 Ana Sustarsic1
Ana Sustarsic1 Vedran Hadzic1
Vedran Hadzic1 Cécil J. W. Meulenberg2
Cécil J. W. Meulenberg2 Ensar Abazovic3
Ensar Abazovic3 Mateja Videmsek1
Mateja Videmsek1 Tanja Burnik Papler4
Tanja Burnik Papler4 Armin H. Paravlic1,5*
Armin H. Paravlic1,5*- 1Faculty of Sports, University of Ljubljana, Ljubljana, Slovenia
- 2Science and Research Center Koper, Institute for Kinesiology Research, Koper, Slovenia
- 3Faculty of Sport and Physical Education, University of Sarajevo, Sarajevo, Bosnia and Herzegovina
- 4Division of Gynecology, Department of Human Reproduction, University Medical Center Ljubljana, Ljubljana, Slovenia
- 5Faculty of Sports Studies, Masaryk University, Brno, Czechia
This study aimed to investigate the effect of lifestyle intervention (LSI) on diagnosed infertility in overweight and obese women. A systematic review and meta-analysis were conducted. A literature search was performed on the following databases from September 2022 to December 2022: PubMed, Web of Science, and SPORTDiscus. The inclusion criteria were the following: women between 18 and 45 years of age, BMI over 25.0 kg/m2, diagnosed with infertility, a weight loss intervention, and control group part of RCTs. In total, 15 studies were identified and included. The meta-analysis shows a beneficial effect of LSI on reducing weight, waist circumference, and BMI and increasing infertility. A significantly beneficial effect of lifestyle intervention on weight reduction was observed for participants who initially had a higher BMI, while a non-significant effect was observed for individuals with a BMI above 35 kg/m2. The meta-analysis showed a beneficial effect of lifestyle intervention on ovulation incidence and sex hormone-binding globulin. The lifestyle intervention group had 11.23 times more ovulatory incidence than the control group, which in turn increased the ability to conceive. As robust evidence for the effect of lifestyle interventions on infertility in obese and overweight women was found, it is advised to integrate similar interventions into future infertility treatment processes.
Introduction
Infertility is a medical state generally defined as a failure to conceive after 12 months of regular intercourse. Infertility is a rising problem in human society, and although the prevalence worldwide has been difficult to ascertain with limited population-based studies and inconsistent clinical definitions, it is estimated to affect between 8 and 12% of reproductive-age couples (1). There are no exact data for Slovenia, but it is estimated that the situation is comparable to that in other European countries, which means that every 8 out of 12 couples face fertility problems (2). Primary infertility means that a couple has never achieved pregnancy, whereas secondary infertility means that a couple has had at least one prior successful conception (3).
Causes of infertility can be found in both female and male partners of reproductive-age couples. In 40–50% of the cases, the cause of infertility can be found in the reproductive system of the female partner, while in 30–40%, the cause of infertility is found in that of the male partner, and in 10% of cases, the cause is found in that of both partners. However, in 10% of couples, the cause of infertility remains unknown—idiopathic infertility (4). In women, as much as 80% of infertility can be attributed to three causes: endometriosis (5), tubal factor infertility, and polycystic ovary syndrome (PCOS) (6). Besides, a couple’s lifestyle (inactivity, stress, unsuitable diet), smoking habits (6–8), excessive consumption of alcohol (6, 7) and coffee (7), environmental pollutants (9), and psychological factors (6) can play major roles in human fertility. Excessive body weight is also an important cause of infertility (6, 10–12) and may trigger certain factors that negatively affect infertility (abnormal metabolism, hormonal disorders, menstrual and ovulary disorders, PCOS, hyperinsulinemia, hyperandrogenism, etc.) (11, 12).
The prevalence of obesity and overweight is rising worldwide and has a detrimental effect on different functions of the human body, including reproduction. In particular, obese women suffer from hormone disorders, which lead to menstrual dysfunction, anovulation, and, consequently, infertility. In women with PCOS, hormone disorders and subfertility are common, while with additional obesity, the adipocytes begin to function as endocrine organs (13). A higher BMI is associated with a poorer fertility prognosis and simultaneously shows poorer reproductive results, regardless of the method of conception. Furthermore, a high BMI leads to a higher miscarriage rate, poor pregnancy outcomes, a higher risk of complications during pregnancy, and impaired fetal wellbeing (14). It was found that weight reduction in obese and overweight women improves reproductive outcomes by ameliorating fertility, regularizing menstrual cycles, and increasing the chance of spontaneous ovulation and conception in anovulation (11, 12, 15).
Various approaches are used to reduce weight, including interventions that change lifestyle habits such as applying regular sports activities as well as nutritional and psychological counseling, while drugs that can contribute to weight loss have been used less frequently. Various studies have shown that weight-loss lifestyle-changing interventions in overweight and obese women have a positive effect on hormonal and metabolic factors. These interventions affect the levels of fasting glucose, insulin, androstenedione, testosterone, anti-Mullerian hormone, estrogen, the homeostasis model assessment of insulin resistance (HOMA-IR), and sex hormone-binding globulin (SHBG) (16–18). Lifestyle interventions (LSI) also increase the rate of spontaneous as well as in vitro fertilization (IVF) pregnancies and the number of live births (19–21).
Physical activity (PA) has an important role during preconception, pregnancy, and postpartum. Well-balanced PA and energy state have fundamentally been related to an optimal reproductive system and good general health (22). It is necessary to consider the intensity and frequency of exercise because excessive exercise can have a negative effect on fertility. However, several studies have confirmed the positive effect of regular and moderate PA on fertility in women. A systematic review by Hakimi and Cameron has shown that exercise, with or without diet, can lead to a resumption of ovulation in overweight/obese women suffering from PCOS or anovulatory infertility (23). A prospective cohort study investigated the relationship between PA and time to pregnancy. In this study, moderate PA was associated with a small increase in fecundability, regardless of BMI. These findings indicate that PA of any type might improve fertility among overweight and obese women, a subgroup at higher risk of infertility (24).
In a recent meta-analysis, the effect of PA on the reproductive health of young women was analyzed (15). However, in that particular study, there were no data on which intervention and PA might have the best results or the greatest effect of the included components. Moreover, no data on PA frequency, intensity, or duration were reported. PA is an important factor in weight loss, which is sometimes underestimated, but it is necessary to realize that not all forms of PA are suitable for obese people. Thus, to establish more detailed associations between weight-loss lifestyle-changing interventions and infertility, the present study performed a meta-analysis with the inclusion of recent studies that clearly stated the abovementioned relevant LSI parameters. Potential results from effective detailed PA interventions would be very relevant to integrate as evidence-based recommended LSI within the health system, specifically in the treatment of infertility in overweight and obese women.
Materials and methods
Search strategy and study selection
The literature search was conducted from September 2022 to December 2022. The following databases were examined: PubMed, Web of Science, and SPORTDiscus. The word AND was used between the main groups of keywords related to infertility (“infertility”, “sterility”, “subfertility”, “in vitro fertilization”, “IVF”), gender (“female”, “women”), weight (“obesity”, “overweight”), and intervention (“weight reduction”, “lifestyle”, “healthy lifestyle”, “lifestyle intervention”, “intervention”, “physical activity” or “training”), and the word OR was used between the keywords within the group.
The first review of study titles and abstracts was conducted by the first reviewer (AS), and the final review and selection were conducted by another reviewer (AP). Eligible studies that passed the selection process were included according to the determined inclusion and exclusion criteria. The inclusion criteria were the following: women between 18 and 45 years of age, BMI over 25.0 kg/m2, diagnosed with infertility or PCOS or both, a weight loss intervention, a control group, availability in the full-text English language, and research design RCTs. In the final review of the selected articles, studies that did not have results for further and definitive analysis were excluded. The study selection process is illustrated in Figure 1 following Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (25).
Figure 1. PRISMA flow diagram of the study of the first and second selection processes.
The primary outcome measures included ovulation improvement, pregnancy rates, and live birth rates, while the secondary outcome measures included changes in weight, BMI, waist circumference, and hormonal and blood factors.
Data extraction
The methodological quality of the included studies was assessed using the PEDro scale (26) by two reviewers independently (EA and AP). The PEDro scale comprises 11 items designed to rate methodological quality (26). Each satisfied item contributes 1 point to the overall PEDro score (range 0–10 points). However, item 1 (indicate briefly pertaining to external validity) was not included as part of the study quality rating for this review because it pertains to external validity, which was beyond the scope of the current review questions. Additionally, the Template for Intervention Description and Replication (TIDieR) checklist was used to assess the completeness of the intervention descriptions for both the experimental and control groups (27). The quality of evidence was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system, where classifications were made as follows: “high quality,” “moderate quality,” “low quality,” and “very low quality” (28). However, several reasons might lead to the degradation of the quality of the evidence (28). Thus, in the current study, the following criteria were considered when assessing confidence in evidence: design limitation (if the majority of studies in the meta-analysis had a PEDro score of <6); imprecision based on small sample size [< 300 for each pooled outcome (29)]; and inconsistency of the results (substantial heterogeneity within effect estimates, I2 ≥ 50%). This review did not consider the indirectness criterion because the eligibility criteria ensured a specific population with relevant outcomes.
Statistical analysis
The meta-analyses were performed using Comprehensive Meta-analysis software (version 2.0; Biostat Inc., Englewood, NJ, United States). Except for ovulation and pregnancy, for all reported outcome measures, the difference in means (DM) and 95% CIs were calculated and presented in their respective units. Thus, weight was presented in kilograms (kg), BMI in kg/m2, waist circumference in centimeters (cm), blood glucose in mmol/l, blood insulin in milli mass units per liter (mU/L), SHBG and testosterone (nmol/L), and FAI index (no unit). HOMA-IR was calculated by multiplying fasting serum insulin (μU/ml) and fasting plasma glucose (mmol/L) in arbitrary units. The odds ratio (OR) was reported for ovulation, pregnancy, and live births. The random-effects model of the meta-analysis was applied in all comparisons to determine the effect of the intervention on measures of interest. To investigate the effects of BMI on weight management and waist circumference, a subgroup analysis was performed by comparing groups with initially lower (i.e., <35 kg/m2) and greater (i.e., ≥35 kg/m2) BMI, respectively.
Furthermore, a random-effects meta-regression was performed to examine whether the effects of LSI on weight and pregnancy were moderated by the initial age and BMI of the participants, as well as different training variables. Training variables were grouped according to the following: training volume (i.e., period, weekly frequency, and the total number of training sessions) and time spent in training (i.e., duration of a single training session). To minimize the risk of overfitting, a meta-regression was performed when a minimum of 10 studies were eligible per examined covariate (30).
The publication bias was assessed by examining the asymmetry of the funnel plots using Egger’s test, and a significant publication bias was considered if the value of p was <0.10. The I2 statistic was used to investigate between-study heterogeneity, where values of 25, 50, and 75% represent low, moderate, and high statistical heterogeneity, respectively (31). Statistical significance was set at the level of a value of p of <0.05.
Results
Egger’s test was performed to provide statistical evidence of funnel plot asymmetry. The results indicated no publication bias for the following meta-analysis: weight management (p = 0.497), waist circumference (p = 0.777), glucose (p = 0.732), insulin (p = 0.804), HOMA-R (p = 0.901), SHBG (p = 0.106), and FAI (p = 0.246), respectively. For all other analyses, the results indicated publication bias (p < 0.10).
Study selection and characteristics
Following a systematic literature search in different databases, 15 studies were identified and included (Table 1). The trials included a mix of three study design types: seven RCTs, three randomized comparison trials, and five RCT pilot studies. The research covered different LSIs: diet, PA, pharmacological treatment, and psychological help.
Table 1. Characteristics of the included studies.
Quality and completeness of reporting
The reported completeness of intervention reporting was higher for the experimental conditions (mean: 73%; range from 27 to 100%) than for the control groups (mean: 57%; range from 18 to 91%). Compared to previously published data about the completeness of intervention reporting in interventional studies (32), the current meta-analysis included studies with sufficiently detailed exercise program descriptions. Table 2 shows the summarized results of the GRADE system and the PEDro scale, both used for assessing the quality of evidence.
Table 2. Grades of recommendation, assessment, development, and evaluation (GRADE) for results summarized.
The TIDieR checklist (Figure 2) provides a systematic way to describe the intervention, including rationale, materials used, procedures, how, where, when, and by whom the training was provided, and how the training was tailored and modified.
Figure 2. TIDieR checklist.
Effect of LSI on the anthropometric measures
Weight
The current meta-analysis of twelve studies with a total of 1,205 patients showed a beneficial effect (DM = −3.52 kg, 95% CI -6.57 to −0.47, df = 11; p = 0.024) of weight management on infertility (Figure 3). The evidence was downgraded from high to moderate due to high heterogeneity (I2 = 78%; p < 0.001). Owing to this substantial heterogeneity, sub-analysis and meta-regression analyses were performed. Sub-group analysis revealed that the effects of the interventions were not moderated by BMI (Q = 0.001; p = 0.980). In brief, a significantly beneficial effect was observed only for participants who had initially high BMI (DM = −3.69 kg, 95% CI -6.76 to −0.61, n = 6, p = 0.019) and not for those with less than 35 kg/m2 of BMI (DM = −3.62 kg, 95% CI -8.05 to 0.81, n = 6, p = 0.109).
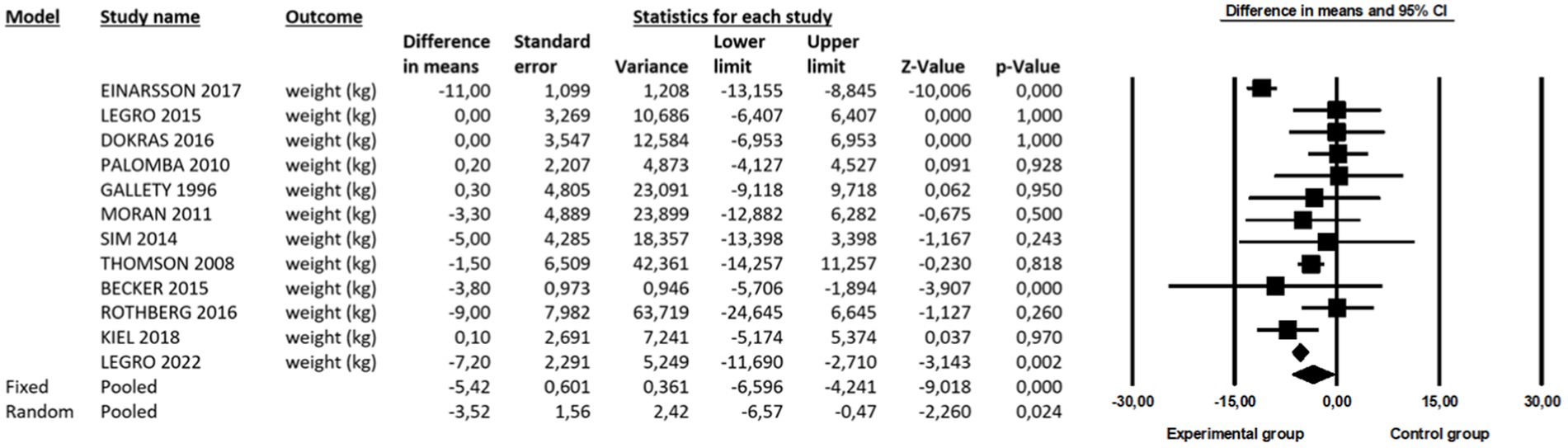
Figure 3. A beneficial effect of LSI on weight.
BMI
The meta-analysis of nine studies with a total of 977 patients showed a beneficial effect (DM = −1.75 kg/m2, 95% CI -2.60 to −0.90, df = 8; p < 0.001) on BMI management. The evidence was downgraded from high to moderate due to moderate to high heterogeneity (I2 = 65%; p = 0.004). Hence, sub-analysis and meta-regression analyses were performed. Sub-group analysis revealed that the effects of the interventions were not moderated by BMI (Q = 0.081; p = 0.776). In brief, LSI significantly had a notably positive impact on reducing BMI for the participants with an initial BMI of less than 35.0 kg/m2 (DM = −1.82 kg/m2, 95% CI -2.91 to −0.72, n = 5, p = 0.001). This beneficial effect was also observed for more obese individuals with a BMI over 35.0 kg/m2 (DM = −1.56 kg/m2, 95% CI -2.93 to −0.19, n = 4, p = 0.025).
Waist circumference
The meta-analysis of nine studies with a total of 749 patients showed a beneficial effect (DM = −3.34 cm, 95% CI -5.06 to −1.63, df = 8; p = 0.001) on WC management. The evidence was graded as high quality.
Effect of LSI on blood-related parameters
The meta-analysis of five studies with a total of 183 patients showed no beneficial effect on blood glucose (DM = −0.19 mmoL/L, 95% CI -0.29 to −0.09, df = 4; p < 0.001), insulin (DM = −0.98 mU/L, 95% CI -2.23 to 0.28, df = 4; p = 0.127), HOMA-IR (DM = −0.01, 95% CI -0.45 to 0.43, df = 5; p = 0.974), testosterone (DM = −0.12 nmoL/L, 95% CI -0.02 to 0.23, df = 4; p = 0.024), and FAI index management (DM = −0.53, 95% CI -1.91 to 0.86, df = 2; p = 0.457), respectively. However, a beneficial effect was found for SHBG (DM = −5.55 nmoL/L, 95% CI -1.89 to −9.211, df = 4; p = 0.003). The quality of evidence for all parameters investigated was downgraded to moderate due to imprecision or moderate to high heterogeneity (Table 2).
Effect of LSI on ovulation, pregnancy, and live birth incidence
The meta-analysis of four studies with a total of 123 patients showed a beneficial effect of LSI on ovulation (OR = 11.23, 95% CI 2.51 to 50.23, df = 3; p = 0.002), pregnancy (OR = 1.49, 95% CI 1.04 to 2.15, df = 10; p = 0.032, I2 = 44%), and live births (OR = 1.51, 95% CI 0.92 to 2.47, df = 8; p = 0.099; I2 = 65%), respectively. The evidence for ovulation was downgraded from high to moderate due to the reported imprecision (sample size <300), while data on pregnancy were rated as high-quality evidence.
Table 3 shows the results of the meta-regression analysis for two categories of variables: (a) patient-related (initial age, weight, and BMI) and (b) training variables such as training volume (i.e., period, weekly frequency, total number of training sessions) and time spent in training (i.e., duration of a single training session). No significant predictors were found for weight reduction following LSI.
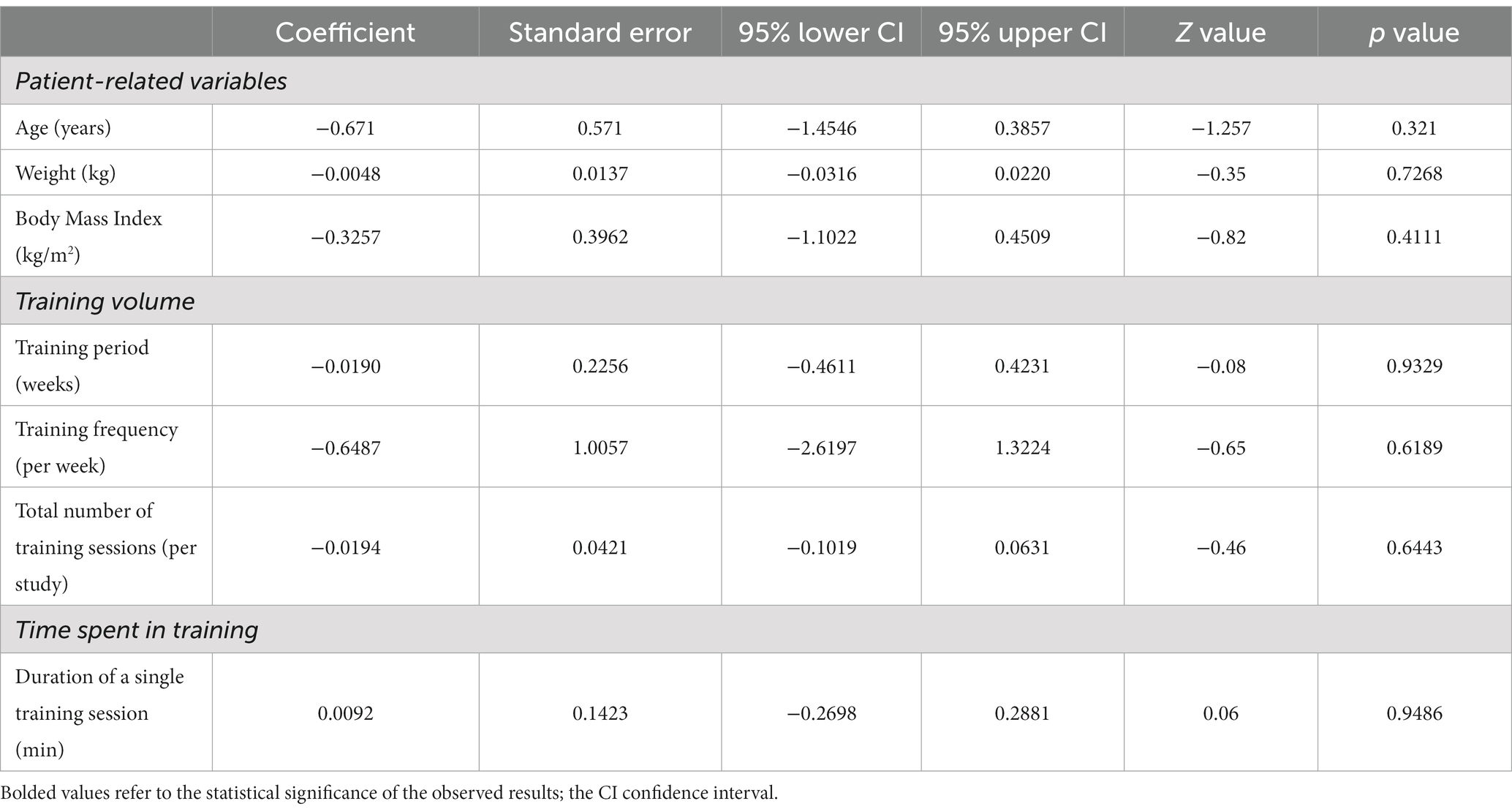
Table 3. Meta-regression for patient-related and training variables of different subscales to predict intervention effect on weight management.
Meta-regression analysis for patient-related and training variables in pregnancy
Table 4 shows the results of the meta-regression analysis for two categories of variables: (a) patient-related (initial age and BMI) and (b) training variables such as training volume (i.e., period, weekly frequency, and total number of training sessions) and time spent in training (i.e., duration of a single training session). It was found that a training period (weeks) is a predictor of successful pregnancy following LSI.
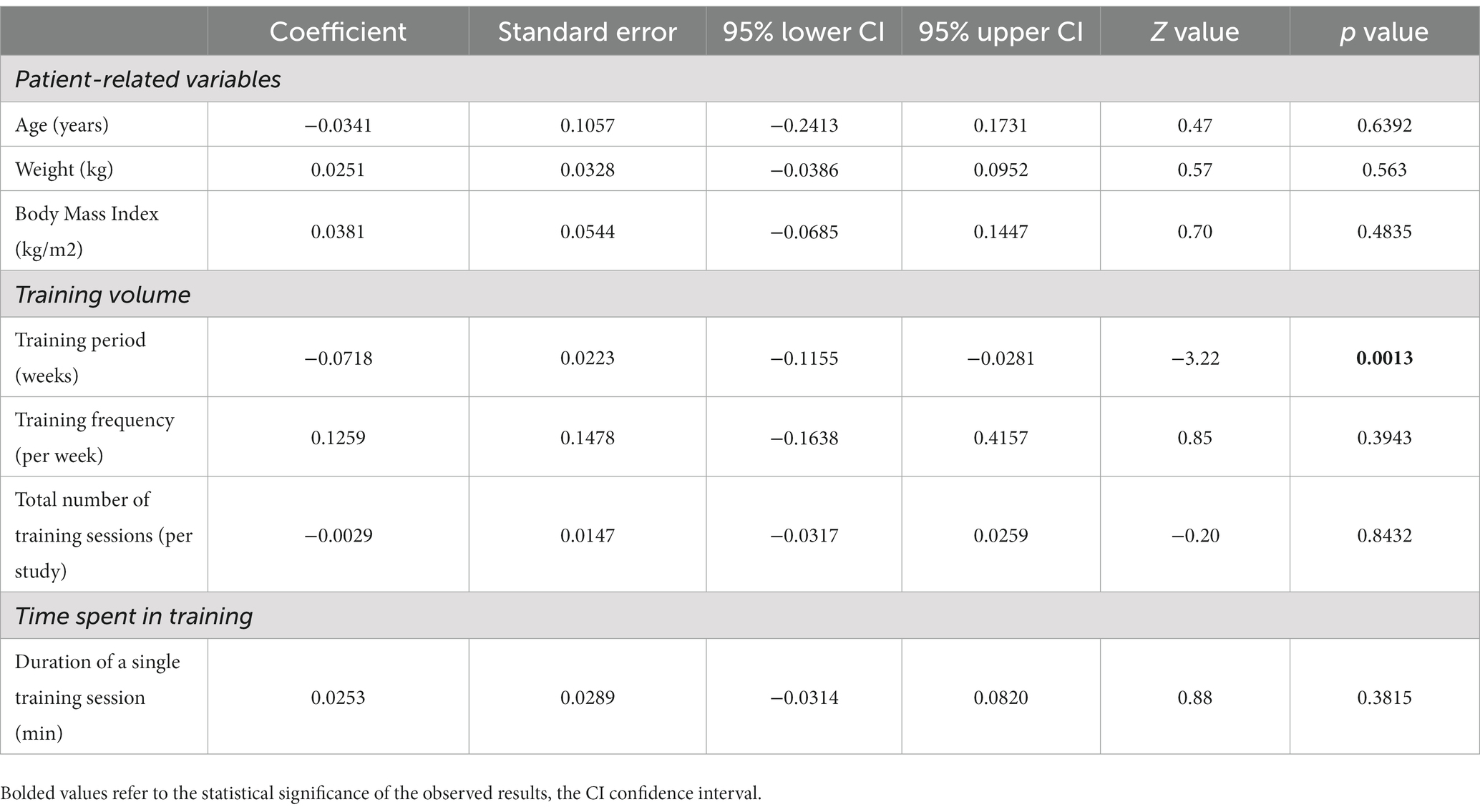
Table 4. Meta-regression for patient-related and training variables of different subscales to predict intervention effect on pregnancy.
Discussion
In this systematic review and meta-analysis, 576 journals were screened, and 10 articles were selected. During an additional literature review conducted in December 2022, 498 journal articles were screened. Of these, five articles were selected for their qualitative insights on LSI and infertility intervention in overweight and obese women. Only a limited number of articles specifically explored the relationship between LSI, female infertility, and obesity. Furthermore, only a few studies followed the included subjects for a longer period of time so that long-term results on pregnancy and live births were also visible. The results of the present meta-analysis indicate that LSI can be an effective treatment for weight management, as evidenced by decreased weight (DM = −3.52 kg, p = 0.024), BMI (DM = −1.75 kg/m2, p < 0.001), and WC (DM = −3.34 cm, p = 0.001) after LSI. Moreover, we observed positive effects of LSI on increasing ovulation and pregnancy rates in overweight women with infertility. Furthermore, a meta-regression analysis showed no significant predictors among the related variables for the effect of LSI on weight management.
Our results are in line with previously published studies showing that LSI is efficient in reducing body weight (15, 33): for 12 of the 15 included studies, the reduction ranged from 0.7 to 12.9%, while in the control group, the average weight loss ranged from 0.1 to 8.4%. However, one study also found a weight gain (34). Additional subgroup analysis showed that the initial BMI of the participants was not a significant moderator of those effects (Q = 0.001; p = 0.980). On the contrary, the summarized effects of a pairwise comparison showed that the initial BMI of participants may influence the overall decrease in weight after LSI. Data processing was performed separately for two groups according to the initial BMI level, namely for subjects with a BMI below 35.0 kg / m2 and a BMI above 35.0 kg / m2. For subjects with a BMI below 35.0 kg / m2, the BMI decreased, but not significantly (DM = −3.62 kg, p = 0.109), while for the subjects in the group with a BMI above 35.0 kg / m2, the BMI decreased significantly (DM = −3.69 kg, p = 0.019). This raises the question of what kind of intervention and lifestyle change would be most appropriate for women with a BMI below 35.0 kg/m2. Moreover, the form of exercise (including type, volume, and intensity) and progression should probably be more frequent and/or intense for women with a BMI below 35.0 kg/ m2 than for women with a BMI above 35.0 kg/ m2, as tailored exercise could lead to a greater reduction in weight and BMI.
WC was reported in 9 of the 15 studies, and the meta-analytic approach showed a reduction of WC in the experimental group on average from 1.4 to 12.2%, while in the control group, there was an average reduction between 0.0 and 10.6%. Phy et al. previously showed that an 8-week and 12-week weight loss intervention in overweight and obese women with PCOS has an effect on reduction in WC and consequently improved insulin sensitivity, reduced testosterone, and improved fertility (35, 36).
Regular PA has been found to increase SHBG levels (37), and low serum SHBG levels are considered a relevant biomarker of abnormal metabolism and are related to insulin resistance and abnormalities in glucose and lipid metabolism (38). Previously published meta-analyses showed that LSI does impact SHBG, which was reported in five studies (20, 39–42).
In 4 of the 15 studies in the present meta-analysis, LSI was shown to have a beneficial effect on ovulation, and in 11 of the 15 studies on the pregnancy of overweight and obese women diagnosed with infertility. The LSI group had 11.23 times more ovulatory incidence than the control group, which in turn increased the ability to conceive. Furthermore, it was established that a 2–5% reduction in body weight has been associated with the restoration of ovulation (43). Accordingly, the proportion of pregnancies was higher in the intervention group, as almost a fifth of the subjects became pregnant, that is, 18.40%. In the LSI group, there was a higher proportion of live births: 17.83%.
Our findings are consistent with the systematic reviews already carried out. However, our analysis differs from the previous studies (7, 11, 15) because here we used the meta-analytic approach to identify various LSIs to explore their effects on fertility factors. LSI includes various components, and a variation was observed even in the length of LSI included in the presented MA. The mean length of LSI was 14.2 weeks, with the shortest intervention being 4 weeks (44) and the longest being 24 weeks (19, 45, 46), with 12 and 16 weeks being the most common durations. PA was part of the intervention in the fourteen studies included, but they were very differently defined. Ten LSI involved only aerobic exercises such as walking, brisk walking, jogging, or similar activity (18, 19, 39, 42, 44, 45, 47–50), two interventions involved structured exercise training (20, 41), one intervention included both aerobic and resistance training (51), and two did not specify the type of exercise intervention (34, 40). Three interventions with aerobic exercise were defined as 10,000 steps per day (19, 44, 48).
Pharmacological treatment was used in 2 intervention groups and 6 control groups out of the 15 included studies. In three of the 15 intervention groups and one control group, psychological or behavioral advice was provided to the subjects and performed by a health professional (34). Psychotherapy can be an important intervention that should be recommended for couples suffering from any form of infertility.
In addition to the intervention and control groups, 3 out of 15 studies had a second experimental group (20, 39, 47), and one intervention had an active control group (18). However, the present study’s focus was on comparing the LSI and control groups, even though several comparisons between studies were possible. At the same time, this might be one of the limitations of the present meta-analysis.
It should be mentioned that some of the selected studies had additional groups not addressed in the present analysis: 3 out of 15 studies had a third test group (20, 39, 47), and one intervention had a real control group (18). Since the focus of the present study was on comparing the LSI and control groups, it was decided that additional comparisons between studies were not performed. This is one of the limitations of the present meta-analysis.
When it comes to the issue of infertility, it is necessary to mention two aspects that were not known in the past, but their understanding and influence can help in comprehending the problem of infertility in the future. Scientists have determined that COVID-19 has had and continues to have an effect on the reproductive health of both women and men. Angiotensin-converting enzyme 2 (ACE2), a functional receptor for SARS-CoV-2, is a key component of the renin-angiotensin (SRA) system that modulates the cleavage of angiotensin II (Ang II) and Ang (1–7). Upon cell invasion, COVID-19 disrupts SRA by reducing ACE2 expression in host cells, leading to an increased Ang II inflammatory response (52). Ang II, ACE2, and Ang (1–7) regulate basic functions in the female and male reproductive systems. In women, this includes folliculogenesis, steroidogenesis, oocyte maturation, ovulation, and endometrial regeneration (53). According to the researchers, knowing the effect of the virus on fertility also changes and adapts infertility treatment (54), which slowed down a bit during the pandemic as clinics that perform artificial insemination procedures had stopped or limited treatment (55, 56).
Artificial intelligence (AI) has been widely applied in the field of reproductive health to enhance diagnosis, treatment, and overall healthcare delivery. Medenica et al. have found that AI has proven to be a very important and effective tool that will bring great innovation to the field of reproductive medicine. There are many ways in which artificial intelligence affects reproductive health: medical imaging and diagnostics (analyze medical images, MRIs, etc., to assist in detecting conditions), ART (AI can optimize and predict the success rate of IVF), customized and individualized treatment plans (based on patients’ medical histories and genetic information), and fertility tracking and predictions (to optimize timing for conception) (57, 58).
Limitations and research recommendations
The advantage of the present research was the narrow and precise inclusion criteria, with which a small number of studies with comparable LSI were obtained. A meta-analysis was performed for each factor, using the PEDro scale to assess the reporting quality of randomized controlled trials and the TIDieR rating for reporting details of the intervention elements of a study.
The present review is limited because the studies and LSI parameters are very diverse. Consequently, the selection presented difficulties for comparison. Moreover, as there was a range of types of PA inside each LSI, it is not obvious which type of PA can improve fertility and better influence reproductive health. Only a few studies have defined PA as FITT (frequency, intensity, time or duration, and type). For future research, it is suggested that the PA with the acronym FITT be precisely defined, allowing other researchers to perform the exercise. In addition, it would be of great interest for research and practice to directly compare the effects of LSI on the body anthropometrics of subjects with BMIs above and below 35.0 kg/m2, as the results from the present meta-analysis showed inconclusive findings. Thus, these results must be interpreted with caution as the group comparison did not achieve a level of significance (Q = 0.001, p = 0.980), while pairwise comparisons did for women with BMI ≥35 kg/m2 (DM = −3.69 kg, p = 0.019) but not for those with less than 35 kg/m2 of the initial BMI (DM = −3.62 kg, p = 0.109). Thus, it is necessary to define the form and progression of the exercise, which probably should be different for women with a BMI above and below 35.0 kg/m2 when weight loss is a primary goal. Moreover, it would be of great interest to assess the adherence to an intervention in relation to LSI effectiveness in weight management. For future research, it is suggested that LSI be defined in greater detail, structured more carefully to suit the participants’ characteristics, and conducted over a longer period. The suggested modifications might lead to a greater effect of LSI, which consequently means that, in the case of appropriate findings, they could be implemented in practice and healthcare.
We would like to emphasize that an investigation of motor skills combined with BMI might provide further insights into the LS-fertility association and, in that sense, whether physical fitness parameters might be relevant biomarkers that can describe the risk of infertility.
Conclusion
The findings of the present meta-analysis LSI (PA, diet, pharmacological treatment, or psychological advice) may have beneficial effects on some reproductive health outcomes in overweight and obese women with diagnosed infertility. The present meta-analysis showed that LSI has a beneficial effect on anthropometric measures (weight, BMI, and WC) and no beneficial effect on blood-related parameters, except SHBG. Moreover, the beneficial effects of the LSI were established as improved ovulation, a higher chance of pregnancy, and live births for overweight and obese infertile women.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
AS: Conceptualization, Data curation, Investigation, Project administration, Writing – original draft, Writing – review & editing. VH: Conceptualization, Writing – review & editing. CJWM: Data curation, Supervision, Validation, Visualization, Writing – review & editing. EA: Data curation, Validation, Writing – review & editing. MV: Funding acquisition, Resources, Validation, Writing – review & editing. TBP: Supervision, Validation, Writing – review & editing. AP: Conceptualization, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing, Data curation, Supervision, Validation.
Funding
The author(s) declare that no financial support was received for the research, and authorship. This research was conducted under research programme KINESIOLOGY OF MONOSTRUCTURAL, POLYSTRUCTURAL AND CONVENTIONAL SPORTS (Project number P5-0147), which also covered the cost of the open access publication of this article.
Acknowledgments
CJWM’s contribution was co-financed by ARRS Research Program P5-0381: Kinesiology for Quality of Life.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
BMI, body mass index; PCOS, polycystic ovary syndrome; LSI, lifestyle interventions; IVF, in vitro fertilization; WC, waist circumference; PA, physical activity; CI, confidence intervals; OR, odds ratio.
References
1. Vander Borght, M, and Wyns, C. Fertility and infertility: definition and epidemiology. Clin Biochem. (2018) 62:2–10. doi: 10.1016/J.CLINBIOCHEM.2018.03.012
3. Sormunen, T, Aanesen, A, Fossum, B, Karlgren, K, and Westerbotm, M. Infertility-related communication and coping strategies among women affected by primary or secondary infertility. J Clin Nurs. (2018) 27:335–44. doi: 10.1111/JOCN.13953
4. Vasilopoulos, E, Fragkiadaki, P, Kalliora, C, Fragou, D, Docea, A, Vakonaki, E, et al. The association of female and male infertility with telomere length (review). Int J Mol Med. (2019) 44:375–89. doi: 10.3892/IJMM.2019.4225
5. Kalima-munalula, MN, Ahmed, Y, and Vwalika, B. Factors associated with infertility among women attending the gynaecology clinic at university teaching hospital, Lusaka, Zambia. Med J Zambia. (2017) 44:41–4. doi: 10.55320/mjz.44.1.58
6. Silvestris, E, Lovero, D, and Palmirotta, R. Nutrition and female fertility: an interdependent correlation. Front Endocrinol (Lausanne). (2019) 10:00346. doi: 10.3389/fendo.2019.00346
7. Homan, GF, Davies, M, and Norman, R. The impact of lifestyle factors on reproductive performance in the general population and those undergoing infertility treatment: a review. Hum Reprod Update. (2007) 13:209–23. doi: 10.1093/humupd/dml056
8. Penzias, A, Bendikson, K, Butts, S, Coutifaris, C, Falcone, T, Gitlin, S, et al. Smoking and infertility: a committee opinion. Fertil Steril. (2018) 110:611–8. doi: 10.1016/J.FERTNSTERT.2018.06.016
9. Orton, F, Säfholm, M, Jansson, E, Carlsson, Y, Eriksson, A, Fick, J, et al. Exposure to an anti-androgenic herbicide negatively impacts reproductive physiology and fertility in Xenopus tropicalis. Sci Rep. (2018) 8:9124–15. doi: 10.1038/s41598-018-27161-2
10. the LIFEstyle study groupKarsten, MDA, van Oers, AM, Groen, H, Mutsaerts, MAQ, van Poppel, MNM, et al. Determinants of successful lifestyle change during a 6-month preconception lifestyle intervention in women with obesity and infertility. Eur J Nutr. (2019) 58:2463–75. doi: 10.1007/s00394-018-1798-7
11. Nelson, SM, and Fleming, RF. The preconceptual contraception paradigm: obesity and infertility. Hum Reprod. (2007) 22:912–5. doi: 10.1093/humrep/del473
12. Pasquali, R, Pelusi, C, Genghini, S, Cacciari, M, and Gambineri, A. Obesity and reproductive disorders in women. Hum Reprod Update. (2003) 9:359–72. doi: 10.1093/humupd/dmg024
13. Silvestris, E, de Pergola, G, Rosania, R, and Loverro, G. Obesity as disruptor of the female fertility. Reprod Biol Endocrinol. (2018) 16. doi: 10.1186/s12958-018-0336-z
14. Talmor, A, and Dunphy, B. Female obesity and infertility. Best Pract Res Clin Obstet Gynaecol. (2015) 29:498–506. doi: 10.1016/j.bpobgyn.2014.10.014
15. Mena, GP, Mielke, GI, and Brown, WJ. The effect of physical activity on reproductive health outcomes in young women: a systematic review and meta-analysis. Hum Reprod Update. (2019) 25:542–64. doi: 10.1093/humupd/dmz013
16. Cong, J, Li, P, Zheng, L, and Tan, JT. Prevalence and risk factors of infertility at a rural site of northern China. PLoS One. (2016) 11:1–12. doi: 10.1371/journal.pone.0155563
17. Gholinezhad, M, Gholsorkhtabaramiri, M, Esmaeilzadeh, S, and Ghanbarpour, A. Insulin resistance and adverse metabolic profile in overweight/obese and normal weight of young women with polycystic ovary syndrome. Casp J Intern Med. (2018) 9:260–7. doi: 10.22088/cjim.9.3.260
18. Legro, RS, Dodson, WC, Kris-Etherton, PM, Kunselman, AR, Stetter, CM, Williams, NI, et al. Randomized controlled trial of preconception interventions in infertile women with polycystic ovary syndrome. J Clin Endocrinol Metab. (2015) 100:4048–58. doi: 10.1210/jc.2015-2778
19. Mutsaerts, MAQ, van Oers, AM, Groen, H, Burggraaff, JM, Kuchenbecker, WKH, Perquin, DAM, et al. Randomized trial of a lifestyle program in obese infertile women. N Engl J Med. (2016) 374:1942–53. doi: 10.1056/NEJMoa1505297
20. Palomba, S, Falbo, A, Giallauria, F, Russo, T, Rocca, M, Tolino, A, et al. Six weeks of structured exercise training and hypocaloric diet increases the probability of ovulation after clomiphene citrate in overweight and obese patients with polycystic ovary syndrome: a randomized controlled trial. Hum Reprod. (2010) 25:2783–91. doi: 10.1093/humrep/deq254
21. van Elten, T, Karsten, MDA, Geelen, A, Gemke, RJBJ, Groen, H, Hoek, A, et al. Preconception lifestyle intervention reduces long term energy intake in women with obesity and infertility: a randomised controlled trial. Int J Behav Nutr Phys Act. (2019) 16:1–10. doi: 10.1186/s12966-018-0761-6
22. Harrison, CL, Brown, WJ, Hayman, M, Moran, LJ, and Redman, LM. The role of physical activity in preconception, pregnancy and postpartum health. Semin Reprod Med. (2016) 34:e28–37. doi: 10.1055/S-0036-1583530
23. Hakimi, O, and Cameron, LC. Effect of exercise on ovulation: a systematic review. Sports Med. (2017) 47:1555–67. doi: 10.1007/s40279-016-0669-8
24. Wise, LA, Rothman, KJ, Mikkelsen, EM, Sorensen, HT, Riis, AH, and Hatch, EE. A prospective cohort study of physical activity and time to pregnancy. Fertil Steril. (2012) 97:1136–1142.e4. doi: 10.1016/j.fertnstert.2012.02.025
25. Moher, D, Liberati, A, Tetzlaff, J, and Altman, DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/JOURNAL.PMED.1000097
26. Maher, C. G., Sherrington, C., Herbert, R. D., Moseley, A. M., and Elkins, M., “Reliability of the PEDro scale for rating quality of randomized controlled trials,” (2003).. [Online]. Available at: https://academic.oup.com/ptj/article-abstract/83/8/713/2805287.
27. Hoffmann, TC, Glasziou, PP, Boutron, I, Milne, R, Perera, R, Moher, D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. Gesundheitswesen. (2016) 78:175–88. doi: 10.1055/s-0041-111066
28. Guyatt, GH, Oxman, AD, Vist, GE, Kunz, R, Falck-Ytter, Y, Alonso-Coello, P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. (2008) 336:924–6. doi: 10.1136/BMJ.39489.470347.AD
29. Guyatt, GH, Oxman, AD, Kunz, R, Brozek, J, Alonso-Coello, P, Rind, D, et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J Clin Epidemiol. (2011) 64:1283–93. doi: 10.1016/J.JCLINEPI.2011.01.012
31. Hopkins, WG, Marshall, SW, Batterham, AM, and Hanin, J. Progressive statistics for studies in sports medicine and exercise science. Med Sci Sports Exerc. (2009) 41:3–12. doi: 10.1249/MSS.0b013e31818cb278
32. Yamato, TP, Maher, CG, Saragiotto, BT, Hoffmann, TC, and Moseley, AM. How completely are physiotherapy interventions described in reports of randomised trials? Physiother. (2016) 102:121–6. doi: 10.1016/j.physio.2016.03.001
33. Hoek, A, Wang, Z, van Oers, AM, Groen, H, and Cantineau, AEP. Effects of preconception weight loss after lifestyle intervention on fertility outcomes and pregnancy complications. Fertil Steril. (2022) 118:456–62. doi: 10.1016/j.fertnstert.2022.07.020
34. Einarsson, S, Bergh, C, Friberg, B, Pinborg, A, Klajnbard, A, Karlström, PO, et al. Weight reduction intervention for obese infertile women prior to IVF: a randomized controlled trial. Hum Reprod. (2017) 32:1621–30. doi: 10.1093/humrep/dex235
35. Šuštaršič, A, Vrtačnik Bokal, E, and Burnik Papler, T. The impact of COVID-19 lockdown on weight loss program in infertile polycystic ovary syndrome women with obesity. Obes Facts. (2021) 14:650–7. doi: 10.1159/000519946
36. Phy, JL, Pohlmeier, AM, Cooper, JA, Watkins, P, Spallholz, J, Harris, KS, et al. Low starch/low dairy diet results in successful treatment of obesity and co-morbidities linked to polycystic ovary syndrome (PCOS). J Obes Weight Loss Ther. (2015) 5:1000259. doi: 10.4172/2165-7904.1000259
37. Orio, F., Muscogiuri, G., Ascione, A., Marciano, F., Volpe, A., La Sala, G., et al. “Effects of physical exercise on the female reproductive system - PubMed,” Minerva Endorinologica, vol. 38, no. 3, pp. 305–319, (2013), Accessed: May 29, 2020. [Online]. Available at: https://pubmed.ncbi.nlm.nih.gov/24126551/
38. Zhu, JL, Chen, Z, Feng, WJ, Long, SL, and Mo, ZC. Sex hormone-binding globulin and polycystic ovary syndrome. Clin Chim Acta. (2019) 499:142–8. doi: 10.1016/J.CCA.2019.09.010
39. Thomson, RL, Buckley, JD, Noakes, M, Clifton, PM, Norman, RJ, and Brinkworth, GD. The effect of a hypocaloric diet with and without exercise training on body composition. J Clin Endocrinol Metab. (2008) 93:3373–80. doi: 10.1210/jc.2008-0751
40. Becker, GF, Passos, EP, and Moulin, CC. Short-term effects of a hypocaloric diet with low glycemic index and low glycemic load on body adiposity, metabolic variables, ghrelin, leptin, and pregnancy rate in overweight and obese infertile women: a randomized controlled trial. Am J Clin Nutr. (2015) 102:1365–72. doi: 10.3945/AJCN.115.117200
41. Kiel, IA, Lundgren, KM, Mørkved, S, Kjøtrød, SB, Salvesen, Ø, Romundstad, LB, et al. Women undergoing assisted fertilisation and high-intensity interval training: a pilot randomised controlled trial. BMJ Open Sport Exerc Med. (2018) 4:e000387. doi: 10.1136/BMJSEM-2018-000387
42. Legro, RS, Hansen, KR, Diamond, MP, Steiner, AZ, Coutifaris, C, Cedars, MI, et al. Effects of preconception lifestyle intervention in infertile women with obesity: the FIT-PLESE randomized controlled trial. PLoS Med. (2022) 19:e1003883. doi: 10.1371/JOURNAL.PMED.1003883
43. Best, D, and Bhattacharya, S. Obesity and fertility. Horm Mol Biol Clin Investig. (2015) 24:5–10. doi: 10.1515/HMBCI-2015-0023
44. Nagelberg, J, Burks, H, Mucowski, S, and Shoupe, D. The effect of home exercise on ovulation induction using clomiphene citrate in overweight underserved women with polycystic ovarian syndrome. Contracept Reprod Med. (2016) 1:14–5. doi: 10.1186/s40834-016-0025-2
45. Galletly, C, Clark, A, Tomlinson, L, and Blaney, F. A group program for obese, infertile women: weight loss and improved psychological health. J Psychosom Obstet Gynaecol. (1996) 17:125–8. doi: 10.3109/01674829609025672
46. van Dammen, L, Wekker, V, van Oers, AM, Mutsaerts, MAQ, Painter, RC, Zwinderman, AH, et al. Effect of a lifestyle intervention in obese infertile women on cardiometabolic health and quality of life: a randomized controlled trial. PLoS One. (2018) 13:e0190662. doi: 10.1371/journal.pone.0190662
47. Dokras, A, Sarwer, DB, Allison, KC, Milman, L, Kris-Etherton, PM, Kunselman, AR, et al. Weight loss and lowering androgens predict improvements in health-related quality of life in women with PCOS. J Clin Endocrinol Metab. (2016) 101:2966–74. doi: 10.1210/jc.2016-1896
48. Sim, KA, Dezarnaulds, GM, Denyer, GS, Skilton, MR, and Caterson, ID. Weight loss improves reproductive outcomes in obese women undergoing fertility treatment: A randomized controlled trial. Clin Obes. (2014):61–8. doi: 10.1111/cob.12048
49. Espinós, JJ, Polo, A, Sánchez-Hernández, J, Bordas, R, Pares, P, Martínez, O, et al. Weight decrease improves live birth rates in obese women undergoing IVF: a pilot study. Reprod Biomed Online. (2017) 35:417–24. doi: 10.1016/J.RBMO.2017.06.019
50. Rothberg, A, Lanham, M, Randolph, J, Fowler, C, Miller, N, and Smith, Y. Feasibility of a brief, intensive weight loss intervention to improve reproductive outcomes in obese, subfertile women: a pilot study. Fertil Steril. (2016) 106:1212–20. doi: 10.1016/J.FERTNSTERT.2016.06.004
51. Moran, L, Tsagareli, V, Norman, R, and Noakes, M. Diet and IVF pilot study: short-term weight loss improves pregnancy rates in overweight/obese women undertaking IVF. Aust New Zeal J Obstet Gynaecol. (2011) 51:455–9. doi: 10.1111/j.1479-828X.2011.01343.x
52. Madjunkov, M, Dviri, M, and Librach, C. A comprehensive review of the impact of COVID-19 on human reproductive biology, assisted reproduction care and pregnancy: a Canadian perspective. J Ovarian Res. (2020) 13:140. doi: 10.1186/S13048-020-00737-1
53. Reis, FM, Bouissou, DR, Pereira, VM, Camargos, AF, Dos Reis, AM, and Santos, RA. Angiotensin-(1-7), its receptor mas, and the angiotensin-converting enzyme type 2 are expressed in the human ovary. Fertil Steril. (2011) 95:176–81. doi: 10.1016/J.FERTNSTERT.2010.06.060
54. Basile, G, Billone, V, and Umani Ronchi, F. COVID-19 and its aftermath, new drivers of infertility? Clin Ter. (2023) 174:343–4. doi: 10.7417/CT.2023.2448
55. Cutting, E, Catt, S, Vollenhoven, B, Mol, BW, and Horta, F. The impact of COVID-19 mitigation measures on fertility patients and clinics around the world. Reprod Biomed Online. (2022) 44:755–63. doi: 10.1016/J.RBMO.2021.12.016
56. Ory, SJ, Miller, KA, Horton, M, and Giudice, L. The global impact of COVID-19 on infertility services. Glob Reprod Heal. (2020) 5:e43–3. doi: 10.1097/GRH.0000000000000043
57. Medenica, S, Zivanovic, D, Batkoska, L, Marinelli, S, Basile, G, Perino, A, et al. The future is coming: artificial intelligence in the treatment of infertility could improve assisted reproduction outcomes—the value of regulatory frameworks. Diagnostics. (2022) 12:12122979. doi: 10.3390/diagnostics12122979
Keywords: physical activity, infertility, intervention, overweight, pregnancy, ovulation
Citation: Sustarsic A, Hadzic V, Meulenberg CJW, Abazovic E, Videmsek M, Burnik Papler T and Paravlic AH (2023) The influence of lifestyle interventions and overweight on infertility: a systematic review, meta-analysis, and meta-regression of randomized controlled trials. Front. Med. 10:1264947. doi: 10.3389/fmed.2023.1264947
Edited by:
Roland Eghoghosoa Akhigbe, Ladoke Akintola University of Technology, NigeriaReviewed by:
Roger D. Jones, Ca 'Foscari University of Venice, ItalyGiuseppe Basile, IRCCS Istituto Ortopedico Galeazzi, Italy
Copyright © 2023 Sustarsic, Hadzic, Meulenberg, Abazovic, Videmsek, Burnik Papler and Paravlic. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Armin H. Paravlic, YXJtaW4ucGFyYXZsaWNAZnNwLnVuaS1sai5zaQ==