 Balázs Mészáros
Balázs Mészáros Dániel S. Veres2
Dániel S. Veres2 Zoltán Kukor
Zoltán Kukor Sándor Valent
Sándor Valent- 1Department of Obstetrics and Gynecology, Semmelweis University, Budapest, Hungary
- 2Department of Biophysics and Radiation Biology, Semmelweis University, Budapest, Hungary
- 3Dél-Pest Centrum Hospital National Hematology and Infectious Diseases Institute, Budapest, Hungary
- 4Department of Molecular Biology, Institute of Biochemistry and Molecular Biology, Semmelweis University, Budapest, Hungary
Objective: Meta-analysis focusing on the role of first-trimester neutrophil-to-lymphocyte ratio (NLR) in the prediction of preeclampsia.
Data sources: PubMed, Scopus, Web of Science, Cochrane Library, and Embase databases were queried from inception up to December 31, 2022.
Study eligibility criteria: The study included all types of original research that was conducted in humans and values of NLR were measured during the first trimester, among patients who later developed preeclampsia, compared to the values of control groups.
Study appraisal and synthesis methods: Two reviewers independently performed data abstraction and quality appraisal, and disagreements were resolved by consensus and, if necessary, by the opinion of a third reviewer. During the analysis, PRISMA and MOOSE guidelines were followed. All statistical analyses were made with R.
Results: For the research on the predictive role of NLR values in the first trimester for preeclampsia, a total of 6 studies were selected for analysis, covering 2,469 patients. The meta-analysis revealed a 95% confidence interval (CI) for the effect size of 0.641 to 1.523, with a prediction interval of 0.027 to 2.137.
Conclusion: Based on the analysis, NLR is a promising biochemical marker for future pieces of research that try to find new screening methods for first-trimester preeclampsia. We encourage other researchers to examine NLR’s predictive value combined with other markers in preeclampsia screening, this way being able to find new and affordable protocols for first-trimester preeclampsia screening.
Systematic review registration: identifier CRD42023392663.
1 Introduction
Preeclampsia is a pregnancy-specific disorder, and it was defined for decades by the new onset of hypertension and proteinuria. According to the latest guidelines such as NICE (National Institute for Health and Care Excellence) and ISSHP (International Society for the Study of Hypertension in Pregnancy) proteinuria is not mandatory for the diagnosis of preeclampsia: according to NICE -preeclampsia is characterized by the onset of new hypertension after 20 weeks of pregnancy, accompanied by one or more newly emerging features: these features may include substantial proteinuria or maternal organ dysfunction, such as renal insufficiency, liver involvement, neurological complications, or hematological complications (1, 2). By the definition of - ISSHP, which closely resembles NICE’s definition—pre-eclampsia is diagnosed when new-onset hypertension (systolic blood pressure >140 mmHg, diastolic blood pressure >90 mmHg) occurs after 20 weeks of pregnancy, accompanied by at least one additional symptom or group of symptoms, which may include: proteinuria; dysfunction of other maternal organs (such as liver, kidney, central nervous system); hematological abnormalities; uteroplacental dysfunction (e.g., intrauterine growth restriction—IUGR, and/or abnormal Doppler ultrasound results concerning uteroplacental circulation) (3). Preeclampsia affects 2–8% of pregnant women and is one of the leading causes of maternal and neonatal morbidity and mortality in the world, particularly in low-income countries (4–6). According to WHO, in developing countries, 16% of maternal deaths are attributed to hypertensive disorders, and the reduction of maternal mortality is a global goal (7, 8). Despite its significant impact on obstetrics and healthcare in general, preeclampsia has remained an enigmatic field of medicine. However, recently, new preventive and screening methods have been tested (9).
The early identification of patients at high risk for preeclampsia can be crucial for achieving significantly improved maternal and perinatal outcomes. This involves providing closer surveillance, considering prophylactic use of low-dose aspirin therapy, administering antihypertensive medications, and opting for earlier induced delivery (10, 11).
Since inflammatory reactions are suggested behind the pathomechanism of preeclampsia (12–16) in recent years publications have been evaluating the role of white blood cells both in clinical studies and animal models in the prediction of preeclampsia (17, 18). The distribution of white blood cells can be monitored through the neutrophil-to-lymphocyte ratio (NLR), which has been found to be a useful marker for inflammatory diseases such as systemic lupus erythematosus (SLE), spondyloarthritis, psoriasis, psoriatic arthritis, various types of tumors, and Takayasu arteritis (TA) (19–25). There have also been studies that evaluated the role of NLR in pregnancy-related diseases (26, 27). Moreover, in recent years, several meta-analyses have been published that found elevated NLRs in blood samples from mothers who experienced preeclampsia (28, 29).
The fact that laboratory findings are widely affordable and accessible even in developing countries (30, 31) and neutrophil and lymphocyte counts are usually part of routine laboratory tests (32) are other reasons why NLR would provide beneficial predictive value in preeclampsia.
2 Object
This current meta-analysis aims to evaluate the role that first-trimester NLR values can play in preeclampsia screening.
3 Methods
3.1 Eligibility criteria, information sources, search strategy
The data for the meta-analysis were collected by two independent researchers from PubMed, Scopus, Web of Science, Cochrane Library, and Embase databases. Disagreements were resolved through consensus and, if necessary, by the opinion of a third reviewer. The database searches were conducted until December 31, 2022, without any additional time restrictions. Language restrictions were not applied.
For the preparation and planning of this analysis, a PRISMA checklist and the MOOSE method were utilized (33, 34).
3.2 Study selection
For this research, the keywords “NLR” supplemented with “preeclampsia” were used. Each search was conducted across five online medical databases: PubMed, Cochrane Library, Scopus, Embase, and Web of Science. During the screening process, the research group aimed to select studies that reported NLR values in the first trimester of pregnancy in women who later developed preeclampsia. These values were compared to control groups consisting of women who remained normotensive and free of obstetrical complications during their pregnancies.
3.3 Data extraction
From the studies collected for further review, the following data were extracted: the study objective; the number of mild preeclamptic patients included in the study; the number of severe preeclamptic patients included in the study; the total number of preeclamptic patients included in the study; the number of control (healthy, normotensive) pregnant patients; the time of data collection (trimester, weeks); NLR values of mild preeclamptic patients and their corresponding standard deviations; NLR values of severe preeclamptic patients and their corresponding standard deviations; NLR values of preeclamptic patients and their corresponding standard deviations; NLR values of healthy, normotensive patients (control group) and their corresponding standard deviations; and p-values. Additionally, both researchers collected the articles’ titles, authors, publication years, publishers, and DOIs.
3.4 Assessment of risk of bias
The Newcastle–Ottawa scale (NOS) (35) was used to assess the quality of the included studies. The quality assessment was conducted independently by two authors, with any disagreements resolved through consensus or, if necessary, by involving a third author. The NOS evaluates articles based on three main factors: the selection of study groups, the comparability of groups, and the ascertainment of exposure, assigning scores ranging from 0 to 9. A score of 0 represents the worst possible quality, while 9 indicates the best possible quality. Studies scoring 0–4 stars are considered low quality, while those receiving 5 or more stars are deemed moderate to high quality. According to the authors, all the included articles received 6 or more stars on the NOS.
3.5 Data synthesis
Mean difference (MD) with a 95% confidence interval (CI) was used to express the effect size. To calculate the mean difference the number of patients, the mean, and standard deviation (SD) of the variable of interest for the “preeclampsia” and “without preeclampsia” (i.e., control) groups were extracted from the studies. The mean difference is calculated as the mean of the “preeclampsia” group minus the mean of the “without preeclampsia” group. In some cases (highlighted with * in the forest plots) means and SDs were given for moderate and severe preeclampsia subgroups separately and we combined them using established formulae https://training.cochrane.org/handbook/archive/v6.1/chapter-06#section-6-5-2-1 (36).
As we anticipated considerable between-study heterogeneity, a random-effects model was used to pool effect sizes. The inverse variance weighting method was used to calculate the pooled mean difference. Hartung-Knapp adjustment (37, 38) was applied as the study number and sample sizes were relatively small. To estimate the heterogeneity variance measure (tau squared), a restricted maximum-likelihood estimator was applied with the Q profile method (39). Additionally, between-study heterogeneity was described by Higgins and Thompson’s (I squared) statistics (40). Forest plots were used to graphically summarize the results. The confidence interval of each individual study was calculated based on the t-distribution. Additionally, where applicable, we reported prediction intervals (i.e., the expected range of effects of future studies) of results following the recommendations of IntHout et al. (41).
Outlier and influence analyses were carried out following the recommendations of Harrer et al. (42) and Viechtbauer and Cheung (43). Publication bias was assessed with Egger’s test (at a significance level of 10%) (44)—however, results should handled critically due to the small number of studies.
All statistical analyses were made with R software (45) using the meta package (46) for main calculations, and the dmetar package (47) for influential analysis.
4 Results
4.1 Study selection
4.1.1 Study selection for evaluating NLR’s predictive role in preeclampsia
For the research, the keywords “NLR” and “preeclampsia” were combined, and searches were conducted in 5 online medical databases (PubMed, Cochrane Library, Scopus, Embase, Web of Science). In total, 324 articles were found, and 134 remained after removing duplicates. An additional 103 articles were excluded because they were irrelevant to the conducted research. In our meta-analysis, we aimed to find clinical studies that utilized first-trimester NLR values as predictive markers of preeclampsia. We excluded studies that were not clinical (e.g., systematic reviews, meta-analyses), letters to other publications, and clinical studies that focused on NLRP3 (NOD-, LRR-, and pyrin domain-containing protein) 3 values in pre-eclamptic women, studies which were results for our searches because they used negative likelihood ratio which’s short form is also NLR and the studies which were clinical but did not use first trimester NLR findings. The remaining 31 pieces of research were selected for detailed screening and out of these 25 got excluded because the samples were not collected during the first trimester (23 studies), only a part of the patients’ samples were collected during the first trimester and the researchers did not publish the data separately (1 study) or first trimester NLR values were presented but the research’s focus was not on preeclampsia prediction (1). The PRISMA flow diagram was conducted regarding strictly The PRISMA 2020 statement: an updated guideline for reporting systematic reviews (34) (Figure 1). Of the remaining 6 (48–53) pieces of research the data (the NLR values in the control and preeclampsia groups and their standard deviations) got extracted for the meta-analysis.
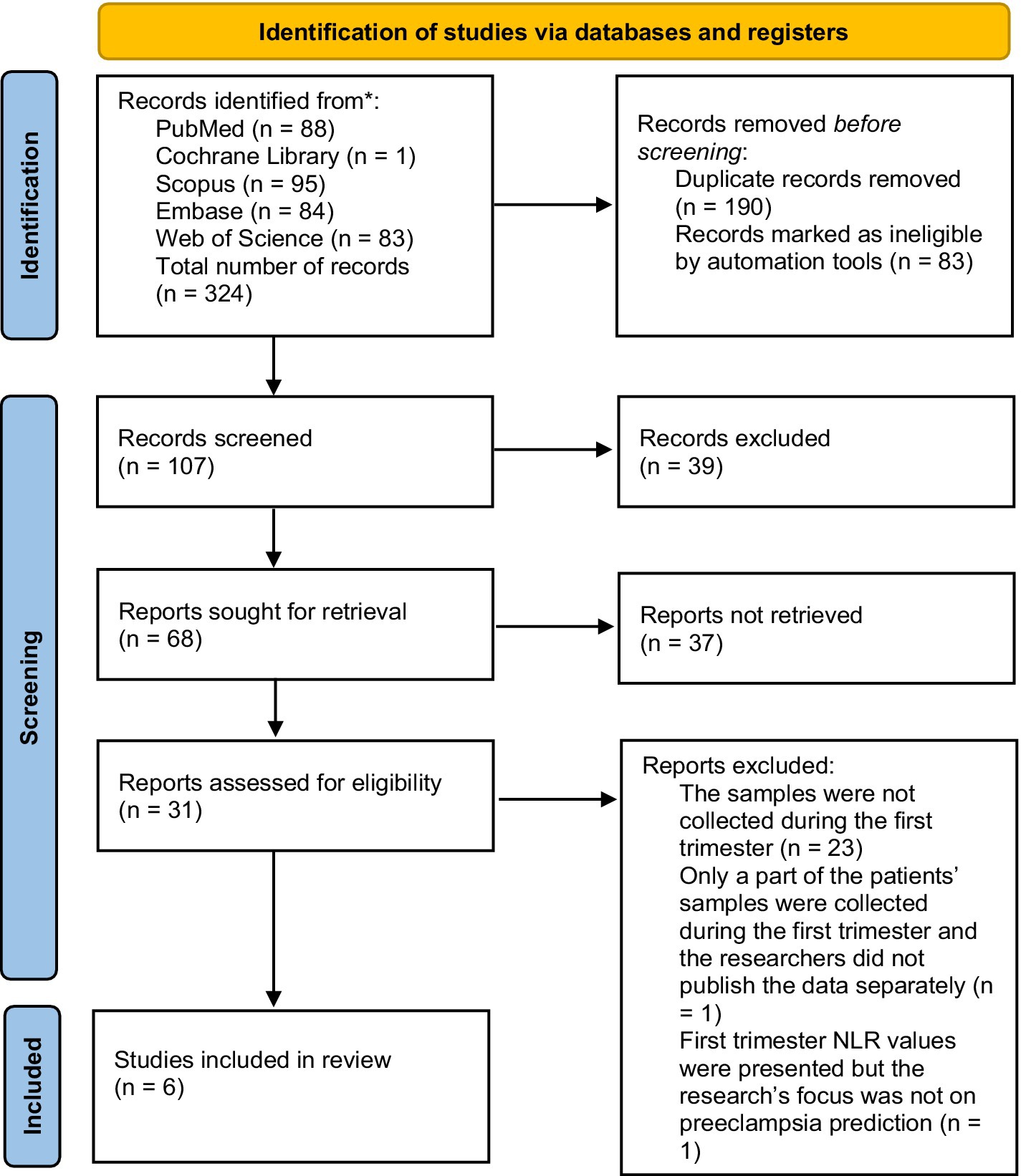
Figure 1. Selection of the studies for the analysis of NLR values’ predictive role in first-trimester preeclampsia.
4.2 Study characteristics
In our study, we included overall 6 studies, the number of preeclampsia patients, the number of the control groups, the ages of the patients (both mean and standard deviation) and the BMIs of the patients (both mean and standard deviation), gestational age at delivery (both mean and standard deviation), are presented on Table 1.
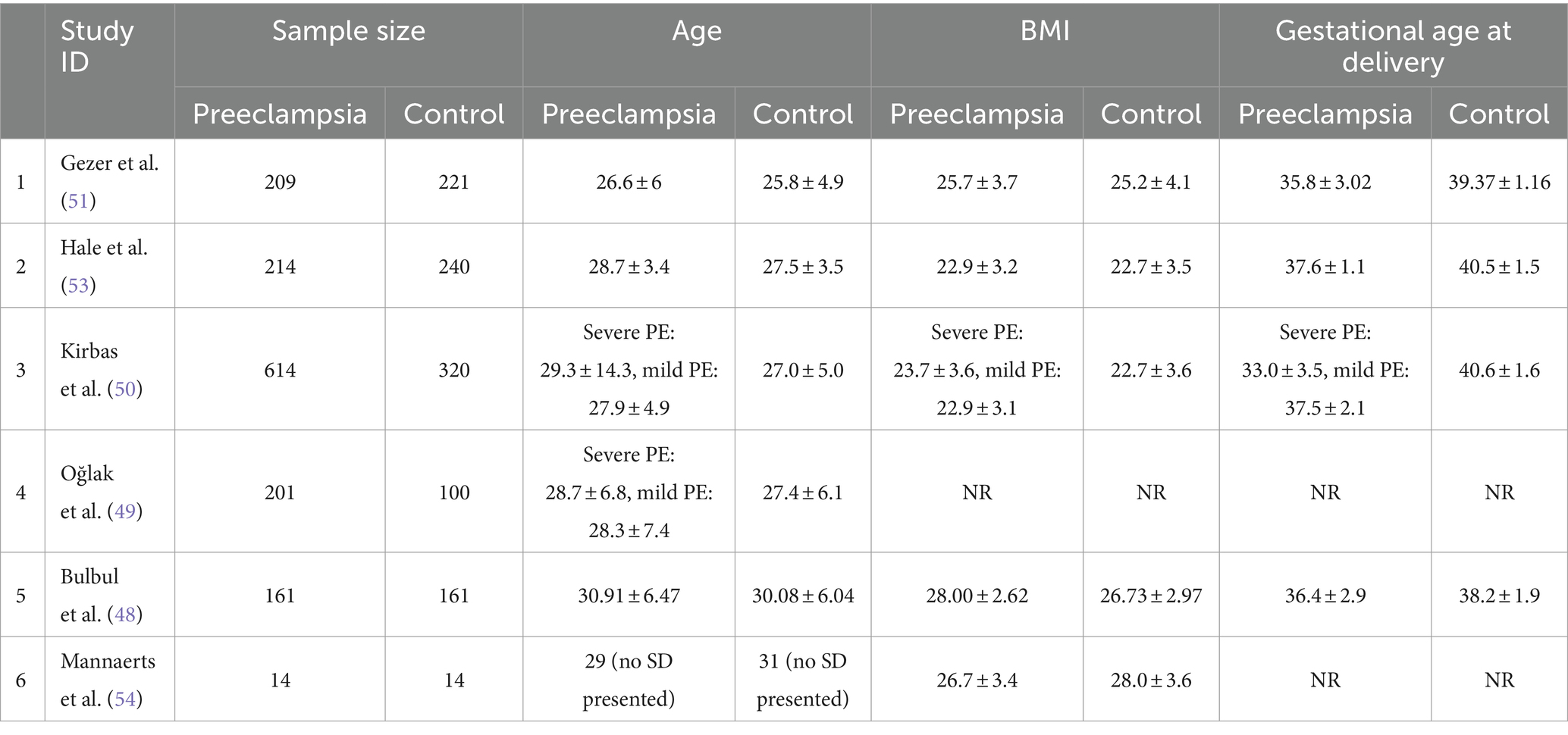
Table 1. Studies included in the meta-analysis.
4.3 Risk of bias
As mentioned above, publication bias was assessed with Egger’s test (at a significance level of 10% due to the small study number).
4.3.1 Bias in NLR research
Although Egger’s test p-value is 0.2132, the meta-analysis contains few studies therefore Egger’s test may lack the statistical power to detect bias or it could give a false “positive” result.
4.4 Synthesis of results
4.4.1 NLR results
A total of 6 studies were selected for analyses covering a total of 2,469 patients.
On average, the effect size is 1.082. The 95% confidence interval of the effect size is 0.641 to 1.523, which tells us that the mean effect size in the universe of comparable studies could fall in this range.
The between-study heterogeneity expressed as I2 value is 0.765 (95% CI, 0.473–0.895), which tells us that 76.5% of the variance in observed effects reflects variance in true effects rather than sampling error. The variance of true effects Τ2 is 0.12 and the standard deviation of true effects Τ is 0.34.
The prediction interval is 0.027 to 2.137. Based on that we would expect in some 95% of all populations comparable to those in the analysis, the true effect size will fall in this range (Figure 2).
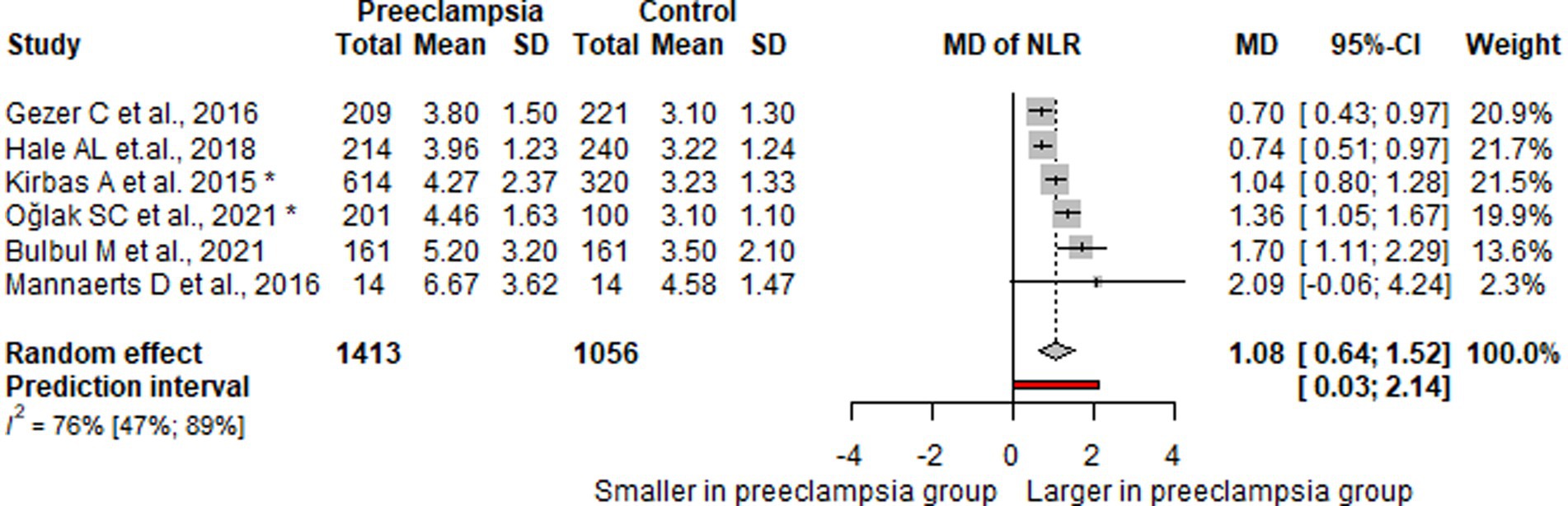
Figure 2. Forest plot of NLR values.
5 Comment
5.1 Principal findings
NLR’s prediction interval fell in the range of 0.027 to 2.137, and the 95% confidence interval of the effect size is 0.641 to 1.523, all the evaluated studies found elevated levels of NLR in mothers who later during their pregnancies developed preeclampsia.
5.2 Comparison with existing literature
5.2.1 The possible explanation behind the elevation of NLR in preeclampsia
Recent studies show that IL-6, IL-8, and IL-17 play an important role in preeclampsia and the production of neutrophil (55–58). One of IL-8’s most important roles is the attraction of neutrophils to the inflamed areas, they play a role in neutrophil recruitment to the endometrium (this way contributing to preeclampsia development), and IL-8 also stimulates neutrophil degranulation (59–62). While IL-6 is linked to genes that stimulate the proliferation, maturation, and activation of neutrophils (63–67). Levels of IL-17A are elevated in preeclampsia and it stimulates the expression of neutrophil chemokines in vascular smooth muscle, IL-17A also increases the levels of G-CSF and GM-CSF which both increase the production of neutrophils (57, 68, 69).
5.2.2 The neutrophil-to-lymphocyte ratio in clinical research
NLR is more and more getting at the center of new studies: while in the PubMed database for the search “neutrophil-to-lymphocyte ratio” there are 65 results from 2012, this number was 1,669 in 2022.
NLR is also studied as a predictive biomarker in COVID-19 (70–72): Fernandes et al. (73) found that NLR levels are higher in COVID-19 patients who needed invasive mechanical ventilation than the control group of COVID-19 patients who did not require invasive mechanical ventilation.
NLR was studied in pregnant COVID-19 patients as well (74, 75): Aydin Güzey et al. (76) evaluated 254 cesarean sections with COVID-19 and found elevated levels of NLR among the symptomatic patients. Our research group also presented a case report where we found elevated NLR in a preeclamptic COVID-19 patient (77). Our research group additionally conducted a case–control study, which included 45 pregnant patients with COVID-19. Statistical analyses revealed that NLR values were notably elevated in patients who succumbed to fatal COVID-19 compared to those who survived the disease (78).
Even though Lurie et al. (79) published their results as early as 1998 of growing neutrophil counts and declining lymphocyte counts in preeclamptic patients, they did not try to evaluate the quotient of these data in PE screening. The first study on NLR’s predictive role in preeclampsia was published in 2015 by Kurtoglu et al. (80) and since then a handful of other studies were published evaluating NLR’s role in all the 3 trimesters (54, 81, 82).
It is important to mention Kang’s et al. (29) meta-analysis from 2019, which found that NLR levels are higher in symptomatic preeclamptic patients compared to control groups. Their meta-analysis also suggests that NLR values can be used to evaluate disease severity. Despite the existence of this prior meta-analysis, our work provides valuable insights as we aimed to evaluate NLR values in the first trimester, before the onset of preeclampsia. Therefore, our study assesses the potential role of NLR values in the screening of preeclampsia. Furthermore, our meta-analysis was justified because, nearly 4 years after their study, numerous new clinical studies have emerged investigating NLR in relation to preeclampsia. However, to the best of our knowledge, there is still no meta-analysis that specifically evaluates the role of this laboratory marker purely in preeclampsia prediction.
5.2.3 Preeclampsia’s first-trimester detection, its importance
As preeclampsia is a relatively common clinical syndrome of the human pregnancy, with a prevalence of 2–8% (5), its only definitive treatment currently the termination of the pregnancy: the delivery of the placenta and the neonate (83) and remains one of the leading causes of maternal- and neonatal morbidity (84) it is eager to find more and more accurate screening methods and therapies.
Large cohort studies and meta-analyses indicate that the main risk factors for preeclampsia development are obesity, antiphospholipid antibody syndrome, chronic hypertension, pregestational diabetes, the use of assisted reproductive technology, nulliparity, and irregular antenatal visits (85–87).
In the screening of preeclampsia, the evaluation of maternal characteristics (maternal age, weight, height, ethnicity, and smoking), medical (chronic hypertension, diabetes, family history of preeclampsia), and obstetrical history (prior pregnancies affected by preeclampsia) is key in the risk calculation of preeclampsia (88, 89). The two most frequently used guidelines that aim to stratify risk using maternal risk factors and characteristics are the American College of Obstetricians and Gynecologists (ACOG) and the National Institute for Health and Care Excellence (NICE) (1, 90). However, the use of risk factors for first-trimester preeclampsia screening performs with poor sensitivity (91).
Another important basis of preeclampsia screening is the usage of Doppler ultrasound, in which case MAP (mean arterial pressure) and uterine artery pulsatility index (UtA-PI) are measured (88, 92).
Biochemical markers are also widely used in preeclampsia’s first-trimester screening: abnormal serum levels of placental growth factor (PlGF), pregnancy-associated plasma protein A (PAPP-A), placental growth factor (PlGF), alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG), unconjugated estriol (uE3), Inhibin A, soluble-endoglin (sEng), and soluble Flt-1 (sFlt-1) are all associated with higher risks of preeclampsia (93–96).
While these methods and the combination of them keep improving it is still urgent to find new markers (possibly ones that can be applied in developing countries as well) to supplement and to make better the currently existing protocols which are key to the reduction of maternal mortality (7, 97).
As a result of our meta-analysis, we found, that to the list of useful biochemical markers, higher levels of NLR can be added: according to the studies used in our analysis, this marker is elevated in first-trimester preeclampsia, moreover, NLR is also easily and widely accessible. However, we maintain that further research should evaluate the usage of the above-mentioned biochemical and biophysical markers combined with NLR, to find more and more beneficial and affordable screening methods.
5.2.4 Preventive medication for preeclampsia
We evaluated NLR’s first-trimester predictive role because we maintain that novel and more accurate screening methods could help obstetricians to detect preeclampsia earlier and consequently, start the treatment or the preventive treatment earlier.
In preeclampsia prevention, the most widely used medication is low-dose aspirin therapy (98, 99). However, there is a growing skepticism against aspirin use in preeclampsia prevention: Lin et al. found that 100 mg of aspirin per day, initiated from 12 to 20 gestational weeks until 34 weeks of gestation, did not reduce the incidence of preeclampsia in pregnant women with high-risk factors (100).
Consequently, new studies are experimenting with other treatments in preeclampsia prevention: Cruz-Lemini et al. (101) published a meta-analysis on low-molecular-weight heparin therapy in women at high risk of preeclampsia. They found that LMWH therapy significantly reduces the risk of preeclampsia and other placenta-mediated complications if the treatment is started before the 16th gestational week.
Our research group’s earlier meta-analysis highlighted that pravastatin therapy started before the 20th gestational week reduces preeclampsia development. The therapy is also beneficial for neonates, as it reduces the number of neonates born with IUGR, neonatal admissions to intensive care units, and the occurrence of preterm deliveries (102).
Calcium, magnesium, and vitamin D supplementation may also be useful in preeclampsia prevention (103–107).
As there are more and more medications that are proven to be effective in preeclampsia prevention it would be key to find more screening methods that would help doctors to detect the risk of preeclampsia earlier and define which patients would need to take preventive medications: this is another reason why we think that first-trimester NLR values in preeclampsia screening should be furtherly evaluated.
5.2.5 The importance of finding cost-effective screening methods
Preeclampsia, even in the 21st century in developed countries remains one of the leading causes of maternal mortality (108–111) and it also puts a large financial burden on health care systems: in 2012, the cost of preeclampsia within the first 12 months of delivery was $2.18 billion in the United States ($1.15 billion for infants and $1.03 billion for mothers) (112). While preeclampsia is a huge and unsolved problem even in developed countries, developing countries are affected more severely (7, 113–117).
In developing countries, it is key to find cost-effective ways the screening and treatment of diseases, but the price is an important aspect in developed countries also.
As NLR is proven to be a cost-effective, relatively accessible biomarker of several diseases (118–121), and the results of our analysis also highlight it as a promising addition to first-trimester preeclampsia screening methods, we maintain that elevated levels of NLR in preeclampsia screening should be evaluated in further clinical studies.
5.3 Strengths and limitations
We are pleased to present our work as the first meta-analysis or systematic review examining the role of NLR in predicting preeclampsia during the first trimester of pregnancy. While previous meta-analyses (28, 29) have explored NLR in preeclampsia prediction, our study uniquely focuses on evaluating first-trimester laboratory findings. We believe that our analysis offers valuable insights into the potential utility of these values for screening preeclampsia during the first trimester. Consequently, our study contributes to a more structured understanding of this area and may serve as a foundation for future clinical investigations, both prospective and retrospective, into the use of NLR in first-trimester preeclampsia screenings.
However, we acknowledge that despite our study’s significant contribution to the field, its primary limitation lies in the small number of eligible studies and patients included. Owing to this limited pool, we faced challenges in estimating the prediction interval of true study effect sizes with a high degree of certainty. Additionally, the limited number of studies prevented us from thoroughly evaluating publication bias or conducting outlier and influential analyses.
6 Conclusions and implications
As the presented statistics show the effect size (1.082), the 95% confidence interval of the effect size (0.641 to 1.523), the standard deviation of true effects (0.34), and the prediction interval (0.027 to 2.137) all fall in a range that lets us conclude that NLR can have a role in first-trimester preeclampsia screening.
We encourage other researchers to examine NLR in cohort studies and randomized clinical studies, alone and combined with other screening methods to find new screening protocols for preeclampsia early on, in the first trimester during pregnancy, this way allowing prophylactic preeclampsia treatment to start earlier.
We maintain that because of the circumstances mentioned in the part “Discussions” it is desired to experiment with screening methods that are: (a) can help to detect preeclampsia early during pregnancy (b) are applicable in low-resource settings-based on our analysis NLR fulfills both criteria.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
BM: Conceptualization, Investigation, Writing – original draft. DV: Formal analysis, Investigation, Software, Validation, Visualization, Writing – original draft. LN: Formal analysis, Investigation, Writing – original draft. BK: Supervision, Writing – review & editing. ZK: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing. SV: Conceptualization, Investigation, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. BM was supported by the MD-PhD Excellence Program of Semmelweis University (EFOP-3.6.3-VEKOP-16-2017-00009), and by the New National Excellence Program of the Ministry for Culture and Innovation from the source of the National Research, Development and Innovation Fund (ÚNKP-23-3-II-SE-81).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Webster, K, Fishburn, S, Maresh, M, Findlay, SC, and Chappell, LCGuideline Committee. Diagnosis and management of hypertension in pregnancy: summary of updated NICE guidance. BMJ. (2019) 366:l5119. doi: 10.1136/bmj.l5119
2. Phumsiripaiboon, P, Suksai, M, Suntharasaj, T, and Geater, A. Screening for pre-eclampsia: performance of National Institute for Health and Care Excellence guidelines versus American College of Obstetricians and Gynecologists recommendations. J Obstet Gynaecol Res. (2020) 46:2323–31. doi: 10.1111/jog.14425
3. Burton, GJ, Redman, CW, Roberts, JM, and Moffett, A. Pre-eclampsia: pathophysiology and clinical implications. BMJ. (2019) 366:l2381. doi: 10.1136/bmj.l2381
4. Ananth, CV, Keyes, KM, and Wapner, RJ. Pre-eclampsia rates in the United States, 1980–2010: age-period-cohort analysis. BMJ. (2013) 347:f6564. doi: 10.1136/bmj.f6564
5. Steegers, EA, von Dadelszen, P, Duvekot, JJ, and Pijnenborg, R. Pre-eclampsia. Lancet. (2010) 376:631–44. doi: 10.1016/S0140-6736(10)60279-6
6. Chappell, LC, Cluver, CA, Kingdom, J, and Tong, S. Pre-eclampsia. Lancet. (2021) 398:341–54. doi: 10.1016/S0140-6736(20)32335-7
7. Khan, KS, Wojdyla, D, Say, L, Gülmezoglu, AM, and Van Look, PF. WHO analysis of causes of maternal death: a systematic review. Lancet. (2006) 367:1066–74. doi: 10.1016/S0140-6736(06)68397-9
8. Nyfløt, L, and Sitras, V. Strategies to reduce global maternal mortality. Acta Obstet Gynecol Scand. (2018) 97:639–40. doi: 10.1111/aogs.13356
9. Mészáros, B, Kukor, Z, and Valent, S. Recent advances in the prevention and screening of preeclampsia. J Clin Med. (2023) 12:6020. doi: 10.3390/jcm12186020
10. Coviello, EM, Iqbal, SN, Grantz, KL, Huang, CC, Landy, HJ, and Reddy, UM. Early preterm preeclampsia outcomes by intended mode of delivery. Am J Obstet Gynecol. (2019) 220:100.e1–9. doi: 10.1016/j.ajog.2018.09.027
11. Rolnik, DL, Wright, D, Poon, LC, O’Gorman, N, Syngelaki, A, de Paco Matallana, C, et al. Aspirin versus placebo in pregnancies at high risk for preterm preeclampsia. N Engl J Med. (2017) 377:613–22. doi: 10.1056/NEJMoa1704559
12. Michalczyk, M, Celewicz, A, Celewicz, M, Woźniakowska-Gondek, P, and Rzepka, R. The role of inflammation in the pathogenesis of preeclampsia. Mediat Inflamm. (2020) 2020:3864941–9. doi: 10.1155/2020/3864941
13. Perucci, LO, Corrêa, MD, Dusse, LM, Gomes, KB, and Sousa, LP. Resolution of inflammation pathways in preeclampsia-a narrative review. Immunol Res. (2017) 65:774–89. doi: 10.1007/s12026-017-8921-3
14. Bu, C, Wang, Z, Ren, Y, Chen, D, and Jiang, SW. Syncytin-1 nonfusogenic activities modulate inflammation and contribute to preeclampsia pathogenesis. Cell Mol Life Sci. (2022) 79:290. doi: 10.1007/s00018-022-04294-2
15. Shamshirsaz, AA, Paidas, M, and Krikun, G. Preeclampsia, hypoxia, thrombosis, and inflammation. J Pregnancy. (2012) 2012:374047. doi: 10.1155/2012/374047
16. Alston, MC, Redman, LM, and Sones, JL. An overview of obesity, cholesterol, and systemic inflammation in preeclampsia. Nutrients. (2022) 14:2087. doi: 10.3390/nu14102087
17. Banerjee, S, Huang, Z, Wang, Z, Nakashima, A, Saito, S, Sharma, S, et al. Etiological value of sterile inflammation in preeclampsia: is it a non-infectious pregnancy complication? Front Cell Infect Microbiol. (2021) 11:694298. doi: 10.3389/fcimb.2021.694298
18. Zeng, H, Han, X, Zhu, Z, Yu, S, Mei, S, Cheng, X, et al. Increased uterine NLRP3 inflammasome and leucocyte infiltration in a rat model of preeclampsia. Am J Reprod Immunol. (2021) 86:e13493. doi: 10.1111/aji.13493
19. Qin, B, Ma, N, Tang, Q, Wei, T, Yang, M, Fu, H, et al. Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) were useful markers in assessment of inflammatory response and disease activity in SLE patients. Mod Rheumatol. (2016) 26:372–6. doi: 10.3109/14397595.2015.1091136
20. Gasparyan, AY, Ayvazyan, L, Mukanova, U, Yessirkepov, M, and Kitas, GD. The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann Lab Med. (2019) 39:345–57. doi: 10.3343/alm.2019.39.4.345
21. Wang, L, Wang, C, Jia, X, Yang, M, and Yu, J. Relationship between neutrophil-to-lymphocyte ratio and systemic lupus erythematosus: a meta-analysis. Clinics. (2020) 75:e1450. doi: 10.6061/clinics/2020/e1450
22. Seringec Akkececi, N, Yildirim Cetin, G, Gogebakan, H, and Acipayam, C. The C-reactive protein/albumin ratio and complete blood count parameters as indicators of disease activity in patients with Takayasu arteritis. Med Sci Monit. (2019) 25:1401–9. doi: 10.12659/MSM.912495
23. Seng, JJB, Kwan, YH, Low, LL, Thumboo, J, and Fong, WSW. Role of neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR) and mean platelet volume (MPV) in assessing disease control in Asian patients with axial Spondyloarthritis. Biomarkers. (2018) 23:335–8. doi: 10.1080/1354750X.2018.1425916
24. Ren, Z, Yang, J, Liang, J, Xu, Y, Lu, G, Han, Y, et al. Monitoring of postoperative neutrophil-to-lymphocyte ratio, D-dimer, and CA153 in: diagnostic value for recurrent and metastatic breast cancer. Front Surg. (2023) 9:927491. doi: 10.3389/fsurg.2022.927491
25. Justesen, MM, Jakobsen, KK, Bendtsen, SK, Garset-Zamani, M, Mordhorst, C, Carlander, ALF, et al. Pretreatment neutrophil-to-lymphocyte ratio as a prognostic marker for the outcome of HPV-positive and HPV-negative oropharyngeal squamous cell carcinoma. Viruses. (2023) 15:198. doi: 10.3390/v15010198
26. Sisti, G, Faraci, A, Silva, J, and Upadhyay, R. Neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and routine complete blood count components in HELLP syndrome: a matched case control study. Medicina. (2019) 55:123. doi: 10.3390/medicina55050123
27. Christoforaki, V, Zafeiriou, Z, Daskalakis, G, Katasos, T, and Siristatidis, C. First trimester neutrophil to lymphocyte ratio (NLR) and pregnancy outcome. J Obstet Gynaecol. (2020) 40:59–64. doi: 10.1080/01443615.2019.1606171
28. Zheng, WF, Zhan, J, Chen, A, Ma, H, Yang, H, and Maharjan, R. Diagnostic value of neutrophil-lymphocyte ratio in preeclampsia: a PRISMA-compliant systematic review and meta-analysis. Medicine. (2019) 98:e18496. doi: 10.1097/MD.0000000000018496
29. Kang, Q, Li, W, Yu, N, Fan, L, Zhang, Y, Sha, M, et al. Predictive role of neutrophil-to-lymphocyte ratio in preeclampsia: a meta-analysis including 3982 patients. Pregnancy Hypertens. (2020) 20:111–8. doi: 10.1016/j.preghy.2020.03.009
30. Tsai, ER, Tintu, AN, Demirtas, D, Boucherie, RJ, de Jonge, R, and de Rijke, YB. A critical review of laboratory performance indicators. Crit Rev Clin Lab Sci. (2019) 56:458–71. doi: 10.1080/10408363.2019.1641789
31. Sayed, S, Cherniak, W, Lawler, M, Tan, SY, El Sadr, W, Wolf, N, et al. Improving pathology and laboratory medicine in low-income and middle-income countries: roadmap to solutions. Lancet. (2018) 391:1939–52. doi: 10.1016/S0140-6736(18)30459-8
32. Thomas, RE, Vaska, M, Naugler, C, and Turin, TC. Interventions at the laboratory level to reduce laboratory test ordering by family physicians: systematic review. Clin Biochem. (2015) 48:1358–65. doi: 10.1016/j.clinbiochem.2015.09.014
33. Stroup, DF, Berlin, JA, Morton, SC, Olkin, I, Williamson, GD, Rennie, D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
34. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
35. Wells, G, Shea, BJ, O’Connell, D, Peterson, J, Welch, V, Losos, M, et al. The Newcastle–Ottawa scale (NOS) for assessing the quality of non-randomized studies in meta-analyses. Ottawa: Ottawa Hospital Research Institute (2014) Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
36. Higgins, JPT, Li, T, and Deeks, JJ. Chapter 6: choosing effect measures and computing estimates of effect In: JPT Higgins, J Thomas, J Chandler, M Cumpston, T Li, and MJ Page, et al., editors. Cochrane handbook for systematic reviews of interventions : Cochrane (2020) Available at: www.training.cochrane.org/handbook
37. Knapp, G, and Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat Med. (2003) 22:2693–710. doi: 10.1002/sim.1482
38. IntHout, J, Ioannidis, JP, and Borm, GF. The Hartung-Knapp–Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian–Laird method. BMC Med Res Methodol. (2014) 14:25. doi: 10.1186/1471-2288-14-25
39. Veroniki, AA, Jackson, D, Viechtbauer, W, Bender, R, Bowden, J, Knapp, G, et al. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Res Synth Methods. (2016) 7:55–79. doi: 10.1002/jrsm.1164
40. Higgins, JP, and Thompson, SG. Quantifying heterogeneity in a meta-analysis. Stat Med. (2002) 21:1539–58. doi: 10.1002/sim.1186
41. IntHout, J, Ioannidis, JP, Rovers, MM, and Goeman, JJ. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open. (2016) 6:e010247. doi: 10.1136/bmjopen-2015-010247
42. Harrer, M, Cuijpers, P, Furukawa Toshi, A, and Ebert, DD. Doing meta-analysis with R: A hands-on guide. 1st ed. Boca Raton, FL: Chapman & Hall/CRC Press (2021).
43. Viechtbauer, W, and Cheung, MW. Outlier and influence diagnostics for meta-analysis. Res Synth Methods. (2010) 1:112–25. doi: 10.1002/jrsm.11
44. Egger, M, Davey Smith, G, Schneider, M, and Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ. (1997) 315:629–34. doi: 10.1136/bmj.315.7109.629
45. R Core Team . R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2022) Available at: https://www.R-project.org/.
46. Schwarzer, G . (2022). meta: General package for meta-analysis. Available at: https://github.com/guido-s/meta/
47. Cuijpers, P, Furukawa, T, and Ebert, DD. (2022). dmetar: Companion R package for the guide doing meta-analysis in R. Available at: https://dmetar.protectlab.org
48. Bulbul, M, Uckardes, F, Karacor, T, Nacar, MC, Kaplan, S, Kirici, P, et al. Can complete blood count parameters that change according to trimester in pregnancy be used to predict severe preeclampsia? J Obstet Gynaecol. (2021) 41:1192–8. doi: 10.1080/01443615.2020.1854697
49. Oğlak, SC, Tunç, Ş, and Ölmez, F. First trimester mean platelet volume, neutrophil to lymphocyte ratio, and platelet to lymphocyte ratio values are useful markers for predicting preeclampsia. Ochsner J. (2021) 21:364–70. doi: 10.31486/toj.21.0026
50. Kirbas, A, Ersoy, AO, Daglar, K, Dikici, T, Biberoglu, EH, Kirbas, O, et al. Prediction of preeclampsia by first trimester combined test and simple complete blood count parameters. J Clin Diagn Res. (2015) 9:QC20–3. doi: 10.7860/JCDR/2015/15397.6833
51. Gezer, C, Ekin, A, Ertas, IE, Ozeren, M, Solmaz, U, Mat, E, et al. High first-trimester neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios are indicators for early diagnosis of preeclampsia. Ginekol Pol. (2016) 87:431–5. doi: 10.5603/GP.2016.0021
52. Mannaerts, D, Faes, E, Goovaerts, I, Stoop, T, Cornette, J, Gyselaers, W, et al. Flow-mediated dilation and peripheral arterial tonometry are disturbed in preeclampsia and reflect different aspects of endothelial function. Am J Physiol Regul Integr Comp Physiol. (2017) 313:R518–25. doi: 10.1152/ajpregu.00514.2016
53. Hale, AL, Karaca, N, Akpak, YK, and Arslan, E. The role of hematological and biochemical markers in preeclampsia prediction. J Clin Anal Med. (2017) 8:306–9. doi: 10.4328/JCAM.5033
54. Mannaerts, D, Heyvaert, S, De Cordt, C, Macken, C, Loos, C, and Jacquemyn, Y. Are neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR), and/or mean platelet volume (MPV) clinically useful as predictive parameters for preeclampsia? J Matern Fetal Neonatal Med. (2019) 32:1412–9. doi: 10.1080/14767058.2017.1410701
55. Vilotić, A, Nacka-Aleksić, M, Pirković, A, Bojić-Trbojević, Ž, Dekanski, D, and Jovanović, KM. IL-6 and IL-8: an overview of their roles in healthy and pathological pregnancies. Int J Mol Sci. (2022) 23:14574. doi: 10.3390/ijms232314574
56. Saito, S . Cytokine network at the feto-maternal Interface. J Reprod Immunol. (2000) 47:87–103. doi: 10.1016/S0165-0378(00)00060-7
57. Walsh, SW, Nugent, WH, Archer, KJ, Al Dulaimi, M, Washington, SL, and Strauss, JF 3rd. Epigenetic regulation of interleukin-17-related genes and their potential roles in neutrophil vascular infiltration in preeclampsia. Reprod Sci. (2022) 29:154–62. doi: 10.1007/s43032-021-00605-3
58. Aneman, I, Pienaar, D, Suvakov, S, Simic, TP, Garovic, VD, and McClements, L. Mechanisms of key innate immune cells in early- and late-onset preeclampsia. Front Immunol. (2020) 11:1864. doi: 10.3389/fimmu.2020.01864
59. Arici, A, Seli, E, Senturk, LM, Gutierrez, LS, Oral, E, and Taylor, HS. Interleukin-8 in the human endometrium. J Clin Endocrinol Metab. (1998) 83:1783–7. doi: 10.1210/jcem.83.5.4754
60. Corre, I, Pineau, D, and Hermouet, S. Interleukin-8: an autocrine/paracrine growth factor for human hematopoietic progenitors acting in synergy with colony stimulating factor-1 to promote monocyte-macrophage growth and differentiation. Exp Hematol. (1999) 27:28–36. doi: 10.1016/S0301-472X(98)00032-0
61. Bellos, I, Karageorgiou, V, Kapnias, D, Karamanli, K-E, and Siristatidis, C. The role of interleukins in preeclampsia: a comprehensive review. Am J Reprod Immunol. (2018) 80:e13055. doi: 10.1111/aji.13055
62. Walsh, SW, Nugent, WH, Al Dulaimi, M, Washington, SL, Dacha, P, and Strauss, JF 3rd. Proteases activate pregnancy neutrophils by a protease-activated receptor 1 pathway: epigenetic implications for preeclampsia. Reprod Sci. (2020) 27:2115–27. doi: 10.1007/s43032-020-00232-4
63. Ding, W, Chim, SSC, Wang, CC, Lau, CSL, and Leung, TY. Molecular mechanism and pathways of normal human parturition in different gestational tissues: a systematic review of transcriptome studies. Front Physiol. (2021) 12:730030. doi: 10.3389/fphys.2021.730030
64. Ding, W, Lau, SL, Wang, CC, Zhang, T, Getsko, O, Lee, NMW, et al. Dynamic changes in maternal immune biomarkers during labor in nulliparous vs multiparous women. Am J Obstet Gynecol. (2022) 227:627.e1–627.e23. doi: 10.1016/j.ajog.2022.05.036
65. Willems, J, Joniau, M, Cinque, S, and van Damme, J. Human granulocyte chemotactic peptide (IL-8) as a specific neutrophil degranulator: comparison with other monokines. Immunology. (1989) 67:540–2.
66. Wang, Y, Gu, Y, Alexander, JS, and Lewis, DF. Preeclampsia status controls interleukin-6 and soluble IL-6 receptor release from neutrophils and endothelial cells: relevance to increased inflammatory responses. Pathophysiology. (2021) 28:202–11. doi: 10.3390/pathophysiology28020013
67. Cemgil Arikan, D, Aral, M, Coskun, A, and Ozer, A. Plasma IL-4, IL-8, IL-12, interferon-γ and CRP levels in pregnant women with preeclampsia, and their relation with severity of disease and fetal birth weight. J Matern Fetal Neonatal Med. (2012) 25:1569–73. doi: 10.3109/14767058.2011.648233
68. Matsubara, K, Ochi, H, Kitagawa, H, Yamanaka, K, Kusanagi, Y, and Ito, M. Concentrations of serum granulocyte-colony-stimulating factor in normal pregnancy and preeclampsia. Hypertens Pregnancy. (1999) 18:95–106. doi: 10.3109/10641959909009614
69. Hayashi, M, Hamada, Y, and Ohkura, T. Elevation of granulocyte-macrophage colony-stimulating factor in the placenta and blood in preeclampsia. Am J Obstet Gynecol. (2004) 190:456–61. doi: 10.1016/j.ajog.2003.07.032
70. Petrakis, V, Panagopoulos, P, Trypsianis, G, Papazoglou, D, and Papanas, N. Fasting plasma glucose increase and neutrophil to lymphocyte ratio (NLR) as risk predictors of clinical outcome of COVID-19 pneumonia in type 2 diabetes mellitus. Exp Clin Endocrinol Diabetes. (2023) 131:194–7. doi: 10.1055/a-2009-6937
71. Wei, T, Li, J, Cheng, Z, Jiang, L, Zhang, J, Wang, H, et al. Hematological characteristics of COVID-19 patients with fever infected by the omicron variant in Shanghai: a retrospective cohort study in China. J Clin Lab Anal. (2023) 37:e24808. doi: 10.1002/jcla.24808
72. Retief, CA, Retief, HJ, and Van der Merwe, S. Evaluating the neutrophil-to-lymphocyte ratio as an indicator for early referral of patients with COVID-19 pneumonia to a high-care facility. S Afr Med J. (2022) 112:795–9. doi: 10.7196/SAMJ.2022.v112i10.16590
73. Fernandes, NF, Costa, IF, Pereira, KN, de Carvalho, JAM, and Paniz, C. Hematological ratios in coronavirus disease 2019 patients with and without invasive mechanical ventilation. J Investig Med. (2023) 71:321–8. doi: 10.1177/10815589221149189
74. Arslan, B, Bicer, IG, Sahin, T, Vay, M, Dilek, O, and Destegul, E. Clinical characteristics and hematological parameters associated with disease severity in COVID-19 positive pregnant women undergoing cesarean section: a single-center experience. J Obstet Gynaecol Res. (2022) 48:402–10. doi: 10.1111/jog.15108
75. Aldika Akbar, MI, Gumilar, KE, Rahestyningtyas, E, Wardhana, MP, Mulawardhana, P, Anas, JY, et al. Accuracy of screening methods of COVID-19 in pregnancy: a cohort study. Minerva Obstet Gynecol. (2023) 75:117–25. doi: 10.23736/S2724-606X.21.04979-4
76. Aydin Güzey, N, and Uyar, TE. Evaluation of 254 cesarean sections with COVID-19 in terms of anesthesia and clinical course: 1-year experience. J Anesth. (2022) 36:514–23. doi: 10.1007/s00540-022-03086-z
77. Supák, D, Mészáros, B, Nagy, M, Gáspár, D, Wagner, LJ, Kukor, Z, et al. Case report: COVID-19 infection in a pregnant 33-year-old kidney transplant recipient. Front Med. (2022) 9:948025. doi: 10.3389/fmed.2022.948025
78. Supák, D, Mészáros, B, Turi, B, Herold, Z, Kukor, Z, and Valent, S. Predicting potentially fatal COVID-19 disease in pregnant patients using the neutrophil-to-lymphocyte ratio (NLR). J Clin Med. (2023) 12:6896. doi: 10.3390/jcm12216896
79. Lurie, S, Frenkel, E, and Tuvbin, Y. Comparison of the differential distribution of leukocytes in preeclampsia versus uncomplicated pregnancy. Gynecol Obstet Investig. (1998) 45:229–31. doi: 10.1159/000009973
80. Kurtoglu, E, Kokcu, A, Celik, H, Tosun, M, and Malatyalioglu, E. May ratio of neutrophil to lymphocyte be useful in predicting the risk of developing preeclampsia? A pilot study. J Matern Fetal Neonatal Med. (2015) 28:97–9. doi: 10.3109/14767058.2014.905910
81. Aslan, MM, Yeler, MT, Yuvacı, HU, Cerci, IA, Cevrioğlu, AS, and Ozden, S. Can the neutrophil-to-lymphocyte ratio (NLR) predicts fetal loss in preeclampsia with severe features? Pregnancy Hypertens. (2020) 22:14–6. doi: 10.1016/j.preghy.2020.07.005
82. Çintesun, E, Incesu Çintesun, FN, Ezveci, H, Akyürek, F, and Çelik, Ç. Systemic inflammatory response markers in preeclampsia. J Lab Physicians. (2018) 10:316–9. doi: 10.4103/JLP.JLP_144_17
83. Bokslag, A, van Weissenbruch, M, Mol, BW, and de Groot, CJ. Preeclampsia; short and long-term consequences for mother and neonate. Early Hum Dev. (2016) 102:47–50. doi: 10.1016/j.earlhumdev.2016.09.007
84. Ma’ayeh, M, and Costantine, MM. Prevention of preeclampsia. Semin Fetal Neonatal Med. (2020) 25:101123. doi: 10.1016/j.siny.2020.101123
85. Yang, Y, Le Ray, I, Zhu, J, Zhang, J, Hua, J, and Reilly, M. Preeclampsia prevalence, risk factors, and pregnancy outcomes in Sweden and China. JAMA Netw Open. (2021) 4:e218401. doi: 10.1001/jamanetworkopen.2021.8401
86. Bartsch, E, Medcalf, KE, Park, AL, and Ray, JGHigh Risk of Pre-Eclampsia Identification Group. Clinical risk factors for pre-eclampsia determined in early pregnancy: systematic review and meta-analysis of large cohort studies. BMJ. (2016) 353:i1753. doi: 10.1136/bmj.i1753
87. Hamzah, STR, Aminuddin, II, and Rachmat, M. Antenatal care parameters that are the risk factors in the event of preeclampsia in primigravida. Gac Sanit. (2021) 35:S263–7. doi: 10.1016/j.gaceta.2021.10.073
88. Poon, LC, Shennan, A, Hyett, JA, Kapur, A, Hadar, E, Divakar, H, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention. Int J Gynaecol Obstet. (2019) 146:390–1. doi: 10.1002/ijgo.12892
89. Kay, VR, Wedel, N, and Smith, GN. Family history of hypertension, cardiovascular disease, or diabetes and risk of developing preeclampsia: a systematic review. J Obstet Gynaecol Can. (2021) 43:227–236.e19. doi: 10.1016/j.jogc.2020.08.010
90. Gestational hypertension and preeclampsia: ACOG practice bulletin summary, number 222. Obstet Gynecol. (2020) 135:1492–5. doi: 10.1097/AOG.0000000000003892
91. MacDonald, TM, Walker, SP, Hannan, NJ, Tong, S, and Kaitu’u-Lino, TJ. Clinical tools and biomarkers to predict preeclampsia. EBioMedicine. (2022) 75:103780. doi: 10.1016/j.ebiom.2021.103780
92. Skråstad, RB, Hov, GG, Blaas, HG, Romundstad, PR, and Salvesen, KÅ. A prospective study of screening for hypertensive disorders of pregnancy at 11–13 weeks in a Scandinavian population. Acta Obstet Gynecol Scand. (2014) 93:1238–47. doi: 10.1111/aogs.12479
93. Huang, T, Bedford, HM, Rashid, S, Rasasakaram, E, Priston, M, Mak-Tam, E, et al. Modified multiple marker aneuploidy screening as a primary screening test for preeclampsia. BMC Pregnancy Childbirth. (2022) 22:190. doi: 10.1186/s12884-022-04514-4
94. Rana, S, Lemoine, E, Granger, JP, and Karumanchi, SA. Preeclampsia: pathophysiology, challenges, and perspectives. Circ Res. (2019) 124:1094–112. doi: 10.1161/CIRCRESAHA.118.313276
95. Lin, TY, Huang, HY, Chan, KS, Chen, YT, Chu, FC, and Shaw, SW. Current update of first trimester preeclampsia screening in Asia. J Obstet Gynaecol Res. (2021) 47:26–33. doi: 10.1111/jog.14524
96. Mosimann, B, Amylidi-Mohr, SK, Surbek, D, and Raio, L. First trimester screening for preeclampsia—a systematic review. Hypertens Pregnancy. (2020) 39:1–11. doi: 10.1080/10641955.2019.1682009
97. Acestor, N, Goett, J, Lee, A, Herrick, TM, Engelbrecht, SM, Harner-Jay, CM, et al. Towards biomarker-based tests that can facilitate decisions about prevention and management of preeclampsia in low-resource settings. Clin Chem Lab Med. (2016) 54:17–27. doi: 10.1515/cclm-2015-0069
98. Rolnik, DL, Nicolaides, KH, and Poon, LC. Prevention of preeclampsia with aspirin. Am J Obstet Gynecol. (2022) 226:S1108–19. doi: 10.1016/j.ajog.2020.08.045
99. Huai, J, Lin, L, Juan, J, Chen, J, Li, B, Zhu, Y, et al. Preventive effect of aspirin on preeclampsia in high-risk pregnant women with stage 1 hypertension. J Clin Hypertens. (2021) 23:1060–7. doi: 10.1111/jch.14149
100. Lin, L, Huai, J, Li, B, Zhu, Y, Juan, J, Zhang, M, et al. A randomized controlled trial of low-dose aspirin for the prevention of preeclampsia in women at high risk in China. Am J Obstet Gynecol. (2022) 226:251.e1–251.e12. doi: 10.1016/j.ajog.2021.08.004
101. Cruz-Lemini, M, Vázquez, JC, Ullmo, J, and Llurba, E. Low-molecular-weight heparin for prevention of preeclampsia and other placenta-mediated complications: a systematic review and meta-analysis. Am J Obstet Gynecol. (2022) 226:S1126–S1144.e17. doi: 10.1016/j.ajog.2020.11.006
102. Mészáros, B, Veres, DS, Nagyistók, L, Somogyi, A, Rosta, K, Herold, Z, et al. Pravastatin in preeclampsia: a meta-analysis and systematic review. Front Med. (2023) 9:2023. doi: 10.3389/fmed.2022.1076372
103. Khaing, W, Vallibhakara, SA, Tantrakul, V, Vallibhakara, O, Rattanasiri, S, McEvoy, M, et al. Calcium and vitamin D supplementation for prevention of preeclampsia: a systematic review and network meta-analysis. Nutrients. (2017) 9:1141. doi: 10.3390/nu9101141
104. Poniedziałek-Czajkowska, E, and Mierzyński, R. Could vitamin D be effective in prevention of preeclampsia? Nutrients. (2021) 13:3854. doi: 10.3390/nu13113854
105. Patrelli, TS, Dall’Asta, A, Gizzo, S, Pedrazzi, G, Piantelli, G, Jasonni, VM, et al. Calcium supplementation and prevention of preeclampsia: a meta-analysis. J Matern Fetal Neonatal Med. (2012) 25:2570–4. doi: 10.3109/14767058.2012.715220
106. Fogacci, S, Fogacci, F, Banach, M, Michos, ED, Hernandez, AV, Lip, GYH, et al. Vitamin D supplementation and incident preeclampsia: a systematic review and meta-analysis of randomized clinical trials. Clin Nutr. (2020) 39:1742–52. doi: 10.1016/j.clnu.2019.08.015
107. Yuan, J, Yu, Y, Zhu, T, Lin, X, Jing, X, and Zhang, J. Oral magnesium supplementation for the prevention of preeclampsia: a meta-analysis or randomized controlled trials. Biol Trace Elem Res. (2022) 200:3572–81. doi: 10.1007/s12011-021-02976-9
108. Ozimek, JA, and Kilpatrick, SJ. Maternal mortality in the twenty-first century. Obstet Gynecol Clin N Am. (2018) 45:175–86. doi: 10.1016/j.ogc.2018.01.004
109. Collier, AY, and Molina, RL. Maternal mortality in the United States: updates on trends, causes, and solutions. NeoReviews. (2019) 20:e561–74. doi: 10.1542/neo.20-10-e561
110. Bødker, B, Hvidman, L, Weber, T, Møller, M, Andersen, BR, Westergaard, HB, et al. Reduction in maternal mortality in Denmark over three decades. Dan Med J. (2021) 68:A02210143.
111. Diguisto, C, Saucedo, M, Kallianidis, A, Bloemenkamp, K, Bødker, B, Buoncristiano, M, et al. Maternal mortality in eight European countries with enhanced surveillance systems: descriptive population based study. BMJ. (2022) 379:e070621. doi: 10.1136/bmj-2022-070621
112. Stevens, W, Shih, T, Incerti, D, Ton, TGN, Lee, HC, Peneva, D, et al. Short-term costs of preeclampsia to the United States health care system. Am J Obstet Gynecol. (2017) 217:237–248.e16. doi: 10.1016/j.ajog.2017.04.032
113. Dymara-Konopka, W, Laskowska, M, and Oleszczuk, J. Preeclampsia—current management and future approach. Curr Pharm Biotechnol. (2018) 19:786–96. doi: 10.2174/1389201019666180925120109
114. Ghulmiyyah, L, and Sibai, B. Maternal mortality from preeclampsia/eclampsia. Semin Perinatol. (2012) 36:56–9. doi: 10.1053/j.semperi.2011.09.011
115. von Dadelszen, P, Firoz, T, Donnay, F, Gordon, R, Justus Hofmeyr, G, Lalani, S, et al. Preeclampsia in low and middle income countries-health services lessons learned from the PRE-EMPT (PRE-Eclampsia-Eclampsia Monitoring, Prevention and Treatment) project. J Obstet Gynaecol Can. (2012) 34:917–26. doi: 10.1016/S1701-2163(16)35405-6
116. Bossman, E, Johansen, MA, and Zanaboni, P. mHealth interventions to reduce maternal and child mortality in sub-Saharan Africa and southern Asia: a systematic literature review. Front Glob Womens Health. (2022) 3:942146. doi: 10.3389/fgwh.2022.942146
117. Dasari, A, Jacob, PM, Jeyapaul, S, Mathew, AJ, Abraham, VJ, and Cherian, AG. Description and outcomes of patients with eclampsia and severe pre-eclampsia in a rural hospital in north-eastern Bihar: a retrospective study. J Family Med Prim Care. (2022) 11:6096–100. doi: 10.4103/jfmpc.jfmpc_286_22
118. Kerboua, KE . NLR: a cost-effective nomogram to guide therapeutic interventions in COVID-19. Immunol Investig. (2021) 50:92–100. doi: 10.1080/08820139.2020.1773850
119. Tadesse, Z, Bekele Bayissa, A, Diriba, T, Chernet, N, Tsegaye, S, and Tsega, M. Neutrophil-to-lymphocyte ratio and cut-off values as predictor of severity and mortality in COVID-19 patients in millennium COVID-19 care center, Addis Ababa, Ethiopia. Int J Gen Med. (2022) 15:6739–55. doi: 10.2147/IJGM.S375565
120. Zhang, J, Zeng, J, Zhang, L, Yu, X, Guo, J, and Li, Z. The utility of peripheral blood leucocyte ratios as biomarkers in neonatal sepsis: a systematic review and meta-analysis. Front Pediatr. (2022) 10:908362. doi: 10.3389/fped.2022.908362
121. Can, E, Hamilcikan, Ş, and Can, C. The value of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio for detecting early-onset neonatal Sepsis. J Pediatr Hematol Oncol. (2018) 40:e229–32. doi: 10.1097/MPH.0000000000001059
Glossary
Keywords: NLR, neutrophil-to-lymphocyte ratio, first trimester, pre-eclampsia, preeclampsia screening
Citation: Mészáros B, Veres DS, Nagyistók L, Kovács BG, Kukor Z and Valent S (2024) A meta-analysis on first-trimester blood count parameters—is the neutrophil-to-lymphocyte ratio a potentially novel method for first-trimester preeclampsia screening? Front. Med. 11:1336764. doi: 10.3389/fmed.2024.1336764
Edited by:
Simcha Yagel, Hadassah Medical Center, IsraelReviewed by:
Federico Romano, Institute for Maternal and Child Health Burlo Garofolo (IRCCS), ItalyMihai Emil Capilna, George Emil Palade University of Medicine, Pharmacy, Sciences and Technology of Târgu Mureş, Romania
Reinaldo Marín, Instituto Venezolano de Investigaciones Científicas (IVIC), Venezuela
Copyright © 2024 Mészáros, Veres, Nagyistók, Kovács, Kukor and Valent. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zoltán Kukor, a3Vrb3Iuem9sdGFuQG1lZC5zZW1tZWx3ZWlzLXVuaXYuaHU=
†These authors have contributed equally to this work