 Guang Yang1†
Guang Yang1† Lin-yuan Pan
Lin-yuan Pan- 1Department of Anesthesiology, Xi'an Honghui Hospital Affiliated to Xi'an Jiaotong University, Xi'An, China
- 2Department of Orthopaedics, Xiangya Hospital, Central South University, Changsha, Hunan, China
- 3Department of Anesthesiology, Northwest Women's and Children's Hospital, Xi'An, China
- 4Department of Orthopaedics, Xi'an Honghui Hospital Affiliated to Xi'an Jiaotong University, Xi'An, China
Purpose: Our purpose was to assess job stress and burnout among anesthesiologists in the tertiary class A hospitals in Northwest China, analyze the possible causes and adverse consequences of increased job stress and burnout of anesthesiologists in this region, and put forward suggestions in combination with the current national policies.
Methods: We sent 500 electronic questionnaires to all anesthesiologists practicing in the tertiary class A hospitals in Northwest China from 1960 to 2017 on April 2020. A total of 336 (67.2%) questionnaires were returned and could be used for analysis. Burnout and job stress were assessed by using the modified Maslach Burnout Inventory—Human Services Survey and Chinese Perceived Stress Scale, respectively.
Results: First, as for emotional exhaustion, the situations of anesthesiologists with different working years and workloads are different with statistical significance (P < 0.05). Second, as for depersonalization, the situations of anesthesiologists with different ages, professional titles, working years, physical health status, and workload are different (P < 0.05). Third, as for personal accomplishment, the situations of anesthesiologists with different physical health status are different (P < 0.05). Finally, the regression results showed that the longer the fatigue working years and the worse the physical health of anesthesiologists in Northwest China, the more likely these two factors were to cause burnout (P < 0.05), as for job stress, there was a negative correlation between job stress and physical health status (P < 0.05).
Conclusion: Burnout and high job pressure are common among anesthesiologists in tertiary class A hospitals in Northwest China. We should focus on the allocation of labor intensity, pay attention to the physical and mental health of employees, establish targeted incentive mechanism, and improve the system of promotion and income rises for grassroots doctors. This may be not only conducive to the quality of medical care for patients but also conducive to the development of anesthesiology in China.
Trial registration: Identifier: ChiCTR2000031316.
Introduction
Burnout is a comprehensive symptom of physical and mental exhaustion and energy exhaustion, which includes emotional exhaustion, depersonalization, and reduced personal accomplishment (1). Job pressure refers to the pressure on people due to excessive workload, change of post, and excessive work responsibility (2).
An Italian study in 2020 assessed burnout among anesthesiologists and intensivists and showed that 79.9% (686) exhibited moderate levels of burnout (3). A cross-sectional study in Kosovo surveyed 154 anesthesiologists and anesthesia technicians in Kosovo and found that approximately one-third of Kosovar anesthesiologists and anesthesia technicians exhibited high levels of burnout (4). A U.S. study included 3,898 members of the American Society of Anesthesiologists and showed that 59.2% of the study subjects were at high risk of burnout (5). Numerous similar studies have shown a high risk of burnout in the group of anesthesiologists. As the world's most populous country, medical resources are relatively more scarce in China.
In China, the number of anesthesiologists per 10,000 population is only 0.4, far lower than the number of anesthesiologists per 10,000 population in developed countries in Europe and America (6). With the aging of the population in our country and increasing serious perioperative complications, the anesthesia risk is also increasing day by day. At the same time, the shortage of anesthesiologists and the uneven distribution of medical resources lead to increased job stress and burnout of anesthesiologists, which will not only affect the physical and mental health of anesthesiologists but also bring hidden dangers to the safety and quality of anesthesia (7).
Some studies have shown that the level of burnout in other occupations is related to the knowledge gap, for example, working sailors (8) and nurses in the operating room (9). There was also a knowledge gap in the level of burnout among frontline physicians in Bangladesh during the COVID-19 pandemic (10).
In Northwest China, the economy is relatively backward, the distribution of medical resources is unbalanced, and the level of medical and health services lags behind other regions (11). Therefore, to fully mobilize the enthusiasm of the medical staff, improve the level of medical services, and fully understand both the advantages and disadvantages of medical resources in this region is important for promoting the development of medical services. Thus, in this study, 500 anesthesiologists' job stress and burnout were investigated and analyzed in order to provide a reference for instructing anesthesiologists to relieve the pressure and improve the level of burnout.
Methods
The Research Ethics Committee of Xi'an Honghui Hospital affiliated with Xi'an Jiaotong University (Chairperson: Peng Xu) approved the study on 9 April 2020, and written informed consent from patients was obtained.
This article adheres to the applicable Enhancing the QUAlity and Transparency of Health Research (EQUATOR) guidelines.
Using a random sampling method, an anonymous cross-sectional design was conducted among anesthesiologists in the tertiary class A hospitals in Northwest China. For sample size estimation, a pilot study of 167 cases before the survey indicated a burnout rate of 48%. We assumed that a 5% error was acceptable and then the confidence level was set at 95%. By considering the response rate, the sample size was 308. Based on this, a total of 500 questionnaires were sent out, of which 408 were recovered and 336 were effective. Thus, among the returned questionnaires, the effective rate was 82.4%.
First section
The first section of the questionnaire included 11 questions designed to capture demographic, social, and work characteristics of the anesthesiologists, such as gender, age, educational background, professional title, working years, family economic status, physical health status, type of hospital, proportion of anesthesiologists in your department to the operating room, ratio of anesthesiologists to surgeons, and operation volume in recent 2 years.
Second section
Burnout: The modified Maslach Burnout Inventory—Human Service Survey (MBI-HSS) (12) was used to assess burnout. The modified Maslach Burnout Inventory—Human Service Survey is widely used to assess burnout in healthcare workers. Research has shown that the Maslach Burnout Inventory—Human Service Survey has acceptable validity and reliability in measuring nurse burnout and can help healthcare administrators provide interventions to reduce nurse burnout (13). The measurement invariance of the MBI-HSS in gender and occupation was also confirmed in a Vietnamese study (14). The 16-item MBI is a measure of burnout and is subdivided into three subscales as follows: (a) Emotional exhaustion (six items): This subscale refers to a lack of emotional resources, that is, the feeling of having given everything and having nothing left to give. (b) Lack of personal accomplishment (six items): This subscale assesses feelings of doubt about one's ability to perform tasks and lack of successful achievement in one's work with people. (c) Depersonalization (four items): This subscale measures an unfeeling and impersonal response toward recipients of one's service, care, treatment, or instruction. The scoring method of four points was used, never so scored 0 points, rarely so scored 1 point, sometimes so scored 2 points, and often so scored 3 points. In the subscale of “emotional exhaustion”, values ≥19 are considered to indicate burnout; in the subscale of “personal accomplishment”, values ≤ 2.5 are considered to indicate burnout; and in the “depersonalization” subscale, values ≥17 are considered to indicate burnout.
Third section
Job stress: The work stress of anesthesiologists was evaluated by the Chinese Perceived Stress Scale (CPSS) (15). The CPSS is a reliable and valid instrument for patients with common mental disorders with different employment status, exhibiting a stable two-factor structure with satisfactory internal consistency and construct validity (16, 17).
There were 14 items in CPSS, which had never scored 0, rarely scored 0.5, sometimes scored 1, and often scored 1.5. It was conceived to assess how many life situations are appraised as stressful, that is, how unpredictable and overloaded respondents find their lives. Higher scores indicate higher levels of job stress. At the end of the questionnaire, an open question was included for respondents to identify the main job stress factors encountered in their daily lives. The seven most frequently referred factors were identified.
Procedures
The electronic version of the questionnaire was built on the Wenjuanxing platform (https://www.wjx.cn). WeChat publishing is a widely used mobile social platform that attracts a broad range of users in China. As of September 2015, WeChat had more than a billion created accounts and 650 million active users. Throughout the nation, the coverage of WeChat has more than 90% of smartphone users (18). It is considered a valid questionnaire if it is collected within 3 days, and the time for filling in the questionnaire is not < 15 min.
Statistical analysis
Data were analyzed using the SPSS software package (Released 2017. IBM SPSS Statistics for Mac, version 25.0. Armonk, NY: IBM Corp.). The descriptive analysis uses the number and percentage of cases to describe the general data (such as gender, age, educational background, and professional title), makes an independent sample t-test on the scores of burnout and job stress of anesthesiologists of different gender, and makes one-way ANOVA on the situation of burnout and job stress of anesthesiologists of different age, professional title, education background, etc., among which, in one-way ANOVA, the variables with P < 0.15 were included in the multivariate analysis, the entry and removal criteria of multiple linear regression were 0.10 and 0.15, respectively. The multiple linear regression model was used to evaluate the independent correlation between the included variables, such as job stress and burnout. A two-tailed P < 0.05 was considered statistically significant.
Results
The questionnaire was distributed and collected on April 2020. Of the 32 tertiary class A hospitals (there are 32 tertiary class A hospitals in three Northwest provinces) and 500 anesthesiologists and anesthesia residents, 32 hospitals and 336 individuals completed the survey (response rates 100% and 82.4%, respectively). The descriptive statistics are shown in Table 1.
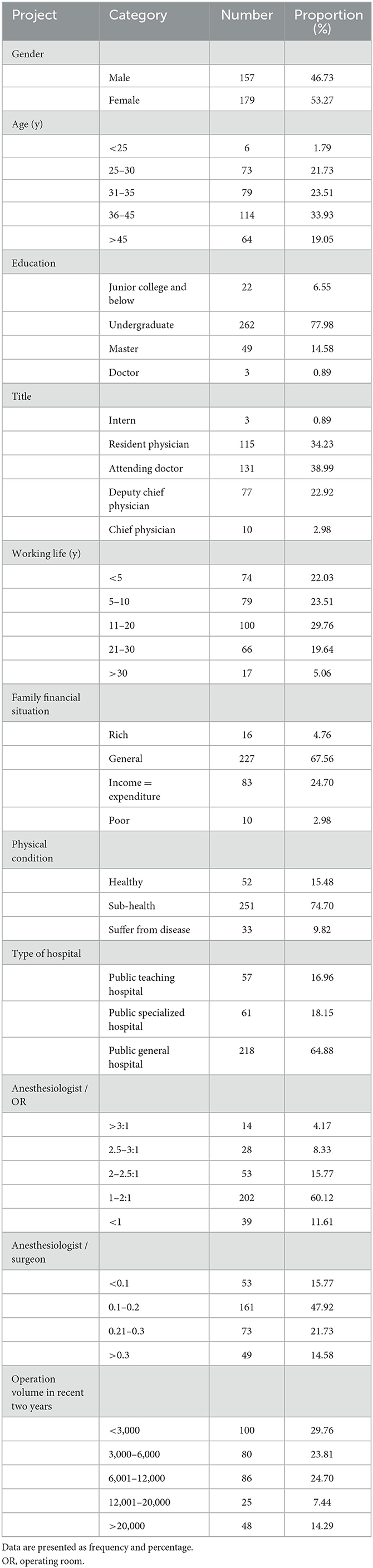
Table 1. Descriptive statistics of the survey (n = 336).
In Northwest China, the economy is relatively backward, the distribution of medical resources is unbalanced, and the level of medical and health services lags behind other regions (11).
The results of the burnout analysis showed that the scores of emotional exhaustion, depersonalization, and personal accomplishment were 20.23 ± 3.515, 17.98 ± 2.310, and 2.43 ± 0.670, respectively. 1. The emotional exhaustion of anesthesiologists with different working years and workloads was different, and the difference was statistically significant (P < 0.05); 2. The depersonalization of anesthesiologists with different ages, titles, working years, physical conditions, and workloads was different, and the difference was statistically significant (P < 0.05); and 3. The personal accomplishment of anesthesiologists with different physical conditions was different, and the difference was statistically significant (P < 0.05) (Table 2).
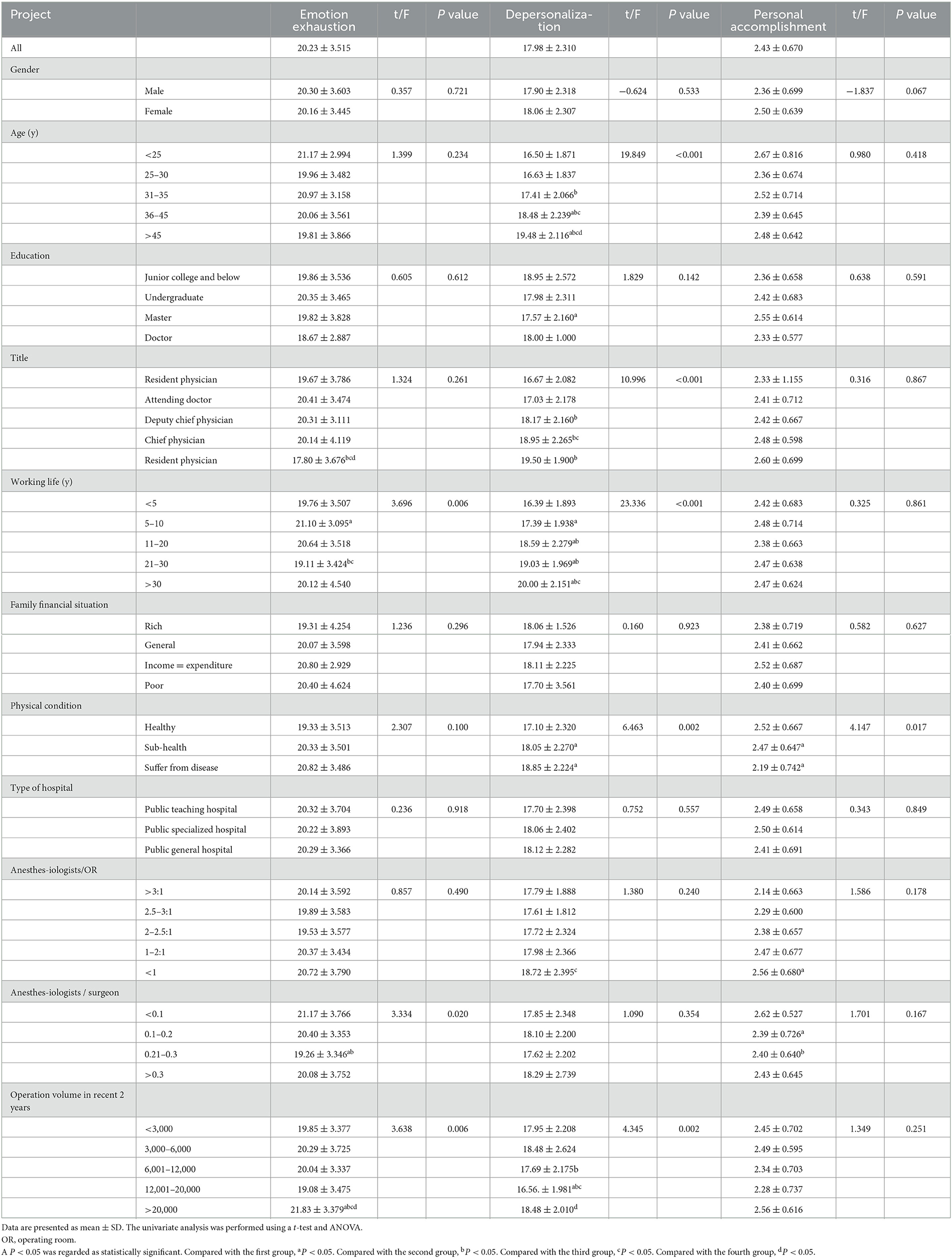
Table 2. Score of burnout ( ± s).
Analysis of job stress: anesthesiologists with different physical health statuses and workloads had different job stress, and the difference was statistically significant (P < 0.05) (Table 3).
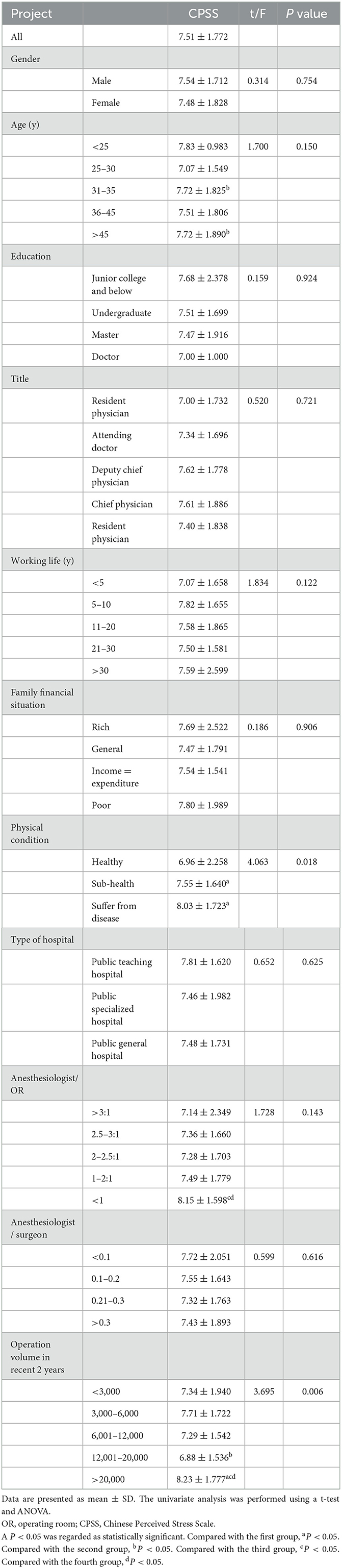
Table 3. Score of job stress (s).
Correlation analysis of influencing factors of anesthesiologists' burnout: the longer the anesthesiologists' working life, the worse the health status and the more serious the depersonalization, and the difference was statistically significant (P < 0.05). The better the anesthesiologists' physical condition, the longer the working life and the higher the sense of personal accomplishment. The difference was statistically significant (P < 0.05) (Tables 4–6).
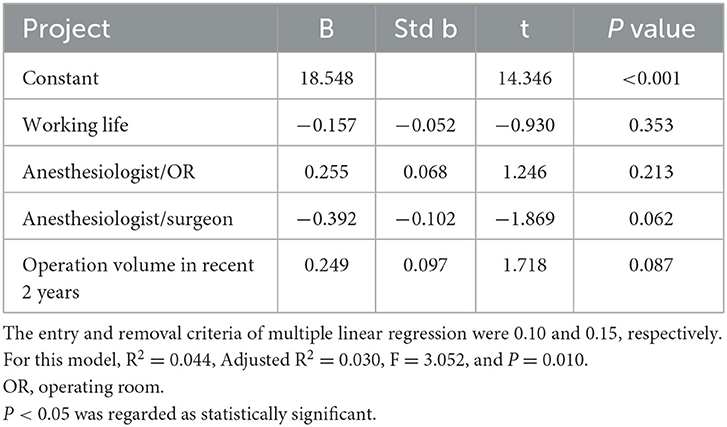
Table 4. Results of multiple linear regression of emotional exhaustion.
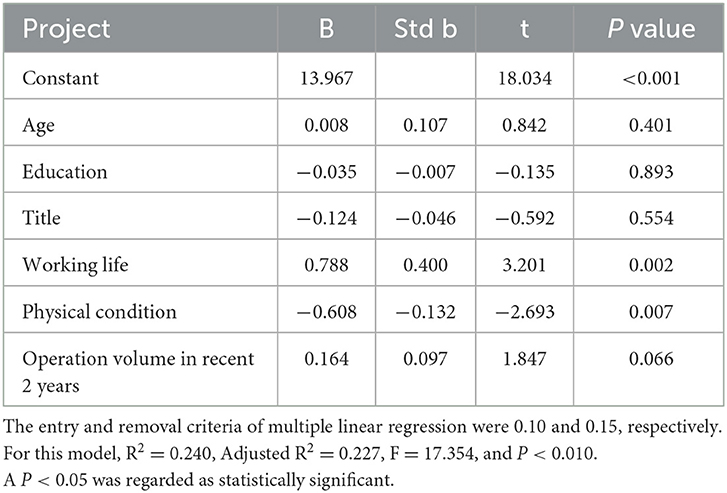
Table 5. Results of multiple linear regression of depersonalization.
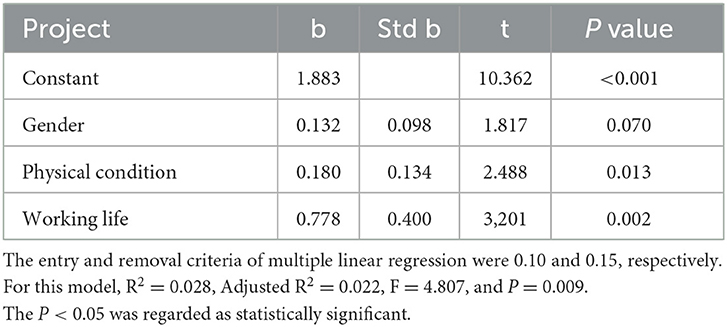
Table 6. Results of multiple linear regression of personal accomplishment.
Correlation analysis of influencing factors of job stress of anesthesiologists: the better the physical health condition of anesthesiologists, the less the job pressure, and the difference was statistically significant (P < 0.05) (Table 7).
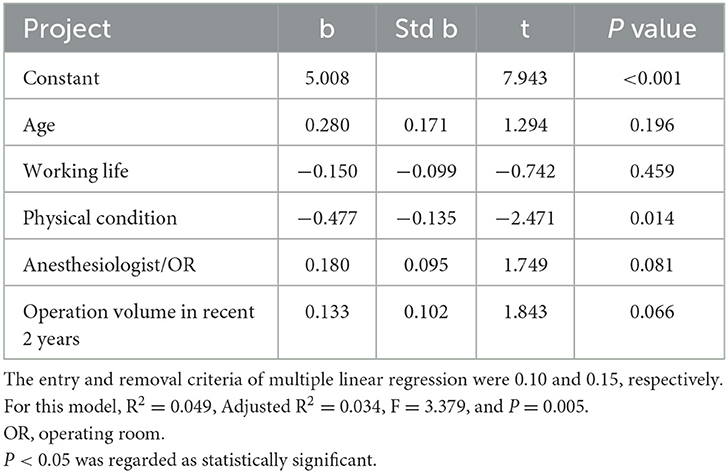
Table 7. Results of multiple linear regression of personal accomplishment job stress.
Discussion
This study assesses both burnout and job stress among anesthesiologists and provides a good understanding of the current psychological status of anesthesiologists among all colleagues and related personnel in the anesthesia industry. Using Northwest China as the background of the study is relevant and can cause the relevant departments to care for anesthesiologists in Northwest China and incline resources. However, this study also has limitations. For example, the sample size was limited. We distributed 500 questionnaires, yet only 406 were returned, of which only 336 were valid, which may have led to selection bias in the study results. In further research studies in the future, we can expand the sample size, keep in touch with the study participants after distributing the questionnaire, and supervise them to complete the questionnaire to reduce selective bias.
The medical and health industry is a profession with high requirements and a low sense of control, and a profession with a high incidence of burnout (19). At present, there are 76,000 anesthesiologists in China. The number of anesthesiologists per 10,000 people in China is ~0.4, compared with three in the United States and 2.8 in the United Kingdom. According to British and American standards, China should have 310,000 anesthesiologists. In fact, the total number of anesthesiologists in China is < 100,000 and also less than one-third of the standard configuration, and the gap is 200,000 (20). At the same time, China's surgery volume accounts for approximately 10% of the global surgery volume, and it is still growing at a rate of 10% (21). In recent years, the doctor–patient relationship has become increasingly tense, coupled with factors such as the income, promotion, and physical condition of anesthesiologists, which make the environment of anesthesiologists worse, thus, job stress and burnout are increasing day by day (22).
As for emotional exhaustion, the phenomenon of emotional exhaustion with working years of 5–10 years is serious. Most anesthesiologists who have worked for 5–10 years have accumulated professional knowledge and skills and can play an independent role at work. In hospitals at all levels, they are the main force of their department. Therefore, their emotional exhaustion is severe, which is consistent with the research results of Filippo (23). With the increase in working years, the phenomenon of emotional exhaustion began to ease. This may be explained by the fact that, with the continuous increase of working years, their medical experience continues to be accumulated, and technical literacy is more and more suitable for the needs of the post, and then, the burnout will reduce. The higher the annual operation volume is, the more serious the emotional exhaustion is. The increase in workload will directly lead to the excessive fatigue of anesthesiologists. Excessive fatigue not only affects the physical and mental health of anesthesiologists but also causes great potential harm to patients. In the study of Gordon (24), it was found that as many as 50% of the anesthesiologists interviewed admitted that they had medical errors when they were tired.
With the increase in age, working years, and professional titles of anesthesiologists, their depersonalization is more and more serious. With the increasing age and working years of an anesthesiologist, the accumulated fatigue, work pressure, dissatisfaction, and sub-health will reach a peak, which makes the phenomenon of depersonalization more serious. The phenomenon is manifested in negative work and indifference to colleagues. From the correlation analysis, it is found that the length of working years is positively related to the occurrence of depersonalization, while the health status is negatively related to the occurrence of depersonalization, and the difference is statistically significant. Therefore, the relevant departments should pay attention to the physical and mental health of anesthesiologists, which will help to delay depersonalization and improve burnout (25).
In Northwest China, the better an anesthesiologist's health is, the higher his accomplishment will be. In Northwest China, the economy is underdeveloped, and the medical level is relatively backward. People are still in the dilemma of difficult and expensive medical treatment (26). Novel coronavirus pneumonia (COVID-19) has been prevalent worldwide in 2020, which has caused millions of people to die. The number of deaths has reached 60,000, and the number of infections and deaths is rising (27, 28). This makes us more convinced that nothing matters except for a healthy body. A healthy body can bring more sense of personal achievement to anesthesiologists in Northwest China. There was a positive correlation between personal accomplishment, physical health, and working years, and the difference was statistically significant. With the accumulation of working years, the academic level, experience and technology, and salary and income of anesthesiologists will reach a new level, and the sense of personal accomplishment will naturally increase. Coupled with a healthy body, a great sense of personal accomplishment can often be obtained, reducing the occurrence of burnout.
In total, 88.1% of anesthesiologists in this questionnaire had high job stress, among whom the greater the workload, the worse the physical health, and the higher the job stress of anesthesiologists, and the difference was statistically significant. In the correlation analysis, job stress was negatively correlated with physical health, and the difference was statistically significant. The aforementioned shortage of anesthesiologists in China and the increasing workload lead to the physical and mental fatigue of medical staff and the sudden rise of pressure (29). In addition, the sudden death rate of anesthesiologists is increasing year by year. According to the researchers such as Shan, the proportion of sudden death of anesthesiologists in China is the highest, reaching 26% (30). As for the reasons of excessive workload, worry about medical litigation, sleep deprivation, and interpersonal relationship processing, anesthesiologists will often be in a certain degree of physiological or psychological disease states (31), and anesthesiologists in a sick state will naturally feel the job stress increase at work. Therefore, the healthy body and mind of an anesthesiologist are the premise and guarantee of his normal work.
In conclusion, burnout and high job pressure are common among anesthesiologists in Northwest China. The increasing workload, unfair promotion system, and long-term sub-health lead to a decline in their physical health. In terms of anesthesiologists themselves, they should improve their psychological quality, maintain their mental health, constantly enrich and improve their professional level, and improve the communication ability between doctors and patients (32). For the department leaders and the health administrative departments, we should first reduce the risk of occupational exposure of anesthesiologists, then adjust the overall allocation of resources in the hospital, pay attention to the improvement and renewal of medical equipment, and more importantly, ensure the fairness and impartiality of the salary and promotion system, strengthen the overall input and construction of the anesthesiology department, and strive to establish contact with the international community soon (33). Only when we pay attention to the problems of anesthesiologists, we can guarantee the safety and service quality of patients in the northwest region and even in the whole country, and anesthesiologists in China can make great progress (34).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Research Ethics Committee, Xi'an Honghui Hospital Affiliated to Xi'an Jiaotong University. The patients/participants provided their written informed consent to participate in this study.
Author contributions
J-mY: conceptualization. GY: writing—original draft preparation. L-yP: writing—reviewing and editing. B-hD: methodology. X-lF: software. ZQ: visualization. All authors have read and agreed to the published version of the manuscript.
Acknowledgments
The authors thank the anesthesiologists who participated in the study for their help and support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Durham M, Bush P, Ball A. Evidence of burnout in health-system pharmacists. Am J Health Syst Pharm. (2018) 75:S93–S100. doi: 10.2146/ajhp170818
2. Chirico F. Job stress models for predicting burnout syndrome: a review. Annali dell'Istituto superiore di sanita. (2016) 52:443–56. doi: 10.4415/ANN_16_03_17
3. Vargas M, Spinelli G, Buonanno P, Iacovazzo C, Servillo G, De Simone S. Burnout among anesthesiologists and intensive care physicians: results from an Italian National Survey. Inquiry. (2020) 57:46958020919263. doi: 10.1177/0046958020919263
4. Neziri S, Tahirbegolli B, Selmani E, Gallopeni F. Assessment of burnout levels among anesthesiologists and anesthesiology technicians in Kosovo: a cross-sectional study. Int J Risk Saf Med. (2022) 33:261–8. doi: 10.3233/JRS-200038
5. Afonso AM, Cadwell JB, Staffa SJ, Zurakowski D, Vinson AE. Burnout rate and risk factors among anesthesiologists in the United States. Anesthesiology. (2021) 134:683–96. doi: 10.1097/ALN.0000000000003722
6. Li Q, Han T, Zhang Y, Zhang Q, Kong X, Yang Y, et al. A nationwide survey on neonatal medical resources in mainland China: current status and future challenges. BMC Pediatr. (2019) 19:436. doi: 10.1186/s12887-019-1780-4
7. Lapa T, Madeira F, Viana J, Pinto-Gouveia J. Burnout syndrome and wellbeing in anesthesiologists: the importance of emotion regulation strategies. Minerva Anestesiol. (2017) 83:191–9. doi: 10.23736/S0375-9393.16.11379-3
8. Shi LC Dai JJ, Wang HR, Wang JL, Miao LQ, Yang LR. Current status of job burnout in in-service sailors from 13 provinces and cities in China. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. (2017) 35:893–7. doi: 10.3760/cma.j.issn.1001-9391.2017.12.003
9. Lv AQ, Sun CN, Liu X, Li WH. [tudy on the relationship between job stress, job burnout and turnover intention of nurses in the operating room of a provincial top three hospital. Zhonghua Lao Dong Wei Sheng Zhi Ye Bing Za Zhi. (2020) 38:577–80. doi: 10.3760/cma.j.cn1210942-20200203-000039
10. Rashid F, Erfan Uddin RAM, Mehedi HMH, Dhar S, Bhuiyan NH, Sattar MA, et al. Burnout syndrome among frontline doctors of secondary and tertiary care hospitals of Bangladesh during COVID-19 pandemic. PLoS ONE. (2022) 17:e0277875. doi: 10.1371/journal.pone.0277875
11. Cai H, Wang H, Guo T, Bao G. Application of Telemedicine in Gansu Province of China. PLoS ONE. (2016) 11:e0158026. doi: 10.1371/journal.pone.0158026
12. Maslach Burnout InventoryAvailable online at: https://www.mindgarden.com/117-maslach-burnout-inventory-mbi (accessed May 2, 2019).
13. Pisanti R, Lombardo C, Lucidi F, Violani C, Lazzari D. Psychometric properties of the Maslach Burnout Inventory for Human Services among Italian nurses: a test of alternative models. J Adv Nurs. (2013) 69:697–707. doi: 10.1111/j.1365-2648.2012.06114.x
14. Bui THT, Tran TMD, Nguyen TNT, Vu TC, Ngo XD, Nguyen THP, et al. Reassessing the most popularly suggested measurement models and measurement invariance of the Maslach Burnout Inventory - human service survey among Vietnamese healthcare professionals. Health Psychol Behav Med. (2022) 10:104–20. doi: 10.1080/21642850.2021.2019585
15. Lu W, Bian Q, Wang W, Wu X, Wang Z, Zhao M. Chinese version of the Perceived Stress Scale-10: a psychometric study in Chinese university students. PLoS ONE. (2017) 12:e0189543. doi: 10.1371/journal.pone.0189543
16. Ng SM. Validation of the 10-item Chinese perceived stress scale in elderly service workers: one-factor versus two-factor structure. BMC Psychol. (2013) 1:9. doi: 10.1186/2050-7283-1-9
17. Shih S, Chan A, Yeung E, Tsang A, Chiu R, Chu M, et al. Psychometric properties and correlates of Chinese version of Perceived Stress Scale (CPSS-10) in people with common mental disorders with different employment Statuses. Hong Kong J Occup Ther. (2021) 34:103–12. doi: 10.1177/15691861211032318
18. Montag C, Becker B, Gan C. The multipurpose application wechat: a review on recent research. Frontiers in psychology. (2018) 9:2247. doi: 10.3389/fpsyg.2018.02247
19. Lederer W, Paal P, von Langen D, Sanwald A, Traweger C, Kinzl J. Consolidation of working hours and work-life balance in anaesthesiologists—a cross-sectional national survey. PLoS One. (2018) 13:e0206050. doi: 10.1371/journal.pone.0206050
20. Li Z, Yang J, Wu Y, Pan Z, He X, Li B, et al. Challenges for the surgical capacity building of township hospitals among the Central China: a retrospective study. Int J Equity Health. (2018) 17:55. doi: 10.1186/s12939-018-0766-4
21. Lu J, Wang W, Cheng W, Chen L, Huang J, Ethridge C, et al. Current status of cardiovascular anesthesia in China. Anesth Analg. (2017) 125:1855–62. doi: 10.1213/ANE.0000000000002051
22. De Hert S. Burnout among anesthesiologists: it's time for action! J Cardiothorac Vasc Anesth. (2018) 32:2467–8. doi: 10.1053/j.jvca.2018.06.010
23. Sanfilippo F, Noto A, Foresta G, Santonocito C, Palumbo G, Arcadipane A, et al. Incidence and factors associated with burnout in anesthesiology: a systematic review. Biomed Res Int. (2017) 2017:8648925. doi: 10.1155/2017/8648925
24. Gordon P, Llewellyn R, James M. Drug administration errors by South African anaesthetists–a survey. S Afr Med J. (2006) 96:630–2. doi: 10.1080/22201173.2006.10872432
25. Katz J. The impaired and/or disabled anesthesiologist. Curr Opin Anaesthesiol. (2017) 30:217–22. doi: 10.1097/ACO.0000000000000423
26. Zeng C, Lane N, Englund M, Xie D, Chen H, Zhang Y, et al. In-hospital mortality after hip arthroplasty in China: analysis of a large national database. Bone Joint J. 2019:1209–17. doi: 10.1302/0301-620X.101B10.BJJ-2018-1608.R1
27. Velavan T, Meyer C. The COVID-19 epidemic. Trop Med Int Health. (2020) 25:278–80. doi: 10.1111/tmi.13383
28. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. (2020) 109:102433. doi: 10.1016/j.jaut.2020.102433
29. Saadat H, Kain Z. Wellness interventions for anesthesiologists. Curr Opin Anaesthesiol. (2018) 31:375–81. doi: 10.1097/ACO.0000000000000598
30. Zhang H, Li F, Lei H, Xu S. Rising sudden death among anaesthesiologists in China. Br J Anaesth. (2017) 119:167–9. doi: 10.1093/bja/aex167
31. De Oliveira G. Biological evidence of the impact of burnout on the health of anesthesiologists. J Clin Anesth. (2017) 41:62. doi: 10.1016/j.jclinane.2017.06.011
32. Scaioli G, Schafer WLA, Boerma WGW, Spreeuwenberg P, van den Berg M, Schellevis FG, et al. Patients' perception of communication at the interface between primary and secondary care: a cross-sectional survey in 34 countries. BMC Health Serv Res. (2019) 19:1018. doi: 10.1186/s12913-019-4848-9
33. Ravi S. Strengthening health systems through international blood product sharing agreements. Health security. (2017) 15:110–7. doi: 10.1089/hs.2016.0039
Keywords: anesthesiologist, burnout, job stress, questionnaire, tertiary class A hospital
Citation: Yang G, Pan L-y, Fu X-l, Qing Z, Dong B-h and Ye J-m (2023) Burnout and job stress of anesthesiologists in the tertiary class A hospitals in Northwest China: A cross-sectional design. Front. Med. 10:1140552. doi: 10.3389/fmed.2023.1140552
Received: 09 January 2023; Accepted: 13 March 2023;
Published: 11 April 2023.
Edited by:
Nilgun Ulutasdemir, Gümüşhane University, TürkiyeReviewed by:
Majed Wadi, Qassim University, Saudi ArabiaPasquale Buonanno, University of Naples Federico II, Italy
Copyright © 2023 Yang, Pan, Fu, Qing, Dong and Ye. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jiu-min Ye, MzE1MTMwNTU2QHFxLmNvbQ==
†These authors have contributed equally to this work