 Roberta Bevilacqua1*
Roberta Bevilacqua1* Luca Soraci2
Luca Soraci2 Vera Stara1
Vera Stara1 Giovanni Renato Riccardi3
Giovanni Renato Riccardi3 Andrea Corsonello2,4
Andrea Corsonello2,4 Giuseppe Pelliccioni5
Giuseppe Pelliccioni5 Fabrizia Lattanzio1Sara Casaccia6Johanna Möller7Rainer Wieching8Toshimi Ogawa9
Fabrizia Lattanzio1Sara Casaccia6Johanna Möller7Rainer Wieching8Toshimi Ogawa9 Suichiro Watanabe9Keisuke Kokobun9Izumi Kondo10Eiko Takano10
Suichiro Watanabe9Keisuke Kokobun9Izumi Kondo10Eiko Takano10 Elvira Maranesi1
Elvira Maranesi1- 1Scientific Direction, IRCCS INRCA, Ancona, Italy
- 2Unit of Geriatric Medicine, IRCCS INRCA, Cosenza, Italy
- 3Clinical Unit of Physical Rehabilitation, IRCCS INRCA, Ancona, Italy
- 4Unit of Geriatric Pharmacoepidemiology and Biostatistics, IRCCS INRCA, Cosenza, Italy
- 5Unit of Neurology, IRCCS INRCA, Ancona, Italy
- 6Department of Industrial Engineering and Mathematical Sciences, Polytechnic University of Marche, Ancona, Italy
- 7Department Elderly Care, Diocesan Caritas Association for the Archdiocese of Cologne, Cologne, Germany
- 8Universität Siegen, Wirtschaftsinformatik und Neue Medien, Siegen, Germany
- 9Smart-Aging Research Center, Tohoku University, Sendai, Japan
- 10Department of Rehabilitation Medicine, National Center for Geriatrics and Gerontology, Obu, Japan
Introduction: The focus on intrinsic capacity (IC) could help clinicians to design interventions to improve the health of the older population. This review aims to map the current state of the art in the field of multi-domain interventions based on the IC framework, to allow health professionals in identifying personalized clinical interventions, oriented to empower the older people with a holistic and positive approach.
Methods: A systematic review of the literature was conducted in July 2021 analyzing manuscripts and articles of the last 10.5 years from PubMed, Scopus, Embase, Google Scholar and Elsevier databases. A total of 12 papers were included.
Results: The majority of successful interventions are based on a goal setting approach where the older people are involved in the definition of the strategy to follow to remain active and independent. None of the study have used the IC as a framework to design a clinical intervention.
Conclusion: To the best of our knowledge, no other reviews are reported in the literature regarding the IC. Our study offers several research directions, which may take the existing debates to the next level.
Introduction
Intrinsic capacity (IC) was defined as “the composite of all the physical and mental capacities of an individual” (1), including ability to walk, think, see, hear and re-member. Although older age is often characterized by a decline in baseline IC, the rate of decline widely varies among individuals and baseline IC reflects multiple setbacks and potential recoveries (2, 3). If some older adults are able to maintain functional in-dependence up to very advanced ages, other one’s experience early onset of severe functional disability which substantially affects their quality of life. According to WHO, such biological diversity can arise from inequity, understood as the differential influences of several factors including genetics, sex, ethnicity, and environment on aging itself (4). Anyway, progressive decline in IC may be more or less tolerated up to a critical point when individuals require care and support. IC is only one of many factors that determine biological age, but it can be an important focus for intervention to reduce the biological and functional age of older adults. Therefore, evaluation of bio-logical age through IC can enhance understanding of the functional trajectories and vulnerabilities of individuals and populations and guide individualized preventive measures and interventions that are tailored to the persons’ age, abilities and comorbidities (5).
Assessment of biological age through IC is of extreme importance for the future; losses of IC during the aging process may significantly affect quality of life and become manifested as common problems, such as hearing and vision impairments, memory loss, walking problems, urinary incontinence and loss of positive affect. For such impairments, older people often misbelief that there is no treatment available, and may then disengage from services, lack treatment adherence, with subsequent devastating effects on their quality of life. Recent studies have also shown that loss of IC may decrease quality of life and worsen prognosis in older adults (6). Moreover, IC decline was significantly associated with increased risk of frailty, disability, falls, fractures and death (7).
Regarding frailty and its connection with IC, Belloni et al. (8) assume that the two concepts can be seen as distinct but correlated points on a continuum in which IC represents the reserves of the individual on one side, while frailty is associated with the deficits accumulated with aging on the other. For this reason, it is essential to include also the concept of frailty in the assessment and analysis of the IC-driven interventions.
Due to the heterogeneity of the aging population, characterized by different levels of intrinsic capacity, personalized multicomponent health interventions may represent an effective way to promote health and subjective well-being achievements (9). However, to date, no systematic review focused on evidence about appropriate interventions to preserve intrinsic capacity and daily functioning in older individuals; for this reason, the aim of this systematic review is to map current state of the art in the field of multi-domain interventions based on the IC framework. The availability of evidence on multi-domain interventions that include the IC framework is essential to allow health professionals in identifying personalized clinical interventions, oriented to empower the older people with a holistic and positive approach.
Materials and methods
Literature search and study selection
The methodology of this systematic review was based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines with the main aim of mapping the state of art of multi-domain interventions for older people, grounded on the IC framework. A systematic review of the literature was conducted in July 2021. The data were collected from PubMed, Scopus, Embase, Google Scholar and Elsevier databases, analyzing manuscripts and articles of the last 10.5 years (from January 2011 to June 2021), in order to obtain the latest evidence in the field. The PICOS format (P = population, I = interventions, C = comparator, O = outcome, S = study design) was adopted to formulate inclusion criteria. The inclusion criteria are as follows: (1) randomized controlled trials, quasi-experimental studies, or prospective or retrospective cohort studies, pre-post study with or without control groups; (2) testing of a multi-domain intervention to prevent or treat frailty in people aged ≥ 65 years; (3) classification in terms of (pre) frailty status according to an operationalized definition. Systematic and narrative reviews were excluded. A multi-domain intervention was defined as an intervention that intervenes in at least two different do-mains, including exercise therapy, nutritional intervention, hormone, cognitive or psychosocial interventions (10). As we refer to Intrinsic Capacity, we have included papers on multi-domain interventions on at least three areas within locomotion, cognitive, psychological, vitality and sensory.
Based on consultation with the multidisciplinary research team, multi-modal intervention studies were searched using the following search terms, and the combination thereof: olde*, elde*, intrinsic capacit*, functional ability*/functional status/functional trajectory*, healthy aging/successful aging, prefrail, virtual agent, coaching, self-management, multi-domain intervention, robotic*. The full search string is provided in Table 1.
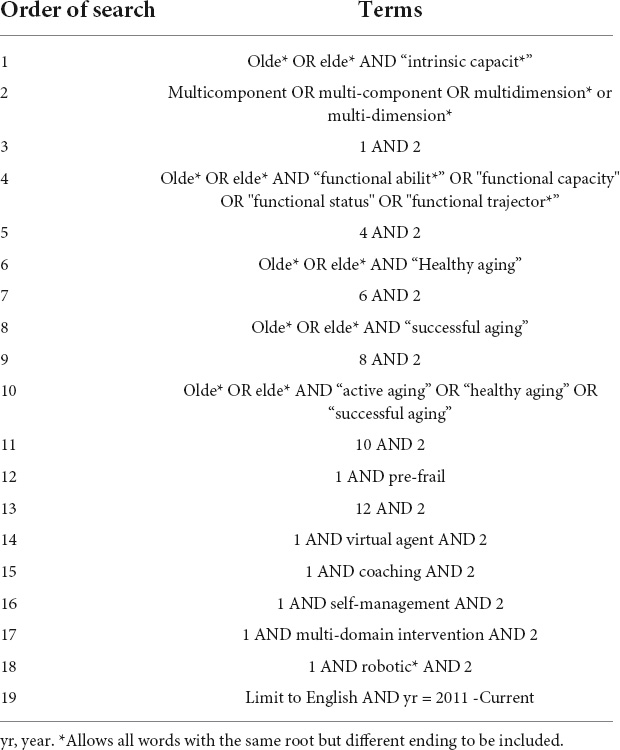
Table 1. Search strategy.
After the preliminary search, 327,563 articles resulted from PubMed, 40,250 from Scopus, 40,098 from Embase, 91,898 from Google Scholar and 492,403 from Elsevier.
The findings were analyzed and screened by four experts of the team, a bioengineer, a clinical neuropsychologist, a statistician and a geriatrician. In particular, three review authors independently reviewed titles and abstract retrieved from the search in order to determine if they met the predefined inclusion criteria. The full text articles were subsequently analyzed.
The first screening was based on the analysis of the title of the findings. After the first step, 61 articles resulted from PubMed, 23 from Scopus, 16 from Embase, 33 from Google Scholar and 55 from Elsevier. A second screening was based on abstract analysis and deduplication of the findings. After this step 41 papers included from Pubmed, 18 from Scopus, 0 from Embase, 11 from Google Scholar and 33 from Elsevier. Another researcher (a statistician) confirmed the accuracy of the papers selection and screened for any possible omission.
Data collection
After the screening based on the inclusion/exclusion criteria, conducted on the full text articles, the studies were selected as follows: 9 from PubMed, 3 from Scopus, 0 from Embase, 0 from Google Scholar, 0 from Elsevier database. Figure 1 shows the flowchart search strategy applied.
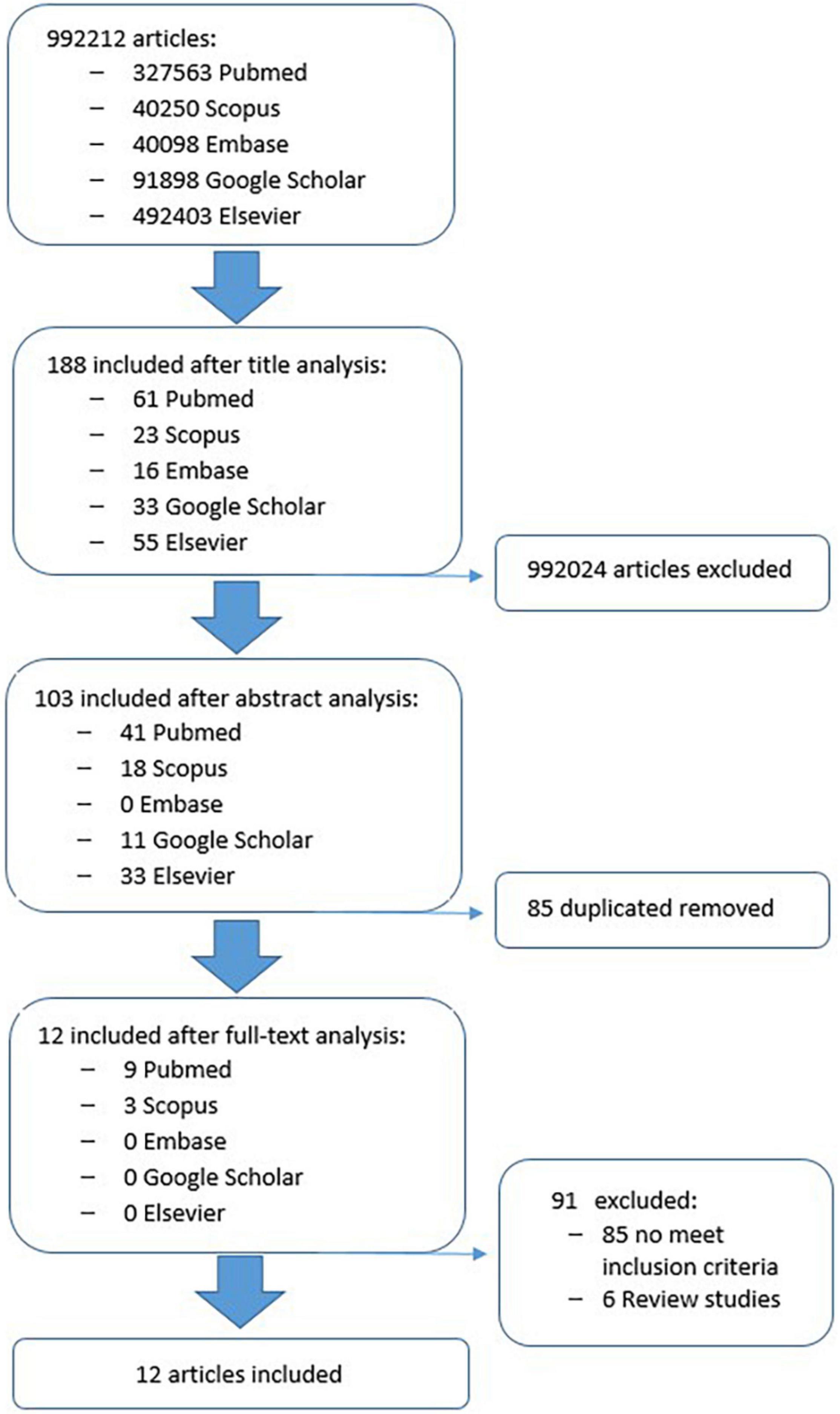
Figure 1. The flowchart search strategy.
Results
A total of 12 papers were included (11–22). The results could not be pooled into a meta-analysis due to clinical heterogeneity clearly observed in the participants’ involvement, in the type of intervention conducted, and in the outcome measures of the included studies.
Study quality evaluation
Quality evaluation of 12 population-based studies was performed based on the PEDro scale, suggested for evidence-based reviews (23). The final score was settled when 3 authors reached agreement after repeated review and analysis. Of the twelve studies considered, the PEDro score ranged from 4 (12) to a maximum of 10 (11) (Table 2). In particular, 10 studies were rated as having a high (11, 13–22), 2 studies (12, 19) as having fair methodological quality.
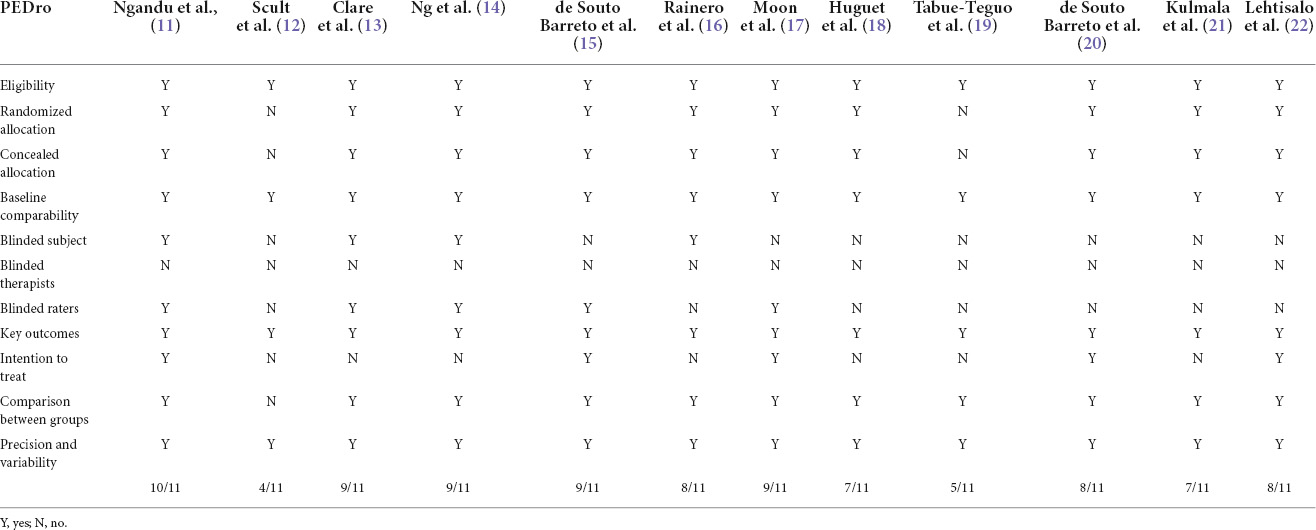
Table 2. Scores of methodological quality assessment of the included studies.
General characteristics of the study population
All the studies were focused on older people with a mean age of 72.9 (± 5.5) years for the multi-domain intervention group and 73.2 (± 5.5) years in the control group. The number of participants involved in all the studies is 8,319, ranging from 46 to 1,827. There were 3,925 males and 4,394 females.
Descriptive analysis and outcome measures
Table 3 shows the characteristics of the included studies. All studies evaluated the impact of multidimensional interventions on some domains of IC, but no one specifically focused on the IC framework as a whole entity. As regards evaluated domains, cognitive functioning was assessed by 7 studies (11, 13–15, 17, 19, 22), physical functioning by 6 studies (13–15, 18, 20, 21), vitality by 5 studies (13–16, 18), and psychosocial well-being by 6 studies (12–16, 18); none of the included studies has instead evaluated the sensory functioning.
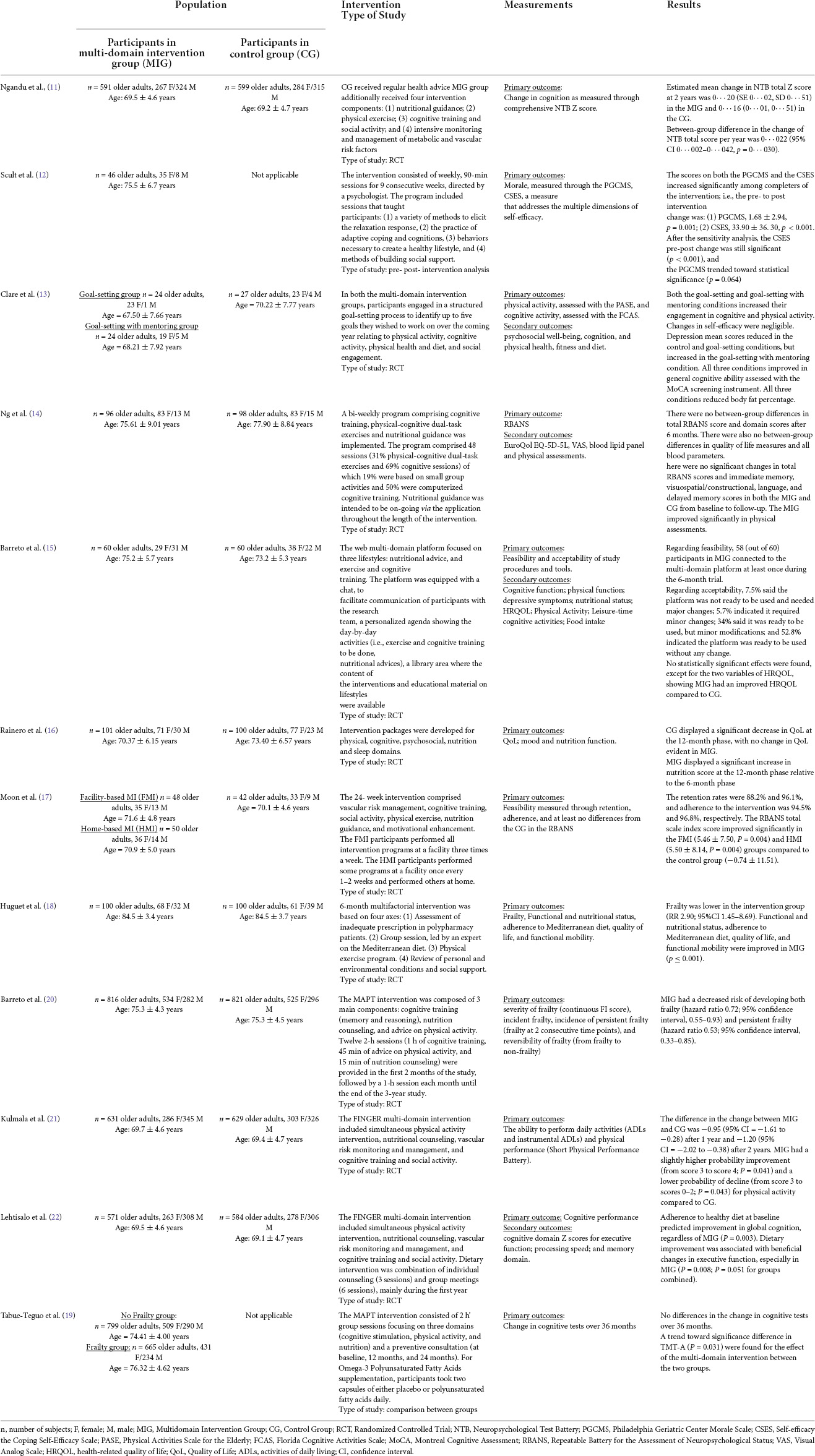
Table 3. Descriptive analysis of the included clinical studies.
Intervention effects
Below is a brief description of the main results reported in the 12 population-based studies categorized according to domains of intervention.
Cognitive functioning
Seven out of twelve studies assessed the effects of interventions on cognitive functioning (11, 13–15, 17, 19, 22). In six studies (11, 14, 15, 17, 19, 22) the intervention was represented by a multidomain training addressing some or all IC domains and made of several components, such as physical activity, cognitive training and social activity, nutritional advice, monitoring and management of risk factors; in one study (13), the multidimensional intervention was designed through a goal-setting approach, asking patients to set up to five goals they wished to accomplish within the coming year.
Four (11, 17, 19, 22) out of the six studies using multidomain intervention training (11, 14, 15, 17, 19, 22) showed a significant benefit on individual cognitive function over time. In particular, in the study by Ngandu et al. (11), individuals in the intervention group (IG) underwent a significant improvement of cognitive scores, executive function and processing speed, even after 2 years; similarly, Moon et al. (11) showed benefits of a 24-week multidomain training on cognitive scores; in the study by Tabue-Tego et al. (19), despite cognitive tests were not significantly different between the control group (CG) and the IG after 36 months of follow-up, a significant trend toward improvement in Trail Making test part A (TMT-A) performance was found in the IG; finally, Lehtisalo et al. (22) showed how adherence to nutritional guidelines in the context of a multidimensional intervention led to benefits in terms of global cognition and executive functioning; only one study (13) assessed the usefulness of a goal-setting approach; individuals in the IG were asked to set up to five goals to accomplish within the coming year; individuals following the goal-setting approach were divided in two groups according to the presence of bi-monthly telephone mentoring. The two goal-setting groups increased their level of cognitive activity relative to controls and achieved additional benefits compared to control in memory and executive function. Adding follow-up mentoring produced further benefits compared to goal-setting alone in global cognition and memory.
Finally, two studies (14, 15) showed no significant effects of multidomain interventions on cognitive scores during follow-up.
Physical activity
Six out of twelve studies assessed the effects of interventions on physical functioning (13–15, 18, 20, 21). In five studies (13–15, 18, 20, 21), the intervention was represented by a multidimensional training program, while in the study by Clare et al. (13) a goal-setting approach was used. Most of the studies reported beneficial effects of multidomain interventions on physical function over time (13, 14, 18, 20, 21), whereas one study (15) showed no significant effect.
In the pilot study by Clare et al. (13), the goal-setting approach with or without mentoring was associated with improved engagement in physical activity, as well as flexibility, grip strength, balance, and agility; furthermore, the goal-setting approach with mentoring improved physical fitness compared to goal-setting approach without mentoring.
In the study by Ng et al. (14), a 24-week multi-domain intervention for older adults at risk of cognitive impairment at neighborhood senior centers was implemented. The program comprised dual-task exercises, cognitive training, and mobile application-based nutritional guidance. Patients in the IG underwent an improvement in Chair Stand Test and grip strength after 24 weeks. Similarly, in the study by Huguet et al. (18), potential benefits of a multidimensional training program were evaluated among 200 community-dwelling pre-frail older patients; at 12 months, individuals in the IG were characterized by lower prevalence of frailty and improved function mobility, with better performance in both the Timed Up and Go (TUG) and Five Time Sit to Stand (FTSST) tests. In the secondary analysis of the MAPT study by de Souto Barreto et al. (20), the effects of a long-term (3-years) multi-domain lifestyle intervention on the severity and incidence of frailty in older adults was investigated. Compared with controls, subjects in the multi-domain group had a decreased risk of developing both frailty and persistent frailty.
Another important study aimed to investigate the effect of multi-domain lifestyle intervention on daily functioning of older people was the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) conducted by Kulmala et al. In their first publication (21) they analyzed, for 2 years, a total of 1,260 older adults who were at risk of cognitive decline. The multi-domain intervention included simultaneous physical activity intervention, nutritional counseling, vascular risk monitoring and management, and cognitive training and social activity. During the 2-year intervention, the activity of daily living (ADL) disability score slightly increased in the control group, while in the intervention group, it remained relatively stable. In terms of physical performance, the intervention group had a slightly higher probability of improvement and a lower probability of decline for chair rise compared to the control group.
As previously reported, only one study (15) showed no benefit of multidomain intervention on physical activity. In this 6-month eMIND project by Barreto et al. (15), researchers evaluated the effects of a multi-domain lifestyle intervention composed of cognitive training, exercise training, and nutritional advices among community-dwelling older adults. One hundred-twenty participants were enrolled and randomized in the multi-domain intervention group and control group. Compared to controls, the intervention had a positive effect on health-related quality of life; no significant effects were observed across the other clinical and lifestyle outcomes.
Vitality
Five out of twelve studies assessed the effects of multi-intervention training on vitality (13–16, 18). Explored aspects of this domain included physical health (13–15, 18, 21), nutritional status (13, 15, 16, 18), and laboratory parameters (13, 14). In four studies (14, 15, 18, 21), the intervention was represented by a multidimensional training program, while in the study by Clare et al. (13) a goal-setting approach was used. Most of the studies reported beneficial effects of multidomain interventions on vitality at follow-up (13, 14, 18, 21), whereas one study (15) showed no significant effect.
The goal-setting approach (13) was associated with increased physical health, as measured in terms of aerobic capacity, flexibility, balance, agility, and hand grip strength; such approach was also associated with decreased serum cholesterol levels and decreased body fat percentage. Similarly, several multidomain trainings resulted to add some benefit in the IG; observed benefits included increased hand grip strength (14), preservation of daily functioning assessed via ADL (21), and increased nutrition and adherence to healthy diet habits (16, 18).
Psychosocial well being
Six out of twelve studies assessed the effects of multi-intervention training on psychosocial well-being (12–16, 18). Several aspects of this domain were investigated: self-efficacy and morale (12), mood (12, 13, 15), quality of life perception (14–16, 18), engagement in social and leisure activities (15). Most of the studies reported beneficial effects of multidomain interventions on psychosocial well-being (12, 13, 15, 16, 18), whereas only one study (14) showed no significant benefits.
In the study by Scult et al. (11), the researchers evaluated the effect of a healthy aging program for older adults on self-efficacy and morale. The Mind Body Intervention consisted of weekly, 90-min sessions for 9 consecutive weeks, directed by a psychologist. The program included sessions that taught participants: (1) a variety of methods to elicit the relaxation response, (2) the practice of adaptive coping and cognitions, (3) behaviors necessary to create a healthy lifestyle, and (4) methods of building social support. Significant increases in self-efficacy and morale were observed for program completers. In the study by Clare et al. (13), the goal-setting approach was associated with decreased depression scores, whilst changes in self-efficacy among groups were negligible.
Effects of multidimensional interventions on quality-of-life improvement were largely confirmed; in the study by Barreto et al. (14), HRQoL was the only dimension to improve in patients belonging to IG compared to CG; similarly, Rainero et al. (16) showed the effects of multidimensional interventions in preserving quality of life of pre-frail older adults after 12 months of follow-up; additionally, active participants showed an increase in mood during the follow-up period; furthermore, Huguet et al. (18) demonstrated a net improvement in quality of life perception among participants undergoing a 6-month four-dimensional intervention.
The secondary analysis of the MAPT study was conducted by de Souto Barreto et al. (20) to investigate whether a long-term (3-years) multi-domain lifestyle intervention was associated with the severity and incidence of frailty in older adults. Authors recruited 1,637 older people divided in 821 controls and 816 who received a multi-domain lifestyle intervention (cognitive training, nutrition counseling, and advice on physical activity). The intervention involved 12 2-h sessions (in the first 2 months) followed by a 1-h session each month until the study end. Controls received the usual care but did not receive any personalized lifestyle intervention. The 4 outcomes were severity of frailty (continuous FI score), incident frailty, incidence of persistent frailty (frailty at 2 consecutive time points), and reversibility of frailty (from frailty to no-frailty). Compared with controls, subjects in the multi-domain group had a decreased risk of developing both frailty and persistent frailty.
Another important study aimed to investigate the effect of multi-domain lifestyle intervention on daily functioning of older people is the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) conducted by Kulmala et al. In their first publication (21) they analyzed, for 2 years, a total of 1,260 older adults who were at risk of cognitive decline. The multi-domain intervention included simultaneous physical activity intervention, nutritional counseling, vascular risk monitoring and management, and cognitive training and social activity. During the 2-year intervention, the activity of daily living disability score slightly increased in the control group, while in the intervention group, it remained relatively stable. In terms of physical performance, the intervention group had a slightly higher probability of improvement and a lower probability of decline for chair rise compared to the control group.
The same data have been used by Lehtisalo et al. (22) to evaluate the effect of dietary changes adopted in older age. Adherence to healthy diet at baseline predicted improvement in global cognition, regardless of intervention allocation. Dietary improvement was associated with beneficial changes in executive function, especially in the intervention group.
Discussion
In the past, the study of aging process was strongly focused on health deficits (8), such as diseases, disabilities, and limitations; this view was supported by the strong relationship between increase in socio-economic burden on healthcare systems world-wide and the increase in prevalence of multimorbidity and disability among populations with high life expectancy. Despite the relevance of this model, aging should be investigated more broadly, since absence of diseases does not always go hand-in-hand with aging well. Rather than considering healthy aging from the disease-based perspective, the functioning-based approach promoted by WHO is oriented around building and maintaining the ability of older people to be and to do the things they have reason to value (4).
The availability of evidence on multi-domain interventions that include the IC framework is of paramount relevance for the health professionals, as they may provide them useful personalized strategies, to support the older patients’ resilience and autonomy in daily life, and can be easily integrated with more traditional therapies and treatments. From the analysis of the selected multi-domain interventions, there are important considerations that can be taken into account.
First of all, the majority of successful interventions are based on a goal setting approach (24, 25): the older people are involved in the definition of the strategies to follow to remain active and independent. The wellbeing of the elderly does not necessarily fit the intervention goals derived from the prevention perspective of the researcher. It is very important to include the elderly themselves in the goal-setting process, as they prefer to set goals to achieve well-being that are more focused on the process of adaptation to any functional loss (26). However, a balance between personalization and clinical effectiveness should be reached in agreement with the participants, before the testing phase, in order to find a minimum core of standardized strategies to complement the personalized approach. This may allow the comparability and replicability of the intervention, in addition to assure the adherence and the compliance of the older people.
Despite the undeniable wealth of the IC framework, none of the study have used this to design the intervention, but only to assess the improvement in IC domains. From the analysis of the studies, Physical Activity is the domain that has been received the most of the attention, including specific multicomponent interventions to improve different functional capabilities such as aerobics, muscle strength, balance and gait, while Psychological support has been addressed mostly as counseling activity through pre-selected contents instead of a more patient-centered approach. How to include sensory domain still represents an open topic for the studies in the field. Within the clinical outcomes, moreover, self-efficacy and goal attainment should be considered as important psychosocial determinants to be assessed after any multi-domain intervention previous studies have shown that self-efficacy and social support in older women enhances adherence to strength-training programs (27). In the meta-analysis, barrier self-efficacy was involved in the maintenance of exercise behavior (28). Those competences, in fact, are drivers for the improvement of the health status, as well as for IC and functional ability maintenance (29). They also constitute the basis for the adoption of healthy lifestyles, assuring the sustainability of positive behaviors in the long-term (30). Nevertheless, an assessment tool to identify improvement of Intrinsic Capacity as a whole, not only as sum of domains, is still missing.
In order to be effective, any intervention should be adapted to the older people, easily accessible and integrated into the everyday life (31). At this purpose, the field of coaching through technology is receiving more and more interest, as effective strategies to provide patient-centered multicomponent healthcare interventions integrated with technology to foster self-management, prevention, adherence to treatments, positive health outcomes, and resilience, all factors that improve the IC (32). Therefore, the relevance of this study stands also in the way to identify the existing research trends and possible gaps that need to be applied in the near future when designing technology-based interventions. Indeed, all the aforementioned key strategies (i.e., the goal set-ting approach, the involvement of older adults in the definition of the strategy to follow to remain active and independent, etc.), could be seen as interconnectors between the field of technologies and the IC.
Despite this positive aspect, there are some limitations to this review. Firstly, data sources were drawn from specific databases (i.e., PubMed, Scopus, Embase, Google Scholar and Elsevier). The choice of using specific search terms could have omitted some results from the search. Moreover, we collected a relatively small sample of studies and excluded non-English language studies. It could be possible that other literary sources were available in other unselected databases or in other languages. Another possible limitation is the average age of the patients included in the studies analyzed, which is rather low and refers to an audience of young old people. Therefore, the conclusions we reached cannot be transferred to the entire elderly population. Moreover, results obtained should be interpreted with caution because some studies included in the review were reported as being built with low methodological quality. Despite these limitations, our study offers several research directions, which may take the existing debates to the next level.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author/s.
Author contributions
EM and RB: study concept and design. EM, RB, SC, and ET: acquisition of data (literature search and study selection). EM, RB, LS, and ET: analysis and interpretation of data (literature). EM, RB, LS, and VS: writing—original draft preparation. FL, GR, AC, and GP: critical revision of the manuscript for important intellectual content. JM, RW, TO, SW, KK, and IK: supervision. JM and TO: writing—review and editing. All authors contributed to the article and approved the submitted version.
Funding
This research is based on data collected for the “EU-Japan Virtual Coach for Smart Aging - e-Vita” project, funded from the European Union H2020 Program under grant agreement no. 101016453 and the Japanese Ministry of Internal Affairs and Communication (MIC), Grant no. JPJ000595.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Beard JR, Officer A, de Carvalho IA, Sadana R, Pot AM, Michel JP, et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet. (2016) 387:2145–54. doi: 10.1016/S0140-6736(15)00516-4
2. Gutiérrez-Robledo LM, García-Chanes RE, Pérez-Zepeda MU. Allostatic load as a biological substrate to intrinsic capac-ity: a secondary analysis of CRELES. J Nutr Health Aging. (2019) 23:788-95. doi: 10.1007/s12603-019-1251-5
3. Low LF, Yap M, Brodaty H. A systematic review of different models of home and community care services for older per-sons. BMC Health Serv Res. (2011) 11:93.
4. Rudnicka E, Napierała P, Podfigurna A, Mêczekalski B, Smolarczyk R, Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. (2020) 139:6-11.
5. Althoff T, Sosič R, Hicks JL, King AC, Delp SL, Leskovec J. Large-scale physical activity data reveal worldwide activity inequality. Nature. (2017) 547:336-9. doi: 10.1038/nature23018
6. Gonzalez-Bautista E, Andrieu S, Gutiérrez-Robledo LM, García-Chanes RE, De Souto Barreto P. In the quest of a standard index of intrinsic capacity. a critical literature review. J. Nutr. Health Aging. (2020) 24:959–65. doi: 10.1007/s12603-020-1394-4
7. Ma L, Chhetri JK, Zhang L, Sun F, Li Y, Tang Z. Cross-sectional study examining the status of intrinsic capacity de-cline in community-dwelling older adults in China: prevalence, associated factors and implications for clinical care. BMJ Open. (2021) 11:e043062. doi: 10.1136/bmjopen-2020-043062
8. Belloni G, Cesari M. Frailty and Intrinsic Capacity: Two Distinct but Related Constructs. Front Med. (2019) 6:133. doi: 10.3389/fmed.2019.00133
9. Abdullahi AM, Orji R, Rabiu A, Abubakar Kawu A. Personality and subjective well-being: towards personalized per-suasive interventions for health and well-being. Online J. Public Health Inform. (2020) 12:1–24.
10. Dedeyne L, Deschodt M, Verschueren S, Tournoy J, Gielen E. Effects of multi-domain interventions in (pre)frail elderly on frailty, functional, and cognitive status: a systematic review. Clin Interv Aging. (2017) 12:873–96. doi: 10.2147/CIA.S130794
11. Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Antikainen R, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a ran-domised controlled trial. Lancet. (2015) 385:2255–63. doi: 10.1016/S0140-6736(15)60461-5
12. Scult M, Haime V, Jacquart J, Takahashi J, Moscowitz B, Webster A, et al. A healthy aging program for older adults: effects on self-efficacy and morale. Adv Mind Body Med. (2015) 29:26–33.
13. Clare L, Nelis SM, Jones IR, Hindle JV, Thom JM, Nixon JA, et al. The Agewell trial: a pilot randomised controlled trial of a behaviour change intervention to promote healthy ageing and reduce risk of dementia in later life. BMC Psychiatry. (2015) 15:25. doi: 10.1186/s12888-015-0402-4
14. Ng PEM, Nicholas SO, Wee SL, Yau TY, Chan A, Chng I, et al. Implementation and effectiveness of a multi-domain program for older adults at risk of cognitive impairment at neighborhood centres. Sci Rep. (2021) 11:3787. doi: 10.1038/s41598-021-83408-5
15. de Souto Barreto P, Pothier K, Soriano G, Lussier M, Bherer L, Guyonnet S, et al. Web-Based multidomain lifestyle intervention for older adults: the emind randomized controlled trial. J Prev Alzheimers Dis. (2021) 8:142–50.
16. Rainero I, Summers MJ, Monter M, Bazzani M, Giannouli E, Aumayr G, et al. The my active and healthy aging ICT platform prevents quality of life decline in older adults: a randomised controlled study. Age Ageing. (2021) 50:1261–7. doi: 10.1093/ageing/afaa290
17. Moon SY, Hong CH, Jeong JH, Park YK, Na HR, Song HS, et al. Facili-ty-based and home-based multidomain interventions including cognitive training, exercise, diet, vascular risk management, and motivation for older adults: a randomized controlled feasibility trial. Aging. (2021) 13:15898–916. doi: 10.18632/aging.203213
18. Gené Huguet L, Navarro González M, Kostov B, Ortega Carmona M, Colungo Francia C, Carpallo Nieto M, et al. Pre Frail 80: multifactorial intervention to prevent pro-gression of pre-frailty to frailty in the elderly. J Nutr Health Aging. (2018) 22:1266–74. doi: 10.1007/s12603-018-1089-2
19. Tabue-Teguo M, Barreto de Souza P, Cantet C, Andrieu S, Simo N, Fougère B, et al. Effect of mul-tidomain intervention, omega-3 polyunsaturated fatty acids supplementation or their combinaison on cognitive function in non-demented older adults according to frail status: results from the mapt study. J Nutr Health Aging. (2018) 22:923–7.
20. de Souto Barreto P, Rolland Y, Maltais M, Vellas B, Mapt Study Group. Associations of multidomain lifestyle interven-tion with frailty: secondary analysis of a randomized controlled trial. Am J Med. (2018) 131:.e7–1382. doi: 10.1016/j.amjmed.2018.06.002
21. Kulmala J, Ngandu T, Havulinna S, Levälahti E, Lehtisalo J, Solomon A, et al. The effect of multidomain lifestyle intervention on daily functioning in older people. J Am Geriatr Soc. (2019) 67:1138–44.
22. Lehtisalo J, Levälahti E, Lindström J, Hänninen T, Paajanen T, Peltonen M, et al. Dietary changes and cognition over 2 years within a mul-tidomain intervention trial-the finnish geriatric intervention study to prevent cognitive impairment and disability (FIN-GER). Alzheimers Dement. (2019) 15:410–7. doi: 10.1016/j.jalz.2018.10.001
23. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) 83:713–21.
24. Vermunt NPCA, Harmsen M, Westert GP, Olde Rikkert MGM, Faber MJ. Collaborative goal setting with elderly patients with chronic disease or multimorbidity: a systematic review. BMC Geriatr. (2017) 17:167.
25. Alanko T, Karhula M, Kröger T, Piirainen A, Nikander R. Rehabilitees perspective on goal setting in rehabilitation - a phe-nomenological approach. Disabil Rehabil. (2019) 41:2280–8.
26. Kusumastuti S, Derks MG, Tellier S, Di Nucci E, Lund R, Mortensen EL, et al. Successful ageing: a study of the literature using citation network analysis. Maturitas. (2016) 93:4–12. doi: 10.1016/j.maturitas.2016.04.010
27. Rhodes RE, Martin AD, Taunton JE. Temporal relationships of self-efficacy and social support as predictors of adherence in a 6-month strength-training program for older women. Percept. Mot. Skills. (2001) 93:693–703. doi: 10.2466/pms.2001.93.3.693
28. Higgins TJ, Middleton KR, Winner L, Janelle CM. Physical activity interventions differentially affect exercise task and barrier self-efficacy: a meta-analysis. Health Psychol. (2014) 33:891–903. doi: 10.1037/a0033864
29. Liu S, Kang L, Liu X, Zhao S, Wang X, Li J, et al. Trajectory and correlation of intrinsic capacity and frailty in a beijing elderly community. Front Med (Lausanne). (2021) 8:751586. doi: 10.3389/fmed.2021.751586
30. Fourteau M, Virecoulon Giudici K, Rolland Y, Vellas B, de Souto Barreto P. Associations between multidomain lifestyle inter-ventions and intrinsic capacity domains during aging: a narrative review. J Aging Res Lifestyle. (2020) 9:16–25.
31. Hestevik CH, Molin M, Debesay J, Bergland A, Bye A. Older persons’ experiences of adapting to daily life at home after hos-pital discharge: a qualitative metasummary. BMC Health Serv Res. (2019) 19:224. doi: 10.1186/s12913-019-4035-z
Keywords: intrinsic capacity, active and healthy aging, functional ability, geriatrics, cognitive support, psychological support, multidomain, multicomponent intervention
Citation: Bevilacqua R, Soraci L, Stara V, Riccardi GR, Corsonello A, Pelliccioni G, Lattanzio F, Casaccia S, Möller J, Wieching R, Ogawa T, Watanabe S, Kokobun K, Kondo I, Takano E and Maranesi E (2022) A systematic review of multidomain and lifestyle interventions to support the intrinsic capacity of the older population. Front. Med. 9:929261. doi: 10.3389/fmed.2022.929261
Received: 26 April 2022; Accepted: 28 June 2022;
Published: 15 July 2022.
Edited by:
Marios Kyriazis, National Gerontology Center, CyprusReviewed by:
Fahadul Islam, Daffodil International University, BangladeshSandra Oliveira, Fiocruz Mato Grosso do Sul, Brazil
Copyright © 2022 Bevilacqua, Soraci, Stara, Riccardi, Corsonello, Pelliccioni, Lattanzio, Casaccia, Möller, Wieching, Ogawa, Watanabe, Kokobun, Kondo, Takano and Maranesi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberta Bevilacqua, ci5iZXZpbGFjcXVhQGlucmNhLml0