 Carmen Scheibenbogen1
Carmen Scheibenbogen1 Judith Theresia Bellmann-Strobl2,3,4
Judith Theresia Bellmann-Strobl2,3,4 Cornelia Heindrich1*
Cornelia Heindrich1* Kirsten Wittke1
Kirsten Wittke1 Elisa Stein1
Elisa Stein1 Christiana Franke5
Christiana Franke5 Harald Prüss5,6
Harald Prüss5,6 Hannah Preßler5
Hannah Preßler5 Marie-Luise Machule5
Marie-Luise Machule5 Heinrich Audebert5
Heinrich Audebert5 Carsten Finke5
Carsten Finke5 Hanna Gwendolyn Zimmermann2,3,4Birgit Sawitzki1,7
Hanna Gwendolyn Zimmermann2,3,4Birgit Sawitzki1,7 Christian Meisel1,8
Christian Meisel1,8 Markus Toelle9Anne Krueger9
Markus Toelle9Anne Krueger9 Anna C. Aschenbrenner10Joachim L. Schultze10,11,12
Anna C. Aschenbrenner10Joachim L. Schultze10,11,12 Marc D. Beyer10,11Markus Ralser13,14
Marc D. Beyer10,11Markus Ralser13,14 Michael Mülleder13Leif Erik Sander15
Michael Mülleder13Leif Erik Sander15 Frank Konietschke16
Frank Konietschke16 Friedemann Paul2,3,4
Friedemann Paul2,3,4 Silvia Stojanov17Lisa Bruckert18
Silvia Stojanov17Lisa Bruckert18 Dennis M. Hedderich19
Dennis M. Hedderich19 Franziska Knolle19
Franziska Knolle19 Gabriela Riemekasten20
Gabriela Riemekasten20 Maria J. G. T. Vehreschild21
Maria J. G. T. Vehreschild21 Oliver A. Cornely22,23,24
Oliver A. Cornely22,23,24 Uta Behrends17,25,26†Susen Burock18†
Uta Behrends17,25,26†Susen Burock18†- 1Institute of Medical Immunology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Berlin, Germany
- 2Experimental and Clinical Research Center, a cooperation between the Max Delbrück Center for Molecular Medicine in the Helmholtz Association and Charité Universitätsmedizin Berlin, Berlin, Germany
- 3NeuroCure Clinical Research Center, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 4Max Delbrück Center for Molecular Medicine in the Helmholtz Association (MDC), Berlin, Germany
- 5Department of Neurology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Berlin, Germany
- 6Deutsches Zentrum für Neurodegenerative Erkrankungen (DZNE), Berlin, Germany
- 7Berlin Institute of Health at Charité – Universitätsmedizin Berlin, Center of Immunomics, Berlin, Germany
- 8Department of Immunology, Labor Berlin - Charité Vivantes GmbH, Berlin, Germany
- 9Department of Nephrology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Berlin, Germany
- 10Systems Medicine, Deutsches Zentrum für Neurodegenerative Erkrankungen (DZNE), Bonn, Germany
- 11PRECISE Platform for Single Cell Genomics and Epigenomics, DZNE and University of Bonn, Bonn, Germany
- 12Genomics and Immunoregulation, Life and Medical Sciences Institute, University of Bonn, Bonn, Germany
- 13Institute of Biochemistry, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 14The Wellcome Centre for Human Genetics, Nuffield Department of Medicine, University of Oxford, Oxford, United Kingdom
- 15Department of Infectious Diseases and Respiratory Medicine, Charité–Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 16Institute of Biochemistry, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Germany
- 17Childrens’ Hospital, School of Medicine, Technical University of Munich, Munich, Germany
- 18Clinical Trial Office, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt Universität zu Berlin, Berlin, Germany
- 19Department of Neuroradiology, School of Medicine, Technical University of Munich, Munich, Germany
- 20Department of Rheumatology, University Medical Center Schleswig-Holstein Campus Lübeck, Lübeck, Germany
- 21Department of Internal Medicine, Infectious Diseases, University Hospital Frankfurt, Goethe University Frankfurt, Frankfurt am Main, Germany
- 22Department of Internal Medicine, University Hospital Cologne, Cologne, Germany
- 23German Centre for Infection Research (DZIF), Partner Site Bonn-Cologne, Germany
- 24University of Cologne, Faculty of Medicine, Institute of Translational Research, Cologne Excellence Cluster on Cellular Stress Responses in Aging-Associated Diseases (CECAD), Cologne, Germany
- 25German Center for Infection Research (DZIF), Berlin, Germany
- 26AGV Research Unit Gene Vectors, Helmholtz Center Munich (HMGU), Munich, Germany
The sequela of COVID-19 include a broad spectrum of symptoms that fall under the umbrella term post-COVID-19 condition or syndrome (PCS). Immune dysregulation, autoimmunity, endothelial dysfunction, viral persistence, and viral reactivation have been identified as potential mechanisms. However, there is heterogeneity in expression of biomarkers, and it is unknown yet whether these distinguish different clinical subgroups of PCS. There is an overlap of symptoms and pathomechanisms of PCS with postinfectious myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). No curative therapies are available for ME/CFS or PCS. The mechanisms identified so far provide targets for therapeutic interventions. To accelerate the development of therapies, we propose evaluating drugs targeting different mechanisms in clinical trial networks using harmonized diagnostic and outcome criteria and subgrouping patients based on a thorough clinical profiling including a comprehensive diagnostic and biomarker phenotyping.
Introduction
COVID-19 frequently results in persistent debilitating symptoms lasting longer than 3 months, referred to as post-COVID-19 syndrome (PCS). Based on large epidemiological studies, approximately 10% of adults who had a positive SARS-CoV-2 PCR suffer from persisting symptoms beyond 3 months (1). Vaccination confers partial protection against PCS (2). In the majority of adult PCS patients, severity of symptoms persists or even increases after 12 months (3). Predominantly, healthy young and middle-aged adults with female preponderance are affected. Less data is available for children and adolescents, indicating a lower prevalence and severity (4, 5).
The clinical presentation is complex with various clinical phenotypes and most likely different mechanisms (6, 7). In most younger patients, there is no evidence for organ damage, and the majority has a symptom cluster with predominance of fatigue, exertion intolerance, cognitive impairment, orthostatic intolerance, and autonomous dysfunction (8).
Postinfectious syndromes have been described for more than a century and can be triggered by various infections (9). There is now clear evidence that a subset of PCS complies with standard case definitions of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) (10, 11). We will refer to such cases as post-COVID (PC) ME/CFS. Post-infectious ME/CFS (ICD-10 code G93.3) is a complex and severely disabling disease with no approved treatment and therefore, a very high and so far unmet medical need (12). Key symptoms are central and muscle fatigue, exertion intolerance with post-exertional malaise (PEM), cognitive impairment, orthostatic intolerance, headache, and muscle pain - hence a large overlap of symptoms with PCS. ME/CFS had an estimated prevalence of 0.3–0.8% before COVID-19, including children and adolescents (12). The prevalence of PCS that fits ME/CFS diagnostic criteria will likely be substantial, and poses a major problem for health care and society. A recent study from Germany that analyzed health insurance data from nearly 30 million individuals showed an annual incidence rate in 2020 of 6 versus 2/1000 in adults with and without prior COVID-19, respectively (13). So far, there is no proven effective therapy for PCS or ME/CFS (14).
Pathomechanisms of pcs and Me/Cfs
There is accumulating evidence from large well-performed studies that immune activation and dysregulation with inflammation and alteration of immune cells are frequently found in PCS. Various autoantibodies have been described to be triggered by COVID-19 and to be associated with the development of PCS. Correlations of both, soluble markers of inflammation and autoantibodies, including antinuclear antibodies (ANA), neurological and G protein-coupled receptor (GPCR) antibodies with symptom severity were found (15–17). Endothelitis is common in acute COVID-19, and can persist in PCS with endothelial dysfunction and various biomarkers of endothelial inflammation, microclots and hypoperfusion shown (7, 18). There is evidence for viral persistence with detection of spike and nucleoprotein in serum in a subset of PCS (7, 19). However, there is a broad heterogeneity in expression of biomarkers, and it is unknown yet whether we face distinct subgroups of PCS or overlapping mechanisms. Although there are correlations of some biomarkers with symptom severity, it is not possible to delineate clinical phenotypes from biomarker profiles yet. Similarly, there is evidence that immune dysregulation and autoantibodies play a key role in ME/CFS, including the high frequency of autoimmune diseases among first-degree family members, associations with autoimmunity-related gene variants and MHC alleles, skewed B cell receptor genes, and association of symptom severity with GPCR antibodies (15, 20–22). Further, there is ample evidence for endothelial dysfunction affecting both medium arteries, assessed by flow-mediated dilation, and capillaries assessed by post occlusive reactive hyperemia (20, 23). Many reports have found altered cytokine levels and their correlation with severity in ME/CFS, though many are inconsistent with each other (24–26). Of interest, reactivation of Epstein–Barr virus (EBV) during COVID-19 frequently occurs and is a risk factor to develop PCS (6, 7). In a subset of individuals, infectious mononucleosis precedes ME/CFS (27).
Drugs of interest to study in pcs and Me/Cfs
Conceptually, selection criteria for therapeutic strategies should be based on potential mechanisms, defined by specific biomarkers. There are numerous drugs already licensed for other indications that target mechanisms identified in PCS and/or ME/CFS. Repurposing of such drugs may offer faster clinical approval.
In PCS, several interventional randomized controlled trials (RCT) have been initiated for targeted drug therapy worldwide (Table 1). This includes anti-inflammatory drugs, including corticosteroids, loratadine, montelukast, atorvastatin, baricitinib and phosphodiesterase inhibitors. Treatment studies depleting autoantibodies have been started with plasma exchange and immunoadsorption. The first specific drug in a clinical trial is the neonatal Fc receptor inhibitor efgartigimod, which enhances IgG degradation and was recently licensed for therapy in myasthenia gravis (28). Another study was initiated with the aptamer BC007, which has shown safety and GPCR antibody neutralizing capacity in a phase I trial (29). Antivirals include targeting of potential residual SARS-CoV-2 as well as a monoclonal antibody against a reactivated endogenous retrovirus. Further several neuromodulators are studied in RCT, including vortioxetine, an antidepressant with established pro-cognitive properties, lithium with anti-depressive and anti-inflammatory properties, fampridine, a potassium channel-blocking agent linked to working memory and approved for multiple sclerosis, and dexamphetamine with first evidence for efficacy in ME/CFS (30). Targeting endothelial dysfunction and hypoperfusion holds promise in both, PCS and ME/CFS, and a phase II RCT with the guanylate cyclase inhibitor vericiguat already licensed in heart failure has started in PCS and PC ME/CFS (31). Hyperbaric oxygen therapy (HBOT) was already shown to improve neurocognitive function in a phase II RCT in PCS, and is currently studied in another RCT (32).
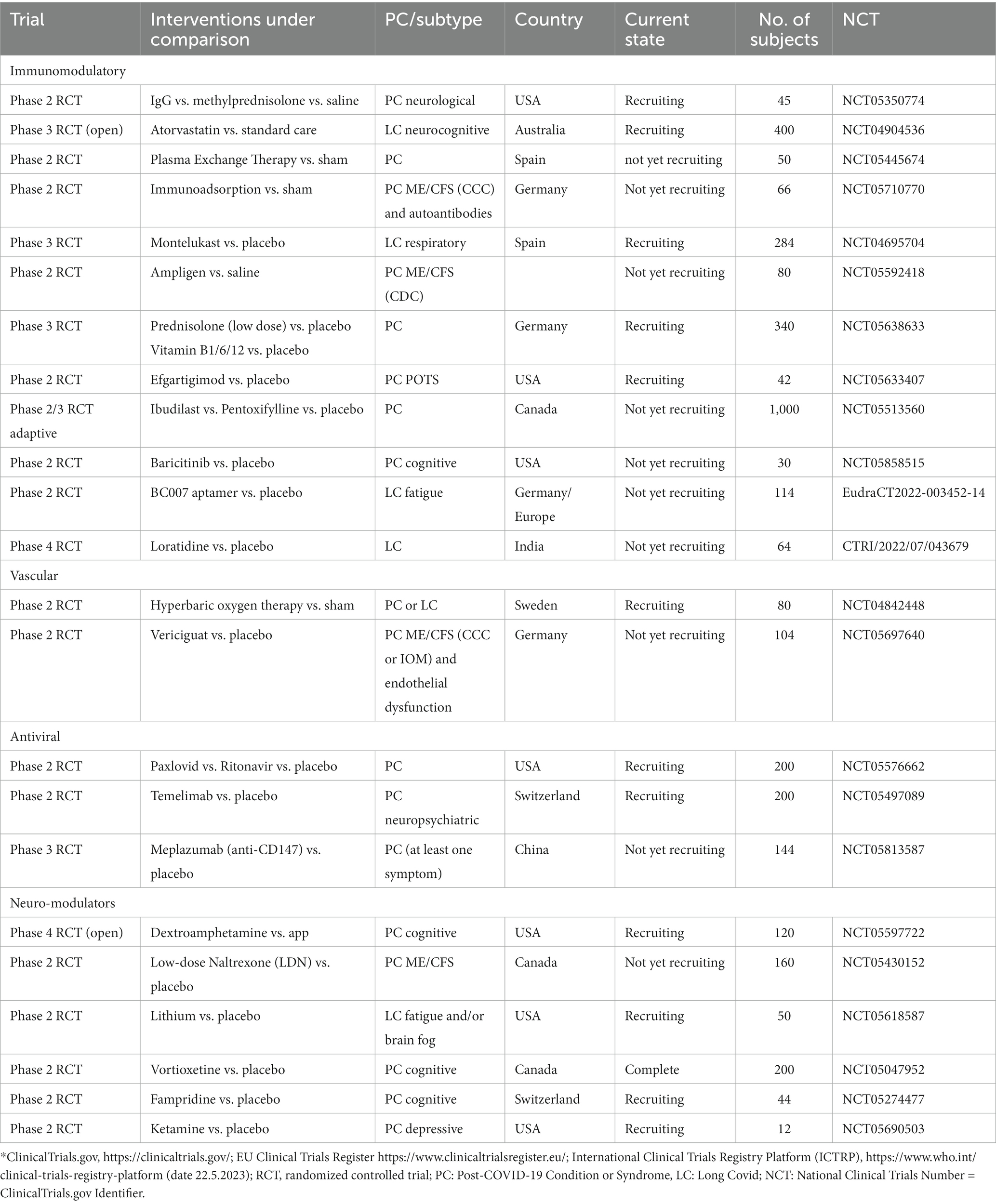
Table 1. Randomized controlled trials in PCS registered in clinical trial platforms*.
In ME/CFS, there has been little interest of pharmaceutical companies in clinical trials for decades, presumably due to the complexity of the disease, conflicting concepts of etiology and paucity of research on pathomechanisms. There are now 2 trials conducted in PC ME/CFS including rintatolimod, a TLR-3 agonist. This is one of the few drugs, which has been studied in a phase III trial in ME/CFS showing evidence for efficacy in patients with shorter disease duration (33). Inclusion criteria are, however, the Fukuda criteria not requiring PEM. Further low dose naltrexone with evidence for efficacy from case reports in ME/CFS and recently also in an open trial in PCS will be studied in a RCT phase 2 trial (34, 35). For non-PC ME/CFS only one interventional RCT pharmacological trial with N-acetylcysteine could be found (NCT04542161). However, there is reasonable hope that some of the drugs that are effective in LC can also be used in ME/CFS.
Further drugs of interest to study in PCS and ME/CFS are listed in Table 2. A novel approach to alleviate inflammation is to target kinases that regulate inflammatory mediators like Janus kinase (JAK) inhibitors and several others (36, 37). Further certain drugs exert, besides their licensed indication, anti-inflammatory effects like metformin or certain antibiotics with evidence for efficacy in acute COVID or from non-controlled trials in ME/CFS like minocycline (36, 39, 40). Further, there is first data that H1 and H2 antihistamines can have beneficial effects (38). There are numerous drugs to target autoantibody-producing B cells including monoclonal antibodies and more recently Bruton tyrosinkinase (BTK) inhibitors. Rituximab has been studied in ME/CFS in several phase II and one phase III study with inconclusive results (49, 50). Newer and more effective antibodies targeting CD20, CD19 or CD38 depleting both, B cells and/or plasma cells, are thus promising candidates (41). There are further groups of drugs targeting endothelial dysfunction via PDE5, β2/3 adrenergic or acetylcholine receptors (43–45). A small study was already performed with the PDE5 inhibitor sildenafil in ME/CFS showing a significant improvement of fatigue in 5 treated patients compared to 6 receiving placebo (NCT00598585). There is also evidence from various small trials in ME/CFS that the neuromodulators low dose aripiprazole and methylphenidate can have efficacy (46, 47). Also guanfacine was described in a case series to ameliorate symptoms in PCS (48). PCS and ME/CFS patients frequently suffer from dysautonomia and postural tachycardia syndrome (POTS). There are several pharmacological treatment options from small clinical trials, but no licensed drugs are available. Similarly, for other key symptoms of ME/CFS and PCS, sleep disturbances and post exertional malaise there is no evidence for medications from clinical trials.
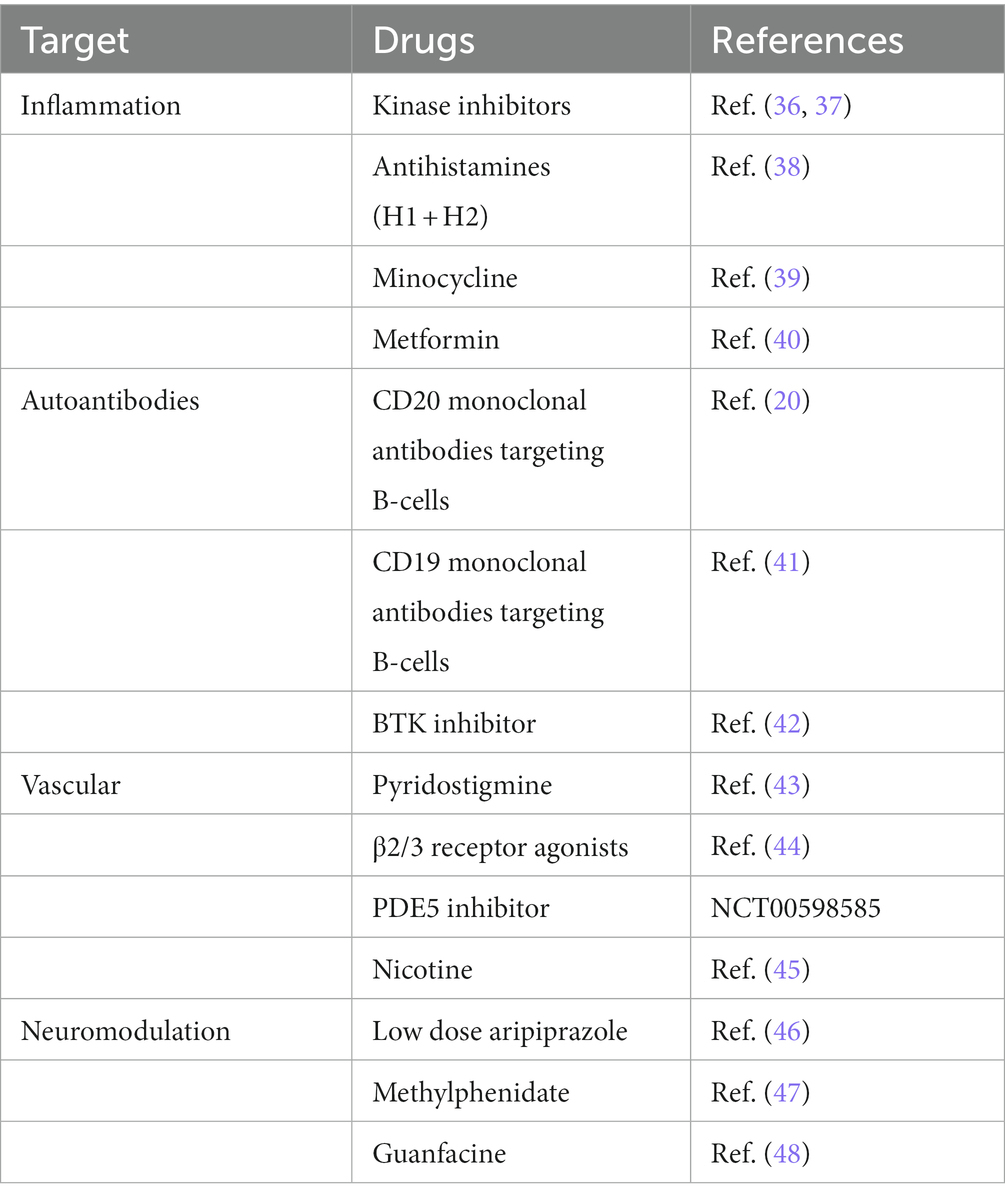
Table 2. Further drugs of interest in PCS and ME/CFS.
Concept for clinical trial networks
Due to the complexity of PCS and ME/CFS harmonization of diagnostic and inclusion and outcome criteria for clinical trials would be desirable. So far, many clinical trials do not specify PCS subgroups or clinical phenotypes. In several ongoing trials Long COVID (LC) is mentioned as inclusion criterium, which is poorly defined as persistent symptoms for more than 4 weeks. For ME/CFS, various diagnostic criteria exist and only stricter criteria requiring the cardinal symptom PEM should be used for clinical trials (12). Clinical trial platforms or networks would allow proof-of-concept clinical trials with various drugs in a harmonized manner using similar diagnostic criteria, evaluation tools, clinical outcome criteria and pre-enrolment phenotyping of patients to categorize them according to potential underlying mechanisms. Further clinical trial networks allow to rapidly recruit larger sample size when moving from phase II to phase III trials or to recruit ME/CFS patients triggered by another infection, e.g., EBV. Due to the diversity of pathological mechanisms, clinical trials should be accompanied by comprehensive biomarker analyses, focusing on both, classical biomarkers as well as compound biomarkers, and biomarker signatures that become increasingly accessible. Besides achieving further insights into the mechanisms and into drug efficacy, such approaches can lead to the development of companion diagnostics for consecutive trials. Specific diagnostic assessments including advanced structural and functional magnetic resonance imaging (MRI), neurocognitive testing, autonomic testing, and vascular imaging should be implemented to visualize key clinical and functional abnormalities of PCS (18, 51–53).
Based on the concept outlined above, a German consortium was recently established, the National Clinical Study Group (NKSG) for PCS and ME/CFS. The interdisciplinary team includes clinical experts from neurology, neuroimmunology, clinical immunology, rheumatology, cardiology, pediatrics, psychiatry, neuropsychology, neuroradiology, and infection medicine, with specific expertise in diagnosing and treating patients with PCS and ME/CFS, as well as experts in human immunology, molecular medicine, biochemistry, data sciences, bioinformatics, and artificial intelligence (AI), with long-standing expertise in biomedical research. Patient inclusion criteria refer to defined clinical phenotypes, objective clinical measures, and potential biomarkers. Patients with PCS and/or ME/CFS are being diagnosed according to standard diagnostic criteria as published for PCS by the WHO and for ME/CFS by the Canadian Consensus Criteria (54). In addition to quantification of symptoms and functional impairment by specific questionnaires and patient reported outcome measures (PROMs), neurocognitive and autonomic testing, multimodal MRI of the brain, as well as assessment of physical fatigue and endothelial dysfunction will be performed before and after treatment (18, 51–53). Further we offer regular education and support in diagnostic assessment of ME/CFS.
Regulatory requirements make investigator-initiated clinical trials challenging. For clinical trial management, a clinical trial office (CTO) platform aids in protocol preparation and is in charge of all regulatory and data safety affairs, trial submission, monitoring, data management, and biostatistical support. Harmonized clinical study documents including protocols, diagnostic criteria, and clinical outcome parameters are provided for all studies to allow rapid preparation of clinical trials and comparison of outcomes among the various trials. Measures for quality assurance include recruitment of patients from specialized university institutions and from observational studies, the use of standardized diagnostic criteria, and the collection of a harmonized set of data in a secure common database. This approach will allow to perform excellent systematic and comprehensive analyses, and to compare the results across all trials.
Clinical trials will be accompanied by a comprehensive biomarker program to understand pathomechanisms of relevance for drug efficacy and to identify companion diagnostics. The biomarker platform will provide comprehensive phenotyping for all trials including the analyses of soluble markers for inflammation and endothelial dysfunction, autoantibodies, immune cell phenotyping, viral persistence, and reactivation, as well as high-resolution approaches such as single-cell RNA sequencing (scRNA-seq) and proteomics (15, 55–57). Special attention needs to be given to the observation that single biomarkers often fail to capture the properties of complex diseases. New proteomic techniques allow to measure signatures in human serum und plasma at low costs, and can rapidly be translated into panel assays that suit routine testing (56, 57). High-resolution scRNA-seq can assess all immune cells and deviations of their molecular programs in parallel, allowing unravelling alterations in subpopulations unamenable by routine diagnostics as well as the development of novel signatures for disease and treatment outcome (55, 58). To assure quality of biomaterial and comparability of laboratory results, all blood samples will be collected in a harmonized manner, and then processed and stored according to standard operating procedures (SOPs) at local biobanks.
A diagnostic platform will perform structural and functional MRI studies and vascular diagnostics before and after interventions, including assessments of endothelial function and perfusion using non-invasive detection and measurement of endothelial dysfunction via Endo-PAT™, optical coherence tomography angiography (OCT-A), and arterial spin labeling (ASL) MRI (18, 59). Diagnostic assessments will be performed using harmonized protocols that have been previously established within the German National Pandemic Cohort Network (NAPKON) (60).
Links between clinical, diagnostic, and biomarker data will be established via bioinformatics, statistics, machine learning, and AI with the overarching goal to identify subgroups responding to the different therapeutic strategies, to further elucidate the pathogenesis of PCS and ME/CFS, and to identify diagnostic and prognostic biomarkers.
The first proof-of-concept trials (in phase II settings) performed are hypothesis-driven with a rationale based on clinical phenotypes and existing biomarkers. Repurposing of drugs will guarantee rapid trial initiation and drug availability. To assess the role of autoantibodies, a proof-of-concept trial with repetitive immunoadsorption in PC ME/CFS (NCT05629988) as well as a randomized controlled trial (RCT) with a sham-apheresis in postinfectious and PC ME/CFS with autoantibodies will be performed (NCT05710770) (61). Patients responding to immunoadsorption but relapsing will be treated in a consecutive trial with a B cell depleting monoclonal antibody. To treat endothelial dysfunction and hypoperfusion in PCS and PC ME/CFS, a phase II trial with the sGC stimulator vericiguat has been initiated (NCT05697640). Positive effects of prednisolone treatment in PCS with neurological symptoms have been suggested in case series (62). A RCT with high dose prednisolone will therefore be performed in PCS with predominant neurocognitive impairment, in which inflammation and autoantibodies targeting brain epitopes are common (17). Hyperbaric oxygen therapy was already shown to improve fatigue and cognitive impairment in a sham-controlled trial in long COVID patients (32). The efficacy of HBOT in patients with ME/CFS with moderate to severe cognitive impairment will be studied, too.
Based on results of these phase II trials, drugs and medical devices will be identified to be further evaluated in phase III trials together with the NAPKON-TIP (National Pandemic Cohort Network – Therapeutic Intervention Platform) supported by the German Network University Medicine (NUM) and international partners. The patient organizations Long Covid Deutschland and Deutsche Gesellschaft für ME/CFS are included and participate in the conception and conduction of all clinical trials as well as in the translation of the biomedical research results. Collaboration with the pharmaceutical industry is desired for fast access to drugs, financial support, achieving rapid licensing, and integrating further drugs to be developed.
Conclusion
Our concept of a multipronged clinical trial platform approach addresses the complexity and heterogeneity of PCS and ME/CFS, enabling to test numerous drugs in clinical trials in a harmonized manner accompanied by comprehensive mechanistic studies. Such an approach will pave the way for more rapid development of drugs for PCS and ME/CFS to find therapeutic solutions for specific subgroups and finally all patients. Further, it will allow the development and identification of precise diagnostic, prognostic and companion biomarkers ultimately leading to targeted and individualized therapies combatting the different disease mechanisms. Finally, the identification of biomarkers predicting response to treatment provides strong evidence for causative pathomechanisms.
Author’s note
Further members of the NKSG Study Group are: Fatma Amari, Christine Appelt, Silvia Augustin, Sandra Bauer, Janina Behrends, Fabian Boesl, Benno Bremer, Isabel Bünger, Adeline Dehlinger, Vadim Farztdinov, Manuela Fiedler, Helma Freitag, Anja Freiwald, Anna Hausruckinger, Tim Hartung, Johanna Herzog, Uta Hoppmann, Claudia Kedor, Kristin Kräker, Stephan Krohn, Joseph Kuchling, Carla Leutloff, Lucie Yuanting Li, Philippe Manceau, Maron Mantwill, Kirstin Mittelstraß, Astrid Nümann, Vanessa Raeder, Lukas Reeß, Valentin Riedl, Hadi Salih, Franziska Sotzny, Silvia Thiel, Friederike Ufer, Katrin Vogt, Katharina Wurdack, Claus Zimmer.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
CS, SB, and UB developed the concept of the studies. BS, CaF, HPru, ChF, and JB-S gave important input to the study concepts. CS was the guarantor, wrote the original draft of the paper. CS, UB, BS, CaF, HA, JBS, CM, ACA, JLS, FP, MR, SS, DH, and CH reviewed and edited the paper. CH attested that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted. All authors contributed to the article and approved the submitted version.
Funding
The clinical trial platform is funded by the Bundesministerium für Bildung und Forschung (German Ministry of Education and Research), Grant 01EP2201.
Conflict of interest
The Charité Universitaetsmedizin Berlin holds a patent for the use of vericiguat in Post-COVID Syndrome. CS, JB-S, CH, KW, ES, CaF, HPru, HPre, M-LM, HA, ChF, HZ, BS, CM, MT, AK, MR, MM, LS, FKo, FP, LB, and SB are employed at Charité Universitaetsmedizin Berlin.
CM was employed by Labor Berlin - Charité Vivantes GmbH.
The remaining authors declare that the research was conducted in the absence of any comercial or financial relationships that could be construed as a potential conflict of interest.
The Handling Editor NS declared a past collaboration with the Author CS.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ballering, AV, van Zon, SKR, Olde Hartman, TC, and Rosmalen, JGM. Persistence of somatic symptoms after COVID-19 in the Netherlands: an observational cohort study. Lancet. (2022) 400:452–61. doi: 10.1016/S0140-6736(22)01214-4
2. Al-Aly, Z, Bowe, B, and Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med. (2022) 28:1461–7. doi: 10.1038/s41591-022-01840-0
3. Tran, VT, Porcher, R, Pane, I, and Ravaud, P. Course of post COVID-19 disease symptoms over time in the ComPaRe long COVID prospective e-cohort. Nat Commun. (2022) 13:1812. doi: 10.1038/s41467-022-29513-z
4. Nittas, V, Gao, M, West, EA, Ballouz, T, Menges, D, Wulf Hanson, S, et al. Long COVID through a public health Lens: an umbrella review. Public Health Rev. (2022) 43:1604501. doi: 10.3389/phrs.2022.1604501
5. Behnood, SA, Shafran, R, Bennett, SD, Zhang, AXD, O'Mahoney, LL, Stephenson, TJ, et al. Persistent symptoms following SARS-CoV-2 infection amongst children and young people: a meta-analysis of controlled and uncontrolled studies. J Infect. (2022) 84:158–70. doi: 10.1016/j.jinf.2021.11.011
6. Su, Y, Yuan, D, Chen, DG, Ng, RH, Wang, K, Choi, J, et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cells. (2022) 185:881–95.e20. doi: 10.1016/j.cell.2022.01.014
7. Davis, HE, McCorkell, L, Vogel, JM, and Topol, EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. (2023) 21:133–46. doi: 10.1038/s41579-022-00846-2
8. Subramanian, A, Nirantharakumar, K, Hughes, S, Myles, P, Williams, T, Gokhale, KM, et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat Med. (2022) 28:1706–14. doi: 10.1038/s41591-022-01909-w
9. Choutka, J, Jansari, V, Hornig, M, and Iwasaki, A. Unexplained post-acute infection syndromes. Nat Med. (2022) 28:911–23. doi: 10.1038/s41591-022-01810-6
10. Kedor, C, Freitag, H, Meyer-Arndt, L, Wittke, K, Hanitsch, LG, Zoller, T, et al. A prospective observational study of post-COVID-19 chronic fatigue syndrome following the first pandemic wave in Germany and biomarkers associated with symptom severity. Nat Commun. (2022) 13:5104. doi: 10.1038/s41467-022-32507-6
11. Bonilla, H, Quach, TC, Tiwari, A, Bonilla, AE, Miglis, M, Yang, PC, et al. Myalgic encephalomyelitis/chronic fatigue syndrome is common in post-acute sequelae of SARS-CoV-2 infection (PASC): results from a post-COVID-19 multidisciplinary clinic. Front Neurol. (2023) 14:1090747. doi: 10.3389/fneur.2023.1090747
12. Nacul, L, Authier, FJ, Scheibenbogen, C, Lorusso, L, Helland, IB, Martin, JA, et al. European network on Myalgic encephalomyelitis/chronic fatigue syndrome (EUROMENE): Expert consensus on the diagnosis, service provision, and Care of People with ME/CFS in Europe. Medicina. (2021) 57:510. doi: 10.3390/medicina57050510
13. Roessler, M, Tesch, F, Batram, M, Jacob, J, Loser, F, Weidinger, O, et al. Post-COVID-19-associated morbidity in children, adolescents, and adults: a matched cohort study including more than 157,000 individuals with COVID-19 in Germany. PLoS Med. (2022) 19:e1004122. doi: 10.1371/journal.pmed.1004122
14. Ledford, H . Long-COVID treatments: why the world is still waiting. Nature. (2022) 608:258–60. doi: 10.1038/d41586-022-02140-w
15. Sotzny, F, Filgueiras, IS, Kedor, C, Freitag, H, Wittke, K, Bauer, S, et al. Dysregulated autoantibodies targeting vaso- and immunoregulatory receptors in post COVID syndrome correlate with symptom severity. Front Immunol. (2022) 13:981532. doi: 10.3389/fimmu.2022.981532
16. Son, K, Jamil, R, Chowdhury, A, Mukherjee, M, Venegas, C, Miyasaki, K, et al. Circulating anti-nuclear autoantibodies in COVID-19 survivors predict long COVID symptoms. Eur Respir J. (2023) 61:2200970. doi: 10.1183/13993003.00970-2022
17. Franke, C, Boesl, F, Goereci, Y, Gerhard, A, Schweitzer, F, Schroeder, M, et al. Association of cerebrospinal fluid brain-binding autoantibodies with cognitive impairment in post-COVID-19 syndrome. Brain Behav Immun. (2023) 109:139–43. doi: 10.1016/j.bbi.2023.01.006
18. Haffke, M, Freitag, H, Rudolf, G, Seifert, M, Doehner, W, Scherbakov, N, et al. Endothelial dysfunction and altered endothelial biomarkers in patients with post-COVID-19 syndrome and chronic fatigue syndrome (ME/CFS). J Transl Med. (2022) 20:138. doi: 10.1186/s12967-022-03346-2
19. Newell, KL, and Waickman, AT. Inflammation, immunity, and antigen persistence in post-acute sequelae of SARS-CoV-2 infection. Curr Opin Immunol. (2022) 77:102228. doi: 10.1016/j.coi.2022.102228
20. Fluge, Ø, Tronstad, KJ, and Mella, O. Pathomechanisms and possible interventions in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J Clin Invest. (2021) 131:e150377. doi: 10.1172/JCI150377
21. Steiner, S, Becker, SC, Hartwig, J, Sotzny, F, Lorenz, S, Bauer, S, et al. Autoimmunity-related risk variants in PTPN22 and CTLA4 are associated with ME/CFS with infectious onset. Front Immunol. (2020) 11:578. doi: 10.3389/fimmu.2020.00578
22. Sato, W, Ono, H, Matsutani, T, Nakamura, M, Shin, I, Amano, K, et al. Skewing of the B cell receptor repertoire in myalgic encephalomyelitis/chronic fatigue syndrome. Brain Behav Immun. (2021) 95:245–55. doi: 10.1016/j.bbi.2021.03.023
23. Sandvik, MK, Sørland, K, Leirgul, E, Rekeland, IG, Stavland, CS, Mella, O, et al. Endothelial dysfunction in ME/CFS patients. PLoS One. (2023) 18:e0280942. doi: 10.1371/journal.pone.0280942
24. Hornig, M, Montoya, JG, Klimas, NG, Levine, S, Felsenstein, D, Bateman, L, et al. Distinct plasma immune signatures in ME/CFS are present early in the course of illness. Sci Adv. (2015) 1:e1400121. doi: 10.1126/sciadv.1400121
25. VanElzakker, MB, Brumfield, SA, and Lara Mejia, PS. Neuroinflammation and cytokines in Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): a critical review of research methods. Front Neurol. (2018) 9:1033. doi: 10.3389/fneur.2018.01033
26. Montoya, JG, Holmes, TH, Anderson, JN, Maecker, HT, Rosenberg-Hasson, Y, Valencia, IJ, et al. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proc Natl Acad Sci U S A. (2017) 114:E7150–8. doi: 10.1073/pnas.1710519114
27. Jason, LA, Cotler, J, Islam, MF, Sunnquist, M, and Katz, BZ. Risks for developing Myalgic encephalomyelitis/chronic fatigue syndrome in college students following infectious mononucleosis: a prospective cohort study. Clin Infect Dis. (2021) 73:e3740–6. doi: 10.1093/cid/ciaa1886
28. Saccà, F, Barnett, C, Vu, T, Peric, S, Phillips, GA, Zhao, S, et al. Efgartigimod improved health-related quality of life in generalized myasthenia gravis: results from a randomized, double-blind, placebo-controlled, phase 3 study (ADAPT). J Neurol. (2023) 270:2096–105. doi: 10.1007/s00415-022-11517-w
29. Becker, NP, Haberland, A, Wenzel, K, Göttel, P, Wallukat, G, Davideit, H, et al. A three-part, randomised study to investigate the safety, tolerability, pharmacokinetics and mode of action of BC 007, Neutraliser of pathogenic autoantibodies against G-protein coupled receptors in healthy, Young and elderly subjects. Clin Drug Investig. (2020) 40:433–47. doi: 10.1007/s40261-020-00903-9
30. Young, JL . Use of lisdexamfetamine dimesylate in treatment of executive functioning deficits and chronic fatigue syndrome: a double blind, placebo-controlled study. Psychiatry Res. (2013) 207:127–33. doi: 10.1016/j.psychres.2012.09.007
31. Armstrong, PW, Anstrom, KJ, and O'Connor, CM, VICTORIA Study Group. Vericiguat in heart failure with reduced ejection fraction. Reply. N Engl J Med. (2020) 383:1497–8. doi: 10.1056/NEJMc2027731
32. Zilberman-Itskovich, S, Catalogna, M, Sasson, E, Elman-Shina, K, Hadanny, A, Lang, E, et al. Hyperbaric oxygen therapy improves neurocognitive functions and symptoms of post-COVID condition: randomized controlled trial. Sci Rep. (2022) 12:11252. doi: 10.1038/s41598-022-15565-0
33. Strayer, DR, Young, D, and Mitchell, WM. Effect of disease duration in a randomized phase III trial of rintatolimod, an immune modulator for Myalgic encephalomyelitis/chronic fatigue syndrome. PLoS One. (2020) 15:e0240403. doi: 10.1371/journal.pone.0240403
34. O'Kelly, B, Vidal, L, McHugh, T, Woo, J, Avramovic, G, and Lambert, JS. Safety and efficacy of low dose naltrexone in a long covid cohort; an interventional pre-post study. Brain Behav Immun Health. (2022) 24:100485. doi: 10.1016/j.bbih.2022.100485
35. Polo, O, Pesonen, P, and Tuominen, E. Low-dose naltrexone in the treatment of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Fatigue: Biomed Health Behav. (2019) 7:207–17. doi: 10.1080/21641846.2019.1692770
36. RECOVERY Collaborative Group . Baricitinib in patients admitted to hospital with COVID-19 (RECOVERY): a randomised, controlled, open-label, platform trial and updated meta-analysis. Lancet. (2022) 400:359–68. doi: 10.1016/S0140-6736(22)01109-6
37. Zheng, J, Wu, J, Ding, X, Shen, HC, and Zou, G. Small molecule approaches to treat autoimmune and inflammatory diseases (part I): kinase inhibitors. Bioorg Med Chem Lett. (2021) 38:127862. doi: 10.1016/j.bmcl.2021.127862
38. Glynne, P, Tahmasebi, N, Gant, V, and Gupta, R. Long COVID following mild SARS-CoV-2 infection: characteristic T cell alterations and response to antihistamines. J Investig Med. (2022) 70:61–7. doi: 10.1136/jim-2021-002051
39. Miwa, K . Oral minocycline therapy improves symptoms of Myalgic encephalomyelitis, especially in the initial disease stage. Intern Med. (2021) 60:2577–84. doi: 10.2169/internalmedicine.6082-20
40. Bramante, CT, Buse, JB, Liebovitz, D, Nicklas, J, Puskarich, MA, Cohen, K, et al. Outpatient treatment of Covid-19 with metformin, ivermectin, and fluvoxamine and the development of long Covid over 10-month follow-up. medRxiv [Epub ahead of preprint] (2022). doi: 10.1101/2022.12.21.22283753
41. Siebert, N, Duchow, A, Paul, F, Infante-Duarte, C, and Bellmann-Strobl, J. Inebilizumab in AQP4-ab-positive neuromyelitis optica spectrum disorder. Drugs Today (Barc). (2021) 57:321–36. doi: 10.1358/dot.2021.57.5.3265453
42. Neys, SFH, Rip, J, Hendriks, RW, and Corneth, OBJ. Bruton's tyrosine kinase inhibition as an emerging therapy in systemic autoimmune disease. Drugs. (2021) 81:1605–26. doi: 10.1007/s40265-021-01592-0
43. Joseph, P, Pari, R, Miller, S, Warren, A, Stovall, MC, Squires, J, et al. Neurovascular dysregulation and acute exercise intolerance in Myalgic encephalomyelitis/chronic fatigue syndrome: a randomized, Placebo-Controlled Trial of Pyridostigmine. Chest. (2022) 162:1116–26. doi: 10.1016/j.chest.2022.04.146
44. Dal Negro, RW, Turco, P, and Povero, M. Nebivolol: an effective option against long-lasting dyspnoea following COVID-19 pneumonia - a pivotal double-blind, cross-over controlled study. Multidiscip Respir Med. (2022) 17:886. doi: 10.4081/mrm.2022.886
45. Leitzke, M . Is the post-COVID-19 syndrome a severe impairment of acetylcholine-orchestrated neuromodulation that responds to nicotine administration? Bioelectron Med. (2023) 9:2. doi: 10.1186/s42234-023-00104-7
46. Crosby, LD, Kalanidhi, S, Bonilla, A, Subramanian, A, Ballon, JS, and Bonilla, H. Off label use of aripiprazole shows promise as a treatment for Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): a retrospective study of 101 patients treated with a low dose of aripiprazole. J Transl Med. (2021) 19:50. doi: 10.1186/s12967-021-02721-9
47. Blockmans, D, and Persoons, P. Long-term methylphenidate intake in chronic fatigue syndrome. Acta Clin Belg. (2016) 71:407–14. doi: 10.1080/17843286.2016.1200816
48. Fesharaki-Zadeh, A, Lowe, N, and Arnsten, AFT. Clinical experience with the α2A-adrenoceptor agonist, guanfacine, and N-acetylcysteine for the treatment of cognitive deficits in “Long-COVID19”. Neuroimmunol Rep. (2023) 3:100154. doi: 10.1016/j.nerep.2022.100154
49. Fluge, Ø, Rekeland, IG, Lien, K, Thürmer, H, Borchgrevink, PC, Schäfer, C, et al. B-lymphocyte depletion in patients with Myalgic encephalomyelitis/chronic fatigue syndrome: a randomized, double-blind, Placebo-Controlled Trial. Ann Intern Med. (2019) 170:585–93. doi: 10.7326/M18-1451
50. Fluge, Ø, Risa, K, Lunde, S, Alme, K, Rekeland, IG, Sapkota, D, et al. B-lymphocyte depletion in Myalgic encephalopathy/ chronic fatigue syndrome. An open-label phase II study with rituximab maintenance treatment. PLoS One. (2015) 10:e0129898. doi: 10.1371/journal.pone.0129898
51. Bungenberg, J, Humkamp, K, Hohenfeld, C, Rust, MI, Ermis, U, Dreher, M, et al. Long COVID-19: objectifying most self-reported neurological symptoms. Ann Clin Transl Neurol. (2022) 9:141–54. doi: 10.1002/acn3.51496
52. Heine, JSK, Schwichtenberg, K, Hartung, TJ, Rekers, S, Chien, C, Boesl, F, et al. Structural brain changes in patients with post-COVID fatigue: a prospective observational study. EClinicalMedicine. (2023) 58:101874. doi: 10.1016/j.eclinm.2023.101874
53. Jäkel, B, Kedor, C, Grabowski, P, Wittke, K, Thiel, S, Scherbakov, N, et al. Hand grip strength and fatigability: correlation with clinical parameters and diagnostic suitability in ME/CFS. J Transl Med. (2021) 19:159. doi: 10.1186/s12967-021-02774-w
54. Carruthers, BM, Jain, AK, de Meirleir, KL, Peterson, DL, Klimas, NG, Lerner, AM, et al. Myalgic encephalomyelitis/chronic fatigue syndrome. J Chronic Fatigue Syndr. (2003) 11:7–115. doi: 10.1300/J092v11n01_02
55. Schulte-Schrepping, J, Reusch, N, Paclik, D, Baßler, K, Schlickeiser, S, Zhang, B, et al. Severe COVID-19 is marked by a dysregulated myeloid cell compartment. Cells. (2020) 182:1419–40.e23. doi: 10.1016/j.cell.2020.08.001
56. Messner, CB, Demichev, V, Wendisch, D, Michalick, L, White, M, Freiwald, A, et al. Ultra-high-throughput clinical proteomics reveals classifiers of COVID-19 infection. Cell Syst. (2020) 11:11–24.e4. doi: 10.1016/j.cels.2020.05.012
57. Wang, Z, Cryar, A, Lemke, O, Tober-Lau, P, Ludwig, D, Helbig, ET, et al. A multiplex protein panel assay for severity prediction and outcome prognosis in patients with COVID-19: an observational multi-cohort study. EClinicalMedicine. (2022) 49:101495. doi: 10.1016/j.eclinm.2022.101495
58. German COVID-19 Omics Initiative (DeCOI)Aschenbrenner, AC, Mouktaroudi, M, Krämer, B, Oestreich, M, Antonakos, N, et al. Disease severity-specific neutrophil signatures in blood transcriptomes stratify COVID-19 patients. Genome Med. (2021) 13:7. doi: 10.1186/s13073-020-00823-5
59. Schlick, S, Lucio, M, Wallukat, G, Bartsch, A, Skornia, A, Hoffmanns, J, et al. Post-COVID-19 syndrome: retinal microcirculation as a potential marker for chronic fatigue. Int J Mol Sci. (2022) 23:13683. doi: 10.3390/ijms232213683
60. Schons, M, Pilgram, L, Reese, JP, Stecher, M, Anton, G, Appel, KS, et al. The German National Pandemic Cohort Network (NAPKON): rationale, study design and baseline characteristics. Eur J Epidemiol. (2022) 37:849–70. doi: 10.1007/s10654-022-00896-z
61. Mohamed Hussein, AAR, Ibrahim, M, Makhlouf, HA, Makhlouf, NA, Abd-Elaal, HK, Kholief, KMS, et al. Value of montelukast as a potential treatment of post-COVID-19 persistent cough: a non-randomized controlled pilot study. Egypt J Bronchol. (2022) 16:1–5. doi: 10.1186/s43168-022-00154-6
62. Utrero-Rico, A, Ruiz-Ruigómez, M, Laguna-Goya, R, Arrieta-Ortubay, E, Chivite-Lacaba, M, González-Cuadrado, C, et al. A short corticosteroid course reduces symptoms and immunological alterations underlying long-COVID. Biomedicine. (2021) 9:1540. doi: 10.3390/biomedicines9111540
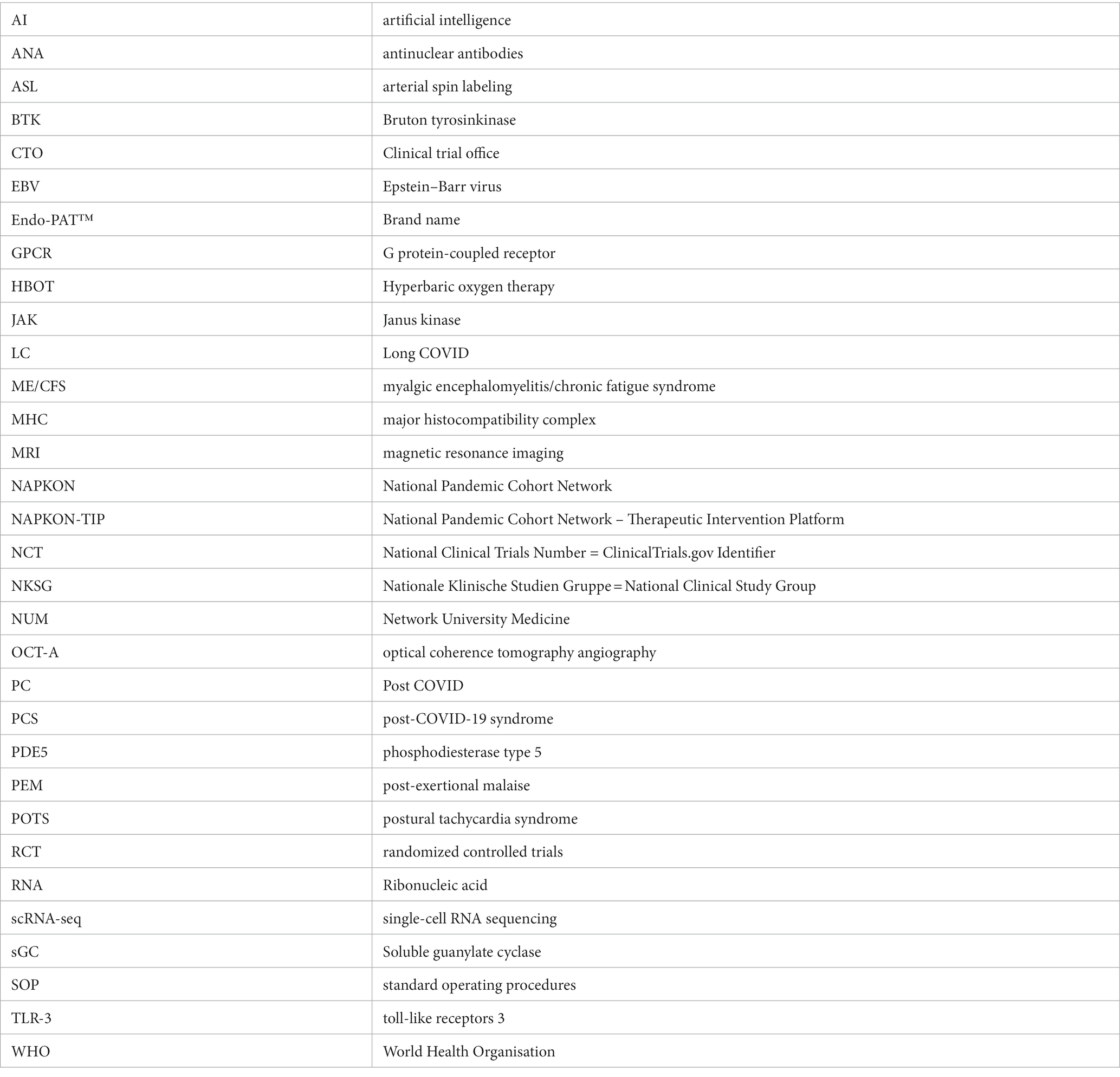
Glossary
Keywords: COVID-19, post-COVID, ME/CFS, inflammation, endothelial dysfunction, autoantibodies, clinical trials
Citation: Scheibenbogen C, Bellmann-Strobl JT, Heindrich C, Wittke K, Stein E, Franke C, Prüss H, Preßler H, Machule M-L, Audebert H, Finke C, Zimmermann HG, Sawitzki B, Meisel C, Toelle M, Krueger A, Aschenbrenner AC, Schultze JL, Beyer MD, Ralser M, Mülleder M, Sander LE, Konietschke F, Paul F, Stojanov S, Bruckert L, Hedderich DM, Knolle F, Riemekasten G, Vehreschild MJGT, Cornely OA, Behrends U and Burock S (2023) Fighting Post-COVID and ME/CFS – development of curative therapies. Front. Med. 10:1194754. doi: 10.3389/fmed.2023.1194754
Edited by:
Nuno Sepulveda, Warsaw University of Technology, PolandCopyright © 2023 Scheibenbogen, Bellmann-Strobl, Heindrich, Wittke, Stein, Franke, Prüss, Preßler, Machule, Audebert, Finke, Zimmermann, Sawitzki, Meisel, Toelle, Krueger, Aschenbrenner, Schultze, Beyer, Ralser, Mülleder, Sander, Konietschke, Paul, Stojanov, Bruckert, Hedderich, Knolle, Riemekasten, Vehreschild, Cornely, Behrends and Burock. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cornelia Heindrich, Y29ybmVsaWEuaGVpbmRyaWNoQGNoYXJpdGUuZGU=
†These authors share last authorship