019) 10:2684 doi: 10.3389/fimmu.2019.02684
12. Wirth K, Scheibenbogen C. A Unifying Hypothesis of the Pathophysiology of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS): Recognitions from the finding of autoantibodies against ß2-adrenergic receptors. Autoimmun Rev. (2020) 19:102527. doi: 10.1016/j.autrev.2020.102527
13. Stanculescu D, Larsson L, Bergquist J. Hypothesis: Mechanisms That Prevent Recovery in Prolonged ICU Patients Also Underlie Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Front Med. (2021) 8:628029. doi: 10.3389/fmed.2021.628029
14. Morris G, Maes M, Berk M, Puri BK. Myalgic encephalomyelitis or chronic fatigue syndrome: how could the illness develop? Metab Brain Dis. (2019) 34:385–415. doi: 10.1007/s11011-019-0388-6
15. Underhill RA. Myalgic encephalomyelitis, chronic fatigue syndrome: An infectious disease. Med Hypotheses. (2015) 85:765–73. doi: 10.1016/j.mehy.2015.10.011
16. Hatziagelaki E, Adamaki M, Tsilioni I, Dimitriadis G, Theoharides TC. Myalgic encephalomyelitis/chronic fatigue syndrome—metabolic disease or disturbed homeostasis due to focal inflammation in the hypothalamus? J Pharmacol Exp Ther. (2018) 367:155–67. doi: 10.1124/jpet.118.250845
17. Steiner S, Becker SC, Hartwig J, Sotzny F, Lorenz S, Bauer S, et al. Autoimmunity-related risk variants in PTPN22 and CTLA4 are associated with ME/CFS with infectious onset. Front Immunol. (2020) 11:578. doi: 10.3389/fimmu.2020.00578
18. Lande A, Fluge Ø, Strand EB, Flåm ST, Sosa DD, Mella O, et al. Human leukocyte antigen alleles associated with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Sci Rep. (2020) 10:5267. doi: 10.1038/s41598-020-62157-x
19. Smith J, Fritz EL, Kerr JR, Cleare AJ, Wessely S, Mattey DL. Association of chronic fatigue syndrome with human leucocyte antigen class II alleles. J Clin Pathol. (2005) 58:860–3. doi: 10.1136/jcp.2004.022681
20. Smith AK, Fang H, Whistler T, Unger ER, Rajeevan MS. Convergent genomic studies identify association of GRIK2 and NPAS2 with chronic fatigue syndrome. Neuropsychobiology. (2011) 64:183–94. doi: 10.1159/000326692
21. Nacul L, O'Boyle S, Palla L, Nacul FE, Mudie K, Kingdon CC, et al. How myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) progresses: the natural history of ME/CFS. Front Neurol. (2020) 11:826. doi: 10.3389/fneur.2020.00826
22. Chu L, Valencia IJ, Garvert DW, Montoya JG. Onset patterns and course of myalgic encephalomyelitis/chronic fatigue syndrome. Front Pediatr. (2019) 7:12. doi: 10.3389/fped.2019.00012
23. Johnston SC, Staines DR, Marshall-Gradisnik SM. Epidemiological characteristics of chronic fatigue syndrome/myalgic encephalomyelitis in Australian patients. Clin Epidemiol. (2016) 8:97–107. doi: 10.2147/CLEP.S96797
24. Rasa S, Nora-Krukle Z, Henning N, Eliassen E, Shikova E, Harrer T, et al. Chronic viral infections in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J Transl Med. (2018) 16:268. doi: 10.1186/s12967-018-1644-y
25. Ariza ME. Myalgic encephalomyelitis/chronic fatigue syndrome: The human herpesviruses are back! Biomolecules. (2021) 11:1–17. doi: 10.3390/biom11020185
26. Nacul L, Lacerda EM, Kingdon CC, Curran H, Bowman EW. How have selection bias and disease misclassification undermined the validity of myalgic encephalomyelitis/chronic fatigue syndrome studies? J Health Psychol. (2019) 24:1765–69. doi: 10.1177/1359105317695803
27. Malato J, Graça L, Nacul L, Lacerda E, Sepúlveda N. Statistical challenges of investigating a disease with a complex diagnosis. medRxiv. (2021) 2021.03.19.21253905. doi: 10.1101/2021.03.19.21253905
28. Jason LA, Corradi K, Torres-Harding S, Taylor RR, King C. Chronic fatigue syndrome: the need for subtypes. Neuropsychol Rev. (2005) 15:29–58. doi: 10.1007/s11065-005-3588-2
29. Ariza ME. Commentary: antibodies to human herpesviruses in myalgic encephalomyelitis/chronic fatigue syndrome patients. Front Immunol. (2020) 11:1945. doi: 10.3389/fimmu.2020.01400
30. Loebel M, Eckey M, Sotzny F, Hahn E, Bauer S, Grabowski P, et al. Serological profiling of the EBV immune response in Chronic Fatigue Syndrome using a peptide microarray. PLoS ONE. (2017) 12:e0179124. doi: 10.1371/journal.pone.0179124
31. Blomberg J, Rizwan M, Böhlin-Wiener A, Elfaitouri A, Julin P, Zachrisson O, et al. Antibodies to human herpesviruses in myalgic encephalomyelitis/chronic fatigue syndrome patients. Front Immunol. (2019) 10:1946. doi: 10.3389/fimmu.2019.01946
32. Cliff JM, King EC, Lee JS, Sepúlveda N, Wolf AS, Kingdon C, et al. Cellular immune function in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Front Immunol. (2019) 10:796. doi: 10.3389/fimmu.2019.00796
33. Lacerda EM, Geraghty K, Kingdon CC, Palla L, Nacul L. A logistic regression analysis of risk factors in ME/CFS pathogenesis. BMC Neurol. (2019) 19:275. doi: 10.1186/s12883-019-1468-2
34. Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann Intern Med. (1994) 121:953–9. doi: 10.7326/0003-4819-121-12-199412150-00009
35. Carruthers BM, Jain AK, De Meirleir KL, Peterson DL, Klimas NG, Lemer AM, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: clinical working case definition, diagnostic and treatment protocols. J Chronic Fatigue Syndr. (2003) 11:7–115. doi: 10.1300/J092v11n01_02
36. Lacerda EM, Bowman EW, Cliff JM, Kingdon CC, King EC, Lee J-S, et al. The UK ME/CFS biobank for biomedical research on myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and multiple sclerosis. Open J Bioresour. (2017) 4:4. doi: 10.5334/ojb.28
37. Lacerda EM, Mudie K, Kingdon CC, Butterworth JD, O'Boyle S, Nacul L. The UK ME/CFS biobank: a disease-specific biobank for advancing clinical research into myalgic encephalomyelitis/chronic fatigue syndrome. Front Neurol. (2018) 9:1026. doi: 10.3389/fneur.2018.01026
38. Domingues TD, Mouriño H, Sepúlveda N. Analysis of antibody data using finite mixture models based on scale mixtures of skew-normal distributions. medRxiv. (2021) 2021.03.08.21252807. doi: 10.1101/2021.03.08.21252807
39. Domingues TD, Mouriño H, Sepúlveda N. “A statistical analysis of serological data from the UK myalgic encephalomyelitis/chronic fatigue syndrome BioBank,” in AIP Conference Proceedings 2293:420099. doi: 10.1063/5.0026633
40. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B. (1995) 57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
41. Benjamini Y, Yekutieli D. The control of the false discovery rate in multiple testing under dependency. Ann Stat. (2001) 29:1165–88. doi: 10.1214/aos/1013699998
42. Efron B, Tibshirani RJ. An Introduction to the Bootstrap. 1st Edn. Dordrecht: Springer Science+Business Media (1993).
43. Robin X, Turck N, Hainard A, Tiberti N, Lisacek F, Sanchez JC, et al. pROC: an open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinformatics. (2011) 12:77. doi: 10.1186/1471-2105-12-77
44. Venables WN, Ripley BD. Modern Applied Statistics with S. Fourth. New York, NY: Springer. (2002).
45. Melvin A, Lacerda E, Dockrell HM, O'Rahilly S, Nacul L. Circulating levels of GDF15 in patients with myalgic encephalomyelitis/chronic fatigue syndrome. J Transl Med. (2019) 17:409. doi: 10.1186/s12967-019-02153-6
46. Szklarski M, Freitag H, Lorenz S, Becker S, Sotzny F, Bauer S, et al. Delineating the association between soluble CD26 and autoantibodies against G-protein coupled receptors, immunological and cardiovascular parameters identifies distinct patterns in post-infectious vs. non-infection-triggered Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front Immunol. (2021) 12:1077. doi: 10.3389/fimmu.2021.644548
47. Monto AS. Epidemiology of viral respiratory infections. Am J Med. (2002) 112:4–12. doi: 10.1016/S0002-9343(01)01058-0
48. Maceiras AR, Fonseca VR, Agua-Doce A, Graca L. T follicular regulatory cells in mice and men. Immunology. (2017) 152:25–35. doi: 10.1111/imm.12774
49. Chung Y, Tanaka S, Chu F, Nurieva RI, Martinez GJ, Rawal S, et al. Follicular regulatory T cells expressing Foxp3 and Bcl-6 suppress germinal center reactions. Nat Med. (2011) 17:983–8. doi: 10.1038/nm.2426
50. Wollenberg I, Agua-Doce A, Hernández A, Almeida C, Oliveira VG, Faro J, et al. Regulation of the germinal center reaction by Foxp3+ follicular regulatory T Cells. J Immunol. (2011) 187:4553–60. doi: 10.4049/jimmunol.1101328
51. Lunardi C, Bason C, Corrocher R, Puccetti A. Induction of endothelial cell damage by hCMV molecular mimicry. Trends Immunol. (2005) 26:19–24. doi: 10.1016/j.it.2004.10.009
52. Krmpotić A, Podlech J, Reddehase MJ, William ·, Britt J, Jonjić S. Role of antibodies in confining cytomegalovirus after reactivation from latency: three decades' résumé. Med Microbiol Immunol. (2019) 208:415–29. doi: 10.1007/s00430-019-00600-1
53. Rooney BV, Crucian BE, Pierson DL, Laudenslager ML, Mehta SK. Herpes virus reactivation in astronauts during spaceflight and its application on earth. Front Microbiol. (2019) 10:16. doi: 10.3389/fmicb.2019.00016
54. Nacul LC, Lacerda EM, Pheby D, Campion P, Molokhia M, Fayyaz S, et al. Prevalence of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) in three regions of England: a repeated cross-sectional study in primary care. BMC Med. (2011) 9:91. doi: 10.1186/1741-7015-9-91
55. Tengvall K, Huang J, Hellström C, Kammer P, Biström M, Ayoglu B, et al. Molecular mimicry between Anoctamin 2 and Epstein-Barr virus nuclear antigen 1 associates with multiple sclerosis risk. Proc Natl Acad Sci USA. (2019) 116:16955–60. doi: 10.1073/pnas.1902623116
56. Kafatos G, Andrews NJ, McConway KJ, Maple PAC, Brown K, Farrington CP. Is it appropriate to use fixed assay cut-offs for estimating seroprevalence? Epidemiol Infect. (2016) 144:887–95. doi: 10.1017/S0950268815001958
57. Migchelsen SJ, Martin DL, Southisombath K, Turyaguma P, Heggen A, Rubangakene PP, et al. Defining seropositivity thresholds for use in trachoma elimination studies. PLoS Negl Trop Dis. (2017) 11:e0005230. doi: 10.1371/journal.pntd.0005230
58. Bouman JA, Bonhoeffer S, Regoes RR. Estimating seroprevalence with imperfect serological tests: exploiting cutoff-free approaches. bioRxiv. (2020) 2020.04.29.068999. doi: 10.1101/2020.04.29.068999
59. Ridge SE, Vizard AL. Determination of the optimal cutoff value for a serological assay: An example using the Johne's Absorbed EIA. J Clin Microbiol. (1993) 31:1256–61. doi: 10.1128/JCM.31.5.1256-1261.1993
60. Nhat NTD, Todd S, De Bruin E, Thao TTN, Vy NHT, Quan TM, et al. Structure of general-population antibody titer distributions to influenza A virus. Sci Rep. (2017) 7:6060. doi: 10.1038/s41598-017-06177-0
61. Pothin E, Ferguson NM, Drakeley CJ, Ghani AC. Estimating malaria transmission intensity from Plasmodium falciparum serological data using antibody density models. Malar J. (2016) 15:79. doi: 10.1186/s12936-016-1121-0
62. Moreira da Silva J, Prata S, Domingues TD, Leal RO, Nunes T, Tavares L, et al. Detection and modeling of anti-Leptospira IgG prevalence in cats from Lisbon area and its correlation to retroviral infections, lifestyle, clinical and hematologic changes. Vet Anim Sci. (2020) 10:100144. doi: 10.1016/j.vas.2020.100144
Keywords: disease trigger, cutoff value, stratification, Epstein-Barr virus, human cytomegalovirus, varicella-zoster virus, human herpesvirus-6, herpes simplex virus 1 and 2
Citation: Domingues TD, Grabowska AD, Lee J-S, Ameijeiras-Alonso J, Westermeier F, Scheibenbogen C, Cliff JM, Nacul L, Lacerda EM, Mouriño H and Sepúlveda N (2021) Herpesviruses Serology Distinguishes Different Subgroups of Patients From the United Kingdom Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Biobank. Front. Med. 8:686736. doi: 10.3389/fmed.2021.686736
Received: 27 March 2021; Accepted: 01 June 2021;
Published: 05 July 2021.
Edited by:
Ana Afonso, University of São Paulo, BrazilReviewed by:
Ronald Balczon, University of South Alabama, United StatesMichael White, Institut Pasteur, France
Copyright © 2021 Domingues, Grabowska, Lee, Ameijeiras-Alonso, Westermeier, Scheibenbogen, Cliff, Nacul, Lacerda, Mouriño and Sepúlveda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nuno Sepúlveda, bnVub3NlcEBnbWFpbC5jb20=