 Julia Kubasch1
Julia Kubasch1 Miriam Ortiz1
Miriam Ortiz1 Sylvia Binting1Stephanie Roll1Katja Icke1
Sylvia Binting1Stephanie Roll1Katja Icke1 Joanna Dietzel1Rainer Nögel2Josef Hummelsberger2
Joanna Dietzel1Rainer Nögel2Josef Hummelsberger2 Stefan N. Willich1Benno Brinkhaus1Michael Teut1Julia Siewert1*
Stefan N. Willich1Benno Brinkhaus1Michael Teut1Julia Siewert1*- 1Charité – Universitätsmedizin Berlin, Freie Universität Berlin and Humboldt-Universität zu Berlin, Institute of Social Medicine, Epidemiology and Health Economics, Berlin, Germany
- 2International Society for Chinese Medicine (SMS), Munich, Germany
Study objectives: Non-pharmacological interventions for restless legs syndrome (RLS) are frequently used, although scientific evidence remains limited. The study aimed to investigate the feasibility and effects of self-applied hydrotherapy and self-applied acupressure in patients with RLS.
Methods: In a three-armed randomized single-center open exploratory pilot study, adults with moderate to severe RLS were randomly allocated to 6 weeks of daily hydrotherapy plus routine care (HT group), acupressure plus routine care (AP group), or routine care alone (RC group). Outcome measures included RLS symptom severity (IRLS), disease-specific quality of life (RLSQoL), the impression of change (PGI-C), health-related quality of life (SF-12), psychological outcomes (SGW-B, HADS, and GSE), and adherence and adverse events (AEs) after 6 and 12 weeks.
Results: Fifty-four adults (mean age 57.5 ± 11.4 years, 63% women) were included. The study showed good feasibility with an 83% retention rate. After 6 weeks, baseline-adjusted mean IRLS scores were 19.8 (95% [16.4, 23.2]) for HT, 22.9 (19.2, 26.6) for AP, and 24.0 (20.8, 27.2) for RC. RLSQoL adjusted means were 65.3 (59.7, 70.9) for HT, 68.3 (62.3, 74.3) for AP, and 56.2 (50.9, 61.5) for RC, after 6 weeks. Both interventions were safe, with high adherence rates.
Conclusion: Self-applied hydrotherapy and acupressure appear to be feasible and safe interventions for patients with RLS. This exploratory pilot study suggests potential benefits, though larger, well-designed confirmatory studies are needed to validate these findings.
Clinical trial registration: This study was registered in the German Clinical Trials Register (number DRKS00029960) on August 09, 2022. https://drks.de/search/de/trial/DRKS00029960.
1 Introduction
Restless legs syndrome (RLS) is a common, circadian, sensorimotor disorder characterized by unpleasant sensations in the legs at rest and an urge to move them (1). Symptoms typically appear in the evening and at night, causing severe sleep disturbances and poor quality of life (2, 3). The prevalence of RLS in adults is estimated at 5.9% in Europe (4), leading to absence from work, loss of social networks, and even early retirement (5, 6), thus causing considerable costs (7). The prevalence of RLS is consistently higher in patients with a high burden of comorbidity (8).
The clinical history as the primary diagnostic method follows the five diagnostic criteria for RLS developed by the International Restless Legs Syndrome Study Group (IRLSSG) and can be obtained by any physician (8–10). The quality of life (QoL) of RLS patients is generally worse than that of individuals with type 2 diabetes, depression, and osteoarthritis (11). In comparison with control subjects without sleep disorders, RLS patients often exhibit anxiety or symptoms of depression, other psychopathological symptoms, and poor wellbeing (12). Psychological stress is known to exacerbate RLS symptoms (13, 14). RLS is a complex disorder in which dopamine and iron metabolism, predisposing genetic factors, environmental factors, and comorbidities could be involved (15).
The treatment of RLS initially focuses on iron metabolism and iron supplementation (16). Dopaminergic drugs are used if iron supplementation does not improve symptoms or the requirements are not met. Many dopaminergic drugs can cause augmentation, which is the amplification of RLS symptoms and occurs in 30–68% of patients (17). Several nondopaminergic drugs for RLS, including opioids, anticonvulsants, and alpha-adrenergic agonists (clonidine), also have common and well-known side effects that limit the effectiveness of therapy, including nausea, vomiting, urinary retention, and constipation (18–22).
Non-pharmacological interventions are often recommended as treatments for mild and intermittent RLS (16, 23, 24). However, the recommendations are generally unspecific, and to date, there are few conclusive research results, with insufficient and inconclusive evidence for many interventions requiring further research and innovation (25–27). Systematic reviews and a meta-analysis indicate that acupuncture (AC) significantly reduces RLS symptoms (25, 28–30). While AC uses needles to stimulate acupuncture points, acupressure (AP) involves manual stimulation of the same points, making it suitable for self-treatment. An AP pilot study reported a reduction in RLS severity for dialysis patients with RLS (31).
In pregnant women, cold water applications (20–25°C) may reduce RLS symptoms (32), and cold air applications (local cryotherapy [17°C] on the legs) can reduce sleep-related symptoms (25, 28, 29).
Hydrotherapy (HT) according to the German self-taught naturopath and priest Sebastian Kneipp (1821–1897) is characterized by serial, mostly cold water applications (e.g., affusions, compresses, washes, and baths) and has been known in German-speaking countries since the 19th century for preventive health care and the treatment of various diseases (33, 34). Self-applied AP and Kneipp HT showed little to no side effects in various trials (34–37). Sixty-five percent of RLS patients regularly use traditional complementary and integrative medicine (TCIM) to relieve their symptoms (38). To our knowledge, there are no randomized controlled trials that have investigated the effect, safety, and feasibility of self-applied AP and Kneipp-HT in patients with RLS.
We conducted this exploratory clinical study to evaluate the feasibility and effects of self-applied AP or HT in patients with RLS, providing preliminary data for future confirmatory trials.
2 Materials and methods
2.1 Design
This randomized, controlled, three-armed, explorative clinical trial was conducted at the outpatient department for Integrative Medicine at the German Charité Universitätsmedizin, Berlin between September 2022 and March 2023. The trial was approved by the Ethics Committee in Berlin (EA2/132/22, 12 July 2022) and followed Good Clinical Practice and the Helsinki Declaration. Prior to the study, all patients gave informed written and oral consent. The study is registered in the German Clinical Trials Register (DRKS00029960). The study design and methods were published earlier (39).
2.2 Patients and recruitment
Patients were recruited via digital newsletters of medical institutions, the homepage of the research institute, public transport advertising, and flyers at general practitioners’ clinics and neurological specialist practices.
The following study inclusion criteria applied: patients of all sexes, aged 18–75, with a confirmed RLS diagnosis meeting the diagnostic criteria defined by the International Restless Legs Syndrome Study Group (IRLSSG) (10), RLS-related complaints of at least 30 mm on a visual analog scale (VAS 0 mm = no complaints to 100 mm = the worst complaints possible), at least moderate RLS symptoms (IRLS – total score ≥ 11), and no planned change in medication during the study. Exclusion criteria included: indications for iron replacement therapy (except if already administered without symptom improvement or if refused by patient); regular intake of RLS-triggering medications (e.g., mirtazapine, mianserin, clozapine, olanzapine, risperidone, haloperidol, sulpiride, and promethazine); use of hydrotherapy, acupuncture, or acupressure within 4 weeks before or planned within 12 weeks after inclusion; acute SARS-CoV-2 infection or long-COVID syndrome; pregnancy or breastfeeding; serious acute/chronic organic or mental illness preventing study participation (e.g., advanced cardio/pulmonary disease NYHA/GOLD III + IV); Raynaud’s disease or advanced peripheral circulatory disorders; untreated dermatological conditions in treatment areas (e.g., severe atopic dermatitis, severe psoriasis, and large wounds); substance abuse; opioid therapy; concurrent study participation or participation within previous 3 months; and dependence on the study site (e.g., employment or any other professional or personal dependency relationship with the research institution).
2.3 Randomization and blinding
Randomization was performed centrally using a computer-generated randomization list (created with R software [version 4.1.2]) as block randomization with variable block length. The groups were allocated using a 1:1:1 ratio. Concealed allocation was carried out at the end of the inclusion examination by the study physician using an administrative database. The informed consent process and the assessment of inclusion and exclusion criteria were completed before the inclusion examination. Surname, given name, date of birth, and sex were entered into the administrative database by the study physician. All other personal data were filled in later by the study nurse. After a patient’s inclusion in the study, the system carried out automatic randomization and created the randomization confirmation which was initiated. Study physicians did not have access to the randomization list, which only showed one result at a time. After completing the baseline questionnaires, patients were informed of their randomization results and subsequently received training in the respective interventions. Patients and physicians were not blinded to treatment allocation. Statisticians were blinded to group allocation.
2.4 Study interventions and control
The 6-week intervention phase of the study was followed by a 6-week follow-up phase, during which the patients could optionally continue the learned interventions. Until the end of week 12, the control group did not receive any study intervention. After being randomized and allocated, patients received a 15-min instruction in self-therapy of acupressure (AP group) or hydrotherapy (HT group) by a study physician and were given an instruction booklet. During the following 6 weeks, the patients performed daily AP and HT at home. In both intervention groups, patients were contacted by telephone in the second and fourth weeks (w2 and w4) to inquire about difficulties with the application and to improve adherence. Discontinuations and withdrawals were documented with reasons, where known.
Hydrotherapy was carried out in a semi-standardized manner alongside routine care with obligatory and optional affusions according to the principles of one of the pioneers of hydrotherapy, the German priest Sebastian Kneipp (1821–1897). The patients performed treatments at least twice daily for 6 weeks. Two cold affusions up to the knees daily for 30–60 s with water colder than 18°C (ideally 10–15°C) were recommended (Figure 1). The total treatment time including preparation and post-processing should take approximately 20 min daily. Optional affusions included cold or alternating warm arm or knee affusions and cold face affusions. The optional affusions could be conducted as often as desired during the day according to Kneipp’s basic rules.
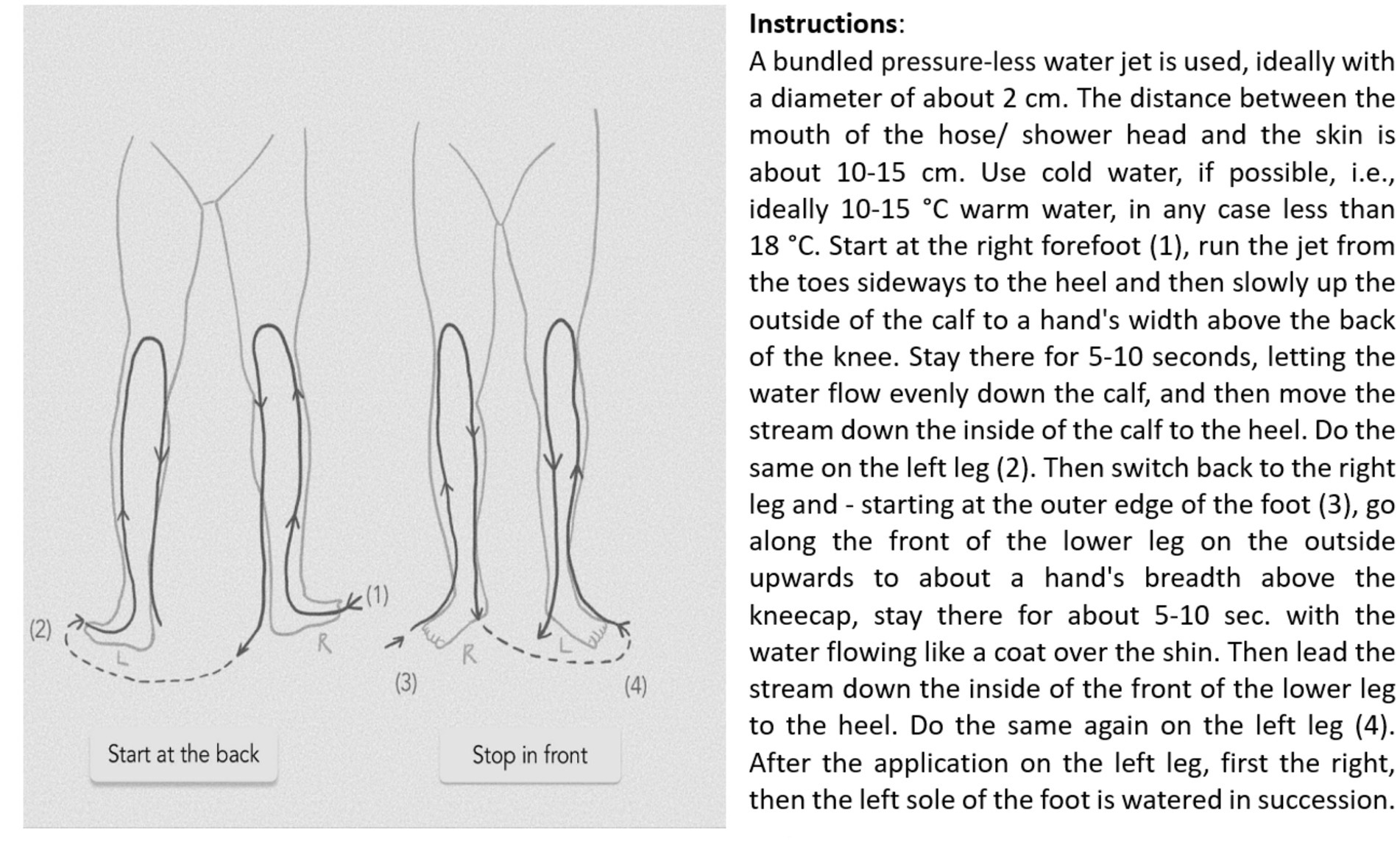
Figure 1. Hydrotherapy procedure for knee affusion.
Acupressure was performed in addition to routine care by manually stimulating six acupressure points, which were determined in advance by a modified expert consensus procedure according to the rules and principles of Chinese medicine. The following points were used bilaterally: Large Intestine 4, Pericardium 6, Stomach 36, Spleen 6, Kidney 3, and Liver 3 (see Figure 2). Patients performed the treatment at least once a day for 6 weeks, or more often if desired. The total treatment time was set at approximately 20 min per day, while the pressure duration per point was approximately 2 min.
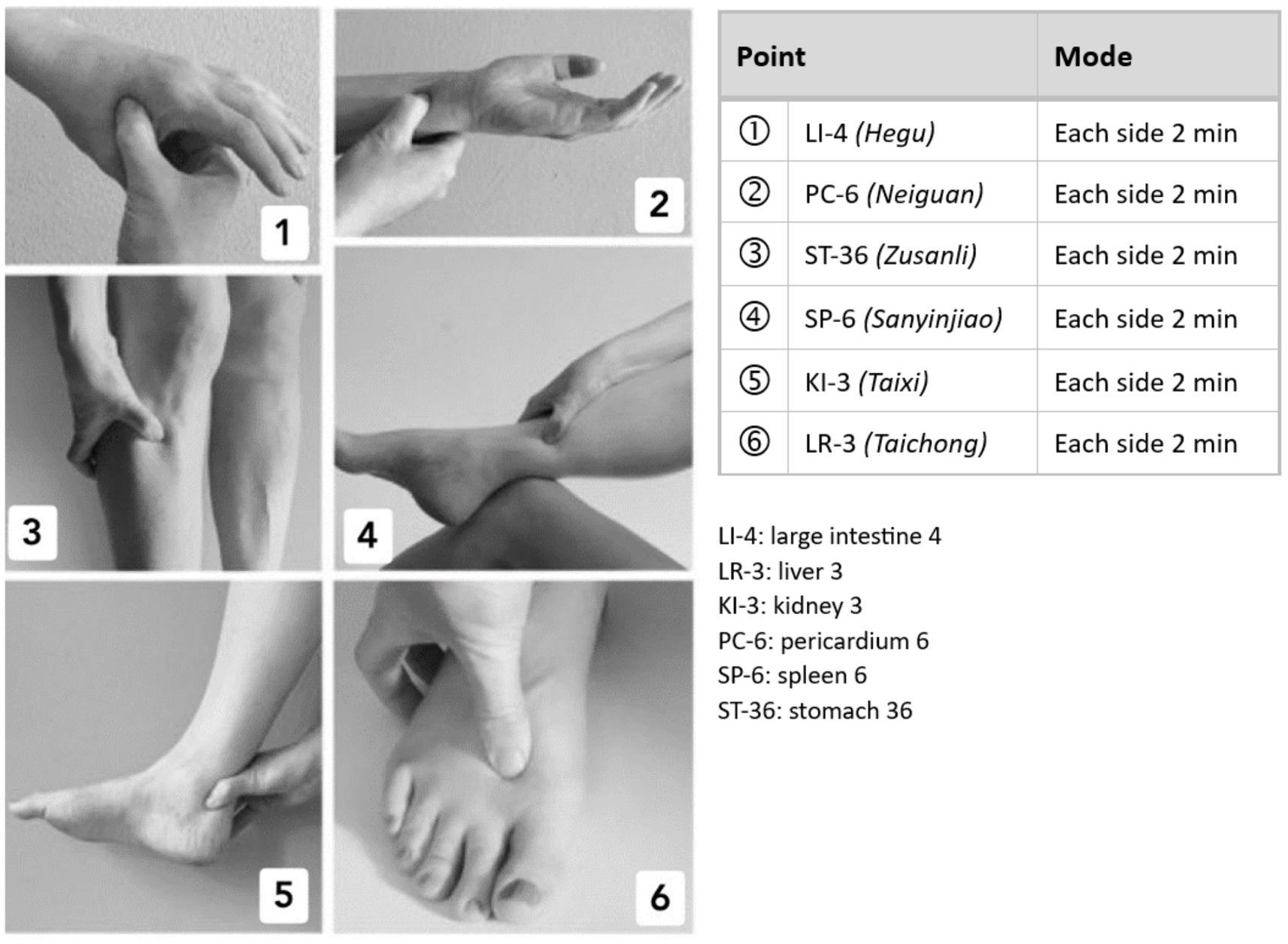
Figure 2. Acupressure points 1 to 6: LI 4, PC 6, ST 36, SP 6, KI 3, LR 3.
The control group was asked to continue only their routine care for 12 weeks. Details on the interventions were published before (39).
All patients were asked not to start other treatments for RLS-related symptoms during the study.
2.5 Outcomes
Exploratory outcome parameters were assessed after 6 and 12 weeks. Outcome parameters included RLS severity (IRLS; range 0–40, higher scores indicating more severe symptoms) (40), disease- and health-related quality of life measured with the Restless Legs Syndrome Quality of Life questionnaire (RLSQoL; range 0–100, higher scores indicating better disease-related quality of life) and the Short-Form 12 (SF-12) questionnaire yielding Physical and Mental Component Summary scores (PCS, MCS; range 0–100, higher scores indicating better health-related quality of life) (41–43), Patient Global Impressions Scale-Change (PGI-C; range 1–7, lower scores indicating greater improvement) (44), subjective global wellbeing with a 0–100 mm VAS (SGW-B; higher scores indicating better wellbeing) (45), depression and anxiety using the Hospital Anxiety and Depression Scale (HADS-D; range 0–21 for each subscale, higher scores indicating more severe symptoms) (46), and self-efficacy via the General Self-Efficacy Scale (GSE; range 10–40, higher scores indicating greater self-efficacy) (47, 48).
The minimum clinically important difference (MCID) is defined as the smallest difference between two groups on an outcome measure that is considered clinically relevant to patients.
RLS-specific MCIDs were only found for the IRLS (MCID = 3) (49). Thus, the MCID for the quality of life instrument RLSQoL was estimated based on existing evidence that MCIDs/MIDs measuring differences in quality of life are consistently close to half a standard deviation, which corresponds to 7.1% or 0.5 points on a 7-point scale (50, 51). The estimated MCID for RLSQoL is therefore 7.1 points on a respective scale of 0–100. For the SF-12, several studies were found in which the MCID was reported for patients with orthopedic conditions, obesity, and prostate cancer. The MCID for the SF-12 MCS score ranged from 1.5 to 15.9, for the PCS from 1.8 to 12 points for patients with orthopedic conditions, 4 points for MCS/PCS for patients with prostate cancer, and 5 points for MCS/PCS for patients with obesity. Based on the average of these data, we estimated the MCID of the SF-12 MCS score to be 5.9 points and that of the PCS score to be 5.3 points (52–54).
As the PGI-C is a Likert scale from 1 to 7, a difference of 0.5 points was assumed to be clinically relevant (51). The MCID for subjective global wellbeing (SGW-B), a visual analog scale (0–100 mm), was set at 14 points for our study, comparable to the MCID for the visual analog scale in the field of pain therapy. Here, differences of 14 or 30 mm on a 100 mm scale are regarded as a minimal clinically important difference (MCID) (55, 56). The MCID for the HADS-D was estimated to be 1.7 points in our study, analogous to the MCID for patients with cardiovascular disease, where it was triangulated from distribution-based, anchor-based, and Delphi-based results (57). As no MCID was found at all for the GSE, a threshold value was defined based on clinical experience. Usual threshold values here are 15% of the achieved value from the total value, which for the GSE scale (values from 10 to 40) would be a difference of 4.5 points (15% out of 30) (58).
Furthermore, the patients kept a diary during weeks 1–6 in which they recorded the frequency at which the study interventions were carried out, as well as medication changes and adverse events (AEs) (59). Patients received a second diary 12 weeks after enrolment in the study to retrospectively record safety, treatment adherence, and frequency of voluntary treatment in the follow-up phase (weeks 7–12).
Two telephone calls (w2 and w4) inquired about the feasibility of the application and were documented by the study physicians.
2.6 Safety
AEs and severe adverse events (SAEs) were recorded in addition to the diaries during phone calls in weeks 2 and 4. Study physicians classified adverse events as treatment-related or non-treatment-related.
2.7 Statistics
As this is an exploratory study, the sample size was determined primarily considering feasibility aspects. Assuming that approximately 10% of patients drop out of the study before week 6, 17 patients per group (51 randomized patients in total) were planned, which seemed logistically feasible at the study center, to obtain 15 patients per group at the end of week 6.
All data collected were analyzed descriptively: means, standard deviations, medians, and quartiles. Outcomes were analyzed using analysis of covariance (ANCOVA), depending on the scale, including the treatment group as a fixed-effect factor and the respective baseline value (where applicable) as a fixed covariate. For group comparisons, adjusted means with 95% confidence intervals are provided. p-values are considered exploratory without adjustment for multiple testing. Analysis was conducted on the full analysis set (FAS) defined according to the intention-to-treat principle without imputation of missing data. Analyses were performed using SPSS (IBM SPSS Statistics, version 25), R (version 4.1.2), and SAS (SAS for Windows, version 9.4).
Post-hoc analyses included the calculation of Cohen’s d effect sizes, which were not originally specified in the study protocol.
3 Results
In total, 231 patients were screened for eligibility: 177 patients did not meet the eligibility criteria (see consort flowchart in Figure 3). The main reasons for not qualifying for participation were age over 75, the use of opioids, or only mild RLS symptoms. Fifty-four patients were included and randomly assigned to the intervention or RC group (18 patients per group). The retention rate was 83% with 45 out of 54 patients completing the 12-week study. One patient in the AP group discontinued treatment after the first week for personal reasons but continued to complete diaries and questionnaires, showing a worsening in all scores except PGI-C after 12 weeks; these data were included in the analysis.
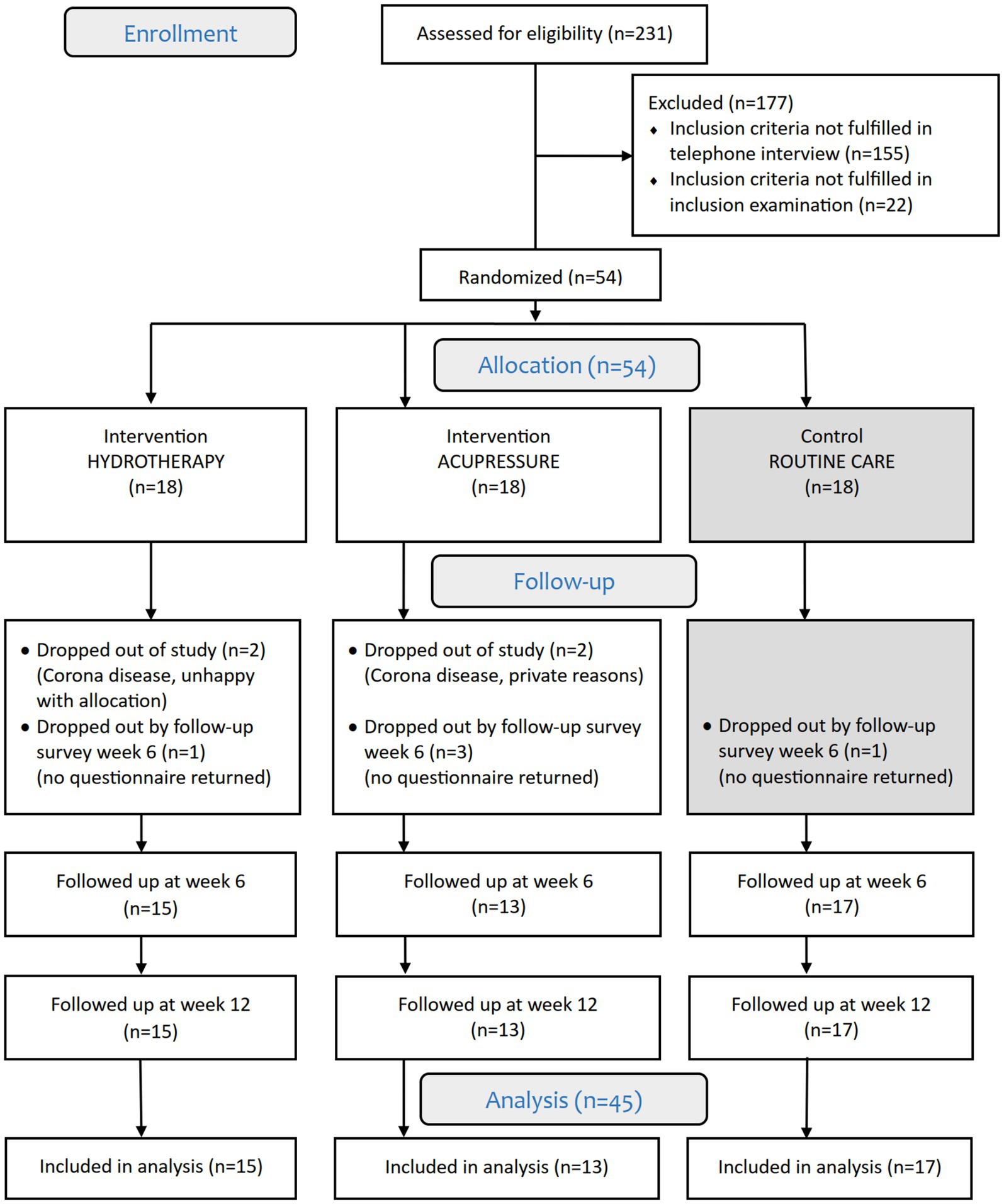
Figure 3. HYDRAC CONSORT study flowchart.
Patient characteristics at baseline regarding age, height, weight, psychological assessment, disease-specific assessment (IRLS, RLSQoL), number of patients taking RLS medication, and average disease duration were comparable between groups (Table 1). More women were represented in the study population (63%). The sex ratio (female/male) was different between the HT group (9/9), AP group (11/7), and RC group (14/4). Compared to the intervention groups, the RC group had a higher proportion of smokers (RC: n = 7, AP: n = 4, HT: n = 3) and a higher level of education (RC: n = 13, AP: n = 10, HT: n = 9). The number of patients with concomitant diseases was high in both intervention groups. Expectations regarding the improvement potential of HT and AP did not differ between the groups and were high for both forms of therapy, although experience with both interventions was similarly low. However, the overall expectation of an improvement for AP was slightly higher than for HT, as four patients assumed that HT would not bring any improvement at all.
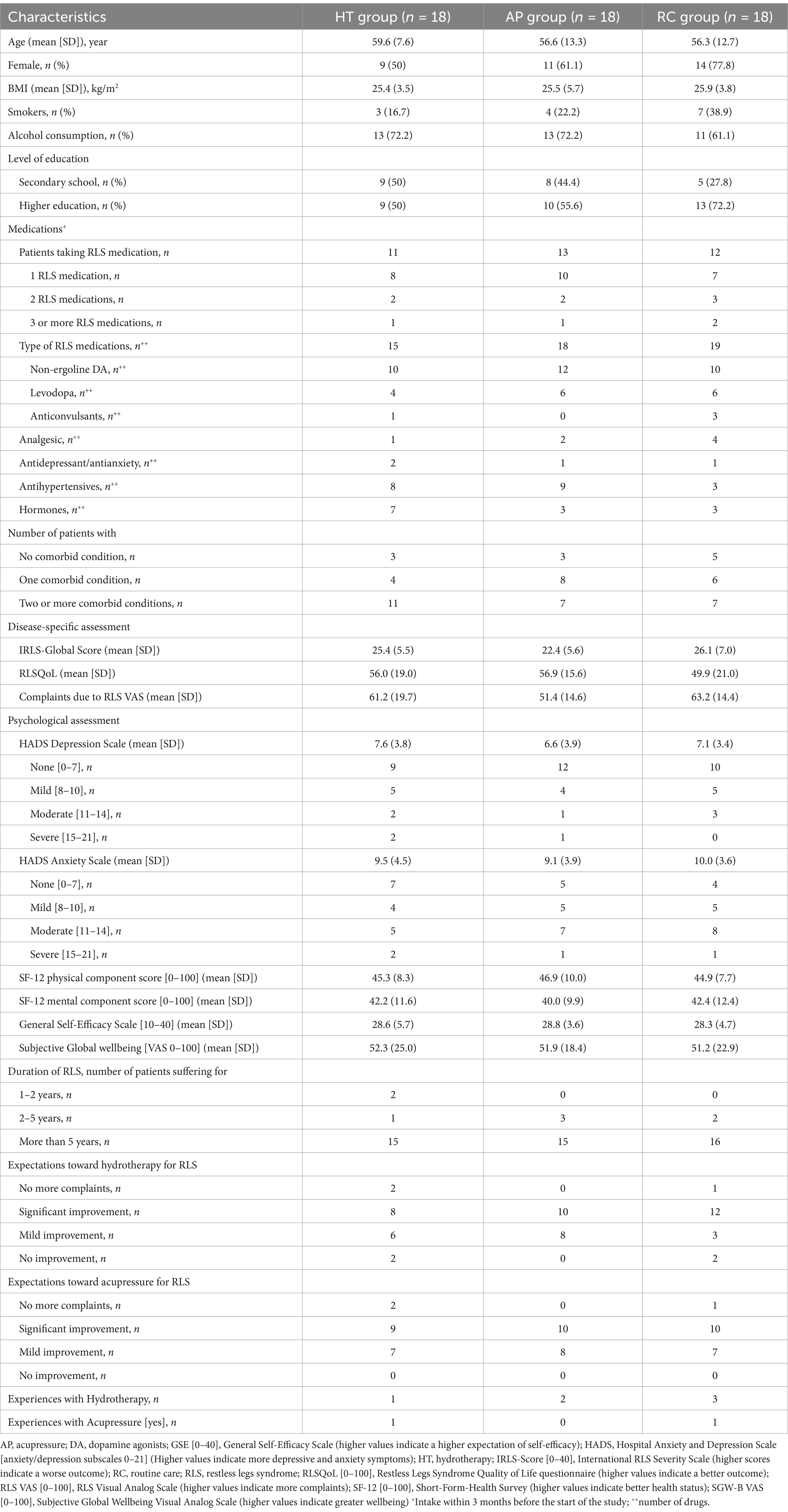
Table 1. Baseline characteristics of trial participants.
The average intervention duration of the daily treatments differed between the intervention groups. On average, HT was performed for 5.1 min per day, while AP lasted 22.5 min per day. Adherence among the participants was similarly high in both intervention groups after 6 weeks, with self-treatment more than 6 days per week with recommended daily use (HT: 6.5, AP: 6.4 days per week, Figures 4, 5). After a 12-week follow-up, including a 6-week optional self-treatment phase, adherence remained high (HT: 4.3, AP: 3.5 days per week). During this optional self-treatment phase, a majority of patients continued their self-treatments (11/15 [73.3%] in the HT group and 10/13 [76.9%] in the AP group). After a 6-week follow-up, all participants indicated they were still motivated to continue the applications (HT: 2.2, AP: 2.5; 1 = highly motivated, 4 = no motivation). The option of additional affusions in the hydrotherapy group was used by 7 of 15 patients in the first 6 weeks. Cold arm affusions (n = 76, the total number of arm affusions in weeks 1–6) used by 5 of 15 patients were preferred over facial affusions (n = 13, the total number of face affusions in weeks 1–6) which were used by 3 of 15 patients.
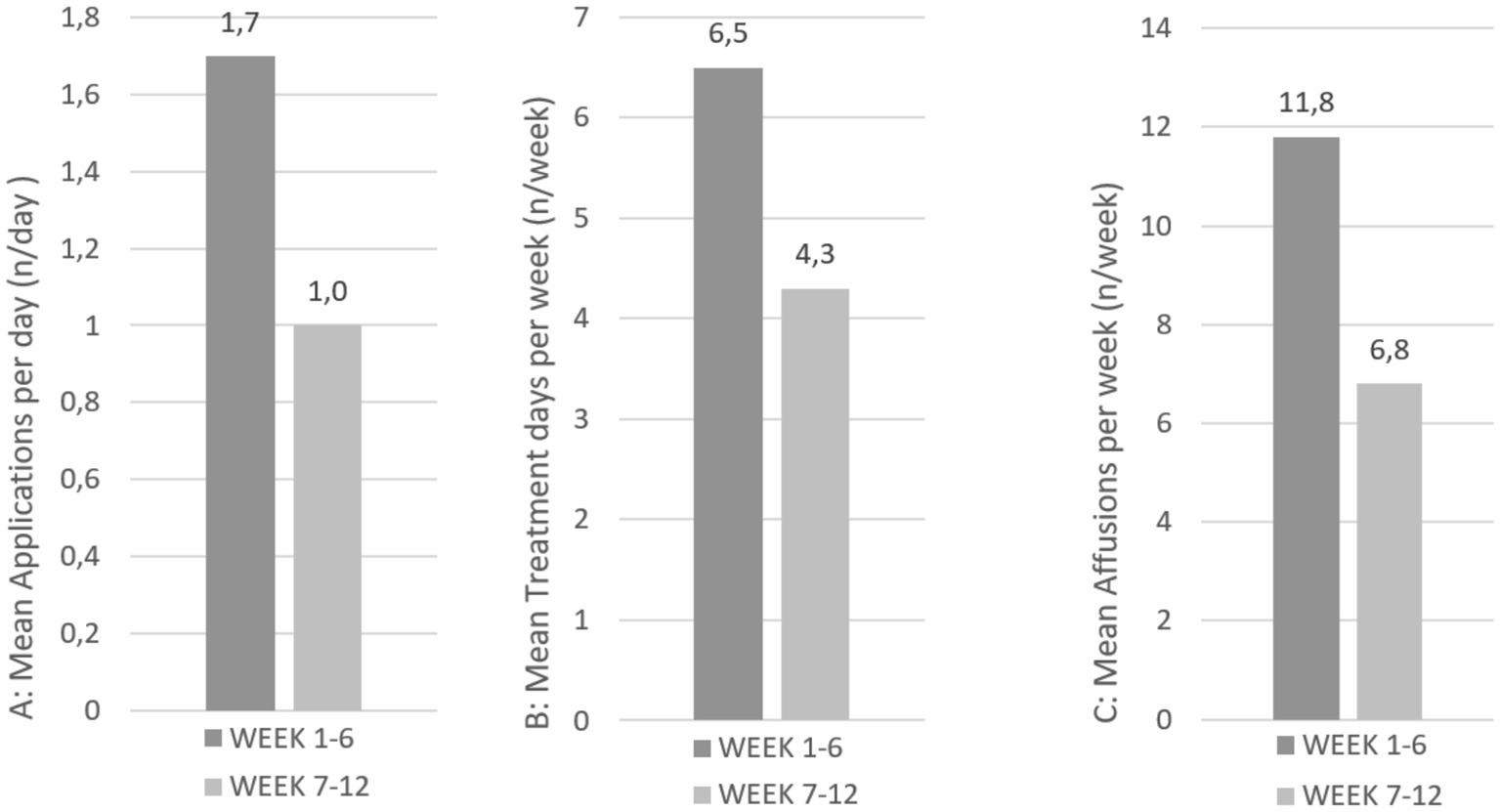
Figure 4. Treatment adherence of patients in the hydrotherapy group at weeks 6 and 12.
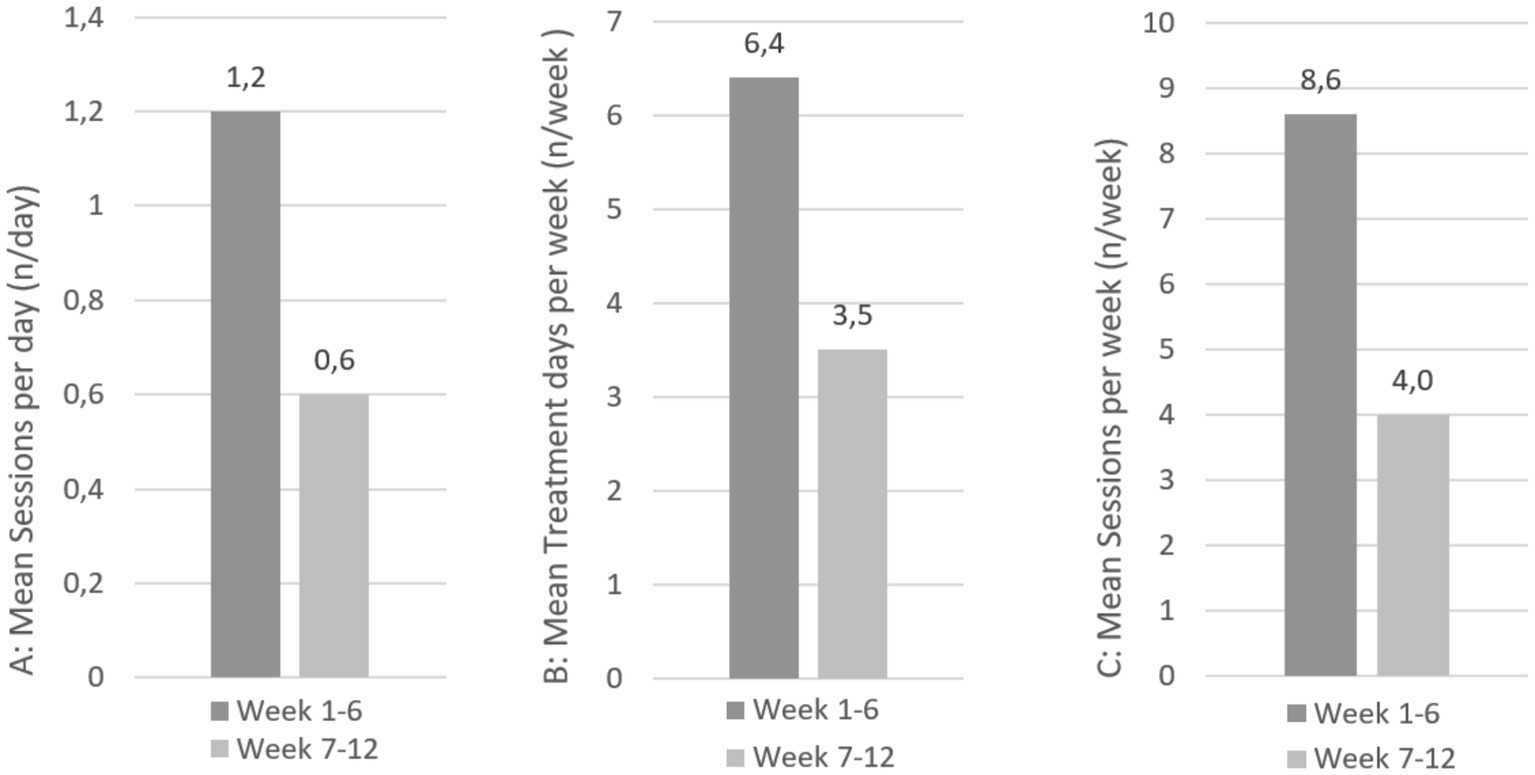
Figure 5. Treatment adherence of patients in the acupressure group at weeks 6 and 12.
After 6 weeks, for IRLS (MCID = 3), adjusted mean scores were 19.8 (95% CI [16.4, 23.2]; Figure 6; Table 2) for HT, 22.9 (19.2, 26.6) for AP, and 24.0 (20.8, 27.2) for RC, with mean differences compared to RC of −4.2 for HT and −1.1 for AP (negative values indicate improvement in IRLS). For RLSQoL (MCID = 7.1), adjusted means were 65.3 (59.7, 70.9) for HT, 68.3 (62.3, 74.3) for AP, and 56.2 (50.9, 61.5) for RC, with mean differences compared to RC of 9.1 for HT and 12.1 for AP (positive values indicate improvement in RLSQoL) (Figure 7; Table 2).
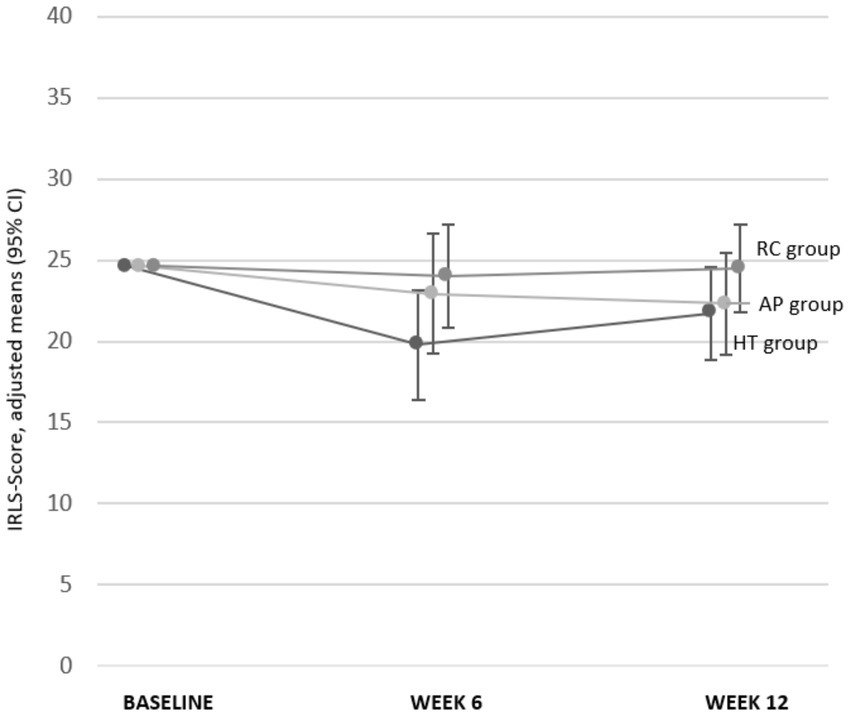
Figure 6. IRLS global score at baseline, at weeks 6 and 12. AP, Acupressure; CI, Confidence Interval; HT, Hydrotherapy; IRLS-Score [0–40], International RLS Severity Scale (higher scores indicate a worse outcome); RC, Routine Care.
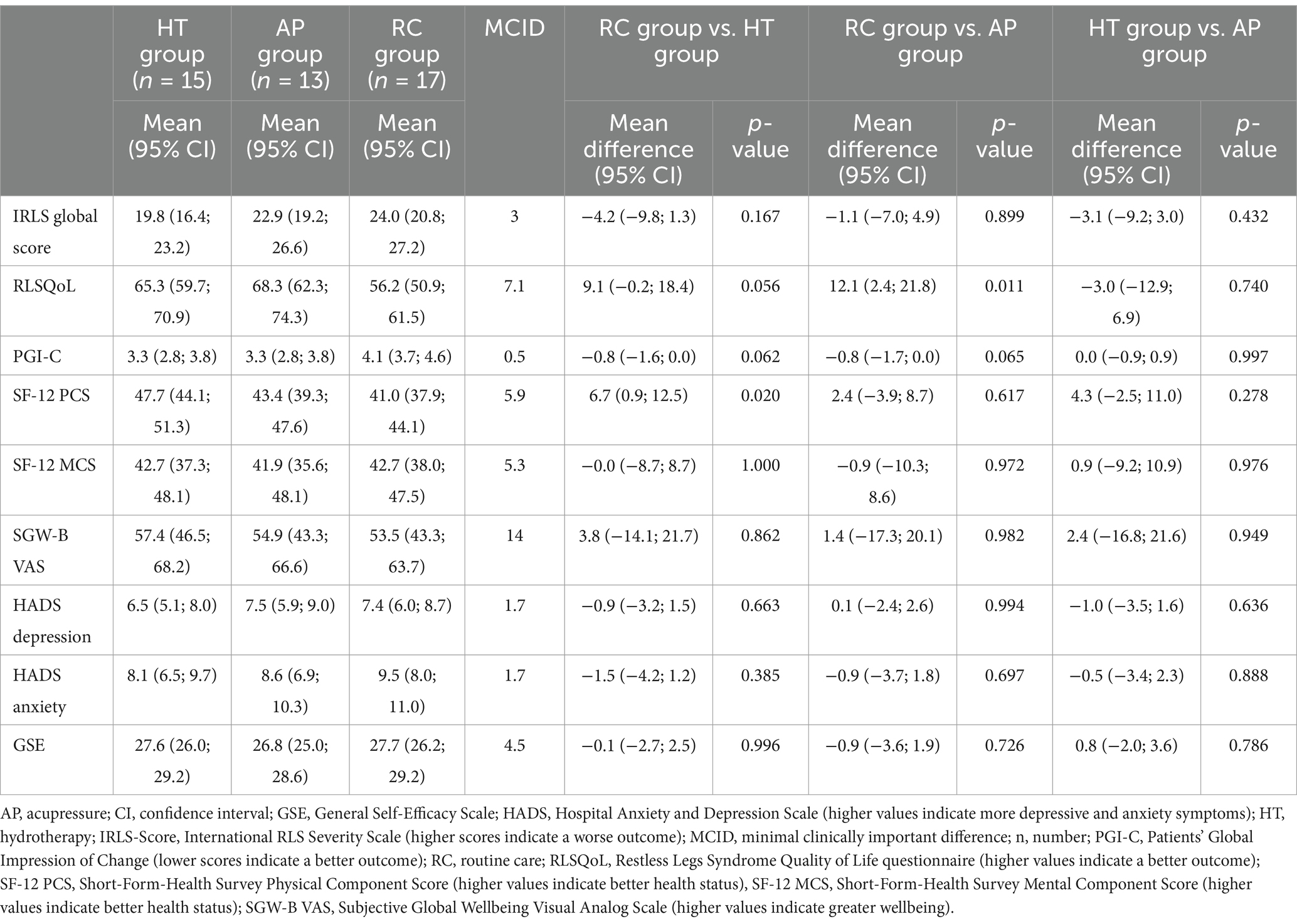
Table 2. Outcomes at week 6: group means and group differences with 95% confidence interval (CI), adjusted for respective baseline value.
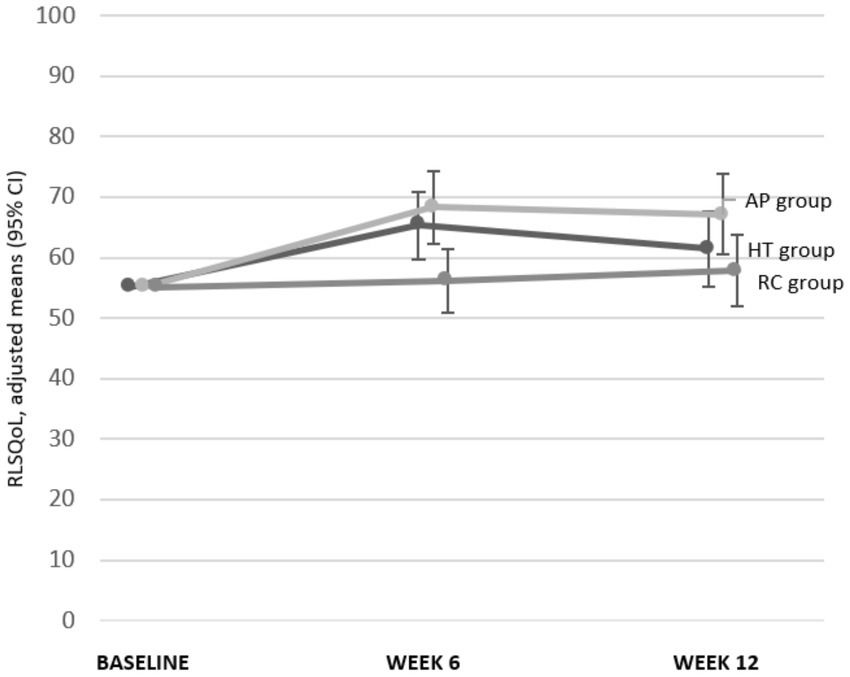
Figure 7. RLSQoL at baseline, at weeks 6 and 12. AP, Acupressure; CI, Confidence Interval; HT, Hydrotherapy; RLSQoL [0–100], Restless Legs Syndrome Quality of Life questionnaire (higher values indicate a better outcome).
For PGI-C (MCID = 0.5), adjusted means were 3.3 (2.8, 3.8) for HT, 3.3 (2.8, 3.8) for AP, and 4.1 (3.7, 4.6) for RC, with mean differences compared to RC of −0.8 for HT and − 0.8 for AP (negative values indicate improvement in PGI-C). For SF-12 PCS (MCID = 5.9), adjusted means were 47.7 (44.1, 51.3) for HT, 43.4 (39.3, 47.6) for AP, and 41.0 (37.9, 44.1) for RC, with mean differences compared to RC of 6.7 for HT and 2.4 for AP (positive values indicate improvement in SF-12 PCS). The differences in adjusted means between groups at week 6 suggest potential clinical relevance in symptom severity for the HT group, in disease-related quality of life for both intervention groups, and in physical functioning for the HT group.
Neither of the two intervention groups showed clinically relevant differences in psychological outcomes (SGW-B VAS, HADS, GSE) or mental health-related quality of life (SF-12 MCS) compared to RC at week 6 (Table 2). The baseline values were already within the normal range or only slightly altered in all groups. However, subjective global wellbeing scores were reported as being close to the mid-level of the visual analog scale, which is consistent with a mild psychological burden in RLS patients without severe mental health impairments.
Effect size calculations (Cohen’s d) at 6 weeks showed varying magnitudes across outcomes, with positive values indicating effects in favor of the intervention (Table 3). Compared to RC, HT demonstrated small effects in IRLS (d = 0.44), medium effects in RLSQoL (d = 0.57), and large effects in PGI-C (d = 0.94 [Figure 8; Table 3]). AP showed medium effects in IRLS (d = 0.56), large effects in RLSQoL (d = 0.88), and medium effects in PGI-C (d = 0.77). Psychological outcomes showed predominantly negligible effects across all groups (Figure 9; Table 3).
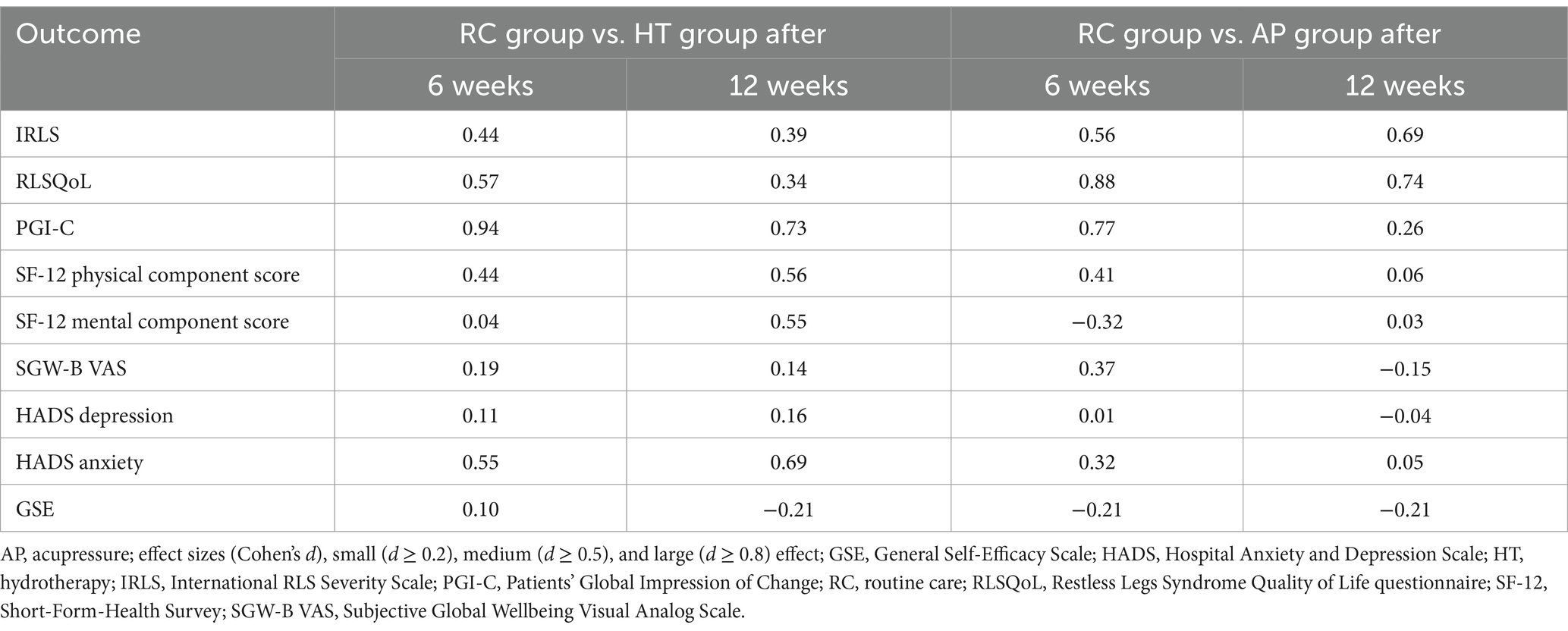
Table 3. Effect sizes (Cohen’s d) group differences adjusted for baseline differences.
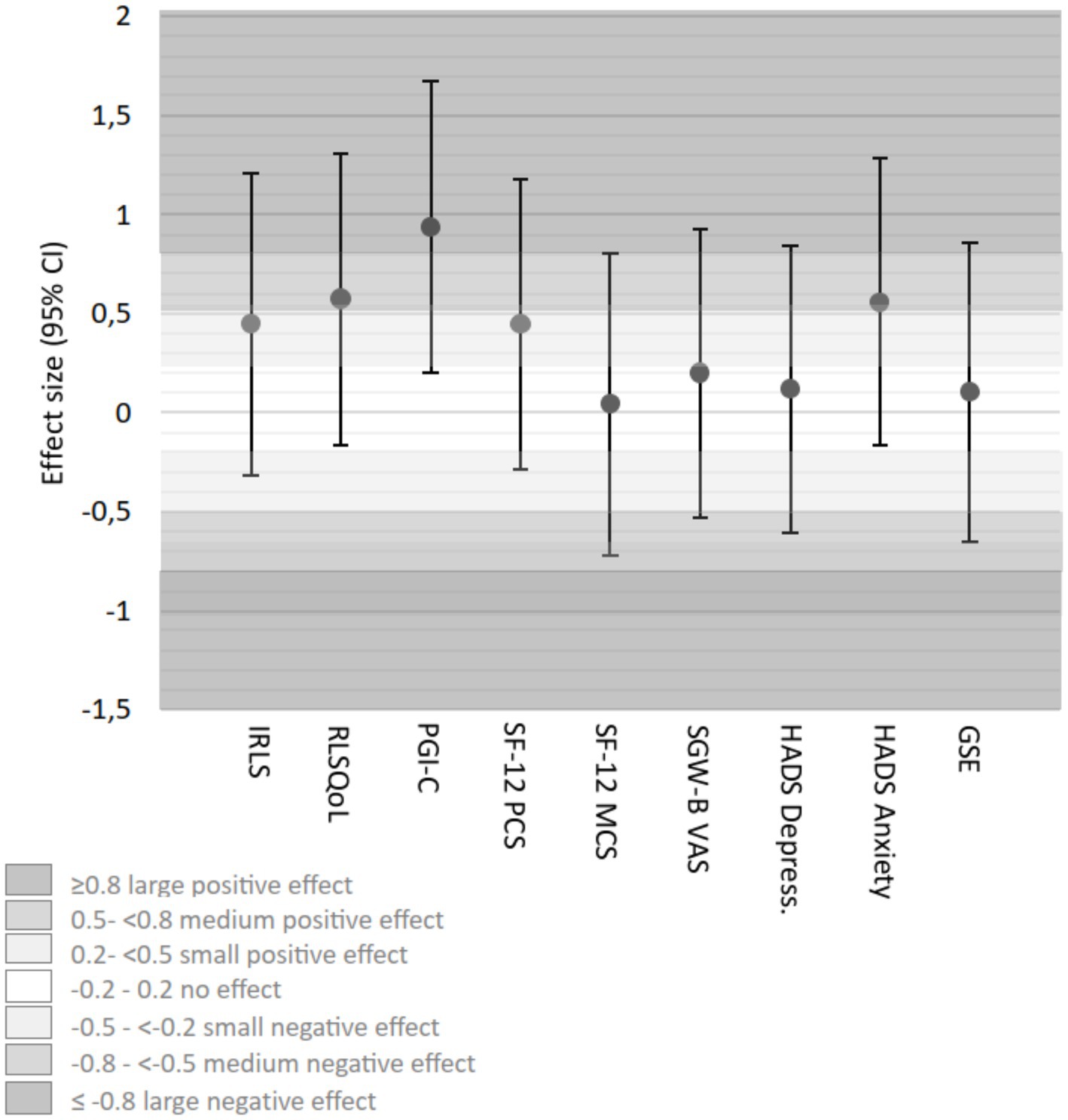
Figure 8. Effect sizes (Cohen’s d) (adjusted for baseline differences) HT group vs. RC group week 6. CI, confidence interval; GSE, General Self-Efficacy Scale; HADS, Hospital Anxiety and Depression; HT, hydrotherapy; IRLS-Score, International RLS Severity Scale; PGI-C, Patients’ Global Impression of Change; RC, routine care; RLSQoL, Restless Legs Syndrome Quality of Life questionnaire; SF-12, Short-Form-Health Survey, PCS, Physical Component Score, MCS, Mental Component Score; SGW-B VAS, Subjective Global Wellbeing Visual Analog Scale.
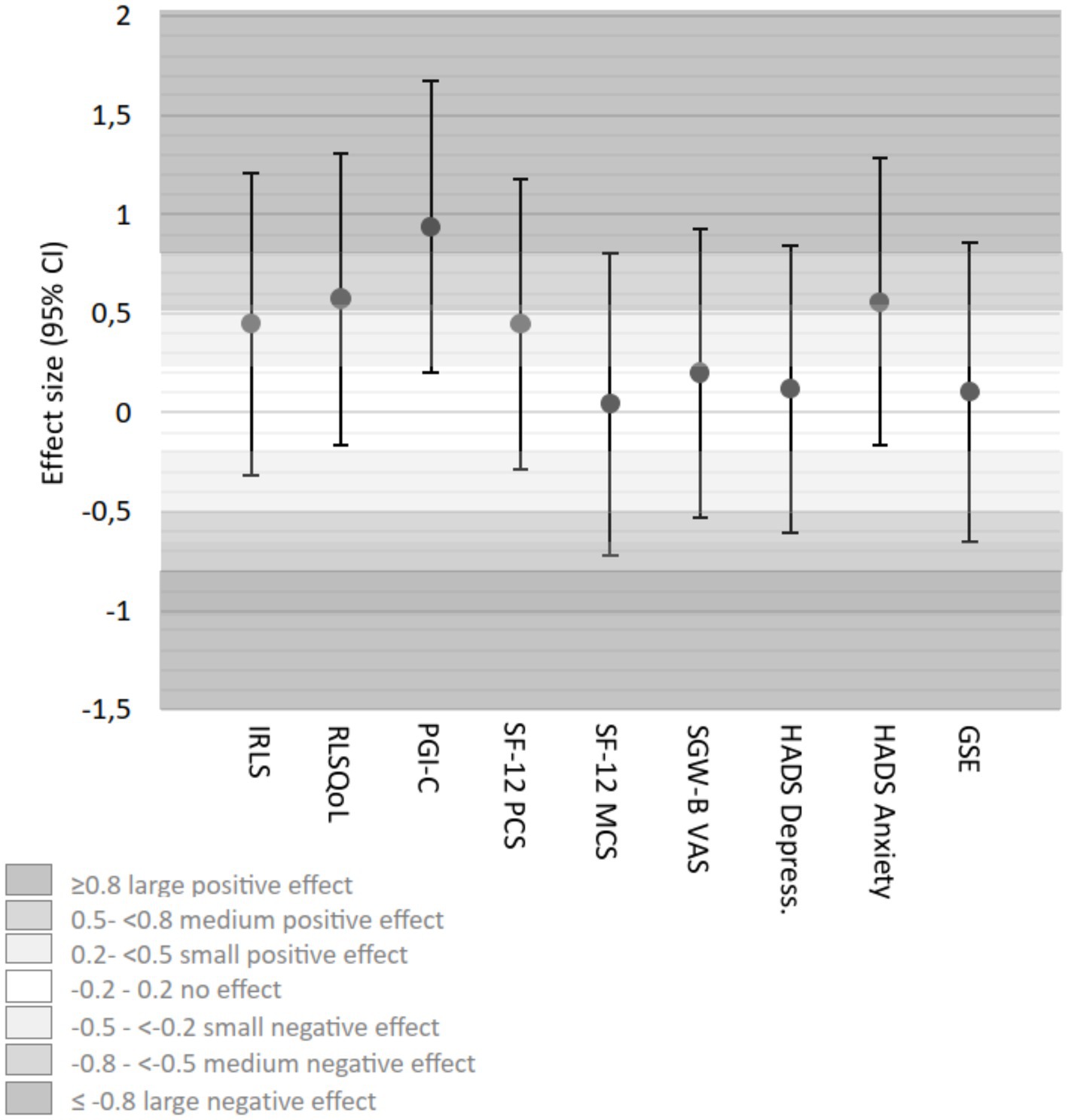
Figure 9. Effect sizes (Cohen’s d) (adjusted for baseline differences) AP group vs. RC group week 6. CI, confidence interval; GSE, General Self-Efficacy Scale; HADS, Hospital Anxiety and Depression; HT, hydrotherapy; IRLS-Score, International RLS Severity Scale; PGI-C, Patients’ Global Impression of Change; RC, routine care; RLSQoL, Restless Legs Syndrome Quality of Life questionnaire; SF-12, Short-Form-Health Survey, PCS, Physical Component Score, MCS, Mental Component Score; SGW-B VAS, Subjective Global Wellbeing Visual Analog Scale.
After 12 weeks, neither HT nor AP showed clinically relevant differences for IRLS compared to RC. In RLSQoL, AP continued to maintain a potential clinical benefit (MD = 9.2, 95% CI [−1.6, 20.1]) exceeding the estimated MCID of 7.1, while HT did not. PGI-C differences were no longer considered clinically relevant for either intervention group compared to RC. For SF-12 PCS and MCS, no relevant group differences were observed at 12 weeks. The psychological outcomes (SGW-B VAS, HADS, and GSE) continued to show no clinically relevant differences between the intervention groups and RC (Table 4).
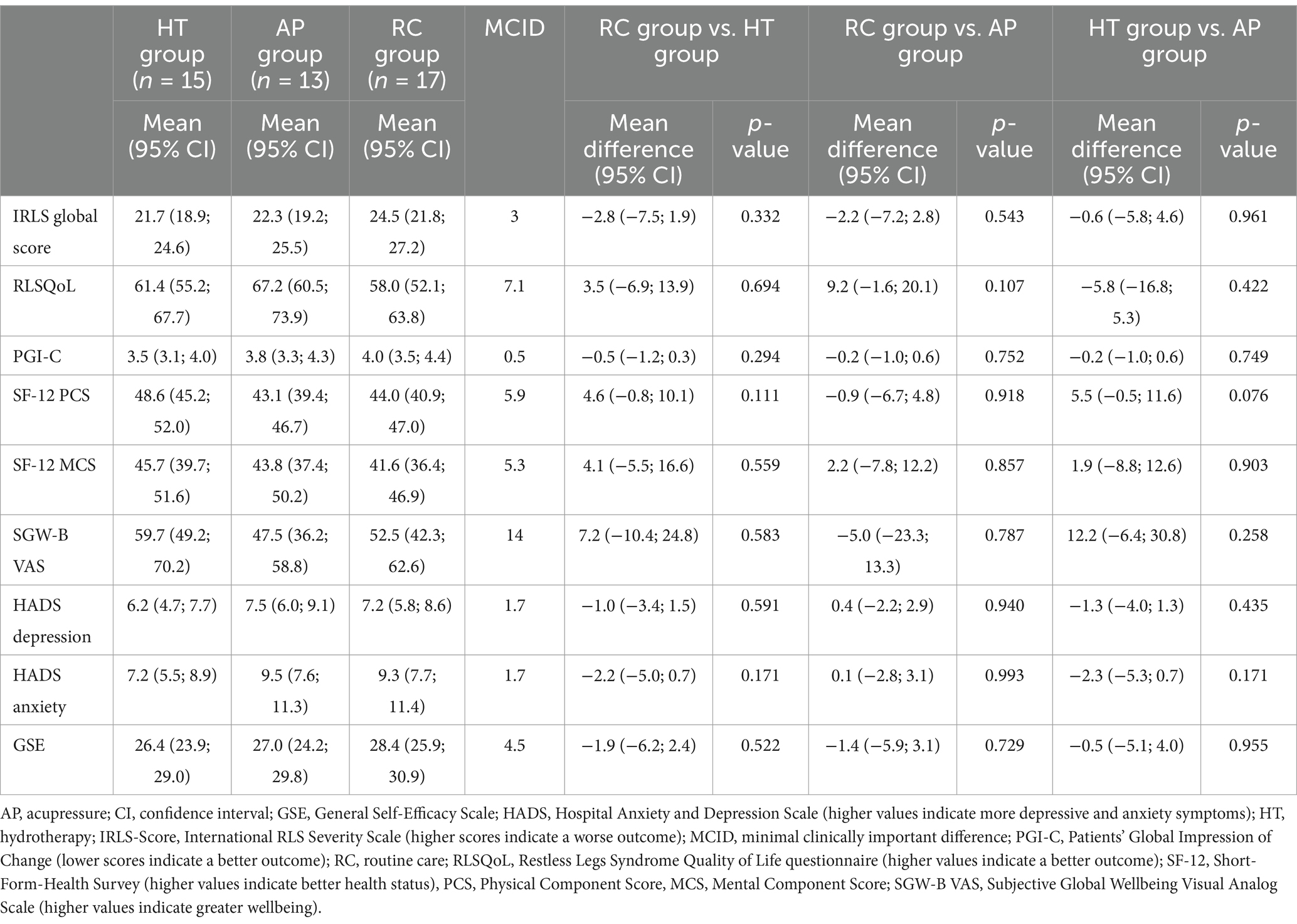
Table 4. Outcomes at week 12: group means and group differences with 95% confidence interval (CI), adjusted for respective baseline values.
Exploratory effect size analyses (Cohen’s d) at 12 weeks showed some changes compared to week 6 (Table 3). Compared to RC, HT maintained small effects in IRLS, showed small effects in RLSQoL, and moderate effects in PGI-C. AP maintained moderate effects for IRLS, showed moderate effects for RLSQoL, and small effects for PGI-C compared to RC. Consistent with the 6-week results, psychological outcomes showed negligible effects across all groups.
The total amount of medication taken and the percentage of patients taking medication remained quite stable over the course of the study in all groups. Thirty-six out of 54 patients (66.7%) were taking RLS medication at the start of the study (HT: n = 11/18, 61.1%; AP: n = 13/18, 72.2%; RC: n = 12/18, 66.7%) and 28 out of 45 patients (62.2%) at the end of weeks 6 and 12 (HT: n = 8/15, 53.3%; AP: n = 9/13, 69.2%; RC: n = 11/17, 64.7%).
None of the patients reported any serious adverse event (SAE) or adverse events (AEs) requiring medical treatment during the entire study period (Table 5). In the HT group, three patients reported mild treatment-related AEs including cold feet, foot and leg pain, and transient mild dizziness with pins and needles. In the AP group, six patients reported treatment-related AEs, mainly related to pressure application (pain in hands and finger joints, pain at acupressure points, cracked fingertips) and one patient reported headache while another reported short-term symptoms worsening during the first days. All reported AEs were mild and temporary.
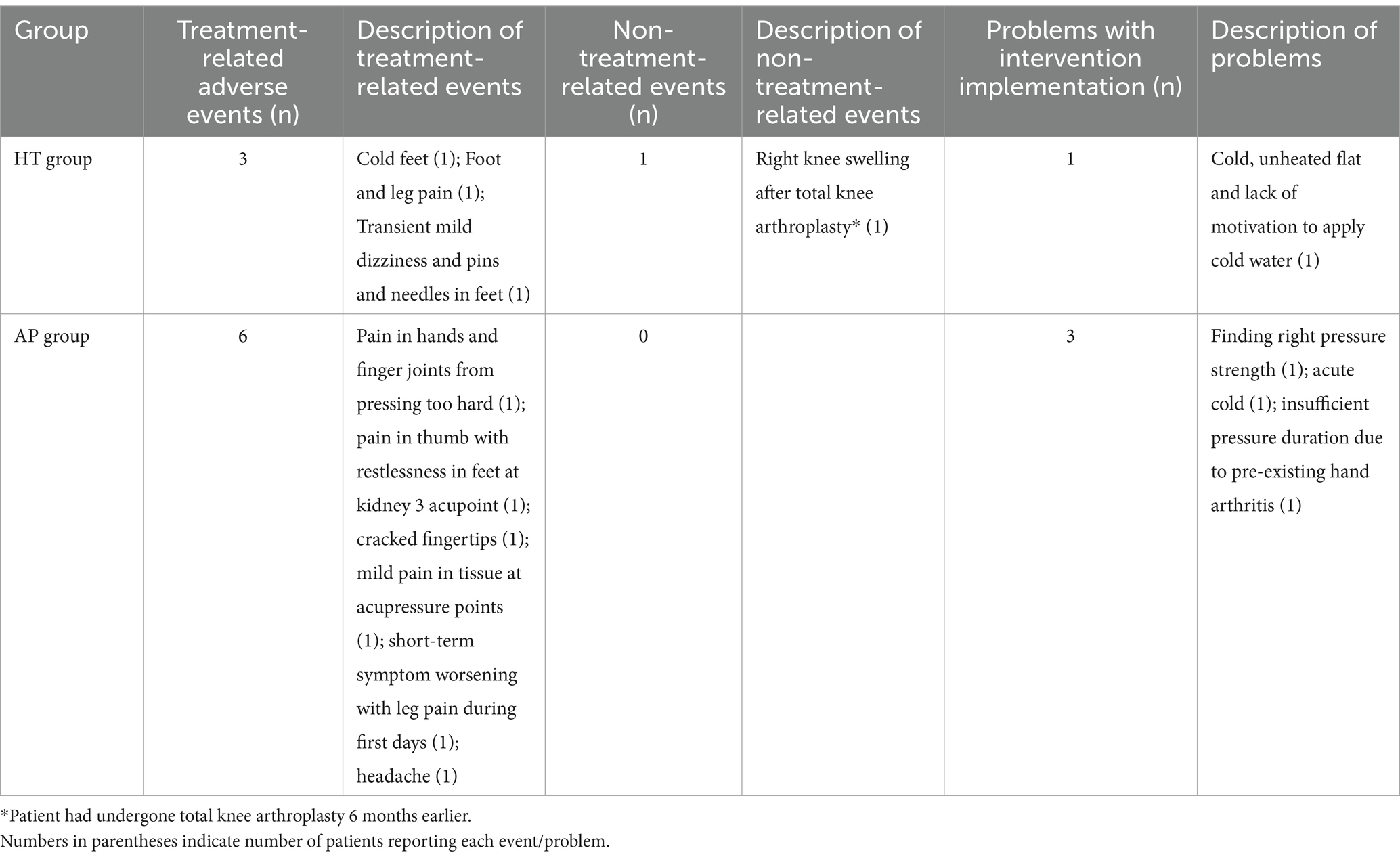
Table 5. Reported adverse events and problems with intervention implementation.
4 Discussion
Our results suggest that self-applied Kneipp hydrotherapy and acupressure are feasible. Moreover, self-applied hydrotherapy and acupressure were well-tolerated and showed high adherence overall.
With regard to the MCIDs of the outcomes both interventions suggest potentially clinically relevant differences compared to RC alone in disease-related quality of life and patients’ overall impression of change in clinical condition within the first 6 weeks. Furthermore, hydrotherapy resulted in a potentially clinically relevant difference in restless legs severity and the physical score of health-related quality of life after 6 weeks. After 12 weeks, there were still trends for clinically relevant differences in RLSQoL for the AP group. Notably, psychological outcomes remained largely unchanged across all groups, possibly due to near-normal baseline scores. As non-pharmacological treatments, hydrotherapy and acupressure could facilitate reducing or avoiding RLS medication side effects. However, given the exploratory nature and small sample size of this pilot study, these results should be interpreted as trends.
To our knowledge, this is the first RCT to assess the potential effects and feasibility of self-applied HT in the form of cold water affusions and self-applied AP in adults with RLS. Our study examined the effects on RLS symptom severity as well as on quality of life, depression/anxiety symptoms, and self-efficacy.
The strengths of the study include randomization, a high retention rate of 83%, the use of validated measurement instruments, and the development of a practical treatment manual, which is suitable for everyday clinical practice. The similarity in baseline characteristics across study groups suggests that the randomization process was effective. All participants scored in the moderate to severe range of RLS severity, with symptom scores comparable to those of participants in other RLS intervention trials (60–62). The calculation of Cohen’s d effect sizes, while not initially specified in our exploratory study protocol, provides additional standardized measures of the observed differences. Overall, the adverse events were mild and few in number, and patient adherence and motivation for self-application were high. The training was short and easy to conduct, and HT proved to be a time-saving option, as it only took 5 min a day to complete at home. Another positive aspect is that both interventions are low threshold, low-cost, can be used at home, and are easy to carry out.
However, due to its design, this exploratory RCT has several limitations such as the small sample size, which impairs the evaluation of effects and limits the generalizability of the study. Furthermore, generalizability is limited by the single-center design. The intervention training only took place once and implementation was subsequently only monitored by telephone twice. Therefore, the present study may have underestimated the impact of the interventions due to short training and little support for self-application. The comparability of the intervention groups is limited. Despite the prescribed 20-min daily intervention for both groups, the actual daily intervention duration differed substantially after 6 weeks (HT 5.2 min, AP 22.5 min), likely due to hydrotherapy’s integration into participants’ existing bathroom routines, eliminating anticipated preparation time. This study design cannot quantify various non-specific effects (such as placebo, nocebo, Hawthorne effect, regression to the mean, time effects, experimenter effect, response bias, and expectation effects) due to the absence of a placebo-controlled intervention. Future studies should consider a placebo-controlled arm (e.g., sham acupressure or temperature-matched water therapy) to better isolate the specific effects of hydrotherapy and acupressure. Moreover, an additional group of patients treated simultaneously with acupressure and hydrotherapy could provide valuable comparative findings. Furthermore, the lack of blinding may have introduced additional biases and influenced participants’ expectations, potentially affecting the results. Possible influences of concomitant medication and comorbidities on the course of symptom severity and patient’s conditions cannot be ruled out, although at least the amount of RLS medication was similar in all three groups and changed minimally over the course of the study.
Previous studies investigating cold water applications in pregnant women with RLS (32) and cryotherapy in patients with idiopathic RLS (63) reported statistically significant improvements in symptom severity (IRLS) within the group, which can also be considered clinically relevant. However, a group comparison was not performed, so the clinically relevant difference between the groups after the intervention cannot be assessed. Our findings with Kneipp-hydrotherapy suggested potential clinical benefits in symptom severity for the HT group and in quality of life for both intervention groups.
Additionally, our findings suggested potential clinically relevant benefits in the SF-12 Physical Component within 6 weeks of HT compared to control. Previous studies on hydrotherapy for post-polio syndrome and polyneuropathy showed either no or only minor improvements in physical functioning using the SF-36 Physical Component (34, 64, 65).
There are several possible pathways through which hydrotherapy may benefit RLS patients, although the exact mechanisms are unknown. Cold water stimuli activate the vegetative nervous system, triggering local and reflex-like effects such as local reactive hyperemia (66, 67) and a reduced sympathetic tone when repeated regularly (67). Reactive hyperemia is accompanied by an increase in oxygen concentration, muscular relaxation, and a subjective feeling of wellbeing (66–68). The suspected causes of the multifactorial development of RLS include peripheral hypoxia (69, 70), impaired microvascular blood flow (71), low oxygen partial pressure in the legs (72), increased spindle activity and muscle tone (73), and autonomic dysfunction (74–77).
Our pilot study suggested potential clinically relevant benefits in terms of disease-specific quality of life (RLSQoL) and patient’s global impression of change (PGI-C) after 6 weeks of self-applied acupressure compared to control, while effects on symptom severity (IRLS) were less pronounced. These results contrast with previous studies on acupuncture and non-self-applied acupressure, which showed greater symptom reduction: In three systematic reviews on acupuncture (25, 28, 29) and one meta-analysis of acupuncture (30), comparisons between the groups showed statistically significant differences in IRLS, which were also clinically relevant for acupuncture. Additionally, clinically relevant IRLS reductions within-group improvements were found in one RCT using a crossover design testing acupressure in hemodialysis patients with RLS (31). The differences in our findings compared to previous research regarding symptom severity may be due to the self-application method, sample size limitations, and the exploratory design of our study.
Acupressure and acupuncture activate identical acupoints, though self-applied acupressure may be limited to accessing certain potent paraspinal points, which are commonly used in both general and RLS-specific acupuncture treatments. It is assumed that the activation of the acupoint targets the autonomic nervous system to unfold its effect. This could be helpful in the treatment of RLS as we see an apparent autonomic dysfunction (74–76, 78). Acupressure stimulation regulates parasympathetic nervous system activity, which increases sleep quality by increasing autonomic responses and reducing psychological distress (79, 80). Since psychological stress can contribute to an unfavorable treatment outcome and may exacerbate symptoms in RLS patients, it must be considered in the treatment of severely affected patients. In addition, acupuncture has been shown to have anti-inflammatory effects (81) via multiple physiological pathways including the hypothalamus–pituitary–adrenal (HPA) axis (82–85), sympathetic pathways (via both sympathetic postganglionic neurons and the sympathoadrenal medullary axis) (84, 85), peripheral opioid mechanisms (86) and possibly parasympathetic cholinergic pathways (87–90). The anti-inflammatory effects of acupoint activation, which also runs through the opioid system, can be helpful in the treatment of RLS, as we observe impairment of the body’s opioid system (91, 92) and signs of increased inflammation (93–95) in RLS patients. It is also reported that acupuncture reduces oxidative stress (96, 97), which is discussed in the pathogenesis of RLS (98, 99).
The study results demonstrate the feasibility, acceptability, and potential effects of the study interventions and, in our opinion, justify larger confirmatory clinical trials. In addition to a larger sample size, future randomized clinical studies should have a multicenter design to achieve better generalizability and representativeness. Intervention groups with more detailed and longer treatment instruction, as well as personal follow-up meetings with the option of correcting the intervention’s execution could show greater intervention effects. A longer intervention and follow-up phase could provide a better assessment of long-term effects and the sustainability of the interventions. The impact of water affusions should be examined through a systematic comparison of different temperatures, application methods, and locations. In addition, objective measures such as heart rate variability and periodic leg movements can be included as study outcomes. Future studies should consider the use of acupressure devices with pressure sensors to achieve better standardization. Additionally, exploring alternative acupressure schemes, including paraspinal points, could provide further insights into RLS treatment. For future studies, we suggest considering the RLSQoL as a key outcome measure, given its clinical relevance in capturing the multifaced impact of RLS on patients’ lives.
5 Conclusion
Self-applied hydrotherapy and acupressure appear to be feasible and safe interventions for patients with RLS. This exploratory pilot study suggests potential benefits, though larger, well-designed confirmatory studies are needed to validate these findings.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by ethics committee of Charité-Universitätsmedizin Berlin. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JK: Conceptualization, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. MO: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. SB: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. SR: Formal analysis, Methodology, Writing – original draft, Writing – review & editing. KI: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. JD: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. RN: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. JH: Conceptualization, Methodology, Writing – original draft, Writing – review & editing. SW: Conceptualization, Writing – original draft, Writing – review & editing. BB: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. MT: Conceptualization, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. JS: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Funding for this study was provided in part by the Karl and Veronica Carstens Foundation, which has made grants available as part of the Young Clinician Scientists grant program (scholarship recipient: JS). The foundation had no influence on the design, methodology, conduct, analysis, or publication of the study.
Acknowledgments
We would like to thank the entire study team, including Margit Cree and Katharina Kleinsteuber (members of the HYDRAC study secretary) and the experts for their outstanding work on this study. We thank Ryan King for performing the statistical analyses and for their valuable input into the interpretation of the data.
Conflict of interest
JH and RN are associate board members of the SMS - Societas Medicinae Sinensis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Allen, RP, and Earley, CJ. Restless legs syndrome: a review of clinical and pathophysiologic features. J Clin Neurophysiol. (2001) 18:128–47. doi: 10.1097/00004691-200103000-00004
2. Happe, S, Reese, JP, Stiasny-Kolster, K, Peglau, I, Mayer, G, Klotsche, J, et al. Assessing health-related quality of life in patients with restless legs syndrome. Sleep Med. (2009) 10:295–305. doi: 10.1016/j.sleep.2008.01.002
3. Broström, A, Alimoradi, Z, Odzakovic, E, Kaldo, V, Jernelöv, S, Lind, J, et al. Quality of life among patients with restless legs syndrome: a systematic review and meta-analysis. J Clin Neurosci. (2024) 122:80–91. doi: 10.1016/j.jocn.2024.02.027
4. Broström, A, Alimoradi, Z, Lind, J, Ulander, M, Lundin, F, and Pakpour, A. Worldwide estimation of restless legs syndrome: a systematic review and meta-analysis of prevalence in the general adult population. J Sleep Res. (2023) 32:e13783. doi: 10.1111/jsr.13783
5. Trenkwalder, C, Tinelli, M, Sakkas, GK, Dauvilliers, Y, Ferri, R, Rijsman, R, et al. Socioeconomic impact of restless legs syndrome and inadequate restless legs syndrome management across European settings. Eur J Neurol. (2021) 28:691–706. doi: 10.1111/ene.14582
6. Trenkwalder, C, Allen, R, Högl, B, Paulus, W, and Winkelmann, J. Restless legs syndrome associated with major diseases: a systematic review and new concept. Neurology. (2016) 86:1336–43. doi: 10.1212/WNL.0000000000002542
7. Salas, RE, and Kwan, AB. The real burden of restless legs syndrome: clinical and economic outcomes. Am J Manag Care. (2012) 18:S207–12.
8. Manconi, M, Garcia-Borreguero, D, Schormair, B, Videnovic, A, Berger, K, Ferri, R, et al. Restless legs syndrome. Nat Rev Dis Primers. (2021) 7:80. doi: 10.1038/s41572-021-00311-z
9. Garcia-Borreguero, D, Ferini-Strambi, L, Kohnen, R, O'Keeffe, S, Trenkwalder, C, Högl, B, et al. European guidelines on management of restless legs syndrome: report of a joint task force by the European Federation of Neurological Societies, the European Neurological Society and the European Sleep Research Society. Eur J Neurol. (2012) 19:1385–96. doi: 10.1111/j.1468-1331.2012.03853.x
10. Allen, RP, Picchietti, DL, Garcia-Borreguero, D, Ondo, WG, Walters, AS, Winkelman, JW, et al. Restless legs syndrome/Willis-Ekbom disease diagnostic criteria: updated International Restless Legs Syndrome Study Group (IRLSSG) consensus criteria--history, rationale, description, and significance. Sleep Med. (2014) 15:860–73. doi: 10.1016/j.sleep.2014.03.025
11. Abetz, L, Allen, R, Follet, A, Washburn, T, Earley, C, Kirsch, J, et al. Evaluating the quality of life of patients with restless legs syndrome. Clin Ther. (2004) 26:925–35. doi: 10.1016/s0149-2918(04)90136-1
12. Didriksen, M, Allen, RP, Burchell, BJ, Thørner, LW, Rigas, AS, Di Angelantonio, E, et al. Restless legs syndrome is associated with major comorbidities in a population of Danish blood donors. Sleep Med. (2018) 45:124–31. doi: 10.1016/j.sleep.2018.02.007
13. Scholz, H, Benes, H, Happe, S, Bengel, J, Kohnen, R, and Hornyak, M. Psychological distress of patients suffering from restless legs syndrome: a cross-sectional study. Health Qual Life Outcomes. (2011) 9:73. doi: 10.1186/1477-7525-9-73
14. Castillo, PR, Mera, RM, Fredrickson, PA, Zambrano, M, Del Brutto, VJ, and Del Brutto, OH. Psychological distress in patients with restless legs syndrome (Willis-Ekbom disease): a population-based door-to-door survey in rural Ecuador. BMC Res Notes. (2014) 7:911. doi: 10.1186/1756-0500-7-911
15. Vlasie, A, Trifu, SC, Lupuleac, C, Kohn, B, and Cristea, MB. Restless legs syndrome: an overview of pathophysiology, comorbidities and therapeutic approaches (review). Exp Ther Med. (2022) 23:185. doi: 10.3892/etm.2021.11108
16. Heidbreder, A, Trenkwalder, C, Bachmann, C, Bartl, M, Fulda, S, Habersack, L, et al. Restless legs syndrom, S2k-Leitlinie Deutsche Gesellschaft für Neurologie und Deutsche Gesellschaft für Schlafforschung und Schlafmedizin (Berlin, Germany: DGSM) (2022).
17. Garcia-Borreguero, D, Silber, MH, Winkelman, JW, Högl, B, Bainbridge, J, Buchfuhrer, M, et al. Guidelines for the first-line treatment of restless legs syndrome/Willis-Ekbom disease, prevention and treatment of dopaminergic augmentation: a combined task force of the IRLSSG, EURLSSG, and the RLS-foundation. Sleep Med. (2016) 21:1–11. doi: 10.1016/j.sleep.2016.01.017
18. García-Borreguero, D, Högl, B, Ferini-Strambi, L, Winkelman, J, Hill-Zabala, C, Asgharian, A, et al. Systematic evaluation of augmentation during treatment with ropinirole in restless legs syndrome (Willis-Ekbom disease): results from a prospective, multicenter study over 66 weeks. Mov Disord. (2012) 27:277–83. doi: 10.1002/mds.24889
19. Allen, RP, Ondo, WG, Ball, E, Calloway, MO, Manjunath, R, Higbie, RL, et al. Restless legs syndrome (RLS) augmentation associated with dopamine agonist and levodopa usage in a community sample. Sleep Med. (2011) 12:431–9. doi: 10.1016/j.sleep.2011.03.003
20. Högl, B, García-Borreguero, D, Kohnen, R, Ferini-Strambi, L, Hadjigeorgiou, G, Hornyak, M, et al. Progressive development of augmentation during long-term treatment with levodopa in restless legs syndrome: results of a prospective multi-center study. J Neurol. (2010) 257:230–7. doi: 10.1007/s00415-009-5299-8
21. Voon, V, Schoerling, A, Wenzel, S, Ekanayake, V, Reiff, J, Trenkwalder, C, et al. Frequency of impulse control behaviours associated with dopaminergic therapy in restless legs syndrome. BMC Neurol. (2011) 11:117. doi: 10.1186/1471-2377-11-117
22. Trenkwalder, C, Hening, WA, Montagna, P, Oertel, WH, Allen, RP, Walters, AS, et al. Treatment of restless legs syndrome: an evidence-based review and implications for clinical practice. Mov Disord. (2008) 23:2267–302. doi: 10.1002/mds.22254
23. Garcia-Borreguero, D, Kohnen, R, Silber, MH, Winkelman, JW, Earley, CJ, Högl, B, et al. The long-term treatment of restless legs syndrome/Willis-Ekbom disease: evidence-based guidelines and clinical consensus best practice guidance: a report from the international restless legs syndrome study group. Sleep Med. (2013) 14:675–84. doi: 10.1016/j.sleep.2013.05.016
24. Bozorg Ali, M. Restless legs syndrome guidelines: treatment and management. (2022). Available online at: https://emedicine.medscape.com/article/1188327-treatment (Accessed December 4, 2022).
25. Harrison, EG, Keating, JL, and Morgan, PE. Non-pharmacological interventions for restless legs syndrome: a systematic review of randomised controlled trials. Disabil Rehabil. (2019) 41:2006–14. doi: 10.1080/09638288.2018.1453875
26. Selfe, TK, Wen, S, Sherman, K, Klatt, M, and Innes, KE. Acceptability and feasibility of a 12-week yoga vs. educational film program for the management of restless legs syndrome (RLS): study protocol for a randomized controlled trial. Trials. (2019) 20:134. doi: 10.1186/s13063-019-3217-7
27. Winkelman, JW, Berkowski, JA, DelRosso, LM, Koo, BB, Scharf, MT, Sharon, D, et al. Treatment of restless legs syndrome and periodic limb movement disorder: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. (2024) 21:137–52. doi: 10.5664/jcsm.11390
28. Xu, X-M, Liu, Y, Jia, S-Y, Dong, M-X, Cao, D, and Wei, Y-D. Complementary and alternative therapies for restless legs syndrome: an evidence-based systematic review. Sleep Med Rev. (2018) 38:158–67. doi: 10.1016/j.smrv.2017.06.003
29. Guay, A, Houle, M, O'Shaughnessy, J, and Descarreaux, M. Current evidence on diagnostic criteria, relevant outcome measures, and efficacy of nonpharmacologic therapy in the management of restless legs syndrome (RLS): a scoping review. J Manip Physiol Ther. (2020) 43:930–41. doi: 10.1016/j.jmpt.2020.05.004
30. Huang, C, Tang, J-F, Sun, W, Wang, L-Z, and Jin, Y-S. Effectiveness of acupuncture in the management of restless leg syndrome: a systematic review and meta-analysis. Ann Palliat Med. (2021) 10:10495–505. doi: 10.21037/apm-21-2309
31. Tsai, L-H, Chen, C-M, Lin, L-M, Tsai, C-C, Han, Y, and See, L-C. Acupressure reduces the severity of restless legs syndrome in hemodialysis patients: a cluster-randomized crossover pilot study. Biom J. (2021) 45:533–41. doi: 10.1016/j.bj.2021.05.005
32. Jafarimanesh, H, Vakilian, K, and Mobasseri, S. Thermo-therapy and cryotherapy to decrease the symptoms of restless leg syndrome during the pregnancy: a randomized clinical trial. Complement Ther Med. (2020) 50:102409. doi: 10.1016/j.ctim.2020.102409
33. Haug, C. Literaturrecherche und Bewertung klinischer Therapiestudien zur Wassertherapie nach Kneipp (Literature research and evaluation of clinical therapy studies on water therapy according to Kneipp) [Ulm, Univ, Diss.]. (2005).
34. Ortiz, M, Koch, AK, Cramer, H, Linde, K, Rotter, G, Teut, M, et al. Clinical effects of Kneipp hydrotherapy: a systematic review of randomised controlled trials. BMJ Open. (2023) 13:e070951. doi: 10.1136/bmjopen-2022-070951
35. Yeung, W-F, Ho, FY-Y, Chung, K-F, Zhang, Z-J, Yu, BY-M, Suen, LK-P, et al. Self-administered acupressure for insomnia disorder: a pilot randomized controlled trial. J Sleep Res. (2018) 27:220–31. doi: 10.1111/jsr.12597
36. Shen, K, Cho, Y, Pascoe, EM, Hawley, CM, Oliver, V, Hughes, KM, et al. The SIESTA trial: a randomized study investigating the efficacy, safety, and tolerability of acupressure versus sham therapy for improving sleep quality in patients with end-stage kidney disease on hemodialysis. Evid Based Complement Alternat Med. (2017) 2017:7570352. doi: 10.1155/2017/7570352
37. Israel, L, Rotter, G, Förster-Ruhrmann, U, Hummelsberger, J, Nögel, R, Michalsen, A, et al. Acupressure in patients with seasonal allergic rhinitis: a randomized controlled exploratory trial. Chin Med. (2021) 16:137–14. doi: 10.1186/s13020-021-00536-w
38. Bega, D, and Malkani, R. Alternative treatment of restless legs syndrome: an overview of the evidence for mind-body interventions, lifestyle interventions, and neutraceuticals. Sleep Med. (2016) 17:99–105. doi: 10.1016/j.sleep.2015.09.009
39. Kubasch, J, Ortiz, M, Binting, S, King, R, Dietzel, J, Nögel, R, et al. Hydrotherapy and acupressure in restless legs syndrome: a randomized, controlled, 3-armed, explorative clinical trial. Medicine (Baltimore). (2023) 102:e34046. doi: 10.1097/MD.0000000000034046
40. Abetz, L, Arbuckle, R, Allen, RP, Garcia-Borreguero, D, Hening, W, Walters, AS, et al. The reliability, validity and responsiveness of the international restless legs syndrome study group rating scale and subscales in a clinical-trial setting. Sleep Med. (2006) 7:340–9. doi: 10.1016/j.sleep.2005.12.011
41. Abetz, L, Vallow, SM, Kirsch, J, Allen, RP, Washburn, T, and Earley, CJ. Validation of the restless legs syndrome quality of life questionnaire. Value Health. (2005) 8:157–67. doi: 10.1111/j.1524-4733.2005.03010.x
42. Bullinger, M, and Morfeld, M. Der health survey SF-36/SF-12: Darstellung und aktuelle Entwicklungen (the SF-36/SF-12 health survey: presentation and current developments) In: C Maurischat, M Morfeld, T Kohlmann, and M Bullinger, editors. Lebensqualität: Nützlichkeit und Psychometrie des health survey SF-36/SF-12 in der medizinischen rehabilitation (Quality of life: usefulness and psychometrics of the SF-36/SF-12 health survey in medical rehabilitation). Pabst: Lengerich (2004). 15–27.
43. Bullinger, M, Morfeld, M, Kohlmann, T, Nantke, J, van den Bussche, H, Dodt, B, et al. Der SF-36 in der rehabilitationswissenschaftlichen Forschung. Rehabilitation (Stuttg). (2003) 42:218–25. doi: 10.1055/s-2003-41645
44. Guy, W. ECDEU assessment manual for psychopharmacology. Rockville, Maryland, USA: U.S. Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs (1976).
45. Aitken, RC. Measurement of feelings using visual analogue scales. Proc R Soc Med. (1969) 62:989–93. doi: 10.1177/003591576906201005
46. Hermann-Lingen, C, Buss, U, and Snaith, RP. Hospital anxiety and depression scale - German version (HADS-D). 3., aktualisierte und neu normierte Aufl. Bern: Verlag Hans Huber (2011).
47. Schwarzer, R, and Jerusalem, M. General self-efficacy scale (GSE). In: Weinman J, Wright S, Johnston M, editors. Measures in health psychology: A user’s portfolio. Causal and control beliefs. Windsor (UK): NFER-NELSON (1995). p. 35–7.
48. Schwarzer, R, and Jerusalem, M. SWE - Skala zur Allgemeinen Selbstwirksamkeitserwartung: [Verfahrensdokumentation, Autorenbeschreibung und Fragebogen] ; Trier: Leibniz-Zentrum für Psychologische Information und Dokumentation (ZPID); (2003). doi: 10.23668/psycharchives.307
49. Allen, RP. Minimal clinically significant change for the international restless legs syndrome study group rating scale in clinical trials is a score of 3. Sleep Med. (2013) 14:1229. doi: 10.1016/j.sleep.2013.08.001
50. Norman, GR, Sloan, JA, and Wyrwich, KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care. (2003) 41:582–92. doi: 10.1097/01.MLR.0000062554.74615.4C
51. Jaeschke, R, Singer, J, and Guyatt, GH. Measurement of health status. Ascertaining the minimal clinically important difference. Control Clin Trials. (1989) 10:407–15. doi: 10.1016/0197-2456(89)90005-6
52. Hoerster, KD, Hunter-Merrill, R, Nguyen, T, Rise, P, Barón, AE, McDowell, J, et al. Effect of a remotely delivered self-directed behavioral intervention on body weight and physical health status among adults with obesity: the D-ELITE randomized clinical trial. JAMA. (2022) 328:2230–41. doi: 10.1001/jama.2022.21177
53. Maltenfort, M, and Díaz-Ledezma, C. Statistics in brief: minimum clinically important difference-availability of reliable estimates. Clin Orthop Relat Res. (2017) 475:933–46. doi: 10.1007/s11999-016-5204-6
54. Palumbo, C, Bruni, A, Antonelli, A, Artibani, W, Bassi, P, Bertoni, F, et al. Health-related quality of life 24 months after prostate cancer diagnosis: an update from the pros-IT CNR prospective observational study. Minerva Urol Nephrol. (2022) 74:11–20. doi: 10.23736/S2724-6051.20.04032-1
55. Lee, JS, Hobden, E, Stiell, IG, and Wells, GA. Clinically important change in the visual analog scale after adequate pain control. Acad Emerg Med. (2003) 10:1128–30. doi: 10.1111/j.1553-2712.2003.tb00586.x
56. Tashjian, RZ, Deloach, J, Porucznik, CA, and Powell, AP. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease. J Shoulder Elb Surg. (2009) 18:927–32. doi: 10.1016/j.jse.2009.03.021
57. Lemay, KR, Tulloch, HE, Pipe, AL, and Reed, JL. Establishing the minimal clinically important difference for the hospital anxiety and depression scale in patients with cardiovascular disease. J Cardiopulm Rehabil Prev. (2019) 39:E6–E11. doi: 10.1097/HCR.0000000000000379
58. Institut für Qualität und Wirtschaftlichkeit im Gesundheitswesen. Dokumentation und Würdigung der Anhörung zum Entwurf der Allgemeinen Methoden 6.0. Available online at: https://www.iqwig.de/methoden/allgemeine-methoden_dwa-entwurf-fuer-version-6-0_v1-0.pdf (Accessed November 13, 2024).
59. U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) [Internet]. Version 5.0. Bethesda (MD): National Cancer Institute; (2017). Available from: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm
60. Pan, W, Wang, M, Li, M, Wang, Q, Kwak, S, Jiang, W, et al. Actigraph evaluation of acupuncture for treating restless legs syndrome. Evid Based Complement Alternat Med. (2015) 2015:343201. doi: 10.1155/2015/343201
61. Aukerman, MM, Aukerman, D, Bayard, M, Tudiver, F, Thorp, L, and Bailey, B. Exercise and restless legs syndrome: a randomized controlled trial. J Am Board Fam Med. (2006) 19:487–93. doi: 10.3122/jabfm.19.5.487
62. Hornyak, M, Scholz, H, Kohnen, R, Bengel, J, Kassubek, J, and Trenkwalder, C. What treatment works best for restless legs syndrome? Meta-analyses of dopaminergic and non-dopaminergic medications. Sleep Med Rev. (2014) 18:153–64. doi: 10.1016/j.smrv.2013.03.004
63. Happe, S, Evers, S, Thiedemann, C, Bunten, S, and Siegert, R. Whole body and local cryotherapy in restless legs syndrome: a randomized, single-blind, controlled parallel group pilot study. J Neurol Sci. (2016) 370:7–12. doi: 10.1016/j.jns.2016.09.006
64. Koch, B. Evaluation der Wirksamkeit einer häuslichen Kneippschen Hydrotherapie bei Patient/innen mit polyneuropathischen Beschwerden an den unteren Extremitäten. Berlin, Germany: Charité - Universitätsmedizin Berlin (2015).
65. Hackermeier, U. Evaluation der Wirksamkeit einer häuslichen Kneipp’schen Hydrotherapie bei Patient/innen mit Post-Polio-Syndrom: Eine randomisierte klinische Pilotstudie [Berlin, Medizinische Fakultät Charité - Universitätsmedizin Berlin, Diss., 2013]. Berlin: Medizinische Fakultät Charité - Universitätsmedizin Berlin (2013).
66. Goedsche, K, Förster, M, Kroegel, C, and Uhlemann, C. Serielle Kaltwasserreize (Kneipp'scher Oberguss) bei Patienten mit chronisch obstruktiver Bronchitis (COPD). Forsch Komplementmed. (2007) 14:158–66. doi: 10.1159/000101948
67. Ortiz, M. Evaluation der Wirksamkeit Kneippscher Hydrotherapie im ambulanten Setting bei menopausalen Beschwerden - eine randomisierte, klinische Pilotstudie. Berlin: Charité - Universitätsmedizin Berlin (2009).
68. Coccarelli, A, and Nelson, MD. Modeling reactive hyperemia to better understand and assess microvascular function: a review of techniques. Ann Biomed Eng. (2023) 51:479–92. doi: 10.1007/s10439-022-03134-5
69. Salminen, AV, Rimpilä, V, and Polo, O. Peripheral hypoxia in restless legs syndrome (Willis-Ekbom disease). Neurology. (2014) 82:1856–61. doi: 10.1212/WNL.0000000000000454
70. Wåhlin-Larsson, B, Ulfberg, J, Aulin, KP, and Kadi, F. The expression of vascular endothelial growth factor in skeletal muscle of patients with sleep disorders. Muscle Nerve. (2009) 40:556–61. doi: 10.1002/mus.21357
71. Anderson, KN, Di Maria, C, and Allen, J. Novel assessment of microvascular changes in idiopathic restless legs syndrome (Willis-Ekbom disease). J Sleep Res. (2013) 22:315–21. doi: 10.1111/jsr.12025
72. Koo, BB, Bagai, K, and Walters, AS. Restless legs syndrome: current concepts about disease pathophysiology. Tremor Other Hyperkinet Mov. (2016) 6:401. doi: 10.7916/D83J3D2G
73. van Dijkman, SC, De, JNCB, Rauwé, WM, Danhof, M, and Della, PO. Effect of age-related factors on the pharmacokinetics of lamotrigine and potential implications for maintenance dose optimisation in future clinical trials. Clin Pharmacokinet. (2018) 57:1039–53. doi: 10.1007/s40262-017-0614-5
74. Izzi, F, Placidi, F, Romigi, A, Lauretti, B, Marfia, GA, Mercuri, NB, et al. Is autonomic nervous system involved in restless legs syndrome during wakefulness? Sleep Med. (2014) 15:1392–7. doi: 10.1016/j.sleep.2014.06.022
75. Innes, KE, Selfe, TK, and Agarwal, P. Restless legs syndrome and conditions associated with metabolic dysregulation, sympathoadrenal dysfunction, and cardiovascular disease risk: a systematic review. Sleep Med Rev. (2012) 16:309–39. doi: 10.1016/j.smrv.2011.04.001
76. Goulart, LI, Delgado Rodrigues, RN, and Prieto Peres, MF. Restless legs syndrome and pain disorders: what's in common? Curr Pain Headache Rep. (2014) 18:461. doi: 10.1007/s11916-014-0461-0
77. Chenini, S, Barateau, L, Rassu, AL, Lopez, R, Guiraud, L, Cavaillès, C, et al. Systematic assessment of autonomic symptoms in restless legs syndrome. Sleep Med. (2021) 80:30–8. doi: 10.1016/j.sleep.2021.01.017
78. Li, Y-W, Li, W, Wang, S-T, Gong, Y-N, Dou, B-M, Lyu, Z-X, et al. The autonomic nervous system: a potential link to the efficacy of acupuncture. Front Neurosci. (2022) 16:1038945. doi: 10.3389/fnins.2022.1038945
79. Aygin, D, and Şen, S. Acupressure on anxiety and sleep quality after cardiac surgery: a randomized controlled trial. J Perianesth Nurs. (2019) 34:1222–31. doi: 10.1016/j.jopan.2019.03.014
80. Wiyatno, ER, Pujiastuti, RS, Suheri, T, and Saha, D. Effect of acupressure on quality of sleep and pulse rate in patients with acute myocardial infarction. Belitung Nurs J. (2017) 3:360–9. doi: 10.33546/bnj.162
81. McDonald, JL, Cripps, AW, Smith, PK, Smith, CA, Xue, CC, and Golianu, B. The anti-inflammatory effects of acupuncture and their relevance to allergic rhinitis: a narrative review and proposed model. Evid Based Complement Alternat Med. (2013) 2013:591796. doi: 10.1155/2013/591796
82. Li, A, Zhang, R-X, Wang, Y, Zhang, H, Ren, K, Berman, BM, et al. Corticosterone mediates electroacupuncture-produced anti-edema in a rat model of inflammation. BMC Complement Altern Med. (2007) 7:27. doi: 10.1186/1472-6882-7-27
83. Li, A, Lao, L, Wang, Y, Xin, J, Ren, K, Berman, BM, et al. Electroacupuncture activates corticotrophin-releasing hormone-containing neurons in the paraventricular nucleus of the hypothalamus to alleviate edema in a rat model of inflammation. BMC Complement Altern Med. (2008) 8:20. doi: 10.1186/1472-6882-8-20
84. Kim, H-W, Uh, D-K, Yoon, S-Y, Roh, D-H, Kwon, Y-B, Han, H-J, et al. Low-frequency electroacupuncture suppresses carrageenan-induced paw inflammation in mice via sympathetic post-ganglionic neurons, while high-frequency EA suppression is mediated by the sympathoadrenal medullary axis. Brain Res Bull. (2008) 75:698–705. doi: 10.1016/j.brainresbull.2007.11.015
85. Kim, H-W, Kang, S-Y, Yoon, S-Y, Roh, D-H, Kwon, Y-B, Han, H-J, et al. Low-frequency electroacupuncture suppresses zymosan-induced peripheral inflammation via activation of sympathetic post-ganglionic neurons. Brain Res. (2007) 1148:69–75. doi: 10.1016/j.brainres.2007.02.030
86. Kim, H-W, Roh, D-H, Yoon, S-Y, Kang, S-Y, Kwon, Y-B, Han, H-J, et al. The anti-inflammatory effects of low- and high-frequency electroacupuncture are mediated by peripheral opioids in a mouse air pouch inflammation model. J Alternat Compl Med. (2006) 12:39–44. doi: 10.1089/acm.2006.12.39
87. Kavoussi, B, and Ross, BE. The neuroimmune basis of anti-inflammatory acupuncture. Integr Cancer Ther. (2007) 6:251–7. doi: 10.1177/1534735407305892
88. Borovikova, LV, Ivanova, S, Zhang, M, Yang, H, Botchkina, GI, Watkins, LR, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. (2000) 405:458–62. doi: 10.1038/35013070
90. Pavlov, VA, Wang, H, Czura, CJ, Friedman, SG, and Tracey, KJ. The cholinergic anti-inflammatory pathway: a missing link in neuroimmunomodulation. Mol Med. (2003) 9:125–34.
91. Walters, AS, Ondo, WG, Zhu, W, and Le, W. Does the endogenous opiate system play a role in the restless legs syndrome? A pilot post-mortem study. J Neurol Sci. (2009) 279:62–5. doi: 10.1016/j.jns.2008.12.022
92. Gonzalez-Latapi, P, and Malkani, R. Update on restless legs syndrome: from mechanisms to treatment. Curr Neurol Neurosci Rep. (2019) 19:54. doi: 10.1007/s11910-019-0965-4
93. Uslu, FI, Demir, E, Güler, EM, and Koçyiğit, A. Circulating levels of cytokines are increased in restless legs syndrome. Sleep Breath. (2021) 25:1581–5. doi: 10.1007/s11325-020-02218-7
94. Dowsett, J, Didriksen, M, Von, SJH, Larsen, MH, Thørner, LW, Sørensen, E, et al. Chronic inflammation markers and cytokine-specific autoantibodies in Danish blood donors with restless legs syndrome. Sci Rep. (2022) 12:1672. doi: 10.1038/s41598-022-05658-1
95. Jiménez-Jiménez, FJ, Alonso-Navarro, H, García-Martín, E, and Agúndez, JAG. Inflammatory factors and restless legs syndrome: a systematic review and meta-analysis. Sleep Med Rev. (2023) 68:101744. doi: 10.1016/j.smrv.2022.101744
96. Zeng, B-Y, Salvage, S, and Jenner, P. Current development of acupuncture research in Parkinson's disease. Int Rev Neurobiol. (2013) 111:141–58. doi: 10.1016/B978-0-12-411545-3.00007-9
97. Xiao, D. Acupuncture for Parkinson's disease: a review of clinical, animal, and functional magnetic resonance imaging studies. J Trad Chinese Med. (2015) 35:709–17. doi: 10.1016/s0254-6272(15)30164-3
98. Jiménez-Jiménez, FJ, Ayuso, P, Alonso-Navarro, H, Calleja, M, Díez-Fairén, M, Álvarez, I, et al. Serum trace elements concentrations in patients with restless legs syndrome. Antioxidants (Basel). (2022) 11:272. doi: 10.3390/antiox11020272
99. Jiménez-Jiménez, FJ, Alonso-Navarro, H, García-Martín, E, and Agúndez, JAG. Neurochemical features of idiopathic restless legs syndrome. Sleep Med Rev. (2019) 45:70–87. doi: 10.1016/j.smrv.2019.03.006
Glossary
AC - Acupuncture
AEs - Adverse events
ANCOVA - Analysis of covariance
AP - Acupressure
CI - Confidence interval
CM - Centimeter
COVID-19 - Coronavirus disease 2019
DRKS - Deutsches Register Klinischer Studien (German Clinical Trials Register)
FAS - Full analysis set
GSE - General Self-Efficacy Scale
HADS-D - Hospital Anxiety and Depression Score in German
HT - Hydrotherapy according to Kneipp
IRLSSG - International Restless Legs Syndrome Study Group
IRLS - International Restless Legs Syndrome Study Group Rating Scale
ITT - Intention-to-treat
MCID - Minimal clinically important difference
MD - Mean difference
MID - Minimal important difference
MS - Adjusted means
NYHA - New York Heart Association classification
PGI-C - Patient Global Impressions Scale – Change
QoL - Quality of life
RC - Routine care alone (control group)
RCT - Randomized controlled trial
RLS - Restless legs syndrome
RLSQoL - Restless-Legs-Syndrome Quality of Life questionnaire
SARS-COV-2 - Severe acute respiratory syndrome coronavirus type 2
SGW-B - Subjective Global Wellbeing
SF-12 - Short-Form (12) Health Survey
SPSS - Statistical Package for Social Sciences
TCIM - Traditional Complementary and Integrative Medicine
VAS - Visual analog scale
W - Week
Y - Year(s)
Keywords: restless legs syndrome, complementary and integrative medicine, hydrotherapy, Kneipp therapy, acupressure, randomized controlled trial
Citation: Kubasch J, Ortiz M, Binting S, Roll S, Icke K, Dietzel J, Nögel R, Hummelsberger J, Willich SN, Brinkhaus B, Teut M and Siewert J (2025) Hydrotherapy and acupressure in restless legs syndrome: results of a randomized, controlled, three-armed, pilot study (HYDRAC-study). Front. Med. 12:1571045. doi: 10.3389/fmed.2025.1571045
Edited by:
Pathirage Kamal Perera, University of Colombo, Sri LankaReviewed by:
Félix Javier Jiménez-Jiménez, Hospital Universitario del Sureste, SpainMaria-Eleni Roumelioti, University of New Mexico, United States
Duy-Thai Nguyen, Ministry of Health, Vietnam
Copyright © 2025 Kubasch, Ortiz, Binting, Roll, Icke, Dietzel, Nögel, Hummelsberger, Willich, Brinkhaus, Teut and Siewert. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia Siewert, anVsaWEuc2lld2VydEBjaGFyaXRlLmRl