 Carmen de Jesús-Gil1
Carmen de Jesús-Gil1 Lídia Sans-de San Nicolàs1
Lídia Sans-de San Nicolàs1 Irene García-Jiménez1
Irene García-Jiménez1 Marta Ferran2Ramon M. Pujol2
Marta Ferran2Ramon M. Pujol2 Luis F. Santamaria-Babí1*
Luis F. Santamaria-Babí1*- 1Translational Immunology, Department of Cellular Biology, Physiology and Immunology, Faculty of Biology, Universitat de Barcelona, Parc Científic de Barcelona, Barcelona, Spain
- 2Department of Dermatology, Hospital del Mar (Institut Hospital del Mar d'Investigacions Mèdiques), Universitat Autònoma de Barcelona, Barcelona, Spain
Psoriasis is a common inflammatory skin condition resulting from the interplay between epidermal keratinocytes and immunological cellular components. This sustained inflammation is essentially driven by pro-inflammatory cytokines with the IL-23/IL-17 axis playing a critical central role, as proved by the clinical efficacy of their blockade in patients. Among all the CD45R0+ memory T cell subsets, those with special tropism for cutaneous tissues are identified by the expression of the Cutaneous Lymphocyte-associated Antigen (CLA) carbohydrate on their surface, that is induced during T cell maturation particularly in the skin-draining lymph nodes. Because of their ability to recirculate between the skin and blood, circulating CLA+ memory T cells reflect the immune abnormalities found in different human cutaneous conditions, such as psoriasis. Based on this premise, studying the effect of different environmental microbial triggers and psoriatic lesional cytokines on CLA+ memory T cells, in the presence of autologous epidermal cells from patients, revealed important IL-17 cytokines responses that are likely to enhance the pro-inflammatory loop underlying the development of psoriatic lesions. The goal of this mini-review is to present latest data regarding cytokines implicated in plaque and guttate psoriasis immunopathogenesis from the prism of CLA+ memory T cells, that are specifically related to the cutaneous immune system.
Introduction
The regulation of cytokine production and signaling in chronic cutaneous inflammation is influenced by genetic and environmental factors. This minireview focuses on human psoriasis, both plaque and guttate forms of the disease, and the cytokine production by human circulating CLA+ memory T cells, a relevant subset of memory T cells associated to the regional cutaneous immune system. In translational research in dermatology, there is a need to develop new approaches beyond animal models and in vitro studies (1, 2), since the results in those models are not always translated into the clinic (3). For instance, excellent basic science results in the field of cytokines in psoriasis have been generated for IFN-α, IFN-γ, IL-20, or IL-22, but their in vivo neutralization with monoclonal antibodies in clinical trials did not improve psoriasis severity (4–7), indicating that those cytokines, despite their presence in the lesions, are not suitable for patients' treatment.
When studying human chronic cutaneous inflammatory diseases, an alternative approach focused on the human regional cutaneous immune system in disease would allow to focus more closely on the immunological mechanism of disease that takes place within the skin, the proper organ where the pathological process is carried out. The presence of the skin associated lymphoid tissue (SALT) was proposed by J. Wayne Streilein based on the existence of some T cells with special function related only to the skin (8). The Cutaneous Lymphocyte-associated Antigen (CLA) identifies the subset of effector memory T cells with skin tropism that recirculates between skin and blood during cutaneous inflammation and reflects immunological abnormalities present in the skin. The CLA molecule is a carbohydrate modification of the platelet selectin ligand-1 (PSGL-1) (9), which binds both endothelial cell and platelet selectins (E-selectin and P-selectin) molecules expressed on post-capillary venules in the skin. Its expression is induced on CD45R0+ memory T cells at skin draining lymph nodes (10) and it is present in more than 90% of cutaneous infiltrating T cells but in <20% of T cells in other peripheral tissues. Interestingly, a proportion of CLA-expressing T cells can be also found in circulation, representing around 15% of human circulating T cells (10). Indeed, the fact that CLA+ memory T cells recirculate between skin and blood was evidenced by action of efalizumab (a monoclonal antibody targeting the CD11a subunit of LFA-1 molecule that blocked lymphocyte extravasation toward the skin) in psoriasis (11) and atopic dermatitis (12) patients, which proved clinical improvement but also resulted in a lymphocytosis effect of CLA+ T cells that caused relapses after treatment discontinuation (13). The recirculating capacity of CLA+ memory T cells is key to their value in translational research, due to their ability to reflect the immune abnormalities found in numerous human cutaneous conditions such as psoriasis, atopic dermatitis, contact dermatitis, drug-induced allergic reactions, vitiligo, herpes simplex, rosacea, cutaneous T cell lymphoma, or alopecia areata (14, 15).
In order to properly study the regional cutaneous immune system in psoriasis, the use of clinical material from non-treated patients provides clear advantages as it is commented below. With this purpose, we have established a new ex vivo coculture model made of lymphoid and epidermal cells from the same patient (16) that integrates relevant elements of psoriasis immunopathology: skin-associated memory T cells (CLA+ T cells) isolated from blood samples, autologous lesional epidermal cells disaggregated from biopsies from the same patient and a clinically relevant trigger of the disease and flares (such as Streptococcus pyogenes). When circulating CLA+ T cells and autologous lesional epidermal cells cocultures are activated by Streptococcus pyogenes extract (SE), specific Th17/Th1/Th22 responses occurs, together with production of disease relevant chemokines (CXCL9, CXCL10, CXCL11), which is not the case in CLA− T cells cocultures or in unstimulated basal conditions. Interestingly, the levels of IL-17A and other cytokines expressed by CLA+ T cells in response to SE are highly correlated with serum anti-Streptolysin O antibody titer (ASO), that is commonly used to assess patients recent infection by S. pyogenes in daily clinical practice. The fact that ASO levels and CLA+ T cells-dependent IL-17A, IFN-γ, and IL-22 production are directly associated shows how these cytokines can be measured ex vivo and integrated with the patient clinical features and environmental exposure to S. pyogenes.
In the following subsections, information on cytokines in psoriasis immunopathology is provided from the prism of T cells that are related to the cutaneous immune system. These results have been generated using clinical material (blood and skin biopsies) from non-treated psoriasis patients.
Influence of Psoriatic Inflammatory Environment on CLA-Dependent IL-17A and IL-17F Production
Memory T cells present in the psoriatic lesion are exposed to the cytokine inflammatory environment and this may influence the effector functions of the IL-17 cytokines, that are clinically relevant mediators in psoriasis. Since peripheral CLA+ memory T cells recirculate between skin and blood during psoriasis and reflect the immunological abnormalities present in the skin, they can be used to study the lesional inflammatory environmental cytokines. The presence of IL-15 and IL-23 is increased in lesional skin from psoriasis patients. Psoriatic epidermal keratinocytes show increased expression of both IL-15 and IL-15R (17). Similarly, injured keratinocytes but also dendritic cells have been proved to produce increased amounts of IL-23 in psoriatic lesions (18). Besides, both pro-inflammatory cytokines are linked to Th17 biology. IL-15 is known to induce IL-17 secretion by T cells and to be critical for maintaining memory Th17 cells (19), whilst IL-23 is considered the “master regulator” of Th17 cell differentiation and development. Single nucleotide polymorphisms (SNPs) associated with psoriasis have been also described for both IL-15 and IL-23 (20–22). However, despite their known connection to psoriasis pathogenesis, it was not until recently that the cooperation between these two cytokines has been addressed. Our group has shown that IL-15 and IL-23 act synergistically on cocultures of CLA+ memory T cells and autologous epidermal cells to produce significantly increased levels of IL-17F and IL-17A in psoriasis when compared to CLA− T cells cocultures (23). Importantly, this synergy was not observed for lesional resident memory T cells or in cocultures from healthy individuals, pointing out the relevance of circulating CLA+ T cells in psoriasis pathogenesis. Altogether, it is a clear example of how the proinflammatory milieu in psoriatic lesions influences specifically skin-tropic memory T cells and induces a Th17 response contributing to the maintenance of the disease.
CLA+ T Cells in Psoriasis Produce More IL-17F Than IL-17A
The IL-17 family comprises six structurally related members (named from A to F) that act as homodimers, except for IL-17A and IL-17F that can form heterodimers together. In psoriasis, IL-17A is pointed out as the most important mediator (24), which is supported by the effectiveness of its blockade in patients. However, its principal homolog, IL-17F, has been also proved to be increased in lesional skin and blood from psoriasis patients (25–27). From our experience, circulating CLA+ memory T cells activated with a relevant disease trigger, such as Streptococcus pyogenes, and in the presence of lesional epidermal cells, secrete a higher amount of IL-17F than IL-17A in vitro (28, 29). Similarly, increased CLA+ memory T cell-dependent IL-17F response was observed when stimulating the cocultures with Candida albicans (30) or the combination of the pro-inflammatory cytokines IL-15 and IL-23 (23). As such, CLA+ memory T cells should be considered an important source of IL-17F in psoriasis. Because IL-17A and IL-17F homodimers and heterodimer share their signaling receptor, constituted by the IL-17RA and IL-17RC subunits, they induce similar gene expression patterns. Nonetheless, the relevance of IL-17F in psoriasis pathogenesis has been shown in patients and animal models. For example, IL-17F knock-out (KO) mice are more resistant to imiquimod-induced psoriasiform inflammation than the IL-17A KO counterparts (31). In humans, the rapid clinical efficacy achieved by brodalumab, a monoclonal antibody targeting the IL-17RA subunit (that is part of the receptor for IL-17A, IL-17F, IL-17A/F heterodimer, and IL-25) first showed the advantages of targeting beyond IL-17A (32, 33). Most importantly, the promising results of the phase 2 and phase 3 clinical trials studying the nanobody sonelokimab and the monoclonal antibody (mAb) bimekizumab, respectively, both of which target IL-17A, IL-17F, and IL-17A/F, further highlight the clinical relevance of IL-17F in psoriasis patients (34, 35).
IL-9 Is Not Produced Transiently by CLA+ T Cells in Human Psoriasis
In humans, IL-9-secreting CD4+ T cells, namely Th9, have been described as a distinct T cell population with preferential skin tropism (36). In this work, CLA+ Th9 cells were transiently induced by Candida albicans-pulsed monocytes particularly but also after non-physiological polyclonal activation, supporting the association of Th9 cells to the skin regardless of their antigen specificity and using lymphocytes from healthy subjects. This transitory Th9 induction peaked just before the increase of IL-17 and IFN-γ induction, suggesting a paracrine regulation by IL-9 that was further confirmed by its own neutralization. More interestingly, a significant increase of IL-9+ cells, mostly CD3+ CD4+ T cells, was found in lesional psoriatic skin compared to atopic dermatitis and healthy cutaneous tissue.
However, when studying the functional role of IL-9 in psoriasis patients (plaque and guttate forms) in our coculture model (29), we found that, after S. pyogenes activation, the kinetic of IL-9 production measured in CLA+ T cells and epidermal cells coculture supernatants was similar to those of IL-17A and IFN-γ, progressively increasing over time and dependent on MHC class I and class II presentation, which contrasted with the transient IL-9 induction reported before (36). Interestingly, IL-9 partially enhanced SE-induced IL-17A, but not IFN-γ, secretion by CLA+ T cells, as well as it promoted the survival of the skin-homing T cell subset in psoriasis.
Using well-defined clinical samples also allows obtaining information on the relationship of cytokines with patient clinical status. CLA+ T cells-derived cytokines are associated with clinical features of skin diseases because they represent a subset of memory T cells that are involved in the regional cutaneous immune system. To support the relevance of our findings regarding the role of IL-9 in psoriasis, it was observed that SE-induced CLA+ T cells-dependent IL-9 correlated with psoriasis severity (measured as Psoriasis Area Severity Index, PASI) in patients. Moreover, in guttate psoriasis, the peak in IL-9 production was found on patients having the highest ASO levels indicating higher exposure to S. pyogenes.
Guttate Psoriasis: Where Genetic and Environmental Factors Interact Producing Th17 Response By CLA+ T Cells
Guttate psoriasis is a form of psoriasis that is strongly associated with the genetic predisposing allele HLA-Cw6 and is commonly triggered by Streptococcus pyogenes throat infections (37). This situation has provided a good opportunity to study genetic and environmental factors influence on cytokine production by CLA+ T cells in psoriasis (28). The coculture of CLA+ T cells activated with S. pyogenes clearly demonstrated that non-treated guttate psoriasis patients produced significantly more IL-17A/F cytokines than IFN-γ. However, the most interesting finding was that guttate psoriasis patients carrying the HLA-Cw6 allele and/or whose flare was produced by S. pyogenes pharyngitis, in comparison to guttate psoriasis patients that did not fulfill those criteria, significantly produced more IL-17A/F by CLA+ T cells. Similar dominant IL-17 response also induced genes that belong to the IL-17 transcriptome in keratinocytes such as DEFB4, LCN2, IL-8, but no to the IFN-γ (CXCL9, CXCL10, and CXCL11). Such influence of genetic and microbe infection on IL-17 response in guttate psoriasis patients has been clarified by analyzing CLA+ T cells.
Plaque Psoriasis: IL-17 Production and Patients Heterogeneity
Chronic plaque psoriasis, or psoriasis vulgaris, is the most common form of psoriasis that is generally diagnosed based on the shape and location of the lesions and the persistent duration of the disease. Heterogeneity among plaque psoriasis patients has been suggested (38) but it is still not well-characterized. Nowadays, plaque psoriasis is considered a single entity in most of the clinical studies yet. However, recent results have suggested that the IL-17 cytokines responses by CLA+ T cells may be differentially influenced by environmental factors, particularly by exposure to microbes that could favor IL-17 production in chronic plaque psoriasis.
Streptococcus pyogenes-induced IL-17 response by CLA+ T cells in psoriasis patients is higher when patients present higher titer of immunoglobulin A against S. pyogenes extract (39). We reported that anti-SE IgA values in psoriasis patients (both plaque and guttate forms) are higher than in atopic dermatitis and healthy controls. But, most importantly, we found that increased mucosal exposure to S. pyogenes was present in chronic plaque psoriasis patients despite negative ASO titer and no clear association of the current flare with Streptococcal infection. This finding is of special interest since there may be multiple cases of plaque psoriasis where the implication of Streptococcus pyogenes has been discarded, but the bacteria may still be present at the tonsils and contribute to recurrent flares in those patients. In this regard, a recent population-based cohort study has reported how tonsillectomy diminished the risk of developing psoriasis (40). Future studies should confirm how such heterogeneity may influence the natural history of psoriasis disease and/or how different patients respond to specific treatments.
Moreover, chronic plaque psoriasis patients also present increased exposure to Candida albicans (CA) (41, 42), that is a potent inducer of IL-17 cytokines in humans (43). Importantly, immune response against this fungus is mainly mediated by CLA+ memory T cells, further supporting the pro-inflammatory loop present at cutaneous lesions in psoriasis patients (30). Interestingly, non-treated chronic plaque psoriasis patients, without clinical signs of candidiasis, present increased levels of both IgA and IgG specific for C. albicans in plasma. In particular, CLA-dependent IL-17A and IL-17F responses correlated with Candida-specific IgA, but not IgG, only in chronic plaque psoriasis. Additionally, a proteomic study of plasma samples from 114 non-treated plaque psoriasis patients revealed that, those with higher anti-Candida IgA levels presented increased levels of proteins involved in antimicrobial humoral response, especially proteins showing anti-candida activity [such as eosinophil cationic protein (ECP/RNASE3), Chitinase-3-like protein 1 (CHI3L1) or azurocidin]. These findings point out the implication of Candida albicans in chronic plaque psoriasis, a matter that we believe should be further explored in the clinic.
Altogether, these results support the existence of heterogeneity among chronic plaque psoriasis patients that can influence IL-17 production and, thus, the evolution of the course of psoriasis disease.
Discussion
In plaque and guttate forms psoriasis, the IL-17 response derived from CLA+ T cells is clearly influenced by different factors that are related to patient features and that can be studied ex vivo using circulating memory T cells belonging to the regional cutaneous immune system (Figure 1). Using clinical samples from non-treated patients has allowed relating in vitro cytokine responses with clinical data in a translational way. For example, these studies reported increased production of IL-17F over IL-17A by skin associated T lymphocytes, which is reflected in the clinic as the greatest response of bimekizumab (neutralizing both IL-17A/F) (34). Also, this approach has shown that guttate psoriasis patients positive for the HLA-C predisposing allele and/or the ASO perform increased cutaneous pro-inflammatory response by CLA+ T cells. In the end, how CLA+ memory T cells are the link between relevant disease triggers and the increased IL-17 response observed in psoriatic skin.
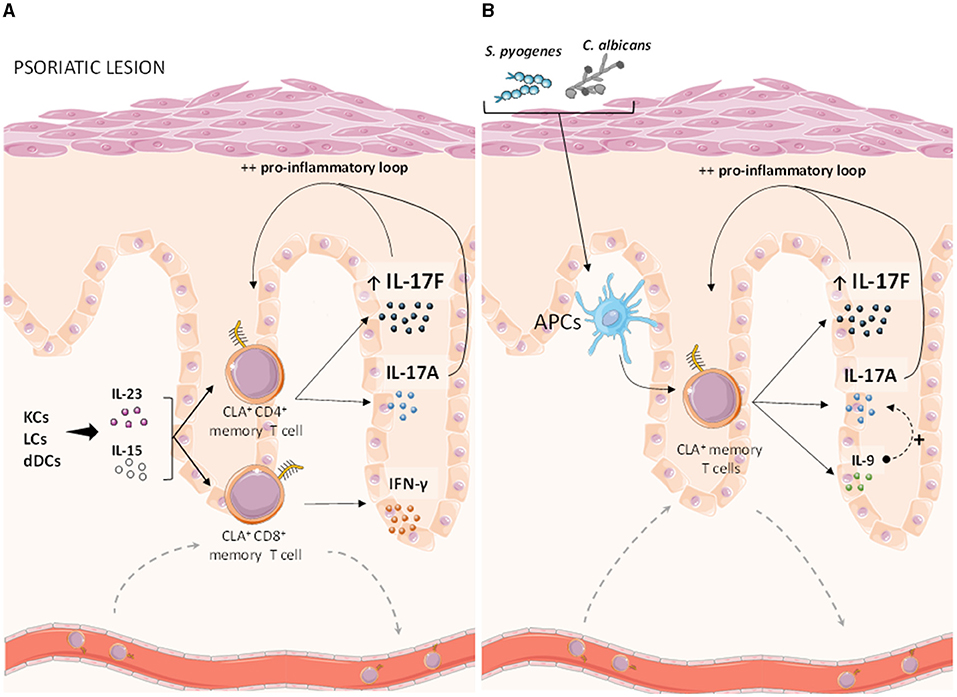
Figure 1. Human CLA+ memory T cells and cytokines in psoriasis. As the subset of memory T cells associated to the cutaneous immune system, circulating CLA+ T cells are key responders to lesional pro-inflammatory cytokines and relevant microbes that induce important type 17 responses, therefore contributing to the pro-inflammatory loop leading to the appearance of psoriatic lesions. (A) IL-15 and IL-23, which are mainly produced by keratinocytes as well as epidermal and dermal dendritic cells, synergistically activate CLA+ CD4+ memory T cells from psoriasis patients leading to an increased induction of IL-17F and IL-17A cytokines, whereas IFN-γ secretion is likely mediated by CLA+ CD8+ memory T cells in psoriasis but also in healthy controls. (B) S. pyogenes and C. albicans antigens, presented by epidermal antigen presenting cells, have been proved to induce significantly higher IL-17A/F and IL-9 responses by CLA+ memory T cells in psoriasis patients, compared to CLA− T cells. Besides, S. pyogenes-induced IL-9 has shown to enhance IL-17A responses, further reinforcing the pro-inflammatory loop underlying psoriasis lesions. CLA, cutaneous leukocyte-associated antigen; KCs, keratinocytes; LCs, Langerhans cells; dDCs, dermal dendritic cells; APCs, antigen presenting cells. This figure was created using Servier Medical Art (smart) images.
Mouse models or complex in vitro systems, although they are key to study basic pathogenic mechanisms, do not integrate elements that can influence IL-17 responses in patients such as the genetic background or their exposure to microbes able to induce IL-17 responses. How these factors may influence patients response to treatment, the natural history of disease or the existence of psoriasis endotypes, if any, is still an open question in this field. In this regard, the possible role of CLA+ memory T cells in the development of psoriatic arthritis (PsA) was early explored but discarded, due to the absence of CLA+ memory lymphocytes within synovial tissue (44, 45). The relevance of heterogeneity in chronic plaque psoriasis due to different immunoglobulins specific for microorganisms and CLA+ T cells-dependent IL-17A/F responses is particularly interesting since these cytokines, in contrast to others that are also increased in lesions, are validated as safe and clinically effective targets by the use of neutralizing monoclonal antibodies (46).
Nonetheless, this review presents some limitations, as other types of psoriasis (pustular, palmoplantar or inverse), have not been addressed and the study of additional relevant cytokines that are present within psoriatic lesions, such as TNF-α or IL-36, in the context of CLA+ memory T cells remains underexplored. Eventually, these limitations evidence how much research is still needed to completely unveil the intricate between cytokines and the cutaneous immune system in the context of psoriasis. Any translational approach that helps to better characterize cytokine biology in the context of the cutaneous immune response will be essential to fully understand patients responses to current therapies and to continue developing novel strategies in the future.
Author Contributions
CJ-G: writing and figure design. LS, IG-J, MF, and RP: writing. LS-B: IP project founding, writing, and manuscript conceptualization. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Eyerich K, Brown SJ, Perez White BE, Tanaka RJ, Bissonette R, Dhar S, et al. Human and computational models of atopic dermatitis: A review and perspectives by an expert panel of the International Eczema Council. J Allergy Clin Immunol. (2019) 143:36–45. doi: 10.1016/j.jaci.2018.10.033
2. Florian P, Flechsenhar KR, Bartnik E, Ding-Pfennigdorff D, Herrmann M, Bryce PJ, et al. Translational drug discovery and development with the use of tissue-relevant biomarkers: towards more physiological relevance and better prediction of clinical efficacy. Exp Dermatol. (2020) 29:4–14. doi: 10.1111/exd.13942
4. Bissonnette R, Papp K, Maari C, Yao Y, Robbie G, White WI, et al. A randomized, double-blind, placebo-controlled, phase I study of MEDI-545, an anti-interferon-alfa monoclonal antibody, in subjects with chronic psoriasis. J Am Acad Dermatol. (2010) 62:427–36. doi: 10.1016/j.jaad.2009.05.042
5. Harden JL, Johnson-Huang LM, Chamian MF, Lee E, Pearce T, Leonardi CL, et al. Humanized anti-IFN-γ (HuZAF) in the treatment of psoriasis. J Allergy Clin Immunol. (2015) 135:553–6.e3. doi: 10.1016/j.jaci.2014.05.046
6. Gottlieb AB, Krueger JG, Lundblad MS, Gothberg M, Skolnick BE. First-in-human, phase 1, randomized, dose-escalation trial with recombinant anti-IL-20 monoclonal antibody in patients with psoriasis. PLoS ONE. (2015) 10:e0134703. doi: 10.1371/journal.pone.0134703
7. Tsai Y-C, Tsai T-F. Anti-interleukin and interleukin therapies for psoriasis: current evidence and clinical usefulness. Ther Adv Musculoskelet Dis. (2017) 9:227–94. doi: 10.1177/1759720X17735756
8. Wayne Streilein J. Skin-Associated lymphoid tissues (SALT): origins and functions. J Invest Dermatol. (1983) 80:S12–6. doi: 10.1038/jid.1983.4
9. Fuhlbrigge RC, David Kieffer J, Armerding D, Kupper TS. Cutaneous lymphocyte antigen is a specialized form of PSGL-1 expressed on skin-homing T cells. Nature. (1997) 389:978–81. doi: 10.1038/40166
10. Picker LJ, Treer JR, Ferguson-Darnell B, Collins PA, Bergstresser P, Terstappen LW. Control of lymphocyte recirculation in man. II. Differential regulation of the cutaneous lymphocyte-associated antigen, a tissue-selective homing receptor for skin-homing T cells. J Immunol. (1993) 150:1122–36.
11. Vugmeyster Y, Kikuchi T, Lowes MA, Chamian F, Kagen M, Gilleaudeau P, et al. Efalizumab (anti-CD11a)-induced increase in peripheral blood leukocytes in psoriasis patients is preferentially mediated by altered trafficking of memory CD8+ T cells into lesional skin. Clin Immunol. (2004) 113:38–46. doi: 10.1016/j.clim.2004.06.001
12. Harper EG, Simpson EL, Takiguchi RH, Boyd MD, Kurtz SE, Bakke AC, et al. Efalizumab therapy for atopic dermatitis causes marked increases in circulating effector memory CD4+ T cells that express cutaneous lymphocyte antigen. J Invest Dermatol. (2008) 128:1173–81. doi: 10.1038/sj.jid.5701169
13. Johnson-Huang LM, Pensabene CA, Shah KR, Pierson KC, Kikuchi T, Lentini T, et al. Post-therapeutic relapse of psoriasis after CD11a blockade is associated with T cells and inflammatory myeloid DCs. PLoS ONE. (2012) 7:e0030308. doi: 10.1371/journal.pone.0030308
14. Ferran M, Romeu ER, Rincón C, Sagristà M, Giménez Arnau AM, Celada A, et al. Circulating CLA+ T lymphocytes as peripheral cell biomarkers in T-cell-mediated skin diseases. Exp Dermatol. (2013) 22:439–42. doi: 10.1111/exd.12154
15. de Jesús-Gil C, Sans-de San Nicolàs L, García-Jimnénez I, Ferran M, Celada A, Chiriac A, et al. The translational relevance of human circulating memory CLA + T cells in inflammatory skin disorders. Front Immunol. (2021) 12:652613. doi: 10.3389/fimmu.2021.652613
16. Ferran M, Galván AB, Rincón C, Romeu ER, Sacrista M, Barboza E, et al. Streptococcus induces circulating CLA+ memory T-cell-dependent epidermal cell activation in psoriasis. J Invest Dermatol. (2013) 133:999–1007. doi: 10.1038/jid.2012.418
17. Villadsen LS, Schuurman J, Beurskens F, Dam TN, Dagnæs-Hansen F, Skov L, et al. Resolution of psoriasis upon blockade of IL-15 biological activity in a xenograft mouse model. J Clin Invest. (2003) 112:1571–80. doi: 10.1172/JCI200318986
18. Piskin G, Sylva-Steenland RMR, Bos JD, Teunissen MBM. In vitro and in situ expression of IL-23 by keratinocytes in healthy skin and psoriasis lesions: enhanced expression in psoriatic skin. J Immunol. (2006) 176:1908–15. doi: 10.4049/jimmunol.176.3.1908
19. Chen Y, Chauhan SK, Tan X, Dana R. Interleukin-7 and−15 maintain pathogenic memory Th17 cells in autoimmunity. J Autoimmun. (2017) 77:96–103. doi: 10.1016/j.jaut.2016.11.003
20. Weger W, Hofer A, Wolf P, El-Shabrawi Y, Renner W, Kerl H, et al. Role of the interleukin 15 96516A > T and IL15 96330C > A gene polymorphisms in caucasian patients with chronic plaque psoriasis. J Dermatol Sci. (2008) 51:147–9. doi: 10.1016/j.jdermsci.2008.02.010
21. Zhang XJ, Yan KL, Wang ZM, Yang S, Zhang GL, Fan X, et al. Polymorphisms in interleukin-15 gene on chromosome 4q31.2 are associated with psoriasis vulgaris in Chinese population. J Invest Dermatol. (2007) 127:2544–51. doi: 10.1038/sj.jid.5700896
22. Filiz B, Yildirim M, Hekimler Öztürk K, Sirin FB, Çelik S, Erturan I, et al. Evaluation of interleukin-23 receptor (Il-23r) gene polymorphisms and serum il-23 levels in patients with psoriasis. Turkish J Med Sci. (2019) 49:1386–94. doi: 10.3906/sag-1904-48
23. de Jesús-Gil C, Ruiz-Romeu E, Ferran M, Sagristà M, Chiriac A, García P, et al. IL-15 and IL-23 synergize to trigger Th17 response by CLA+ T cells in psoriasis. Exp Dermatol. (2020) 29:630–8. doi: 10.1111/exd.14113
24. Brembilla NC, Senra L, Boehncke WH. The IL-17 family of cytokines in psoriasis: IL-17A and beyond. Front Immunol. (2018) 9:1682. doi: 10.3389/fimmu.2018.01682
25. Johansen C, Usher PA, Kjellerup RB, Lundsgaard D, Iversen L, Kragballe K. Characterization of the interleukin-17 isoforms and receptors in lesional psoriatic skin. Br J Dermatol. (2009) 160:319–24. doi: 10.1111/j.1365-2133.2008.08902.x
26. Kolbinger F, Loesche C, Valentin MA, Jiang X, Cheng Y, Jarvis P, et al. β-Defensin 2 is a responsive biomarker of IL-17A–driven skin pathology in patients with psoriasis. J Allergy Clin Immunol. (2017) 139:923–32.e8. doi: 10.1016/j.jaci.2016.06.038
27. Soderstrom C, Berstein G, Zhang W, Valdez H, Fitz L, Kuhn M, et al. Ultra-Sensitive measurement of IL-17A and IL-17F in psoriasis patient serum and skin. AAPS J. (2017) 19:1218–22. doi: 10.1208/s12248-017-0094-4
28. Ruiz-Romeu E, Ferran M, Sagristà M, Gómez J, Giménez-Arnau A, Herszenyi K, et al. Streptococcus pyogenes–induced cutaneous lymphocyte antigen–positive T cell–dependent epidermal cell activation triggers TH17 responses in patients with guttate psoriasis. J Allergy Clin Immunol. (2016) 138:491–9.e6. doi: 10.1016/j.jaci.2016.02.008
29. Ruiz-Romeu E, Ferran M, de Jesús-Gil C, García P, Sagristà M, Casanova JM, et al. Microbe-Dependent induction of IL-9 by CLA+T cells in psoriasis and relationship with IL-17A. J Invest Dermatol. (2018) 138:580–7. doi: 10.1016/j.jid.2017.08.048
30. De Jesús-Gil C, Sans-de San Nicolàs L, Ruiz-romeu E, Ferran M, Soria-martínez L, García-jiménez I, et al. Interplay between humoral and CLA + T cell response against Candida albicans in psoriasis. Int J Mol Sci. (2021) 22:1–14. doi: 10.3390/ijms22041519
31. Pantelyushin S, Haak S, Ingold B, Kulig P, Heppner FL, Navarini AA, et al. Rorγt + innate lymphocytes and γδ T cells initiate psoriasiform plaque formation in mice. J Clin Invest. (2012) 122:2252–6. doi: 10.1172/JCI61862
32. Foulkes AC, Warren RB. Brodalumab in psoriasis: evidence to date and clinical potential. Drugs Context. (2019) 8:212570. doi: 10.7573/dic.212570
33. Warren RB, Hansen JB, Reich K, Paul C, Puig L. Complete clearance and psoriasis area and severity index response for brodalumab and ustekinumab in AMAGINE-2 and−3. J Eur Acad Dermatology Venereol. (2021) 35:450–7. doi: 10.1111/jdv.16816
34. Reich K, Papp KA, Blauvelt A, Langley RG, Armstrong A, Warren RB, et al. Bimekizumab versus ustekinumab for the treatment of moderate to severe plaque psoriasis (BE VIVID): efficacy and safety from a 52-week, multicentre, double-blind, active comparator and placebo controlled phase 3 trial. Lancet. (2021) 397:487–98. doi: 10.1016/S0140-6736(21)00125-2
35. Papp KA, Weinberg MA, Morris A, Reich K. IL17A/F nanobody sonelokimab in patients with plaque psoriasis: a multicentre, randomised, placebo-controlled, phase 2b study. Lancet. (2021) 397:1564–75. doi: 10.1016/S0140-6736(21)00440-2
36. Schlapbach C, Gehad A, Yang C, Watanabe R, Guenova E, Teague JE, et al. Human TH9 cells are skin-tropic and have autocrine and paracrine proinflammatory capacity. Sci Transl Med. (2014) 6:219ra8. doi: 10.1126/scitranslmed.3007828
37. Wisenseel P, Laumbacher B, Besgen P, Ludolph-Hauser D, Herzinger T, Roecken M, et al. Streptococcal infection distinguishes different types of psoriasis. J Med Genet. (2002) 39:767–8. doi: 10.1136/jmg.39.10.767
38. Swindell WR, Xing X, Stuart PE, Chen CS, Aphale A, Nair RP, et al. Heterogeneity of inflammatory and cytokine networks in chronic plaque psoriasis. PLoS One. (2012) 7:e34594. doi: 10.1371/journal.pone.0034594
39. De Jesús-Gil C, San Nicolás LS, Ruiz-Romeu E, Ferran M, Soria-Martinez L, Chiriac A, et al. Specific IgA and CLA+ T-cell IL-17 response to Streptococcus pyogenes in psoriasis. J Invest Dermatol. (2020) 140:1364–70. doi: 10.1016/j.jid.2019.12.022
40. Chen ML, Ku YH, Yip HT, Wei JCC. Tonsillectomy and the subsequent risk of psoriasis: a nationwide population-based cohort study. J Am Acad Dermatol. (2021) 21:S0190–9622. doi: 10.1016/j.jaad.2021.01.094
41. Fry L, Baker BS. Triggering psoriasis: the role of infections and medications. Clin Dermatol. (2007) 25:606–15. doi: 10.1016/j.clindermatol.2007.08.015
42. Pietrzak A, Grywalska E, Socha M, Roli J, Franciszkiewicz-pietrzak K, Rudnicka L, et al. Prevalence and possible role of candida species in patients with psoriasis : a systematic review and meta-analysis. Mediat Inflamm. (2018) 2018:9602362. doi: 10.1155/2018/9602362
43. Kashem SW, Kaplan DH. Skin immunity to Candida albicans. Trends Immunol. (2016) 37:440–50. doi: 10.1016/j.it.2016.04.007
44. Jones SM, Dixey J, Hall ND, McHugh NJ. Expression of the cutaneous lymphocyte antigen and its counter-receptor E-selectin in the skin and joints of patients with psoriatic arthritis. Br J Rheumatol. (1997) 36:748–57. doi: 10.1093/rheumatology/36.7.748
45. Pitzalis C, Cauli A, Pipitone N, Smith C, Barker J, Marchesoni A, et al. Cutaneous lymphocyte antigen-positive T lymphocytes preferentially migrate to the skin but not to the joint in psoriatic arthritis. Arthritis Rheum. (1996) 39:137–45. doi: 10.1002/art.1780390118
Keywords: psoriasis, CLA+ T cell, IL17A, interleukins, IL17F, IL-9, IL-15
Citation: de Jesús-Gil C, Sans-de San Nicolàs L, García-Jiménez I, Ferran M, Pujol RM and Santamaria-Babí LF (2021) Human CLA+ Memory T Cell and Cytokines in Psoriasis. Front. Med. 8:731911. doi: 10.3389/fmed.2021.731911
Received: 28 June 2021; Accepted: 08 October 2021;
Published: 29 October 2021.
Edited by:
Paul Smith, Connect Biopharma, United StatesReviewed by:
Marina Venturini, Civil Hospital of Brescia, ItalyEva Reali, University of Milano-Bicocca, Italy
Copyright © 2021 de Jesús-Gil, Sans-de San Nicolàs, García-Jiménez, Ferran, Pujol and Santamaria-Babí. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis F. Santamaria-Babí, bHVpcy5zYW50YW1hcmlhQHViLmVkdQ==