 Mehlika Bilgi Kirmaci
Mehlika Bilgi Kirmaci Emre Balli
Emre Balli Sezgin Yilmaz
Sezgin Yilmaz- Department of General Surgery, Faculty of Medicine, Afyon Health Sciences University, Afyonkarahisar, Türkiye
Extrahepatic biliary anomalies are rarely diagnosed. These anomalies are usually detected incidentally after investigating clinical findings in patients such as obstructive jaundice, pancreatitis, or biliary tract malignancies. In our study, we describe common bile duct duplication in a patient scheduled for palliative hepaticojejunostomy due to unresectable pancreatic cancer. We are presenting a case with type I common bile duct anomaly.
Introduction
Although congenital anomalies of the bile ducts have been reported with a prevalence of 15% in the literature, congenital duplication of the extrahepatic bile ducts is extremely rare. It is characterized by the presence of a septum in the common bile duct or duplication of the common bile duct. The first case of common bile duct anomaly was identified by Vesalius in 1543, and until 1986, 24 cases were reported in total. Additionally, according to a 2002 article published in Japan, 46 cases have been reported since 1968 (1). Bile tract duplications are associated with biliary lithiasis, choledochelelithiasis, cholangitis, pancreatitis, and upper gastrointestinal tract malignancies (2). Before 2007, four types of bile duct duplication were identified. In 2007, Choi et al. found a new type of bile duct duplication, and this type was named type V (3). In this case report, we will present a rare case of common bile duct duplication in a patient diagnosed with inoperable pancreatic cancer.
Case report
A 78-year-old woman was admitted to our hospital with complaints of abdominal pain, nausea, vomiting, and yellowing of the eyes. In the physical examination; high degree Alzheimer’s disease, the scleras were icteric and there was tenderness in the epigastric region. In the laboratory evaluation of the patient, results were obtained as total Bilirubin 10.4 mg/dL, direct bilirubin 9.0 mg/dL ALP 505 iu/ml Gama Glutamil Transferaz (GGT) 488 iu/ml CA19-92500 u/ml. In ultrasonography, a 5×4 cm hypoechoic lesion with irregular contours was observed in the periampullary region. In contrast-enhanced CT, the largest of metastatic lesions 4×5 cm in the liver’s segment 8, and a 4×5 cm mass at the level of the pancreatic uncinate process extending into the duodenum, surrounding the superior mesenteric vein (SMV) more than 180 degrees, were observed. According to clinical and radiological findings, the patient was diagnosed with an inoperable periampullary tumor that invaded the duodenum. ERCP was planned for biliary passage. During the ERCP procedure, an ulcerous mass surrounding tissues was observed in the region compatible with the papilla, which destroyed the papilla and did not allow placement of a stent, and multiple biopsies were taken from the mass. For biliary drainage, it was decided to perform hepaticojejunostomy. During the operation, type I common bile duct duplication was observed (Figure 1). The patient underwent hepaticojejunostomy, gastroenterostomy, and cholecystectomy, and tru-cut biopsies were taken from the periampullary region and liver during the operation. In the post-operative follow-ups, total bilirubin decreased to 2.2 mg/dL and direct bilirubin decreased to 1.5 mg/dL. The patient’s pathology was identified as indifferent pancreatic adenocarcinoma and liver metastasis. At the oncology council, it was decided to continue the patient’s treatment with chemotherapy. The patient, who suffered from Alzheimer’s disease and had an advanced-stage pancreatic tumor, died 3 months after the operation.
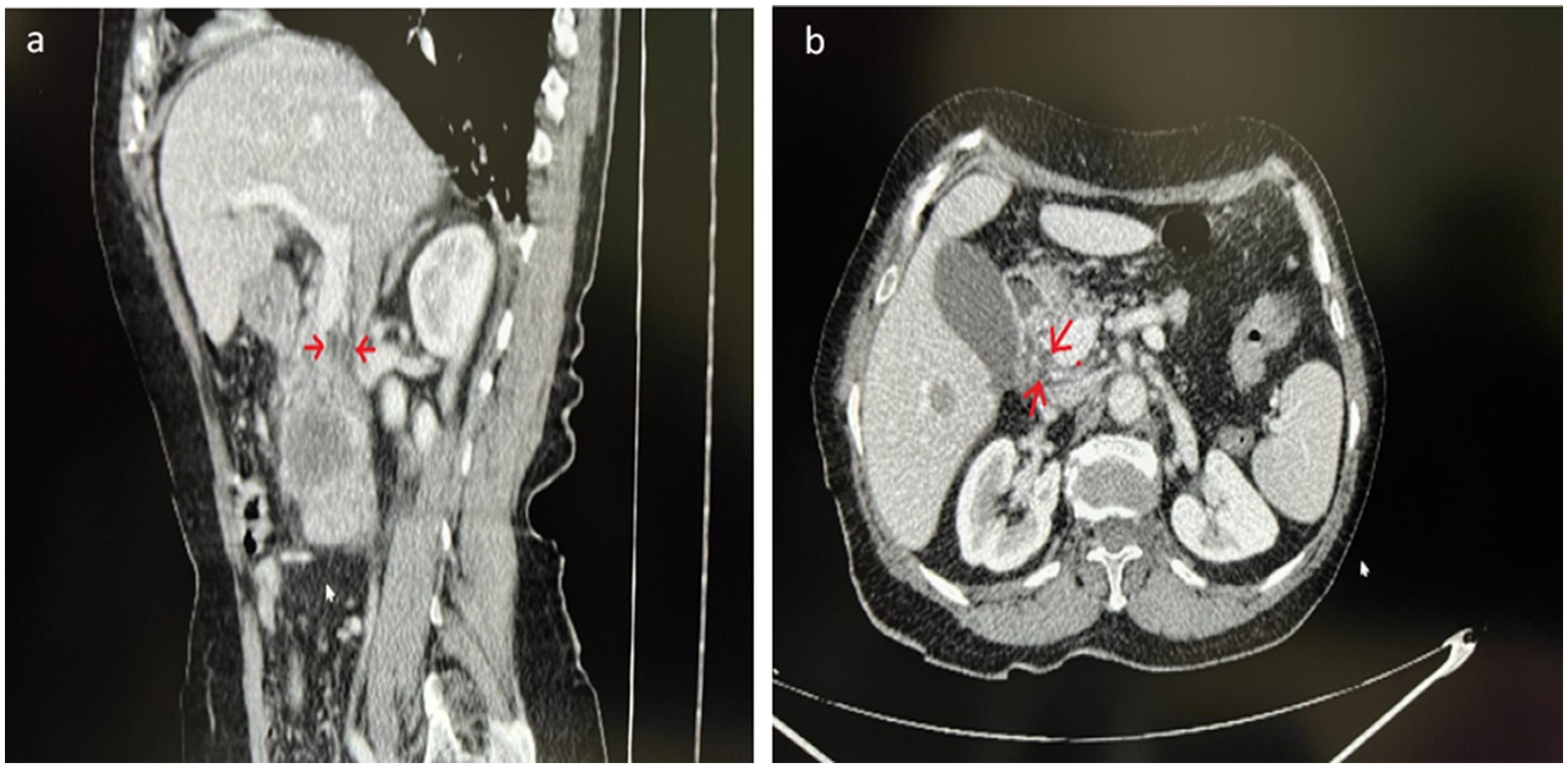
Figure 1. (a) Sagittal vision and (b) axial vision section of the dynamic CT images shows that the septum within the common bile duct. The septum in the common bile duct is seen in the areas marked with arrows.
Discussion
Development of the biliary system is a unique process. The liver, gallbladder, and bile duct system arise as a ventral endodermal outgrowth of the hepatic diverticulum, which develops from the distal part of the foregut in the early 4th week of the intrauterine period. While the liver develops from the tissue bud of the ventral foregut diverticulum, intrahepatic bile ducts form from its cranial part, and the extrahepatic bile tree forms from its caudal part. The small caudal part of the hepatic diverticulum forms the gallbladder, and the stalk of the diverticulum forms the cystic duct.
The extrahepatic bile ducts are initially blocked by endoderm-derived epithelial cells called cholangiocytes. Later, the lumen of these channels is formed due to the vacuolation that occurs with the degeneration of these cells. During this process, as the vacuoles merge, the first two parallel ducts are formed, and then they gradually retract, creating the common bile duct. At the end of this process, double bile ducts are seen in the early stages of the intrauterine period, and a common bile duct consisting of a single common hepatic and bile duct is expected to be seen in the postnatal period (3, 4).
Duplication of the extrahepatic bile duct is one of the rarest congenital variants. Mechanisms involved in this developmental anomaly include impairment in the recanalization of the hepatic primordium, random subdivisions of the hepatic diverticulum during the first week of embryogenesis, and early interruption of double common bile duct (DCBD) development. It regresses in early embryogenesis and with normal development (3, 5, 6).
The first description of DCBD was made by Vesalius in 1543. It is a very rare anomaly, with fewer than 30 cases reported in Western studies from 1,543 to 2007. On the other hand, Yamashita et al. reviewed Japanese literature from 1968 to 2002 and found 46 patients with this anomaly (1). The first classification of this anomaly was made by Goor and Ebert (7) and was later modified by Saito et al. (8). Subsequently, the subtypes made by Choi et al. in 2007 are as follows (3, 7, 8).
The most commonly reported are types III and IV. The least common is type V (9). In our case, we could not visualize a clear biliary tree with ERCP because of the patient’s condition. However, it can be classified as\I variation according to dynamic CT images (Figure 1) and specimen examination (Figure 2).
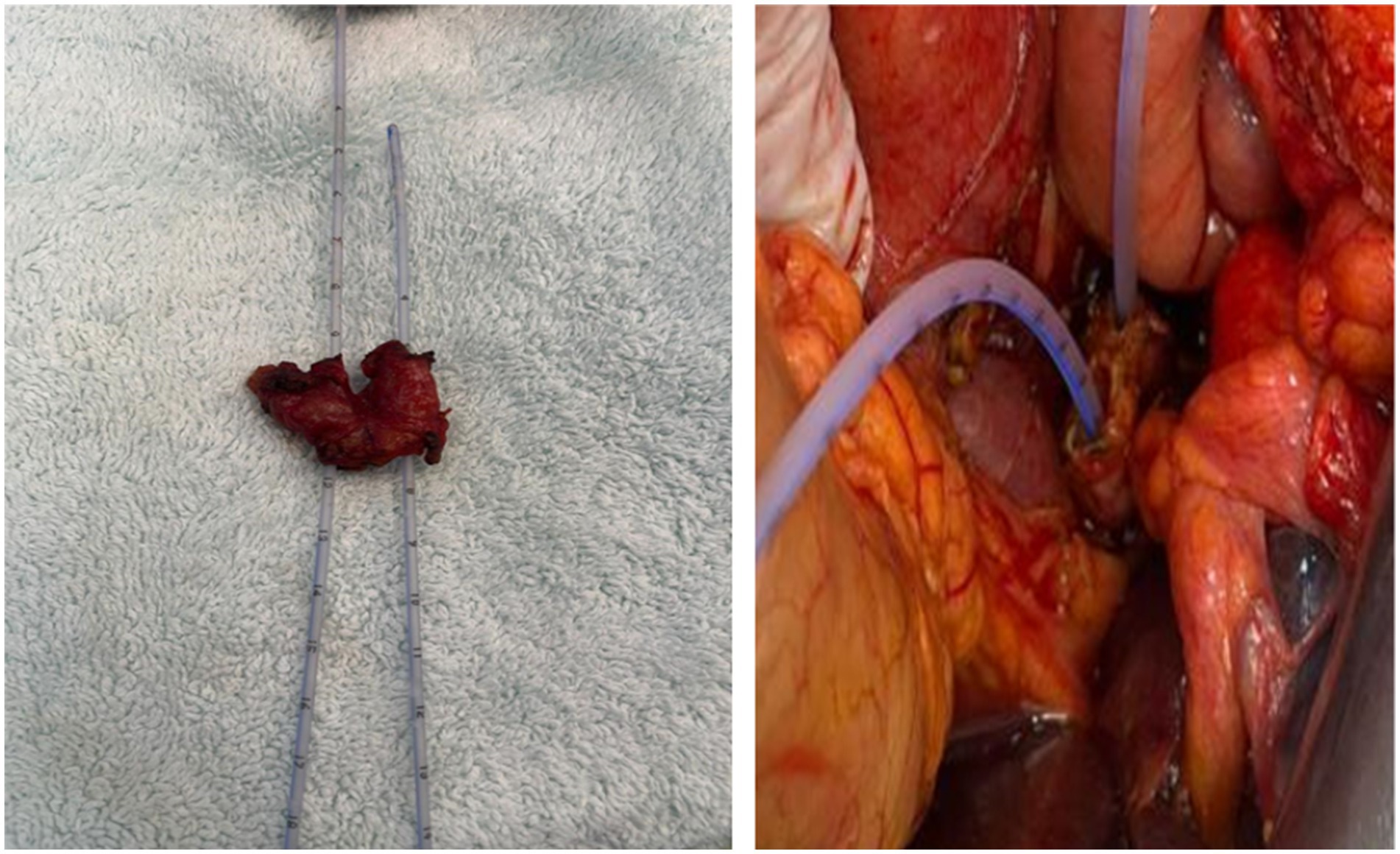
Figure 2. Specimen of the common bile duct with a double lumen. When the common bile duct was cut for hepaticojejunostomy, the catheter was advanced, and the double lumen structure was defined.
Variation in the development of the bile duct is a rare anatomical variation that can cause cholangiopathy and further play a role in the etiology of cancer. Chronic inflammation and fibrosis due to bile flow impairment cause the development of malignancy. Obesity, excessive fatty diet, smoking, alcohol, diabetes mellitus, and hyperlipidemia are other factors that cause biliary tract malignancy (1, 3, 10). However, it cannot be detected with a specific tumor marker. A gene analysis that shows these variations, such as colon or breast cancer, cannot be performed. In patients with bile duct anomalies, clinical findings such as recurrent attacks of biliary cholangitis and attacks of pancreatitis are observed. However, in this case, common bile duct variation was observed during palliative treatment for malignancy. When the patient’s medical history was scanned, no previous clinical findings were found (Table 1).
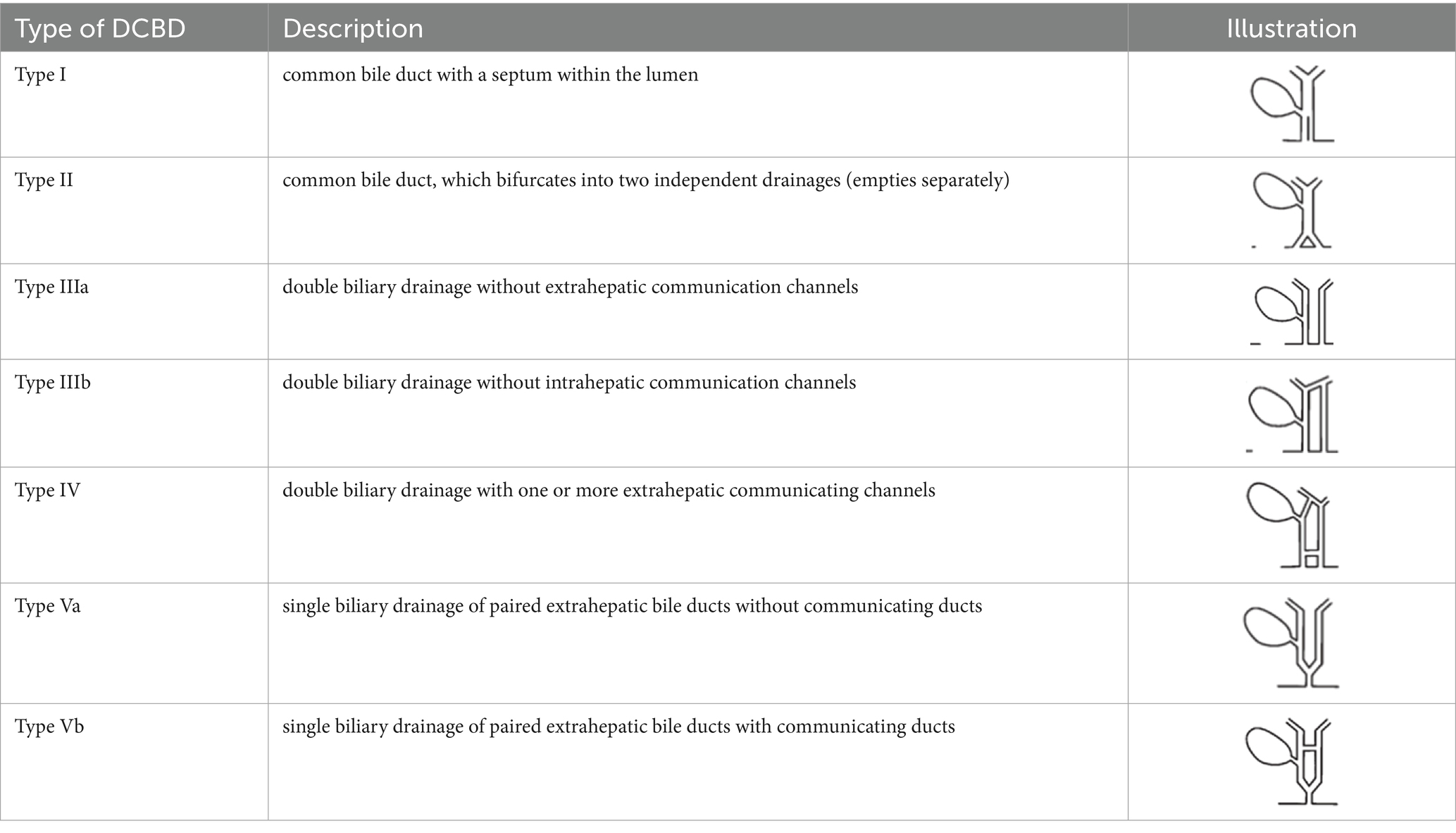
Table 1. Classification of the double extrahepatic bile duct.
Conclusion
In conclusion, recurrent episodes of acute pancreatitis and cholangitis due to sludging or obstruction are seen in cases of impaired bile flow, such as common bile duct or pancreaticobiliary junction anomalies. In these cases, a multidisciplinary approach is required for intensive care follow-up, radiological imaging, endoscopic procedures, and surgical treatment according to the clinical findings of the patient. However, in this case, we observed that such anomalies may cause malignant transformation without any clinical findings.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the studies involving humans because since the study was a Case Report, it was exempt from ethics committee approval. Patient consent form was taken. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
MB: Writing – original draft, Writing – review & editing. EB: Formal analysis, Project administration, Resources, Visualization, Writing – review & editing. MD: Data curation, Investigation, Methodology, Writing – review & editing. SY: Software, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to thank Assoc. Prof. Sevda Lafci Fahrioglu, MD. PhD. (in Anatomy) for her scientific support.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Yamashita, K, Oka, Y, Urakami, A, Iwamoto, S, Tsunoda, T, and Eto, T. Double common bile duct: a case report and a review of the Japanese literature. Surgery. (2002) 131:676–81. doi: 10.1067/msy.2002.124025
2. Hoepfner, L, Sweeney, MK, and White, JA. Duplicated extrahepatic bile duct identified following cholecystectomy injury. J Surg Case Rep. (2016):rjw064. doi: 10.1093/jscr/rjw064
3. Choi, E, Byun, JH, Park, BJ, and Lee, MG. Duplication of the extrahepatic bile duct with abnormal union of the pancreaticobiliary ductal system revealed by MR cholangiopancreatography. Br J Radiol. (2007) 80:e150–4. doi: 10.1259/bjr/50929809
4. Sureka, B, Arora, A, Kasana, V, Patidar, Y, and Bansal, K. Common bile duct duplication: the more the murkier. Saudi J Gastroenterol. (2015) 21:51. doi: 10.4103/1319-3767.151231
5. Nakamura, K, Mitsubuchi, H, and Miyayama, H. Complete absence of bile and pancreatic ducts in a newborn: a new entity of congenital anomaly in hepato-pancreatic development. J Hum Gene. (2003) 48:380–4. doi: 10.1007/s10038-003-0041-3
6. Knisely, AS. Biliary tract malformations. Am J Med Genet A. (2003) 122A:343–50. doi: 10.1002/ajmg.a.20479
7. Goor, DA, and Ebert, PA. Anomalies of the biliary tree. Report of a repair of an accessory bile duct and review of the literature. Arch Surg. (1972) 104:302–9. doi: 10.1001/archsurg.1972.04180030050012
8. Saito, N, Nakano, A, and Arase, M. A case of duplication of the common bile duct with anomaly of the intrahepatic bile duct. Nippon Geka Gakkai Zasshi. (1988) 89:1296–301.
9. Lee, JH, Yu, JS, Park, MS, Dong, SY, and Seok, WY. MR cholangiography of accessory bile duct connected to the stomach. Am J Roentgenol. (2007) 189:W344–7. doi: 10.2214/AJR.05.1570
Keywords: duplication of the common bile duct, bile duct, choledoch duplication, surgery, pancreatic cancer
Citation: Bilgi Kirmaci M, Balli E, Dayanç M and Yilmaz S (2025) Case Report: A rarely observed anomaly of the common bile duct—common bile duct duplication. Front. Med. 12:1584728. doi: 10.3389/fmed.2025.1584728
Edited by:
Phuong Dung (Yun) Trieu, The University of Sydney, AustraliaReviewed by:
Nikolaos Zavras, University General Hospital Attikon, GreeceAdeeb Majid, Calvary Mater, Australia
Copyright © 2025 Bilgi Kirmaci, Balli, Dayanç and Yilmaz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mehlika Bilgi Kirmaci, bWVobGlrYWJpbGdpQGhvdG1haWwuY29t
†ORCID: Mehlika Bilgi Kırmacı, orcid.org/0000-0002-8034-1459